edusepsis: un projecte per millorar els resultats clínics ...• los pilares del tratamiento de la...
TRANSCRIPT
Ricard Ferrer Intensive Care Department
Mutua Terrassa University Hospital Barcelona. SPAIN
Edusepsis: Un Projecte per Millorar
els resultats clínics a la Septicemia
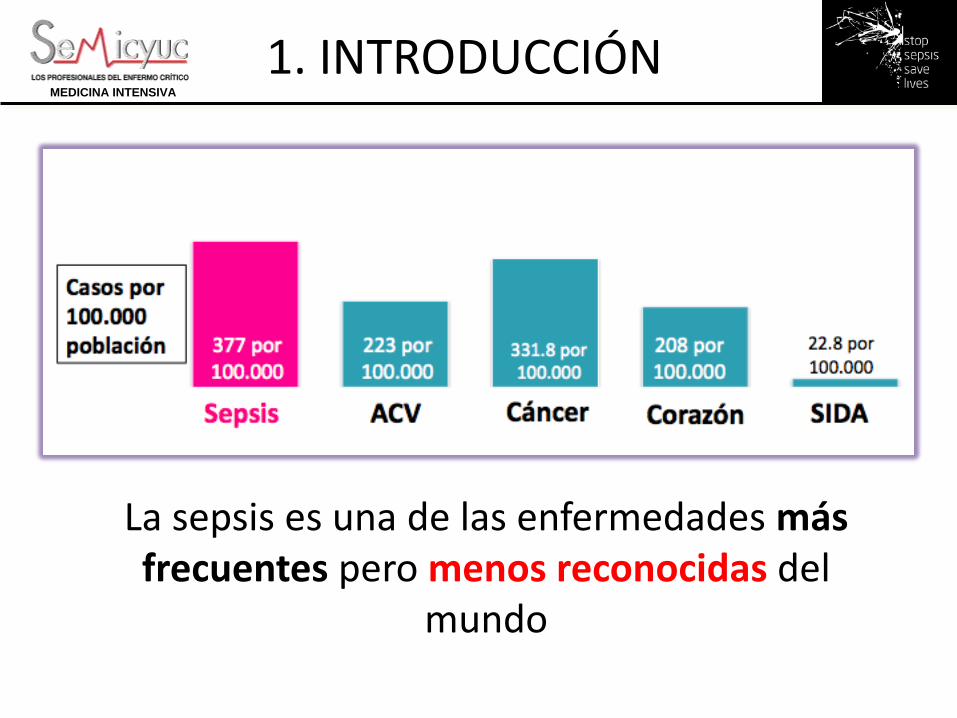
La sepsis es una de las enfermedades más frecuentes pero menos reconocidas del
mundo
1. INTRODUCCIÓN MEDICINA INTENSIVA
Su incidencia está aumentando de
forma exponencial.
Los hospitalizados por sepsis se han duplicado en los últimos 10 años.
1. INTRODUCCIÓN MEDICINA INTENSIVA
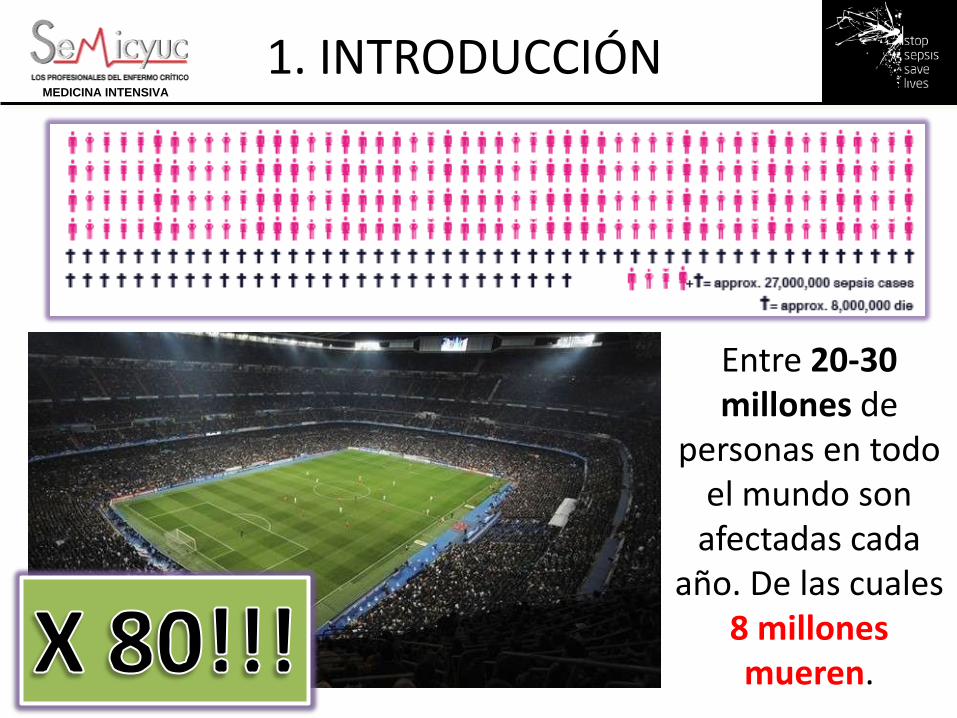
Entre 20-30 millones de
personas en todo el mundo son
afectadas cada año. De las cuales
8 millones mueren.
1. INTRODUCCIÓN MEDICINA INTENSIVA
Cada 4 segundos
alguien muere por sepsis en el
mundo
1. INTRODUCCIÓN MEDICINA INTENSIVA
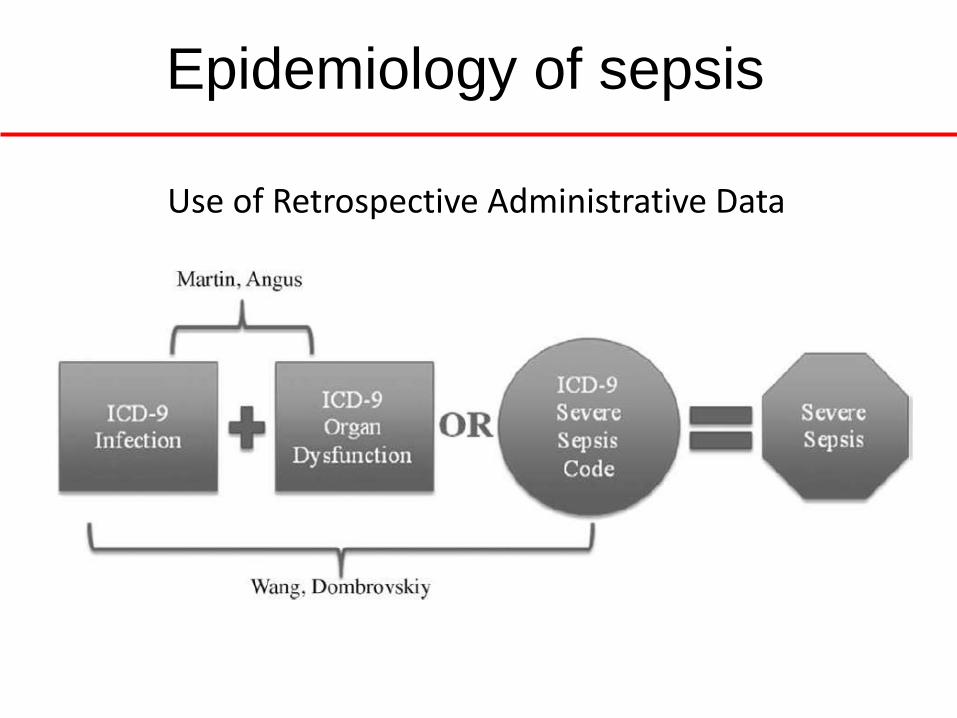
Use of Retrospective Administrative Data
Epidemiology of sepsis
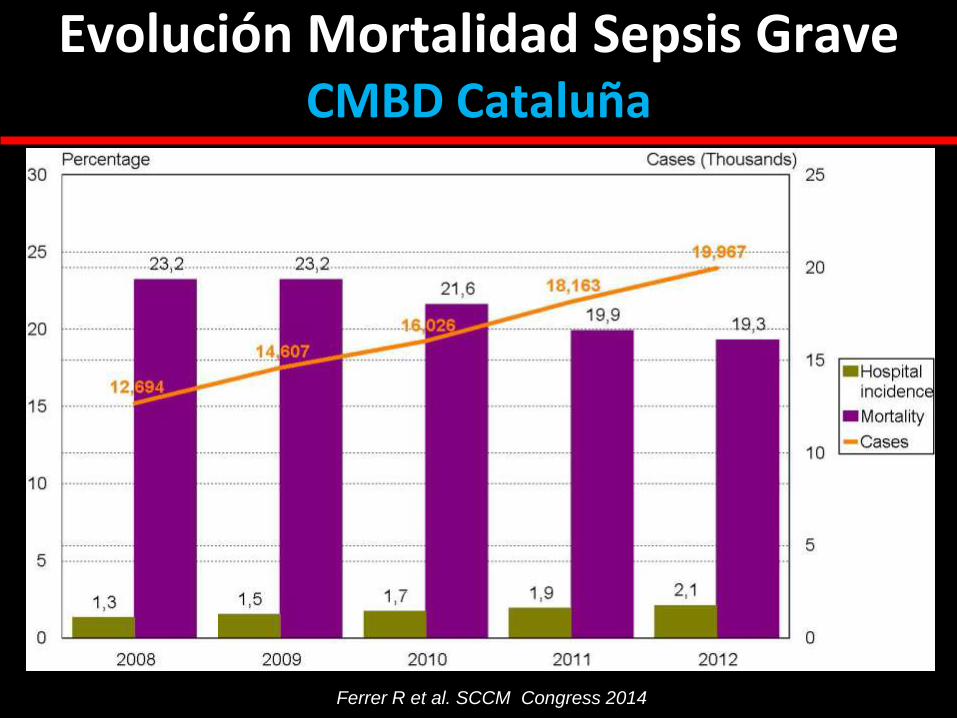
Evolución Mortalidad Sepsis Grave CMBD Cataluña
Ferrer R et al. SCCM Congress 2014
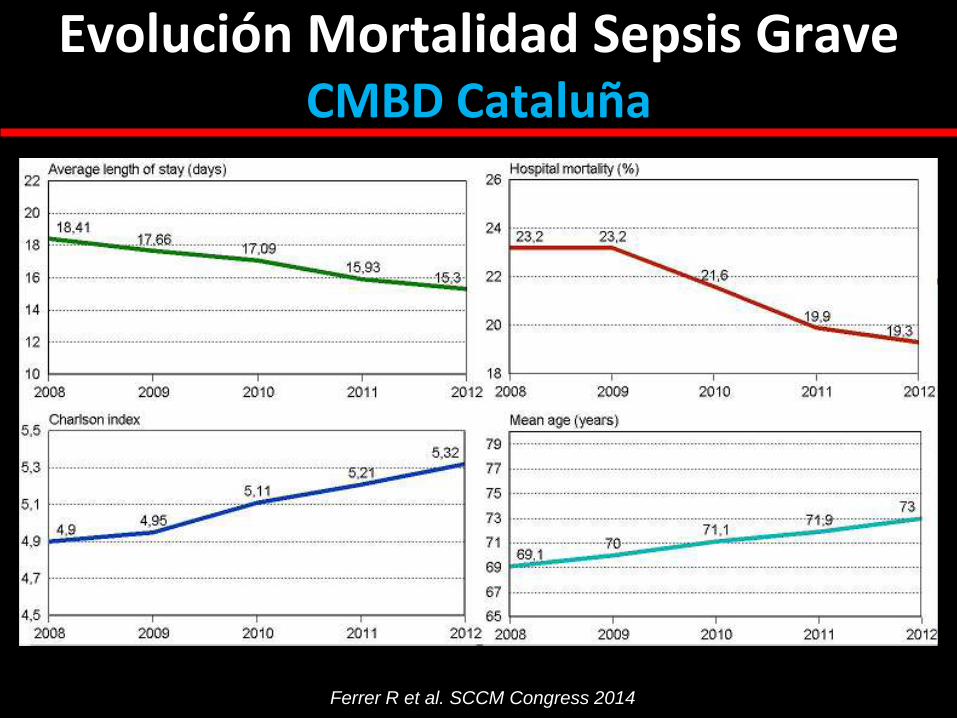
Evolución Mortalidad Sepsis Grave CMBD Cataluña
Ferrer R et al. SCCM Congress 2014
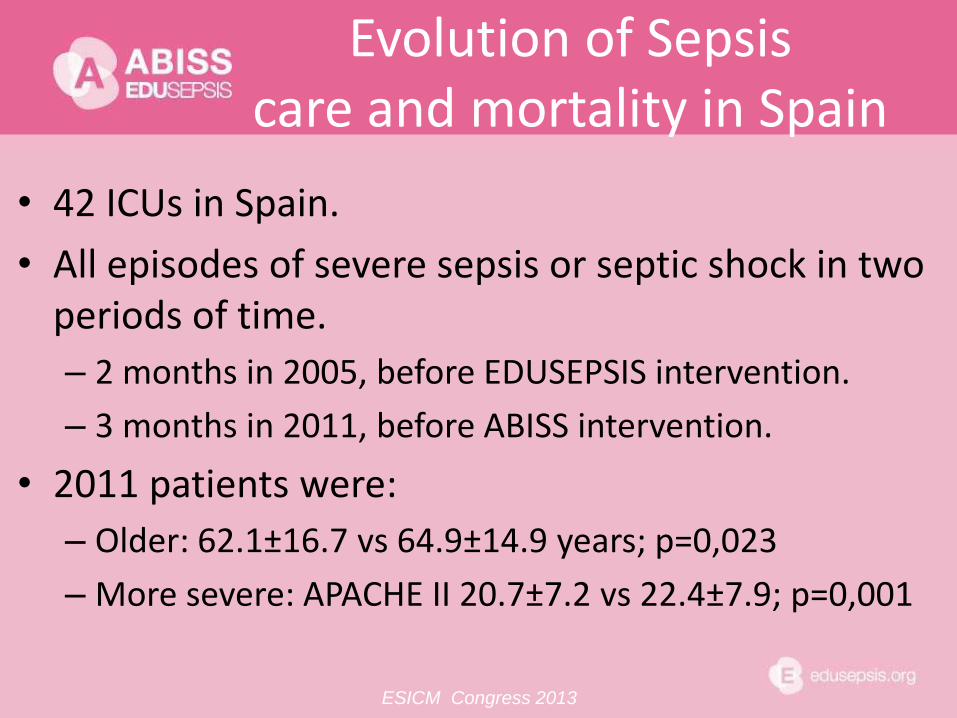
• 42 ICUs in Spain.
• All episodes of severe sepsis or septic shock in two periods of time.
– 2 months in 2005, before EDUSEPSIS intervention.
– 3 months in 2011, before ABISS intervention.
• 2011 patients were:
– Older: 62.1±16.7 vs 64.9±14.9 years; p=0,023
– More severe: APACHE II 20.7±7.2 vs 22.4±7.9; p=0,001
Evolution of Sepsis care and mortality in Spain
ESICM Congress 2013

Evolution of Sepsis Mortality in Spain
p< 0.001
Adjusted mortality: OR 0.638 (0.49-0.831); p=0,001
ESICM Congress 2013
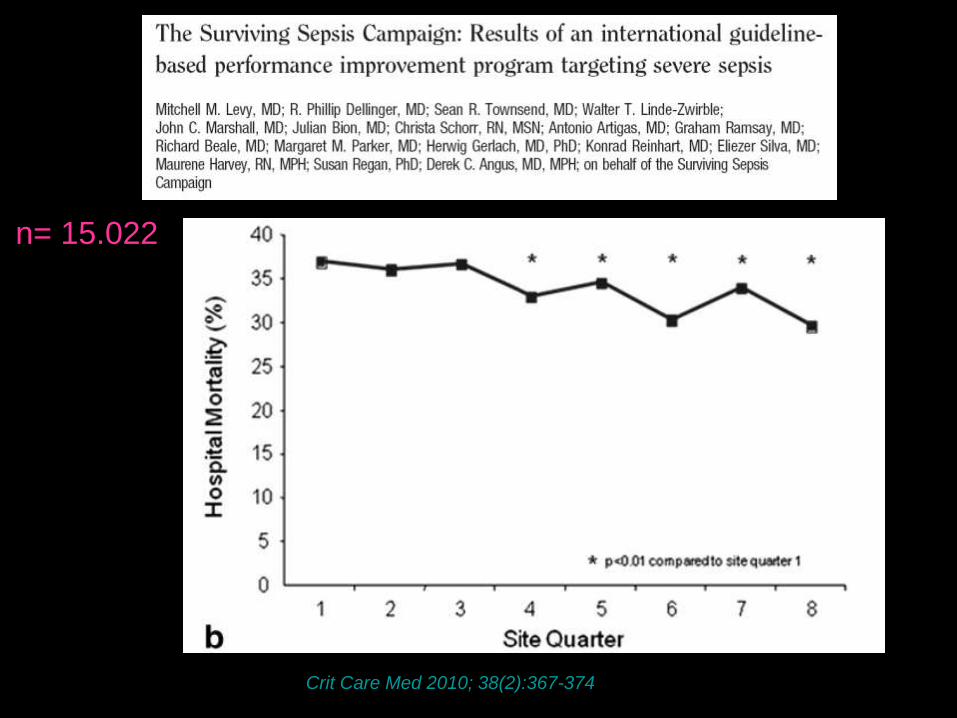
Crit Care Med 2010; 38(2):367-374
n= 15.022
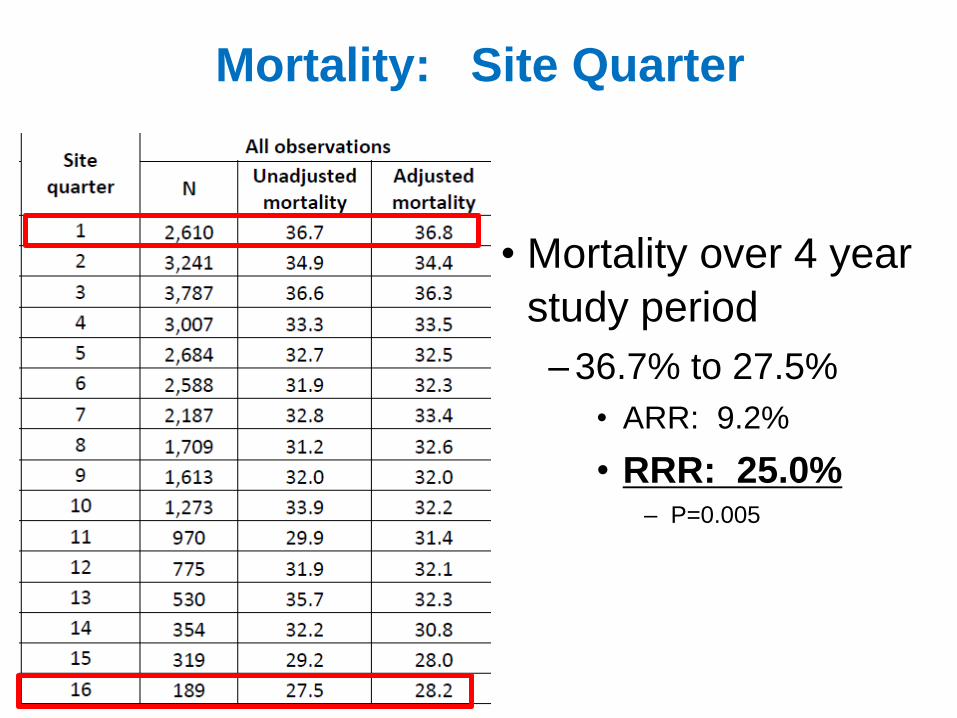
Mortality: Site Quarter
• Mortality over 4 year
study period
–36.7% to 27.5%
• ARR: 9.2%
• RRR: 25.0% – P=0.005
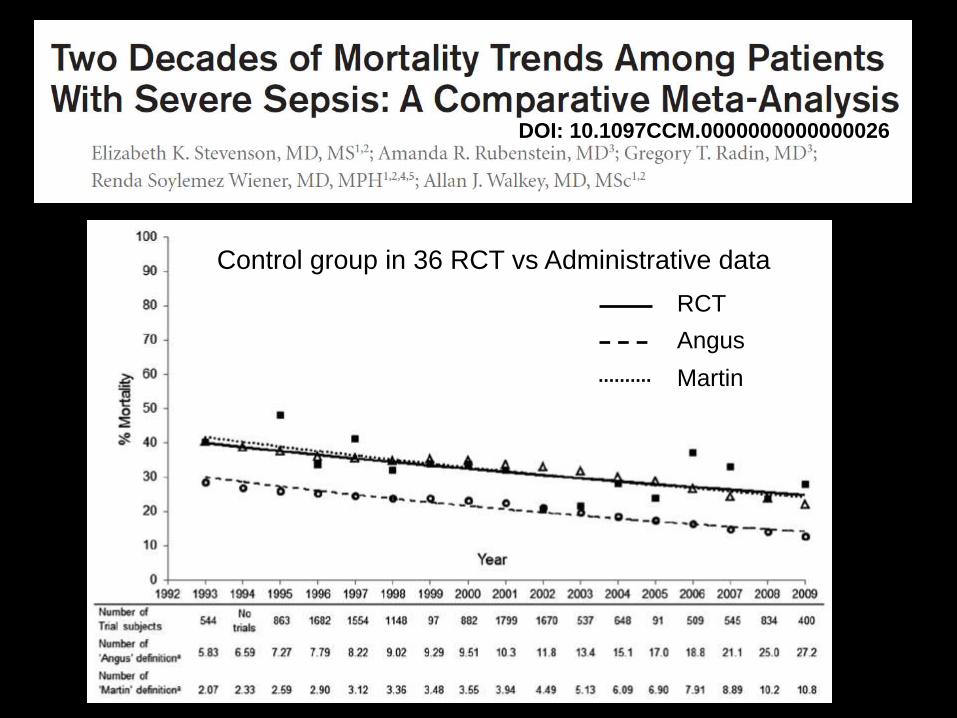
DOI: 10.1097CCM.0000000000000026
Control group in 36 RCT vs Administrative data
RCT
Angus
Martin
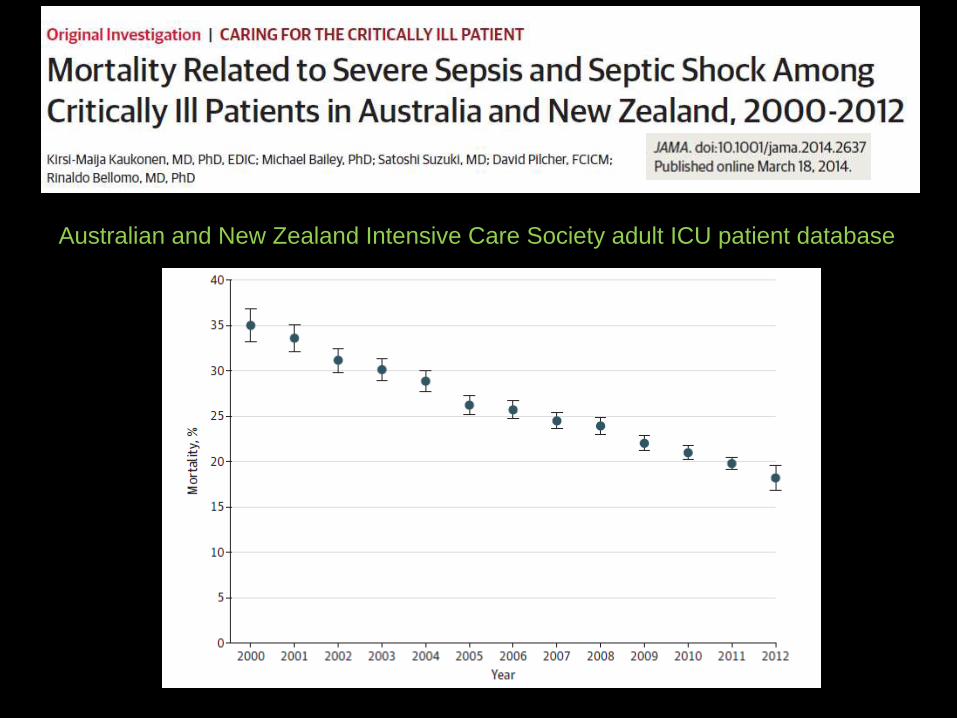
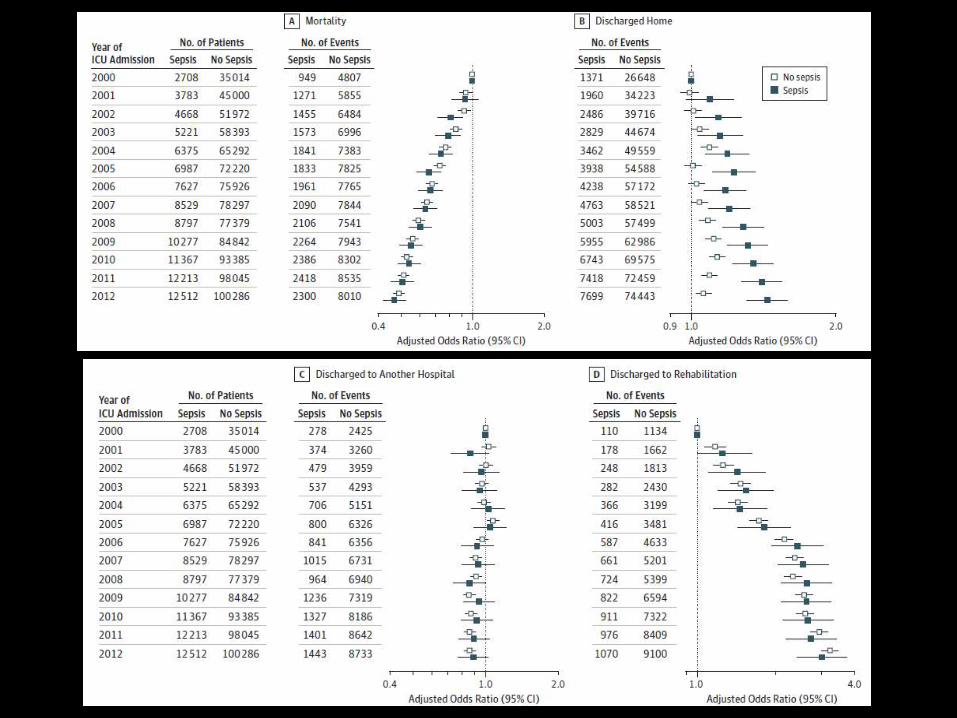
Australian and New Zealand Intensive Care Society adult ICU patient database
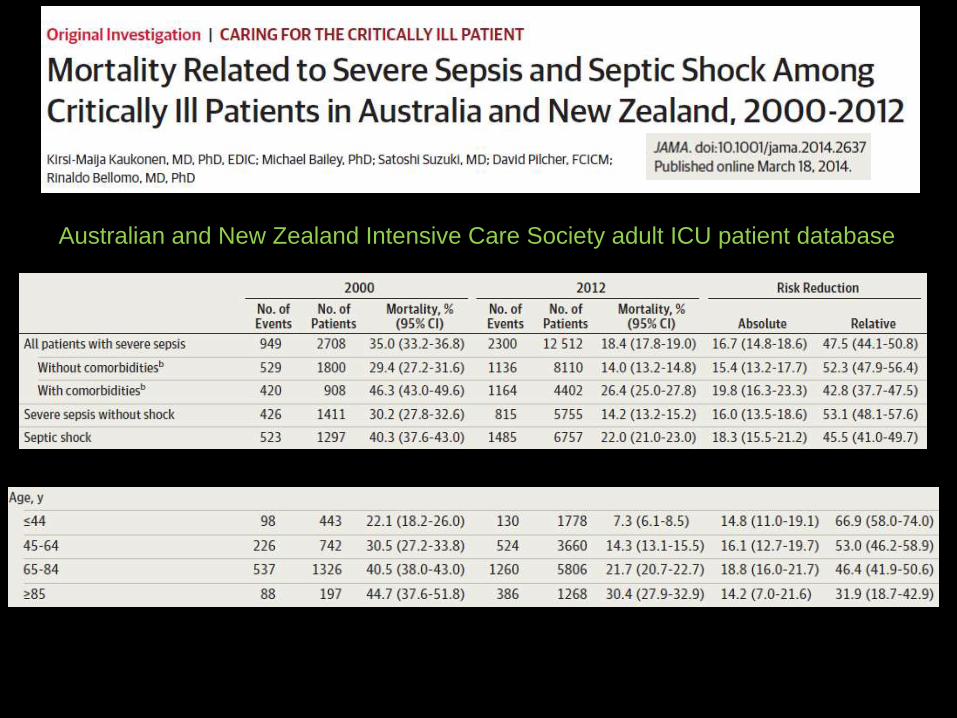
Australian and New Zealand Intensive Care Society adult ICU patient database
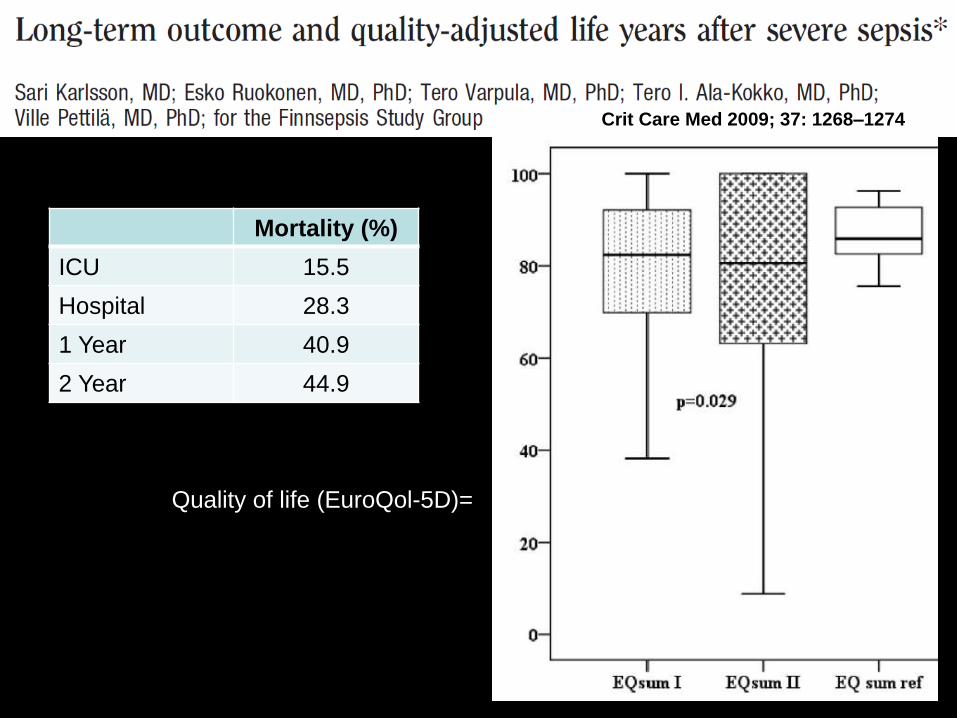
Crit Care Med 2009; 37: 1268–1274
Mortality (%)
ICU 15.5
Hospital 28.3
1 Year 40.9
2 Year 44.9
Quality of life (EuroQol-5D)=
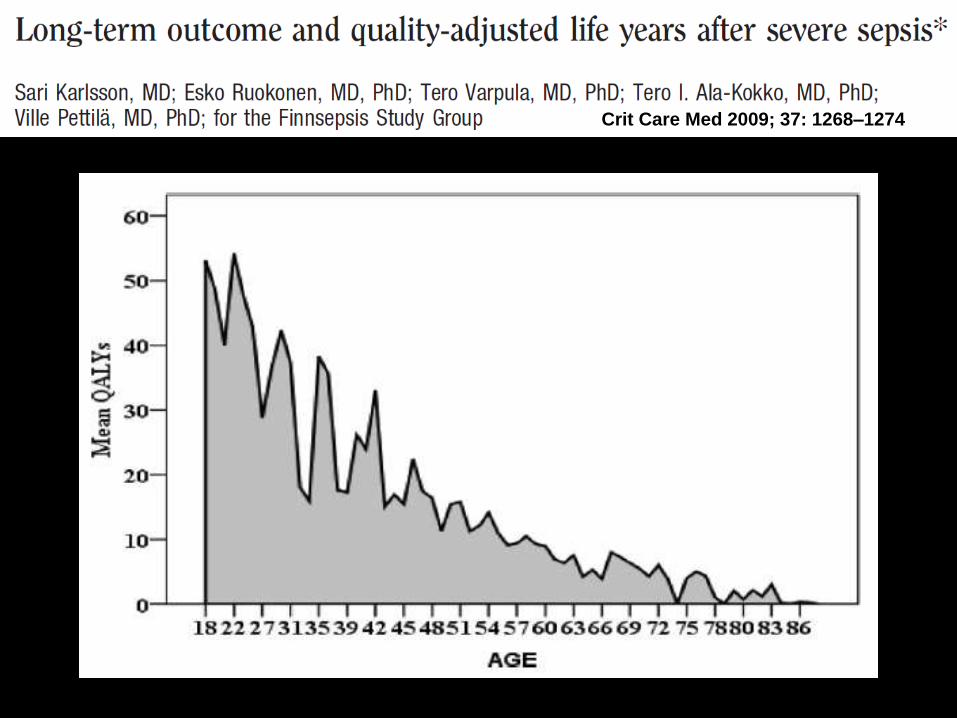
Crit Care Med 2009; 37: 1268–1274
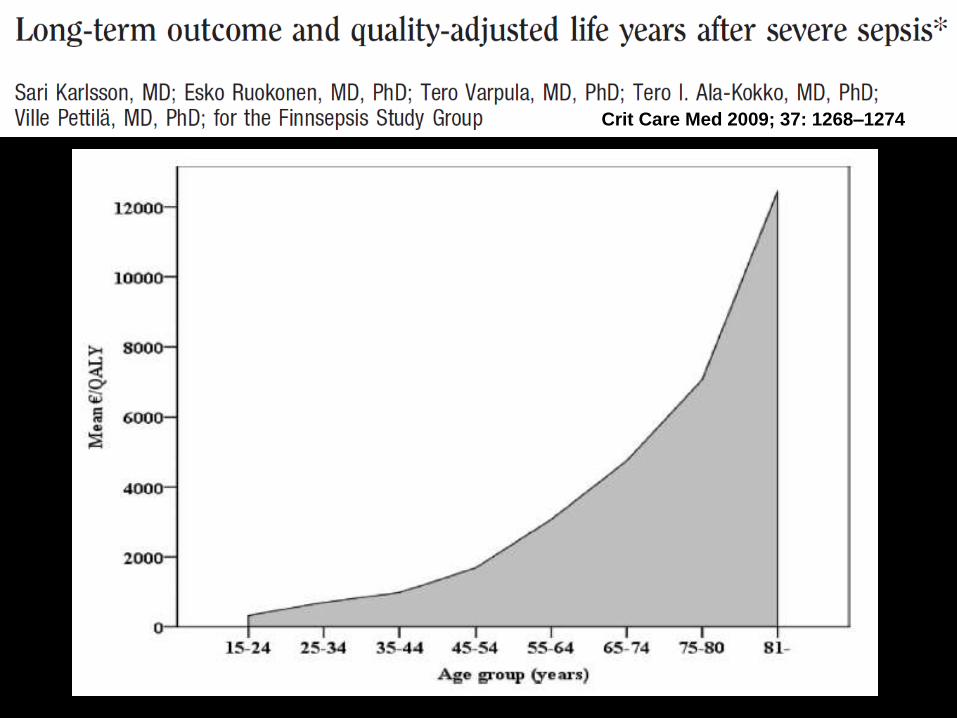
Crit Care Med 2009; 37: 1268–1274
Pillars of Sepsis Treatment
ABX Source Control EGDT
Lactate Radiology
YOUR speed is LIFE!
EDUSEPSIS es una organización independiente de profesionales que
atienden al paciente crítico, tanto adulto como pediátrico, cuyo objetivo es reducir la
mortalidad de la sepsis grave y el shock séptico mediante la evaluación de la
eficacia y eficiencia de los tratamientos y la transferencia del conocimiento científico.
Acciones
• Intervenciones de Transferencia del Conocimiento en Sepsis. – Adultos
– Pediatría
• Evaluaciones de la efectividad de los tratamientos de la sepsis. – Nacional
– Internacional: SSC
• Evaluaciones de costes y Coste-Efectividad.
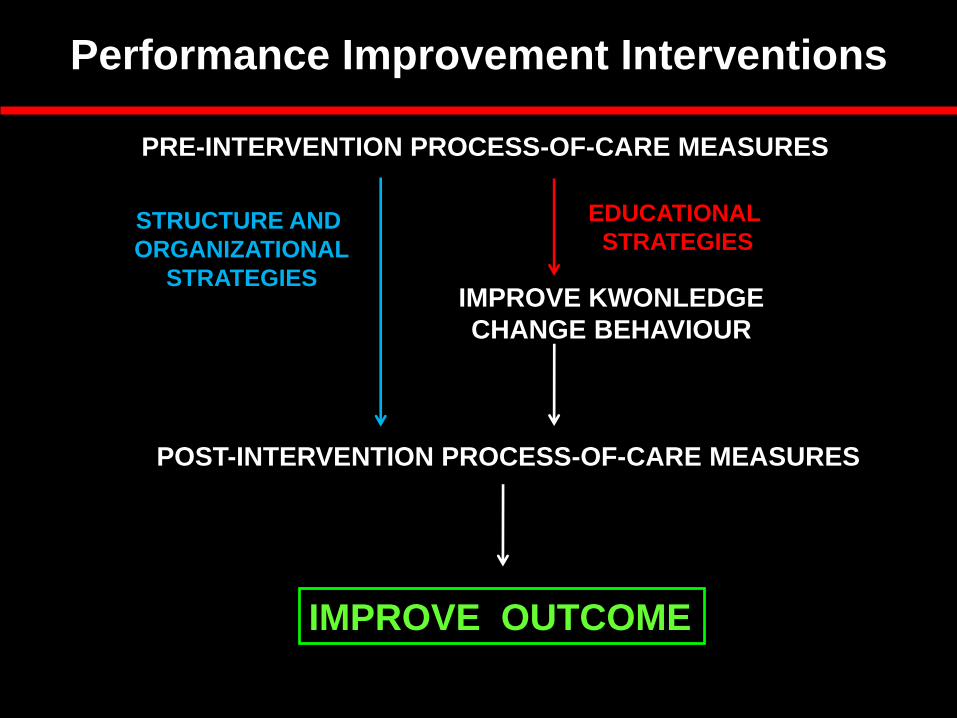
PRE-INTERVENTION PROCESS-OF-CARE MEASURES
POST-INTERVENTION PROCESS-OF-CARE MEASURES
IMPROVE KWONLEDGE
CHANGE BEHAVIOUR
IMPROVE OUTCOME
EDUCATIONAL
STRATEGIES STRUCTURE AND
ORGANIZATIONAL
STRATEGIES
Performance Improvement Interventions
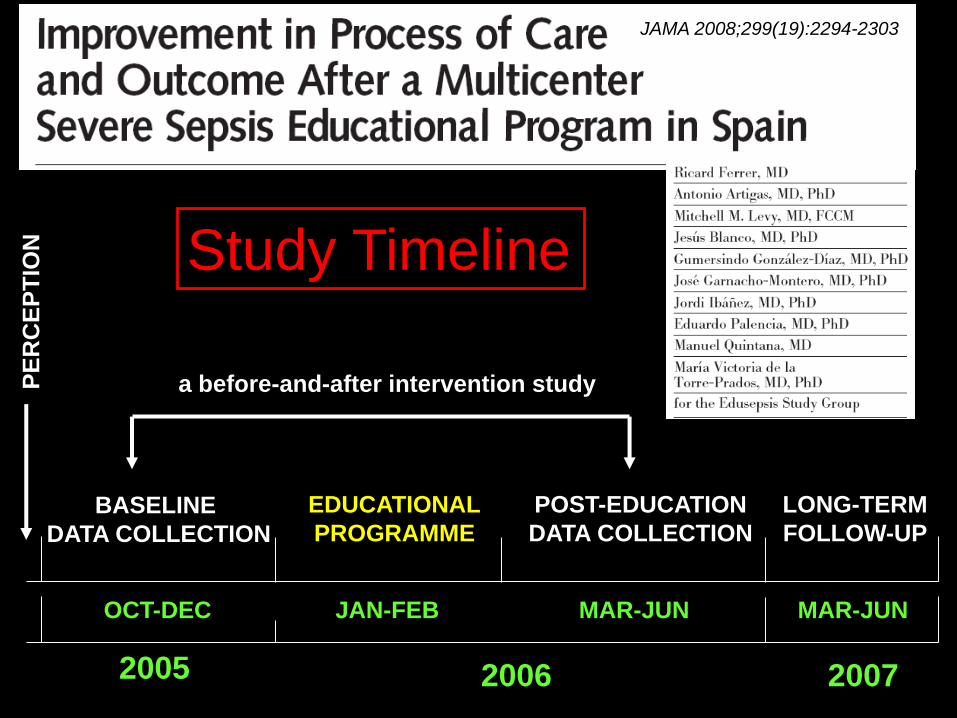
EDUCATIONAL
PROGRAMME
POST-EDUCATION
DATA COLLECTION
OCT-DEC JAN-FEB MAR-JUN
2005 2006
BASELINE
DATA COLLECTION
a before-and-after intervention study
2007
LONG-TERM
FOLLOW-UP
MAR-JUN
JAMA 2008;299(19):2294-2303
Study Timeline
PE
RC
EP
TIO
N
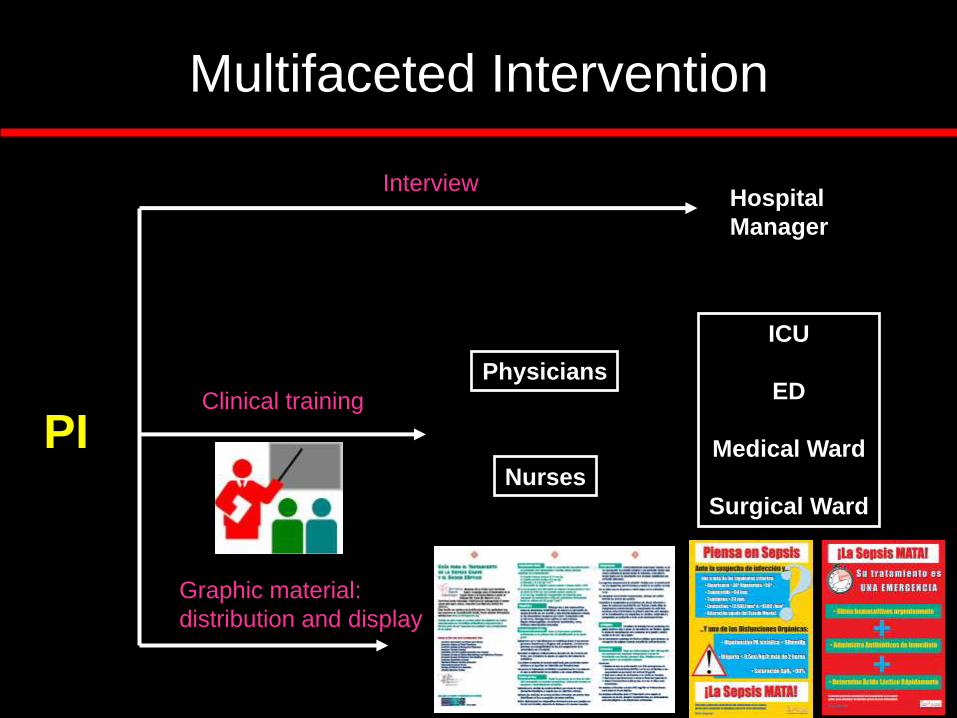
Multifaceted Intervention
PI
Hospital
Manager
Interview
Physicians
Nurses
ICU
ED
Medical Ward
Surgical Ward
Graphic material:
distribution and display
Clinical training
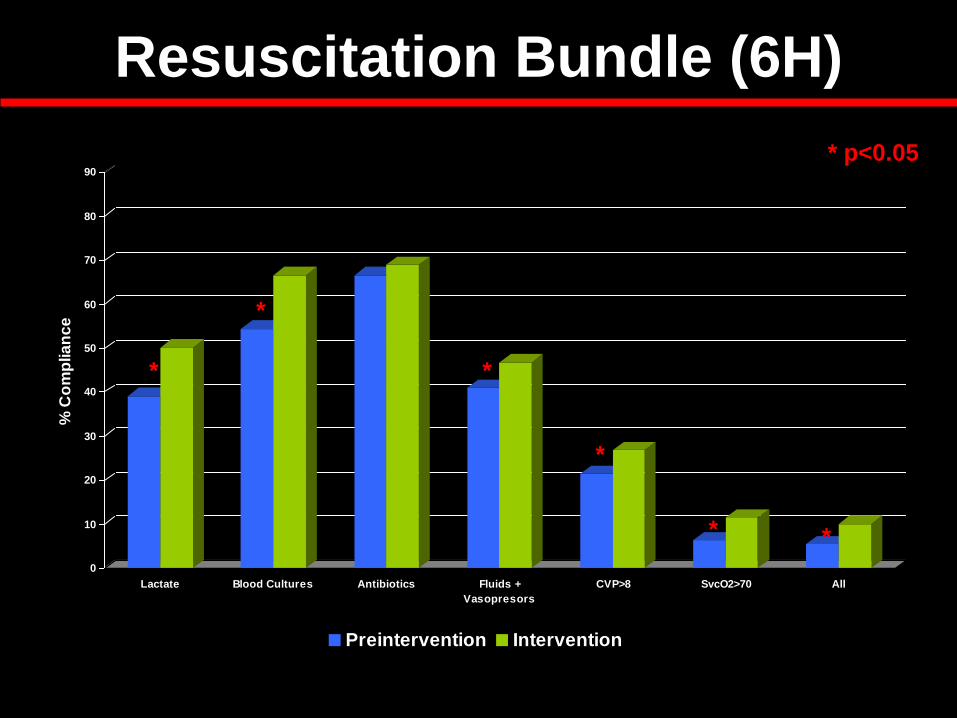
Resuscitation Bundle (6H)
0
10
20
30
40
50
60
70
80
90
% C
om
plia
nc
e
Lactate Blood Cultures Antibiotics Fluids +
Vasopresors
CVP>8 SvcO2>70 All
Preintervention Intervention
* p<0.05
*
*
*
*
* *
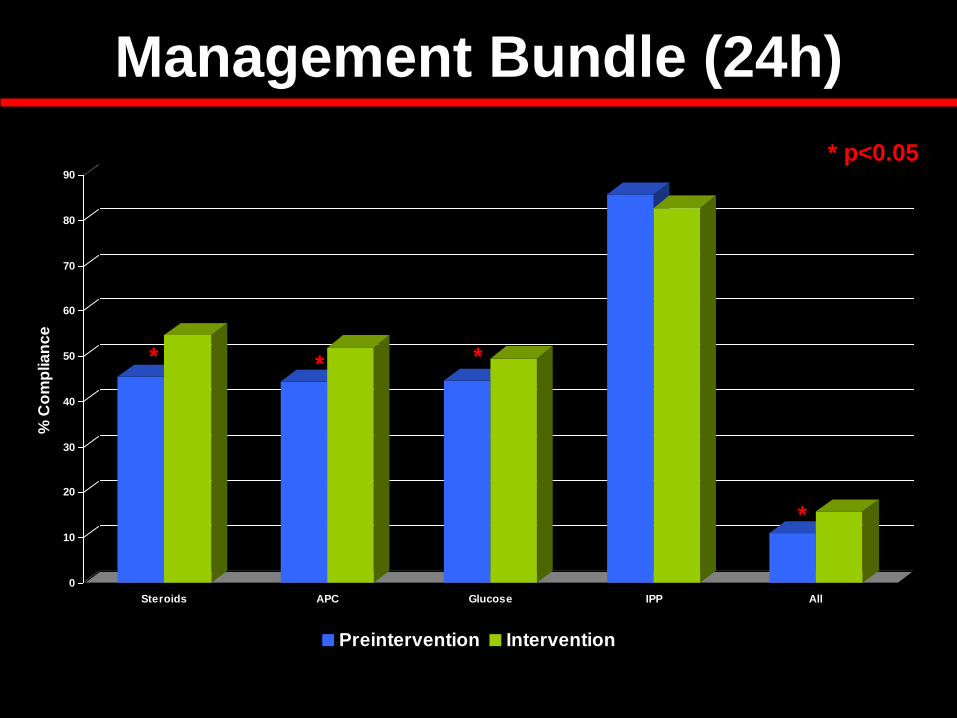
Management Bundle (24h)
0
10
20
30
40
50
60
70
80
90
% C
om
plia
nc
e
Steroids APC Glucose IPP All
Preintervention Intervention
* p<0.05
* * *
*
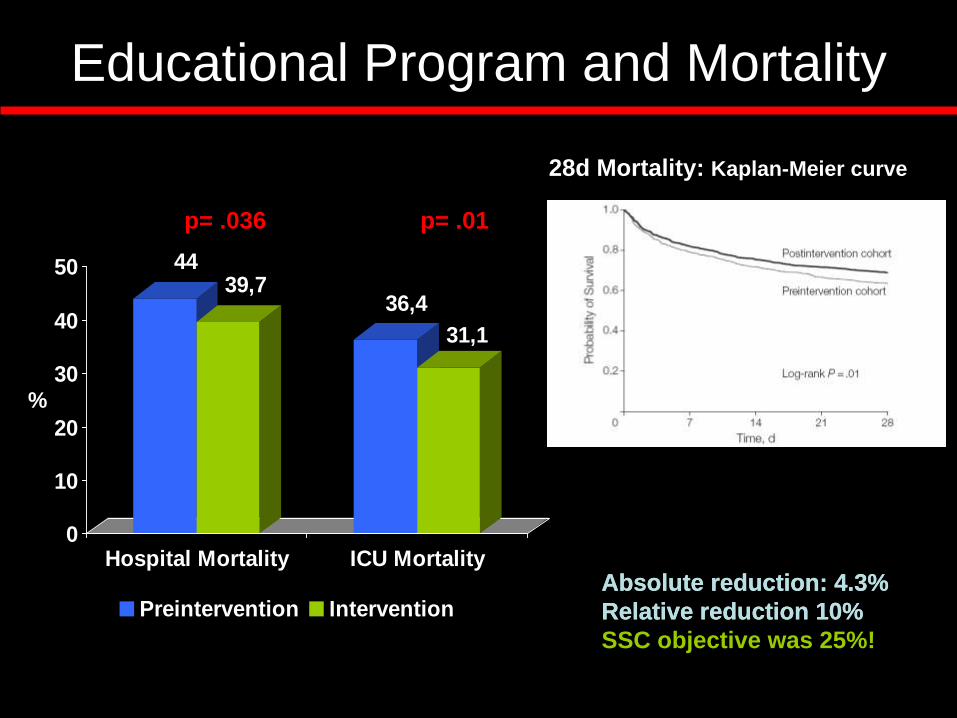
Educational Program and Mortality
4439,7
36,4
31,1
0
10
20
30
40
50
%
Hospital Mortality ICU Mortality
Preintervention Intervention
p= .036 p= .01
Absolute reduction: 4.3%
Relative reduction 10%
28d Mortality: Kaplan-Meier curve
Absolute reduction: 4.3%
Relative reduction 10%
SSC objective was 25%!
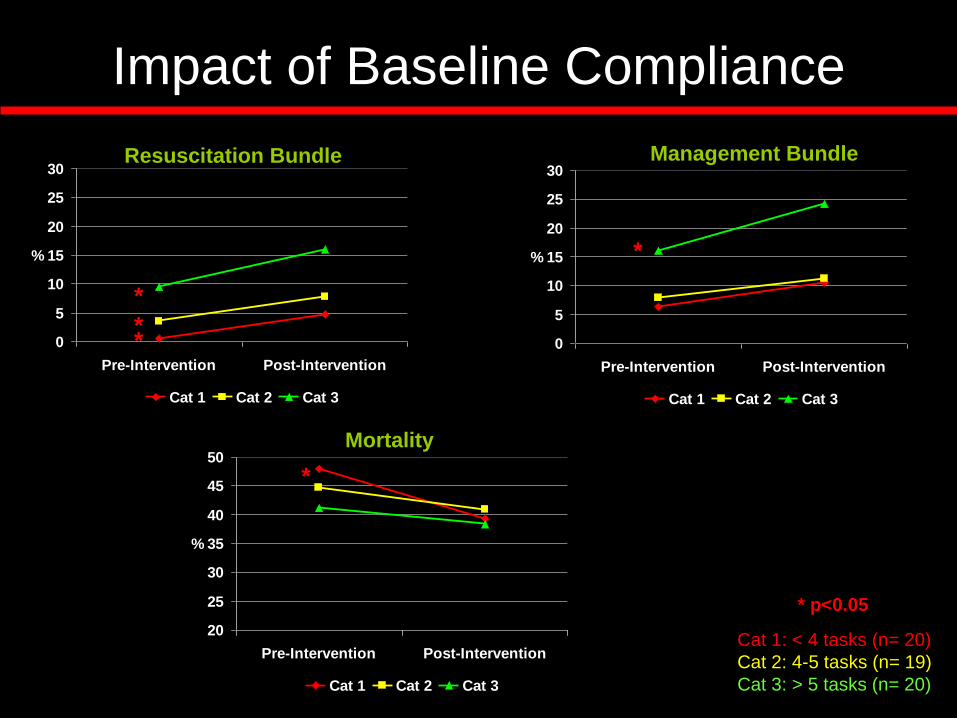
Impact of Baseline Compliance
0
5
10
15
20
25
30
Pre-Intervention Post-Intervention
%
Cat 1 Cat 2 Cat 3
0
5
10
15
20
25
30
Pre-Intervention Post-Intervention
%
Cat 1 Cat 2 Cat 3
20
25
30
35
40
45
50
Pre-Intervention Post-Intervention
%
Cat 1 Cat 2 Cat 3
Resuscitation Bundle Management Bundle
Mortality
* p<0.05
*
* *
*
*
Cat 1: < 4 tasks (n= 20)
Cat 2: 4-5 tasks (n= 19)
Cat 3: > 5 tasks (n= 20)
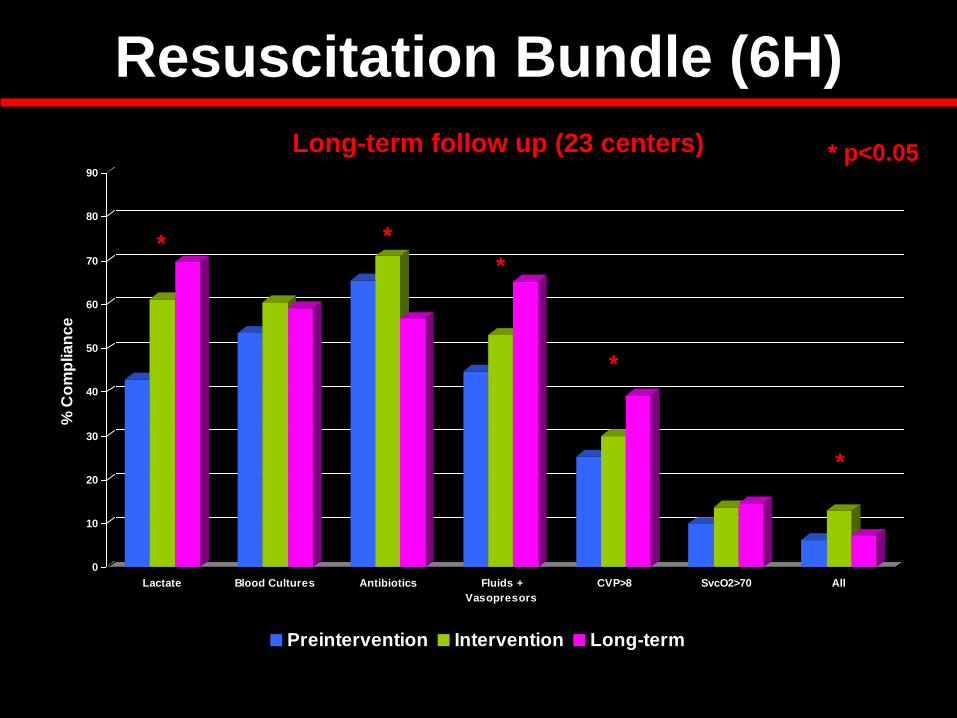
Resuscitation Bundle (6H)
0
10
20
30
40
50
60
70
80
90
% C
om
plia
nc
e
Lactate Blood Cultures Antibiotics Fluids +
Vasopresors
CVP>8 SvcO2>70 All
Preintervention Intervention Long-term
Long-term follow up (23 centers) * p<0.05
* *
*
*
*
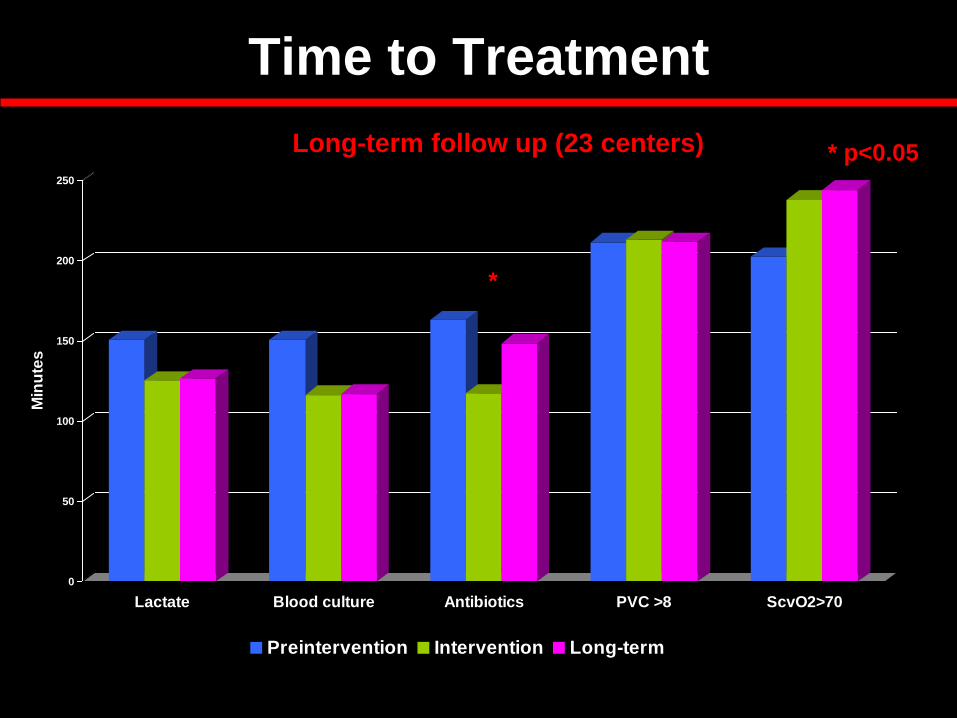
Time to Treatment
0
50
100
150
200
250
Min
ute
s
Lactate Blood culture Antibiotics PVC >8 ScvO2>70
Preintervention Intervention Long-term
* p<0.05
*
Long-term follow up (23 centers)
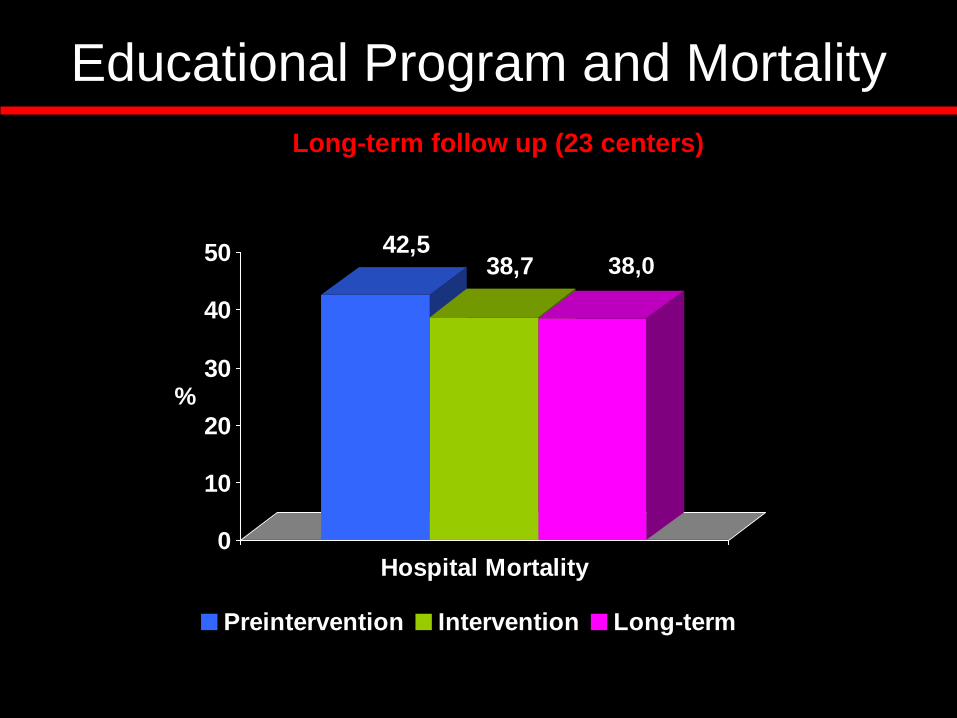
Educational Program and Mortality
42,538,7
0
10
20
30
40
50
%
Hospital Mortality
Preintervention Intervention Long-term
38,0
Long-term follow up (23 centers)
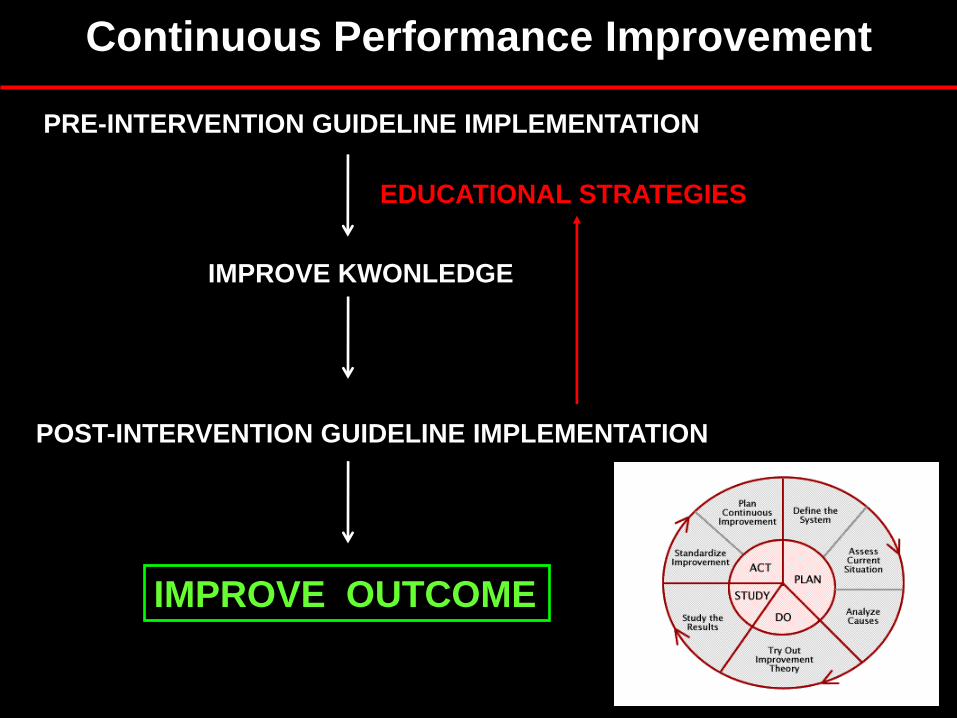
PRE-INTERVENTION GUIDELINE IMPLEMENTATION
POST-INTERVENTION GUIDELINE IMPLEMENTATION
IMPROVE KWONLEDGE
IMPROVE OUTCOME
EDUCATIONAL STRATEGIES
Continuous Performance Improvement
ABISS Edusepsis Study Antibiotic Intervention in Severe Sepsis
Objectives
• Efficacy:
– Reduce time to empiric antibiotic in severe sepsis.
– Increase appropriateness of antibiotic treatment
– Reduce hospital mortality.
• Safety:
– Increase antibiotic deescalation.
By a multifaceted quality-improvement intervention in patients with severe sepsis/septic shock admitted to the Spanish ICUs.
Multifaceted Intervention
• Audit and Feed-back.
• Educational meetings: PP presentation.
• Interactive Sepsis simulation on-line.
• Posters and pocket material about initial TTM.
• Support for antibiotic prescription.
• Remainders by mail and SMS to all staff assisting to educational meetings.
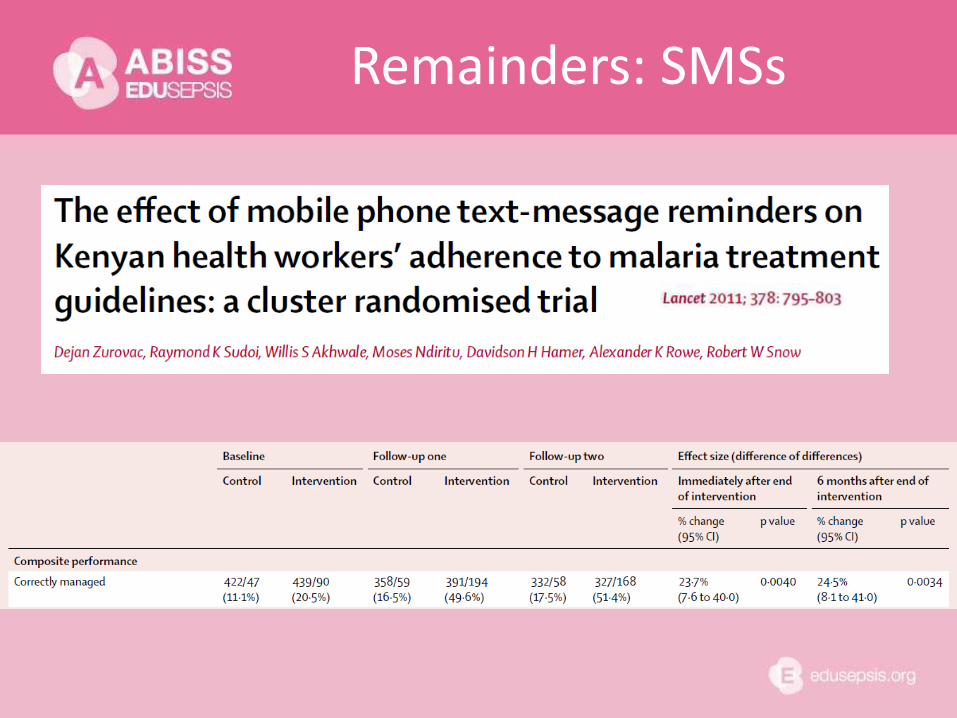
Remainders: SMSs
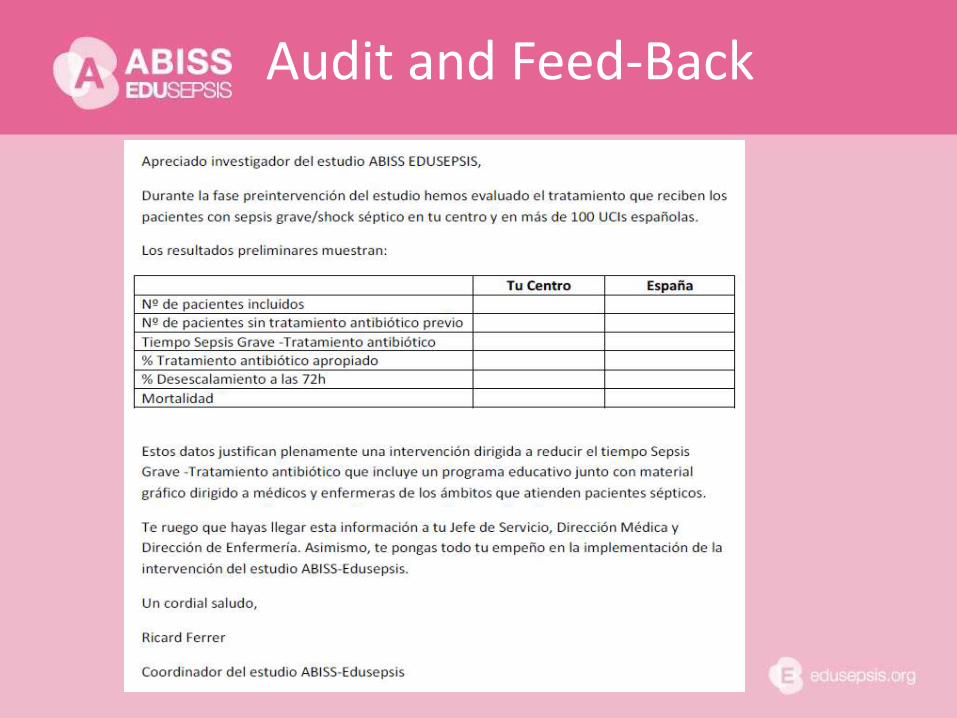
Audit and Feed-Back
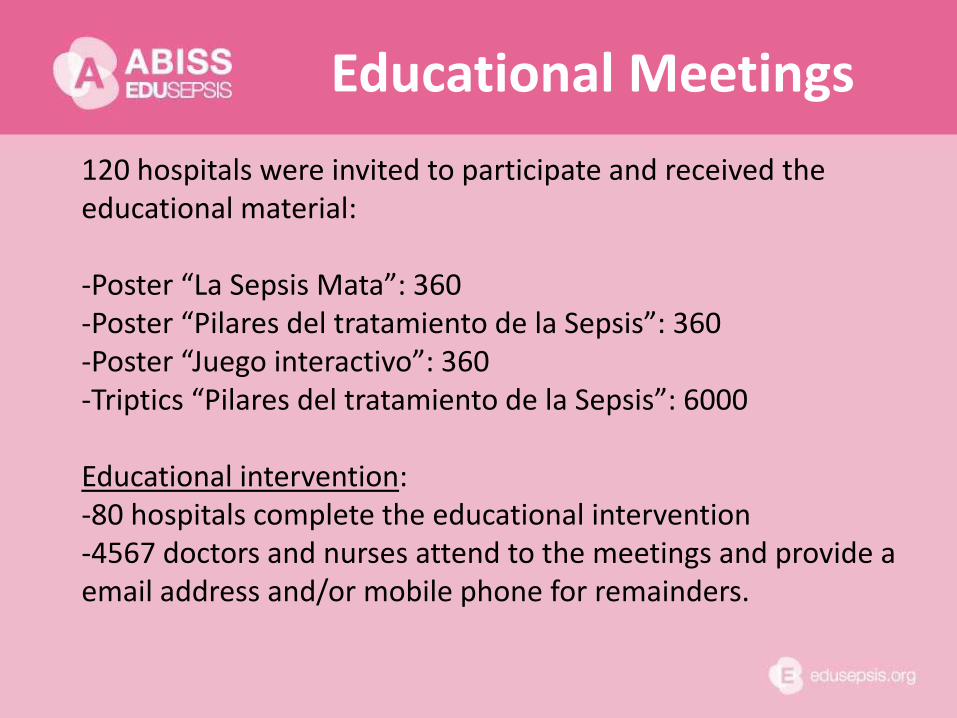
120 hospitals were invited to participate and received the educational material: -Poster “La Sepsis Mata”: 360 -Poster “Pilares del tratamiento de la Sepsis”: 360 -Poster “Juego interactivo”: 360 -Triptics “Pilares del tratamiento de la Sepsis”: 6000 Educational intervention: -80 hospitals complete the educational intervention -4567 doctors and nurses attend to the meetings and provide a email address and/or mobile phone for remainders.
Educational Meetings
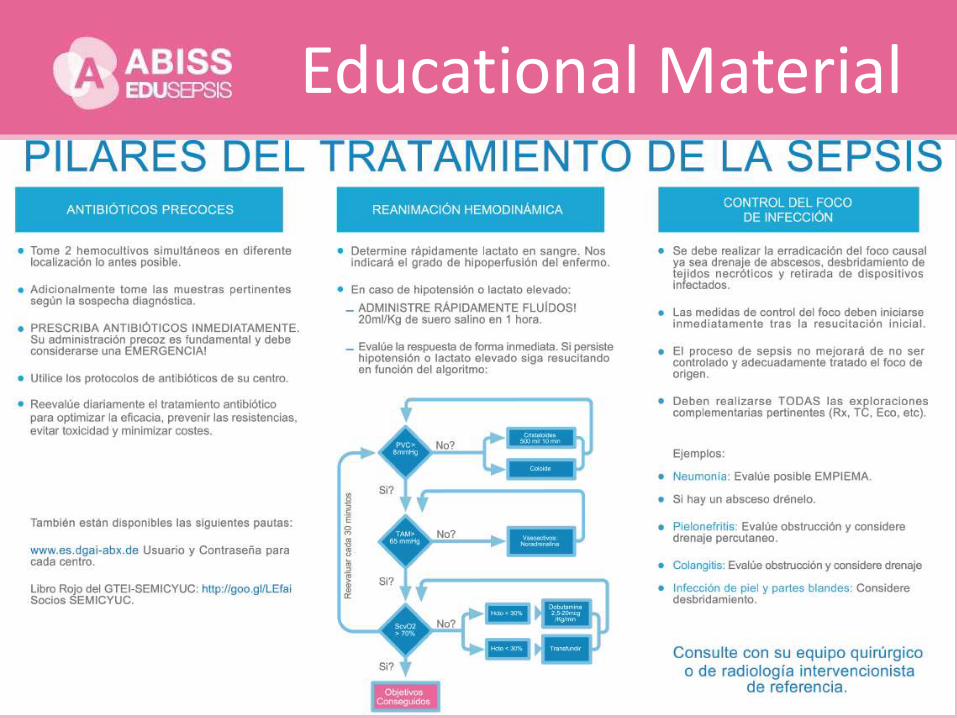
Educational Material
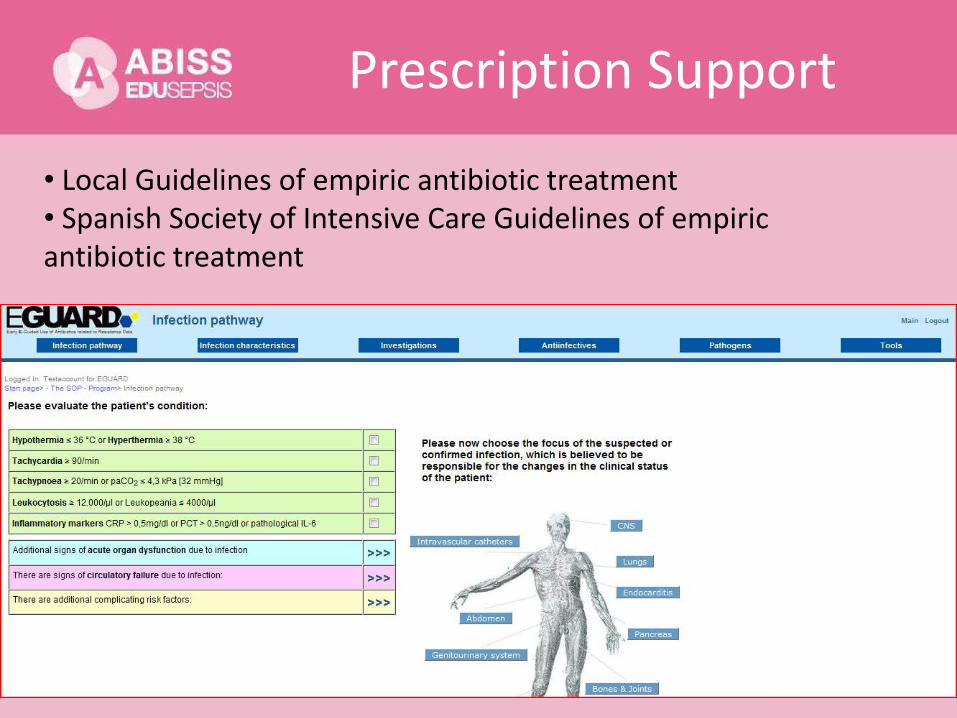
Prescription Support
• Local Guidelines of empiric antibiotic treatment • Spanish Society of Intensive Care Guidelines of empiric antibiotic treatment

Gamification
Remainder. SMSs
• En sepsis la administración del antibiótico adecuado es una emergencia.Consulta tu guia local de tto antibiotico empirico.TU VELOCIDAD ES VIDA.
• Los pilares del tratamiento de la sepsis son:antibióticoterapia, control del foco y resucitación hemodinámica.¡COMPLETALOS RAPIDAMENTE!
• Tardamos 3 horas en administrar antibiótico empírico en sepsis con mortalidad 33%. Administrado en 1h la mortalidad sería inferior!.
• Antes del tto antibiótico, recuerda tomar hemocultivos + cultivos adicionales según foco de sepsis, después podrás ajustar tu tto empírico!.
Results
• 72 hospitals in Spain.
• 2576 patients: PRE 1,325, POST: 1,251
• Age 64.1 ± 15.1 years, 54.1% male.
• CHARLSON 2.7 ± 2.2
• Septic Shock 67.6%, 32.4% severe sepsis.
• Bacteriemia: 33%
• APACHE-II 22 ± 8.
• SOFA 9 ± 3
• PCT 25 ± 35
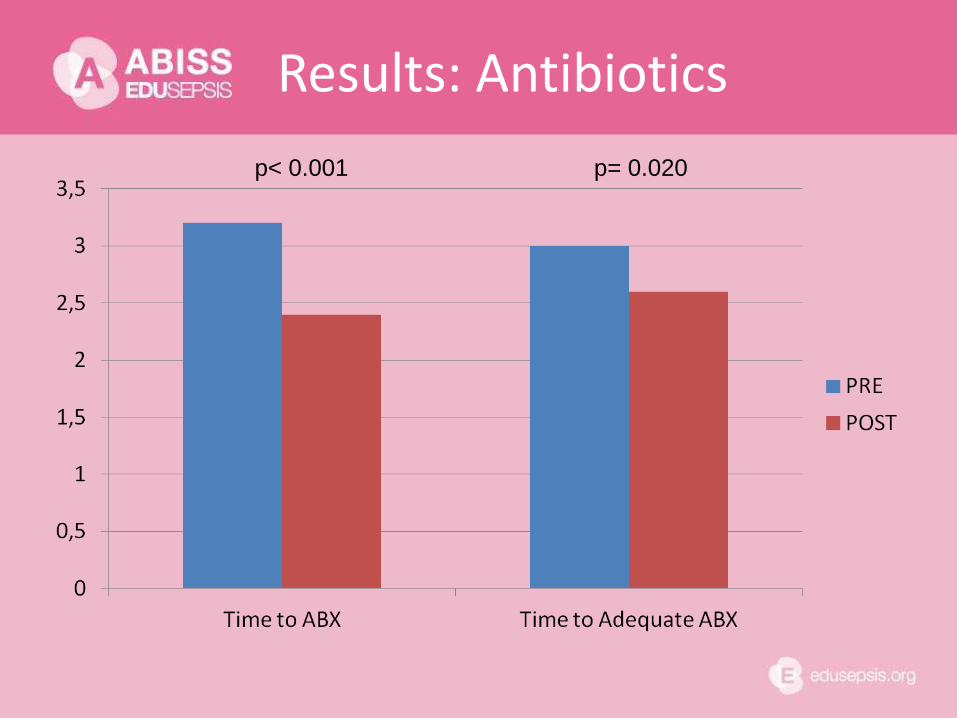
Results: Antibiotics
p< 0.001 p= 0.020

Results
p= 0.002 p= 0.001

Results
p= 0.422 p= 0.182
ABISS Edusepsis
Pediatric
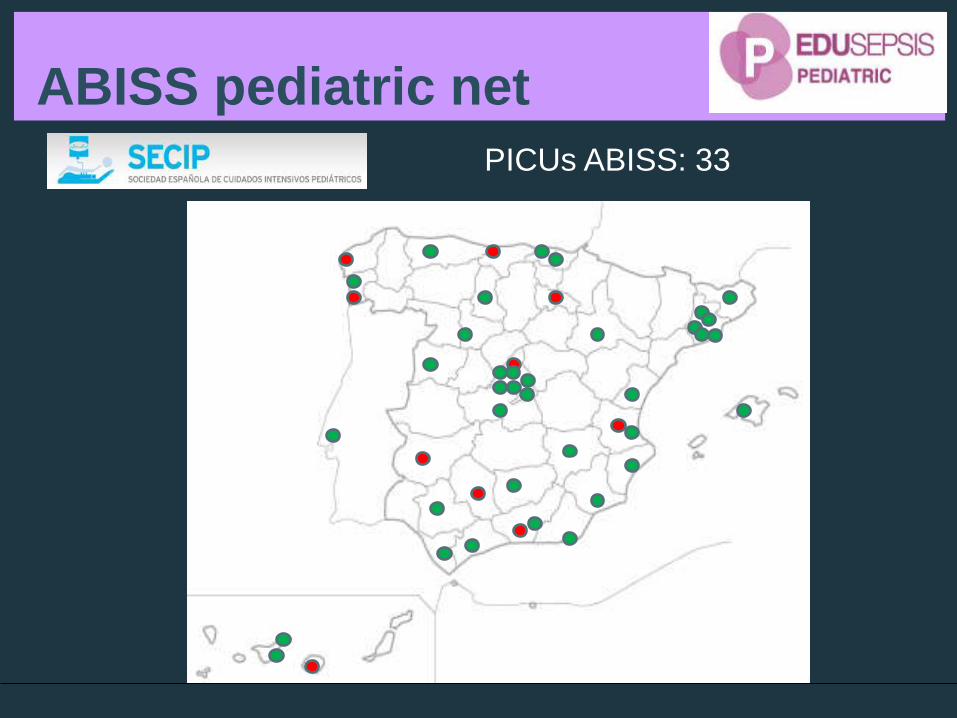
ABISS pediatric net
PICUs ABISS: 33
ABISS pediatric
ABISS PICUs characteristics:
• Total: 380 PICU beds
• Total admissions/month: 1460
• 100% of PICU with residents
• 94% public
• 83.3% medical and surgical, 25% pediatrics-
neonatal
• Protocols for sepsis management 100%
• Use of biomarkers: PCR 100%, PCT 64%
• Hemofiltration: 50%; ECMO: 20%
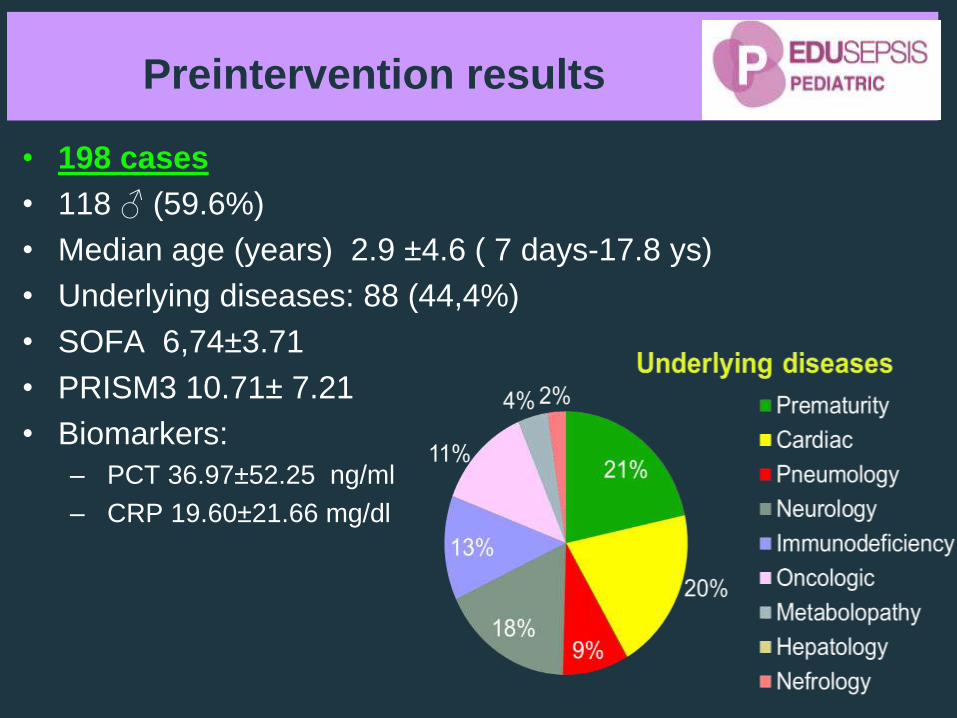
Preintervention results
• 198 cases
• 118 ♂ (59.6%)
• Median age (years) 2.9 ±4.6 ( 7 days-17.8 ys)
• Underlying diseases: 88 (44,4%)
• SOFA 6,74±3.71
• PRISM3 10.71± 7.21
• Biomarkers:
– PCT 36.97±52.25 ng/ml
– CRP 19.60±21.66 mg/dl
Preintervention results
• Global Mortality 15.6%
–Mortality Septic shock 26.2%
• Days of mechanical ventilation: 13.6±42.6
• Days of inotropic support: 5.77± 8.43
• PICU length of stay (days): 12.02±35.03
• Hospital length of stay (days): 26±45.09
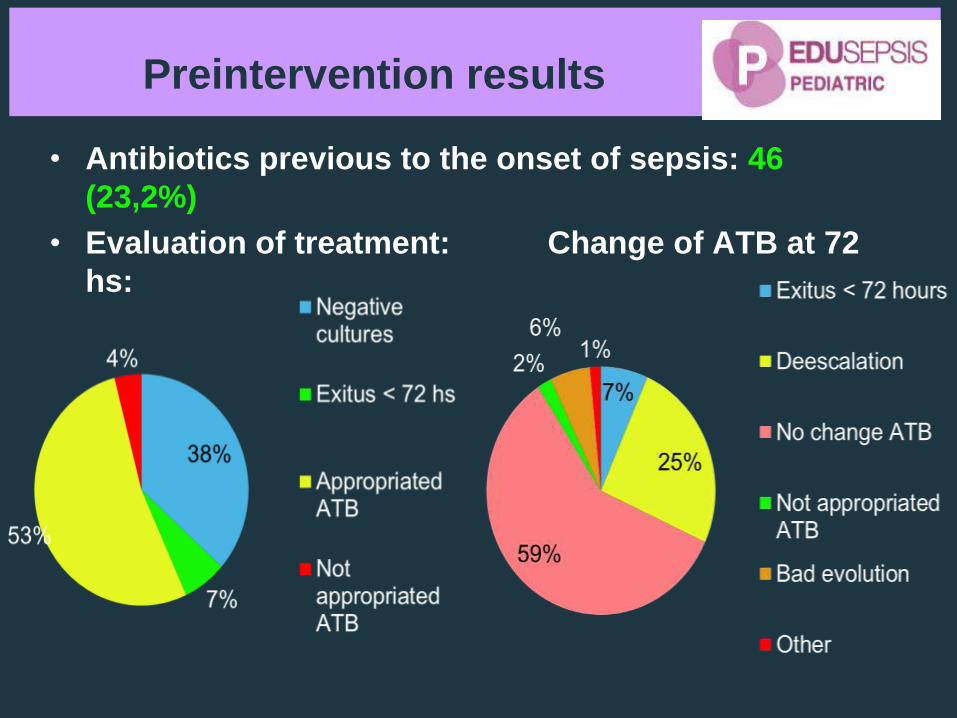
Preintervention results
• Antibiotics previous to the onset of sepsis: 46
(23,2%)
• Evaluation of treatment: Change of ATB at 72
hs:

Objective: To analyze the impact on hospital
mortality of severe sepsis treatments
included in the SSC guidelines in a
prospective multicenter observational
study (n= 2,796 adult patients with
severe sepsis in 77 Spanish ICUs).
Method: The effectiveness of each sepsis
treatment was estimated by using PS.
AJRCCM 2009;180:861–866.

TREATMENTS and MORTALITY
• Adjust for possible confounders:
–Clinical risks factors for mortality
–Other treatments and therapeutic
goals
–Propensity Score
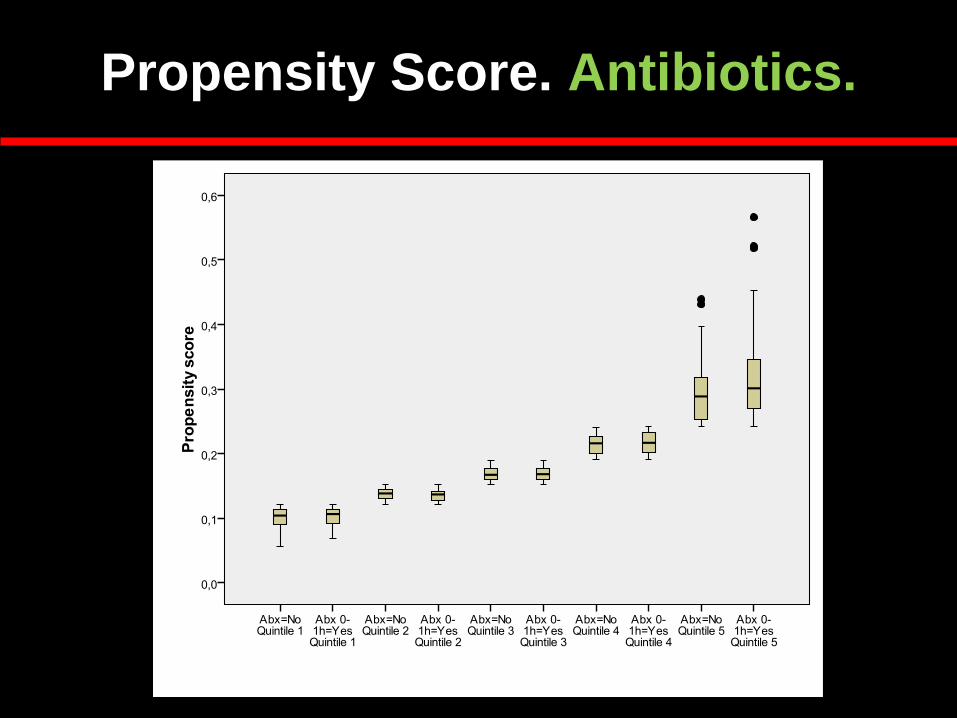
Propensity Score. Antibiotics.
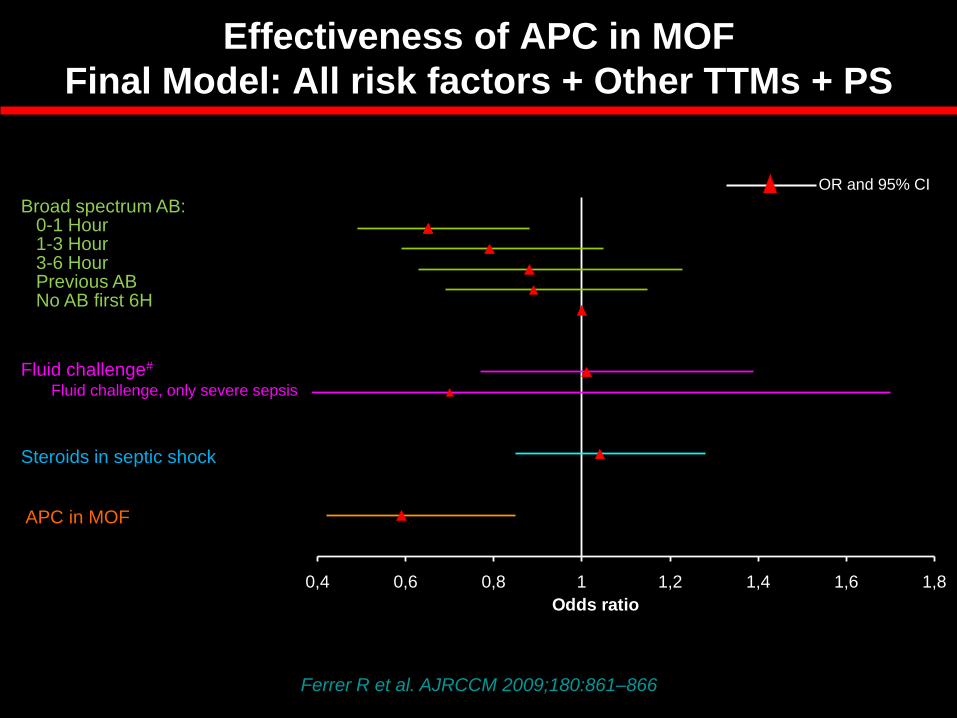
0,4 0,6 0,8 1 1,2 1,4 1,6 1,8
Odds ratio
OR and 95% CI
Broad spectrum AB:
Fluid challenge#
0-1 Hour 1-3 Hour 3-6 Hour Previous AB No AB first 6H
Steroids in septic shock
APC in MOF
Fluid challenge, only severe sepsis
Ferrer R et al. AJRCCM 2009;180:861–866
Effectiveness of APC in MOF
Final Model: All risk factors + Other TTMs + PS
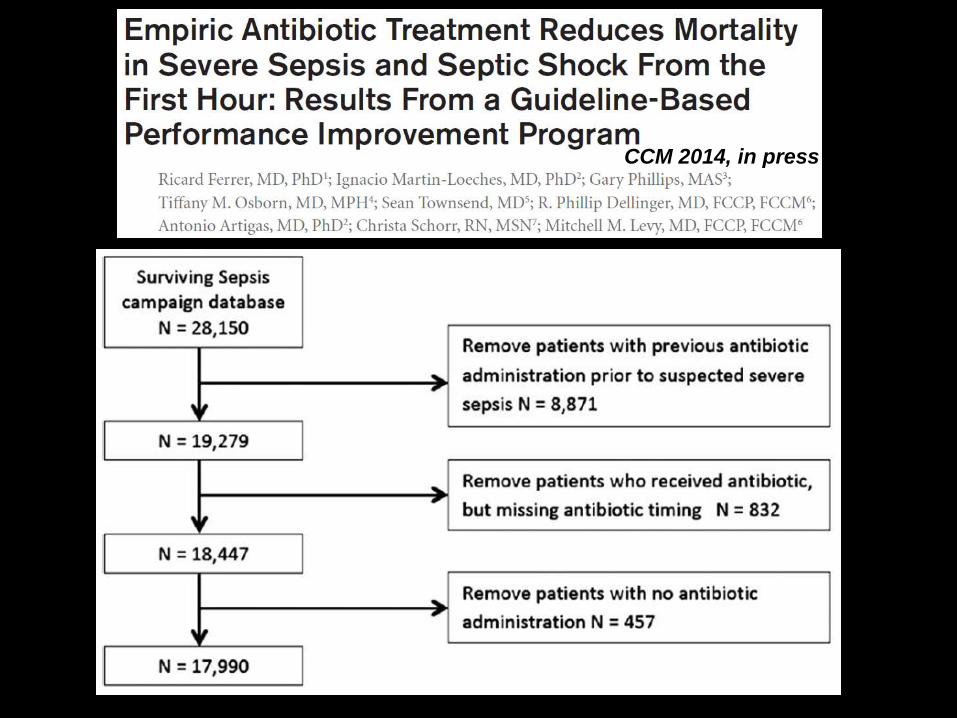
CCM 2014, in press
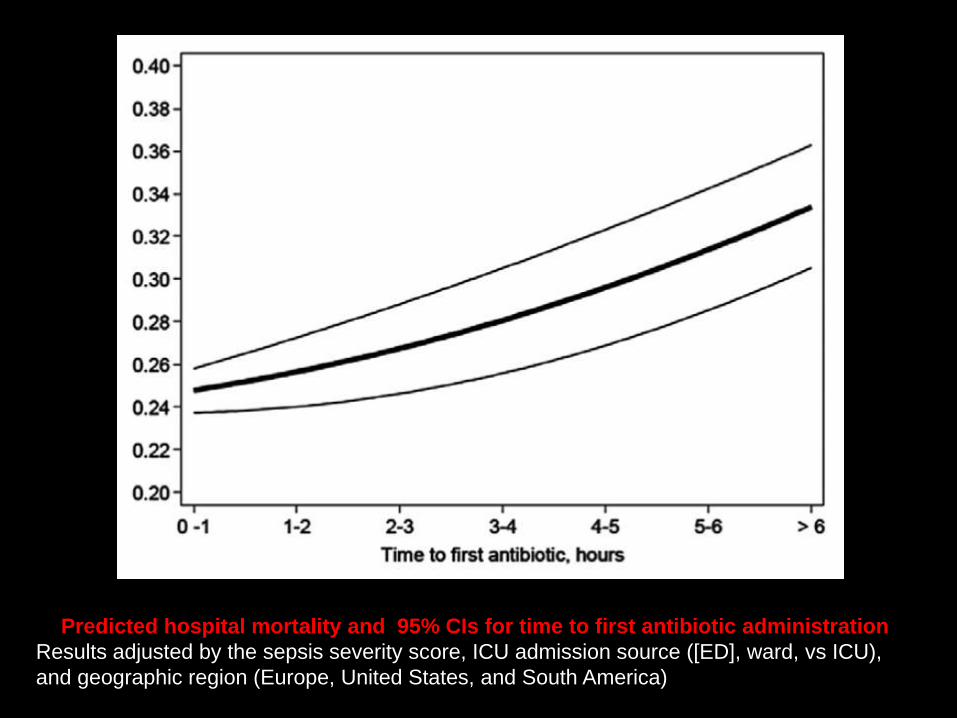
Predicted hospital mortality and 95% CIs for time to first antibiotic administration
Results adjusted by the sepsis severity score, ICU admission source ([ED], ward, vs ICU),
and geographic region (Europe, United States, and South America)
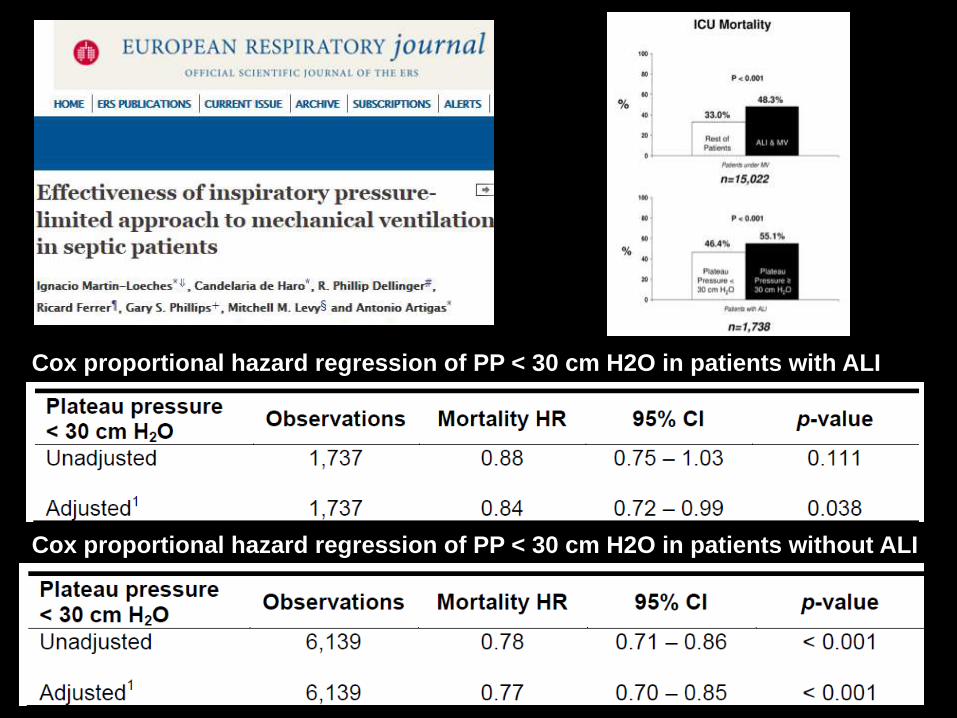
Cox proportional hazard regression of PP < 30 cm H2O in patients without ALI
Cox proportional hazard regression of PP < 30 cm H2O in patients with ALI

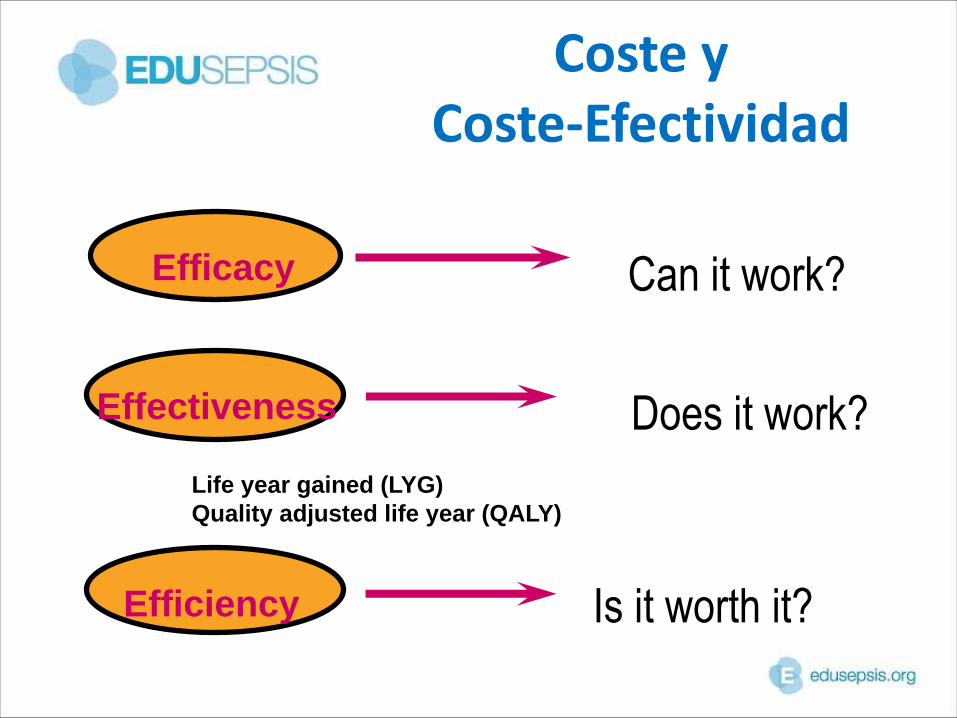
Coste y Coste-Efectividad
Can it work? Efficacy
Does it work? Effectiveness
Efficiency Is it worth it?
Life year gained (LYG)
Quality adjusted life year (QALY)
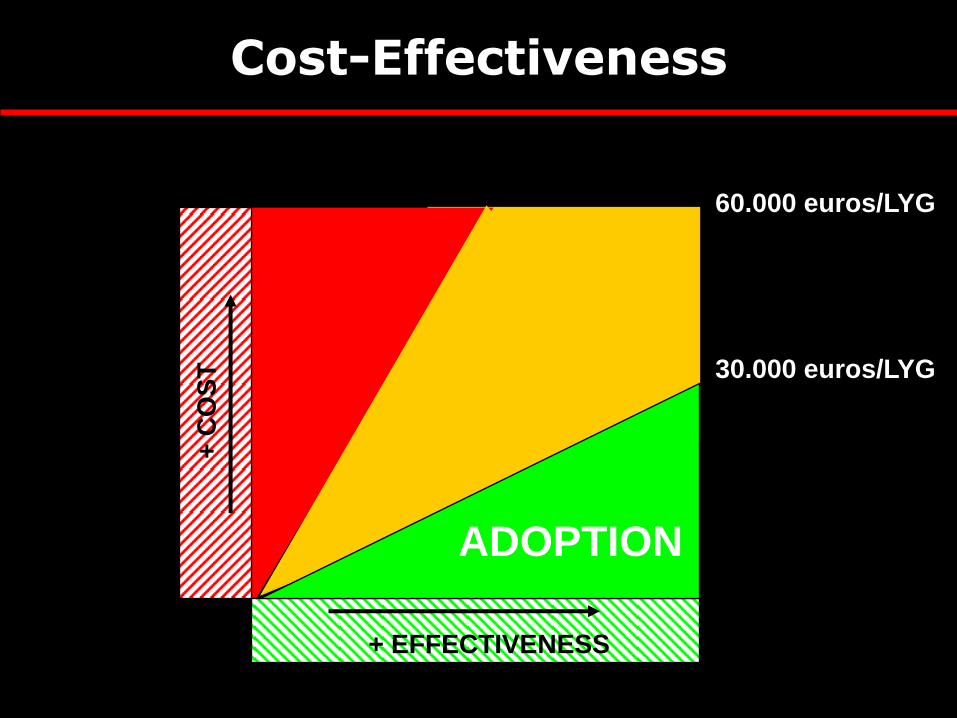
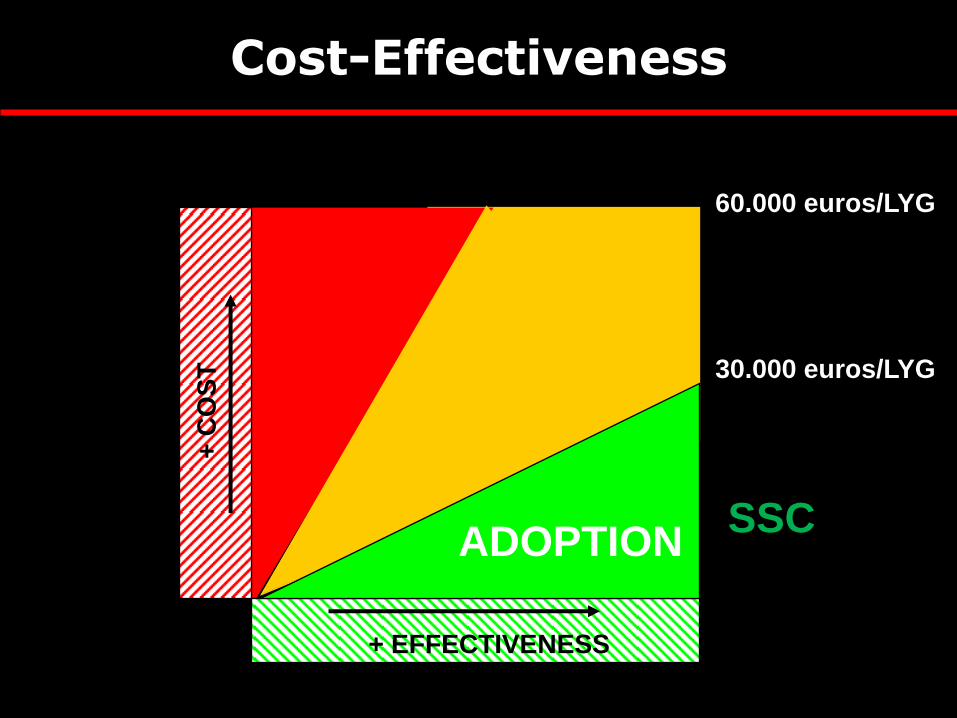
60.000 euros/LYG
30.000 euros/LYG
rechazo
?
adopción ADOPTION
+ EFFECTIVENESS
+ C
OS
T
Cost-Effectiveness
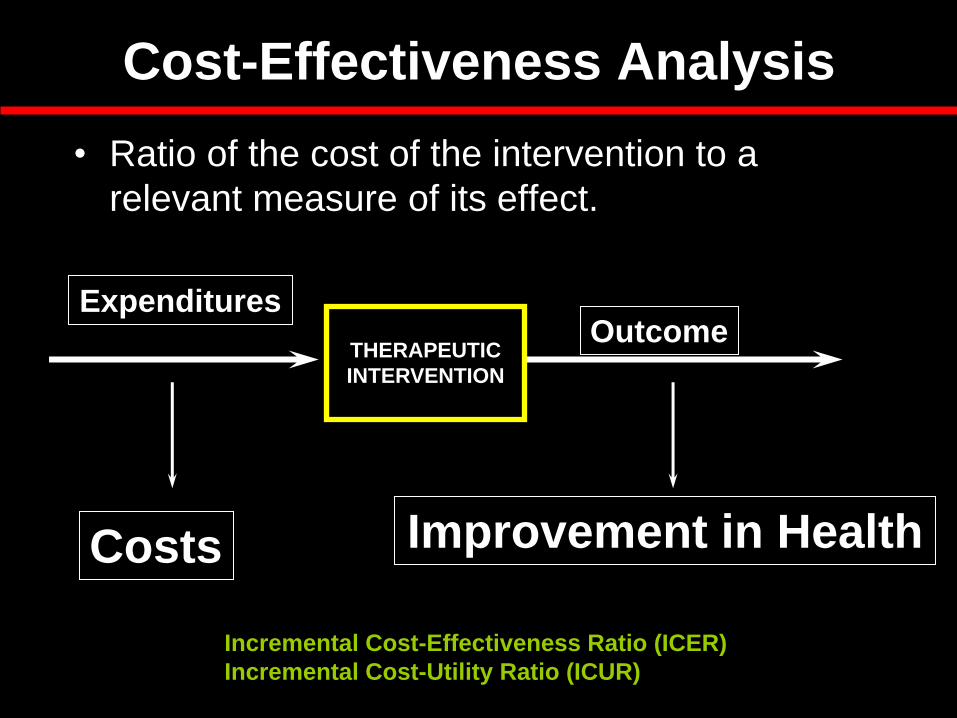
Cost-Effectiveness Analysis
• Ratio of the cost of the intervention to a
relevant measure of its effect.
THERAPEUTIC
INTERVENTION
Expenditures Outcome
Improvement in Health Costs
Incremental Cost-Effectiveness Ratio (ICER)
Incremental Cost-Utility Ratio (ICUR)
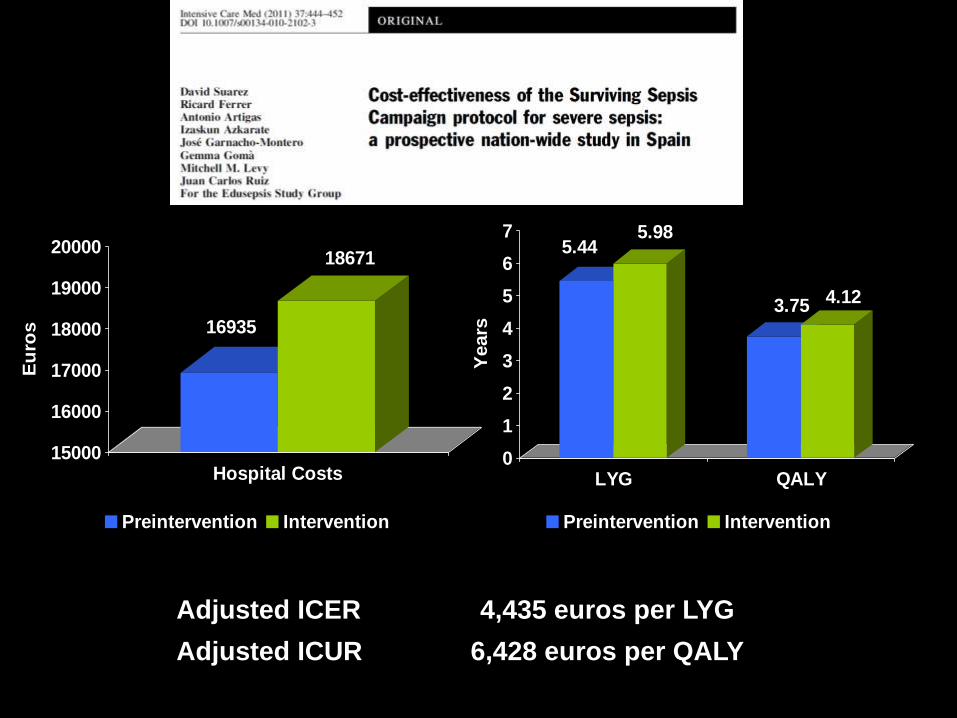
16935
18671
15000
16000
17000
18000
19000
20000
Eu
ros
Hospital Costs
Preintervention Intervention
5.445.98
3.75 4.12
0
1
2
3
4
5
6
7
Years
LYG QALY
Preintervention Intervention
Adjusted ICER 4,435 euros per LYG
Adjusted ICUR 6,428 euros per QALY
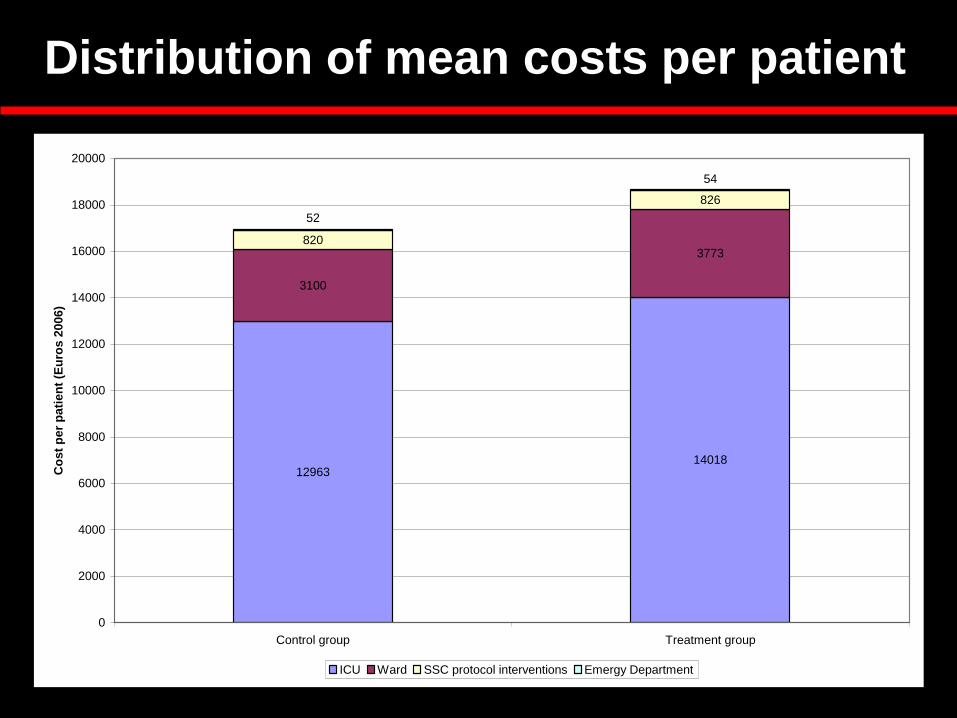
Distribution of mean costs per patient
1296314018
3100
3773820
826
54
52
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
Control group Treatment group
Co
st
per
pati
en
t (E
uro
s 2
006)
ICU Ward SSC protocol interventions Emergy Department
60.000 euros/LYG
30.000 euros/LYG
rechazo
?
adopción ADOPTION
+ EFFECTIVENESS
+ C
OS
T
SSC
Cost-Effectiveness
Conclusions
1. La sepsia greu continua teneint una elevada incidència i mortalitat. El reconeixement social encara és escàs.
2. La sepsia greu és una emergencia mèdica. Cal que rebi una atenció multidisciplinar, coordinada i precoç.
3. Pla Nacional de Sepsis. Indicadors de Qualitat.
4. Codi de Sepsis

Ricard Ferrer Intensive Care Department
Mutua Terrassa University Hospital Barcelona. SPAIN