viernes, mesa 5 elena carreras moratonas
TRANSCRIPT

Predicción precoz
de Preeclampsia y restricción de crecimiento.
Cómo y con qué objetivo
E. Carreras. E. Llurba.
Unidad de medicina materno-fetal
Hospital Univesitari Vall d’Hebron. Barcelona
� Predicción de PE y CIR mediante Doppler
de arterias uterinas y factores angiogénicos
� Predicción de complicaciones placentarias
durante el primer trimestre
� Preeclampsia y CIR precoz vs tardio
Predicción de Preeclampsia & CIR
� Cribado de enfermedad placentaria tardía
� UTOPIA trial: RCT para demostrar que el
control exhaustivo mejora el pronóstico

� Predicción de PE y CIR mediante Doppler
de arterias uterinas y factores angiogénicos
� Predicción de complicaciones placentarias
durante el primer trimestre
� Preeclampsia y CIR precoz vs tardio
Predicción de Preeclampsia & CIR
� Cribado de enfermedad placentaria tardía
� UTOPIA trial: RCT para demostrar que el
control exhaustivo mejora el pronóstico
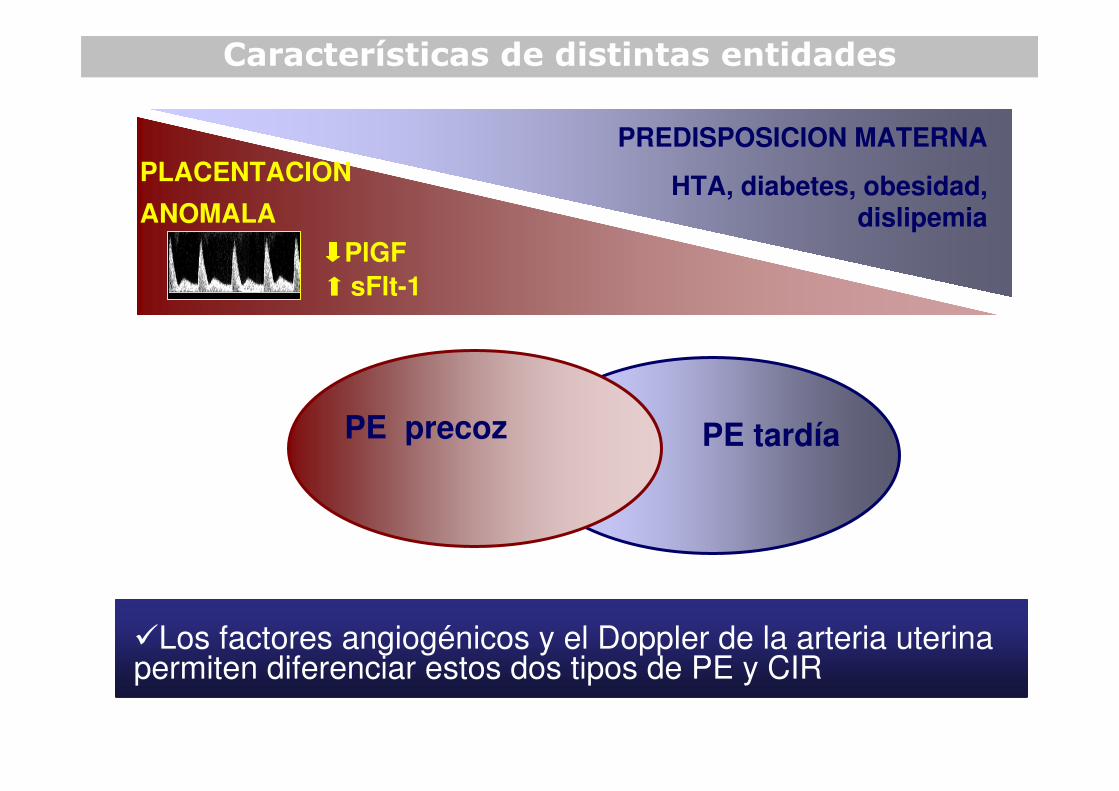
PE tardía
Características de distintas entidades
PE precoz
�Los factores angiogénicos y el Doppler de la arteria uterinapermiten diferenciar estos dos tipos de PE y CIR
PlGF
PLACENTACION
ANOMALA
sFlt-1
PREDISPOSICION MATERNA
HTA, diabetes, obesidad, dislipemia
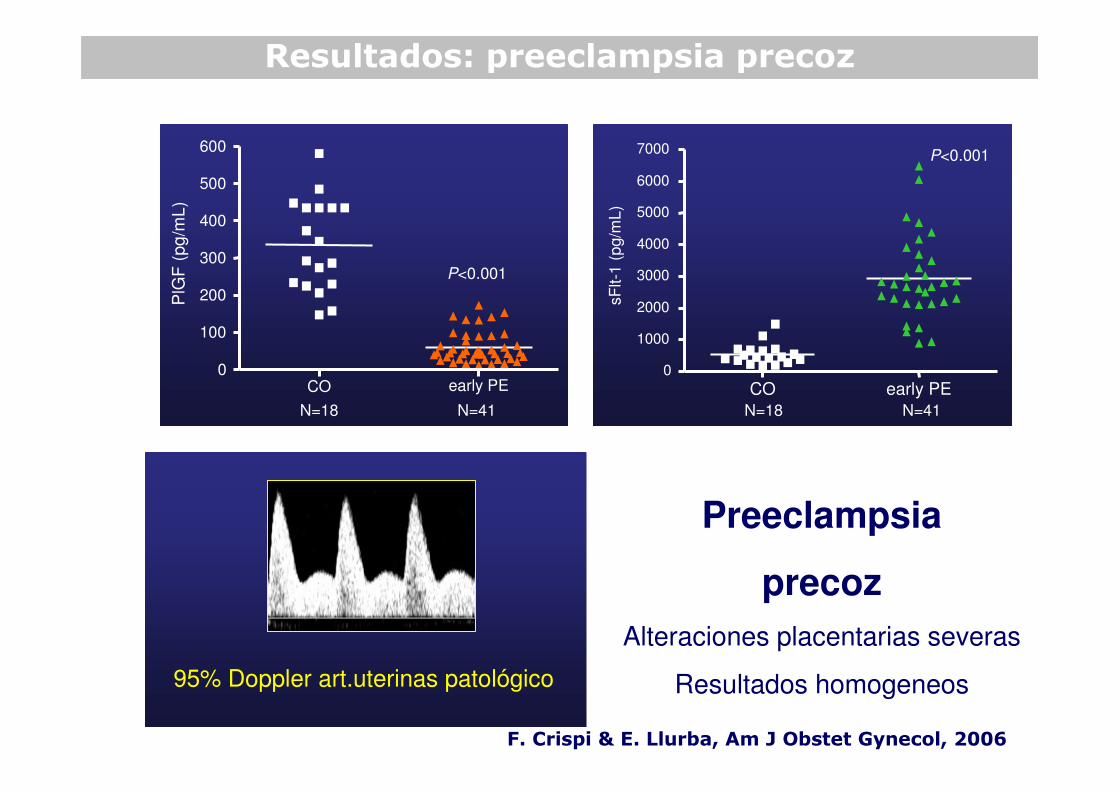
Resultados: preeclampsia precoz
Preeclampsia
precoz
Alteraciones placentarias severas
Resultados homogeneos95% Doppler art.uterinas patológico
CO early PE0
100
200
300
400
500
600
PlG
F(p
g/m
L)
N=18 N=41
P<0.001
CO early PE0
1000
2000
3000
4000
5000
6000
7000
sF
lt-1
(p
g/m
L)
N=41N=18
P<0.001
F. Crispi & E. Llurba, Am J Obstet Gynecol, 2006

Resultados: preeclampsia tardía
Preeclampsia
tardía
Grupo heterogeneo
Distintos subgrupos
CO late PE
0
100
200
300
400
500
PlG
F(p
g/m
L)
N=22 N=35
P<0.05
CO late PE
0
500
1000
1500
2000
2500
3000
3500
4000
4500
sF
lt-1
(p
g/m
L)
N=35N=22
P<0.05
F. Crispi & E. Llurba, Am J Obstet Gynecol, 2006
46% Doppler art.uterinas patológico
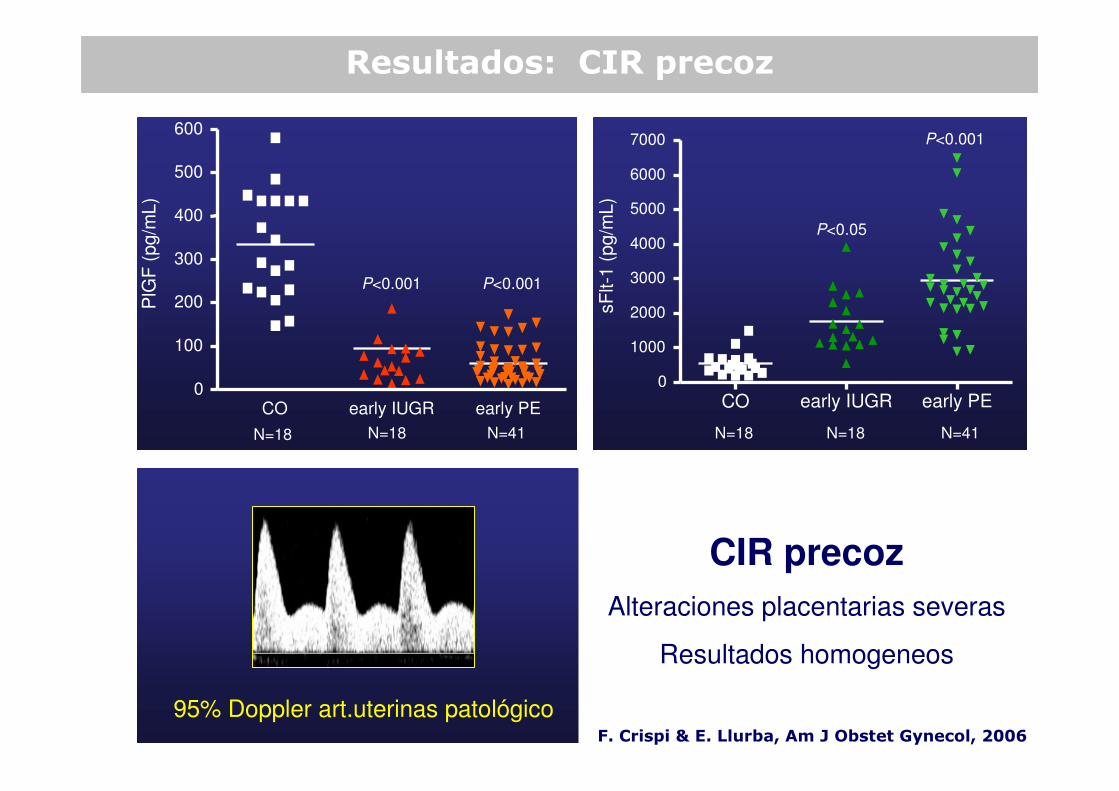
Resultados: CIR precoz
CO early IUGR early PE0
1000
2000
3000
4000
5000
6000
7000
sF
lt-1
(pg/m
L)
P<0.001
P<0.05
N=41N=18 N=18
CO early IUGR early PE0
100
200
300
400
500
600
PlG
F(p
g/m
L)
P<0.001P<0.001
N=18 N=18 N=41
F. Crispi & E. Llurba, Am J Obstet Gynecol, 2006
95% Doppler art.uterinas patológico
CIR precoz
Alteraciones placentarias severas
Resultados homogeneos

� Predicción de PE y CIR mediante Doppler de
arterias uterinas y factores angiogénicos
� Predicción de complicaciones placentarias
durante el primer trimestre
� Preeclampsia y CIR precoz vs tardio
Predicción de Preeclampsia & CIR
� Cribado de enfermedad placentaria tardía
� UTOPIA trial: RCT para demostrar que el
control exhaustivo mejora el pronóstico

84 %
PE< 32w
Factores angiogénicos y Doppler arterias uterinas
1,00,80,60,40,20,0
False Positive Rate
1,0
0,8
0,6
0,4
0,2
0,0S
en
sit
ivit
y
False Positive Rate
1,00,80,60,40,20,0
1,0
0,8
0,6
0,4
0,2
0,0
Se
ns
itiv
ity
PE ≥ 32w
10%
Ut Doppler+PlGF/sFlt-1
E. Llurba & F. Crispi, Ultrasound Obstet Gynecol, 2008

� Predicción de PE y CIR mediante Doppler
de arterias uterinas y factores angiogénicos
� Predicción de complicaciones placentarias
durante el primer trimestre
� Preeclampsia y CIR precoz vs tardio
Predicción de Preeclampsia & CIR
� Cribado de enfermedad placentaria tardía
� UTOPIA trial: RCT para demostrar que el
control exhaustivo mejora el pronóstico
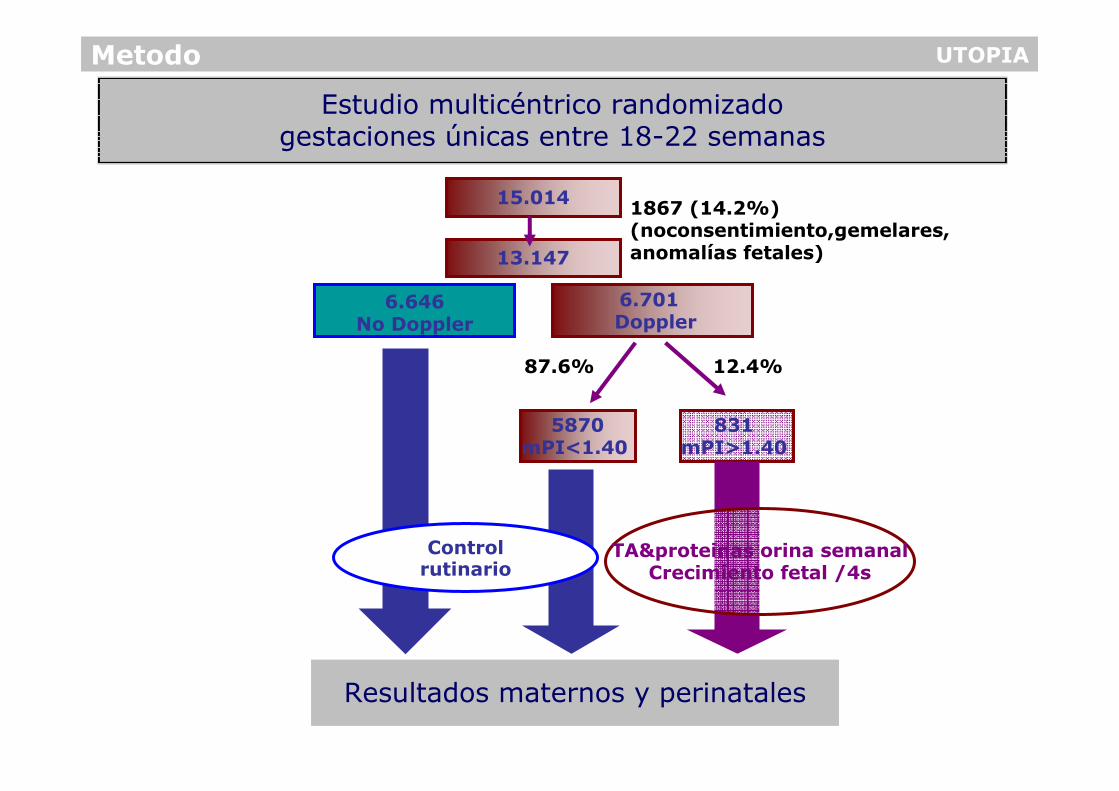
1867 (14.2%)(noconsentimiento,gemelares,anomalías fetales)
UTOPIA
Resultados maternos y perinatales
Metodo
15.014
13.147
6.646 No Doppler
6.701 Doppler
5870mPI<1.40
831 mPI>1.40
TA&proteinas orina semanalCrecimiento fetal /4s
87.6% 12.4%
Estudio multicéntrico randomizadogestaciones únicas entre 18-22 semanas
Control rutinario

UTOPIARESULTS
Outcome No Doppler n=6075
Dopplern=6120
GA at delivery (weeks) 39.4 39.4 0.87
Birth weight (gr) 3237 (580-4680) 3299 (480-4780) 0.23
Comparación entre resultados maternos y perinatales
en los grupos no-Doppler y Doppler
Preeclampsia, n (%) 202 (3.34%) 223 (3.53%) 0.76
FGR, n (%) 336 (5.65%) 383 (6.18%) 0.21
SGA, n (%) 348 (5.85%) 356 (5.74%) 0.44
Intrauterine fetal death (%) 33 (0.55%) 32 (0.52%) 0.77
Maternal complications 132 (2.01%) 140 (2.04%) 0.85
Maternal death 1 (0.007%) 1 (0.007%) 1
Neonatal complications 475 (10.73%) 492 (10.63%) 0.93
Neonatal death 24 (0.54%) 30 (0.66%) 0.50

Resultados
Tratamiento con Sulfato Magnesio
Tratamiento con Corticoides
Inducción por Doppler patológico
Cesárea urgente
Complicaciones maternas
Complicaciones neonatales
Muerte perinatal
1
OR (95% CI)
1.02 (0.62-2.03)
2.18 (1.28-3.73)
2.01 (1.26-3.22)
1.09 (0.74-1.09)
0.61 (0.36-1.03)
1.07 (0.82-1.38)
0.82 (0.43-1.57)
Odds Ratio (95% CI)
p
0.82
0.003
0.004
0.60
0.06
0.62
0.56
Dopplern=962
No-Dopplern=886
Comparación entre resultados maternos y perinatales
en los grupos no-Doppler y Doppler
en pacientes con enfermedad placentaria
� Predicción de PE y CIR mediante Doppler
de arterias uterinas y factores angiogénicos
� Predicción de complicaciones placentarias
durante el primer trimestre
� Preeclampsia y CIR precoz vs tardio
Predicción de Preeclampsia & CIR
� Cribado de enfermedad placentaria tardía
� UTOPIA trial: RCT para demostrar que el
control exhaustivo mejora el pronóstico

AAS PREECLAMPSIA: Doppler artèries uterines primer trimestre? Predicción de Preeclampsia durante el primer trimestre
Poon&Nicolaides, UOG, 2010
PE < 32w PE > 37wPE 32-36.6w

� Predicción de PE y CIR mediante Doppler
de arterias uterinas y factores angiogénicos
� Predicción de complicaciones placentarias
durante el primer trimestre
� Preeclampsia y CIR precoz vs tardio
Predicción de Preeclampsia & CIR
� Cribado de enfermedad placentaria tardía
� UTOPIA trial: RCT para demostrar que el
control exhaustivo mejora el pronóstico

mUtA_PI z-scoresTercer Trimestre
Normal (<2SD) Abnormal (≥ 2SD)
Primer trimestre
Normal (<2SD) 878 31
Abnormal (≥ 2SD) 31 5
RESULTADOS
Concordancia entre 1er y 3er trimestre
mUtA-PI z-scores anómalos
***
***
% p
ati
ents
wit
hP
RD
0
20
40
60
80
100
Normal 1-3T Abnormal 1T-Normal 3T
Normal 1T-Abnormal 3T
Abnormal 1T-3T
Llurba&Baschat, AJ perinatology, 2012

RESULTADOS
20 60
20
60
100
100-Specificity
Sensitivity
100
Δ mUt-PI
1st trimester mUt-PI z-scores
3st trimester mUt-PI z-scores
ROC curves
p=0.003
Llurba&Baschat, AJ perinaltology, 2012

Antioxidantes
Vitaminas
Aspirina
HBPM
Calcio
Prevención de preeclampsia

AAS
HBPM
Calcio
Prevención de preeclampsia
Bajaingesta

GESTACIONES
ALTO RIESGO
DOPPLER ARTERIAS
UTERINAS PATOLOGICO
PREECLAMPSIA
Prevención de preeclampsia: Aspirina
PREECLAMPSIA: antecents obstètrics o médics
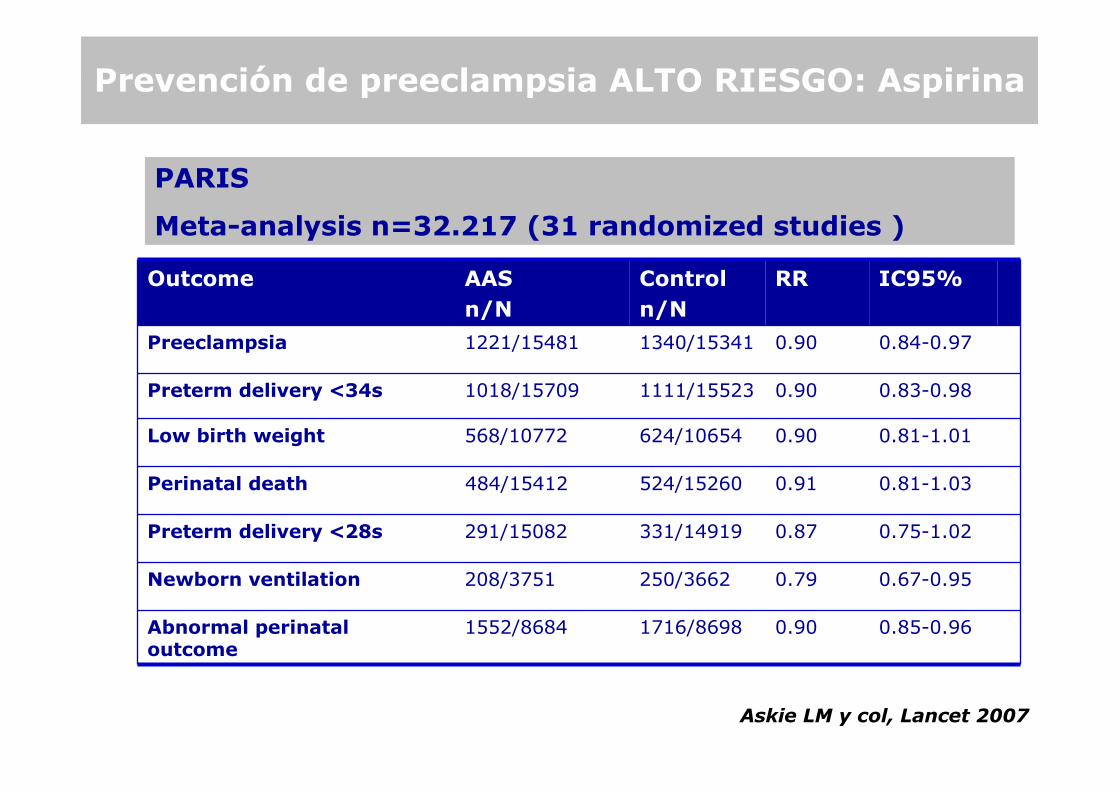
PARIS
Meta-analysis n=32.217 (31 randomized studies )
Outcome AAS
n/N
Control
n/N
RR IC95%
Preeclampsia 1221/15481 1340/15341 0.90 0.84-0.97
Preterm delivery <34s 1018/15709 1111/15523 0.90 0.83-0.98
Low birth weight 568/10772 624/10654 0.90 0.81-1.01
Perinatal death 484/15412 524/15260 0.91 0.81-1.03
Preterm delivery <28s 291/15082 331/14919 0.87 0.75-1.02
Newborn ventilation 208/3751 250/3662 0.79 0.67-0.95
Abnormal perinatal outcome
1552/8684 1716/8698 0.90 0.85-0.96
Askie LM y col, Lancet 2007
Prevención de preeclampsia ALTO RIESGO: Aspirina

Askie LM y col, Lancet 2007
PREECLAMPSIA: antecents obstètrics o médics
PARIS
Meta-analysis n=32.217 (31 randomized studies )
Outcome AAS
n/N
Control
n/N
RR IC95%
Preeclampsia 1221/15481 1340/15341 0.90 0.84-0.97
Preterm delivery <34s 1018/15709 1111/15523 0.90 0.83-0.98
Low birth weight 568/10772 624/10654 0.90 0.81-1.01
Perinatal death 484/15412 524/15260 0.91 0.81-1.03
Preterm delivery <28s 291/15082 331/14919 0.87 0.75-1.02
Newborn ventilation 208/3751 250/3662 0.79 0.67-0.95
Abnormal perinatal outcome
1552/8684 1716/8698 0.90 0.85-0.96
Prevención de preeclampsia ALTO RIESGO: Aspirina

Askie LM y col, Lancet 2007
PREECLAMPSIA: antecents obstètrics o médics
PARIS
Meta-analysis n=32.217 (31 randomized studies )
Inicio tratamiento AAS
n/N
Control
n/N
RR IC95%
<20s 686/9171 776/9023 0.87 0.79-0.96
≥≥≥≥ 20s 534/6263 560/6260 0.95 0.85-1.06
Prevención de preeclampsia ALTO RIESGO: Aspirina
≤≤≤≤ 16s AAS
%
Control
%
RR IC95%
Preeclampsia 9.3 21.3 0.47 0.34-0.65
IUGR 7 16.3 0.44 0.30-0.65
Severe Preeclampsia 0.7 15 0.09 0.02-0.37
Preterm delivery 3.5 16.9 0.22 0.10-0.49
Gestacional Hypertension
16.7 29.7 0.62 0.45-0.84
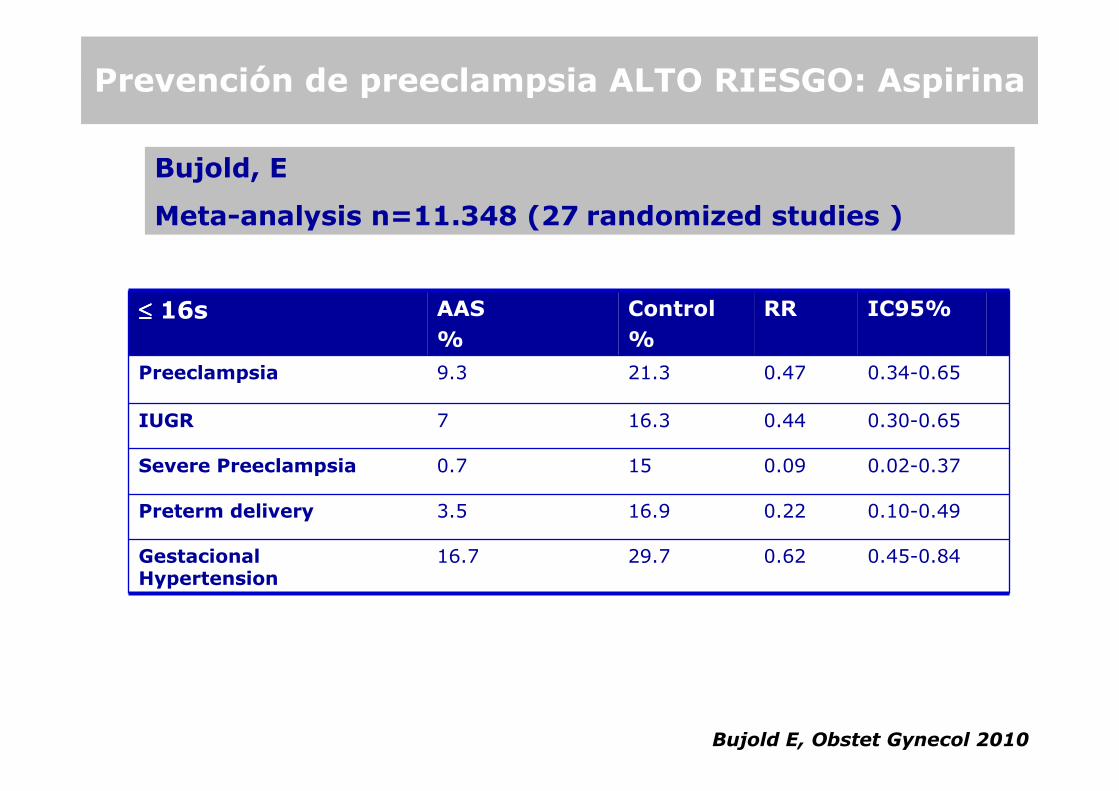
Bujold E, Obstet Gynecol 2010
PREECLAMPSIA: antecents obstètrics o médics
Bujold, E
Meta-analysis n=11.348 (27 randomized studies )
Prevención de preeclampsia ALTO RIESGO: Aspirina
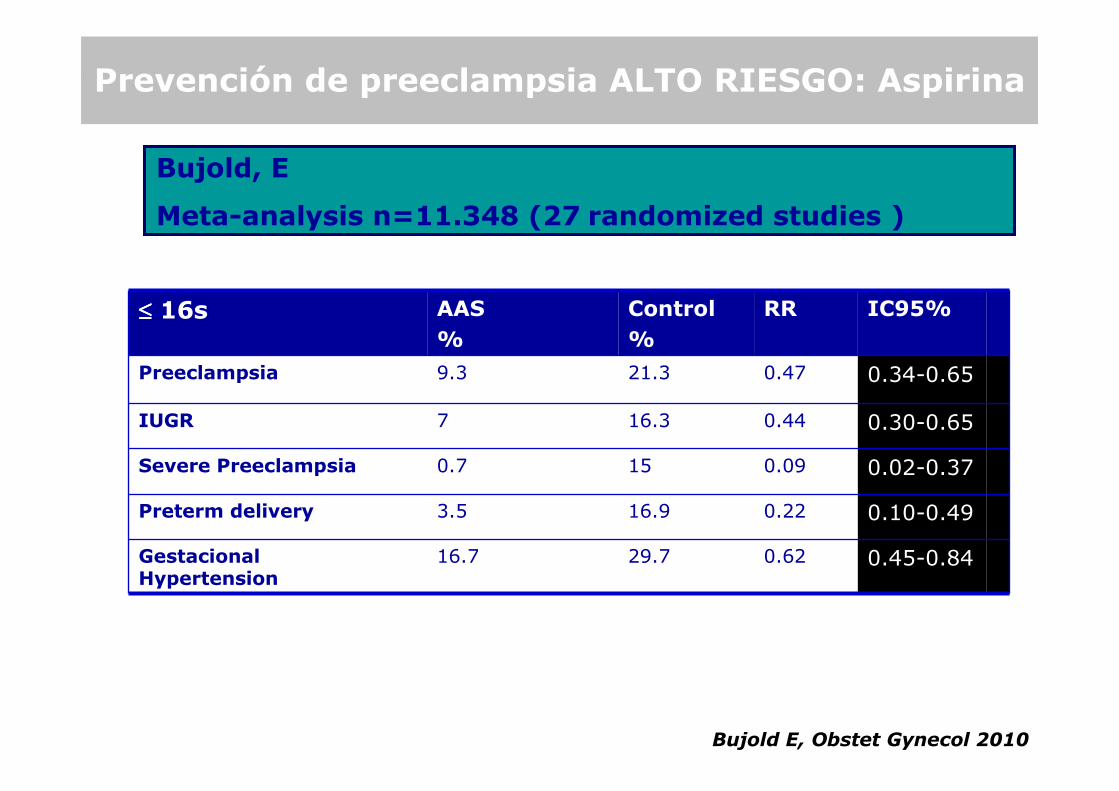
≤≤≤≤ 16s AAS
%
Control
%
RR IC95%
Preeclampsia 9.3 21.3 0.47 0.34-0.65
IUGR 7 16.3 0.44 0.30-0.65
Severe Preeclampsia 0.7 15 0.09 0.02-0.37
Preterm delivery 3.5 16.9 0.22 0.10-0.49
Gestacional Hypertension
16.7 29.7 0.62 0.45-0.84
Bujold E, Obstet Gynecol 2010
PREECLAMPSIA: antecents obstètrics o médics
Bujold, E
Meta-analysis n=11.348 (27 randomized studies )
Prevención de preeclampsia ALTO RIESGO: Aspirina

GESTACIONES
ALTO RIESGO
DOPPLER ARTERIAS
UTERINAS PATOLOGICO
PREECLAMPSIA
Prevención de preeclampsia: Aspirina

12-15 s: Pacientes alto riesgo + Doppler art. uterinas patológico
Fox et al, BJOG, 2010
Aspirina en Doppler uterinas patológico

1st Trimester 3rd Trimester0.0
0.5
1.0
1.5
2.0
***
*
p<0.0001
ASA-group (n=183)
non ASA-group (n=661)
UtA drop between 1st-3th TRESULTADOS
Efecto de Aspirina en Doppler arteria uterinan=183 (19.2%)
Mean uterine
artery PI
Llurba et al, Am J Perinatol, 2012

•Malformaciones congénitasMeta-analysis (22 estudios)
Malformaciones congénitas 1.13 0.94-1.89
Gastrosquisis 2.37 1.44-3.88
Kazer E, Am J Obstet Gynecol, 2002.
•Alteraciones hemorrágicasPARIS Meta-analysis (31 estudios)
Efecto secundario AAS
n/N
Control
n/N
RR IC95%
Hemorragia pre-parto 497/12996 480/12926 1.02 0.90-1.15
Abruptio 115/12213 97/12130 1.13 0.87-1.48
Hemorragia
Post-parto
1790/11662 1677/11565 1.06 1.00-1.13
Askie LM y col, Lancet 2007
Aspirina : efectos secundarios

AAS
HBPM
Calcium
Prevención de preeclampsia
Lowcalciumintake
HBPM
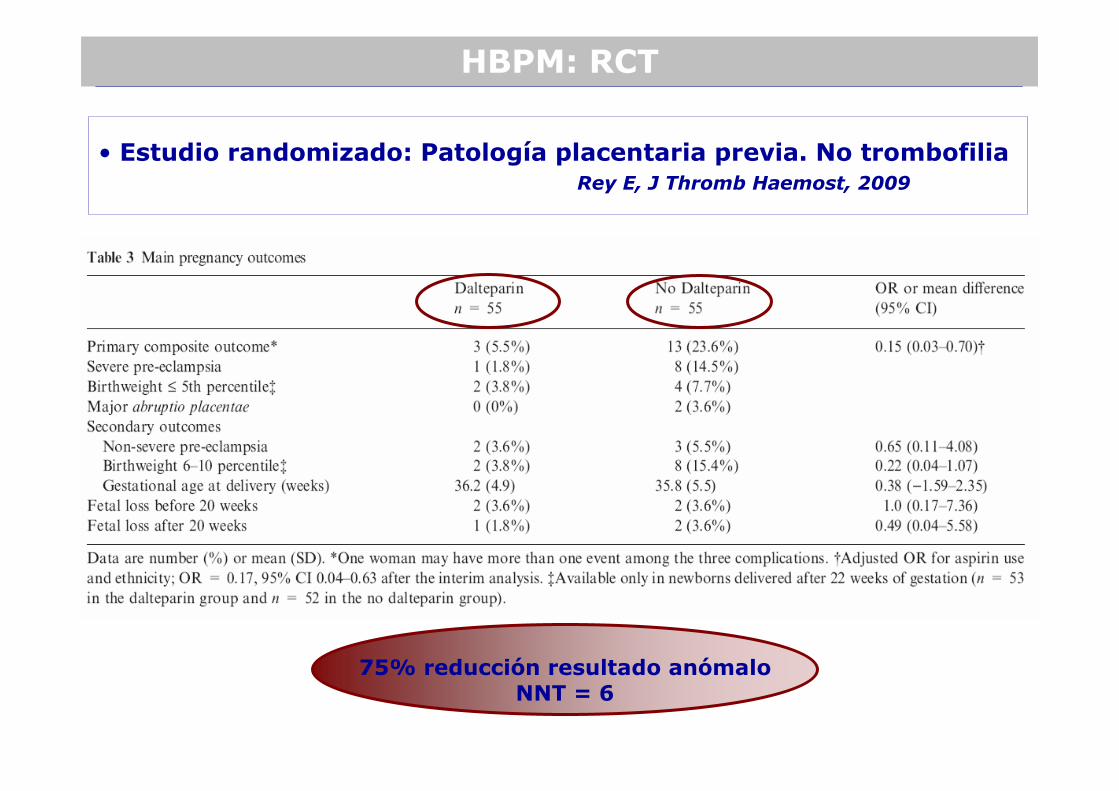
• Estudio randomizado: Patología placentaria previa. No trombofiliaRey E, J Thromb Haemost, 2009
75% reducción resultado anómaloNNT = 6
HBPM: RCT

HBPM
• Estudio randomizado: Patología placentaria previa. Sí trombofilias
LMWH: RCT
Nadroparin ycontrol médico
(n = 63)
Control médico exclusivo (n = 65)
RR (95% CI) P
Recurrent pregnancycomplications, n (%)
13 (20.6) 12 (18.5) 2.2 (−11.6 to 16.0) .76
Preeclampsia 5 (7.9) 3 (4.6) 3.3 (−5.9 to 13.1) .44
Eclampsia 0 0 NA NA
HELLPsyndrome
1 (1.6) 0 1.6 (−4.2 to 8.5) .49
Intrauterinefetal death
2 (3.2) 1 (1.5) 1.6 (−5.4 to 9.4) .62
FGR 5 (7.9) 7 (10.8) −2.8 (−13.6 to 8.0) .58
Placentalabruption
0 1 (1.5) −1.5 (−8.2 to 4.3) 1.0
Martinelli I et al. Blood 2012;119:3269-3275

HBPM HBPM: RCT
�10 estudios, 5 cumplían criterios inclusión, 484 gestantes
�No diferencias significativas para resultados primarios de mortalidad
perinatal, parto prematuro < 34 semanas, déficit neurológico infantil
�Tratamiento con heparina parece prometedor con una reducción de
preeclampsia, eclampsia y peso por debajo del percentil 10
�Se requieren más estudios

Prevención Preeclampsia
Vitamines
anti-oxidants
AAS
HBPM
Calci
?Low
calciumintake

Objectivo
• Evaluar si HBPM antes de la semana 14 puede disminuir lascomplicaciones placentarias en gestaciones de alto riesgo
• Criterios de inclusión: �Preeclampsia severa <34s, �CIR (<10th+Abnormal UA) <34s �Abruptio placenta �Pérdida gestacional >20s�Doppler arterias uterinas anómalo 11+0-13+6 s
HOPPE TRIAL: Heparin prOfilactic Prevention PreEclampsia
Tratamientos en estudio


UTOPIARESULTS
Outcome Normal Doppler n=5353
AbnormalDoppler n=768
GA at delivery (weeks) 39.4 38.6 <0.001
Birth weight (gr) 3346 (520-4780) 2957 (480-4430) 0.009
Comparación de resulatdos maternos y perinatales entreDopplers normales y anómalos
Preeclampsia, n (%) 122 (2.2%) 101 (13%) <0.001
Preeclampsia < 32 w, n (%) 16 (0.29%) 19 (2.54%) <0.001
FGR, n (%) 234 (4.3%) 149 (19.4%) <0.001
SGA, n (%) 267 (4.9%) 89 (11.5%) <0.001
Abruption placenta, n (%) 16(0.29%) 13(1.69%) <0.001
Intrauterine fetal death 22 (0.4%) 11 (1.4%) 0.0003
Maternal complications 80 (1.49%) 60 (7.8%) <0.001
Neonatal complications 423 (7.9%) 69 (14%) 0.3
Neonatal mortality 22 (0.41%) 8 (1.04%) 0.019

Doppler aUT 12-14 s (n=120 High risk)
Abnormal aUTDoppler(n=90)
ASS
(n=45)
Placebo
(n=45)
PE 0.22(0.05-0.86)
Vainio; BJOG, 2002
12-14s
PE 0.57(0.40-0.82)
ASS
(n=74)
Placebo
(n=65)
Ebrashy, CMJ, 2005
Doppler aUT 12-14 s (High risk)
Abnormal aUTDoppler(n=90(n=139)
61% PE23% PE
Aspirin in patients with abnormal uterine Doppler

PE < 32w
1,00,80,60,40,20,0
1,0
0,8
0,6
0,4
0,2
0,0
27%
73%75%
PE ≥ 32w
1,00,80,60,40,20,0
1,0
0,8
0,6
0,4
0,2
0,0
39%
45%
52%
False Positive Rate
Se
ns
itiv
ity
10%
False Positive Rate
Se
ns
itiv
ity
10%
Early-onset Preeclampsia: predicción medianteDoppler arterias uterinas y edad materna
Maternal History Ut Doppler Combination
E. Llurba Obstet Gynecol International, 2009