evaluaciÓn de la respuesta imaginolÓgica en hematologÍa...
TRANSCRIPT

DIEGO A. AGUIRRE MD RADIÓLOGO FUNDACIÓN SANTA FE DE BOGOTÁ
EVALUACIÓN DE LA RESPUESTA IMAGINOLÓGICA EN HEMATOLOGÍA
PET/CT-CHESON
OBJETIVOS
| Presentation Title | Presenter Name | Date | Subject | Business Use Only 2
Importancia Estandarización Criterios Seguimiento y Respuesta
Criterios de Respuesta
Estandarización Criterios Seguimiento y Respuesta
Facilita Interpretación de información
Permiten comparación entre estudios
Identificación de terapias mas efectivas
Esencial en Investigaciones Clínicas
En evolución • 1999 – IWG – criterios anatómicos + Galio • 2007 – IHG – PET + Inmunoquímica
| Presentation Title | Presenter Name | Date | Subject | Business Use Only 4
Revised Response Criteria for Malignant LymphomaBruce D. Cheson, Beate Pfistner, Malik E. Juweid, Randy D. Gascoyne, Lena Specht, Sandra J. Horning,Bertrand Coiffier, Richard I. Fisher, Anton Hagenbeek, Emanuele Zucca, Steven T. Rosen, Sigrid Stroobants,T. Andrew Lister, Richard T. Hoppe, Martin Dreyling, Kensei Tobinai, Julie M. Vose, Joseph M. Connors,Massimo Federico, and Volker Diehl
A B S T R A C T
PurposeStandardized response criteria are needed to interpret and compare clinical trials and for approvalof new therapeutic agents by regulatory agencies.
MethodsThe International Working Group response criteria (Cheson et al, J Clin Oncol 17:1244, 1999)were widely adopted, but required reassessment because of identified limitations and theincreased use of [18F]fluorodeoxyglucose-positron emission tomography (PET), immunohisto-chemistry (IHC), and flow cytometry. The International Harmonization Project was convened toprovide updated recommendations.
ResultsNew guidelines are presented incorporating PET, IHC, and flow cytometry for definitions ofresponse in non-Hodgkin’s and Hodgkin’s lymphoma. Standardized definitions of end pointsare provided.
ConclusionWe hope that these guidelines will be adopted widely by study groups, pharmaceutical andbiotechnology companies, and regulatory agencies to facilitate the development of new and moreeffective therapies to improve the outcome of patients with lymphoma.
J Clin Oncol 25:579-586. © 2007 by American Society of Clinical Oncology
INTRODUCTION
Standardized response criteria provide uniform endpoints for clinical trials, allowing for comparisonsamong studies, facilitating the identification of moreeffective therapies, and aiding the approval processfor new agents by regulatory agencies. Before 1999,response criteria for malignant lymphomas variedwidely among study groups and cancer centers withrespect to the size of a normal lymph node, thefrequency of assessment and the time point the re-sponse assessment was made, the methods used toassess response, whether response was assessed pro-spectively or retrospectively, the percentage increaserequired for disease progression, and many otherfactors.1 Even relatively minor differences in the def-inition of normal size of a lymph node can have amajor influence on response rates.2
In 1999, an international working group (IWG)of clinicians, radiologists, and pathologists with exper-tise in the evaluation and management of patients withnon-Hodgkin’s lymphoma (NHL) published guide-lines for response assessment and outcomes measure-ment.1 These recommendations were adopted rapidly
and widely by clinicians and regulatory agencies, andwere used in the approval process for a number of newagents. However, they were subject to considerableinter- and intraobserver variation and recommendedtechnologies, such as gallium scans, are no longer con-sidered state-of-the-art. Several points were subject tomisinterpretation, notably the application of the com-plete remission/unconfirmed (CRu), and the recom-mendations did not include assessment of extranodaldisease. The widespread use of positron emission to-mography (PET) scans and immunohistochemistrywarranted a reassessment of the prior response criteria.Since the Hodgkin’s lymphoma study groups hadadopted these IWG criteria, any new recommenda-tions needed to account for those patients as well. As aresult,anInternationalHarmonizationProjectwasini-tiated by the German Competence Network Malig-nant Lymphoma to develop recommendations thatwere consistent across study groups.3 Subcommitteeswere organized on Response criteria, End Points forClinical Trials, Imaging, Clinical Features, and Pathol-ogy/Biology,andtherecommendationsarereflectedinthis report.
From the Division of Hematology/Oncology, Georgetown UniversityHospital, Washington, DC; University ofCologne, Cologne; Department ofNuclear Medicine, University of Iowa,Iowa City, IA; Department of Pathology,British Columbia Cancer Agency andthe University of British Columbia,Vancouver, British Columbia, Canada;Department of Oncology and Hematol-ogy, Rigshospitalet, CopenhagenUniversity Hospital, Denmark; Divisionof Oncology and Department of Radia-tion Oncology, Stanford University,Stanford, CA; Department of Hematol-ogy, Hospices Civils de Lyon andUniversité Claude Bernard, Lyon,France; James P. Wilmot CancerCenter, University of Rochester, Roch-ester, NY; Academic Medical Center,Department of Hematology, Amster-dam, the Netherlands; Lymphoma Unit,Department of Medical Oncology,Oncology Institute of Southern Switzer-land, Bellinzona, Switzerland; LurieCancer Center, Northwestern Univer-sity, Chicago, IL; Department ofNuclear Medicine, University HospitalGasthuisberg, Leuven, Belgium; CancerResearch UK Medical Oncology Unit, StBartholomew’s Hospital, London,United Kingdom; Department of Medi-cine III, University of Munich, HospitalGrosshadern, Munich, Germany; Hema-tology and Stem Cell TransplantationDivision, National Cancer Center Hospi-tal, Tokyo, Japan; Section of Hematolo-gy/Oncology, University of NebraskaMedical Center, Omaha, NE; and Dipar-timento di Oncologia ed Ematologia,Universita di Modena e Reggio Emilia,Modena, Italy.
Submitted September 18, 2006;accepted December 20, 2006; publishedonline ahead of print at www.jco.org onJanuary 22, 2007.
Authors’ disclosures of potential con-flicts of interest and author contribu-tions are found at the end of thisarticle.
Address reprint requests to Bruce D.Cheson, MD, Georgetown UniversityHospital, 3800 Reservoir Rd NW,Washington, DC 20007; e-mail:[email protected].
© 2007 by American Society of ClinicalOncology
0732-183X/07/2505-579/$20.00
DOI: 10.1200/JCO.2006.09.2403
JOURNAL OF CLINICAL ONCOLOGY S P E C I A L A R T I C L E
VOLUME 25 ! NUMBER 5 ! FEBRUARY 10 2007
579
132.239.1.231Information downloaded from jco.ascopubs.org and provided by at University of Ca San Diego on January 20, 2011 from
Copyright © 2007 American Society of Clinical Oncology. All rights reserved.
Revised Response Criteria for Malignant LymphomaBruce D. Cheson, Beate Pfistner, Malik E. Juweid, Randy D. Gascoyne, Lena Specht, Sandra J. Horning,Bertrand Coiffier, Richard I. Fisher, Anton Hagenbeek, Emanuele Zucca, Steven T. Rosen, Sigrid Stroobants,T. Andrew Lister, Richard T. Hoppe, Martin Dreyling, Kensei Tobinai, Julie M. Vose, Joseph M. Connors,Massimo Federico, and Volker Diehl
A B S T R A C T
PurposeStandardized response criteria are needed to interpret and compare clinical trials and for approvalof new therapeutic agents by regulatory agencies.
MethodsThe International Working Group response criteria (Cheson et al, J Clin Oncol 17:1244, 1999)were widely adopted, but required reassessment because of identified limitations and theincreased use of [18F]fluorodeoxyglucose-positron emission tomography (PET), immunohisto-chemistry (IHC), and flow cytometry. The International Harmonization Project was convened toprovide updated recommendations.
ResultsNew guidelines are presented incorporating PET, IHC, and flow cytometry for definitions ofresponse in non-Hodgkin’s and Hodgkin’s lymphoma. Standardized definitions of end pointsare provided.
ConclusionWe hope that these guidelines will be adopted widely by study groups, pharmaceutical andbiotechnology companies, and regulatory agencies to facilitate the development of new and moreeffective therapies to improve the outcome of patients with lymphoma.
J Clin Oncol 25:579-586. © 2007 by American Society of Clinical Oncology
INTRODUCTION
Standardized response criteria provide uniform endpoints for clinical trials, allowing for comparisonsamong studies, facilitating the identification of moreeffective therapies, and aiding the approval processfor new agents by regulatory agencies. Before 1999,response criteria for malignant lymphomas variedwidely among study groups and cancer centers withrespect to the size of a normal lymph node, thefrequency of assessment and the time point the re-sponse assessment was made, the methods used toassess response, whether response was assessed pro-spectively or retrospectively, the percentage increaserequired for disease progression, and many otherfactors.1 Even relatively minor differences in the def-inition of normal size of a lymph node can have amajor influence on response rates.2
In 1999, an international working group (IWG)of clinicians, radiologists, and pathologists with exper-tise in the evaluation and management of patients withnon-Hodgkin’s lymphoma (NHL) published guide-lines for response assessment and outcomes measure-ment.1 These recommendations were adopted rapidly
and widely by clinicians and regulatory agencies, andwere used in the approval process for a number of newagents. However, they were subject to considerableinter- and intraobserver variation and recommendedtechnologies, such as gallium scans, are no longer con-sidered state-of-the-art. Several points were subject tomisinterpretation, notably the application of the com-plete remission/unconfirmed (CRu), and the recom-mendations did not include assessment of extranodaldisease. The widespread use of positron emission to-mography (PET) scans and immunohistochemistrywarranted a reassessment of the prior response criteria.Since the Hodgkin’s lymphoma study groups hadadopted these IWG criteria, any new recommenda-tions needed to account for those patients as well. As aresult,anInternationalHarmonizationProjectwasini-tiated by the German Competence Network Malig-nant Lymphoma to develop recommendations thatwere consistent across study groups.3 Subcommitteeswere organized on Response criteria, End Points forClinical Trials, Imaging, Clinical Features, and Pathol-ogy/Biology,andtherecommendationsarereflectedinthis report.
From the Division of Hematology/Oncology, Georgetown UniversityHospital, Washington, DC; University ofCologne, Cologne; Department ofNuclear Medicine, University of Iowa,Iowa City, IA; Department of Pathology,British Columbia Cancer Agency andthe University of British Columbia,Vancouver, British Columbia, Canada;Department of Oncology and Hematol-ogy, Rigshospitalet, CopenhagenUniversity Hospital, Denmark; Divisionof Oncology and Department of Radia-tion Oncology, Stanford University,Stanford, CA; Department of Hematol-ogy, Hospices Civils de Lyon andUniversité Claude Bernard, Lyon,France; James P. Wilmot CancerCenter, University of Rochester, Roch-ester, NY; Academic Medical Center,Department of Hematology, Amster-dam, the Netherlands; Lymphoma Unit,Department of Medical Oncology,Oncology Institute of Southern Switzer-land, Bellinzona, Switzerland; LurieCancer Center, Northwestern Univer-sity, Chicago, IL; Department ofNuclear Medicine, University HospitalGasthuisberg, Leuven, Belgium; CancerResearch UK Medical Oncology Unit, StBartholomew’s Hospital, London,United Kingdom; Department of Medi-cine III, University of Munich, HospitalGrosshadern, Munich, Germany; Hema-tology and Stem Cell TransplantationDivision, National Cancer Center Hospi-tal, Tokyo, Japan; Section of Hematolo-gy/Oncology, University of NebraskaMedical Center, Omaha, NE; and Dipar-timento di Oncologia ed Ematologia,Universita di Modena e Reggio Emilia,Modena, Italy.
Submitted September 18, 2006;accepted December 20, 2006; publishedonline ahead of print at www.jco.org onJanuary 22, 2007.
Authors’ disclosures of potential con-flicts of interest and author contribu-tions are found at the end of thisarticle.
Address reprint requests to Bruce D.Cheson, MD, Georgetown UniversityHospital, 3800 Reservoir Rd NW,Washington, DC 20007; e-mail:[email protected].
© 2007 by American Society of ClinicalOncology
0732-183X/07/2505-579/$20.00
DOI: 10.1200/JCO.2006.09.2403
JOURNAL OF CLINICAL ONCOLOGY S P E C I A L A R T I C L E
VOLUME 25 ! NUMBER 5 ! FEBRUARY 10 2007
579
132.239.1.231Information downloaded from jco.ascopubs.org and provided by at University of Ca San Diego on January 20, 2011 from
Copyright © 2007 American Society of Clinical Oncology. All rights reserved.
Report of an Internat ional Workshop to Standard izeResponse Cr iter ia for Non -Hodgk in ’s Lymphomas
By Bruce D. C heson, Sandra J. Horning, Bertrand Coiffier, Margaret A. Shipp, Richard I. Fisher, Joseph M. Connors,T. Andrew Lister, Julie Vose, Antonio G rillo-Lopez, Anton Hagenbeek, Fernando Cabanillas, Donald Klippensten,
Wolfgang Hiddemann, Ronald Castellino, Nancy L. Harris, James O . Armitage, W illiam Carter,Richard Hoppe, and George P. C anellos
Abstract: Standardized guidelines for response as-sessment are needed to ensure comparability amongclinical trials in non-Hodgkin’s lymphomas (NHL). Toachieve this, tw o meetings were convened among UnitedStates and international lymphoma ex perts represent-ing medical hematology / oncology, radiology, radiationoncology, and pathology to review currently used re-sponse definitions and to develop a uniform set ofcriteria for assessing response in clinical trials. Thecriteria that were developed include anatomic defini-tions of response, with normal lymph node size aftertreatment of 1.5 cm in the longest transverse diameterb y computer-assisted tomography scan. A designationof complete response / unconfirmed w as adopted to in-clude patients with a greater than 75% reduction intumor size after therap y but with a residual mass, toinclude patients—especially those with large-cell NHL—w ho ma y not have residual disease. Single-photon
emission computed tomography gallium scans are en-couraged as a valuable adjunct to assessment of pa-tients with large-cell NHL, but such scans require appro-priate ex pertise. Flo w cytometric, cytogenetic, andmolecular studies are not currently included in responsedefinitions. Response rates ma y be the most importantobjective in phase II trials w here the activity of a newagent is important and ma y provide support for ap-proval b y regulator y agencies. Ho wever, the goals ofmost phase III trials are to identify therapies that willprolong the progression-free survival, if not the overallsurvival, of the treated patients. We hope that theseguidelines will serve to improve communication amonginvestigators and comparability among clinical trialsuntil clinically relevant laborator y and imaging studiesare identified and become more widely available.
J Clin O ncol 17:1244-1253. ! 1999 b y AmericanSociety of Clinical O ncology.
STANDARDIZED RESPONSE criteria are essential for
the conduct of clinical research. They facilitate interpre-
tation of data, comparisons of the results among various
clinical trials, and identification of new agents with promis-
ing activity, and provide a framework on which to evaluate
new biologic and immunologic insights into the diseases
being studied. The availability of uniform guidelines ensures
a reliable analysis of comparable patient groups among
studies and acquisition of similar data. Response criteria
have been developed for patients with chronic lymphocytic
leukemia,1,2 acute myelogenous leukemia,3 and Hodgkin’s
disease (HD),4 and criteria are now standardized for solid
tumors.5 In 1987, Dixon et al6 emphasized the need for
uniform reporting of end points in clinical trials of patients
with non-Hodgkin’s lymphomas (NHL); of particular impor-
tance were the complete remission rate, survival, time to
treatment failure, and time to relapse of complete respond-
ers. Their recommendations were met with controversy that
remained unresolved.7 Therefore, although the need for
common reporting was obvious, the precise definitions of
several major end points were neither provided nor uni-
formly adopted. A consequence is that there are currently no
standardized response criteria for patients with NHL.
Recognizing this need, several United States lymphoma
investigators from National Cancer Institute (NCI)–spon-
sored cooperative groups, the NCI, and the pharmaceutical
industry collaborated in an effort to resolve the issues
regarding response assessment in NHL. The result was a pre-
liminary document that was subsequently reviewed and
approved by European lymphoma experts.8,9 Eventually, a
workshop was held at the NCI on February 25 to 26, 1998,
with a subsequent meeting on May 16, 1998, to come to
consensus on a standardized set of guidelines for response
assessment in adult patients with indolent and aggressive NHL.
This report presents the recommendations from the NCI-
sponsored international working group. These represent, to a
From the National Cancer Institute, Bethesda, MD; Stanford Univer-
sity, Palo Alto, CA; Centre Hospitalier Lyon-Sud, Lyon, France;
Dana-Farber Cancer Institute, Boston, MA; Loyola University, May-
wood, IL; British Columbia Cancer Agency, Vancouver, British Colum-
bia, Canada; St. Bartholomew’s Hospital, London, England; University
of Nebraska, Omaha, NE; IDEC Corporation, San Diego, CA; Univer-
siteit Utrecht, Utrecht, the Netherlands; M.D. Anderson Cancer Center,
Houston, TX; Roswell Park Cancer Institute, Buffalo, NY; Klinikum
Großhadern, Munich, Germany; Memorial Sloan-Kettering Cancer
Center, New York, NY; Massachusetts General Hospital, Boston, MA;
and Sharp Memorial Hospital, San Diego, CA.
Submitted October 27, 1998; accepted January 25, 1999.
Address reprint requests to Bruce D. Cheson, MD, National Cancer
Institute, Executive Plaza North, Rm 741, Bethesda, MD 20892; email
! 1999 by American Society of Clinical Oncology.
0732-183X/99/1704/1244
1244 Journal of C linical O ncology, Vol 17, No 4 (April), 1999: pp 1244-1253
132.239.1.231Information downloaded from jco.ascopubs.org and provided by at University of Ca San Diego on March 1, 2013 from
Copyright © 1999 American Society of Clinical Oncology. All rights reserved.
Report of an Internat ional Workshop to Standard izeResponse Cr iter ia for Non -Hodgk in ’s Lymphomas
By Bruce D. C heson, Sandra J. Horning, Bertrand Coiffier, Margaret A. Shipp, Richard I. Fisher, Joseph M. Connors,T. Andrew Lister, Julie Vose, Antonio G rillo-Lopez, Anton Hagenbeek, Fernando Cabanillas, Donald Klippensten,
Wolfgang Hiddemann, Ronald Castellino, Nancy L. Harris, James O . Armitage, W illiam Carter,Richard Hoppe, and George P. C anellos
Abstract: Standardized guidelines for response as-sessment are needed to ensure comparability amongclinical trials in non-Hodgkin’s lymphomas (NHL). Toachieve this, tw o meetings were convened among UnitedStates and international lymphoma ex perts represent-ing medical hematology / oncology, radiology, radiationoncology, and pathology to review currently used re-sponse definitions and to develop a uniform set ofcriteria for assessing response in clinical trials. Thecriteria that were developed include anatomic defini-tions of response, with normal lymph node size aftertreatment of 1.5 cm in the longest transverse diameterb y computer-assisted tomography scan. A designationof complete response / unconfirmed w as adopted to in-clude patients with a greater than 75% reduction intumor size after therap y but with a residual mass, toinclude patients—especially those with large-cell NHL—w ho ma y not have residual disease. Single-photon
emission computed tomography gallium scans are en-couraged as a valuable adjunct to assessment of pa-tients with large-cell NHL, but such scans require appro-priate ex pertise. Flo w cytometric, cytogenetic, andmolecular studies are not currently included in responsedefinitions. Response rates ma y be the most importantobjective in phase II trials w here the activity of a newagent is important and ma y provide support for ap-proval b y regulator y agencies. Ho wever, the goals ofmost phase III trials are to identify therapies that willprolong the progression-free survival, if not the overallsurvival, of the treated patients. We hope that theseguidelines will serve to improve communication amonginvestigators and comparability among clinical trialsuntil clinically relevant laborator y and imaging studiesare identified and become more widely available.
J Clin O ncol 17:1244-1253. ! 1999 b y AmericanSociety of Clinical O ncology.
STANDARDIZED RESPONSE criteria are essential for
the conduct of clinical research. They facilitate interpre-
tation of data, comparisons of the results among various
clinical trials, and identification of new agents with promis-
ing activity, and provide a framework on which to evaluate
new biologic and immunologic insights into the diseases
being studied. The availability of uniform guidelines ensures
a reliable analysis of comparable patient groups among
studies and acquisition of similar data. Response criteria
have been developed for patients with chronic lymphocytic
leukemia,1,2 acute myelogenous leukemia,3 and Hodgkin’s
disease (HD),4 and criteria are now standardized for solid
tumors.5 In 1987, Dixon et al6 emphasized the need for
uniform reporting of end points in clinical trials of patients
with non-Hodgkin’s lymphomas (NHL); of particular impor-
tance were the complete remission rate, survival, time to
treatment failure, and time to relapse of complete respond-
ers. Their recommendations were met with controversy that
remained unresolved.7 Therefore, although the need for
common reporting was obvious, the precise definitions of
several major end points were neither provided nor uni-
formly adopted. A consequence is that there are currently no
standardized response criteria for patients with NHL.
Recognizing this need, several United States lymphoma
investigators from National Cancer Institute (NCI)–spon-
sored cooperative groups, the NCI, and the pharmaceutical
industry collaborated in an effort to resolve the issues
regarding response assessment in NHL. The result was a pre-
liminary document that was subsequently reviewed and
approved by European lymphoma experts.8,9 Eventually, a
workshop was held at the NCI on February 25 to 26, 1998,
with a subsequent meeting on May 16, 1998, to come to
consensus on a standardized set of guidelines for response
assessment in adult patients with indolent and aggressive NHL.
This report presents the recommendations from the NCI-
sponsored international working group. These represent, to a
From the National Cancer Institute, Bethesda, MD; Stanford Univer-
sity, Palo Alto, CA; Centre Hospitalier Lyon-Sud, Lyon, France;
Dana-Farber Cancer Institute, Boston, MA; Loyola University, May-
wood, IL; British Columbia Cancer Agency, Vancouver, British Colum-
bia, Canada; St. Bartholomew’s Hospital, London, England; University
of Nebraska, Omaha, NE; IDEC Corporation, San Diego, CA; Univer-
siteit Utrecht, Utrecht, the Netherlands; M.D. Anderson Cancer Center,
Houston, TX; Roswell Park Cancer Institute, Buffalo, NY; Klinikum
Großhadern, Munich, Germany; Memorial Sloan-Kettering Cancer
Center, New York, NY; Massachusetts General Hospital, Boston, MA;
and Sharp Memorial Hospital, San Diego, CA.
Submitted October 27, 1998; accepted January 25, 1999.
Address reprint requests to Bruce D. Cheson, MD, National Cancer
Institute, Executive Plaza North, Rm 741, Bethesda, MD 20892; email
! 1999 by American Society of Clinical Oncology.
0732-183X/99/1704/1244
1244 Journal of C linical O ncology, Vol 17, No 4 (April), 1999: pp 1244-1253
132.239.1.231Information downloaded from jco.ascopubs.org and provided by at University of Ca San Diego on March 1, 2013 from
Copyright © 1999 American Society of Clinical Oncology. All rights reserved.

5
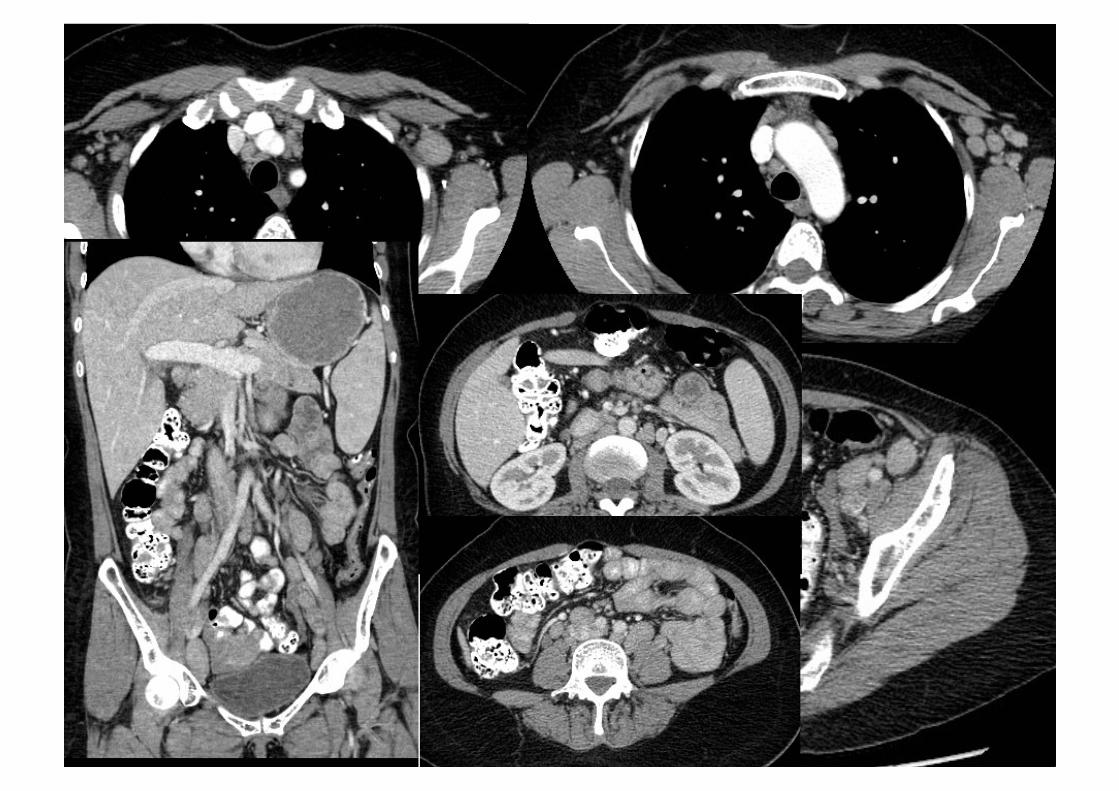
Medición Enfermedad – Ejes
Imágenes Transversales Eje Mayor – Eje Menor
MDCT – 5mms

Tamaño Ganglios
Individuos normales Ganglios < 10 mm en el eje corto
Ganglio > 15mm en el diámetro transverso mayor son considerados anormales
Ganglios entre 10-15mms • Anormales si eje menor > 10mms
Linfoma – compromiso parcial o completo ganglionar
Post- tratamiento los ganglios diminuyen de tamaño pero no desaparecen
En linfoma post- tratamiento hasta 15 mm medido en el eje mayor
Selección de ganglios
Deben ser claramente medibles en al menos dos de sus dimensiones perpendiculares
Medir en regiones diferentes del cuerpo
Incluir ganglios mediastinales y retroperitoneales cuando estén comprometidos
8
PET-CT En linfoma
ESTADIAJE!INICIAL!
EVALUACION!DURANTE EL
TRATAMIENTO!
EVALUACION!DESPUES DEL TRATAMIENTO!

PET-CT Herramienta para estadificación, re-estadificación y
evaluación respuesta de linfomas
Capacidad de diferenciar entre tumor viable, necrosis o fibrosis luego de terapia
Aumenta la capacidad de diferenciar la supervivencia libre de progresión entre remisión completa y respuesta parcial.
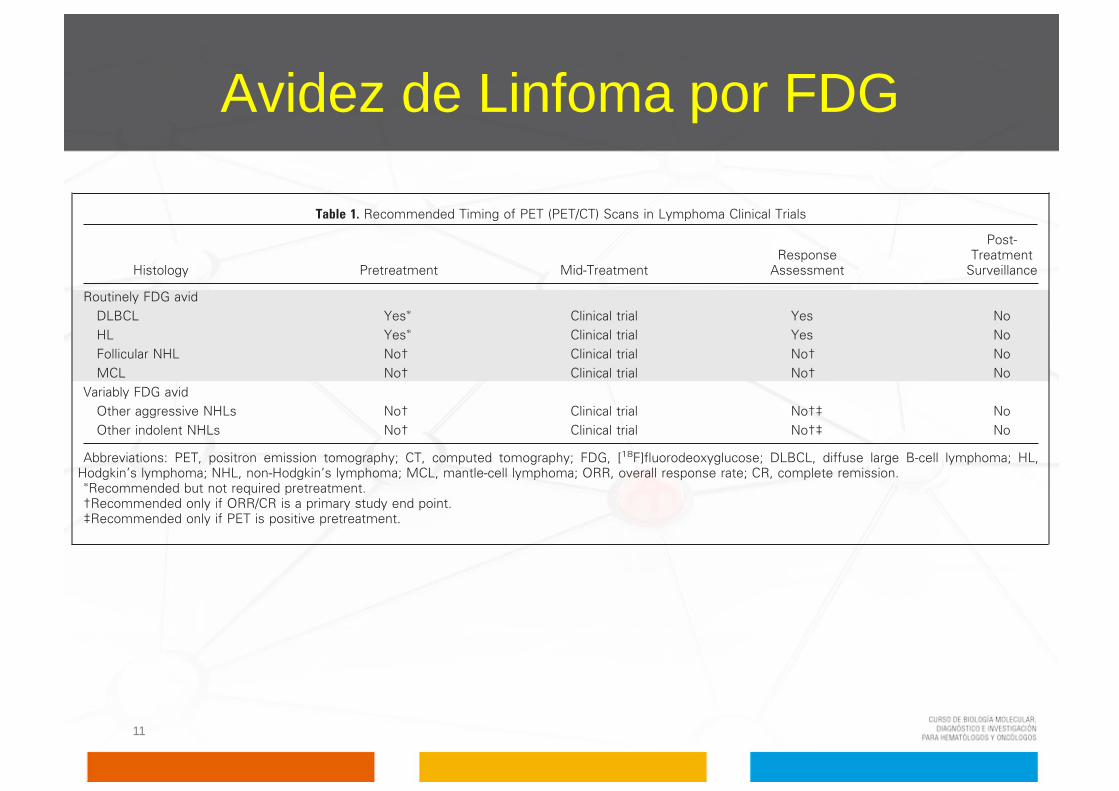
Avidez de Linfoma por FDG
11
MODIFICATIONS OF THE IWG CRITERIA
PETPET using [18F]fluorodeoxyglucose (FDG), has emerged as a
powerful functional imaging tool for staging, restaging, and responseassessment of lymphomas.4-24,25 The advantage of PET over conven-tional imaging techniques such as computed tomography (CT) ormagnetic resonance imaging is its ability to distinguish between viabletumor and necrosis or fibrosis in residual mass(es) often present aftertreatment.9,11,26-28 This information may have important clinical con-sequences. Juweid et al20 evaluated the impact of integrating PET intothe IWG criteria in a retrospective study of 54 patients with diffuselarge B-cell NHL who had been treated with an anthracycline-basedregimen. PET increased the number of complete remission (CR)patients, eliminated the CRu category, and enhanced the ability todiscern the difference in progression-free survival (PFS) between pa-tients experiencing CR and partial remission (PR). Such findingsprovided rationale for incorporating PET into revised criteria.
However, a number of issues with PET need to be considered.The technique for performing and interpreting PET has only re-cently been standardized.29 There is variability among readers andequipment. PET is also associated with false-positive findings dueto rebound thymic hyperplasia, infection, inflammation, sarcoid-osis, or brown fat. Diffusely increased bone marrow uptake is oftenobserved after treatment or administration of hematopoieticgrowth factors.19,29,33,34 There are also false-negative results withPET relating to the resolution of the equipment, technique, andvariability of FDG avidity among histologic subtypes.10,29-32 Theseand other considerations regarding interpretation of PET scanshave recently been addressed.29
Recommendations for the use of PET or PET/CT. Current recom-mendations for the use of PET scans reflect the FDG avidity of thelymphoma subtype, and the relevant end points of the clinical trial(Table 1).
1. PET is strongly recommended before treatment for patientswith routinely FDG-avid, potentially curable lymphomas (eg, diffuselarge B-cell lymphoma [DLBCL], Hodgkin’s lymphoma) to betterdelineate the extent of disease; however, currently it is not mandatedbecause of limitations imposed by cost and availability. For incurable,
routinely FDG-avid, indolent, and aggressive histologies (eg, follicularlymphoma and mantle-cell lymphoma), and for most variably FDG-avid lymphomas, the primary end points for clinical trials generallyinclude PFS, event-free survival, and overall survival. PET is not rec-ommended before treatment unless response rate is a major end pointof the trial.
2. Numerous studies have demonstrated that PET performedafter one to four cycles of multiagent chemotherapy predicts thera-peutic outcome5-7,21,24,35,36; however, no currently available datademonstrate improvement in results by altering treatment based onthis information. Until such data exist, this practice should be re-stricted to clinical trials evaluating PET in this context.
3. PET is essential for the post-treatment assessment of DLBCLand Hodgkin’s lymphoma because a complete response is required fora curative outcome. However, PET is recommended in the other,incurable histologies only if they were PET positive before treatmentand if response rate is a primary end point of a clinical study.
4. Current data are inadequate to recommend routine surveil-lance PET scans after the restaging study.
Timing of PET scans after therapy. Post-therapy inflammatorychanges may persist for up to 2 weeks after chemotherapy alone inlymphoma patients and for up to 2 to 3 months or longer afterradiation therapy or chemotherapy plus radiation. To minimize thefrequency of these potentially confounding interpretation finding,PET scans should not be performed for at least 3 weeks, and preferably6 to 8 weeks, after completion of therapy.29
Definition of a positive PET scan. Visual assessment currently isconsidered adequate for determining whether a PET scan is positive,and use of the standardized uptake value is not necessary.29 A moreextensive description of interpretation of PET scans is provided inthe consensus guidelines of the Imaging Subcommittee.29 In brief,a positive scan is defined as focal or diffuse FDG uptake abovebackground in a location incompatible with normal anatomy orphysiology, without a specific standardized uptake value cutoff.29
Other causes of false-positive scans should be ruled out. Exceptionsinclude mild and diffusely increased FDG uptake at the site ofmoderate- or large-sized masses with an intensity that is lower thanor equal to the mediastinal blood pool, hepatic or splenic nodules1.5 cm with FDG uptake lower than the surrounding liver/spleen
Table 1. Recommended Timing of PET (PET/CT) Scans in Lymphoma Clinical Trials
Histology Pretreatment Mid-TreatmentResponse
Assessment
Post-Treatment
Surveillance
Routinely FDG avidDLBCL Yes! Clinical trial Yes NoHL Yes! Clinical trial Yes NoFollicular NHL No† Clinical trial No† NoMCL No† Clinical trial No† No
Variably FDG avidOther aggressive NHLs No† Clinical trial No†‡ NoOther indolent NHLs No† Clinical trial No†‡ No
Abbreviations: PET, positron emission tomography; CT, computed tomography; FDG, [18F]fluorodeoxyglucose; DLBCL, diffuse large B-cell lymphoma; HL,Hodgkin’s lymphoma; NHL, non-Hodgkin’s lymphoma; MCL, mantle-cell lymphoma; ORR, overall response rate; CR, complete remission.
!Recommended but not required pretreatment.†Recommended only if ORR/CR is a primary study end point.‡Recommended only if PET is positive pretreatment.
Cheson et al
580 JOURNAL OF CLINICAL ONCOLOGY
132.239.1.231Information downloaded from jco.ascopubs.org and provided by at University of Ca San Diego on January 20, 2011 from
Copyright © 2007 American Society of Clinical Oncology. All rights reserved.

Recomendaciones PET-CT
1. Antes del tratamiento en linfomas potencialmente curables (FDG-avid: difuso de células B grandes, Hodgkin)
1. Evaluar extensión
2. Predictor de Respuesta a Terapia – Después de 1 a 4 ciclos de QuimioTx
3. Evaluar Respuesta a Terapia 1. Respuesta completa en FDG-avid 2. Otros linfomas: PET (+) y evaluar respuesta
4. No recomendado como metodo de seguimiento luego de re-estadificación

Linfoma no Hodgkin recaídas mul4ples – quimioterapia Evaluación temprana respuesta quimioterapia 3 ciclos
Evaluación de respuesta durante la terapia

Tiempo Realización PET-CT
Cambios inflamatorios post terapia • Post quimioterapia 2-3 semanas • Post radioterapia 2-3 meses
Realizar PET-CT preferiblemente 6 a 8 semanas post finalización de terapia
De realizarlo antes, al menos después de 3 semanas post terapia
Problemas con PET
Técnica de la realización e interpretación
Variabilidad entre los lectores y los equipos
Falsos positivos
Infecciones e inflamación (adenitis, sarcoidosis, TBC, neumonía, etc.)
Captación fisiológica (grasa parda, sistema urinario, timo, músculo, glándulas salivales, etc.)
Hiperplasia tímica benigna
Hiperreactividad de la médula ósea y bazo debido a factores estimulantes de colonias, sepsis, anemia, etc.

Dificultades
Mediastino
Dificultades
Analisis Ganglios Mediastinales
Dificultades
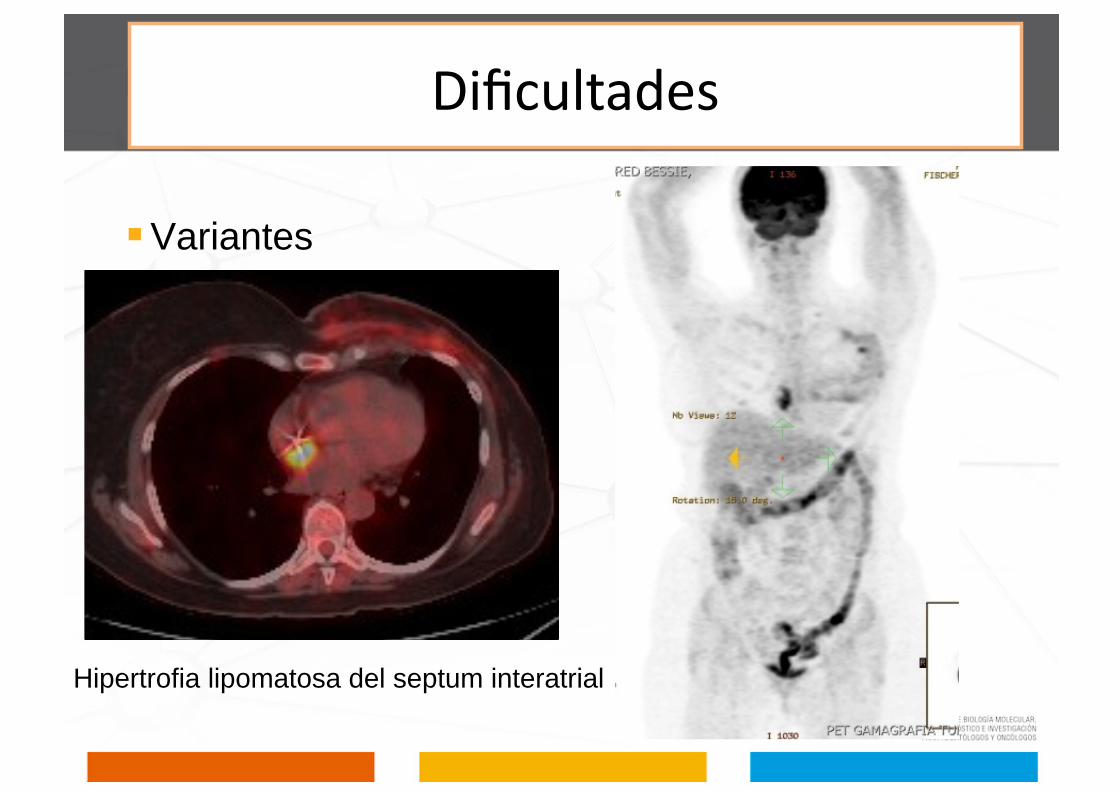
Variantes
Hipertrofia lipomatosa del septum interatrial
Dificultades
Falsos negativos Resolución Anatómica.
• Alrededor de 6-7mms – depende de la localización y características metabólicas del tumor
Variabilidad en la avidez por FDG de los diferentes tipos histológicos de linfomas
Cuando una lesión hipermetabólica está en contacto con un tejido con captación fisiológica como el cerebro o el corazón, presentando un efecto volumen parcial
Hiperglucemia. La glucosa endógena compite con el análogo (FDG). Necesaria glicemia normal o al menos menor a 200 mg/dl.
Cómo se mide la enfermedad
20
Respuesta Completa
Respuesta Parcial
Enfermedad Estable
Recaida o Progresión de Enfermedad
Cómo se mide la enfermedad
21 4. If the bone marrow was involved by lymphoma before treat-
ment, the infiltrate must have cleared on repeat bone marrow biopsy.The biopsy sample on which this determination is made must beadequate (with a goal of ! 20 mm unilateral core). If the sample isindeterminate by morphology, it should be negative by immunohis-tochemistry. A sample that is negative by immunohistochemistry butthat demonstrates a small population of clonal lymphocytes by flowcytometry will be considered a CR until data become available dem-onstrating a clear difference in patient outcome.
CRuThe use of the above definition for CR and that below for PR
eliminates the category of CRu.
PRThe designation of PR requires all of the following:1. At least a 50% decrease in sum of the product of the diameters
(SPD) of up to six of the largest dominant nodes or nodal masses.These nodes or masses should be selected according to all of thefollowing: they should be clearly measurable in at least 2 perpendiculardimensions; if possible they should be from disparate regions of thebody; and they should include mediastinal and retroperitoneal areasof disease whenever these sites are involved.
2. No increase should be observed in the size of other nodes, liver,or spleen.
3. Splenic and hepatic nodules must regress by ! 50% in theirSPD or, for single nodules, in the greatest transverse diameter.
4. With the exception of splenic and hepatic nodules, involve-ment of other organs is usually assessable and no measurable diseaseshould be present.
5. Bone marrow assessment is irrelevant for determination of aPR if the sample was positive before treatment. However, if positive,the cell type should be specified (eg, large-cell lymphoma or smallneoplastic B cells). Patients who achieve a CR by the above criteria, but
who have persistent morphologic bone marrow involvement will beconsidered partial responders.
When the bone marrow was involved before therapy and a clin-ical CR was achieved, but with no bone marrow assessment aftertreatment, patients should be considered partial responders.
6. No new sites of disease should be observed.7. Typically FDG-avid lymphoma: for patients with no pretreat-
ment PET scan or if the PET scan was positive before therapy, thepost-treatment PET should be positive in at least one previously in-volved site.
8. Variably FDG-avid lymphomas/FDG-avidity unknown: forpatients without a pretreatment PET scan, or if a pretreatment PETscan was negative, CT criteria should be used.
In patients with follicular lymphoma or mantle-cell lymphoma, aPET scan is only indicated with one or at most two residual masses thathave regressed by more than 50% on CT; those with more than tworesidual lesions are unlikely to be PET negative and should be consid-ered partial responders.
Stable DiseaseStable disease (SD) is defined as the following:1. A patient is considered to have SD when he or she fails to attain
the criteria needed for a CR or PR, but does not fulfill those forprogressive disease (see Relapsed Disease [after CR]/Progressive Dis-ease [after PR, SD]).
2. Typically FGD-avid lymphomas: the PET should be positive atprior sites of disease with no new areas of involvement on the post-treatment CT or PET.
3. Variably FDG-avid lymphomas/FDG-avidity unknown: forpatients without a pretreatment PET scan or if the pretreatment PETwas negative, there must be no change in the size of the previouslesions on the post-treatment CT scan.
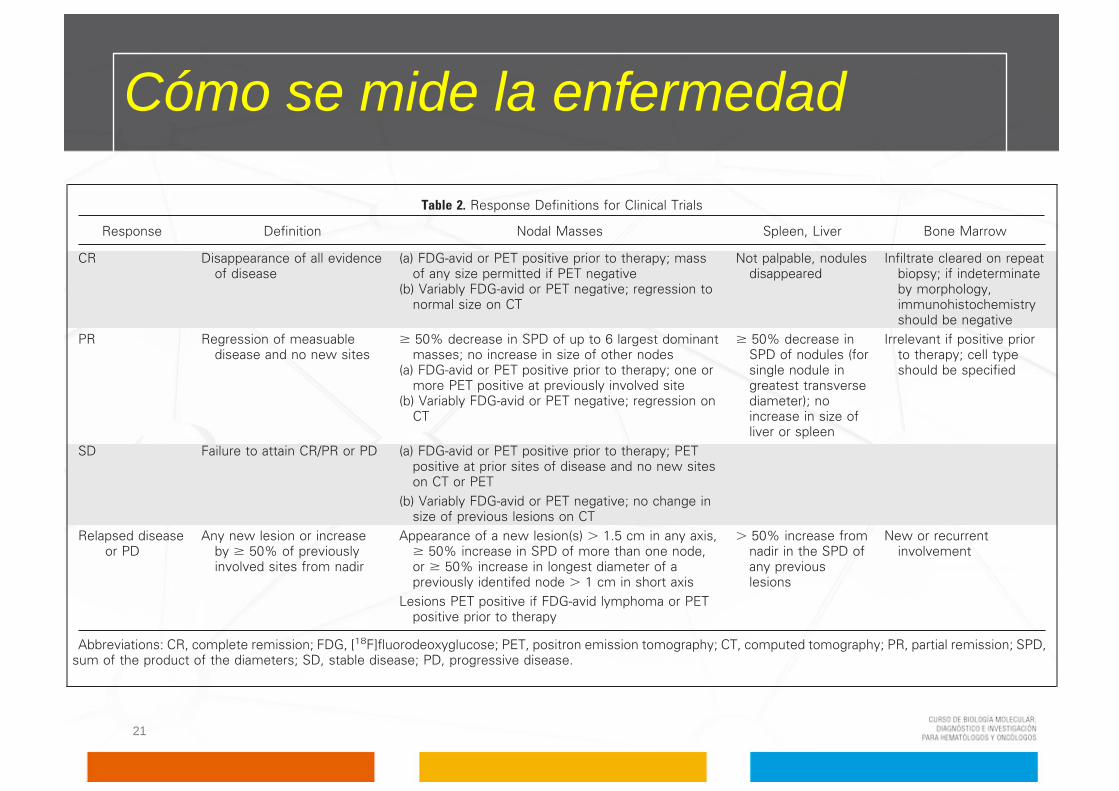
Table 2. Response Definitions for Clinical Trials
Response Definition Nodal Masses Spleen, Liver Bone Marrow
CR Disappearance of all evidenceof disease
(a) FDG-avid or PET positive prior to therapy; massof any size permitted if PET negative
(b) Variably FDG-avid or PET negative; regression tonormal size on CT
Not palpable, nodulesdisappeared
Infiltrate cleared on repeatbiopsy; if indeterminateby morphology,immunohistochemistryshould be negative
PR Regression of measuabledisease and no new sites
! 50% decrease in SPD of up to 6 largest dominantmasses; no increase in size of other nodes
(a) FDG-avid or PET positive prior to therapy; one ormore PET positive at previously involved site
(b) Variably FDG-avid or PET negative; regression onCT
! 50% decrease inSPD of nodules (forsingle nodule ingreatest transversediameter); noincrease in size ofliver or spleen
Irrelevant if positive priorto therapy; cell typeshould be specified
SD Failure to attain CR/PR or PD (a) FDG-avid or PET positive prior to therapy; PETpositive at prior sites of disease and no new siteson CT or PET
(b) Variably FDG-avid or PET negative; no change insize of previous lesions on CT
Relapsed diseaseor PD
Any new lesion or increaseby ! 50% of previouslyinvolved sites from nadir
Appearance of a new lesion(s) ! 1.5 cm in any axis,! 50% increase in SPD of more than one node,or ! 50% increase in longest diameter of apreviously identifed node ! 1 cm in short axis
! 50% increase fromnadir in the SPD ofany previouslesions
New or recurrentinvolvement
Lesions PET positive if FDG-avid lymphoma or PETpositive prior to therapy
Abbreviations: CR, complete remission; FDG, [18F]fluorodeoxyglucose; PET, positron emission tomography; CT, computed tomography; PR, partial remission; SPD,sum of the product of the diameters; SD, stable disease; PD, progressive disease.
Cheson et al
582 JOURNAL OF CLINICAL ONCOLOGY
132.239.1.231Information downloaded from jco.ascopubs.org and provided by at University of Ca San Diego on January 20, 2011 from
Copyright © 2007 American Society of Clinical Oncology. All rights reserved.

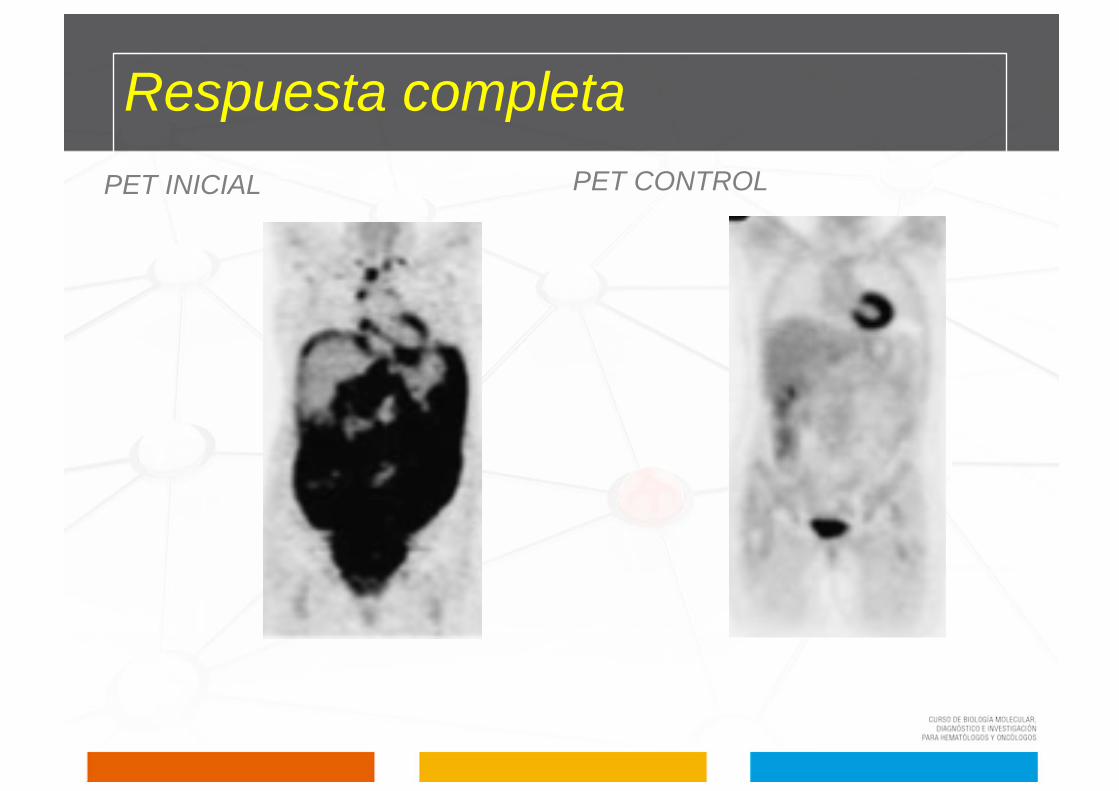
Respuesta completa
1. Desaparición completa de toda evidencia clínica de enfermedad detectable y de los síntomas relacionados con la enfermedad
presentes antes del tratamiento.

Respuesta completa
23
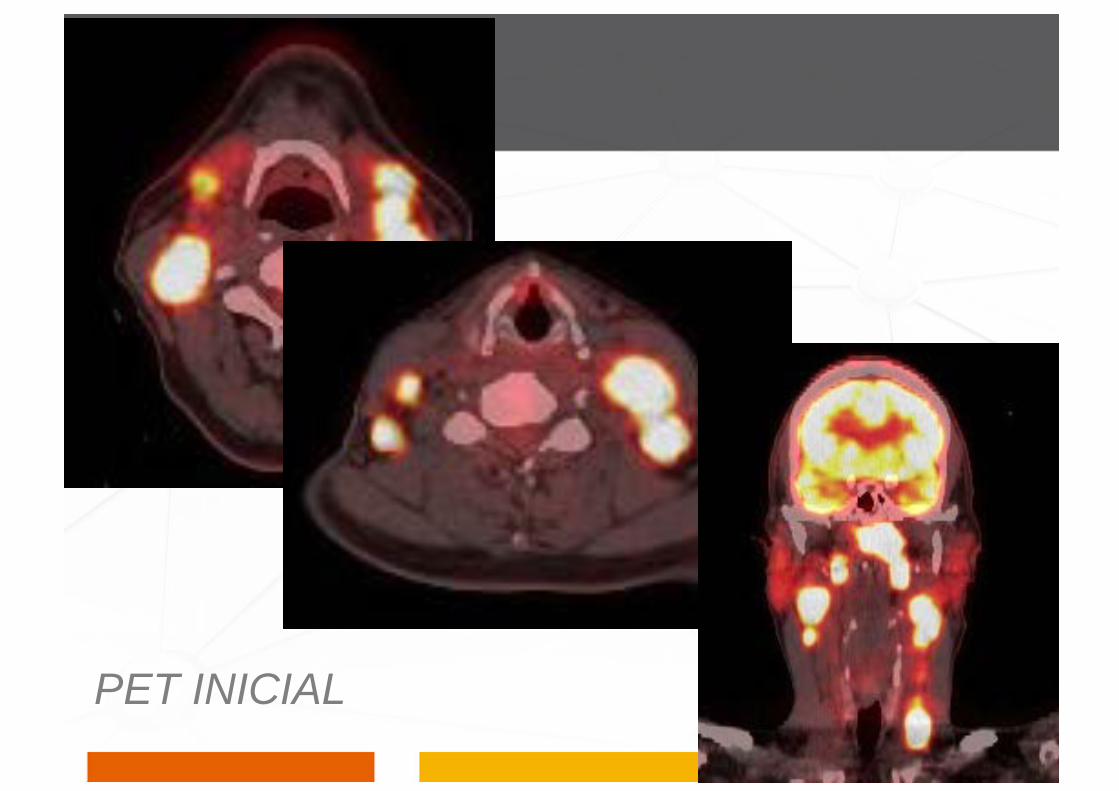
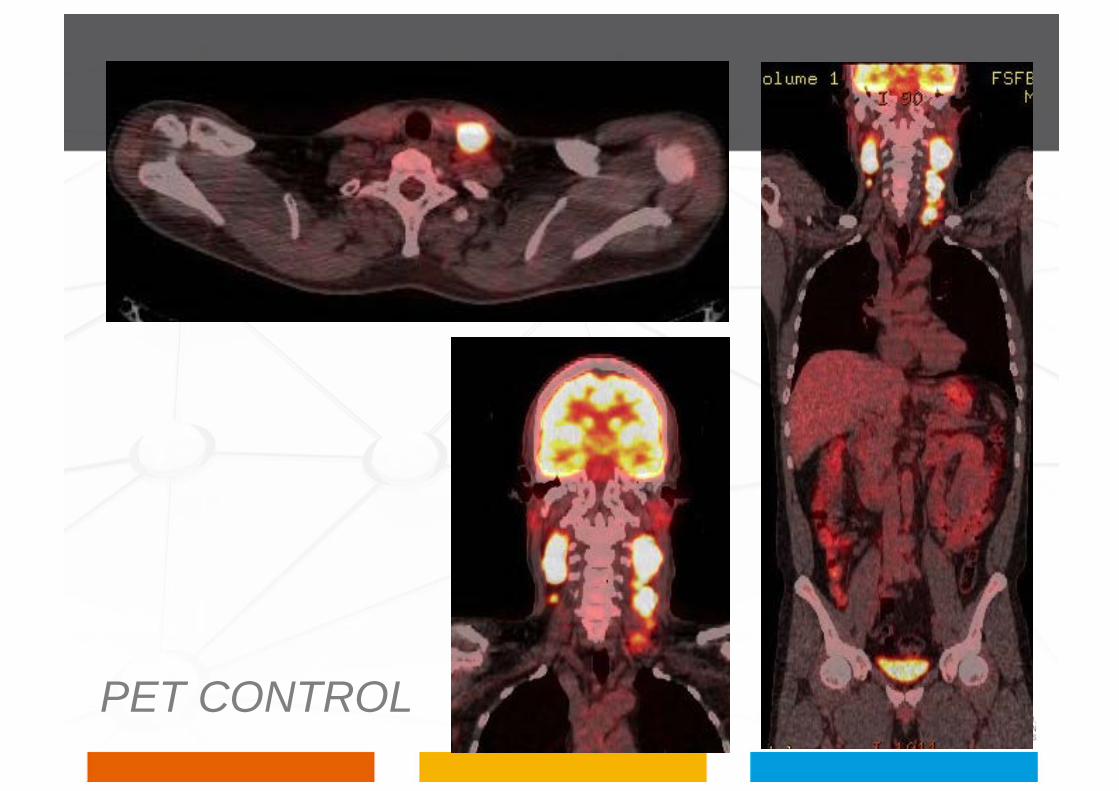
2A. Linfomas ávidos al FDG:
Pacientes con PET pre-tratamiento (+) se permiten masas de cualquier tamaño si PET es negativo.
PET INICIAL
PET CONTROL
Mesotelioma Peritoneal
Respuesta completa
24
2B. Linfomas con avidez variable o desconocida al FDG:
Pacientes sin PET pre-tratamiento o pacientes con PET pre-tratamiento (-), todos los nódulos linfáticos y masas nodales deberán haber regresado a su tamaño normal por CT.

Respuesta Completa – CT
25

Respuesta completa
3. Si hay hepatomegalia o esplenomegalia antes del tratamiento debe regresar a su tamaño y no debe ser palpable clínicamente (hígado, riñones).
4. La médula ósea, si es positiva en el estudio de base, debe ser histológicamente negativa (inmunohistoquímica, citometría de flujo).

27
Respuesta completa

Respuesta completa no confirmada
Categoría eliminada.
Correspondía al periodo entre respuesta completa a respuesta parcial.

Respuesta parcial
Disminución ≥50% en SPD de los 6 nódulos dominantes o masas nodales.
No aumento de otros ganglios, hígado ni bazo.
Nódulos hepáticos y esplénicos deben disminuir ≥50% en la SPD.
Afectación de otros órganos es generalmente valorable y no debe haber enfermedad medible.

Disminucion 82%
Respuesta Parcial
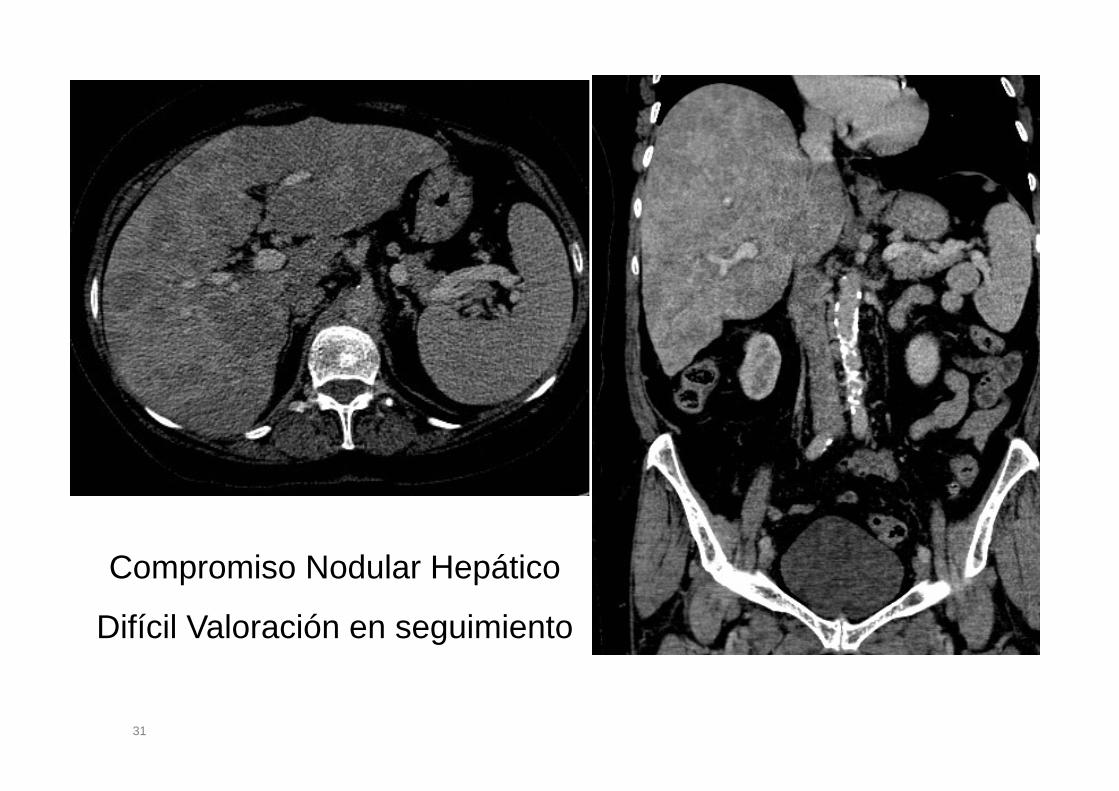
31
Compromiso Nodular Hepático
Difícil Valoración en seguimiento

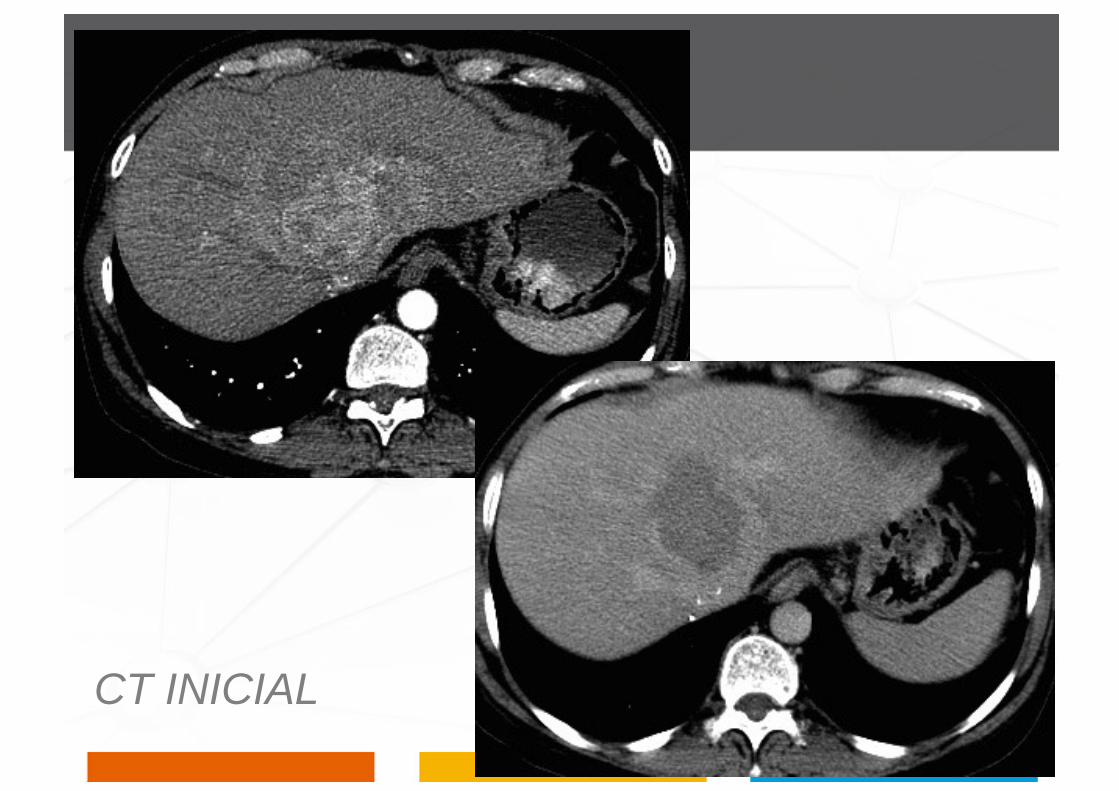
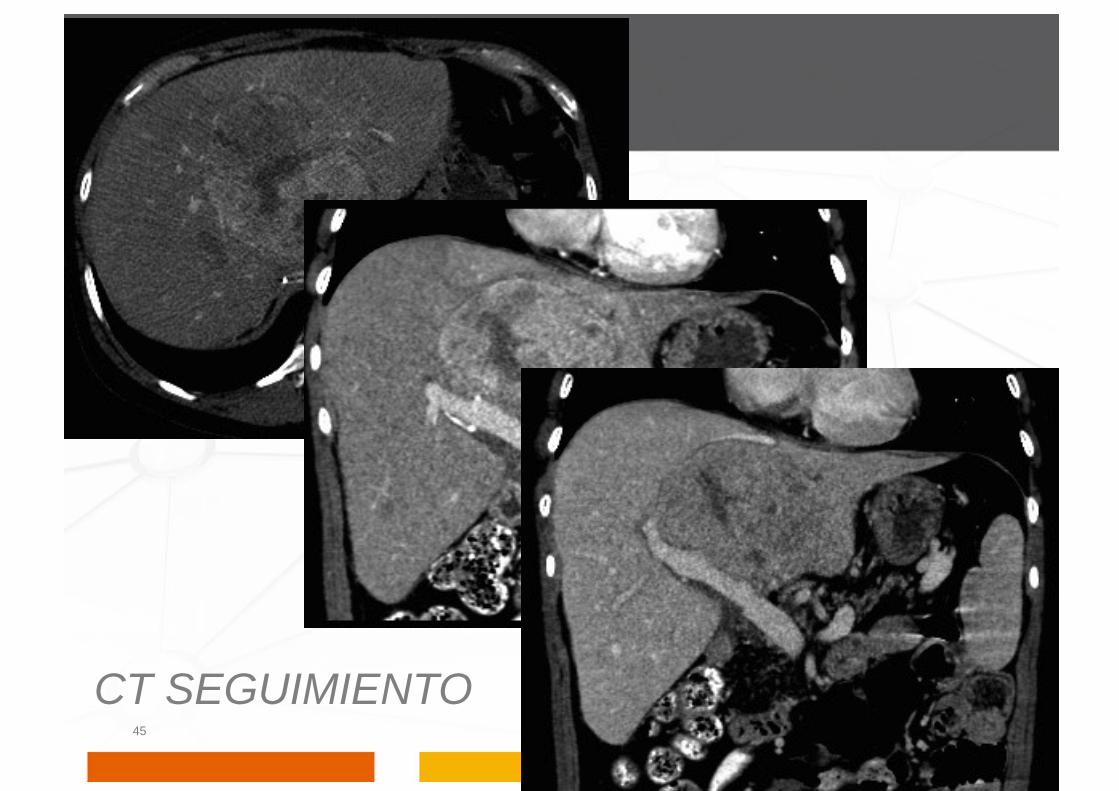
Respuesta parcial
No evidencia de nuevos sitios de enfermedad
Linfomas avidos para FDG: Persistencia de compromiso
Linfomas con avidez variable o no conocida a FDG: se utilizan criterios aplicables a CT.

CT INICIAL

PET INICIAL

CT SEGUIMIENTO
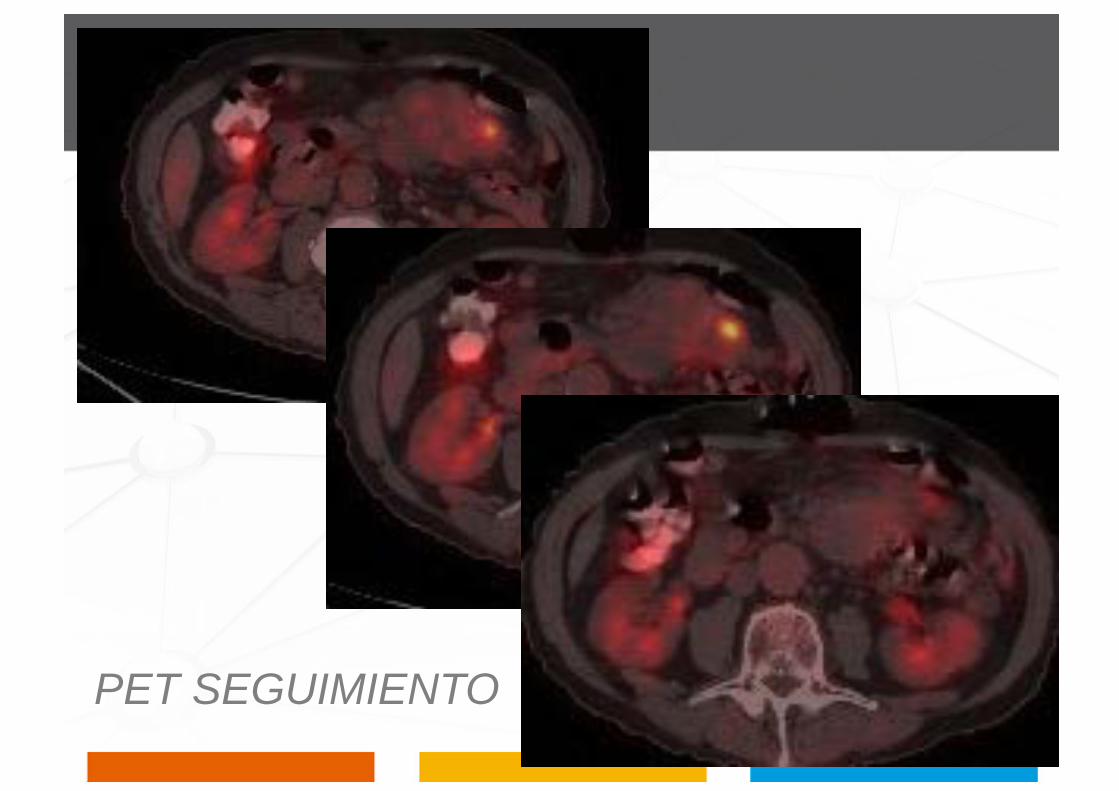
PET SEGUIMIENTO

Enfermedad estable
No cumple los criterios para respuesta completa o respuesta parcial, ni tampoco los criterios para enfermedad en progresión.
Linfomas ávidos FDG: PET positivo, sin nuevas áreas de captación.
Linfomas avidez variable o desconocida FDG: No cambios en el tamaño de lesiones en el CT postratamiento.
No debe haber ningún cambio en el tamaño de los nódulos ni en la captación de los mismos.

CT INICIAL
PET INICIAL

CT CONTROL
PET CONTROL
Aparición de cualquier nueva lesión ≥1.5 cm en cualquiera de los ejes, durante o al final de la terapia, aunque otras lesiones de tamaño.
El de la captación de FDG en área no afectada, solo se considera enfermedad recurrente o en progresión después de confirmar con otras modalidades.
Aumento >50% en el SPD de cualquier ganglio previamente identificado, o en tamaño de otras lesiones (hepáticas / esplénica)
Progresión de la enfermedad Recaida (luego de respuesta completa)
Aumento> 50% en diámetro mayor de un nódulo previamente identificado de mas de 1 cm en eje corto.
Enfermedad extraganglionar medible se debe evaluar similar a la enfermedad nodal.
Enfermedad no medible se registra como presente o ausente (Ej. Derrame pleural).
Progresión de la enfermedad Recaida (luego de respuesta completa)
CT INICIAL
45
CT SEGUIMIENTO

RESUMEN: CRITERIOS DE RESPUESTA Categoria Definicion Ganglios Bazo - Higado Médula Ósea
Respuesta Completa
Desaparición Evidencia Enfermedad
FDG avid / PET (+) – PET Negativo FDG variable o PET (-) –Tamaño normal en CT
No Palpable Desapación de lesiones
Normal en nueva biopsia – Inmuno-histoquímica negativa
Respuesta Parcial
Regresión enfermedad Medible – no nuevo compromiso
≥ 50% disminución SPD lesiones indice (6) sin aumento de lesiones FDG avid / PET (+) – persistencia PET + PET Negativo – regresión CT
Disminución ≥50% SPD nódulos – No megalias
Irrelevante
Enfermedad Estable
Ausencia de RC-RP FDG avid / PET (+) – PET positivo sin nuevo compromiso PET (-) – no cambios en tamaño
Recaída - Progresión
Lesiones nuevas O Aumento ≥50% enfermedad
Aparición nuevas lesiones ≥15mms Aumento ≥50% SPD 1 o mas ganglios Aumento ≥50% diametro mayor de ganglio menor de 10mms eje menor Nuevas lesiones en PET
Aumento ≥50% SPD lesiones
Compromiso nuevo o recurrente

Referencias 1. Drew A. Torigian, Steve S. Huang, Mohamed Houseni and Abass Alavi: Functional Imaging of Cancer with Emphasis on Molecular Techniques. CA Cancer J Clin 2007;57;206-224
2. Hoffman JM, Gambhir S: Molecular Imaging: The Vision and Opportunity for Radiology in the Future. Radiology: 244: 2007
3. Römer W, Hanauske AR, Ziegler S, et al: Positron emission tomography in non Hodgkin’s lymphoma: Assessment of chemotherapy with fluorodeoxyglucose. Blood 91:4464-4471, 1998
4. Hutchings M, Loft A, Hansen M, et al: FDGPET after two cycles of chemotherapy predicts treatment failure and progression-free survival in Hodgkin lymphoma. Blood 107:52-59, 2007
5. PET scans in staging of lymphoma current status Friedberg J. W., Chengazi V. The oncologist 2003; 8: 438-447
6. Schoder H, Noy A, Gonen M, et al. Intensity of 18fluorodeoxyglucose uptake in positron emission tomography distinguishes between indolent and aggressive non-Hodgkin’s lymphoma. J Clin Oncol. 2005;23:4643–4651.
7. Cheson BD, Horning SJ, Coiffier B et al. Report of an International Workshop to standardize response criteria for non-Hodgkin’s lymphoma. J Clin Oncol 1999;17:1244-1253.
8. Juweid ME, Stroobants S, Hoekstra OS et al. Use of positron emission tomography for response assessment of lymhoma: consensus recommendations of the Imagining Subcommittee of the International Harmonization Project in Lymphoma: J Clin Oncol 2007; 25: 571-578
9. Delbeke D, Coleman RE, Guiberteau MJ, et al: Procedure guidelines for tumor imaging with FDGPET/ CT 1.0. J Nucl Med 47:885-894, 2006
10. Guermazi A, Juweid ME, PET poised to alter de current paradigm for response assessment of non Hodgkin´s Lynphoma. The British Journal of Radiology 79 (2006), 365-367
11. Olsen K, Sohi J, Abraham T, Juweid M: Initial validation of standardized qualitative (visual) criteria for FDG-PET assessment of residual masses followinglymphoma therapy. Radiological Society of North America 92nd Scientific Assembly and Annual Meeting Program, 2006, pp 323 (abstr. 55:E23-02)
12. Kostakoglu L. Comparison of FDG PET and Ga-67 in lymphoma. Cancer 2002; 94:879-888
47
Conclusiones
Inmunohistoquímica para evaluación de la médula ósea en el diagnóstico y reclasificación luego de la terapia.
La sensibilidad puede con el uso de páneles de Ac específicos.
Para detección de enfermedad oculta en la médula ósea.
Problemas técnicos impiden su uso general en el momento.

Avidez por FDG en linfomas
Según el tipo histológico presentan variaciones.
• ALTA: Linfomas Hodgkin, linfomas de células difusas tipo B, LNH folicular, Linfoma del manto.
• VARIABLE: MALT, LNH linfocítico de células pequeñas, LH predominio linfocítico, LNH burkitt, Linfoblástico y de células T.
Consideraciones especiales
Precaución en interpretación de biopsias.
Después de terapia para enfermedad residual.
Rituximab puede conducir a falsos (-) por econocimiento o bloqueo de epítopos.
La enfermedad clonal residual puede existir sin evidencia morfológica de linfoma.
Uso de estos métodos diagnósticos deben ser incorporados.
Para determinar su pertinencia y utilidad para dirigir la terapia.
Consideraciones especiales
Respuesta completa PET INICIAL PET CONTROL
Introducción
1999 IWG publicó: Pautas para la evaluación de la respuesta en Linfoma no Hodgkin • Alta variación inter e intraobservador. • Varios puntos fueron puntos de interpretaciones erróneas.
2007 – Pautas revisadas evaluacion respuesta • Incluye PET CT

Indicaciones PET en linfoma
a) Complemento de la estadificación inicial
b) En forma temprana a los 2 a 4 ciclos de quimioterapia.
c) Para su re-estadificación al completar el tratamiento
d) Como seguimiento post Respuesta Completa
e) Como criterio de elegibilidad previo al autotrasplante
f) Como monitoreo temprano de la terapia
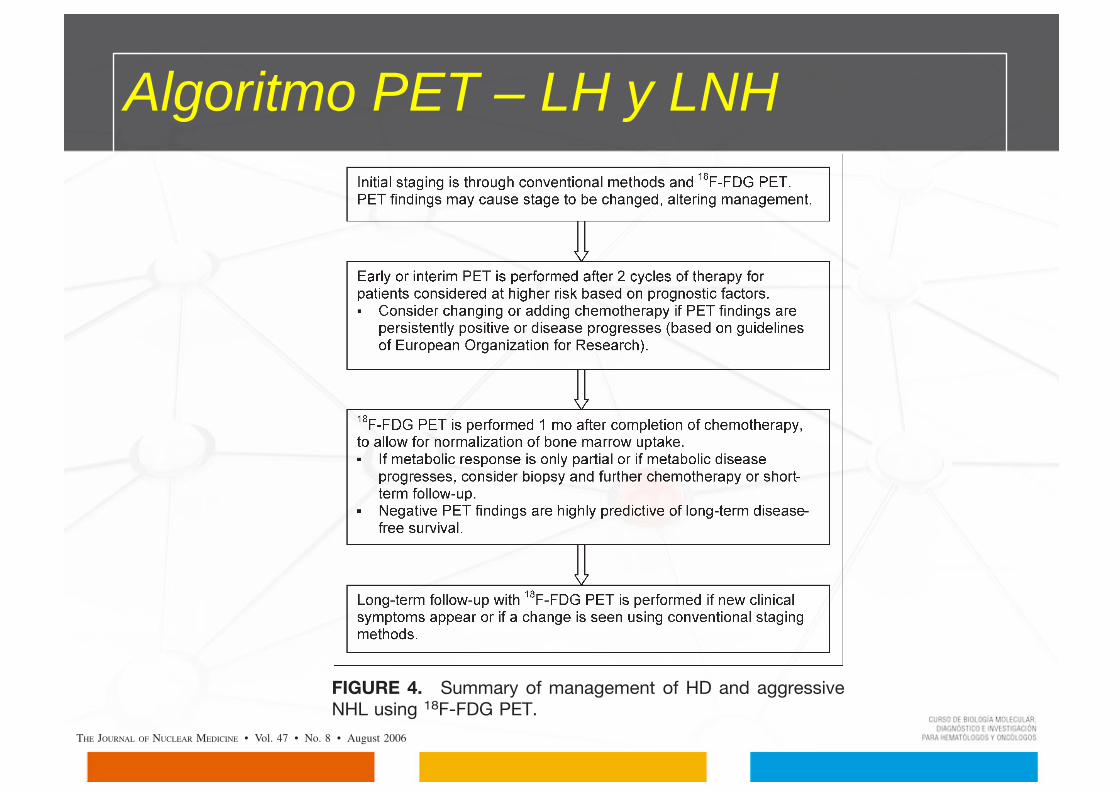
Algoritmo PET – LH y LNH
tumor heterogeneity; and even reconstruction parameters(59). Nevertheless, studies have found measurement of SUVto be consistent: One study that repeated imaging within 10 dshowed the 95% normal range for differences in SUV to beonly 60.9, implying that a change in SUV will be con-sidered significant if the difference is more than 0.9 (60).PET/CT. The widespread use of combined PET/CT
systems offers the potential for more accurate staging with18F-FDG PET. In particular, PET/CT allows accurate spa-tial localization of abnormal radioactivity uptake. Althoughsoftware for merging PET and CT images obtained ondifferent scanners exists, such merging does not alwaysresult in accurately fused images (61). Moreover, combinedPET/CT offers the advantage of maintaining the samepatient positioning on the same bed for both scans. Onestudy compared the reading of side-by-side PET and CTimages with the reading of combined PET/CT images andfollowed the patients for more than 12 mo (62). That studyof only 27 patients demonstrated a sensitivity of 78% forCT alone, 86% for 18F-FDG PET alone, 93% for side-by-side CT and 18F-FDG PET, and 93% for combined PET/CT.This result demonstrates the inherent problem facing com-parisons of PET/CTwith PET alone, in that a careful reviewof functional 18F-FDG images is complete only whencomparable structural (CT or MR) images are reviewed atthe same time. A larger study, of 73 patients, followed upthe patients clinically and through additional imaging andhistology examinations. Discordant results between PETonly and PET/CT were seen in 7 patients, with combinedPET/CT correctly upstaging disease in 2 patients anddownstaging it in 5 patients. PET/CT has been particularlyuseful in decreasing false-positive PET findings, especiallyuptake in brown adipose tissue (28,29). Although uptake inbrown adipose tissue is often symmetric, particularly in theneck and shoulders, proper localization is especially im-portant for areas such as the upper abdomen, where asym-metric uptake may be mistaken for malignancy (30).The CT component is, in most cases, not optimized for
structural imaging but for attenuation correction of the PETimages. The use of CT for attenuation correction (ratherthan a 68Ge or 137Cs transmission source) reduces scanningtime by 40% and also results in virtually noiseless atten-uation correction factors (63,64). Current practice consistsof performing low-dose, unenhanced CT for PET atten-uation and coregistration and, when indicated, separatecontrast-enhanced CT. Because this approach increases thepatient’s exposure to radiation, much attention has beenplaced on the effect of iodinated contrast material on CT-based attenuation correction. Some studies have shown thatPET/CT can be performed with intravenous contrast materialwithout introducing artifacts (65,66), whereas other studiesare investigating whether additional contrast-enhanced CT iseven needed at all in patients with lymphoma (67).Other PET Tracers and Future Directions. Positron-
emitting isotopes of gallium would be a natural choicefor PET, and several are being investigated for use. 68Ga is
convenient because it can be eluted from a germanium–gallium generator, but its short half-life of only 68 min makesit less useful for producing good PET images. 66Ga has alonger half-life (9.5 h) but is difficult to produce in mostcyclotrons. Its longer half-life, however, means that com-mercial manufacturing and distribution would be feasible.
Other 18F-labeled tracers are also under investigation.18F-39-deoxy-39-fluorothymidine (FLT) is a marker of cel-lular proliferation that is currently being investigated as analternative to 18F-FDG PET. Although the bone marrowuptake of 18F-FLT may reduce its sensitivity, initial studieshave demonstrated promise in imaging NHL (68,69). Thesestudies, of only a few patients, have shown comparable re-sults between 18F-FLT and 18F-FDG PET. One perceivedadvantage of 18F-FLT PET is that it does not accumulatein areas of inflammation (which can be common in thisparticular patient population after radiation or infection)and may thus reduce the false-positive rate.
CONCLUSION
Although CT remains the gold standard for the stagingand follow-up of malignant lymphomas, 18F-FDG PET hasa potential role in accurately staging disease and inpredicting response to therapy. This role has the potentialto affect both the initial choice of chemotherapy and thedecision to alter management based on the initial responseto therapy (Fig. 4). PET performed early in a chemother-apeutic regimen has demonstrated a role in identifyingpatients who will experience relapse and may requirefurther treatment, but attention to the timing of the scanin relation to chemotherapy and growth factors is crucial.Many studies have used subjective grading systems to
FIGURE 4. Summary of management of HD and aggressiveNHL using 18F-FDG PET.
1332 THE JOURNAL OF NUCLEAR MEDICINE • Vol. 47 • No. 8 • August 2006
tumor heterogeneity; and even reconstruction parameters(59). Nevertheless, studies have found measurement of SUVto be consistent: One study that repeated imaging within 10 dshowed the 95% normal range for differences in SUV to beonly 60.9, implying that a change in SUV will be con-sidered significant if the difference is more than 0.9 (60).PET/CT. The widespread use of combined PET/CT
systems offers the potential for more accurate staging with18F-FDG PET. In particular, PET/CT allows accurate spa-tial localization of abnormal radioactivity uptake. Althoughsoftware for merging PET and CT images obtained ondifferent scanners exists, such merging does not alwaysresult in accurately fused images (61). Moreover, combinedPET/CT offers the advantage of maintaining the samepatient positioning on the same bed for both scans. Onestudy compared the reading of side-by-side PET and CTimages with the reading of combined PET/CT images andfollowed the patients for more than 12 mo (62). That studyof only 27 patients demonstrated a sensitivity of 78% forCT alone, 86% for 18F-FDG PET alone, 93% for side-by-side CT and 18F-FDG PET, and 93% for combined PET/CT.This result demonstrates the inherent problem facing com-parisons of PET/CTwith PET alone, in that a careful reviewof functional 18F-FDG images is complete only whencomparable structural (CT or MR) images are reviewed atthe same time. A larger study, of 73 patients, followed upthe patients clinically and through additional imaging andhistology examinations. Discordant results between PETonly and PET/CT were seen in 7 patients, with combinedPET/CT correctly upstaging disease in 2 patients anddownstaging it in 5 patients. PET/CT has been particularlyuseful in decreasing false-positive PET findings, especiallyuptake in brown adipose tissue (28,29). Although uptake inbrown adipose tissue is often symmetric, particularly in theneck and shoulders, proper localization is especially im-portant for areas such as the upper abdomen, where asym-metric uptake may be mistaken for malignancy (30).The CT component is, in most cases, not optimized for
structural imaging but for attenuation correction of the PETimages. The use of CT for attenuation correction (ratherthan a 68Ge or 137Cs transmission source) reduces scanningtime by 40% and also results in virtually noiseless atten-uation correction factors (63,64). Current practice consistsof performing low-dose, unenhanced CT for PET atten-uation and coregistration and, when indicated, separatecontrast-enhanced CT. Because this approach increases thepatient’s exposure to radiation, much attention has beenplaced on the effect of iodinated contrast material on CT-based attenuation correction. Some studies have shown thatPET/CT can be performed with intravenous contrast materialwithout introducing artifacts (65,66), whereas other studiesare investigating whether additional contrast-enhanced CT iseven needed at all in patients with lymphoma (67).Other PET Tracers and Future Directions. Positron-
emitting isotopes of gallium would be a natural choicefor PET, and several are being investigated for use. 68Ga is
convenient because it can be eluted from a germanium–gallium generator, but its short half-life of only 68 min makesit less useful for producing good PET images. 66Ga has alonger half-life (9.5 h) but is difficult to produce in mostcyclotrons. Its longer half-life, however, means that com-mercial manufacturing and distribution would be feasible.
Other 18F-labeled tracers are also under investigation.18F-39-deoxy-39-fluorothymidine (FLT) is a marker of cel-lular proliferation that is currently being investigated as analternative to 18F-FDG PET. Although the bone marrowuptake of 18F-FLT may reduce its sensitivity, initial studieshave demonstrated promise in imaging NHL (68,69). Thesestudies, of only a few patients, have shown comparable re-sults between 18F-FLT and 18F-FDG PET. One perceivedadvantage of 18F-FLT PET is that it does not accumulatein areas of inflammation (which can be common in thisparticular patient population after radiation or infection)and may thus reduce the false-positive rate.
CONCLUSION
Although CT remains the gold standard for the stagingand follow-up of malignant lymphomas, 18F-FDG PET hasa potential role in accurately staging disease and inpredicting response to therapy. This role has the potentialto affect both the initial choice of chemotherapy and thedecision to alter management based on the initial responseto therapy (Fig. 4). PET performed early in a chemother-apeutic regimen has demonstrated a role in identifyingpatients who will experience relapse and may requirefurther treatment, but attention to the timing of the scanin relation to chemotherapy and growth factors is crucial.Many studies have used subjective grading systems to
FIGURE 4. Summary of management of HD and aggressiveNHL using 18F-FDG PET.
1332 THE JOURNAL OF NUCLEAR MEDICINE • Vol. 47 • No. 8 • August 2006

57
Se consideran nódulos linfáticos patológicos si su eje mayor es superior a 1,5 cm. independientemente de su eje menor.
Si un nódulo linfático tiene un eje mayor entre 1,1 y 1,5 cm., se debe considerar patológico únicamente si su eje menor es mayor de 1 cm.
Los nódulos linfáticos ≤1,0 cm. x ≤1,0 cm. no se consideran como anormales para criterios de recaída o progresión.
Progresión de la enfermedad o Recaida (luego de respuesta completa)