lesiones mamarias no neos
TRANSCRIPT
8/8/2019 Lesiones Mamarias No Neos
http://slidepdf.com/reader/full/lesiones-mamarias-no-neos 1/7
722 Arch Pathol Lab Med—Vol 133, May 2009 Nonneoplastic Epithelial Changes in the Breast —Murray
Nonneoplastic Alterations of the Mammary EpitheliumCan Mimic Atypia
Melissa Murray, DO
● Context.—The pathologist evaluating breast biopsy spec-imens sometimes encounters nonneoplastic alterations of the mammary epithelium that raise the differential diag-nosis of atypia. Because the identification of atypical duc-tal hyperplasia of the breast has significant clinical impli-cations, it is important to correctly recognize its nonneo-plastic morphologic mimics.
Objective.—To highlight a spectrum of physiologic andtreatment-related changes that can occur in the mammaryepithelium and to discuss the differential diagnosis withtrue atypia.
Data Sources.—A comprehensive review of the pub-
lished English literature on physiologic and treatment-re-lated changes of the breast epithelium was performed.
Conclusions.—Among physiologic alterations of the duc-tal epithelium, luteal-phase changes and secretory changescan sometimes be overinterpreted as atypical. Treatment-related changes, secondary to chemotherapy and radiation,can pose a major diagnostic challenge and their misinter-pretation as neoplastic carries major clinical consequenc-es. Familiarity with the morphology of both physiologicand treatment-related alterations of the mammary epithe-lium is essential to avoid misdiagnosis.
(Arch Pathol Lab Med. 2009;133:722–728)
Histologic examination of tissue biopsy specimens re-mains the cornerstone for the diagnosis of breast
diseases and it is essential for the pathologist to be famil-iar with the spectrum of ‘‘normal’’ histologic alterationsof the mammary epithelium. The breast is a hormone-reg-ulated organ and its morphology is greatly affected byreproductive hormones. In addition to physiologic chang-es, therapeutic interventions, such as chemotherapy and/or radiation, also produce morphologic alterations. Asmore patients with breast cancer undergo breast conser-vation therapy and survival after breast cancer treatmentincreases, pathologists will encounter treatment-relatedchanges of the breast. Knowledge of the histologic spec-trum of both physiologic and treatment-induced alter-ations of the breast is of foremost importance to avoiddiagnostic pitfalls. This review highlights some of the non-neoplastic alterations of the mammary epithelium in thedifferential diagnosis of true atypia.
PHYSIOLOGIC CHANGES
The breast undergoes physiologic changes during pu- berty, pregnancy and lactation, menopause, and postmen-opausal age. Furthermore, the cells of the mature mam-mary lobules (myoepithelium and luminal/ductal cells)
Accepted for publication January 8, 2009.From the Department of Pathology, Memorial Sloan-Kettering Cancer
Center, New York, New York.The author has no relevant financial interest in the products or com-
panies described in this article.Presented in part at the Surgical Pathology of Neoplastic Diseases
course, Memorial Sloan-Kettering Cancer Center, New York, New York,May 12–16, 2008.
Reprints: Melissa Murray, DO, Department of Pathology, MemorialSloan-Kettering Cancer Center, 1275 York Ave, New York, NY 10065(e-mail: [email protected]).
undergo physiologic changes associated with the menstru-al cycle.
During the follicular phase of the menstrual cycle, thelobules are relatively small, and the acini are tightly clus-tered. The specialized intralobular stroma is hypocellularand appears slightly fibrotic. The luminal cells lining theacini are small and polygonal, have pale cytoplasm anddark, round, centrally located nuclei. These cells appearcrowded and nearly flattened and the acini show small orcollapsed lumina. No mitotic activity occurs in the normalepithelium during this phase. The myoepithelial cells areinconspicuous, often barely discernible on close inspec-tion. As the menstrual cycle progresses, the myoepithe-lium becomes more apparent and acquires vacuolated cy-toplasm. Eosinophilic secretions also begin to appearwithin the acinar lumen (Figure 1).
In the luteal phase, the lobules appear increased in sizecompared with the proliferative phase. The specialized in-tralobular stroma responds to progesterone stimulation by becoming loose and edematous and is infiltrated by lym-phocytes. The cytoplasm of the luminal cells usually ac-quires a distinctive basophilic hue and shows polarizedmorphology, with basally located nuclei and more prom-inent apical cytoplasm. The nuclei are enlarged and prom-
inent, with conspicuous nucleoli. The acinar lumina areopen and contain secretions. Mitotic figures are frequentin the luminal layer, as well as focal apoptosis (Figure 2).In this phase of the menstrual cycle, the myoepithelial cellsalso become more prominent and show abundant, vacu-olated cytoplasm and small, round, centrally located nu-clei.1,2 In some instances, the enlarged myoepithelial cellswith clear cytoplasm can mimic classical lobular carcino-ma in situ, undermining normal luminal epithelium. Inthis setting, however, the lobules are not expanded anddo not show increased cellularity and the acinar lumina
8/8/2019 Lesiones Mamarias No Neos
http://slidepdf.com/reader/full/lesiones-mamarias-no-neos 2/7
Arch Pathol Lab Med—Vol 133, May 2009 Nonneoplastic Epithelial Changes in the Breast —Murray 723
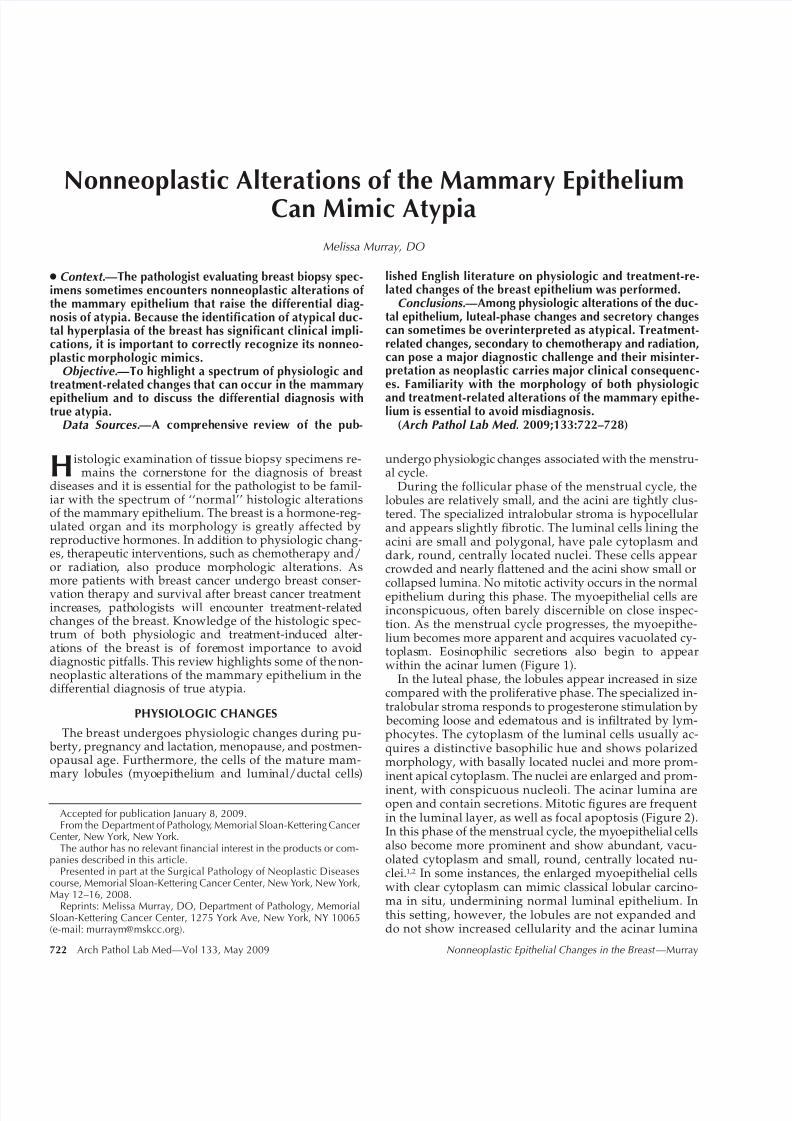
Figure 1. Follicular phase of the menstrual cycle. A lobule shows tightly clustered acini lined by polygonal cells with scant pale cytoplasm and dark round nuclei (hematoxylin-eosin, original magnification 400).
Figure 2. Luteal phase of the menstrual cycle. The luminal cells show enlarged nuclei with prominent nucleoli. Mitotic figures are commonly seen. The intralobular stroma is loose and edematous (hematoxylin-eosin, original magnification 600).
Figure 3. Secretory (pregnancy-like) changes. The acini are dilated and lined by a single layer of cuboidal cells with abundant clear cytoplasm.The lobule resembles those of pregnancy or lactation (hematoxylin-eosin, original magnification 400).
Figure 4. Cystic hypersecretory hyperplasia. Dilated cysts are filled with homogenous, eosinophilic secretion of colloidlike material. The cysts are lined by a single layer of cuboidal or columnar cells (hematoxylin-eosin, original magnification 400).
are patent and lined by polarized cells, also showing lu-teal phase changes.
Presence of mitoses, focal apoptosis, nuclear enlarge-ment, and prominent nucleoli can be worrisome findingson high-power examination. In these cases, the diffuse na-ture of the epithelial changes, the prominent edema of the
intralobular stroma, and the finding of a continuous layerof vacuolated myoepithelial cells are useful clues to thediagnosis. Luteal phase changes mimicking atypia shouldalways be in the differential diagnosis when examining aspecimen from young to premenopausal women.
The postmenopausal breast consists for the most part offibrous and adipose tissue with few scattered residualducts, acini, and vessels. Atrophy of the glandular com-ponent is normal with increasing age and is characterized by loss of the glandular epithelium and increasing thick-ness of the basement membranes, leading to progressiveobliteration of the acini. Cystification of the acini may oc-
cur, but it is not considered part of fibrocystic disease.Exogenous hormones reduce the atrophic changes and canresult in epithelial hyperplasia, with appreciable mitoticactivity.3
Secretory (Pregnancy-like) Changes
Secretory (pregnancy-like) changes (SC) can occur inthe breast independent of pregnancy status. These secre-tory changes have also been reported in men taking ex-ogenous estrogen. The etiology of these changes is un-known and association with medications has been sug-gested.
The lobules with SC resemble those of late pregnancyand lactation, but the alteration is usually limited to only1 or 2 lobules. The affected acini are dilated and lined bya single layer of cuboidal to columnar cells with abundantpale to clear cytoplasm, finely granular or vacuolated. Thenuclei are typically small, round, and darkly stained (Fig-
8/8/2019 Lesiones Mamarias No Neos
http://slidepdf.com/reader/full/lesiones-mamarias-no-neos 3/7
724 Arch Pathol Lab Med—Vol 133, May 2009 Nonneoplastic Epithelial Changes in the Breast —Murray
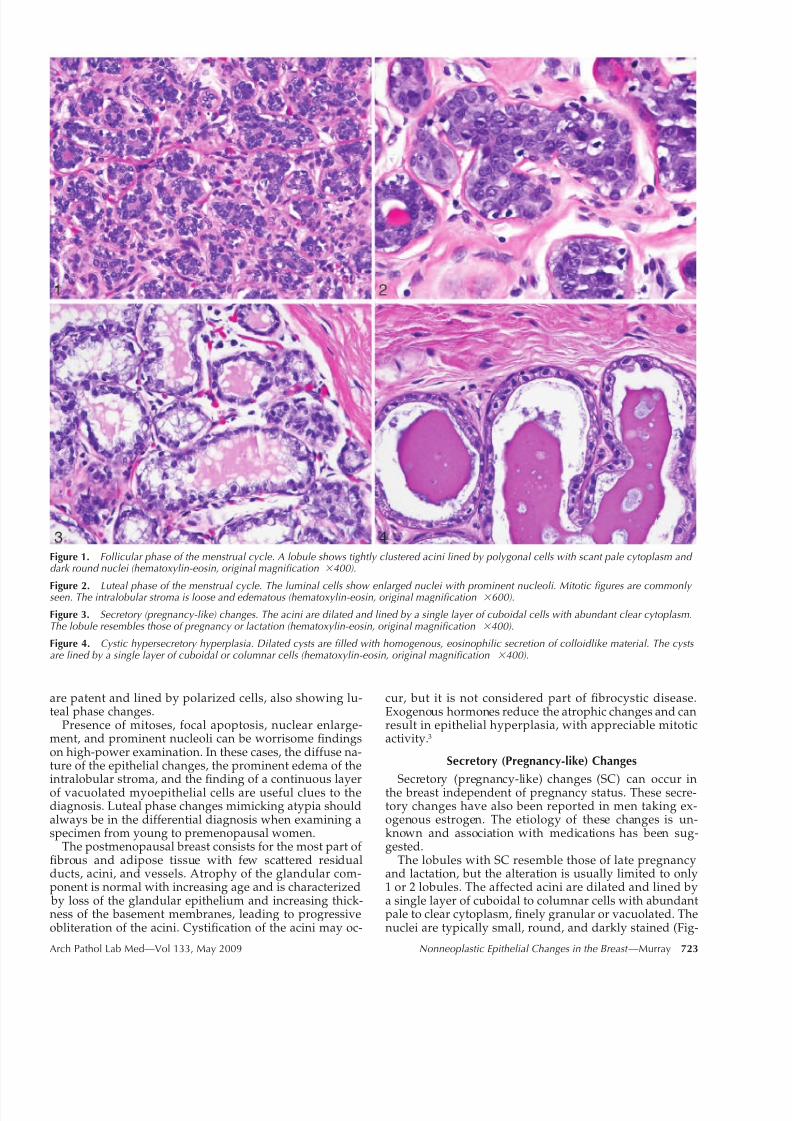
Figure 5. A, Lobule with clear cell change. The cells have abundant clear cytoplasm and small dark nuclei (hematoxylin-eosin). B, Clear cell change. The myoepithelial cells are maintained, as highlighted by positive stain for calponin (immunoperoxidase stain) (original magnifications 200 [A] and 100 [B]).
ure 3). Sometimes the nuclei protrude into the gland lu-
men and impart a hobnail appearance to the cells. Theepithelium in the lobules usually consists of 2 cell layers but the myoepithelium is inconspicuous; rarely, hyperpla-sia can occur and is not worrisome. Secretory material isoften present within the distended lumina and can be-come calcified, resulting in mammographically detectabledeposits. No further treatment is necessary if secretorychanges are present in a core biopsy specimen and thefindings are concordant with the imaging.
Coexistence of SC and cystic hypersecretory hyperplasiahas been reported by Shin and Rosen,4 and is discussedin the next section.
Cystic Hypersecretory Hyperplasia
Cystic hypersecretory hyperplasia (CHH) is regarded as
a benign proliferative lesion. Dilated cysts filled with ho-mogenous, eosinophilic, colloidlike secretions constituteits hallmark feature. The characteristic secretions are usu-ally acellular and often retract from the surrounding epi-thelium, with a smooth or scalloped margin; they rarelyundergo calcification and seldom contain histiocytes. Thecysts of CHH are lined by a single layer of flat, cuboidal,or columnar cells with eosinophilic cytoplasm; myoepi-thelial cells are inconspicuous. The epithelial cells haveround to oval, monotonous, and bland nuclei (Figure 4).Necrosis and mitoses are not found in CHH.5
The differential diagnosis of CHH includes CHH withatypia and cystic hypersecretory carcinoma in situ (CH-CIS), as well as clear cell ductal carcinoma in situ. Some
morphologic overlap exists in the spectrum of the cystichypersecretory lesions of the mammary epithelium. Theterm cystic hypersecretory hyperplasia applies only to cystslined by monostratified, cytologically bland epithelial cellswith low nuclear to cytoplasmic ratio. Increase in nuclearto cytoplasmic ratio, mitotic figures, nuclear pleomor-phism, and/or prominent large nucleoli are features in-dicative of cytologic atypia. Architectural atypia is typi-cally seen in the form of micropapillary growth. Greaterextents of architectural complexity (solid, cribriform, andmicropapillary growth) together with cytologic atypia arerequired for the diagnosis of CH-CIS. The latter may not
show the typical colloidlike secretions, and necrosis and
mitoses can be seen. In contrast to CH-CIS, clear cell duc-tal carcinoma in situ is typically solid with associated ne-crosis, and the cells have clear but nonvacuolated cyto-plasm; nuclei are hyperchromatic with clumped chromatinand prominent nucleoli.
Recently, Shin and Rosen4 showed a close relationship between SC and CHH. The authors reviewed 12 biopsyspecimens with SC and found coexisting CHH in 5 (42%).Secretory changes histologically merged with CHH in 4cases. Four biopsy specimens also showed cytologic atyp-ia, but no carcinoma in situ was identified.4
The same authors have also reported a series of 9 casesof SC and/or CHH adjacent to carcinoma in situ (7 CH-CIS and 2 low-grade micropapillary ductal carcinomas insitu, 1 of which was associated with invasive ductal car-
cinoma). In this series, the breast biopsies were performedfor calcifications (6 cases), mass (2 cases), and nipple dis-charge (1 case). Secretory changes merged with CHH in5 cases and were geographically distinct from it in 3, and1 case showed SC only. All but 3 cases showed atypia inSC, CHH, or both. Six patients underwent mastectomy (2 bilateral) and 2 underwent excision; 1 patient had incom-plete surgical history. The patient with invasive carcinomahad micrometastatic nodal disease, whereas no metastaseswere found in 4 patients who underwent lymph nodestaging. None of the patients had evidence of disease onfollow-up (range, 10 to 69 months).6 The authors conclud-ed that complete excision of the lesion is prudent when-ever CHH is seen on a core biopsy specimen to rule out
the possibility of focal carcinoma.
4,6
Clear Cell Change
The descriptive term clear cell change applies to an al-teration of the epithelium of the terminal duct lobular unitcharacterized by cytoplasmic clearing. No specific etiologyhas been reported for this alteration.
The cells usually have abundant cytoplasm, small darknuclei, and no nucleoli. The myoepithelial cells are main-tained. Clear cell change usually constitutes an incidentalfinding, limited to a lobule or only part of it, and rarelyassociates with calcifications (Figure 5, A and B). Clear cell

8/8/2019 Lesiones Mamarias No Neos
http://slidepdf.com/reader/full/lesiones-mamarias-no-neos 4/7
Arch Pathol Lab Med—Vol 133, May 2009 Nonneoplastic Epithelial Changes in the Breast —Murray 725
change is easily distinguished from clear cell carcinoma,as the latter is usually more extensive and shows mark-edly atypical, enlarged, and hyperchromatic nuclei.
Occasionally, it is the myoepithelium that shows aprominent clear cell change, but it can be recognized be-cause of its location between luminal epithelium and base-ment membrane.
A lobule involved by clear cell changes can mimic atyp-ical lobular hyperplasia or focal lobular carcinoma in situ.The polygonal clear cells, though, are cytologically benign
and tightly cohesive, with sharply defined cell borders,and the acinar lumen is typically preserved. Positive mem- branous immunoreactivity for E-cadherin will decoratethe cells with clear changes, but not lobular carcinoma insitu.
TREATMENT-RELATED CHANGES
Estimates had indicated that more than 182 000 new cas-es of invasive breast cancer and an additional 67 000 casesof carcinoma in situ would require diagnosis and treat-ment in 2008.7 In the modern day and age, treatment of breast carcinoma usually consists of breast-conservingtherapy (BCT), including tumor excision and radiotherapyof the affected breast to eradicate any residual disease.
Studies have demonstrated that the outcome of BCT iscomparable to that of mastectomy.8,9
Both radiation and chemotherapy can induce morpho-logic alterations in the breast epithelium; with the in-creased survival of patients with breast carcinoma, the pa-thologist must be familiar with the histologic changes in-troduced by these therapies. Frequently, patients who un-dergo prior BCT will require a posttreatment biopsy because of new clinically or radiologically detected lesionswithin the breast. This is the most common setting inwhich the pathologist will encounter nonneoplastic epi-thelial atypia secondary to treatment effect.
Chemotherapy
Cytotoxic chemotherapy primarily affects the carcinoma
but it also alters the nonneoplastic breast parenchyma, re-sulting in subtle changes. Following chemotherapy, thenonneoplastic breast parenchyma undergoes diffuse atro-phy, with reduced number of lobules and a decrease insize of those remaining3,10 (Figure 6). Lobular atrophy con-sists of a spectrum of changes ranging from concentricthickening of the basement membrane to almost completefibrous obliteration and sclerosis of the acini. The residualglands are lined by flattened epithelium, but cytomor-phologic alterations may sometimes occur and mimicatypia. The epithelial cells are often enlarged and appearless uniform. The cytoplasm can be vacuolated, granular,clear, or eosinophilic and, occasionally, the degree of vac-uolization can mimic that seen in histiocytes.11,12 Morpho-
logic alterations in the epithelial cells include nucleome-galy, multinucleation, and prominent nucleoli10 (Figure 7).Marked epithelial atypia is not a common finding and oneshould be cautious about interpreting any severe epithelialalteration as secondary to chemotherapy effect in nonneo-plastic epithelium. Morphologic comparison with the un-treated carcinoma is particularly helpful in this situation.
Radiation
The pathologist is often challenged with the difficulttask of evaluating a breast biopsy specimen for a patientwho has previously received radiation therapy. Care is
necessary to avoid overcalling radiation-induced changesas carcinoma because this will result in mastectomy. Onthe other hand, underdiagnosis of recurrent carcinoma asradiation-induced changes will delay appropriate treat-ment of a potentially curable disease.
In the course of radiation for BCT, both neoplastic andnonneoplastic breast tissue receive the same level of ex-posure. Radiation-induced changes are most apparent inthe terminal-duct lobular unit and less pronounced in thelarger ducts.3,13,14 The alterations include fibrosis, lobular
atrophy, collagenization of the intralobular stroma, andthickening of the basement membrane. The epithelial cellsof lobules and terminal ducts show cytologic alterationsthat can mimic atypia, including increased cell size, largepleomorphic nuclei, and often, prominent but small nucle-oli (Figure 8). Irradiated nuclei are sometimes hyperchro-matic but most often show uniform chromatin.15 In radi-ation changes, the cells with enlarged nuclei are scatteredand admixed with benign epithelium. The lobules areatrophic and mitotic activity is absent. Finding of mitoticactivity is suggestive of recurrent malignant disease. Themyoepithelial cells lining the acini tend to be preservedto a greater extent than the luminal cells and may be rel-atively prominent (Figure 9).
Occasionally, fibrosis distorts the terminal-duct lobularunit and obscures the myoepithelium. In lobules severelyaffected by radiation treatment, fibrosis may distort theacini, resulting in a pseudoinfiltrative pattern13 (Figure10). Close attention to the presence of myoepithelial cells,atrophic epithelial changes, and lack of proliferative activ-ity help the pathologist to distinguish this pseudoinfiltra-tive pattern from invasive carcinoma.
Atypical stromal fibroblasts are commonly encounteredin irradiated breast (Figure 11). Nonspecific vascularchanges, such as intimal and myointimal proliferation ofsmall arteries and arterioles, mural hyalinization, andprominence of capillary endothelial cells have also beendescribed.13,15 Fat necrosis and squamous metaplasia arealso frequently encountered in postradiation biopsy spec-
imens14 (Figure 12).The aforementioned changes are typically described in
breast biopsy specimens obtained long after radiotherapy, but occasionally a breast biopsy specimen is obtained inthe course of radiation or shortly after its completion be-cause of suspicious radiologic findings (eg, new or resid-ual calcifications). The epithelial atypia present in earlyposttreatment tends to be severe and diffusely involves the breast epithelium (Figure 13). Severity and extent of thechanges make interpretation of these findings even morechallenging. A very important point to remember is thatthe epithelial changes secondary to radiation do not in-clude mitotic activity. In situ carcinoma persisting afterradiation treatment remains largely intact and the mor-
phology of neoplastic cells in lobules or ducts is not sub-stantially different from that of the untreated tumor.3,16 Re-current carcinoma in irradiated breast has a similar nucle-ar grade as that of the untreated tumor in 84% of cases16
(Figure 14). Therefore, in cases of suspected recurrent orpersistent carcinoma after BCT, comparison of the pre-treatment and posttreatment tissue sample is extremelyhelpful.
Local recurrence tends to appear later in women treatedwith BCT than in those treated with mastectomy. In onereport, for example, the actuarial incidence of local recur-rence was 7%, 14%, and 20% at 5, 10, and 20 years, re-

8/8/2019 Lesiones Mamarias No Neos
http://slidepdf.com/reader/full/lesiones-mamarias-no-neos 5/7
726 Arch Pathol Lab Med—Vol 133, May 2009 Nonneoplastic Epithelial Changes in the Breast —Murray
Figure 6. Chemotherapy-related changes. Atrophy of lobules with decreased number of acini and concentric thickening of the basement mem-brane (hematoxylin-eosin, original magnification 100).
Figure 7. Chemotherapy-related changes. Isolated epithelial cells show enlarged nuclei. Thickening of the basement membrane is evident (he-matoxylin-eosin, original magnification200).
Figure 8. Radiation-induced changes. The epithelial cells have enlarged hyperchromatic nuclei. No mitoses are seen. The myoepithelium is maintained (hematoxylin-eosin, original magnification 400).
Figure 9. Radiation-induced changes. Atrophy of epithelial cells and cytoplasmic clearing in the myoepithelium. A thickened basement membrane surrounds the acini (hematoxylin-eosin, original magnification 400).
Figure 10. Radiation-induced changes. Marked fibrosis induced by radiation can distort a lobule, resulting in a pseudoinfiltrative appearance (hematoxylin-eosin, original magnification100).
Figure 11. Radiation-induced changes. Atypical stromal cells in irradiated breast tissue (hematoxylin-eosin, original magnification 400).

8/8/2019 Lesiones Mamarias No Neos
http://slidepdf.com/reader/full/lesiones-mamarias-no-neos 6/7
Arch Pathol Lab Med—Vol 133, May 2009 Nonneoplastic Epithelial Changes in the Breast —Murray 727
Figure 12. Radiation-induced changes. Squamous metaplasia in ir-radiated breast tissue (hematoxylin-eosin, original magnification200).
Figure 14. Recurrent carcinoma in an irradiated breast. Ductal car-cinoma in situ arising in irradiated breast shows no radiation-induced changes (hematoxylin-eosin, original magnification 200).
Figure 13. Early radiation-induced changes. A and B, Breast biopsy taken within 6 months of radiation treatment. Marked epithelial atypia is present in a lobule and may be mistakenly overinterpreted as residual/recurrent carcinoma with lobular extension. Lack of mitoses and increased cellularity are clues that the process is not neoplastic (hematoxylin-eosin, original magnifications 400).
spectively, after BCT.17 Changes secondary to radiationhave been seen up to 20 years after treatment. One study
showed that the histologic changes induced in the non-neoplastic breast tissue by radiation therapy showed nosignificant progression or improvement during time inter-vals as great as 229 months.13,14 Therefore, the pathologistneeds to be familiar with and watch for radiation-inducedchanges in the nonneoplastic breast tissue even manyyears after treatment.
When faced with epithelial atypia, which may be post-treatment-related, it is necessary to inquire about possibleprior history of BCT; unfortunately, information regardingprior radiation therapy, though extremely important, is notalways provided. Careful search for histologic evidence oftreatment effect in nonepithelial cells can help suggest aprior breast radiation and avoid the overdiagnosing of ep-ithelial changes as ductal carcinoma in situ, even thoughstromal fibrosis alone has been shown to be a poor cor-relate of evidence of treatment-related changes when com-pared with biopsy specimens from nontreated patients.
SUMMARY
The histomorphology of the breast parenchyma varieswith age and is under hormonal influence. Knowledge ofthe physiologic changes that occur in the breast is essentialto distinguish them from pathologic alterations. Treat-ment-related changes secondary to chemotherapy and/orradiation may pose a major diagnostic challenge and theirmisdiagnosis as neoplastic has serious clinical consequenc-es. Because of the success of BCT, pathologists will seeincreasing numbers of postradiation and/or chemothera-py biopsy specimens. Familiarity with the morphologic al-terations of the breast epithelium secondary to treatmenteffect is thus extremely important to avoid misdiagnosisof treatment-induced nonneoplastic changes, which canpersist many years after treatment.
References
1. Longacre TA, Bartow SA. A correlative morphologic study of human breastand endometrium in the menstrual cycle. Am J Surg Pathol. 1986;10(6):382–393.
2. Ramakrishnan R, Khan SA, Badve S. Morphological changes in breast tissuewith menstrual cycle. Mod Pathol. 2002;15(12):1348–1356.

8/8/2019 Lesiones Mamarias No Neos
http://slidepdf.com/reader/full/lesiones-mamarias-no-neos 7/7
728 Arch Pathol Lab Med—Vol 133, May 2009 Nonneoplastic Epithelial Changes in the Breast —Murray
3. Rosen PP. Rosen’s Breast Pathology. 3rd ed. Philadelphia, PA: LippincottWilliams & Wilkins; 2008.
4. Shin SJ, Rosen PP. Pregnancy-like (pseudolactational) hyperplasia: a primarydiagnosis in mammographically detected lesions of the breast and its relationshipto cystic hypersecretory hyperplasia. Am J Surg Pathol. 2000;24(12):1670–1674.
5. Guerry P, Erlandson RA, Rosen PP. Cystic hypersecretory hyperplasia andcystic hypersecretory duct carcinoma of the breast: pathology, therapy, and fol-low-up of 39 patients. Cancer. 1988;61(8):1611–1620.
6. Shin SJ, Rosen PP. Carcinoma arising from preexisting pregnancy-like andcystic hypersecretory hyperplasia lesions of the breast: a clinicopathologic studyof 9 patients. Am J Surg Pathol. 2004;28(6):789–793.
7. American Cancer Society. Surveillance Research: Estimated New CancerCases and Deaths by Sex, US, 2008. http://www.cancer.org/downloads/stt/
CFF2008Table pg4.pdf. Accessed April 1, 2008.8. van Dongen JA, Voogd AC, Fentiman IS, et al. Long-term results of a ran-
domized trial comparing breast-conserving therapy with mastectomy: EuropeanOrganization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst. 2000;92(14):1143–1150.
9. Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a ran-domized study comparing breast-conserving surgery with radical mastectomy forearly breast cancer. N Engl J Med. 2002;347(16):1227–1232.
10. Kennedy S, Merino MJ, Swain SM, Lippman ME. The effects of hormonaland chemotherapy on tumoral and nonneoplastic breast tissue. Hum Pathol.1990;21(2):192–198.
11. Moll UM, Chumas J. Morphologic effects of neoadjuvant chemotherapy inlocally advanced breast cancer. Pathol Res Pract. 1997;193(3):187–196.
12. Aktepe F, Kapucuoglu N, Pak I. The effects of chemotherapy on breastcancer tissue in locally advanced breast cancer. Histopathology. 1996;29(1):63–67.
13. Schnitt SJ, Connolly JL, Harris JR, Cohen RB. Radiation-induced changesin the breast. Hum Pathol. 1984;15(6):545–550.
14. Moore GH, Schiller JE, Moore GK. Radiation-induced histopathologicchanges of the breast: the effects of time. Am J Surg Pathol. 2004;28(1):47–53.
15. Girling AC, Hanby AM, Millis RR. Radiation and other pathological chang-
es in breast tissue after conservation treatment for carcinoma. J Clin Pathol. 1990;43(2):152–156.
16. Millis RR, Pinder SE, Ryder K, Howitt R, Lakhani SR. Grade of recurrentin situ and invasive carcinoma following treatment of pure ductal carcinoma insitu of the breast. Br J Cancer. 2004;90(8):1538–1542.
17. Kurtz JM, Amalric R, Brandone H, et al. Local recurrence after breast-conserving surgery and radiotherapy: frequency, time course, and prognosis. Can-cer. 1989;63(10):1912–1917.