¿cuándo estÁ uno demasiado enfermo? normativa para …exantema vírico de manos, pies y boca...
TRANSCRIPT

¿Cuándo ESTÁ UNO DEMASIADO ENFERMO? Normativa para los padres sobre las
enfermedades
Cuándo su hijo debe quedarse en casa y no ir a la guardería o la escuela
Existen tres motivos principales para que los niños enfermos se queden en casa:
1. Su hijo no se siente lo suficientemente bien para participar en las actividades habituales. Por ejemplo, está demasiado cansado, irritable o no para de llorar.
2. Su hijo necesita más cuidados de lo que los maestros y el personal pueden darle, y además cuidar a los demás niños.
3. La enfermedad está en esta lista y se recomienda que se quede en casa.
***Recuerde, la mejor manera para prevenir que una infección se propague es lavándose bien las manos.
Los niños que presentan los síntomas o las enfermedades siguientes deben quedarse en casa (no ir a la escuela):
Síntomas ¿El niño debe quedarse en casa?
Diarrea Heces sueltas o aguadas frecuentes comparadas con
las habituales del niño, que no son consecuencia de
una comida o medicamentos.
Sí – Si el niño se ve o actúa como que está enfermo;
si el niño tiene diarrea con fiebre y no actúa con normalidad;
si el niño tiene diarrea con vómito; O si el niño tiene diarrea que
sobresale del pañal o el inodoro.
Fiebre
con cambio en el comportamiento u otra enfermedad .
Fiebre de 100°F o superior en los bebés menores de 4
meses necesita atención médica inmediata.
Sí - si el niño también presenta una erupción cutánea, dolor de
garganta, vómito, diarrea, cambios de comportamiento, cuello rígido O
dificultad para respirar, etc.
Síntomas “parecidos a la gripe”
Fiebre superior a 100°F con tos o dolor de garganta.
Otros síntomas de la gripe pueden incluir cansancio,
dolores corporales, vómito y diarrea.
Sí – como mínimo por 24 horas después de que desaparezca la fiebre.
La fiebre debe desaparecer sin el uso de medicamentos para reducir
la fiebre (acetaminofén o ibuprofeno).
Tos Nota: los niños con asma pueden ir a la escuela con un
plan por escrito de cuidado para la salud, a fin de
permitir que la escuela les dé el medicamento y el
tratamiento.
Sí – si la tos es grave;
Sin controlar;
O su hijo tiene sibilancia, dificultad para respirar o respira rápido y es
necesaria la atención médica.
Síntomas respiratorios o de resfriado leves
Nariz tapada con mucosidad trasparente, estornudos,
tos leve.
No – puede asistir si es capaz de participar en las actividades escolares.
Debe quedarse en casa si los síntomas son graves. Esto incluye fiebre y si
el niño no actúa con normalidad y/o tiene problemas para respirar.
Erupción cutánea Sí – Erupción cutánea con fiebre. Llame a su médico.
Deben evaluarlo un médico si presenta alguna erupción cutánea que se
propague rápidamente, si tiene heridas abiertas que supuran y/o no se
sanan.
No—Erupción cutánea sin fiebre. Normalmente no es necesario
quedarse en casa si presenta una erupción cutánea corporal son
fiebre o cambios en el comportamiento. Puede llamar al médico
para pedir consejo.
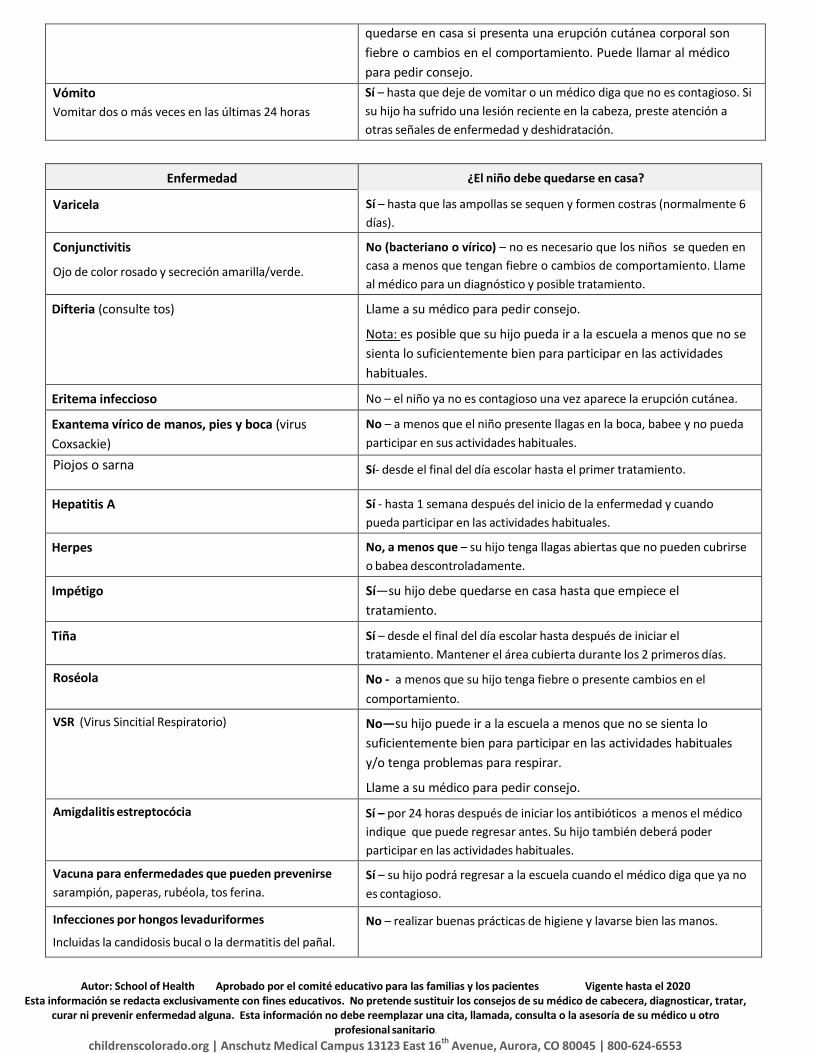
Vómito
Vomitar dos o más veces en las últimas 24 horas
Sí – hasta que deje de vomitar o un médico diga que no es contagioso. Si
su hijo ha sufrido una lesión reciente en la cabeza, preste atención a
otras señales de enfermedad y deshidratación.
Enfermedad ¿El niño debe quedarse en casa?
Varicela Sí – hasta que las ampollas se sequen y formen costras (normalmente 6
días).
Conjunctivitis
Ojo de color rosado y secreción amarilla/verde.
No (bacteriano o vírico) – no es necesario que los niños se queden en
casa a menos que tengan fiebre o cambios de comportamiento. Llame
al médico para un diagnóstico y posible tratamiento.
Difteria (consulte tos) Llame a su médico para pedir consejo.
Nota: es posible que su hijo pueda ir a la escuela a menos que no se
sienta lo suficientemente bien para participar en las actividades
habituales.
Eritema infeccioso No – el niño ya no es contagioso una vez aparece la erupción cutánea.
Exantema vírico de manos, pies y boca (virus
Coxsackie)
No – a menos que el niño presente llagas en la boca, babee y no pueda
participar en sus actividades habituales.
Piojos o sarna Sí- desde el final del día escolar hasta el primer tratamiento.
Hepatitis A Sí - hasta 1 semana después del inicio de la enfermedad y cuando
pueda participar en las actividades habituales.
Herpes No, a menos que – su hijo tenga llagas abiertas que no pueden cubrirse
o babea descontroladamente.
Impétigo Sí—su hijo debe quedarse en casa hasta que empiece el
tratamiento.
Tiña Sí – desde el final del día escolar hasta después de iniciar el
tratamiento. Mantener el área cubierta durante los 2 primeros días.
Roséola No - a menos que su hijo tenga fiebre o presente cambios en el
comportamiento.
VSR (Virus Sincitial Respiratorio) No—su hijo puede ir a la escuela a menos que no se sienta lo
suficientemente bien para participar en las actividades habituales
y/o tenga problemas para respirar.
Llame a su médico para pedir consejo.
Amigdalitis estreptocócia Sí – por 24 horas después de iniciar los antibióticos a menos el médico
indique que puede regresar antes. Su hijo también deberá poder
participar en las actividades habituales.
Vacuna para enfermedades que pueden prevenirse
sarampión, paperas, rubéola, tos ferina.
Sí – su hijo podrá regresar a la escuela cuando el médico diga que ya no
es contagioso.
Infecciones por hongos levaduriformes
Incluidas la candidosis bucal o la dermatitis del pañal.
No – realizar buenas prácticas de higiene y lavarse bien las manos.
Autor: School of Health Aprobado por el comité educativo para las familias y los pacientes Vigente hasta el 2020 Esta información se redacta exclusivamente con fines educativos. No pretende sustituir los consejos de su médico de cabecera, diagnosticar, tratar,
curar ni prevenir enfermedad alguna. Esta información no debe reemplazar una cita, llamada, consulta o la asesoría de su médico u otro profesional sanitario.
childrenscolorado.org | Anschutz Medical Campus 13123 East 16th Avenue, Aurora, CO 80045 | 800-624-6553
Form #201 Colorado Kids with Diabetes Care and Prevention Collaborative August 2019
1
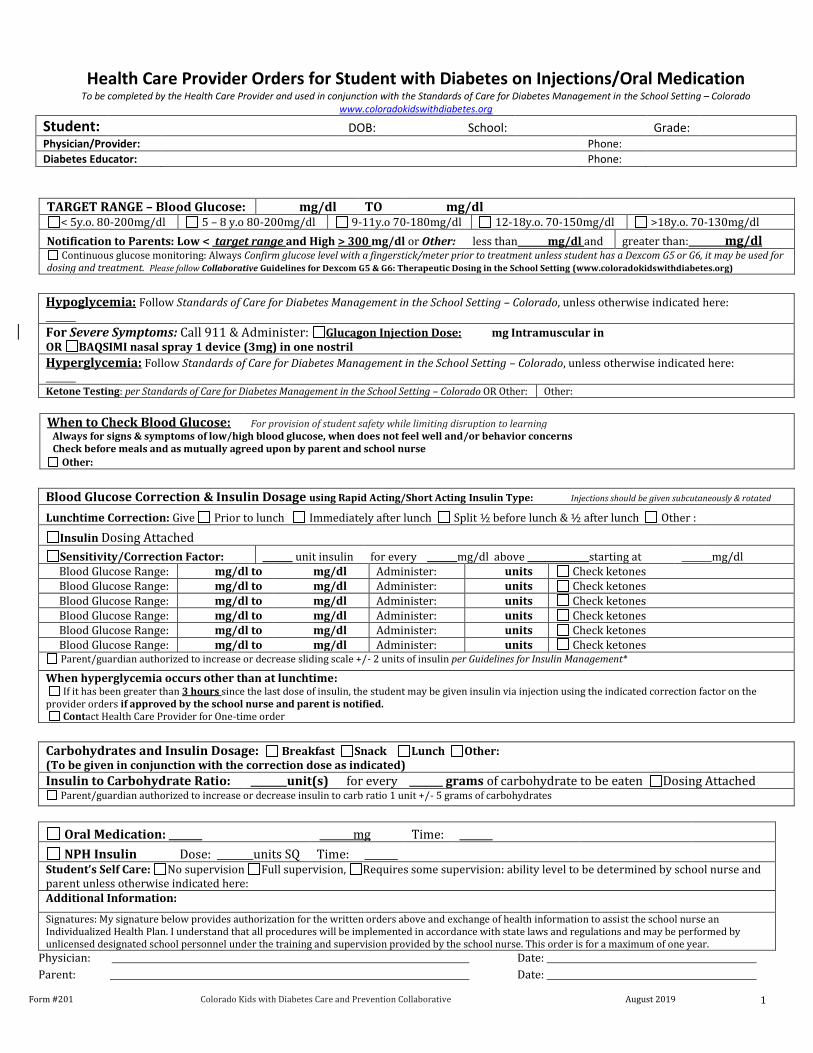
Health Care Provider Orders for Student with Diabetes on Injections/Oral Medication To be completed by the Health Care Provider and used in conjunction with the Standards of Care for Diabetes Management in the School Setting – Colorado
www.coloradokidswithdiabetes.org
Student: DOB: School: Grade: Physician/Provider: Phone:
Diabetes Educator: Phone:
TARGET RANGE – Blood Glucose: mg/dl TO mg/dl
< 5y.o. 80-200mg/dl 5 – 8 y.o 80-200mg/dl 9-11y.o 70-180mg/dl 12-18y.o. 70-150mg/dl >18y.o. 70-130mg/dl
Notification to Parents: Low < target range and High > 300 mg/dl or Other: less than mg/dl and greater than: mg/dl Continuous glucose monitoring: Always Confirm glucose level with a fingerstick/meter prior to treatment unless student has a Dexcom G5 or G6, it may be used for
dosing and treatment. Please follow Collaborative Guidelines for Dexcom G5 & G6: Therapeutic Dosing in the School Setting (www.coloradokidswithdiabetes.org)
Hypoglycemia: Follow Standards of Care for Diabetes Management in the School Setting – Colorado, unless otherwise indicated here:
For Severe Symptoms: Call 911 & Administer: Glucagon Injection Dose: mg Intramuscular in OR BAQSIMI nasal spray 1 device (3mg) in one nostril
Hyperglycemia: Follow Standards of Care for Diabetes Management in the School Setting – Colorado, unless otherwise indicated here: Ketone Testing: per Standards of Care for Diabetes Management in the School Setting – Colorado OR Other: Other:
When to Check Blood Glucose: For provision of student safety while limiting disruption to learning Always for signs & symptoms of low/high blood glucose, when does not feel well and/or behavior concerns Check before meals and as mutually agreed upon by parent and school nurse
Other:
Blood Glucose Correction & Insulin Dosage using Rapid Acting/Short Acting Insulin Type: Injections should be given subcutaneously & rotated
Lunchtime Correction: Give Prior to lunch Immediately after lunch Split ½ before lunch & ½ after lunch Other :
Insulin Dosing Attached
Sensitivity/Correction Factor: unit insulin for every mg/dl above starting at mg/dl Blood Glucose Range: mg/dl to mg/dl Administer: units Check ketones Blood Glucose Range: mg/dl to mg/dl Administer: units Check ketones Blood Glucose Range: mg/dl to mg/dl Administer: units Check ketones Blood Glucose Range: mg/dl to mg/dl Administer: units Check ketones Blood Glucose Range: mg/dl to mg/dl Administer: units Check ketones Blood Glucose Range: mg/dl to mg/dl Administer: units Check ketones
Parent/guardian authorized to increase or decrease sliding scale +/- 2 units of insulin per Guidelines for Insulin Management*
When hyperglycemia occurs other than at lunchtime: If it has been greater than 3 hours since the last dose of insulin, the student may be given insulin via injection using the indicated correction factor on the provider orders if approved by the school nurse and parent is notified. Contact Health Care Provider for One-time order
Carbohydrates and Insulin Dosage: Breakfast Snack Lunch Other: (To be given in conjunction with the correction dose as indicated) Insulin to Carbohydrate Ratio: unit(s) for every grams of carbohydrate to be eaten Dosing Attached
Parent/guardian authorized to increase or decrease insulin to carb ratio 1 unit +/- 5 grams of carbohydrates
Oral Medication: mg Time:
NPH Insulin Dose: units SQ Time: Student’s Self Care: No supervision Full supervision, Requires some supervision: ability level to be determined by school nurse and parent unless otherwise indicated here: Additional Information:
Signatures: My signature below provides authorization for the written orders above and exchange of health information to assist the school nurse an Individualized Health Plan. I understand that all procedures will be implemented in accordance with state laws and regulations and may be performed by unlicensed designated school personnel under the training and supervision provided by the school nurse. This order is for a maximum of one year.
Physician: Date:
Parent: Date:

Form #201 Colorado Kids with Diabetes Care and Prevention Collaborative August 2019
2
School Nurse: Date:
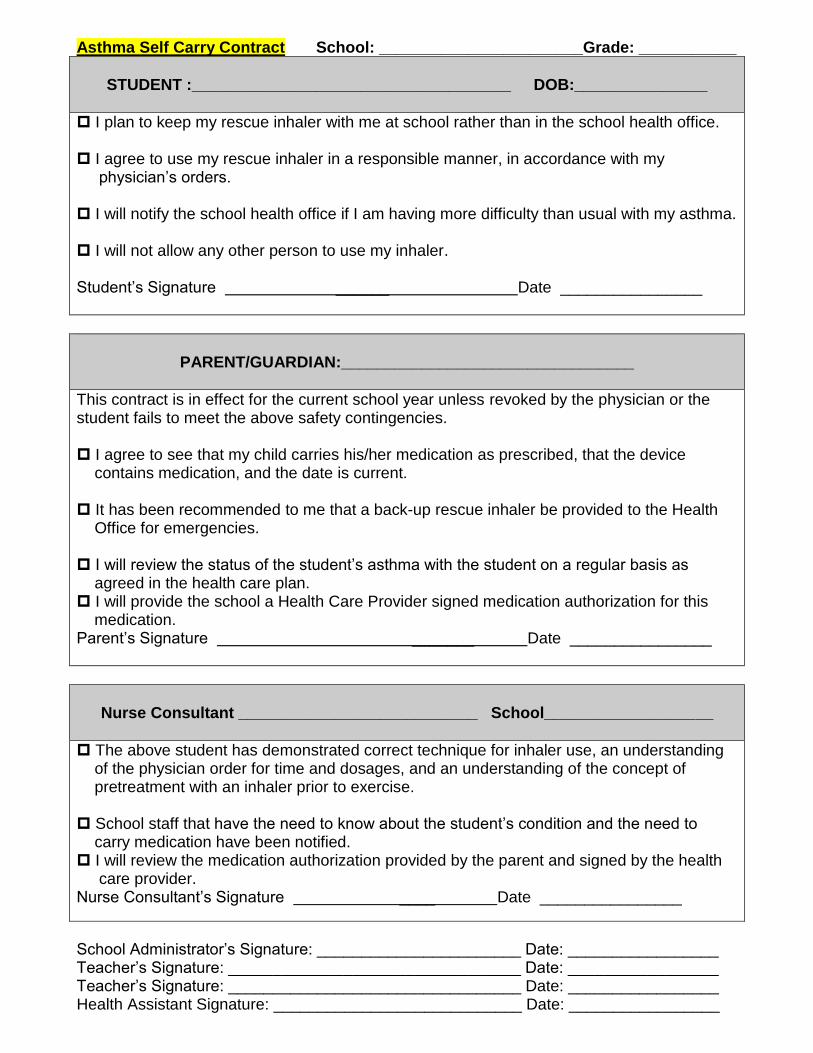
Asthma Self Carry Contract School: _______________________Grade: ___________
STUDENT :____________________________________ DOB:_______________
I plan to keep my rescue inhaler with me at school rather than in the school health office. I agree to use my rescue inhaler in a responsible manner, in accordance with my physician’s orders. I will notify the school health office if I am having more difficulty than usual with my asthma. I will not allow any other person to use my inhaler. Student’s Signature ______ Date ________________
PARENT/GUARDIAN:_________________________________
This contract is in effect for the current school year unless revoked by the physician or the student fails to meet the above safety contingencies. I agree to see that my child carries his/her medication as prescribed, that the device contains medication, and the date is current. It has been recommended to me that a back-up rescue inhaler be provided to the Health Office for emergencies. I will review the status of the student’s asthma with the student on a regular basis as agreed in the health care plan. I will provide the school a Health Care Provider signed medication authorization for this medication. Parent’s Signature _______ Date ________________
Nurse Consultant ___________________________ School___________________
The above student has demonstrated correct technique for inhaler use, an understanding of the physician order for time and dosages, and an understanding of the concept of pretreatment with an inhaler prior to exercise. School staff that have the need to know about the student’s condition and the need to carry medication have been notified. I will review the medication authorization provided by the parent and signed by the health care provider. Nurse Consultant’s Signature ____ Date ________________
School Administrator’s Signature: _______________________ Date: _________________ Teacher’s Signature: _________________________________ Date: _________________ Teacher’s Signature: _________________________________ Date: _________________ Health Assistant Signature: ____________________________ Date: _________________
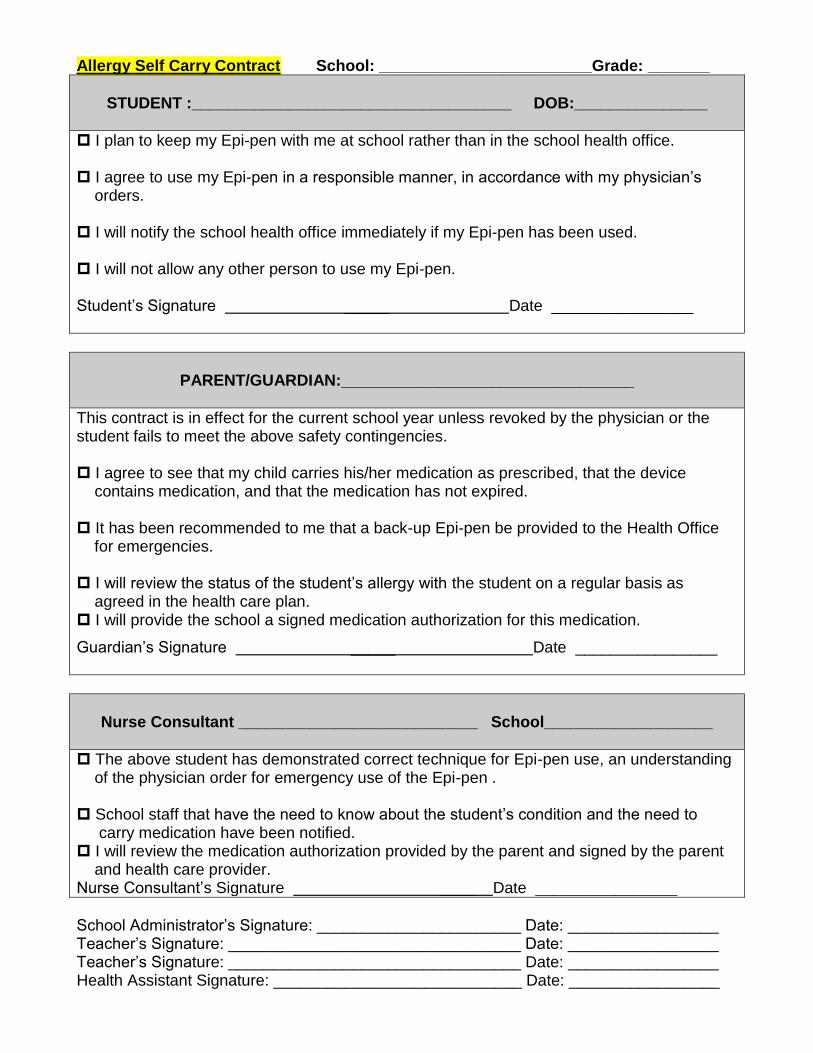
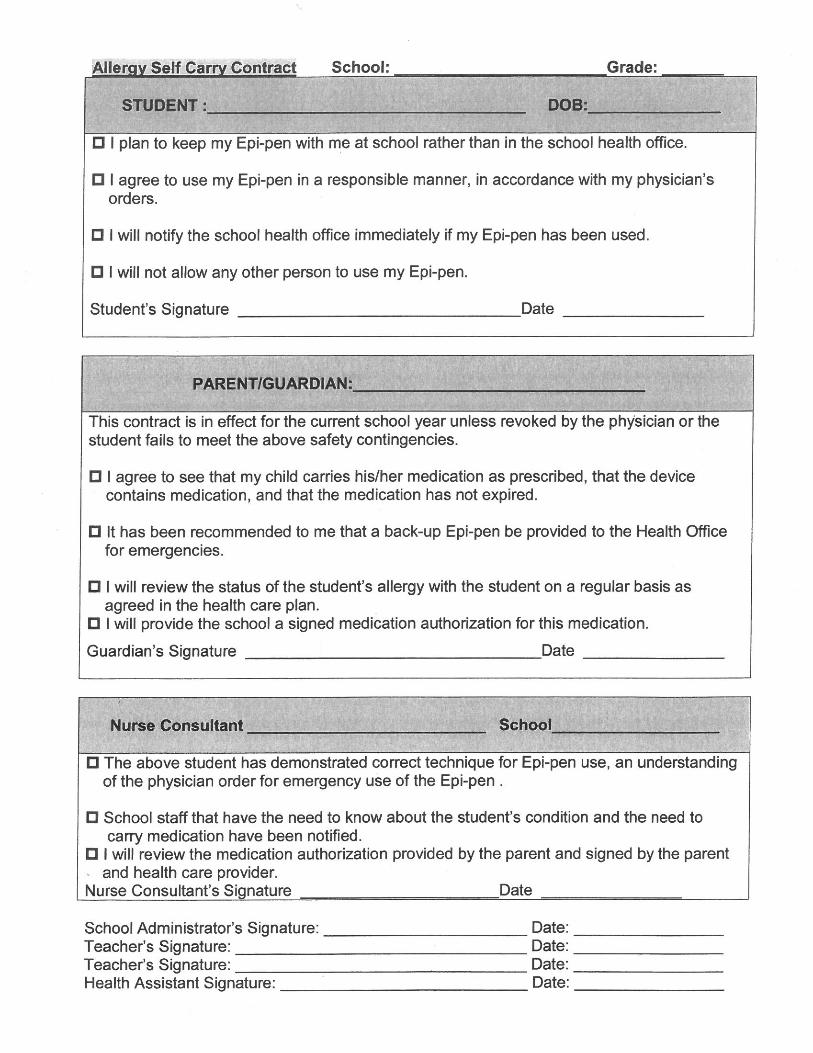
Allergy Self Carry Contract School: ________________________Grade: _______
STUDENT :____________________________________ DOB:_______________
I plan to keep my Epi-pen with me at school rather than in the school health office. I agree to use my Epi-pen in a responsible manner, in accordance with my physician’s orders. I will notify the school health office immediately if my Epi-pen has been used. I will not allow any other person to use my Epi-pen. Student’s Signature _____ Date ________________
PARENT/GUARDIAN:_________________________________
This contract is in effect for the current school year unless revoked by the physician or the student fails to meet the above safety contingencies. I agree to see that my child carries his/her medication as prescribed, that the device contains medication, and that the medication has not expired. It has been recommended to me that a back-up Epi-pen be provided to the Health Office for emergencies. I will review the status of the student’s allergy with the student on a regular basis as agreed in the health care plan. I will provide the school a signed medication authorization for this medication.
Guardian’s Signature _____ Date ________________
Nurse Consultant ___________________________ School___________________
The above student has demonstrated correct technique for Epi-pen use, an understanding of the physician order for emergency use of the Epi-pen . School staff that have the need to know about the student’s condition and the need to carry medication have been notified. I will review the medication authorization provided by the parent and signed by the parent and health care provider. Nurse Consultant’s Signature ____ Date ________________
School Administrator’s Signature: _______________________ Date: _________________ Teacher’s Signature: _________________________________ Date: _________________ Teacher’s Signature: _________________________________ Date: _________________ Health Assistant Signature: ____________________________ Date: _________________

Form #202 Colorado Kids with Diabetes Care and Prevention Collaborative 8/29/2019
1
Health Care Provider Orders for Student with Diabetes on Insulin Pump To be completed by the Health Care Provider and used in conjunction with the Standards of Care for Diabetes Management in the School Setting
www.coloradokidswithdiabetes.org
Student: DOB: School: Grade: Physician/Provider: Phone:
Diabetes Educator: Phone:
TARGET RANGE – Blood Glucose: mg/dl TO mg/dl
< 5y.o. 80-200mg/dl 5 – 8 y.o 80-200mg/dl 9-11y.o 70-180mg/dl 12-18y.o. 70-150mg/dl >18y.o. 70-130mg/dl
Notification to Parents: Low < target range and High > 300 mg/dl or Other: less than mg/dl and greater than: mg/dl Continuous glucose monitoring: Always Confirm glucose level with a fingerstick/meter prior to treatment unless student has a Dexcom G5 or G6, it may be used for
dosing and treatment. Please follow Collaborative Guidelines for Dexcom G5 & G6: Therapeutic Dosing in the School Setting (www.coloradokidswithdiabetes.org)
Hypoglycemia: Follow Standards of Care for Diabetes Management in the School Setting – Colorado, unless otherwise indicated here:
For Severe Symptoms: Call 911, Disconnect Pump, Administer: Glucagon Injection Dose: mg Intramuscular in OR BAQSIMI nasal spray 1 device (3mg) in one nostril Hyperglycemia: Follow Standards of Care for Diabetes Management in the School Setting – Colorado, unless otherwise indicated here: Ketone Testing: per Standards of Care for Diabetes Management in the School Setting – Colorado OR Other:
When to Check Blood Glucose: For provision of student safety while limiting disruption to learning Always for signs & symptoms of low/high blood glucose, when does not feel well and/or behavior concerns Check before meals and as mutually agreed upon by parent and school nurse
Other:
Insulin Pump: Follow Guidelines for Insulin Administration by School Staff, Diabetes Resource Nurses February 2013 Pump settings are established by the student’s healthcare provider and should not be changed by the school staff. All setting changes to be made at home or
by student providing self care as indicated on IHP.
Internal safety features for the insulin pump should be active at all times while the student is at school - (Alarms set conservatively).
Insulin Pump Brand: Type of Insulin in pump
Correction Bolus: Provide Correction bolus per pump calculator. All BG levels should be entered into the pump for administration of pump-calculated corrections unless otherwise indicated on the provider orders.
Sensitivity/Correction Factor: unit insulin for every mg/dl above target BG range starting at mg/dl
InsulinDosing Attached If blood glucose is less than mg/dl, wait to give meal bolus until after meal
When Hyperglycemia occurs other than at lunchtime: If it has been greater than 3 hours since the last dose of insulin, the student may be given insulin via injection using the indicated correction factor on the provider orders if approved by the school nurse and parent is notified. Contact Health Care Provider for One-time order
Carbohydrates and Insulin Dosage per pump: Breakfast Snack Lunch Other: Insulin Dosing Attached Insulin to Carbohydrate Ratio: unit(s) for every grams of carbohydrate to be eaten Bolus for carbohydrates should occur immediately Prior to lunch/snack After lunch/snack Split ½ before lunch & ½ after lunch Other:
Parent/guardian authorized to increase or decrease insulin to carb ratio 1 unit +/- 5 grams of carbohydrates
Pump Malfunctions: Disconnect pump when malfunctioning If pump calculator is operational then the insulin dosing should be calculated by using the pump bolus calculator and then insulin given by injection If pump calculator is not operational: School Nurse or Parent to give insulin according to Insulin to Carbohydrate Ratio and/or Correction Factor Call Parent and Health Care Provider (for orders) Student’s Self Care: No supervision Full supervision, Requires some supervision: ability level to be determined by school nurse and parent unless otherwise indicated here: Additional Information:
Signatures: My signature below provides authorization for the written orders above and exchange of health information to assist the school nurse an Individualized Health Plan. I understand that all procedures will be implemented in accordance with state laws and regulations and may be performed by unlicensed designated school personnel under the training and supervision provided by the school nurse. This order is for a maximum of one year.
Physician: Date:
Parent: Date:

Form #202 Colorado Kids with Diabetes Care and Prevention Collaborative 8/29/2019
2
School Nurse: Date:



