trasplante hepático tratamiento...
TRANSCRIPT

Trasplante hepáticoTRATAMIENTO INMUNSUPRESOR
Manuel L. Rodríguez-PerálvarezFacultativo Especialista de Aparato Digestivo
Sección de Hepatología y Trasplante Hepático
Hospital Universitario Reina Sofía. IMIBIC. CIBERehd
Barcelona, 10-11 Septiembre 2017
PREGUNTA 1
Con respecto al rechazo del injerto tras el trasplante hepático, indique la respuesta CORRECTA:
a) Un episodio de rechazo celular agudo confirmado histológicamente, incluso de grado leve, incrementa el riesgo de rechazo crónico y pérdida del injerto.
b) Ante una elevación de transaminasas en el postrasplante precoz se debe incrementar la dosis de tacrolimus hasta corregir por completo las alteraciones analíticas.
c) El rechazo crónico responde adecuadamente al aumento de la medicación inmunosupresora.
d) Actualmente la tasa de rechazo crónico es <5%
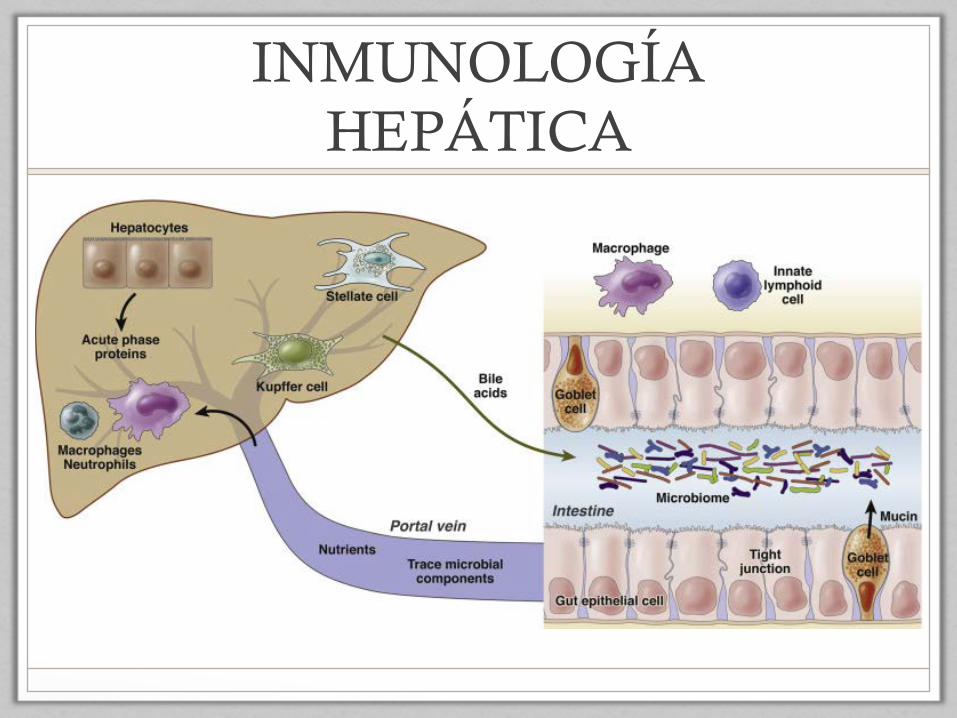
INMUNOLOGÍA HEPÁTICA
exhibited elevated SMRs in all indication groups andamong patients aged 30 or over. SMR for liver diseasewas particularly high in alcoholic liver disease and HCV;this was attributable to disease recurrence in 75% and93%, respectively. SMR for malignancy was particularlyhigh in HCC, followed by HCV and alcoholic liver dis-ease, but not elevated in PBC. Patients with any malig-nant disease as the primary indication for LT showed thehighest SMR for malignancy (Table 4).
Although cardiovascular disease represented the sec-ond most common cause of death overall, its SMRwas significantly elevated only in PBC and alcoholicliver disease and in patients aged 45 to 59. ElevatedSMRs were in particular for ischemic heart disease inboth alcoholic liver disease (SMR 3.43, 95% CI 1.96-5.57) and PBC (7.53, 95% CI 2.44-17.57).
SMR for external causes was elevated in HCV andin female patients. SMR for the subcategory suicide
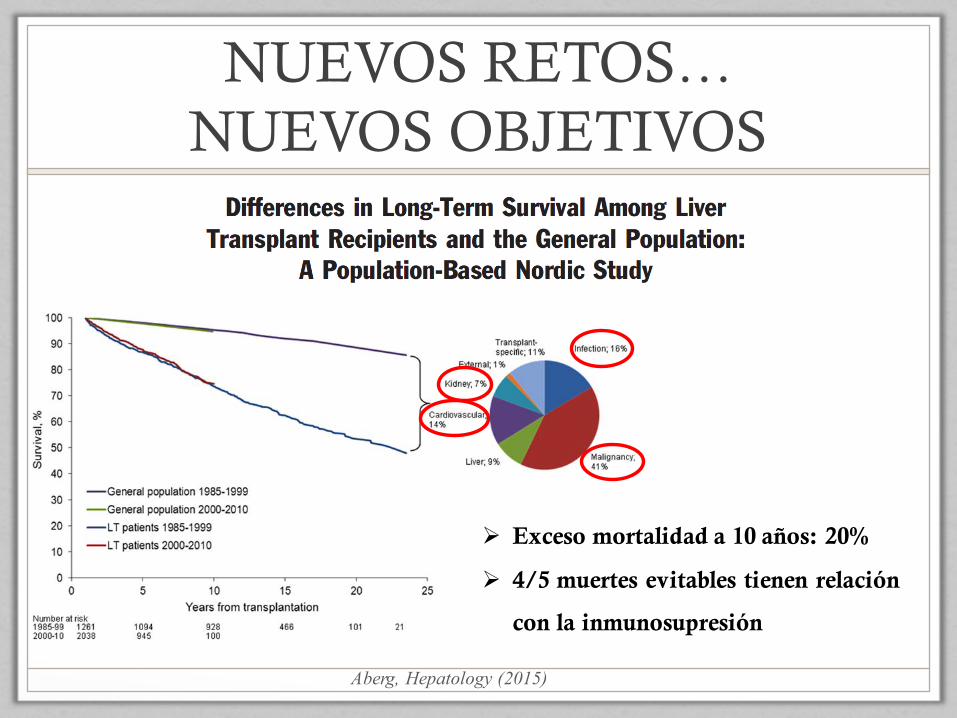
Fig. 1. Patient survival after LTamong 1-year survivors and expectedsurvival based on general populationmortality rates. Pie chart shows thedistribution of causes for the survivalgap, calculated as the differencebetween observed and expectedcause-specific mortality divided by thedifference between observed andexpected all-cause mortality.
Fig. 2. Patient survival after LT according to age at transplantation among 1-year survivors and expected survival based on general populationmortality rates. (A) Patients aged less than 15 years at transplantation; (B) 15-44 years; (C) 45 years and above.
672 ABERG ET AL. HEPATOLOGY, February 2015
NUEVOS RETOS… NUEVOS OBJETIVOS
Aberg, Hepatology (2015)
Ø Exceso mortalidad a 10 años: 20%
Ø 4/5 muertes evitables tienen relación
con la inmunosupresión
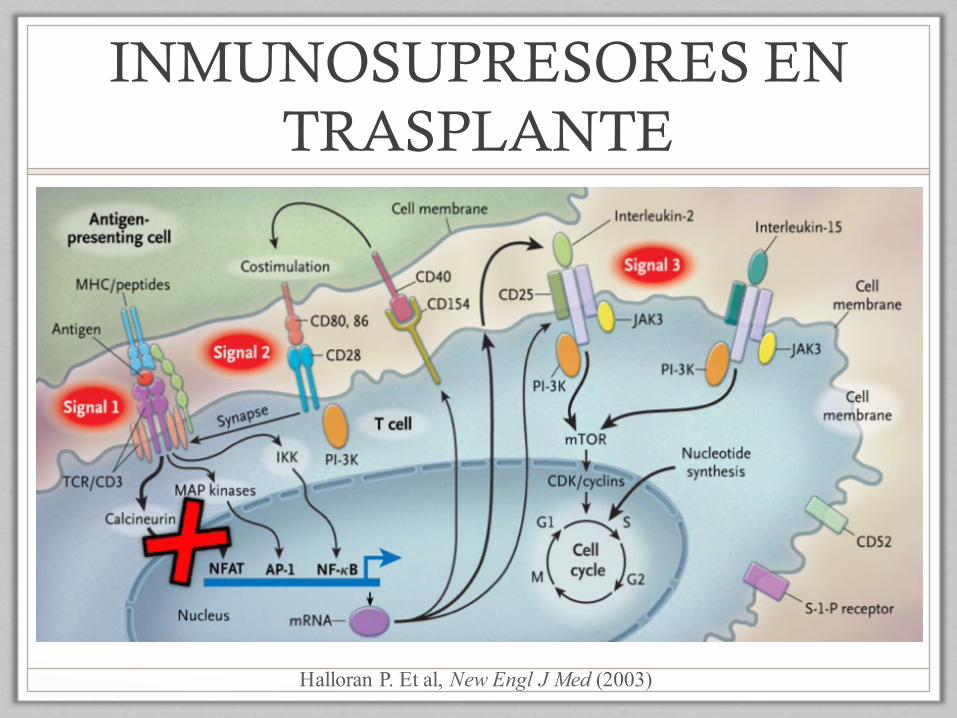
INMUNOSUPRESORES EN TRASPLANTE
Halloran P. Et al, New Engl J Med (2003)
INHIBIDORES CALCINEURINA
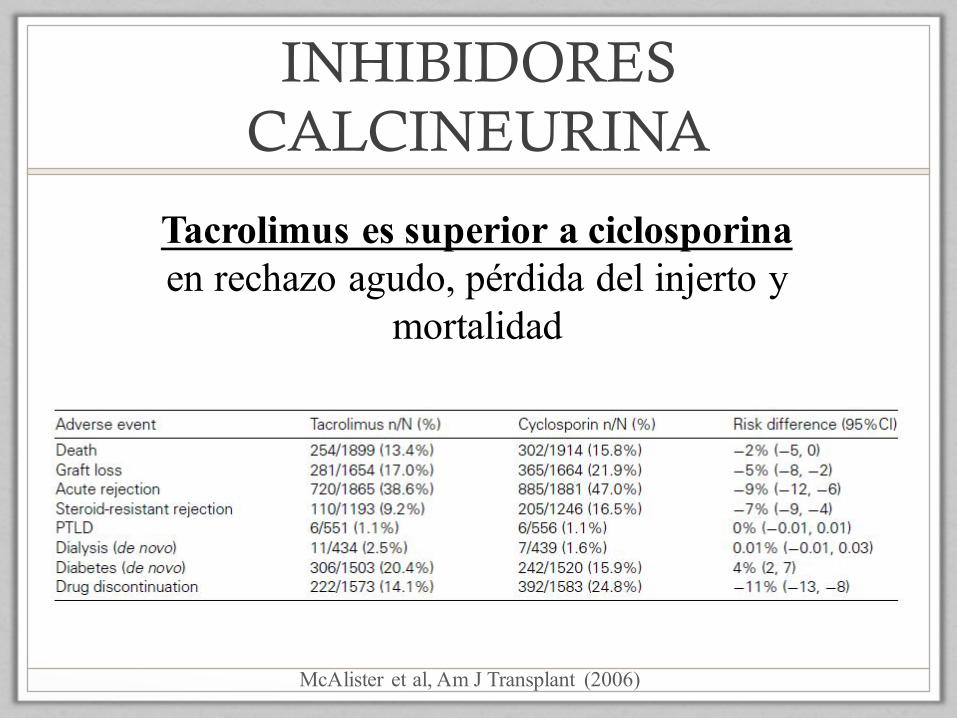
McAlister et al, Am J Transplant (2006)
Tacrolimus es superior a ciclosporinaen rechazo agudo, pérdida del injerto y
mortalidad

PREGUNTA 2
En cuanto a la farmacocinética de tacrolimus, indique la respuesta FALSA:
a) Su eliminación se realiza por vía renal principalmente.
b) Su absorción se produce en intestino delgado, fundamentalmente en duodeno y yeyuno.
c) La biodisponibilidad de tacrolimus es muy variable por lo que precisa de monitorización de niveles.
d) Tacrolimus es metabolizado en hígado y en menor medida en intestino.
<5% de tacrolimus se elimina por vía renal
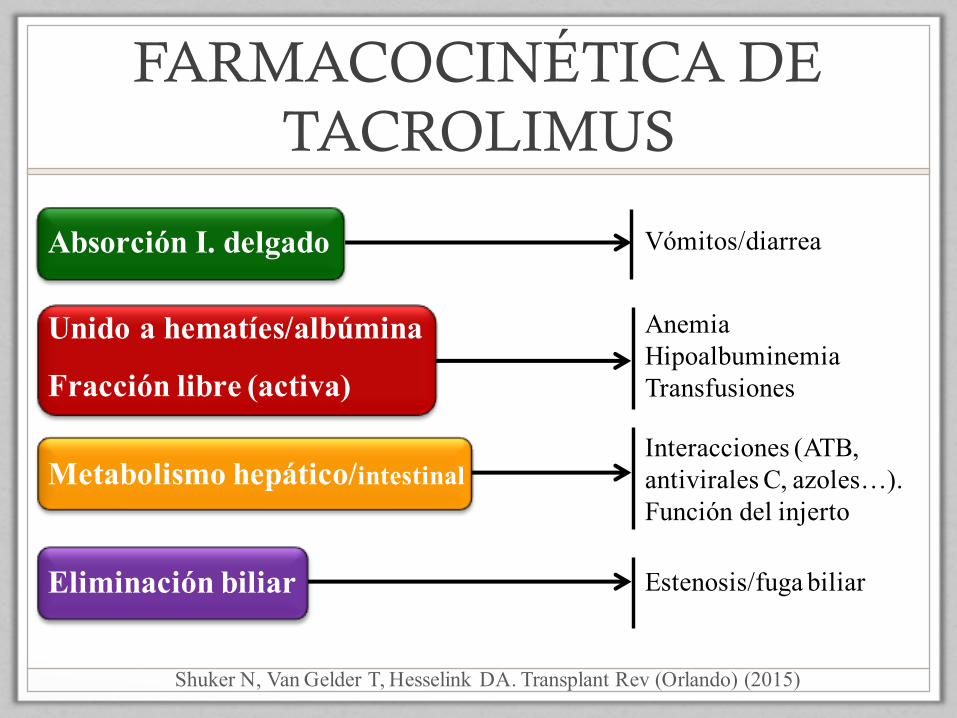
FARMACOCINÉTICA DE TACROLIMUS
Absorción I. delgado
Unido a hematíes/albúmina
Fracción libre (activa)
Metabolismo hepático/intestinal
Eliminación biliar
Shuker N, Van Gelder T, Hesselink DA. Transplant Rev (Orlando) (2015)
Vómitos/diarrea
AnemiaHipoalbuminemiaTransfusiones
Interacciones (ATB, antivirales C, azoles…).Función del injerto
Estenosis/fuga biliar
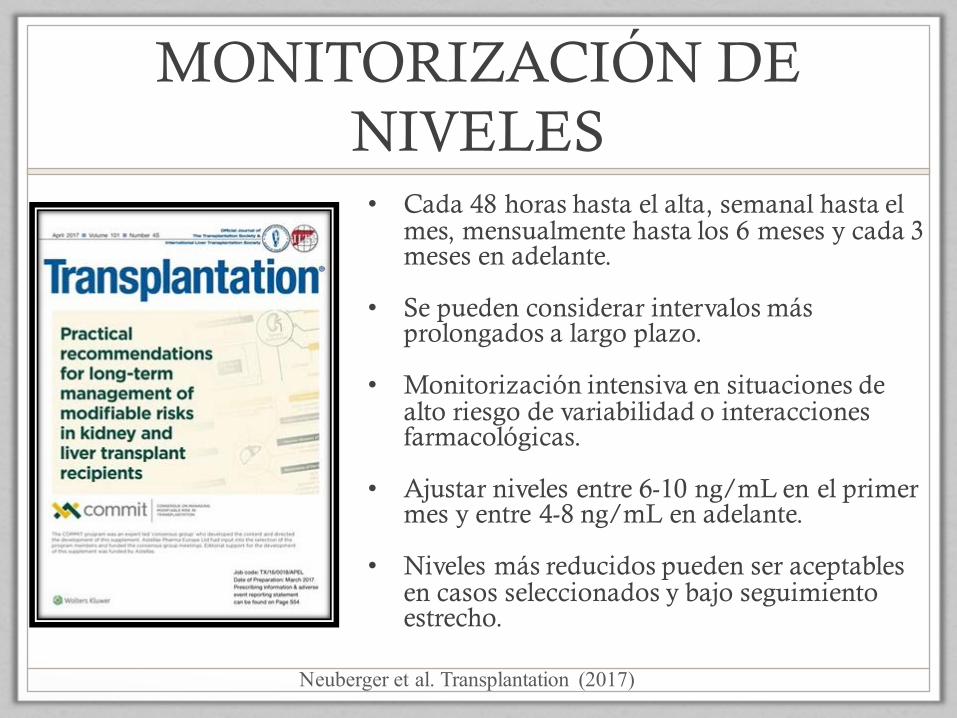
MONITORIZACIÓN DE NIVELES• Cada 48 horas hasta el alta, semanal hasta el
mes, mensualmente hasta los 6 meses y cada 3 meses en adelante.
• Se pueden considerar intervalos más prolongados a largo plazo.
• Monitorización intensiva en situaciones de alto riesgo de variabilidad o interacciones farmacológicas.
• Ajustar niveles entre 6-10 ng/mL en el primer mes y entre 4-8 ng/mL en adelante.
• Niveles más reducidos pueden ser aceptables en casos seleccionados y bajo seguimiento estrecho.
Neuberger et al. Transplantation (2017)
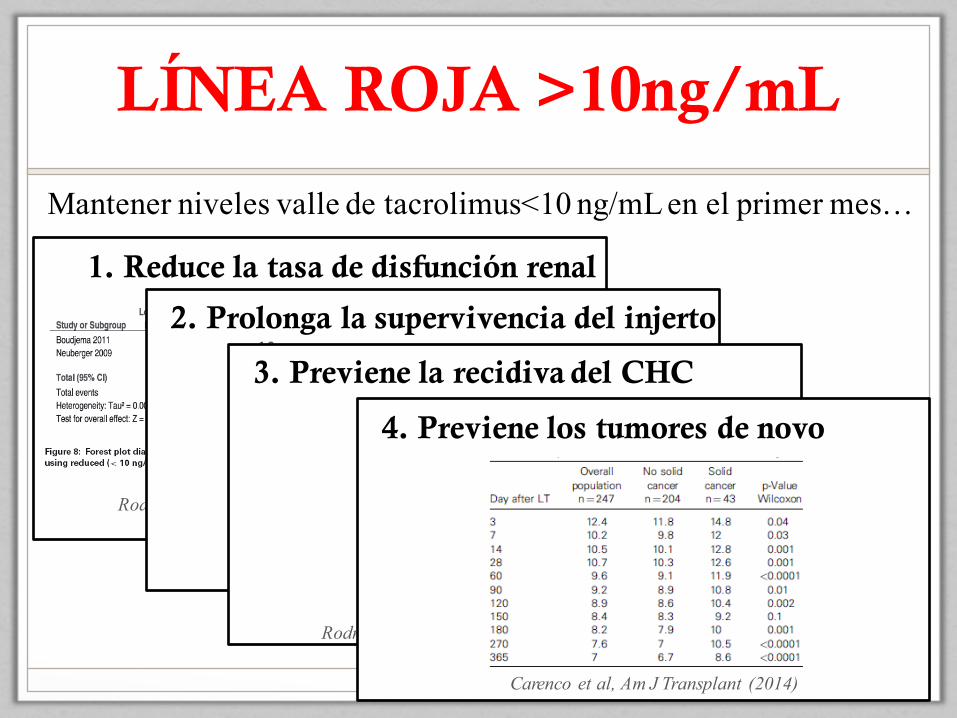
LÍNEA ROJA >10ng/mL
1. Reduce la tasa de disfunción renal
Rodríguez-Perálvarez et al, Am J Transplant (2012)
2. Prolonga la supervivencia del injerto
Rodríguez-Perálvarez et al, J Hepatol (2013)
3. Previene la recidiva del CHC
Rodríguez-Perálvarez et al, J Hepatol (2013)
4. Previene los tumores de novo
Carenco et al, Am J Transplant (2014)
Mantener niveles valle de tacrolimus<10 ng/mL en el primer mes…

INMUNOSUPRESORES EN TRASPLANTE
Halloran P. Et al, New Engl J Med (2003)

LA PAREJA DE BAILE
BASILIXIMAB MICOFENOLATO EVEROLIMUS
DOSIS Dos dosis 20 mg(día 0 y día +5)
1 gr/12 horas Inicio 0,75 mg/12h(ajustar niveles 3-8)
POTENCIA +++ + ++
COBERTURA <7 DIAS NORESTRICCIONES
>1er MES
VENTAJAS Retraso inicio TAC No permite monoterapia*
Buena potenciaPermite monoterapia
a largo plazo*
PROBLEMAS InfeccionesEvita tolerancia?
Efectos gastrointest.Citopenias
CicatrizaciónPerfil seguridad
*En la mayoría de los casos

OPCIONES DE COMBINACIÓN
¿?
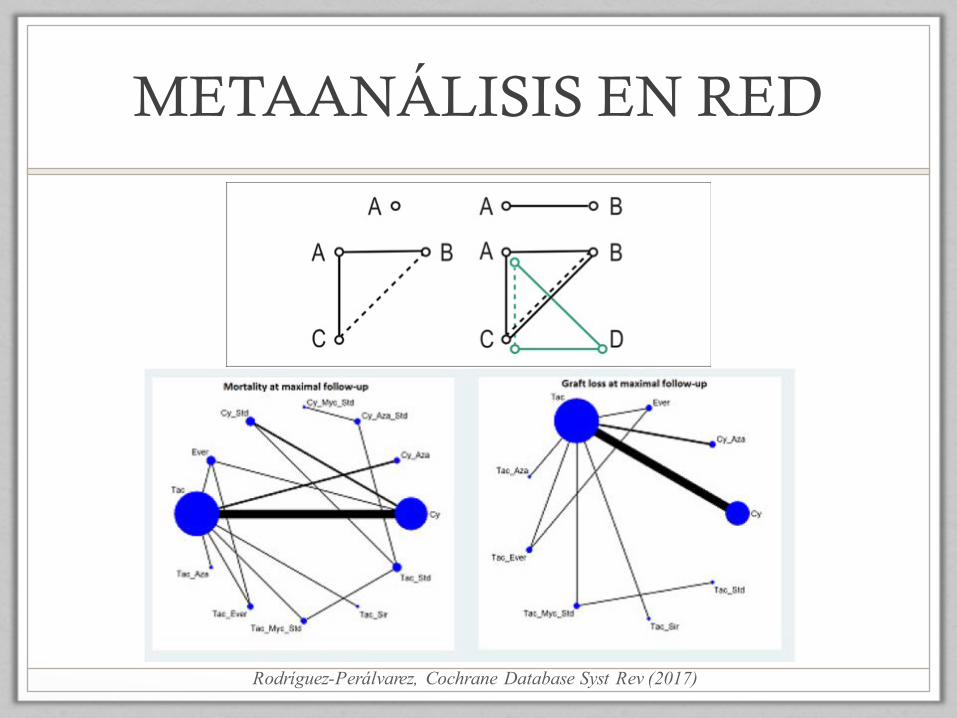
METAANÁLISIS EN RED
Rodríguez-Perálvarez, Cochrane Database Syst Rev (2017)
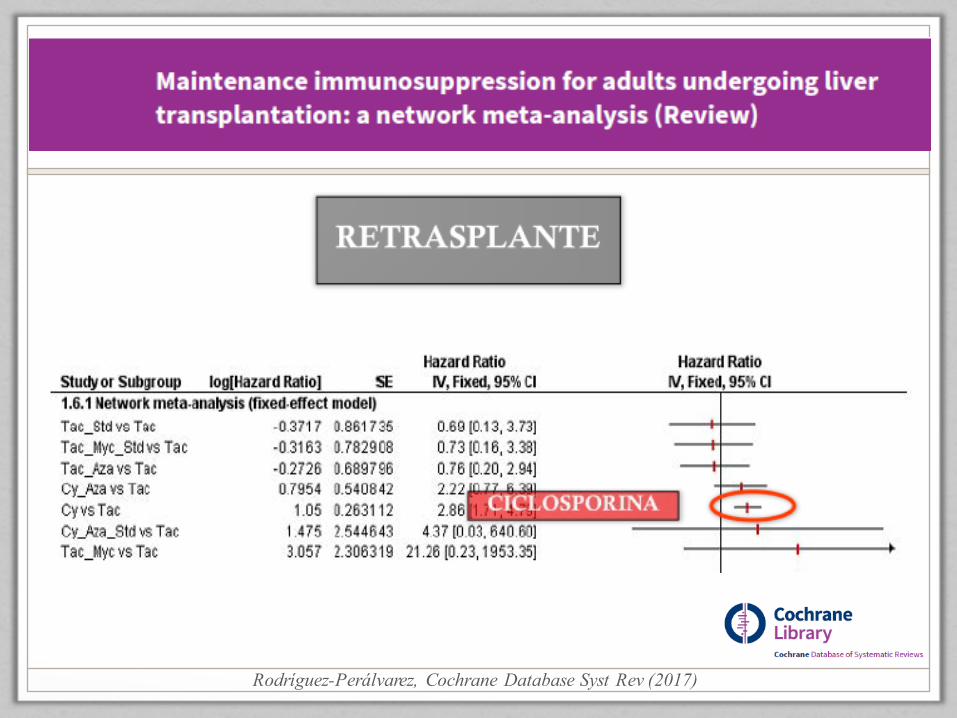
Rodríguez-Perálvarez, Cochrane Database Syst Rev (2017)

Rodríguez-Perálvarez, Cochrane Database Syst Rev (2017)

Rodríguez-Perálvarez, Cochrane Database Syst Rev (2017)
• Se deben evitar protocolos de inmunosupresión basados en sirolimus y en ciclosporina ya que ocasionan mayor mortalidad y retrasplante.
• Los protocolos basados en tacrolimus parecen ser más eficaces y seguros.
• Se precisan estudios con mayor calidad metodológica.


PERFILES DE PACIENTES
BAJO RIESGO DE RECHAZO
DISFUNCIÓN RENAL
COMPLIC. METABÓLICAS
RIESGO TUMORES
ALTO RIESGO DE RECHAZO
- Edad >60 años- MELD muy elevado- Desnutrido- Mala situación clínica
- Disfunción renal pretrasplante.
- DM, HTA- MELD elevado
- Indicación por NASH- DM, HTA mal
control- Dislipemia, obesidad
- Hepatocarcinoma- Cirrosis etílica- Fumador activo
- CEP, CBP o HAI- Retrasplante por
rechazo crónico- Jóvenes con buena
función hepática
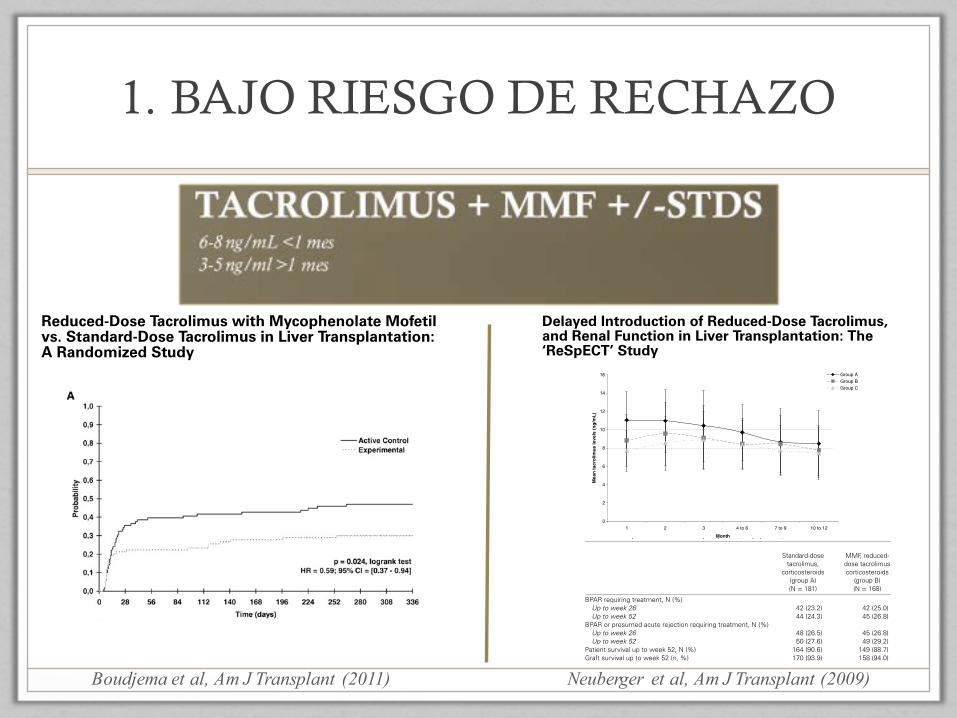
1. BAJO RIESGO DE RECHAZO
Boudjema et al, Am J Transplant (2011)
American Journal of Transplantation 2011; 11: 965–976Wiley Periodicals Inc.
C⃝ 2011 The AuthorsJournal compilation C⃝ 2011 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2011.03486.x
Reduced-Dose Tacrolimus with Mycophenolate Mofetilvs. Standard-Dose Tacrolimus in Liver Transplantation:A Randomized Study
K. Boudjemaa,∗, C. Camusb, F. Salibac,Y. Calmusd, E. Salamee, G. Pageauxf, C. Ducerfg,C. Duvouxh, C. Moucheli,j, A. Renaulti,j, P.Compagnona, R. Lorhok and E. Bellissanti,j
aService de Chirurgie Hepatobiliaire et Digestive, Hopitalde Pontchaillou, Centre Hospitalier Universitaire,Universite de Rennes 1, Rennes, FrancebService de Maladies Infectieuses et ReanimationMedicale, Hopital de Pontchaillou, Centre HospitalierUniversitaire, Universite de Rennes 1, Rennes, FrancecCentre Hepato-biliaire, Serviced’Hepato-gastro-enterologie, Hopital Paul Brousse,Assistance Publique Hopitaux de Paris, Universite ParisXI, Villejuif, FrancedPole Medico-chirurgical d’Hepato-gastro-enterologie,Unite Fonctionnelle de Transplantation Hepatique, HopitalCochin, Assistance Publique Hopitaux de Paris, UniversiteParis 5, Paris, FranceeDepartement de Chirurgie Digestive et deTransplantation Hepatique, Hopital de la Cote de Nacre,Centre Hospitalier Universitaire, Universite de Caen,Caen, FrancefService d’Hepato-gastro-enterologie et TransplantationHepatique, Hopital St Eloi, Centre HospitalierUniversitaire, Universite de Montpellier 1, Montpellier,FrancegService de Chirurgie Digestive et Transplantation, Hopitalde la Croix Rousse, Hospices Civils de Lyon, Universite deLyon 1, Lyon, FrancehService d’Hepato-gastro-enterologie, Hopital HenriMondor, Assistance Publique Hopitaux de Paris,Universite Paris 12, Creteil, FranceiService de Pharmacologie Clinique, Hopital dePontchaillou, Centre Hospitalier Universitaire, Universitede Rennes 1, Rennes, FrancejCentre d’Investigation Clinique INSERM 0203, Hopital dePontchaillou, Centre Hospitalier Universitaire, Universitede Rennes 1, Rennes, FrancekService des Maladies du Foie, Hopital de Pontchaillou,Centre Hospitalier Universitaire, Universite de Rennes 1,Rennes, France*Corresponding author: Karim Boudjema,[email protected]
We conducted a multicenter randomized study in livertransplantation to compare standard-dose tacrolimusto reduced-dose tacrolimus with mycophenolatemofetil to reduce the occurrence of tacrolimus side ef-
fects. Two primary outcomes (censored criteria) weremonitored during 48 weeks post-transplantation: oc-currence of renal dysfunction or arterial hypertensionor diabetes (evaluating benefit) and occurrence ofacute graft rejection (evaluating risk). Interim analyseswere performed every 40 patients to stop the studyin the case of increased risk of graft rejection. Onehundred and ninety-five patients (control: 100; exper-imental: 95) had been included when the study wasstopped. Acute graft rejection occurred in 46 (46%) and28 (30%) patients in control and experimental groups,respectively (HR = 0.59; 95% CI: [0.37–0.94]; p = 0.024).Renal dysfunction or arterial hypertension or diabetesoccurred in 80 (80%) and 61 (64%) patients in con-trol and experimental groups, respectively (HR = 0.68;95% CI: [0.49–0.95]; p = 0.021). Renal dysfunction oc-curred in 42 (42%) and 23 (24%) patients in controland experimental groups, respectively (HR = 0.49; 95%CI: [0.29–0.81]; p = 0.004). Leucopoenia (p = 0.001),thrombocytopenia (p = 0.017) and diarrhea (p = 0.002)occurred more frequently in the experimental group.Reduced-dose tacrolimus with mycophenolate mofetilreduces the occurrence of renal dysfunction and therisk of graft rejection. This immunosuppressive regi-men could replace full-dose tacrolimus in adult livertransplantation.
Key words: Diabetes mellitus, graft rejection, hyper-tension, immunosuppression, mycophenolate mofetil,renal insufficiency, tacrolimus
Abbreviations: CI, confidence interval; CNI, calcineurininhibitor; DSMB, data and safety monitoring board; HR,hazard ratio; MMF, mycophenolate mofetil; OR, odds-ratio.
Received 28 August 2010, revised 18 November 2010and accepted for publication 14 December 2010
Introduction
Long-term immunosuppression using CNIs is essentialto patients undergoing liver transplantation. Randomizedstudies have revealed lower graft rejection rates withtacrolimus than cyclosporine (1–3). According to the man-ufacturer’s recommendations, an initial oral dose of 0.15mg/kg must be administered to obtain whole blood troughlevels between 10 and 20 ng/mL.
965
Reduced-Dose FK + MMF in Liver Transplantation
Figure 2: (A) Kaplan–Meier distribu-tions of occurrence of acute graft re-jection (risk) and (B) Kaplan–Meierdistributions of occurrence of renaldysfunction or arterial hypertensionor diabetes (benefit).
limit of the designed range throughout the study, whilethey tended to decrease in the control group, approachingthe lower limits of the designed range (Figure 4B).
Adverse eventsNo between-group differences were observed except fordiarrhea (p = 0.002), leucopenia (p = 0.001), and throm-bocytopenia (p = 0.017), which were more frequent in theexperimental group. Results are summarized in Table 4. In
the 28 (29%) experimental patients who had leucopenia,the daily dose of MMF was 2, 2.5 and 3 g for 18, 1 and 9patients, respectively. In the 11 (11%) control patients whohad leucopenia, 4 received MMF at a daily dose of 1.5 g for1 patient and 3 g for 3. In the 13 (14%) experimental pa-tients who had thrombocytopenia, the daily dose of MMFwas 2 g or less and 3 g for 7 and 6 patients, respectively.In the 4 (4%) control patients who had thrombocytopenia,none received MMF.
American Journal of Transplantation 2011; 11: 965–976 969
American Journal of Transplantation 2009; 9: 327–336Wiley Periodicals Inc.
C⃝ 2009 The AuthorsJournal compilation C⃝ 2009 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2008.02493.x
Delayed Introduction of Reduced-Dose Tacrolimus,and Renal Function in Liver Transplantation: The‘ReSpECT’ Study
J. M. Neubergera,∗, R. D. Mamelokb,P. Neuhausc, J. Pirenned, D. Samuele,H. Isoniemif, L. Rostaingg, A. Rimolah,S. Marshalli and A. D. Mayera for The ReSpECTStudy Group
aLiver Unit, Queen Elizabeth Hospital, Birmingham, UKbMamelok Consulting, Palo Alto, CAcDepartment of General, Visceral and TransplantationSurgery, Virchow Clinic, Charite-University MedicineBerlin, Berlin, GermanydAbdominal Transplant Surgery Department, UniversityHospital Leuven, Leuven, BelgiumeCentre Hepatobiliaire, Hopital Paul Brousse, UniversityParis XI, Villejuif, FrancefTransplantation and Liver Surgery Clinic, HelsinkiUniversity Hospital, Helsinki, FinlandgMultiorgan Transplant Unit, CHU Rangueil, UniversityHospital, Toulouse, FrancehLiver Unit, Hospital Clınic, IDIBAPS, CIBEREHD,Barcelona, SpainiF. Hoffmann-La Roche Ltd, Basel, Switzerland∗Corresponding author: James M. Neuberger,[email protected]
We report a multicenter, prospective, randomized,open-label trial investigating the effect of lower levelsand delayed introduction of tacrolimus on renal func-tion in liver transplant recipients. Adult patients withgood renal function undergoing primary liver trans-plant were randomized to either: group A (standard-dose tacrolimus [target trough levels >10 ng/mL] andcorticosteroids; n = 183); group B (mycophenolatemofetil [MMF] 2g/day, reduced-dose tacrolimus [targettrough levels ≤8 ng/mL], and corticosteroids; n = 170);group C (daclizumab induction, MMF, reduced-dosetacrolimus delayed until the fifth day posttransplantand corticosteroids, n = 172). The primary endpointwas change from baseline in estimated glomerular fil-tration rate (eGFR) at 52 weeks. The eGFR decreasedby 23.61, 21.22 and 13.63 mL/min in groups A, B and C,respectively (A vs C, p = 0.012; A vs B, p = 0.199). Renaldialysis was required less frequently in group C versusgroup A (4.2% vs. 9.9%; p = 0.037). Biopsy-proven acuterejection rates were 27.6%, 29.2% and 19.0%, respec-tively. Patient and graft survival was similar. In conclu-sion, daclizumab induction, MMF, corticosteroids anddelayed reduced-dose tacrolimus was associated withless nephrotoxicity than therapy with standard-dose
tacrolimus and corticosteroids without compromisingefficacy or tolerability.
Key words: Delayed tacrolimus, immunosuppression,liver transplantation, renal failure
Recieved 04 July 2008, revised 17 September 2008 andaccepted for publication 28 September 2008
Introduction
Although outcomes after liver transplantation are usuallyexcellent, with current 5- and 10-year patient survival ratesexceeding 70% and 60% (1,2), late complications remainof concern. Renal dysfunction remains a major cause ofboth morbidity and mortality (3). Significant renal impair-ment, occurring in up to 27% of liver allograft recipients at5 years (4,5), results in end-stage renal disease in as manyas 10% of patients at 10 years posttransplant (4) and latechronic renal dysfunction or renal failure is associated withthe risk of premature death (3–6).
Late renal failure is associated with both pre- and postlivertransplant factors, including higher concentrations of CNIsboth early and late posttransplant (7,8) and can be pre-dicted by creatinine levels in the first posttransplant year(9,10). Strategies to minimize the adverse renal effects ofCNIs in patients include reducing the CNI dose (11–14)or complete withdrawal of the CNI (14,15), while addingother immunosuppressive agents such as mycophenolatemofetil (MMF) (12–14,16) or sirolimus (11,15). Alterna-tively, a preemptive strategy may be adopted by attemptingto avoid CNI-induced renal impairment. Antibody inductiontherapy (such as interleukin-2 [IL2] receptor antagonists)may allow reduction in dose or delayed introduction of CNIs(17–19).
We conducted the ReSpECT study, a prospective, ran-domized trial in de novo adult liver transplant patientswith good renal function pretransplant, to assess theeffect on renal function, acute rejection, and graft andpatient survival of three regimens: standard-dosetacrolimus and corticosteroids; MMF with reduced-dosetacrolimus and corticosteroids; and induction with da-clizumab, MMF and delayed introduction of reduced-dosetacrolimus and corticosteroids.
327
Neuberger et al, Am J Transplant (2009)
Delayed Tacrolimus and OLT—ReSpECT Study
0
2
4
6
8
10
12
14
16
1 2 3 4 to 6 7 to 9 10 to 12
Month
Mea
n ta
crol
imus
leve
ls (n
g/m
L)
Group AGroup BGroup C
Figure 2: Mean (SD) whole blood tacrolimus trough levels in liver allograft recipients treated with standard-dose tacrolimusand corticosteroids (group A); MMF, reduced-dose tacrolimus and corticosteroids (group B); or daclizumab induction, MMF,reduced-dose tacrolimus given 5 days after transplantation and corticosteroids (group C). Patient numbers at month 1, 2, 3, 4–6,7–9 and 10–12 were 181, 155, 133, 134, 118 and 115, respectively, in group A, 168, 151, 122, 134, 121 and 113, respectively, in group Band 161, 151, 127, 131, 123 and 120, respectively, in group C. The gray lines represent the minimum target trough level for the standardtherapy group and the maximum target trough level for the groups receiving MMF.
on equivalence to prednisolone) for groups A, B and Cwere 25.5 ± 28.9, 22.3 ± 23.8, and 24.7 ± 44.0 mg; at 5–6 months 11.3 ± 11.5, 9.1 ± 10.1, and 22.5 ± 110.9 mgand 8.3 ± 11.4, 7.6 ± 7.3 and 24.8 ± 156.3 mg (9–12months). Cumulative dose was 13.8, 13.5 and 13.1 mg/kgat 1 month; 40.3, 37.2 and 35.2 mg/kg at 5–6 months; and55.0, 58.3 and 49.4 mg/kg at 9–12 months.
Concomitant medicationAlmost all patients (≥99%) received concomitant medi-cation. The use of nonsteroidal anti-inflammatory drugs(NSAIDs) and aminoglycoside antimicrobials was similar ineach group.
Renal functionThe change from baseline at week 52 in calculated creati-nine clearance was significantly smaller (p = 0.012) in pa-tients who received delayed introduction of reduced-dosetacrolimus (group C) than those in group A, whereas therewas no statistically significant between-group differencefor patients in groups A and B (p = 0.199) (Figure 3A).
Sensitivity analyses were performed as described in themethods. The type of sensitivity analysis performed didnot affect the primary efficacy comparison. PP populationanalysis of the change from baseline in calculated creati-nine clearance is shown in Figure 3B. The group C regimen
was also associated with less renal function impairmentthan the standard tacrolimus regimen at earlier time points.The decrease from baseline in calculated creatinine clear-ance was smaller (p < 0.001) in this group than in group Aat week 13 (−13.23 vs. −25.96 mL/min) and 26 (−12.36vs. −26.88 mL/min).
Changes in renal function assessed by estimating GFRbased on the abbreviated MDRD formula (Table 2) wereconsistent with those based on the Cockcroft–Gault for-mula. There was a positive and significant correlation be-tween estimated GFR by Cockcroft–Gault versus MDRDformula (R2 = 0.7112, p < 0.0001).
Increases from baseline in serum creatinine levels weresignificantly smaller in groups B and C than group A, ex-cept at week 26, where changes in group B were not sta-tistically different (p = 0.081) from group A (Table 2). Signif-icantly, fewer patients required dialysis between weeks 2and 52 in group C (n = 7; 4.2%) than group A (n = 18;9.9%) [p = 0.0367], but the between group difference be-tween groups A and B (n = 7; 4.2%) was not statisticallysignificant (p = 0.0558).
Other endpointsOther endpoints are summarized in Table 2. There were noclinically significant differences between groups A and B
American Journal of Transplantation 2009; 9: 327–336 331
Delayed Tacrolimus and OLT—ReSpECT Study
Table 2: Primary and selected secondary endpoints (FAS population)
Daclizumab induction,Standard-dose MMF, reduced- MMF, delayed
tacrolimus, dose tacrolimus reduced-dosecorticosteroids corticosteroids tacrolimus and
(group A) (group B) corticosteroids (group C)(N = 181) (N = 168) (N = 168)
Mean (± SD) baseline GFR based on MDRD-4 (mL/min)1 93.46 (39.63) 95.89 (36.81) 86.71 (29.20)Mean (± SD) change from baseline in GFR −24.89 (36.45) −22.60 (35.5) −14.62 (29.17)
based on MDRD-4 at week 52 (mL/min)1Mean (± SD) baseline GFR based on the 101.83 (44.16) 104.31(± 37.15) 96.51 (± 34.94)
Cockcroft–Gault formula at (mL/min)Mean (95%CI) change from baseline in GFR based −23.61 −21.22 −13.63∗
on the Cockcroft–Gault formula at week 52 (mL/min)(−28.60, −18.62) (−26.12, −16.32) (−17.96, −9.30)
Mean (± SD) baseline serum creatinine levels (ng/mL) 0.97 (0.35) 0.92 (0.27) 1.00 (0.36)Mean (95%CI) change from baseline in
serum creatinine levels (ng/mL)Week 13 0.22 0.16 0.11
(0.16, 0.29) (0.10, 0.21)∗ (0.04, 0.18)∗∗
Week 26 0.23 0.19 0.11(0.16, 0.31) (0.12, 0.25) (0.01, 0.21)∗
Week 52 0.23 0.17 0.12(0.17, 0.29) (0.12, 0.22)∗∗ (0.06, 0.19)∗
Number of episodes of BPAR or presumedacute rejection during 52 weeks, N (%)
0 episodes 119 (65.7) 106 (63.1) 124 (73.8)1 episode 51 (28.2) 52 (31.0) 39 (23.2)2 episodes 10 (5.5) 8 (4.8) 5 (3.0)3 episodes 1 (0.6) 1 (0.6) 0>3 episodes 0 1 (0.6) 0
BPAR requiring treatment, N (%)Up to week 26 42 (23.2) 42 (25.0) 25 (14.9)∗
Up to week 52 44 (24.3) 45 (26.8) 28 (16.7)BPAR or presumed acute rejection requiring treatment, N (%)
Up to week 26 48 (26.5) 45 (26.8) 29 (17.3)∗
Up to week 52 50 (27.6) 49 (29.2) 32 (19.0)Patient survival up to week 52, N (%) 164 (90.6) 149 (88.7) 157 (93.5)Graft survival up to week 52 (n, %) 170 (93.9) 158 (94.0) 156 (92.9)Recurrence of liver disease at week 52, N (%) 7 (9.7) 10 (14.9) 15 (22.1)∗
Composite endpoint of renal function and 167 (92.3) 151 (89.9) 130 (77.4)∗∗∗
graft-related outcomes2 (n, %)
BPAR = biopsy-proven acute rejection; GFR = glomerular filtration rate; MDRD = modification of diet in renal disease.1 Post hoc analysis.2 The composite secondary efficacy parameter was a 20% or greater decrease from baseline in calculated creatinine clearance, or acuterejection, or graft loss or death.∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001 versus group A.
dose used in our study was agreed based on experiencefrom renal allograft recipients (28). Although the combina-tion of tacrolimus and MMF is not currently licensed foruse in liver transplant recipients, they are commonly co-prescribed (2) and are an effective combination (29–33). Inaddition, there was a relatively high rate of withdrawal, es-pecially in group A where many patients were withdrawnso mycophenolate could be given. To address these con-cerns, we defined, post hoc, a ‘per protocol’ set of patientswhere levels of tacrolimus achieved were within 10% oftarget; in this smaller group of patients, similar conclusionswere reached.
There was no significant adverse impact from the tworeduced-dose tacrolimus treatment regimes (B and C), aspatient and graft loss were similar and there was no in-creased risk of infection, or biopsy-proven or treated rejec-tion. Our study was not designed to evaluate the effect ofinduction therapy, so it is not possible to exclude an effectof IL2-receptor on the overall rate of rejection in group C.Moreover, the mechanism underlying the benefits in renalfunction conferred by delayed introduction of tacrolimusremains to be fully elucidated. It is possible that the kid-ney, put at risk by reperfusion and/or in combination withother transplant-related events, is more susceptible to the
American Journal of Transplantation 2009; 9: 327–336 333
Delayed Tacrolimus and OLT—ReSpECT Study
Table 2: Primary and selected secondary endpoints (FAS population)
Daclizumab induction,Standard-dose MMF, reduced- MMF, delayed
tacrolimus, dose tacrolimus reduced-dosecorticosteroids corticosteroids tacrolimus and
(group A) (group B) corticosteroids (group C)(N = 181) (N = 168) (N = 168)
Mean (± SD) baseline GFR based on MDRD-4 (mL/min)1 93.46 (39.63) 95.89 (36.81) 86.71 (29.20)Mean (± SD) change from baseline in GFR −24.89 (36.45) −22.60 (35.5) −14.62 (29.17)
based on MDRD-4 at week 52 (mL/min)1Mean (± SD) baseline GFR based on the 101.83 (44.16) 104.31(± 37.15) 96.51 (± 34.94)
Cockcroft–Gault formula at (mL/min)Mean (95%CI) change from baseline in GFR based −23.61 −21.22 −13.63∗
on the Cockcroft–Gault formula at week 52 (mL/min)(−28.60, −18.62) (−26.12, −16.32) (−17.96, −9.30)
Mean (± SD) baseline serum creatinine levels (ng/mL) 0.97 (0.35) 0.92 (0.27) 1.00 (0.36)Mean (95%CI) change from baseline in
serum creatinine levels (ng/mL)Week 13 0.22 0.16 0.11
(0.16, 0.29) (0.10, 0.21)∗ (0.04, 0.18)∗∗
Week 26 0.23 0.19 0.11(0.16, 0.31) (0.12, 0.25) (0.01, 0.21)∗
Week 52 0.23 0.17 0.12(0.17, 0.29) (0.12, 0.22)∗∗ (0.06, 0.19)∗
Number of episodes of BPAR or presumedacute rejection during 52 weeks, N (%)
0 episodes 119 (65.7) 106 (63.1) 124 (73.8)1 episode 51 (28.2) 52 (31.0) 39 (23.2)2 episodes 10 (5.5) 8 (4.8) 5 (3.0)3 episodes 1 (0.6) 1 (0.6) 0>3 episodes 0 1 (0.6) 0
BPAR requiring treatment, N (%)Up to week 26 42 (23.2) 42 (25.0) 25 (14.9)∗
Up to week 52 44 (24.3) 45 (26.8) 28 (16.7)BPAR or presumed acute rejection requiring treatment, N (%)
Up to week 26 48 (26.5) 45 (26.8) 29 (17.3)∗
Up to week 52 50 (27.6) 49 (29.2) 32 (19.0)Patient survival up to week 52, N (%) 164 (90.6) 149 (88.7) 157 (93.5)Graft survival up to week 52 (n, %) 170 (93.9) 158 (94.0) 156 (92.9)Recurrence of liver disease at week 52, N (%) 7 (9.7) 10 (14.9) 15 (22.1)∗
Composite endpoint of renal function and 167 (92.3) 151 (89.9) 130 (77.4)∗∗∗
graft-related outcomes2 (n, %)
BPAR = biopsy-proven acute rejection; GFR = glomerular filtration rate; MDRD = modification of diet in renal disease.1 Post hoc analysis.2 The composite secondary efficacy parameter was a 20% or greater decrease from baseline in calculated creatinine clearance, or acuterejection, or graft loss or death.∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001 versus group A.
dose used in our study was agreed based on experiencefrom renal allograft recipients (28). Although the combina-tion of tacrolimus and MMF is not currently licensed foruse in liver transplant recipients, they are commonly co-prescribed (2) and are an effective combination (29–33). Inaddition, there was a relatively high rate of withdrawal, es-pecially in group A where many patients were withdrawnso mycophenolate could be given. To address these con-cerns, we defined, post hoc, a ‘per protocol’ set of patientswhere levels of tacrolimus achieved were within 10% oftarget; in this smaller group of patients, similar conclusionswere reached.
There was no significant adverse impact from the tworeduced-dose tacrolimus treatment regimes (B and C), aspatient and graft loss were similar and there was no in-creased risk of infection, or biopsy-proven or treated rejec-tion. Our study was not designed to evaluate the effect ofinduction therapy, so it is not possible to exclude an effectof IL2-receptor on the overall rate of rejection in group C.Moreover, the mechanism underlying the benefits in renalfunction conferred by delayed introduction of tacrolimusremains to be fully elucidated. It is possible that the kid-ney, put at risk by reperfusion and/or in combination withother transplant-related events, is more susceptible to the
American Journal of Transplantation 2009; 9: 327–336 333
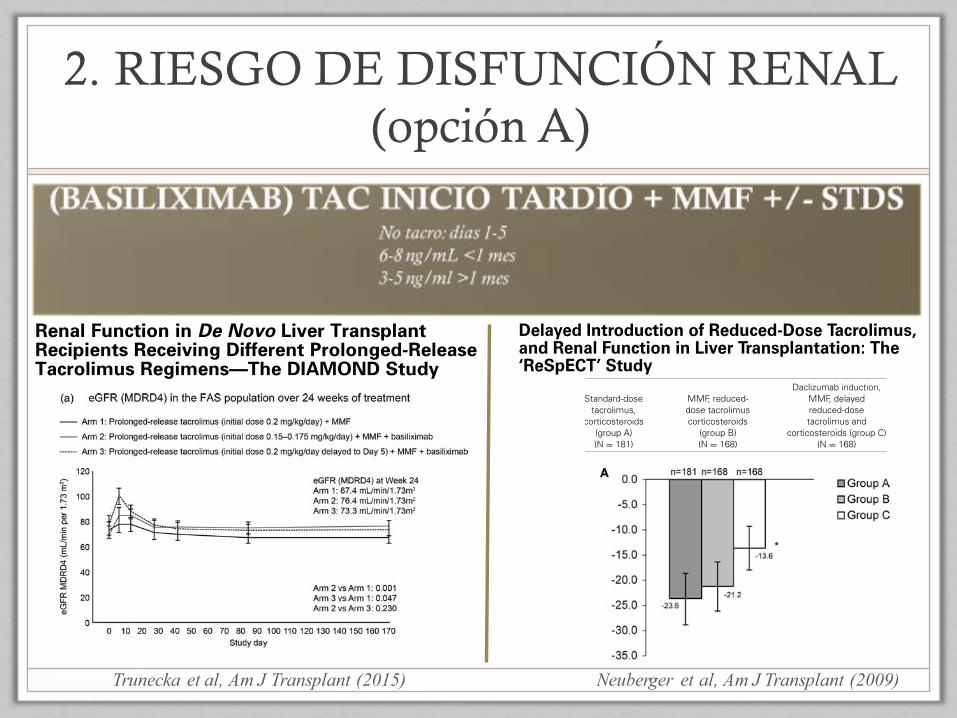
2. RIESGO DE DISFUNCIÓN RENAL (opción A)
Neuberger et al, Am J Transplant (2009)
Figure 4: (a) eGFR (MDRD4) in the FAS population, and (b) Kaplan–Meier analysis of composite efficacy failure-free survival in the mITTpopulation, over 24 weeks of treatment. Data in Figure 4a are represented as least-square means and error bars represent standard error of
the mean. eGFR, estimated glomerular filtration rate; FAS, full-analysis set; MDRD4, Modification of Diet in Renal Disease-4; mITT, modifiedintent to treat; MMF, mycophenolate mofetil.
Trunecka et al
8 American Journal of Transplantation 2015; XX: 1–12
Trunecka et al, Am J Transplant (2015)
Renal Function in De Novo Liver TransplantRecipients Receiving Different Prolonged-ReleaseTacrolimus Regimens—The DIAMOND Study
P. Trunecka1,*, J. Klempnauer2,W. O. Bechstein3, J. Pirenne4, S. Friman5,A. Zhao6, H. Isoniemi7, L. Rostaing8,U. Settmacher9, C. Monch3,10, M. Brown11,N. Undre12, G. Tisone13 and on behalf of theDIAMONDy study group
1Transplantcentre, Institute for Clinical and ExperimentalMedicine, Prague, Czech Republic2Department of General, Visceral and TransplantationSurgery, Hannover Medical School, Hannover, Germany3Department of Surgery, Goethe University Hospital andClinics, Frankfurt, Germany4Abdominal Transplant Surgery, University HospitalsLeuven, Leuven, Belgium5The Transplant Institute, Sahlgrenska UniversityHospital, Gothenburg, Sweden6Department of Abdominal Surgery, A.V. VishnevskyInstitute of Surgery, Moscow, Russian Federation7Department of Transplantation and Liver Surgery Clinic,Helsinki University Hospital, Helsinki, Finland8Department of Nephrology and Organ Transplantation,Toulouse University Hospital, Toulouse, France9Department of General, Visceral and Vascular Surgery,Jena University Hospital, Thuringia, Germany10Department of General, Visceral and TransplantationSurgery, Westpfalz-Klinikum Hospital, Kaiserslautern,Germany11Astellas Pharma Inc., Northbrook, IL12Astellas Pharma Europe Ltd, London, United Kingdom13Liver Transplant Unit, Policlinico di Tor Vergata, Rome,Italy⇤Corresponding author: Pavel Trunecka, [email protected]: ADVAGRAF
TM
studIed in combinAtion withMycOphenolate mofetil aND basiliximab in livertransplantation
This is an open access article under the terms of theCreative Commons Attribution-NonCommercial-NoDerivsLicense, which permits use and distribution in anymedium, provided the original work is properly cited, theuse is non-commercial and no modifications oradaptations are made.
DIAMOND: multicenter, 24-week, randomized trialinvestigating the effect of different once-daily, pro-longed-release tacrolimus dosing regimens on renalfunction after de novo liver transplantation. Arm 1:prolonged-release tacrolimus (initial dose 0.2mg/kg/day); Arm 2: prolonged-release tacrolimus (0.15–
0.175mg/kg/day) plus basiliximab; Arm 3: prolonged-release tacrolimus (0.2mg/kg/day delayed until Day 5)plus basiliximab. All patients received MMF plus abolus of corticosteroid (no maintenance steroids).Primary endpoint: eGFR (MDRD4) at Week 24. Second-ary endpoints: composite efficacy failure, BCAR andAEs. Baseline characteristics were comparable. Tacro-limus trough levels were readily achieved posttrans-plant; initially lower in Arm 2 versus 1 with delayedinitiation in Arm 3. eGFR (MDRD4) was higher in Arms 2and 3 versus 1 (pà0.001, pà0.047). Kaplan–Meierestimates of composite efficacy failure-free survivalwere 72.0%, 77.6%, 73.9% in Arms 1–3. BCAR incidencewas significantly lower in Arm 2 versus 1 and 3(pà 0.016, pà0.039). AEs were comparable. Pro-longed-release tacrolimus (0.15–0.175mg/kg/day) im-mediately posttransplant plus basiliximab and MMF(without maintenance corticosteroids) was associatedwith lower tacrolimus exposure, and significantlyreduced renal function impairment and BCAR inci-dence versus prolonged-release tacrolimus (0.2mg/kg/day) administered immediately posttransplant. De-layed higher-dose prolonged-release tacrolimus initia-tion significantly reduced renal function impairmentcompared with immediate posttransplant administra-tion, but BCAR incidence was comparable.
Abbreviations: AE, adverse event; ANCOVA, analysis ofcovariance; AR, acute rejection; BCAR, biopsy-con-firmed acute rejection; BD, twice daily; CI, confidenceinterval; CKD-EPI, Chronic Kidney Disease Epidemiolo-gy Collaboration; DIAMOND, ADVAGRAFTM studIed incombinAtion with MycOphenolate mofetil aND basi-liximab in liver transplantation; EQ5D, EuroQoL 5-dimensions questionnaire; FAS, full-analysis set; HIV,human immunodeficiency virus; HR-QoL, health-relat-ed quality of life; IV, intravenous; MELD, Model for End-stage Liver Disease; mITT, modified intent-to-treatpopulation; MMF, mycophenolate mofetil; NODM,new-onset diabetes mellitus; PPS, per-protocol set;SAF, safety-analysis set; SD, standard deviation; TEAE,treatment-emergent adverse event
Received 02 September 2014, accepted for publication21 December 2014
Introduction
Tacrolimus is accepted as the mainstay of immunosup-pression in liver transplantation. Results from a previous
American Journal of Transplantation 2015; XX: 1–12Wiley Periodicals Inc.
�C 2015 The Authors. American Journal of Transplantationpublished by Wiley Periodicals Inc.
doi: 10.1111/ajt.13182
1
American Journal of Transplantation 2009; 9: 327–336Wiley Periodicals Inc.
C⃝ 2009 The AuthorsJournal compilation C⃝ 2009 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2008.02493.x
Delayed Introduction of Reduced-Dose Tacrolimus,and Renal Function in Liver Transplantation: The‘ReSpECT’ Study
J. M. Neubergera,∗, R. D. Mamelokb,P. Neuhausc, J. Pirenned, D. Samuele,H. Isoniemif, L. Rostaingg, A. Rimolah,S. Marshalli and A. D. Mayera for The ReSpECTStudy Group
aLiver Unit, Queen Elizabeth Hospital, Birmingham, UKbMamelok Consulting, Palo Alto, CAcDepartment of General, Visceral and TransplantationSurgery, Virchow Clinic, Charite-University MedicineBerlin, Berlin, GermanydAbdominal Transplant Surgery Department, UniversityHospital Leuven, Leuven, BelgiumeCentre Hepatobiliaire, Hopital Paul Brousse, UniversityParis XI, Villejuif, FrancefTransplantation and Liver Surgery Clinic, HelsinkiUniversity Hospital, Helsinki, FinlandgMultiorgan Transplant Unit, CHU Rangueil, UniversityHospital, Toulouse, FrancehLiver Unit, Hospital Clınic, IDIBAPS, CIBEREHD,Barcelona, SpainiF. Hoffmann-La Roche Ltd, Basel, Switzerland∗Corresponding author: James M. Neuberger,[email protected]
We report a multicenter, prospective, randomized,open-label trial investigating the effect of lower levelsand delayed introduction of tacrolimus on renal func-tion in liver transplant recipients. Adult patients withgood renal function undergoing primary liver trans-plant were randomized to either: group A (standard-dose tacrolimus [target trough levels >10 ng/mL] andcorticosteroids; n = 183); group B (mycophenolatemofetil [MMF] 2g/day, reduced-dose tacrolimus [targettrough levels ≤8 ng/mL], and corticosteroids; n = 170);group C (daclizumab induction, MMF, reduced-dosetacrolimus delayed until the fifth day posttransplantand corticosteroids, n = 172). The primary endpointwas change from baseline in estimated glomerular fil-tration rate (eGFR) at 52 weeks. The eGFR decreasedby 23.61, 21.22 and 13.63 mL/min in groups A, B and C,respectively (A vs C, p = 0.012; A vs B, p = 0.199). Renaldialysis was required less frequently in group C versusgroup A (4.2% vs. 9.9%; p = 0.037). Biopsy-proven acuterejection rates were 27.6%, 29.2% and 19.0%, respec-tively. Patient and graft survival was similar. In conclu-sion, daclizumab induction, MMF, corticosteroids anddelayed reduced-dose tacrolimus was associated withless nephrotoxicity than therapy with standard-dose
tacrolimus and corticosteroids without compromisingefficacy or tolerability.
Key words: Delayed tacrolimus, immunosuppression,liver transplantation, renal failure
Recieved 04 July 2008, revised 17 September 2008 andaccepted for publication 28 September 2008
Introduction
Although outcomes after liver transplantation are usuallyexcellent, with current 5- and 10-year patient survival ratesexceeding 70% and 60% (1,2), late complications remainof concern. Renal dysfunction remains a major cause ofboth morbidity and mortality (3). Significant renal impair-ment, occurring in up to 27% of liver allograft recipients at5 years (4,5), results in end-stage renal disease in as manyas 10% of patients at 10 years posttransplant (4) and latechronic renal dysfunction or renal failure is associated withthe risk of premature death (3–6).
Late renal failure is associated with both pre- and postlivertransplant factors, including higher concentrations of CNIsboth early and late posttransplant (7,8) and can be pre-dicted by creatinine levels in the first posttransplant year(9,10). Strategies to minimize the adverse renal effects ofCNIs in patients include reducing the CNI dose (11–14)or complete withdrawal of the CNI (14,15), while addingother immunosuppressive agents such as mycophenolatemofetil (MMF) (12–14,16) or sirolimus (11,15). Alterna-tively, a preemptive strategy may be adopted by attemptingto avoid CNI-induced renal impairment. Antibody inductiontherapy (such as interleukin-2 [IL2] receptor antagonists)may allow reduction in dose or delayed introduction of CNIs(17–19).
We conducted the ReSpECT study, a prospective, ran-domized trial in de novo adult liver transplant patientswith good renal function pretransplant, to assess theeffect on renal function, acute rejection, and graft andpatient survival of three regimens: standard-dosetacrolimus and corticosteroids; MMF with reduced-dosetacrolimus and corticosteroids; and induction with da-clizumab, MMF and delayed introduction of reduced-dosetacrolimus and corticosteroids.
327
Neuberger et al.
Figure 3: The mean change from baseline in calculated cre-atinine clearance based on the Cockcroft–Gault formula at52 weeks in liver allograft recipients from the (A) FAS popu-lation and (B) PP population. Bars represent 95% confidenceintervals for each mean. ∗p < 0.05 versus group A. FAS = fullanalysis set; PP = per protocol.
for the occurrence of biopsy-proven or presumed acute re-jection, first biopsy-proven acute rejection requiring treat-ment and graft loss or death during the 52-week treat-ment period. A similar percentage of patients across allthree groups experienced graft loss (6–7%). The compos-ite endpoint of renal function and graft-related outcomeswas lower for group C compared with group A (p ≤ 0.001).Outcomes related to rejection requiring treatment at week26 were also significantly lower in group C versus group A(p < 0.05; Table 2).
Adverse eventsA summary of the overall adverse event profile is pre-sented in Table 3. Most treatment-emergent adverseevents were of mild or moderate severity as defined bythe investigator. Adverse events leading to withdrawal ordeath: there were more withdrawals because of adverseevents in group A than in the other two groups (Table 3).With the exception of renal insufficiency, there were no no-
table differences between the three groups with respectto the nature of adverse event that led to study withdrawal.Infections were the most frequent adverse events leadingto death (Table 3).
Adverse events of special interest: Treatment-emergentdiarrhea was not more common in the groups receivingMMF (groups B and C) than in group A (Table 4). Indeed,most treatment-emergent adverse events occurred with abroadly similar frequency between treatment groups, withsome notable exceptions. Hypertension occurred less fre-quently in groups B and C versus group A, and leukopeniaoccurred more often in group C than group A (p = 0.0062)(Table 4).
The overall incidence of opportunistic infections was simi-lar in all groups (Table 3). Serious adverse events occurredin about two-thirds of patients in each group (Table 3), themost common being graft dysfunction (4.4%, 4.7% and3.6% in groups A, B and C) and CMV syndrome (3.3%,3.0%, 5.3%, respectively). Malignancies were not com-mon (Table 3) and specific malignancies did not occur inmore than one patient in any treatment group.
There were no notable differences in mean blood chem-istry or hematology values or body mass index betweenthe three treatment groups at day 0, week 26 or 52.
Discussion
This study demonstrated that delayed introduction ofreduced-dose tacrolimus, under the protection of MMFand daclizumab (group C), is associated with less impair-ment of renal function compared with standard therapywith tacrolimus and corticosteroid (group A) without anincreased frequency of rejection, graft loss or death. How-ever, there was no such benefit with a triple therapy regi-men of MMF, reduced-dose tacrolimus and corticosteroids(group B) initiated immediately after transplant relative tothe standard therapy.
We recognize that there are limitations in this study:with increasing experience, regimes of immunosuppres-sion have been modified and, as this was an open-labelstudy conducted in experienced high-volume centers, clin-icians had a low threshold to modify treatment regimes. Inthe registration studies, and according to the license for itsuse, initial tacrolimus target trough levels are 5–20 ng/mL(24), which are then typically tapered to maintenance tar-get trough levels of 5–10 ng/mL (4,25). Target tacrolimustrough levels and the use of daclizumab were determinedby the Steering Group: levels in Group A were in line withrecommended levels. However, we recognize that bothtarget and achieved levels were greater than those usedin most centers currently. Daclizumab is not currently in-dicated for use in liver transplant patients, although it iseffective and safe in this patient population (26,27); the
332 American Journal of Transplantation 2009; 9: 327–336
Neuberger et al.
Table 1: Baseline recipient and donor characteristics of the FAS population
Daclizumab induction,Standard-dose MMF, reduced- MMF, delayed
tacrolimus, dose tacrolimus reduced-dosecorticosteroids corticosteroids tacrolimus and
(group A) (group B) corticosteroids (group C)(N = 181) (N = 168) (N = 168)
Recipient age, median years (min, max) 53.0 (19, 69) 54.0 (18, 73) 55.0 (26, 70)Male, N (%) 127 (70.2) 109 (64.9) 116 (69.0)Caucasian, N (%) 173 (95.6) 163 (97.0) 164 (97.6)Mean (± SD) calculated creatinine clearance based 101.83 (44.15) 104.31 (37.15) 96.51 (34.94)
on Cockcroft–Gault (mL/min) 101.83 (44.15) 104.31 (37.15) 96.51 (34.94)Mean (± SD) MELD score1 15.4 (6.57) 15.2 (5.59) 15.6 (6.26)Median (range) MELD score (unadjusted for HCC) 14 (6 − 49) 15 (5 − 33) 15 (5 − 41)Cause of liver disease, N (%)2
Alcoholic liver disease 79 (43.6) 72 (42.9) 76 (45.2)Primary biliary cirrhosis 18 (9.9) 14 (8.3) 12 (7.1)Primary sclerosing cholangitis 13 (7.2) 18 (10.7) 13 (7.7)Hepatitis B 17 (9.4) 13 (7.7) 10 (6.0)Hepatitis C 36 (19.9) 34 (20.2) 39 (23.2)Hepatitis of unknown etiology 2 (1.1) 0 4 (2.4)Fulminant hepatic failure/toxic hepatitis 0 0 4 (2.4)Hepatocellular carcinoma 37 (20.4) 38 (22.6) 38 (22.6)Autoimmune hepatitis 7 (3.9) 5 (3.0) 6 (3.6)Other 30 (16.6) 28 (16.7) 28 (16.7)
Donor age, mean (± SD) years 48.4 (15.58) 48.3 (16.86) 48.0 (17.61)Type of donor, N (%)
Deceased, heart beating 146 (80.7) 131 (78.0) 146 (86.9)Deceased, nonheart beating 26 (14.4) 28 (16.7) 19 (11.3)Living, related 4 (2.2) 3 (1.8) 1 (0.6)Living, unrelated 5 (2.8) 6 (3.6) 2 (1.2)
Donor/recipient CMV serological status, N (%)+/+ 77 (42.5) 60 (35.7) 63 (37.5)+/− 36 (19.9) 38 (22.5) 38 (22.5)−/+ 37 (20.4) 29 (17.3) 31 (18.5)−/− 21 (11.6) 26 (15.5) 25 (14.9)
1No. of evaluable pts: 170 in standard therapy group, 158 in reduced tacrolimus + MMF group and 159 in reduced, delayed tacrolimus+ MMF group.2Patients may have had more than one cause of liver disease. Some patients with liver disease designated ‘other’ initially were reassignedto more specific categories following medical review.CMV = cytomegalovirus; GFR = glomerular filtration rate; MELD = model for end-stage liver disease; MMF = mycophenolate mofetil;SD = standard deviation.
Baseline patient demographics and disease/transplantcharacteristics for the FAS population were broadly similarbetween groups, including the mean model for end-stageliver disease (MELD) scores (Table 1). Pretransplant renalfunction was lowest in group C, both for the FAS (Table 1)and PP populations.
Exposure to study medicationMost patients (89–95%) initially received oral tacrolimus.Mean tacrolimus trough levels throughout the study inall three treatment groups are shown in Figure 2. Frommonth 4, mean tacrolimus trough levels between treat-ment groups tended to converge (Figure 2). The mean(± SD) tacrolimus concentrations for patients in the threegroups (A, B and C) were 10.7 ± 3.7, 8.6 ± 3.2, 8.4 ±
2.8 ng/mL (at 2 weeks); 11.1 ± 3.2, 8.8 ± 2.8 and 7.7 ±2.3 ng/mL (at 1 month); 10.4 ± 3.9, 9.1 ± 3.5 and 8.9 ±3.1 ng/mL (at 3 months); 9.7 ± 3.1, 8.4 ± 2.8 and8.4 ± 2.7 ng/mL (4–6 months) and 8.5 ± 3.7, 7.8 ± 2.7 and7.4 ± 2.8 ng/mL (10–12 months).
Mean daily doses of MMF from week 1 to month 12 rangedfrom 1562 ± 587 to 1959 ± 382 mg/day in group B, andfrom 1555 ± 531 to 1886 ± 357 mg/day in group C. In groupC, the median and mean first daclizumab doses were both2.0 mg/kg.
Corticosteroid doses were similar for all three groups forall time points. During week 4, mean (± SD) daily main-tenance doses of corticosteroids (dose calculated based
330 American Journal of Transplantation 2009; 9: 327–336
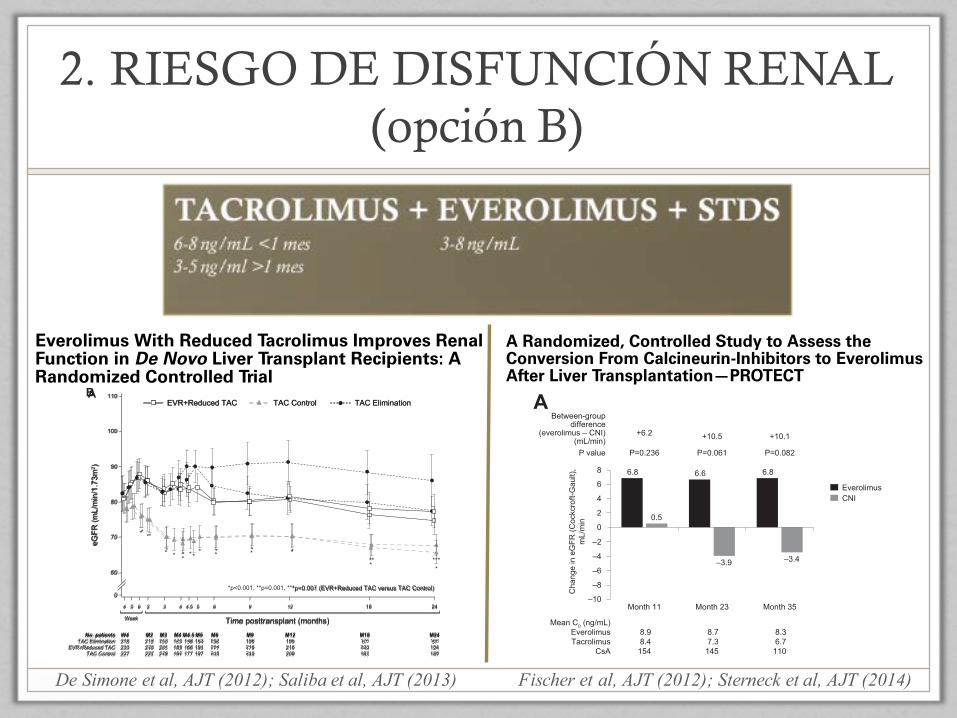
2. RIESGO DE DISFUNCIÓN RENAL (opción B)
De Simone et al, AJT (2012); Saliba et al, AJT (2013) Fischer et al, AJT (2012); Sterneck et al, AJT (2014)
American Journal of Transplantation 2012; 12: 3008–3020Wiley Periodicals Inc.
C⃝ Copyright 2012 The American Society of Transplantationand the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2012.04212.x
Everolimus With Reduced Tacrolimus Improves RenalFunction in De Novo Liver Transplant Recipients: ARandomized Controlled Trial
P. De Simonea,†, F. Nevensb, L. De Carlisc,H. J. Metselaard, S. Beckebaume, F. Salibaf,S. Jonasg, D. Sudanh, J. Fungi, L. Fischerj,C. Duvouxk, K. D. Chavinl, B. Konerum,M. A. Huangn, W. C. Chapmano, D. Foltysp,S. Witteq, H. Jiangr, J. M. Hexhamr
and G. Jungeq for the H2304 Study Group*
aGeneral Surgery and Liver Transplantation, AziendaOspedaliero-Universitaria Pisana, Pisa, ItalybDepartment of Hepatology, University Hospital KULeuven, Leuven, BelgiumcHepato-biliary Surgery and Liver Transplantation Unit,Azienda Ospedaliera Niguarda Ca Granda, Milan, ItalydDepartment of Gastroenterology & Hepatology, ErasmusMC, University Hospital Rotterdam, the NetherlandseDepartment of General, Visceral and TransplantationSurgery, University Hospital Essen, Essen, Germany andDepartment of Transplant Medicine, University HospitalMunster, Munster, GermanyfHepato-Biliary Center, AP-HP Hopital Paul Brousse,Universite Paris-Sud, 94804 Villejuif, FrancegDepartment of Visceral, Transplantation, Thoracic andVascular Surgery, University Medical Center Leipzig,Leipzig, GermanyhDepartment of General Surgery, Division of TransplantSurgery, Duke University Medical Center, Durham, NCiTransplantation Center, Cleveland Clinic, Cleveland, OHjDepartment of Hepatobiliary Surgery and Transplantation,University Medical Center Eppendorf, Hamburg, GermanykLiver Transplant Unit, AP-HP Hopital Henri Mondor,Creteil, FrancelDivision of Transplant Surgery, Medical University ofSouth Carolina, Charleston, SCmDepartment of Surgery, University of Medicine andDentistry—New Jersey Medical School, Newark, NJnDivision of Gastroenterology, Department of InternalMedicine, Henry Ford Hospital, Detroit, MIoDepartment of Surgery, Washington University School ofMedicine, St. Louis, MOpDepartment of Transplant Surgery, University MedicalCenter, Johannes Gutenberg University, Mainz, GermanyqNovartis Pharma AG, Basel, SwitzerlandrNovartis Pharmaceuticals, East Hanover, NJ∗H2304 study investigators are listed in the Appendix.†Corresponding author: Paolo De Simone,[email protected]
Re-use of this article is permitted in accordance with theTerms and Conditions set out at http://wileyonlinelibrary.com/onlineopen#OnlineOpen_Terms
In a prospective, multicenter, open-label study, de novoliver transplant patients were randomized at day 30±5to (i) everolimus initiation with tacrolimus elimina-tion (TAC Elimination) (ii) everolimus initiation withreduced-exposure tacrolimus (EVR+Reduced TAC) or(iii) standard-exposure tacrolimus (TAC Control). Ran-domization to TAC Elimination was terminated prema-turely due to a higher rate of treated biopsy-provenacute rejection (tBPAR). EVR+Reduced TAC was non-inferior to TAC Control for the primary efficacy endpoint(tBPAR, graft loss or death at 12 months posttransplan-tation): 6.7% versus 9.7% (−3.0%; 95% CI −8.7, 2.6%;p<0.001 for noninferiority [12% margin]). tBPAR oc-curred in 2.9% of EVR+Reduced TAC patients versus7.0% of TAC Controls (p = 0.035). The change in ad-justed estimated GFR from randomization to month12 was superior with EVR+Reduced TAC versus TACControl (difference 8.50 mL/min/1.73 m2, 97.5% CI 3.74,13.27 mL/min/1.73 m2, p<0.001 for superiority). Drugdiscontinuation for adverse events occurred in 25.7%of EVR+Reduced TAC and 14.1% of TAC Controls (rel-ative risk 1.82, 95% CI 1.25, 2.66). Relative risk of seri-ous infections between the EVR+Reduced TAC groupversus TAC Controls was 1.76 (95% CI 1.03, 3.00).Everolimus facilitates early tacrolimus minimizationwith comparable efficacy and superior renal function,compared to a standard tacrolimus exposure regimen12 months after liver transplantation.
Key words: Efficacy, everolimus, liver transplantation,reduced, tacrolimus, withdrawal
Abbreviations: ALT, alanine aminotransferase; AN-COVA, analysis of covariance; AST, aspartate amino-transferase; BPAR, biopsy-proven acute rejection; CKDEPI, Chronic Kidney Disease Epidemiology Collabora-tion; CMV, cytomegalovirus; CNI, calcineurin inhibitor;DMC, Data Monitoring Committee; EGFR, estimatedglomerular filtration rate; HAT, hepatic artery throm-bosis; HCC, hepatocellular carcinoma; HCV, hepatitisC virus; ITT, intent-to-treat; MDRD, modification ofdiet in renal disease; MELD, model for end-stage liverdisease; MPA, mycophenolic acid; MTOR, mammaliantarget of rapamycin; RAI, rejection activity index; RR,relative risk; SD, standard deviation; SE, standard er-ror; TBPAR, treated biopsy-proven acute rejection.
3008
Time posttransplant (months)
TAC EliminationEVR+Reduced TAC TAC Control
4
*p<0.001, **p=0.001, ***p=0.007 (EVR+Reduced TAC versus TAC Control)
5
Week
6 654.5432
******** *
***
**
9 12 18 24
No. patientsTAC Elimination
EVR+Reduced TACTAC Control
W4218233227
M3213221229
M4170189192
M2218223227
M4.5148168177
M5163191197
M9196216215
M6202204218
M12195216209
M18175203197
M24163184186
100
90
80
0
70
60
110
eGFR
(mL/
min
/1.7
3m2 )
*p<0.001 (EVR+Reduced TAC versus TAC Control)
Time posttransplant (months)
4 5
Week
6 654.5432 9 12 18 24
No. patientsTAC Elimination
EVR+Reduced TACTAC Control
W4218233227
M3190205218
M4163183191
M2212216225
M4.5138166177
M5154188197
M9106179188
M6136177193
M12195216209
M1867
149163
M2457
124147
100
90
80
0
70
60
110
eGFR
(mL/
min
/1.7
3m2 )
TAC EliminationEVR+Reduced TAC TAC Control
*****
**
* *
* *
A
B
Figure 3: eGFR (MDRD4) according to treatment group (A) ITT population (B) on-treatment patients. Values are shown as meanand 95% CI.
Saliba et al.
1740 American Journal of Transplantation 2013; 13: 1734–1745
Time posttransplant (months)
TAC EliminationEVR+Reduced TAC TAC Control
4
*p<0.001, **p=0.001, ***p=0.007 (EVR+Reduced TAC versus TAC Control)
5
Week
6 654.5432
******** *
***
**
9 12 18 24
No. patientsTAC Elimination
EVR+Reduced TACTAC Control
W4218233227
M3213221229
M4170189192
M2218223227
M4.5148168177
M5163191197
M9196216215
M6202204218
M12195216209
M18175203197
M24163184186
100
90
80
0
70
60
110
eGFR
(mL/
min
/1.7
3m2 )
*p<0.001 (EVR+Reduced TAC versus TAC Control)
Time posttransplant (months)
4 5
Week
6 654.5432 9 12 18 24
No. patientsTAC Elimination
EVR+Reduced TACTAC Control
W4218233227
M3190205218
M4163183191
M2212216225
M4.5138166177
M5154188197
M9106179188
M6136177193
M12195216209
M1867
149163
M2457
124147
100
90
80
0
70
60
110
eGFR
(mL/
min
/1.7
3m2 )
TAC EliminationEVR+Reduced TAC TAC Control
*****
**
* *
* *
A
B
Figure 3: eGFR (MDRD4) according to treatment group (A) ITT population (B) on-treatment patients. Values are shown as meanand 95% CI.
Saliba et al.
1740 American Journal of Transplantation 2013; 13: 1734–1745
American Journal of Transplantation 2012; 12: 1855–1865Wiley Periodicals Inc.
C⃝ Copyright 2012 The American Society of Transplantationand the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2012.04049.x
A Randomized, Controlled Study to Assess theConversion From Calcineurin-Inhibitors to EverolimusAfter Liver Transplantation—PROTECT
L. Fischera, J. Klempnauerb, S. Beckebaumc,H. J. Metselaard, P. Neuhause, P. Schemmerf,U. Settmacherg, N. Heyneh, P-A. Clavieni,F. Muehlbacherj, I. Morardk, H. Woltersl,W. Vogelm, T. Beckern, M. Sternecka, F. Lehnerb,C. Kleinc, G. Kazemierd, A. Paschere, J. Schmidtf,F. Rauchfussg, A. Schnitzbauero, S. Nadalinh,M. Hackp, S. Ladenburgerp and H. J. Schlitto,*
aUniversity Medical Center Hamburg-Eppendorf,Department of Hepatobiliary and Transplant Surgery,Hamburg, GermanybHannover Medical School (MHH), Clinic for General,Abdominal and Transplant Surgery, Hannover, GermanycEssen University Hospital, Department of General,Visceral and Transplantation Surgery, Essen, GermanydErasmus MC, University Hospital Rotterdam,Department of Gastroenterology and Hepatology,Rotterdam, the NetherlandseCharite University Medical Center Berlin, Clinic forGeneral, Abdominal and Transplant Surgery, Berlin,GermanyfUniversity Hospital Heidelberg, Department of General,Visceral and Transplant Surgery, Heidelberg, GermanygJena University Hospital, Department of General,Abdominal and Vascular Surgery, Jena, GermanyhUniversity Hospital Tuebingen, Department of General,Visceral and Transplant Surgery, Tuebingen, GermanyiUniversity of Zurich, Swiss HPB and TransplantationCenter, Department of Surgery, Zurich, SwitzerlandjMedical University of Vienna, Surgical Clinic, Division ofTransplant Surgery, Vienna, AustriakHopitaux Universitaires de Geneve (HUG),Gastroenterologie et Hepatologie, Geneve, SwitzerlandlMuenster University Hospital, Clinic and Policlinic forGeneral Surgery, Muenster, GermanymInnsbruck Medical University, Department of InternalMedicine II (Gastroenterology and Hepatology),Innsbruck, AustrianUniversity Medical Center Schleswig-Holstein,Department of General and Thoracic Surgery, Kiel,GermanyoUniversity Hospital Regensburg, Department of Surgery,Regensburg, GermanypNovartis Pharma GmbH, Nuremberg, Germany
*Corresponding author: Prof Dr. med. Hans. Schlitt,[email protected]
Posttransplant immunosuppression with calcineurininhibitors (CNIs) is associated with impaired renal func-tion, while mTor inhibitors such as everolimus mayprovide a renal-sparing alternative. In this random-ized 1-year study in patients with liver transplantation(LTx), we sought to assess the effects of everolimuson glomerular filtration rate (GFR) after conversionfrom CNIs compared to continued CNI treatment. Eligi-ble study patients received basiliximab induction, CNIwith/without corticosteroids for 4 weeks post-LTx, andwere then randomized (if GFR > 50 mL/min) to contin-ued CNIs (N = 102) or subsequent conversion to EVR(N = 101). Mean calculated GFR 11 months postran-domization (ITT population) revealed no significantdifference between treatments using the Cockcroft-Gault formula (−2.9 mL/min in favor of EVR, 95%-CI:[−10.659; 4.814], p = 0.46), whereas use of the MDRDformula showed superiority for EVR (−7.8 mL/min,95%-CI: [−14.366; −1.191], p = 0.021). Rates of mor-tality (EVR: 4.2% vs. CNI: 4.1%), biopsy-proven acuterejection (17.7% vs. 15.3%), and efficacy failure (20.8%vs. 20.4%) were similar. Infections, leukocytopenia, hy-perlipidemia and treatment discontinuations occurredmore frequently in the EVR group. No hepatic arterythrombosis and no excess of wound healing impair-ment were noted. Conversion from CNI-based to EVR-based immunosuppression proved to be a safe alter-native post-LTx that deserves further investigation interms of nephroprotection.
Key words: Calcineurin inhibitor agents, conversion,everolimus, Liver transplantation, mTor inhibitor, renalfunction
Abbreviations: AE, adverse event; ANCOVA, analy-sis of covariance; BPAR, biopsy-proven acute rejec-tion; CG-GFR, GFR calculated with the Cockcroft-Gaultformula; CI, confidence interval; CS, corticosteroids;CsA, cyclosporine A; CNI, calcineurin inhibitor(s); g,gram; G/L, giga per liter; HAT, hepatic artery throm-bosis; HCV, hepatitis C virus; ILD, interstitial lungdisease; ITT, intent-to-treat (population); LOCF, lastobservation carried forward; LS, least square; LTx,liver transplantation; MDRD-GFR, GFR calculated us-ing the MDRD formula; MedDRA, Medical Dictionaryfor Regulatory Activities; MELD, Model of End-StageLiver Disease; mg, milligram; MMF, mycophenolatemofetil; mTOR, mammalian target of rapamycin; PP,per protocol (population); RCT, randomized controlled
1855
The safety profile of everolimus was acceptable.Peripheral edema was more frequent in the CNI-freearm, a recognized side effect of mTOR inhibitors that isdose dependent (23). In our population, there was noapparent association between peripheral edema and
proteinuria. Incisional hernias were numerically morefrequent in the CNI-free group during the study.Last, no patient had anemia at month 35 and thehematological profile was similar between treatmentgroups.
2
4
6
8
–8
–6
–4
–2
–10
0
Cha
nge
in e
GFR
(Coc
kcro
ft-G
ault)
,m
L/m
in
EverolimusCNI
Month 11
P=0.236
6.8
0.5
Between-groupdifference
(everolimus – CNI)(mL/min)
P value
Mean C0 (ng/mL)EverolimusTacrolimus
CsA
Month 23
P=0.061
Month 35
P=0.082
+6.2 +10.5 +10.1
8.98.4
154
6.6
–3.9 –3.4
8.77.3145
6.8
8.36.7
110
2
4
6
8
–8
–6
–4
–2
–10
0
Cha
nge
in e
GFR
(Nan
kive
ll),
mL/
min
/1.7
3m2
EverolimusCNI
Month 11
P=0.189
2.0
–2.8
Between-groupdifference
(everolimus – CNI)(mL/min)
P value
Mean C0 (ng/mL)EverolimusTacrolimus
CsA
Month 23
P=0.044
Month 35
P=0.028
+4.8 +8.6 +9.5
8.98.4154
2.0
–6.6 –6.5
8.77.3145
3.0
8.36.7110
2
4
6
8
–8
–6
–4
–2
–10
0
Cha
nge
in e
GFR
(MD
RD
4),
mL/
min
/1.7
3m2
EverolimusCNI
Month 11
P=0.164
0.3
–5.7
Between-groupdifference
(everolimus – CNI)(mL/min)
P value
Mean C0 (ng/mL)EverolimusTacrolimus
CsA
Month 23
P=0.071
Month 35
P=0.053
+6.0 +8.9 +9.4
8.98.4154
–0.9
–9.8 –9.6
8.77.3145
–0.2
8.36.7
110
A
C
B
Figure 3: Mean change in adjusted estimatedGFR (eGFR) from baseline tomonths 11, 23 and 35 postrandomization according to(A) Cockcroft-Gault, (B) Nankivell and (C) MDRD4 formulae in patients randomized to everolimus or CNI therapy. The between-group differences in the adjusted change from baseline at each time point are indicated above the bars. p-Values refer to the comparison
between groups. Values below the graphs show mean trough (C0) concentrations of everolimus in the everolimus group and tacrolimusor cyclosporine (CsA) in the CNI cohort at each time point. CNI, calcineurin inhibitor; MDRD4, Modification of Diet in Renal Disease(four-variable).
Table 3: Efficacy endpoints (ITT population)
Randomization to month 11(ITT population)
Randomization to month 11(extension study population)
Months 11–35(extension study population)
CNI-free(n¼96)
CNI(n¼98) p-Value1
CNI-free(n¼41)
CNI(n¼40) p-Value1
CNI-free(n¼41)
CNI(n¼40) p-Value1
BPAR, n (%) 17 (17.7) 15 (15.3) 0.702 8 (19.5) 1 (2.5) 0.029 2 (4.9) 0 (0.0) 0.494Treated BPAR, n (%) 13 (13.5) 10 (10.2) 0.512 7 (17.1) 0 (0.0) 0.012 2 (4.9) 0 (0.0) 0.494
Graft loss, n (%) 2 (2.1) 2 (2.0) 1.000 0 (0.0) 0 (0.0) – 0 (0.0) 0 (0.0) –Death, n (%) 4 (4.2) 4 (4.1) 1.000 0 (0.0) 0 (0.0) – 0 (0.0) 2 (5.0) 0.241Treatment failure (BPAR, graft loss,
death or loss to follow-up)
20 (20.8) 20 (20.4) 1.000 8 (19.5) 1 (2.5) 0.029 2 (4.9) 2 (5.0) 1.000
1Fisher’s exact test.BPAR, biopsy-proven acute rejection; CNI, calcineurin inhibitor; ITT, intent-to-treat.
The PROTECT Study: Results at 3 Years
707American Journal of Transplantation 2014; 14: 701–710

3. COMPLICACIONES METABÓLICAS
ORIGINAL ARTICLE
Corticosteroid-free immunosuppression in liver transplanta-tion: a meta-analysis and meta-regression of outcomesGeorge Sgourakis,1,2 Arnold Radtke,2 Ioannis Fouzas,3 Sofia Mylona,1 Kostantinos Goumas,1
Ines Gockel,1 Hauke Lang2 and Constantine Karaliotas1
1 Second Surgical Department and Surgical Oncology Unit of ‘‘Korgialenio–Benakio’’, Red Cross Hospital, Athens, Greece
2 Department of General and Abdominal Surgery, Johannes Gutenberg University Hospital, Mainz, Germany
3 Organ Transplant Unit, Hippokration Hospital, Aristotle University Medical School, Thessaloniki, Greece
Introduction
The utilization of corticosteroids has been the basis oflessening rejection risk following liver transplantation.Steroids, conversely, are associated with a large numberof side-effects including the potential recurrence ofhepatitis C virus (HCV). Chronic hepatitis C virusinfection is the most prevalent indication for liver trans-plantation, accounting for at least 40% of all transplantsperformed in the United States [1]. With considerablyimproved short-term outcomes over the last two dec-ades [2], the contemporary preoccupations in liver
transplantation have moved away from avoiding rejec-tion per se to precluding toxicity from anti-rejectionregimens. Many authors believe that steroids can bewithdrawn early without jeopardizing safety [3,4], butthe duration of steroid administration after liver trans-plantation and the likely role of total steroid avoidanceremain contentious.
A number of randomized clinical trials (RCT) havebeen published to study outcomes with steroid avoidancein liver transplantation. A recently published good meta-analysis addressing the subject has to be seen with skepti-cism because of some flaws in methodology [5].
Keywords
evidence-based, liver transplantation, meta-
analysis, orthotopic liver transplantation,
publication bias, steroid withdrawal.
Correspondence
George Sgourakis MD, PhD, 11 Mantzarou
str., Neo Psychiko, 15451, Athens, Greece.
Tel.: + 30-210-6716015; fax: +30-210-
6716015; e-mail: [email protected]
Received: 2 March 2009
Revision requested: 2 April 2009
Accepted: 14 April 2009
doi:10.1111/j.1432-2277.2009.00893.x
Abstract
To examine the impact of steroid withdrawal from the immunosuppressionprotocols in liver transplantation. The electronic databases Medline, Embase,Pubmed and the Cochrane Library were searched. Meta-analysis pooled theeffects of outcomes of a total of 2590 patients enrolled into 21 randomizedcontrolled trials (RCTs), using classic and modern meta-analytic methods.Meta-analysis of RCTs addressing patients transplanted for any indicationshowed no differences between corticosteroid-free immunosuppression and ste-roid-based protocols in most of the analyzed outcomes. More importantly,steroid-free cohorts appeared to benefit in terms of de novo diabetes mellitusdevelopment [R.R = 1.86 (1.43, 2.41)], Cytomegalovirus (CMV) infection[R.R = 1.47 (0.99, 2.17)], cholesterol levels [WMD = 19.71 (13.7, 25.7)], thenumber of patients that received the allocated treatment [O.R = 1.55 (1.17,2.05)], severe acute rejection [R.R = 1.71 (1.14, 2.54)] and overall acute rejec-tion [R.R = 1.31 (1.09, 1.58)] (when steroids were replaced in the steroid-freearm). Taking RCTs into account independently when steroids were notreplaced, overall acute rejection was favoring the steroid-based arm [R.R =0.75 (0.58, 0.98)]. Studies addressing exclusively transplanted HCV patientsdemonstrated a significant advantage of steroid-free protocols consideringHCV recurrence [R.R = 1.15 (1.01, 1.13)], acute graft hepatitis [O.R = 3.15(1.18, 8.40)], and treatment failure [O.R = 1.87 (1.33, 2.63)]. No unfavorableeffects were observed after steroid withdrawal during short-term follow-up. Onthe contrary, significant advantages were documented.
Transplant International ISSN 0934-0874
ª 2009 The Authors
892 Journal compilation ª 2009 European Society for Organ Transplantation 22 (2009) 892–905
Sgourakis et al, Transplant Int (2009)
between corticosteroid-free immunosuppression andsteroid-based protocols in most of the analyzed outcomes.More importantly, steroid-free cohorts appeared to bene-fit in terms of de novo diabetes mellitus development,CMV infection, cholesterol levels, the number of patientsthat received the allocated treatment, severe acuterejection and in overall acute rejection (when steroidswere replaced in the steroid-free arm). Taking RCTsinto account independently when steroids were notreplaced, overall acute rejection was favoring the steroid-based arm.
Studies addressing exclusively transplanted HCVpatients demonstrated a significant advantage of steroid-free protocols considering HCV recurrence, acute grafthepatitis, and treatment failure.
We recognize the potential heterogeneity of evaluatingstudies with different immunosuppression protocols.Actually, meta-regression established that differences inthe use of main and complementary immunosuppressionagents did not influence our conclusions: the type of cal-cineurin inhibitor as part of the immunosuppression pro-tocol, the addition of perioperative steroids in the
1.86
0.83
–0.19
–1.22
–2.24
0.34 HCV recurrence
Acute rejectionSteroids not replaced Steroids replaced
Sta
ndar
dize
d ef
fect
siz
eS
tand
ardi
zed
effe
ct s
ize
–0.03
–0.39
–0.76
–1.13
–2.02 –1.01 0.00Normal quantile
1.01 2.02
–1.80 –0.90 0.00Normal quantile
0.90 1.80
Figure 4 Normal quantile plot for
inspection of publication bias concerning
‘acute rejection’ and ‘HCV recurrence’.
The standardized effect size (Odds Ratio)
is plotted against the normal quantile
values. The distribution of effect sizes is
similar to the distribution of normal
quantiles, as data points fall close to the
line X = Y.
Boillot
Relative risk meta-analysis plot (fixed effects)Post-transplant diabetes Relative risk meta-analysis plot (random effects)
CMV infection
Eason
Liado
Margarit
Moench
Lerut
Washbum
Kato
Klintmalm 1–3
Klintmalm 2–3
Reggiani
Combined (fixed) Combined (random)
Boillot2.68 (1.65, 4.38)
8.14 (1.39, 49.42)
1.27 (0.73, 2.23)
2.63 (0.67, 10.86)
0.78 (0.36, 1.66)
0.50 (0.07, 3.71)
1.00 (0.19, 5.17)
4.37 (1.55, 13.30)
1.60 (0.62, 4.08)
2.19 (0.90, 5.27)
0.60 (0.15, 2.21)
1.86 (1.43, 2.41)
Eason
Liado
Margarit
Moench
Pageaux
Tisone
Nashan
Samonakis
1.47 (0.99, 2.17)
2.25 (1.33, 3.83)
4.75 (1.57, 14.91)
1.65 (0.74, 3.69)
2.64 (0.23, infinity)
1.33 (0.75, 2.40)
0.95 (0.72, 1.26)
0.52 (0.07, 3.75)
1.04 (0.26, 4.18)
1.12 (0.40, 3.13)
0.01 0.1 0.2 0.5 1 2 5 10 100Favors steroids Favors steroids-freeRelative risk (95% confidence interval)
0.01 0.1 0.2 0.5 1 2 5 10 100Favors steroids Favors steroids-freeRelative risk (95% confidence interval)
Figure 5 Meta-analysis of outcomes: ‘post-transplant diabetes development’ (fixed effects) and ‘CMV infection’ (random effects).
Sgourakis et al. Steroid withdrawal in liver transplantation
ª 2009 The Authors
Journal compilation ª 2009 European Society for Organ Transplantation 22 (2009) 892–905 901
nonreplacement of steroids in the corticosteroid-freeimmunosuppression group concerning acute rejection(P = 0.036).
Randomization tests were used to test (re-samplingtests generated from 999 iterations) the significance ofour model structure in terms of acute rejection [poolingthe effects of different regimens (different immunosup-pressive agents substituting steroids) in the corticosteroid-free immunosuppression group]. Mean Effect Size wasequal to )0.0802 and Bootstrap 95% CI = )0.1278 to)0.0341and probability P = 0.998).
Cumulative meta-analysis showed a relatively consistentevidence of no statistical difference in the incidence ofHCV recurrence between steroid and corticosteroid-freeimmunosuppression group over the years 2005–2008(Fig. 8). Based on this evidence, the addition of anyfuture study would contribute little to the cumulativebody of evidence (Mean effect size: )0.0802, Bootstrap-ping CI: )0.1231 to )0.0345).
As far as it concerns cumulative meta-analysis for acuterejection, the point estimates and their confidence inter-vals stabilized from year 2005 and on and remainedunchanged when steroids were not replaced (Mean effectsize: 0.1912 Bootstrapping CI: 0.0528 to 0.3542) but whensteroids were replaced this became evident only from year2007 (Mean effect size: )0.2078 Bootstrapping CI:)0.6771 to )0.0786) (Fig. 9).
Discussion
Meta-analysis of RCT addressing collectively patientstransplanted for any indication showed no differences
Relative risk meta-analysis plot (random effects)Steroids not replaced
Relative risk meta-analysis plot (fixed effects)Steroids replaced
Moench 0.73 (0.46, 1.14)
0.72 (0.37, 1.38)
1.23 (0.92, 1.71)
0.80 (0.40, 1.58)
0.56 (0.21, 1.43)
0.22 (0.80, 0.59)
0.45 (0.14, 1.36)
0.64 (0.41, 1.00)
0.62 (0.37, 1.01)
1.20 (0.58, 2.50)
0.36 (0.05, 2.43)
0.33 (0.05, 1.98)
1.05 (0.81, 1.36)
0.75 (0.58, 0.98)
2.59 (1.30, 5.16)
1.24 (0.52, 2.90)
1.60 (0.28, 10.51)
2.63 (1.04, 7.09)
2.26 (1.01, 5.16)
1.22 (0.69, 2.18)
1.75 (0.68, 4.79)
1.03 (0.81, 1.31)
1.50 (0.34, 6.84)
3.12 (1.05, 9.87)
1.31 (1.09, 1.58)
Liado
Samonakis
Margarit
Pelletier
Reggiani
Studenick
Pageaux
Filipponi
Lerut
Belli A vs. B
Belli A vs. C
Tisone
Combined (random)
Combined (fixed)
Relative risk (95% confidence interval)
Klintmalm 1 vs. 3
Klintmalm 2 vs. 3
Kato
Lupo
Varo
Eason
Langrehr
Boillot
Washbum
Nashan
Relative risk (95% confidence interval)0.01
Favors steroids0.1
0.2Favors steroids Favors steroids-free
0.5 1 2 5 10 100
0.2 0.5 1 2 5Favors steroid-free
Figure 2 Meta-analysis of outcomes of ‘acute rejection’ in studies
addressing patients transplanted for any indication. Steroids not
replaced (upper panel); Steroids replaced (lower panel).
0 0.2 0.4 0.61 - specificity
0.8 1 00
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1Sensitivity SensitivitySROC Curve SROC Curve CMV infection
Acute rejectionSteroids not replaced
AsymmetricSROCAUC = 0.5126SE(AUC) = 0.0000Q* = 0.4872SE(Q*) = 0.0195
AsymmetricSROCAUC = 0.5092SE(AUC) = 0.0256Q* = 0.4905SE(Q*) = 0.0265
0.2 0.4 0.61 - specificity
0.8 1
Figure 3 Summary of study results concerning ‘acute rejection (steroids not replaced)’ (left panel) and ‘CMV infection’ (right panel) on a ROC
curve: the fitting of the ROC curve is presented by asymmetrical curves around the ‘Sensitivity–Specificity’ line as the Diagnostic Odds Ratio was
not constant. All but two of the studies (concerning only acute rejection) depicted by the filled circles are within the curvilinear lines.
Steroid withdrawal in liver transplantation Sgourakis et al.
ª 2009 The Authors
900 Journal compilation ª 2009 European Society for Organ Transplantation 22 (2009) 892–905
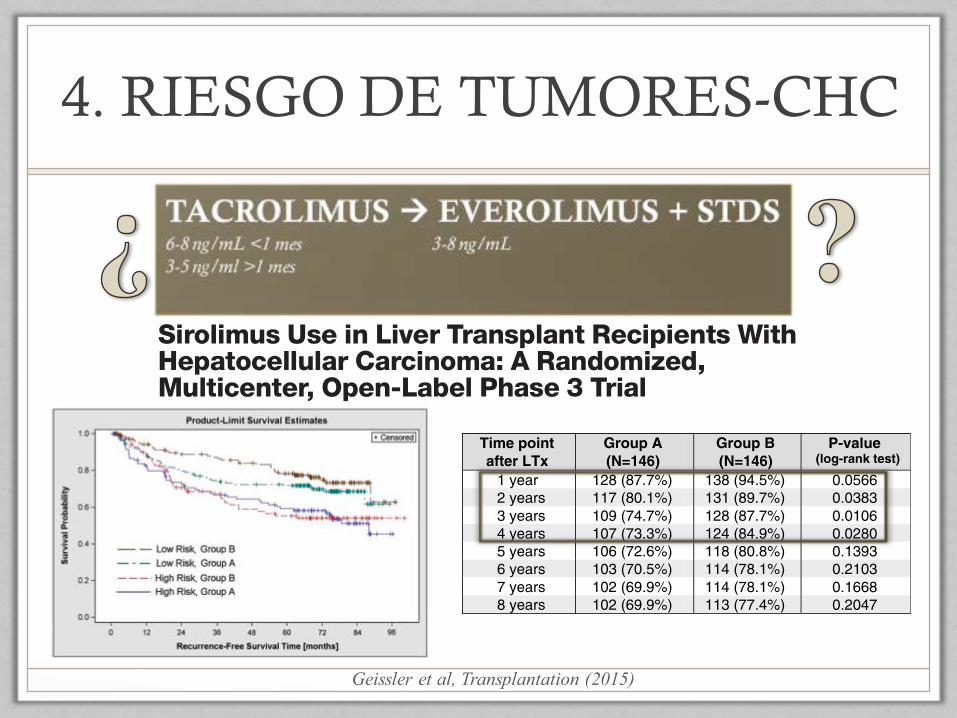
4. RIESGO DE TUMORES-CHC
Sirolimus Use in Liver Transplant Recipients WithHepatocellular Carcinoma: A Randomized,Multicenter, Open-Label Phase 3 TrialEdward K. Geissler, PhD,1 Andreas A. Schnitzbauer, MD,1,2 Carl Zülke, MD,1 Philipp E. Lamby, MD,1
Andrea Proneth, MD,1 Christophe Duvoux, MD,3 Patrizia Burra, MD,4 Karl-Walter Jauch, MD,5
Markus Rentsch, MD,5 Tom M. Ganten, MD,6 Jan Schmidt, MD,6 Utz Settmacher, MD,7 Michael Heise, MD,7,8
Giorgio Rossi, MD,9 Umberto Cillo, MD,10 Norman Kneteman, MD,11 René Adam, MD,12 Bart van Hoek, MD,13
Philippe Bachellier, MD,14 Philippe Wolf, MD,14 Lionel Rostaing, MD,15 Wolf O. Bechstein, MD,2
Magnus Rizell, MD,16 James Powell, MD,17 Ernest Hidalgo, MD,17 Jean Gugenheim, MD,18
Heiner Wolters, MD,19 Jens Brockmann, MD,19 André Roy, MD,20 Ingrid Mutzbauer,1 Angela Schlitt, MD,1
Susanne Beckebaum, MD,21 Christian Graeb, MD,5 Silvio Nadalin, MD,22 Umberto Valente, MD,23
Victor Sánchez Turrión, MD,24 Neville Jamieson, MD,25 Tim Scholz, MD,26 Michele Colledan, MD,27
Fred Fändrich, MD,28 Thomas Becker, MD,28 Gunnar Söderdahl, MD,29 Olivier Chazouillères, MD,30
Heikki Mäkisalo, MD,31 Georges-Philippe Pageaux, MD,32 Rudolf Steininger, MD,33 Thomas Soliman, MD,33
Koert P. de Jong, MD,34 Jacques Pirenne, MD,35 Raimund Margreiter, MD,36 Johann Pratschke, MD,36
Antonio D. Pinna, MD,37 Johann Hauss, MD,38 Stefan Schreiber, MD,38 Simone Strasser, MD,39
Jürgen Klempnauer, MD,40 Roberto I. Troisi, MD,41 Sherrie Bhoori, MD,42 Jan Lerut, MD,43
Itxarone Bilbao, MD,44 Christian G. Klein, MD,21 Alfred Königsrainer, MD,22 Darius F. Mirza, MD,45
Gerd Otto, MD,8 Vincenzo Mazzaferro, MD,42 Peter Neuhaus, MD,46 and Hans J. Schlitt, MD1
Background.We investigated whether sirolimus-based immunosuppression improves outcomes in liver transplantation (LTx)candidates with hepatocellular carcinoma (HCC). Methods. In a prospective-randomized open-label international trial, 525LTx recipients with HCC initially receiving mammalian target of rapamycin inhibitor–free immunosuppression were randomized4 to 6 weeks after transplantation into a group on mammalian target of rapamycin inhibitor–free immunosuppression (group A:264 patients) or a group incorporating sirolimus (group B: 261). The primary endpoint was recurrence-free survival (RFS);intention-to-treat (ITT) analysis was conducted after 8 years. Overall survival (OS) was a secondary endpoint. Results.Recurrence-free survival was 64.5% in group A and 70.2% in group B at study end, this difference was not significant(P = 0.28; hazard ratio [HR], 0.84; 95% confidence interval [95% CI], 0.62; 1.15). In a planned analysis of RFS rates at yearly in-tervals, group B showed better outcomes 3 years after transplantation (HR, 0.7; 95% CI, 0.48-1.00). Similarly, OS (P = 0.21;HR, 0.81; 95% CI, 0.58-1.13) was not statistically better in group B at study end, but yearly analyses showed improvement outto 5 years (HR, 0.7; 95% CI, 0.49-1.00). Interestingly, subgroup (Milan Criteria-based) analyses revealed that low-risk, rather thanhigh-risk, patients benefitedmost from sirolimus; furthermore, younger recipients (age≤60) also benefited, aswell sirolimusmono-therapy patients. Serious adverse event numbers were alike in groups A (860) and B (874). Conclusions. Sirolimus in LTx re-cipients with HCC does not improve long-term RFS beyond 5 years. However, a RFS and OS benefit is evident in the first 3 to5 years, especially in low-risk patients. This trial provides the first high-level evidence base for selecting immunosuppression inLTx recipients with HCC.
(Transplantation 2015;00: 00–00)
Hepatocellular carcinoma (HCC) is a common malig-nancy causing substantial morbidity and mortality
worldwide that can be treated surgically in only about 30%of patients.1 In many of those surgical cases, liver transplan-tation (LTx) is the only potentially curative treatment option,especially in patients where the tumor size, number, andspread are limited according to the Milan Criteria,2 or otherdefined parameters.3, 4 Because the vast majority of these pa-tients have liver cirrhosis, 2 otherwise terminal diseases are
potentially cured by LTx. However, good outcomes in thesepatients are diminished by the problem of HCC recurrenceor redevelopment in about 1 of 5 individuals. Indeed, immu-nosuppression needed to prevent organ rejection has longbeen associated with cancer,5 and the most commonly usedconventional immunosuppressive drugs are calcineurin in-hibitors, which have specific tumor-promoting activities.6, 7
In contrast, although also immunosuppressive, mammaliantarget of rapamycin (mTOR) inhibitors are an exceptional
OriginalClinicalScience
Transplantation ■ Month 2015 ■ Volume 00 ■ Number 00 www.transplantjournal.com 1
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
Geissler et al, Transplantation (2015)
recent trial results showing that everolimus had no effect onadvanced HCC in non-LTx recipients,31 inferring togetherthatmTOR inhibitors alone are not effective deterrents of ad-vanced HCC. On the contrary, patients with tumors stagedwithin Milan Criteria in our study did receive a substantialbenefit. Consistent with the observation of sirolimus beingmost beneficial for lower risk patients, a predetermined sub-group analysis showed that younger recipients (≤60 years)have a greater advantage. From these results, we surmise thatthe anticancer properties of sirolimus are most able to slowdown development of relatively “naive” tumors in their earlystages, which is also in line with our finding that patientswithout pre-LTx treatment of HCC had discernably betteroutcomes, even at study end.
Sirolimus treatment in our study protocol was designed toreflect the “practical” use of immunosuppression in LTx.Therefore, sirolimuswas allowed to be used alone, or in com-bination with approved standard immunosuppressants(eg, calcineurin inhibitors, antimetabolites), because a wide
center-to-center variation is expected in normal practice. In-deed, our study suggests that the presence of sirolimus, evenwhen used in combinatory immunosuppressive regimens,positively influences outcomes for LTx patients with HCC.The degree of advantage for patients on sirolimus can bemeasured if an “area between the curves” analysis32 is per-formed on our ITT data set. Indeed, a post hoc exploratory“area between the curves” statistical analysis revealed thatpatients in group B (including all patients: high and low risk)had an average gain of RFS of 6.4months versus group A pa-tients; the gain in OS in the sirolimus group was 7.0 months.Sirolimus monotherapy may also offer a further advantage.When a planned subgroup analysis of those patients onsirolimus monotherapy was performed, it did show roughly13% to 15% higher RFS and OS rates, versus combinationtherapy patients, but the low proportion (one fifth) of pa-tients on sirolimus monotherapy makes it difficult to knowwhether monotherapy offers reliable advantages. Nonethe-less, our results are consistent with experimental data 7 and
FIGURE 3. Efficacy data on low-versus high risk subgroups (ITT population).
8 Transplantation ■ Month 2015 ■ Volume 00 ■ Number 00 www.transplantjournal.com
Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.
5. ALTO RIESGO DE RECHAZO
Cribado y manejo
agresivo de infecciones
oportunistas
Seguimiento
especializado de riesgo
cardiovascular
Programa específico de
vigilancia oncológica
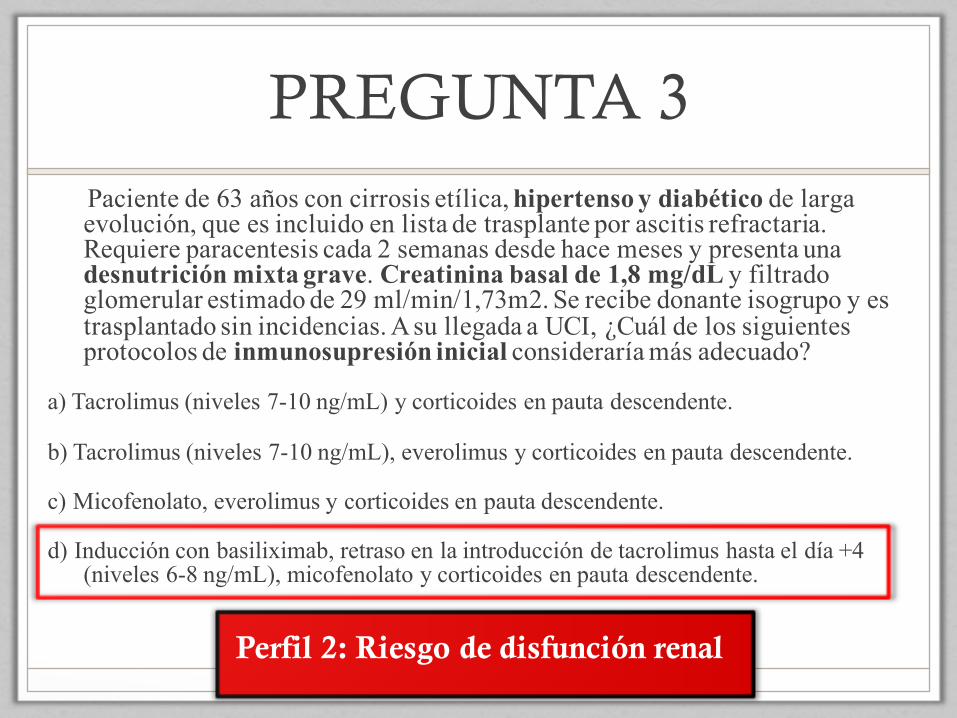
PREGUNTA 3Paciente de 63 años con cirrosis etílica, hipertenso y diabético de larga evolución, que es incluido en lista de trasplante por ascitis refractaria. Requiere paracentesis cada 2 semanas desde hace meses y presenta una desnutrición mixta grave. Creatinina basal de 1,8 mg/dL y filtrado glomerular estimado de 29 ml/min/1,73m2. Se recibe donante isogrupo y es trasplantado sin incidencias. A su llegada a UCI, ¿Cuál de los siguientes protocolos de inmunosupresión inicial consideraría más adecuado?
a) Tacrolimus (niveles 7-10 ng/mL) y corticoides en pauta descendente.
b) Tacrolimus (niveles 7-10 ng/mL), everolimus y corticoides en pauta descendente.
c) Micofenolato, everolimus y corticoides en pauta descendente.
d) Inducción con basiliximab, retraso en la introducción de tacrolimus hasta el día +4 (niveles 6-8 ng/mL), micofenolato y corticoides en pauta descendente.
Perfil 2: Riesgo de disfunción renal
PREGUNTA 4
En cuanto a la inmunosupresión personalizada, señale la respuesta CORRECTA:
a) En un sistema de priorización basado en MELD, la mayoría de los pacientes que acceden al trasplante hepático son inmuno-reactivos y precisan de inmunosupresión intensa.
b) En un sistema de priorización basado en MELD, la mayoría de los pacientes presentan un riesgo elevado de desarrollar disfunción renal post-trasplante, y precisan minimización de anticalcineurínicos.
c) La principal causa de morbimortalidad tras el trasplante hepático es el rechazo en sus diferentes formas clínicas.
d) La recidiva del hepatocarcinoma tras el trasplante se debe únicamente a factores relacionados con el tumor y no está influida por la estrategia de inmunosupresión.

CONCLUSIONES
• Tacrolimus es la pieza central de los protocolos de inmunosupresión en el trasplante hepático.
• En general, no se debe incrementar los niveles en sangre de tacrolimus por encima de10 ng/mL.
• Es importante tener en cuenta las características del paciente a la hora de escoger la pauta de inmunosupresión.
• Se necesitan ensayos clínicos dirigidos a los diferentesperfiles de pacientes.