san jose 2011
TRANSCRIPT
TRATAMIENTO ENDOVASCULAR EN EL
ACV AGUDO
Dr. Marcelo Langleib San Jose 1 de Octubre del 2011
TRATAMIENTO ENDOVASCULAR EN EL
ACV AGUDO
Dr. Marcelo Langleib San Jose 1 de Octubre del 2011
Tratamiento endovascular: objetivos
Expandir la ventana terapeútica
Incluir pacientes resistentes al tratamiento intravenoso o que presentan criterios de exclusión
Aumentar el porcentaje de recanalización
Stroke Tratamiento Stroke Tratamiento
Recanalización o reperfusión
anterograda
Reperfusión global o aumento
de flujo
Reperfusión retrograda
transvenosa
Recanalización o reperfusión
anterograda
Reperfusión global o aumento
de flujo
Reperfusión retrograda
transvenosa
Stroke Tratamiento Recanalización o reperfusión anterograda
Trombolíticos: I/V ó I/A estreptoquinasa, uroquinasa, rtPA
Terapia adyuvante Heparina intra-venosa. Abciximab (ReoPro). Tirofiban (Aggrastat)
Procedimientos mecánicos intra-arteriales Trombectomía endovascular: Catch y Merci Tromboaspiración endovascular: Neurojet, Penumbra Dirrupción mecánica del trombo: Epar Fibrinolisis ultrasónica: MicroLys US Atrapamiento del trombo: Solitaire Stenting primario
Trombolisis IATrombolisis IA
Prolyse in Acute Cerebral Thromboembolism Trial
PROACT-I
PROACT-II
Prolyse in Acute Cerebral Thromboembolism Trial
PROACT-I
PROACT-II r-proUKr-proUK
AlteplaseAlteplase
Emergency Management of Stroke Bridging Trial EMS (IV/IA) Emergency Management of Stroke Bridging Trial EMS (IV/IA)
Stroke 1998
JAMA 1999
PROACT II TrialPROACT II Trial
180 Pacientes
9 mg of IA r-proUK + heparina (n = 121) o solo heparina (n = 59)
Ventana 6hs
Oclusión ACM: Comprobado Angiograficamente
Media NIHSS 17
No HIC o signos tempranos mayores de infarto en TC
180 Pacientes
9 mg of IA r-proUK + heparina (n = 121) o solo heparina (n = 59)
Ventana 6hs
Oclusión ACM: Comprobado Angiograficamente
Media NIHSS 17
No HIC o signos tempranos mayores de infarto en TC
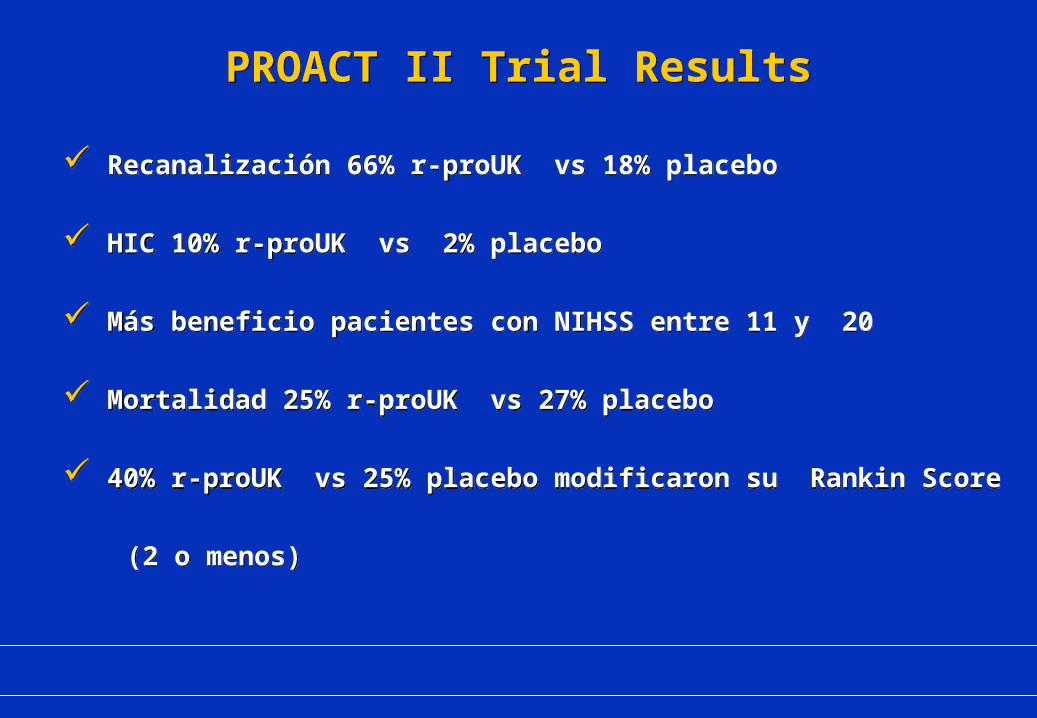
Recanalización 66% r-proUK vs 18% placebo
HIC 10% r-proUK vs 2% placebo
Más beneficio pacientes con NIHSS entre 11 y 20
Mortalidad 25% r-proUK vs 27% placebo
40% r-proUK vs 25% placebo modificaron su Rankin Score
(2 o menos)
Recanalización 66% r-proUK vs 18% placebo
HIC 10% r-proUK vs 2% placebo
Más beneficio pacientes con NIHSS entre 11 y 20
Mortalidad 25% r-proUK vs 27% placebo
40% r-proUK vs 25% placebo modificaron su Rankin Score
(2 o menos)
PROACT II Trial ResultsPROACT II Trial Results
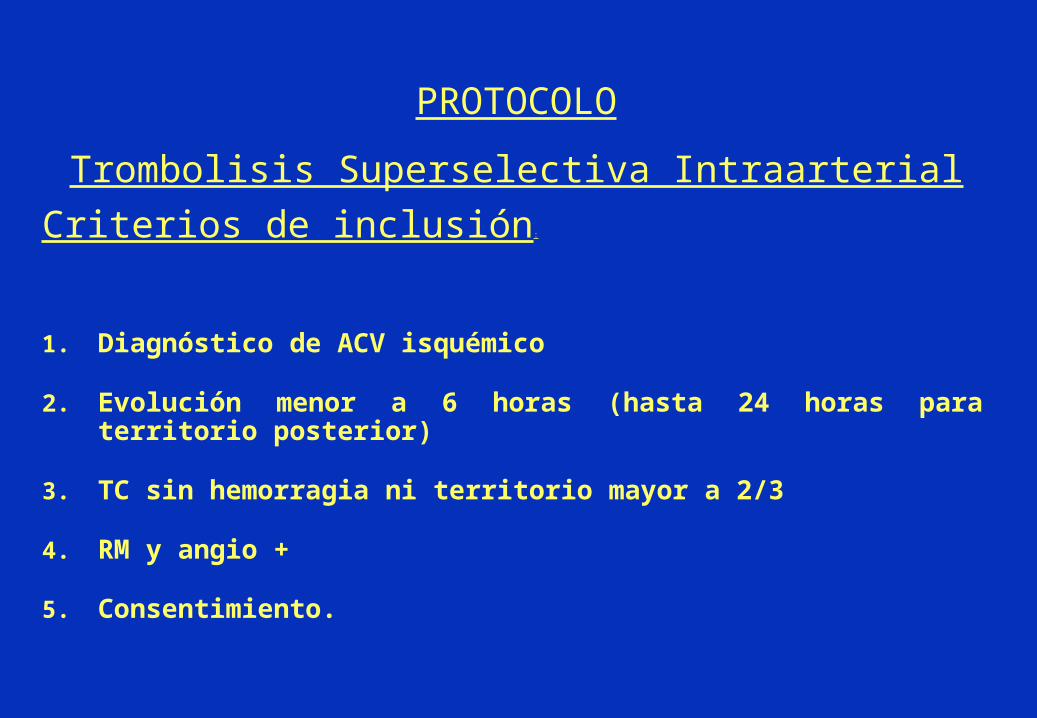
Criterios de inclusión:
1. Diagnóstico de ACV isquémico
2. Evolución menor a 6 horas (hasta 24 horas para territorio posterior)
3. TC sin hemorragia ni territorio mayor a 2/3
4. RM y angio +
5. Consentimiento.
PROTOCOLO
Trombolisis Superselectiva Intraarterial
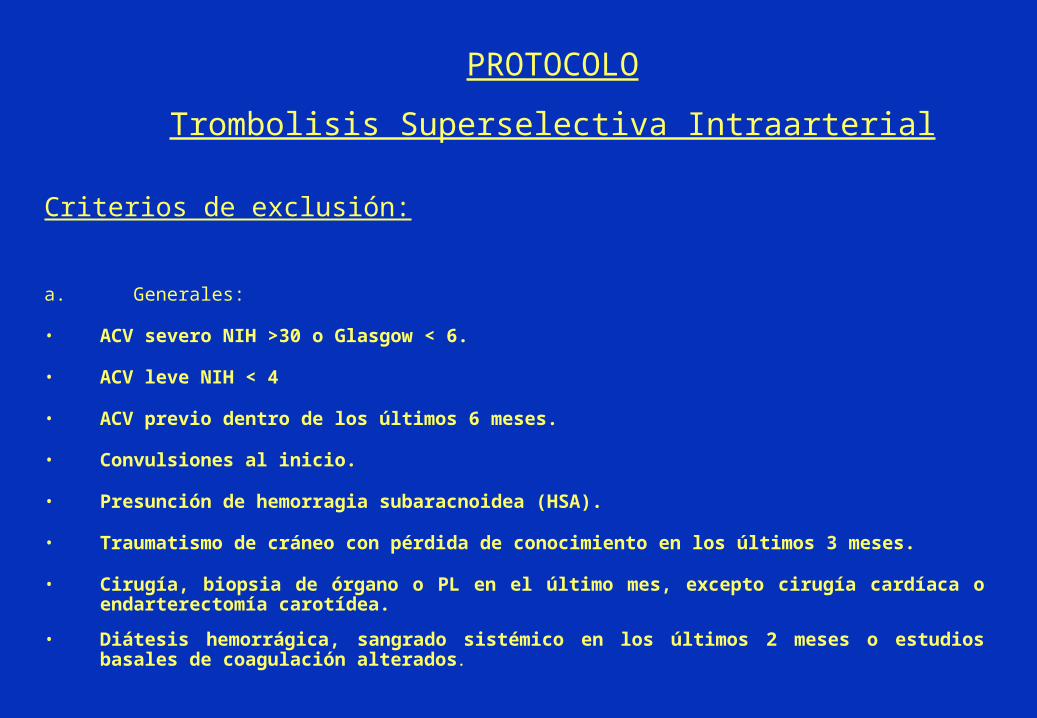
Criterios de exclusión:
a. Generales:
• ACV severo NIH >30 o Glasgow < 6.
• ACV leve NIH < 4
• ACV previo dentro de los últimos 6 meses.
• Convulsiones al inicio.
• Presunción de hemorragia subaracnoidea (HSA).
• Traumatismo de cráneo con pérdida de conocimiento en los últimos 3 meses.
• Cirugía, biopsia de órgano o PL en el último mes, excepto cirugía cardíaca o endarterectomía carotídea.
• Diátesis hemorrágica, sangrado sistémico en los últimos 2 meses o estudios basales de coagulación alterados.
PROTOCOLO
Trombolisis Superselectiva Intraarterial
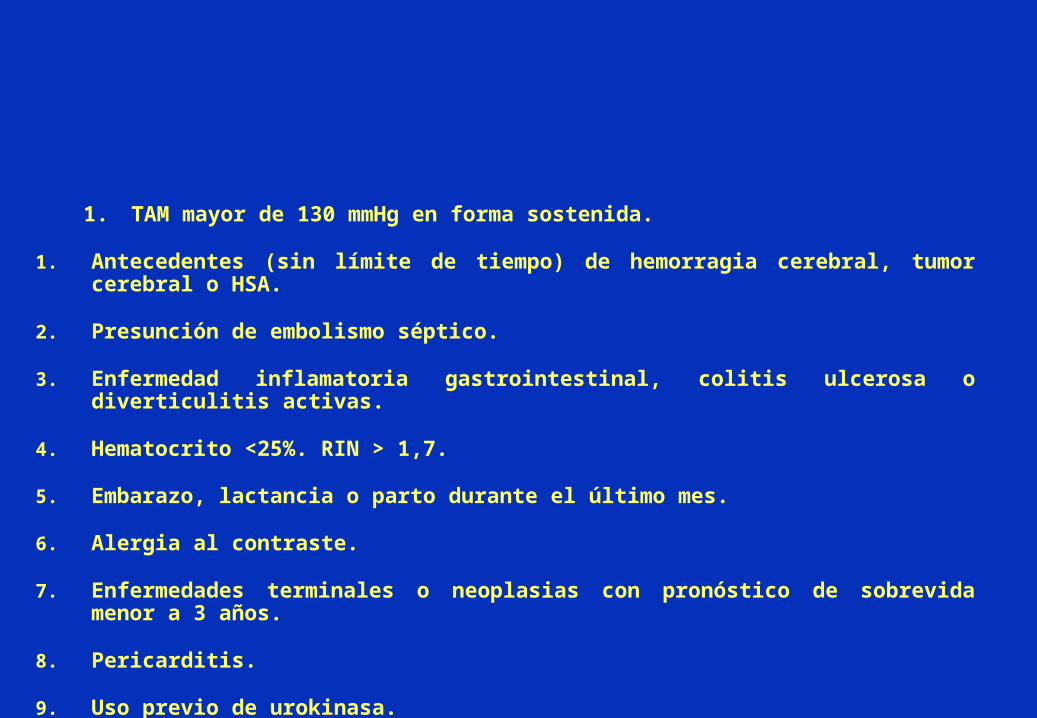
1. TAM mayor de 130 mmHg en forma sostenida.
1. Antecedentes (sin límite de tiempo) de hemorragia cerebral, tumor cerebral o HSA.
2. Presunción de embolismo séptico.
3. Enfermedad inflamatoria gastrointestinal, colitis ulcerosa o diverticulitis activas.
4. Hematocrito <25%. RIN > 1,7.
5. Embarazo, lactancia o parto durante el último mes.
6. Alergia al contraste.
7. Enfermedades terminales o neoplasias con pronóstico de sobrevida menor a 3 años.
8. Pericarditis.
9. Uso previo de urokinasa.
Administración del trombolítico:
Técnica superselectiva con rTPA + 2000 unidades de heparina sistémica.(o rTPA )
Pulse spray con inyecciones de 1mg (rtpa)
Angio de control .
Se suspende infusión a los 60 minutos, ar el fibrinógeno a < 80 mg/dl.
Angio inmediatamente post-infusión.
TAC inmediatamente post-infusión.
Se deja introductor femoral hasta normalización del KPTT.
TAC si existe agravamiento o a las 24 horas.
Tratamiento antitrombótico post-trombolisis:
Luego de retirar introductor y si el fibrinógeno plasmático es mayor a 100 mg/dl comenzar enoxaparina (Clexane®): 40mg (4cc) c/12 hs. vía SC.
A la deambulación o alta se suspende heparinización y se comienza con aspirina 200 mg/día.
Si hay motivos para anticoagulación crónica (p. Ej.. Fuente cardioembólica): warfarina (Coumadin®) 5 mg/día desde el tercer día de la heparinización. Se suspenderá la heparinización en este caso cuando se halla conseguido un RIN de 2-3.
Controles de laboratorio
1. PRE-infusión del trombolítico: hemograma con recuento de plaquetas, Quick, KPTT, fibrinógeno plasmático y muestra adicional para laboratorio de coagulación..
2. Post-infusión a las 1, 6 y 12 horas KPTT y fibrinógeno.
3. Cada 24 horas plaquetas, Quick, KPTT y muestra adicional para laboratorio de coagulación.

COMPLICACIONESCOMPLICACIONES
Stroke 2002
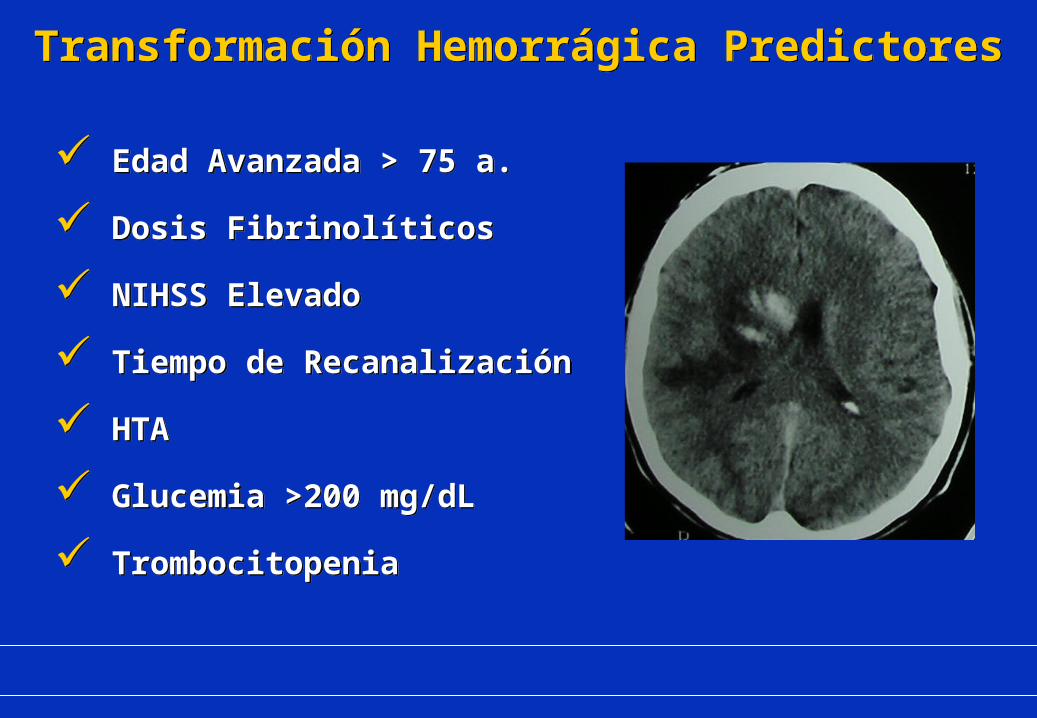
Edad Avanzada > 75 a.
Dosis Fibrinolíticos
NIHSS Elevado
Tiempo de Recanalización
HTA
Glucemia >200 mg/dL
Trombocitopenia
Edad Avanzada > 75 a.
Dosis Fibrinolíticos
NIHSS Elevado
Tiempo de Recanalización
HTA
Glucemia >200 mg/dL
Trombocitopenia
Transformación Hemorrágica PredictoresTransformación Hemorrágica Predictores
“ 8.3% risk of symptomatic brain hemorrhage with
IA thrombolysis in the carotid territory and a 6.5% risk
in the vertebrobasilar territory ”
“ 8.3% risk of symptomatic brain hemorrhage with
IA thrombolysis in the carotid territory and a 6.5% risk
in the vertebrobasilar territory ”
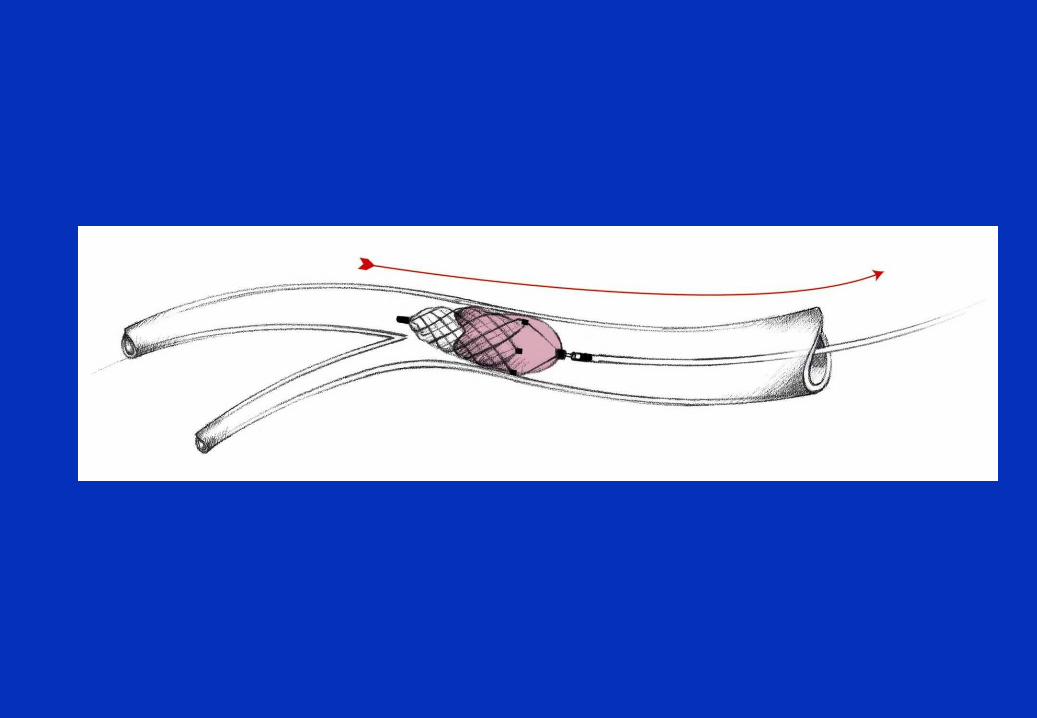
Trombolisis mecánica
Menor riesgo de HIC
Expande la ventana terapéutica
Complementa la trombolisis química
Reemplaza trombolisis ???
Disrupción mecánica
Guías
Lazos
Catéteres y angioplastia
Laser
Cestas metálicas
Stents
Stroke Tratamiento Recanalización mecánica
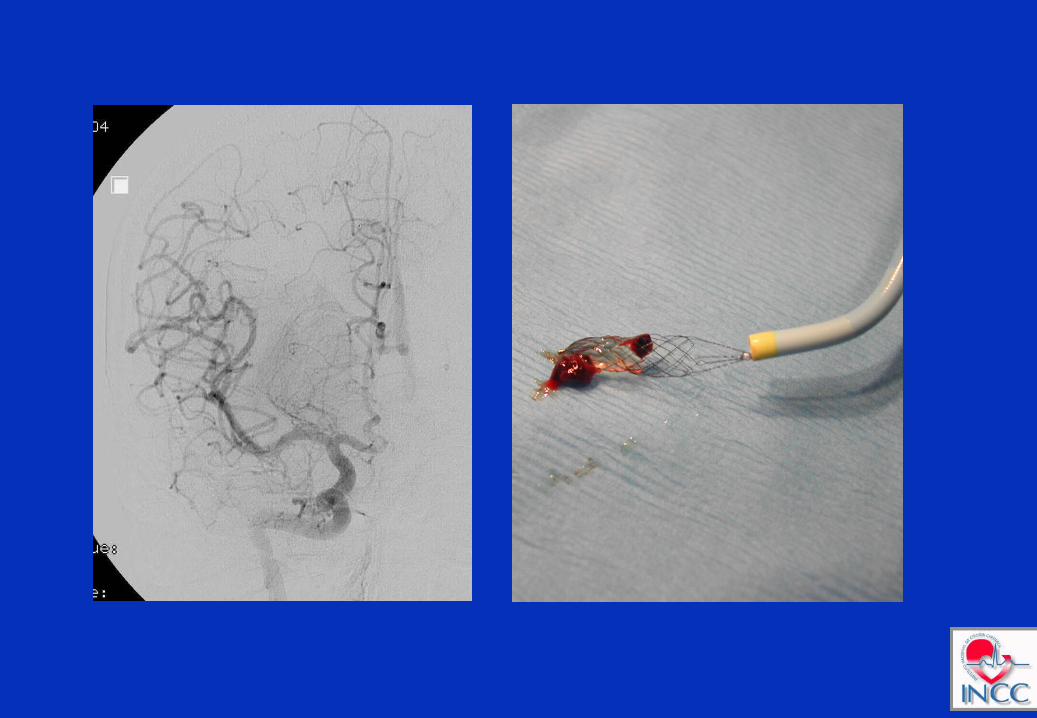
Trombectomía endovascular: Catch y Merci
Tromboaspiración endovascular: Neurojet, Penumbra
Dirrupción mecánica del trombo: Epar
Fibrinolisis ultrasónica: MicroLys US
Atrapamiento del trombo: Solitaire
Stenting primario

Trombolisis mecánica
MERCI Trial
Safety and efficacy of mechanical embolectomy in acute ischemic stroke. Results of the MERCI trial.
Smith WS, Sung G, Starkman S, Saver JL, Kidwell CS, Gobin YP, Lutsep HL, Nesbit GM, Grobelny T, Rymer MM, Silverman IE, Higashida RT, Budzik RF, Marks MP; MERCI Trial Investigators. Department of Neurology, University of California, 505 Parnassus Avenue, San Francisco, CA 94143-0114, USA. [email protected]
BACKGROUND AND PURPOSE
The only Food and Drug Administration (FDA)-approved treatment for acute ischemic stroke is tissue plasminogen activator (tPA) given intravenously within 3 hours of symptom onset. An alternative strategy for opening intracranial vessels during stroke is mechanical embolectomy, especially for patients ineligible for intravenous tPA.
METHODS
We investigated the safety and efficacy of a novel embolectomy device (Merci Retriever®) to open occluded intracranial large vessels within 8 hours of the onset of stroke symptoms in a prospective, nonrandomized, multicenter trial. All patients were ineligible for intravenous tPA. Primary outcomes were recanalization and safety, and secondary outcomes were neurological outcome at 90 days in recanalized versus nonrecanalized patients.
RESULTS
Recanalization was achieved in 46% (69/151) of patients on intention to treat analysis, and in 48% (68/141) of patients in whom the device was deployed. This rate is significantly higher than that expected using an historical control of 18% (P<0.0001). Clinically significant procedural complications occurred in 10 of 141 (7.1%) patients. Symptomatic intracranial hemorrhages were observed in 11 of 141 (7.8%) patients. Good neurological outcomes (modified Rankin score < or =2) were more frequent at 90 days in patients with successful recanalization compared with patients with unsuccessful recanalization (46% versus 10%; relative risk [RR], 4.4; 95% CI, 2.1 to 9.3; P<0.0001), and mortality was less (32% versus 54%; RR, 0.59; 95% CI, 0.39 to 0.89; P=0.01).
CONCLUSIONS
A novel endovascular embolectomy device can significantly restore vascular patency during acute ischemic stroke within 8 hours of stroke symptom onset and provides an alternative intervention for patients who are otherwise ineligible for thrombolytics.
To request a hard copy of this publications to be sent to you in the mail, please click here.Stroke. 2005 Jul;36(7):1432-8. Epub 2005 Jun 16.
linical data show a strong correlation between restoring blood flow to the brain and better overall outcomes for stroke patients. This means that those who have blood flow restored are more often functioning independently and with less disability.
Restoring blood flow is a principal goal when treating ischemic stroke patients. In the Multi MERCI trial, the Merci Retriever® restored blood flow in 55% of patients when used alone, and 68% of the time when used in conjunction with other treatments. For every 3 patients treated with the Merci Retriever, blood flow was restored in approximately 2 patients, and of those 2 patients, one had little or no disability. Specifically, of the patients who had blood flow restored, 49% were functioning independently at their 90-day follow up with the doctor.1
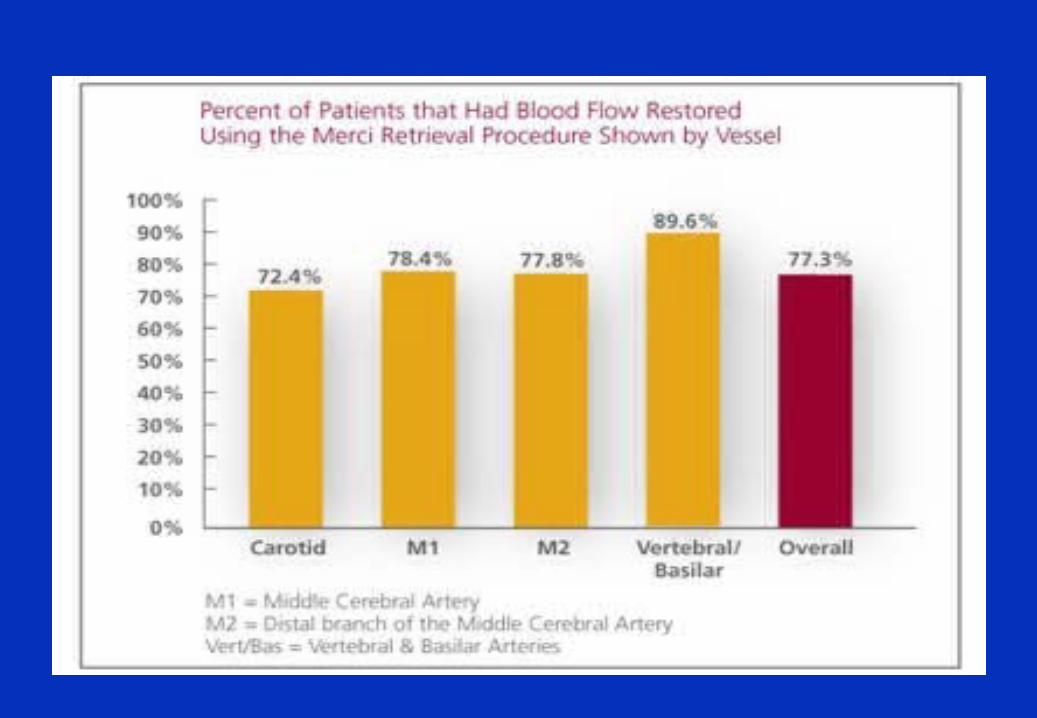
In the Merci Registry, an extensive collection of cases in which the Merci Retriever was used, the revascularization rate was approximately 77% overall and is shown by vessel in the graph.2
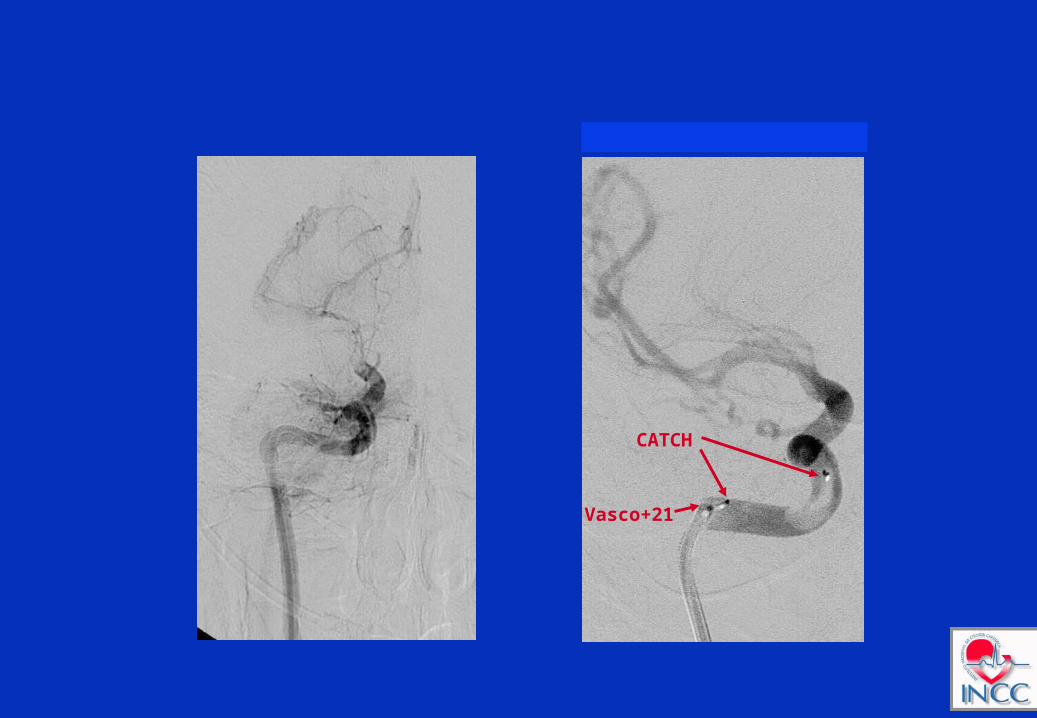
CATCH
Vasco+21
For ev3 Inc. Presentation Use Only – Not for Distribution33
Indication
The ev3 SOLITAIRE™ AB Neurovascular Remodeling Device is designed for the treatment of intracranial neurovascular disease.
*Not approved for sale in the United States. For ev3 Inc. Presentation Use Only – Not for Distribution 33
For ev3 Inc. Presentation Use Only – Not for Distribution34
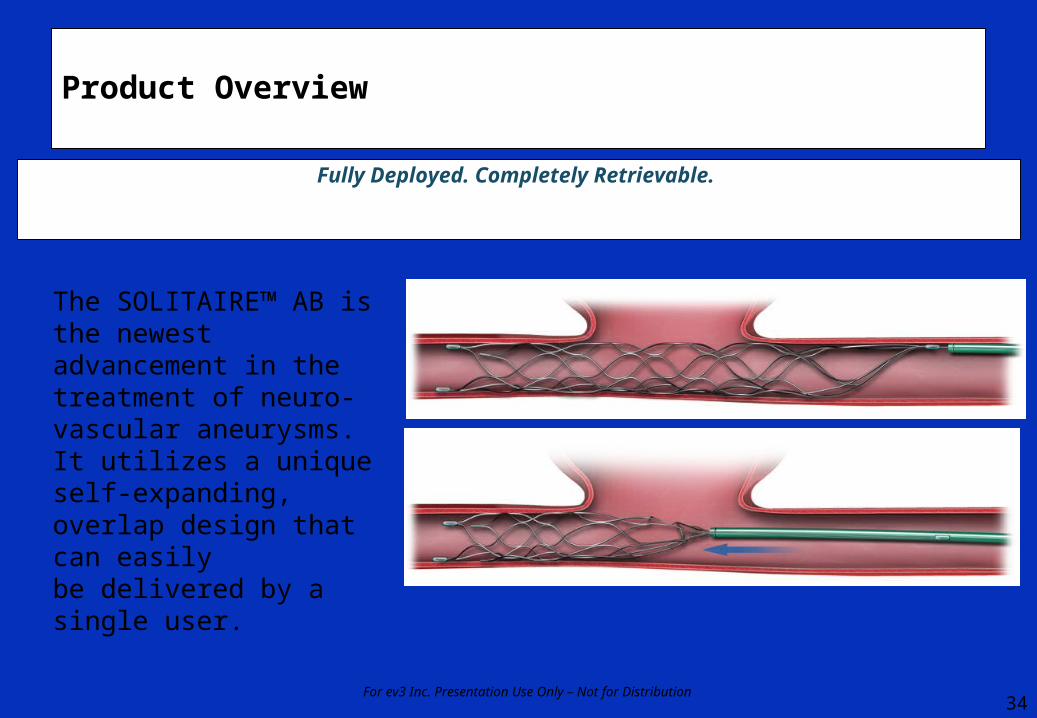
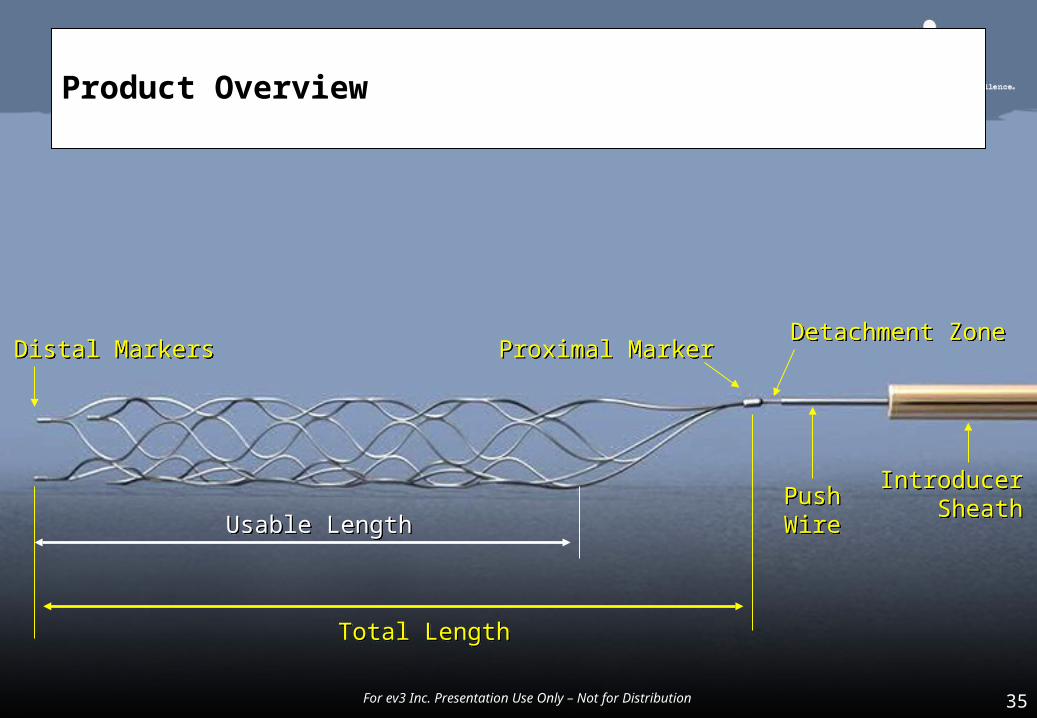
Product Overview
Fully Deployed. Completely Retrievable.
The SOLITAIRE™ AB is the newest advancement in the treatment of neuro-vascular aneurysms. It utilizes a unique self-expanding, overlap design that can easily be delivered by a single user.
For ev3 Inc. Presentation Use Only – Not for Distribution35
Product Overview
Detachment ZoneDetachment Zone
PushWirePushWire
IntroducerSheath
IntroducerSheath
Total LengthTotal Length
Usable LengthUsable Length
Distal MarkersDistal Markers Proximal MarkerProximal Marker
For ev3 Inc. Presentation Use Only – Not for Distribution 35
Submitted on November 25, 2007Accepted on January 28, 2008
Agosto 2008
Interventional Acute Ischemic Stroke Therapy With Intracranial Self-Expanding Stent
Osama O. Zaidat MD, MS*; Thomas Wolfe MD; Syed I. Hussain MD; John R. Lynch MD; Rishi Gupta MD; Joanna Delap RN; Michel T. Torbey MD, MPH; and Brian-Fred Fitzsimmons MD From the Department of Neurology (O.O.Z., T.W., S.I.H., J.R.L., J.D., M.T.T., B.-F.S.), Medical College of Wisconsin and Froedtert Hospital, Milwaukee, Wis; and the Department of Neurology (R.G.), Michigan State University, East Lansing, Mich.
Conclusions—This preliminary experience with SEIS in refractory AIS demonstrated the technical feasibility and high rate of recanalization with acute stenting. Long-term safety and strategies to limit in-stent thrombosis and optimize periprocedural management are crucial before initiating future randomized efficacy studies with SEIS in AIS refractory to standard therapy.
First Food and Drug Administration-Approved Prospective Trial of Primary Intracranial Stenting for Acute StrokeSARIS (stent assisted Recanalization in Acutte Ischemic Stroke)Ehlad Levy et al.November 2009
The Penumbra Pivotal Stroke Trial InvestigatorsThe Penumbra Pivotal Stroke Trial:
Safetly and Effectivenes of a New Generation of Mechanical Devices for Clot Removal in Intracranial Large Vessel Occlusive Disease.
Stroke, August 1, 2009, 40(8): 2761 - 2768
Bewertungen)Business Wire · Mehr Nachrichten von Business Wire · ArchivInitiation of Penumbra, Inc.'s THERAPY Trial Announced at the Society of NeuroInterventional Surgery's 8th Annual Meeting in Colorado Springs, CO
FDA has granted Investigational Device Exemption (IDE) approval and patient enrollment will begin immediately
The THERAPY trial, a Penumbra-sponsored groundbreaking trial designed to prove the clinical benefit of interventional treatment of acute ischemic stroke (AIS) was announced today by the trial''s Principal Investigator J Mocco, MD, MS, Assistant Professor of Neurosurgery, The University of Florida, Gainesville, FL.
"Patient selection is the key to both clinical trial design and high quality patient care. The THERAPY trial focuses on patients who are potentially responsive to aspiration thrombectomy but resistant to intravenous tPA. We believe this design can enable an efficient, cost effective, and most importantly, realistic trial. Treating patients with stroke and providing medical evidence of benefit to those patients'' clinical outcome is the goal of the THERAPY trial," said Dr. Mocco.
"The THERAPY Trial offers the opportunity to prove that embolectomy can improve clinical outcomes in a selective patient group. It complements the more general approach of the NIH-funded 900-subject IMS III Trial. As we pass the half-way point for IMS III, and look forward to its results, we will need further definition of subpopulations that will benefit from endovascular treatments. My hope is that the stroke community will move quickly to randomize patients in these studies and get our current stroke armamentarium established on firmer ground," said Pooja Khatri, MD, MSc., Associate Professor, University of Cincinnati Department of Neurology, Director of Acute Stroke, Greater Cincinnati/Northern Kentucky Stroke Team, and Neurology Principal Investigator.

THE END