un grito en la noche: una complicacion no descrita de saos
TRANSCRIPT
1
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
Dr. Josep Morera 29 noviembre 2016

2
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS

3
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
GUIÓN 1.-‐ Introducción 2.-‐ Presentación de Caso Clínico 3.-‐ Opinión de los Asistentes 4.-‐ DiagnósQco 5.-‐ RaQonale y Discusión 6.-‐ Conclusiones

4
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
NEJM 26 Oct. 1923

5
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
6
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS

7
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS

8
Presentación del Caso Clínico F.H.P. (30-‐10-‐2012) -‐ Varón de 67 años -‐ No fumador -‐ Jubilado. Trabajó como comercial de una FARMA de veterinaria -‐ Sedentario -‐ HepaJJs a los 4 años -‐ Adenoidectomia a los 6 años y apendicetomía a los 22 años -‐ Antecedentes de algunos análisis con hiperglicemia sin diagnósJco definiJvo de diabetes -‐ Acudió a nuestra consulta de neumología porque tres días antes, mientras dormía, despertó por dolor torácico intenso brusco, en hemitórax I. Fue atendido en el Servicio de Urgencias del Hospital CIMA. -‐ En Urgencias las constantes fueron normales, la RX de tórax fue normal, el ECG fue normal. La analíJca que incluyó CPK y Troponina fue normal. -‐ Estuvo en observación durante unas horas, se le administró tratamiento analgésico. -‐ Vista la evolución fue dado de alta con el diagnósJco de dolor torácico y la indicación de acudir a consultas externas de neumología.
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS

9
Presentación del Caso Clínico
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS

10
Presentación del Caso Clínico La exploración en la consulta fue relaQvamente anodina: -‐ Altura 1.72m -‐ Peso 80 Kg -‐ IMC 28.39 (sobrepeso) -‐ Distribución troncular de la grasa -‐ Auscultación respiratoria y cardíaca normal -‐ Sat. O2 de 97%. Fr cardíaca 72 -‐ No edemas -‐ Flacidez palpebral -‐ No adenopagas, no organomegálias. -‐ Presión sobre pared costal izquierda dolorosa
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
11
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
DiagnósQco diferencial de dolor torácico: Origen cardio-‐vascular: Ángor/infarto de miocardio Disección de aorta Angina de Prinzmetal/ S. de Takotsubo PericardiJs Necrosis de grasa pericárdica Otros Origen respiratorio: Neumonía/pleuriJs aguda Infarto pulmonar Neumotórax/NeumomediasJno Neoplasia pulmonar Mesotelioma /Tumor de Pancoast Otros
Presentación del Caso Clínico

12
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
DiagnósQco diferencial de dolor torácico: Origen pared torácica: Fractura costal/fisura costal Metástasis costal/tumores primiJvos Síndrome de Tietze Enfermedad de Mondor Roturas fibrilares musculares/hematoma Herpes Zoster Otros Origen otras localizaciones: Meteorismo abdominal Enfermedad de Bornholm Espasmo esofágico/Boerhaave Hernia discal dorsal Otros
Presentación del Caso Clínico

13
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
Opinión de los Asistentes
14
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
Opinión de los Asistentes
15
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
Opinión de los Asistentes
1.-‐ Cuál cree que es el diagnósQco más probable? 2.-‐ Qué dos exploraciones pediría?

16
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
DiagnósQco
17
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS DiagnósQco

18
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS

19
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
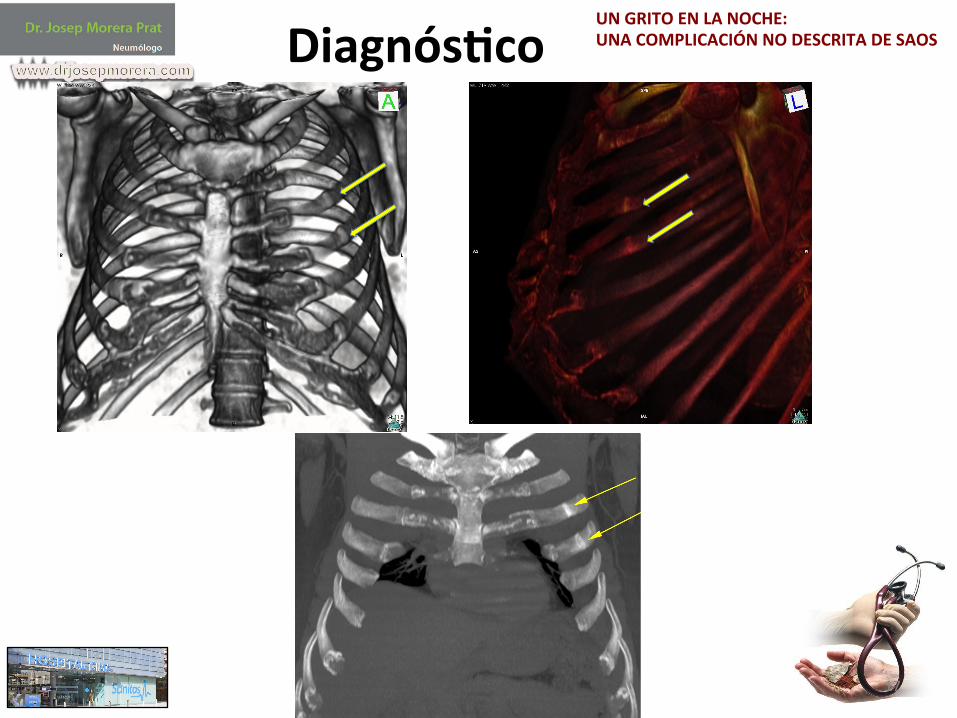
DiagnósQco Fisuras/fracturas costales por estrés secundaria a esfuerzos repeJdos para“vencer apnea”durante la noche Síndrome de Apnea ObstrucQva de grado severo

20
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
RaQonale y Discusión Pistas:
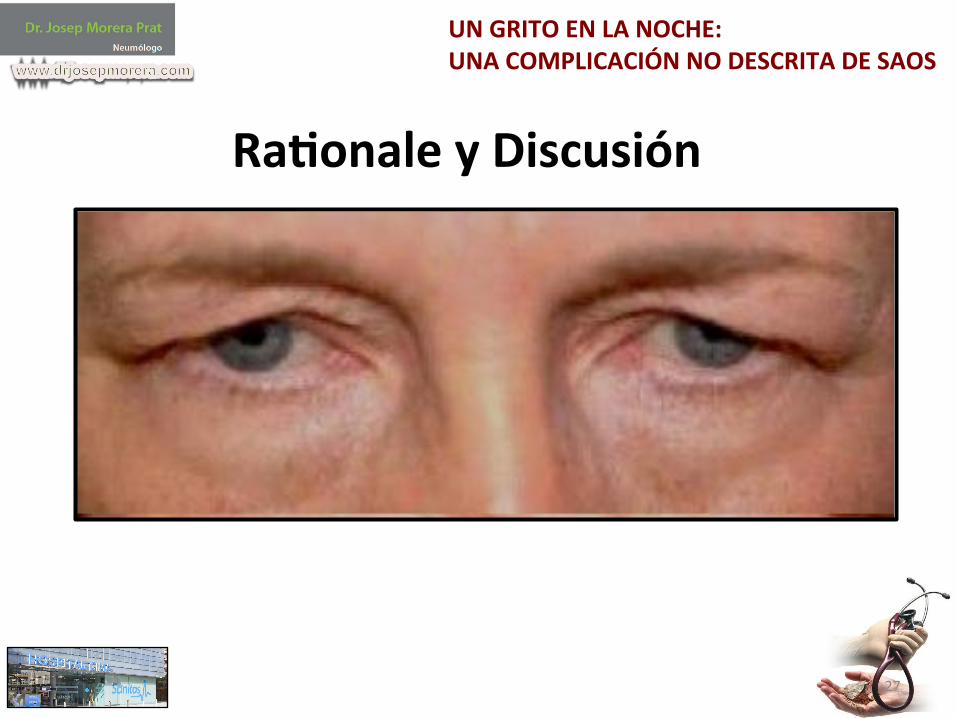
1. Episodio nocturno 2. Descartados angor e infarto, pleuriJs y pericardiJs 3. Dolor a la presión torácica local 4. Signo del párpado flácido(floppy eyelid) 5. IMC de 28.39 con distribución de grasa troncular 6.Conocimiento del mecanismo de presión negaJva intratorácica en apnea prolongada

21
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
RaQonale y Discusión

22
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS RaQonale y Discusión

23
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
RaQonale y Discusión
1530 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003
similar age (56.4 [15.0] vs. 59.6 [14], p ! NS), years of arterialhypertension evolution (6.2 [7.6] vs. 6.1 [6.4], p ! NS), numberof hypertensive drugs (2.4 [1] vs. 2.1 [0.9], p ! NS), and yearsof snoring (18.8 [6.7] vs. 20 [14.1], p ! NS).
In the last imaging test performed before the sleep study,persistence of the aortic dissection was observed in 6 of the 10patients treated surgically and in all of those in whom surgerywas not performed. Four patients were considered to show pro-gression of their aortic disease: one with type A and three withtype B dissections. The latter three presented severe OSAS:Two showed progressive aortic dilation, and one presented evo-lution to dissection of an intramural hematoma.
DISCUSSION
The results of this study show an association between thoracicaortic dissection and OSAS. In particular, a higher AHI wasfound in patients with aortic dissection compared with a controlgroup of hypertensive patients.
Arterial hypertension is the main known risk factor for aorticdissection, and previous studies showed a high prevalence ofOSAS in hypertensive patients referred to a hypertension unit(12–14), which could justify our findings in a group of patientswith aortic dissection. However, the AHI found in our dissectionpatients, with seven suffering more than 30 apneas–hypopneasper hour of sleep, is higher than that previously reported inhypertensive patients. Furthermore, it was significantly higherthan that of a control group of hypertensive patients of similarsex, age, body mass index, and upper body obesity, all knownrisk factors for the development of OSAS (19–21). Isaksson andSvanborg (22) affirmed that OSAS is more common in patientswith poorly controlled hypertension, although this was not en-countered by other authors (14). However, apart from an AHIhigher than that reported by these authors, the aortic dissectionpatients in our study presented arterial hypertension of a numberof years of known evolution, number of drugs required for itscontrol, and blood pressure values on the day of the sleep studysimilar to those of the control group. Antihypertensive treatmentdiffered slightly between groups, and the frequency of "-blockers,a type of medication that some authors have suggested mightworsen OSAS (23), was somewhat higher in the group of patientswith dissection. However, this adverse effect has not been con-firmed in studies comparing the effects of "-blockers and placebo(24) or other antihypertensive drugs (25).
These facts raise the hypothesis that OSAS, besides favoringthe presence of arterial hypertension, could be a contributingfactor to dissection in some patients through the mechanicalstress on the aorta wall caused by repeated episodes of apneaand hypopnea. Inspiratory efforts against an occluded upperairway determine progressively negative intrathoracic pressures,which reach final mean peak values of approximately #60 cmH2O (8, 26). These negative pressures are transmitted to allintrathoracic structures and have been related to worsening ofleft ventricle function (27) and gastroesophageal reflux (28). Inan animal model, Peters and colleagues (29, 30) observed anincrease in systolic and diastolic aortic diameters during obstruc-tive apnea episodes. In parallel to this development of progres-sively negative intrathoracic pressures, a marked increase insympathetic activity and blood pressure is produced during ap-neas, which at the end of the obstructive event may doublethe basal systolic values (9, 31, 32). Upper airway obstructiveepisodes during sleep are known to be frequently asymptomatic(2) and may have been evolving for years before being clinicallydetected. Thus, it could be speculated that in our patients, thesudden rises in the transmural pressure of the aortic wall, re-
peated hundreds of times nightly over years, could have contrib-uted to dissection of the aortic wall, already weakened by factorssuch as diabetes, dyslipemia, or smoking. Apart from by thisincrease in the sheer forces, OSAS could contribute to this weak-ening of the aorta wall because various mechanisms have beensuggested relating it to arteriosclerosis development (33–35) andan increase in intima-media thickness of great arteries has beendemonstrated in OSAS patients (36).
Our study has several limitations. The sleep study was con-ducted several months after the aortic dissection had been diag-nosed; however, we believe that such a short period of time,together with the absence of significant changes in weight, sug-gests that the detected sleep-disordered breathing was presentat the time of the dissection. Furthermore, a case-control studydoes not permit us to elucidate whether OSAS is a risk factorfor aortic dissection. Although the main known variables forthe development of both entities had been controlled, otherconfounding factors may have existed to influence our results.A complementary alternative approach to our study would beto include OSAS as a prognostic variable in follow-up studies,including a greater number of patients with aortic dissection.
Despite these limitations, we believe that our findings mayhave repercussions on the management of these patients. Treat-ment of OSAS with nasal continuous positive airway pressureprevents obstructive episodes of the upper airway and, conse-quently, the development of intrathoracic negative pressures(26), sympathetic discharges, and their associated rise in bloodpressure (9, 37, 38), all of which are desirable in the aorticdissection patient. Furthermore, it has been demonstrated thatantihypertensive medication does not achieve optimum controlof blood pressure in hypertensive OSAS patients (25, 39), whichis achieved when nasal continuous positive airway pressure isadded (40). Although this study was not oriented toward as-sessing the evolution of patients with dissection, despite theshortness of follow-up, three of the four patients who showedaortic disease progression presented severe OSAS.
Thoracic aorta dissection frequently requires surgical treat-ment. OSAS is known to be associated with an increase in periop-erative morbidity and mortality (41, 42) because of a rise in thefrequency and duration of upper airway obstructive episodescaused by the use of analgesics, sedatives, and anesthetics (43).This may be particularly important in patients with aortic dissec-tion and OSAS undergoing surgery in whom, in addition to compli-cations secondary to OSAS per se, rises in transmural pressureduring upper airway obstructive episodes may have a particularlyadverse effect on the recently surgically repaired thoracic aorta.Because the anesthetic and postoperative management of thesepatients with OSAS benefits from specific measures (44, 45), webelieve that the early detection of OSAS could contribute to betterperioperative management of these patients.
Our results indicate the need to assess the presence of symp-toms suggestive of OSAS in patients with thoracic aorta dissec-tion. Given the relative absence of sleepiness detected and thelack of specificity of other symptoms such as snoring, we believethat their presence should be additionally studied by simplescreening tests such as nocturnal pulsioxymetry or a limited sleepstudy and, when the patient is stable, with full polysomnography.
In summary, in this study, a high mean AHI was found inpatients with thoracic aorta dissection. We speculate that thecoexistence of OSAS may impose an additional risk of aorticdissection in predisposed patients or determine worse evolutionbecause of the increase in aortic transmural pressure implied.Because effective treatment for OSAS is available, we believeits diagnosis should be considered in the overall assessment ofpatients with aortic dissection.
1530 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003
similar age (56.4 [15.0] vs. 59.6 [14], p ! NS), years of arterialhypertension evolution (6.2 [7.6] vs. 6.1 [6.4], p ! NS), numberof hypertensive drugs (2.4 [1] vs. 2.1 [0.9], p ! NS), and yearsof snoring (18.8 [6.7] vs. 20 [14.1], p ! NS).
In the last imaging test performed before the sleep study,persistence of the aortic dissection was observed in 6 of the 10patients treated surgically and in all of those in whom surgerywas not performed. Four patients were considered to show pro-gression of their aortic disease: one with type A and three withtype B dissections. The latter three presented severe OSAS:Two showed progressive aortic dilation, and one presented evo-lution to dissection of an intramural hematoma.
DISCUSSION
The results of this study show an association between thoracicaortic dissection and OSAS. In particular, a higher AHI wasfound in patients with aortic dissection compared with a controlgroup of hypertensive patients.
Arterial hypertension is the main known risk factor for aorticdissection, and previous studies showed a high prevalence ofOSAS in hypertensive patients referred to a hypertension unit(12–14), which could justify our findings in a group of patientswith aortic dissection. However, the AHI found in our dissectionpatients, with seven suffering more than 30 apneas–hypopneasper hour of sleep, is higher than that previously reported inhypertensive patients. Furthermore, it was significantly higherthan that of a control group of hypertensive patients of similarsex, age, body mass index, and upper body obesity, all knownrisk factors for the development of OSAS (19–21). Isaksson andSvanborg (22) affirmed that OSAS is more common in patientswith poorly controlled hypertension, although this was not en-countered by other authors (14). However, apart from an AHIhigher than that reported by these authors, the aortic dissectionpatients in our study presented arterial hypertension of a numberof years of known evolution, number of drugs required for itscontrol, and blood pressure values on the day of the sleep studysimilar to those of the control group. Antihypertensive treatmentdiffered slightly between groups, and the frequency of "-blockers,a type of medication that some authors have suggested mightworsen OSAS (23), was somewhat higher in the group of patientswith dissection. However, this adverse effect has not been con-firmed in studies comparing the effects of "-blockers and placebo(24) or other antihypertensive drugs (25).
These facts raise the hypothesis that OSAS, besides favoringthe presence of arterial hypertension, could be a contributingfactor to dissection in some patients through the mechanicalstress on the aorta wall caused by repeated episodes of apneaand hypopnea. Inspiratory efforts against an occluded upperairway determine progressively negative intrathoracic pressures,which reach final mean peak values of approximately #60 cmH2O (8, 26). These negative pressures are transmitted to allintrathoracic structures and have been related to worsening ofleft ventricle function (27) and gastroesophageal reflux (28). Inan animal model, Peters and colleagues (29, 30) observed anincrease in systolic and diastolic aortic diameters during obstruc-tive apnea episodes. In parallel to this development of progres-sively negative intrathoracic pressures, a marked increase insympathetic activity and blood pressure is produced during ap-neas, which at the end of the obstructive event may doublethe basal systolic values (9, 31, 32). Upper airway obstructiveepisodes during sleep are known to be frequently asymptomatic(2) and may have been evolving for years before being clinicallydetected. Thus, it could be speculated that in our patients, thesudden rises in the transmural pressure of the aortic wall, re-
peated hundreds of times nightly over years, could have contrib-uted to dissection of the aortic wall, already weakened by factorssuch as diabetes, dyslipemia, or smoking. Apart from by thisincrease in the sheer forces, OSAS could contribute to this weak-ening of the aorta wall because various mechanisms have beensuggested relating it to arteriosclerosis development (33–35) andan increase in intima-media thickness of great arteries has beendemonstrated in OSAS patients (36).
Our study has several limitations. The sleep study was con-ducted several months after the aortic dissection had been diag-nosed; however, we believe that such a short period of time,together with the absence of significant changes in weight, sug-gests that the detected sleep-disordered breathing was presentat the time of the dissection. Furthermore, a case-control studydoes not permit us to elucidate whether OSAS is a risk factorfor aortic dissection. Although the main known variables forthe development of both entities had been controlled, otherconfounding factors may have existed to influence our results.A complementary alternative approach to our study would beto include OSAS as a prognostic variable in follow-up studies,including a greater number of patients with aortic dissection.
Despite these limitations, we believe that our findings mayhave repercussions on the management of these patients. Treat-ment of OSAS with nasal continuous positive airway pressureprevents obstructive episodes of the upper airway and, conse-quently, the development of intrathoracic negative pressures(26), sympathetic discharges, and their associated rise in bloodpressure (9, 37, 38), all of which are desirable in the aorticdissection patient. Furthermore, it has been demonstrated thatantihypertensive medication does not achieve optimum controlof blood pressure in hypertensive OSAS patients (25, 39), whichis achieved when nasal continuous positive airway pressure isadded (40). Although this study was not oriented toward as-sessing the evolution of patients with dissection, despite theshortness of follow-up, three of the four patients who showedaortic disease progression presented severe OSAS.
Thoracic aorta dissection frequently requires surgical treat-ment. OSAS is known to be associated with an increase in periop-erative morbidity and mortality (41, 42) because of a rise in thefrequency and duration of upper airway obstructive episodescaused by the use of analgesics, sedatives, and anesthetics (43).This may be particularly important in patients with aortic dissec-tion and OSAS undergoing surgery in whom, in addition to compli-cations secondary to OSAS per se, rises in transmural pressureduring upper airway obstructive episodes may have a particularlyadverse effect on the recently surgically repaired thoracic aorta.Because the anesthetic and postoperative management of thesepatients with OSAS benefits from specific measures (44, 45), webelieve that the early detection of OSAS could contribute to betterperioperative management of these patients.
Our results indicate the need to assess the presence of symp-toms suggestive of OSAS in patients with thoracic aorta dissec-tion. Given the relative absence of sleepiness detected and thelack of specificity of other symptoms such as snoring, we believethat their presence should be additionally studied by simplescreening tests such as nocturnal pulsioxymetry or a limited sleepstudy and, when the patient is stable, with full polysomnography.
In summary, in this study, a high mean AHI was found inpatients with thoracic aorta dissection. We speculate that thecoexistence of OSAS may impose an additional risk of aorticdissection in predisposed patients or determine worse evolutionbecause of the increase in aortic transmural pressure implied.Because effective treatment for OSAS is available, we believeits diagnosis should be considered in the overall assessment ofpatients with aortic dissection.
1530 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003
similar age (56.4 [15.0] vs. 59.6 [14], p ! NS), years of arterialhypertension evolution (6.2 [7.6] vs. 6.1 [6.4], p ! NS), numberof hypertensive drugs (2.4 [1] vs. 2.1 [0.9], p ! NS), and yearsof snoring (18.8 [6.7] vs. 20 [14.1], p ! NS).
In the last imaging test performed before the sleep study,persistence of the aortic dissection was observed in 6 of the 10patients treated surgically and in all of those in whom surgerywas not performed. Four patients were considered to show pro-gression of their aortic disease: one with type A and three withtype B dissections. The latter three presented severe OSAS:Two showed progressive aortic dilation, and one presented evo-lution to dissection of an intramural hematoma.
DISCUSSION
The results of this study show an association between thoracicaortic dissection and OSAS. In particular, a higher AHI wasfound in patients with aortic dissection compared with a controlgroup of hypertensive patients.
Arterial hypertension is the main known risk factor for aorticdissection, and previous studies showed a high prevalence ofOSAS in hypertensive patients referred to a hypertension unit(12–14), which could justify our findings in a group of patientswith aortic dissection. However, the AHI found in our dissectionpatients, with seven suffering more than 30 apneas–hypopneasper hour of sleep, is higher than that previously reported inhypertensive patients. Furthermore, it was significantly higherthan that of a control group of hypertensive patients of similarsex, age, body mass index, and upper body obesity, all knownrisk factors for the development of OSAS (19–21). Isaksson andSvanborg (22) affirmed that OSAS is more common in patientswith poorly controlled hypertension, although this was not en-countered by other authors (14). However, apart from an AHIhigher than that reported by these authors, the aortic dissectionpatients in our study presented arterial hypertension of a numberof years of known evolution, number of drugs required for itscontrol, and blood pressure values on the day of the sleep studysimilar to those of the control group. Antihypertensive treatmentdiffered slightly between groups, and the frequency of "-blockers,a type of medication that some authors have suggested mightworsen OSAS (23), was somewhat higher in the group of patientswith dissection. However, this adverse effect has not been con-firmed in studies comparing the effects of "-blockers and placebo(24) or other antihypertensive drugs (25).
These facts raise the hypothesis that OSAS, besides favoringthe presence of arterial hypertension, could be a contributingfactor to dissection in some patients through the mechanicalstress on the aorta wall caused by repeated episodes of apneaand hypopnea. Inspiratory efforts against an occluded upperairway determine progressively negative intrathoracic pressures,which reach final mean peak values of approximately #60 cmH2O (8, 26). These negative pressures are transmitted to allintrathoracic structures and have been related to worsening ofleft ventricle function (27) and gastroesophageal reflux (28). Inan animal model, Peters and colleagues (29, 30) observed anincrease in systolic and diastolic aortic diameters during obstruc-tive apnea episodes. In parallel to this development of progres-sively negative intrathoracic pressures, a marked increase insympathetic activity and blood pressure is produced during ap-neas, which at the end of the obstructive event may doublethe basal systolic values (9, 31, 32). Upper airway obstructiveepisodes during sleep are known to be frequently asymptomatic(2) and may have been evolving for years before being clinicallydetected. Thus, it could be speculated that in our patients, thesudden rises in the transmural pressure of the aortic wall, re-
peated hundreds of times nightly over years, could have contrib-uted to dissection of the aortic wall, already weakened by factorssuch as diabetes, dyslipemia, or smoking. Apart from by thisincrease in the sheer forces, OSAS could contribute to this weak-ening of the aorta wall because various mechanisms have beensuggested relating it to arteriosclerosis development (33–35) andan increase in intima-media thickness of great arteries has beendemonstrated in OSAS patients (36).
Our study has several limitations. The sleep study was con-ducted several months after the aortic dissection had been diag-nosed; however, we believe that such a short period of time,together with the absence of significant changes in weight, sug-gests that the detected sleep-disordered breathing was presentat the time of the dissection. Furthermore, a case-control studydoes not permit us to elucidate whether OSAS is a risk factorfor aortic dissection. Although the main known variables forthe development of both entities had been controlled, otherconfounding factors may have existed to influence our results.A complementary alternative approach to our study would beto include OSAS as a prognostic variable in follow-up studies,including a greater number of patients with aortic dissection.
Despite these limitations, we believe that our findings mayhave repercussions on the management of these patients. Treat-ment of OSAS with nasal continuous positive airway pressureprevents obstructive episodes of the upper airway and, conse-quently, the development of intrathoracic negative pressures(26), sympathetic discharges, and their associated rise in bloodpressure (9, 37, 38), all of which are desirable in the aorticdissection patient. Furthermore, it has been demonstrated thatantihypertensive medication does not achieve optimum controlof blood pressure in hypertensive OSAS patients (25, 39), whichis achieved when nasal continuous positive airway pressure isadded (40). Although this study was not oriented toward as-sessing the evolution of patients with dissection, despite theshortness of follow-up, three of the four patients who showedaortic disease progression presented severe OSAS.
Thoracic aorta dissection frequently requires surgical treat-ment. OSAS is known to be associated with an increase in periop-erative morbidity and mortality (41, 42) because of a rise in thefrequency and duration of upper airway obstructive episodescaused by the use of analgesics, sedatives, and anesthetics (43).This may be particularly important in patients with aortic dissec-tion and OSAS undergoing surgery in whom, in addition to compli-cations secondary to OSAS per se, rises in transmural pressureduring upper airway obstructive episodes may have a particularlyadverse effect on the recently surgically repaired thoracic aorta.Because the anesthetic and postoperative management of thesepatients with OSAS benefits from specific measures (44, 45), webelieve that the early detection of OSAS could contribute to betterperioperative management of these patients.
Our results indicate the need to assess the presence of symp-toms suggestive of OSAS in patients with thoracic aorta dissec-tion. Given the relative absence of sleepiness detected and thelack of specificity of other symptoms such as snoring, we believethat their presence should be additionally studied by simplescreening tests such as nocturnal pulsioxymetry or a limited sleepstudy and, when the patient is stable, with full polysomnography.
In summary, in this study, a high mean AHI was found inpatients with thoracic aorta dissection. We speculate that thecoexistence of OSAS may impose an additional risk of aorticdissection in predisposed patients or determine worse evolutionbecause of the increase in aortic transmural pressure implied.Because effective treatment for OSAS is available, we believeits diagnosis should be considered in the overall assessment ofpatients with aortic dissection.

24
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
RaQonale y Discusión
1530 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003
similar age (56.4 [15.0] vs. 59.6 [14], p ! NS), years of arterialhypertension evolution (6.2 [7.6] vs. 6.1 [6.4], p ! NS), numberof hypertensive drugs (2.4 [1] vs. 2.1 [0.9], p ! NS), and yearsof snoring (18.8 [6.7] vs. 20 [14.1], p ! NS).
In the last imaging test performed before the sleep study,persistence of the aortic dissection was observed in 6 of the 10patients treated surgically and in all of those in whom surgerywas not performed. Four patients were considered to show pro-gression of their aortic disease: one with type A and three withtype B dissections. The latter three presented severe OSAS:Two showed progressive aortic dilation, and one presented evo-lution to dissection of an intramural hematoma.
DISCUSSION
The results of this study show an association between thoracicaortic dissection and OSAS. In particular, a higher AHI wasfound in patients with aortic dissection compared with a controlgroup of hypertensive patients.
Arterial hypertension is the main known risk factor for aorticdissection, and previous studies showed a high prevalence ofOSAS in hypertensive patients referred to a hypertension unit(12–14), which could justify our findings in a group of patientswith aortic dissection. However, the AHI found in our dissectionpatients, with seven suffering more than 30 apneas–hypopneasper hour of sleep, is higher than that previously reported inhypertensive patients. Furthermore, it was significantly higherthan that of a control group of hypertensive patients of similarsex, age, body mass index, and upper body obesity, all knownrisk factors for the development of OSAS (19–21). Isaksson andSvanborg (22) affirmed that OSAS is more common in patientswith poorly controlled hypertension, although this was not en-countered by other authors (14). However, apart from an AHIhigher than that reported by these authors, the aortic dissectionpatients in our study presented arterial hypertension of a numberof years of known evolution, number of drugs required for itscontrol, and blood pressure values on the day of the sleep studysimilar to those of the control group. Antihypertensive treatmentdiffered slightly between groups, and the frequency of "-blockers,a type of medication that some authors have suggested mightworsen OSAS (23), was somewhat higher in the group of patientswith dissection. However, this adverse effect has not been con-firmed in studies comparing the effects of "-blockers and placebo(24) or other antihypertensive drugs (25).
These facts raise the hypothesis that OSAS, besides favoringthe presence of arterial hypertension, could be a contributingfactor to dissection in some patients through the mechanicalstress on the aorta wall caused by repeated episodes of apneaand hypopnea. Inspiratory efforts against an occluded upperairway determine progressively negative intrathoracic pressures,which reach final mean peak values of approximately #60 cmH2O (8, 26). These negative pressures are transmitted to allintrathoracic structures and have been related to worsening ofleft ventricle function (27) and gastroesophageal reflux (28). Inan animal model, Peters and colleagues (29, 30) observed anincrease in systolic and diastolic aortic diameters during obstruc-tive apnea episodes. In parallel to this development of progres-sively negative intrathoracic pressures, a marked increase insympathetic activity and blood pressure is produced during ap-neas, which at the end of the obstructive event may doublethe basal systolic values (9, 31, 32). Upper airway obstructiveepisodes during sleep are known to be frequently asymptomatic(2) and may have been evolving for years before being clinicallydetected. Thus, it could be speculated that in our patients, thesudden rises in the transmural pressure of the aortic wall, re-
peated hundreds of times nightly over years, could have contrib-uted to dissection of the aortic wall, already weakened by factorssuch as diabetes, dyslipemia, or smoking. Apart from by thisincrease in the sheer forces, OSAS could contribute to this weak-ening of the aorta wall because various mechanisms have beensuggested relating it to arteriosclerosis development (33–35) andan increase in intima-media thickness of great arteries has beendemonstrated in OSAS patients (36).
Our study has several limitations. The sleep study was con-ducted several months after the aortic dissection had been diag-nosed; however, we believe that such a short period of time,together with the absence of significant changes in weight, sug-gests that the detected sleep-disordered breathing was presentat the time of the dissection. Furthermore, a case-control studydoes not permit us to elucidate whether OSAS is a risk factorfor aortic dissection. Although the main known variables forthe development of both entities had been controlled, otherconfounding factors may have existed to influence our results.A complementary alternative approach to our study would beto include OSAS as a prognostic variable in follow-up studies,including a greater number of patients with aortic dissection.
Despite these limitations, we believe that our findings mayhave repercussions on the management of these patients. Treat-ment of OSAS with nasal continuous positive airway pressureprevents obstructive episodes of the upper airway and, conse-quently, the development of intrathoracic negative pressures(26), sympathetic discharges, and their associated rise in bloodpressure (9, 37, 38), all of which are desirable in the aorticdissection patient. Furthermore, it has been demonstrated thatantihypertensive medication does not achieve optimum controlof blood pressure in hypertensive OSAS patients (25, 39), whichis achieved when nasal continuous positive airway pressure isadded (40). Although this study was not oriented toward as-sessing the evolution of patients with dissection, despite theshortness of follow-up, three of the four patients who showedaortic disease progression presented severe OSAS.
Thoracic aorta dissection frequently requires surgical treat-ment. OSAS is known to be associated with an increase in periop-erative morbidity and mortality (41, 42) because of a rise in thefrequency and duration of upper airway obstructive episodescaused by the use of analgesics, sedatives, and anesthetics (43).This may be particularly important in patients with aortic dissec-tion and OSAS undergoing surgery in whom, in addition to compli-cations secondary to OSAS per se, rises in transmural pressureduring upper airway obstructive episodes may have a particularlyadverse effect on the recently surgically repaired thoracic aorta.Because the anesthetic and postoperative management of thesepatients with OSAS benefits from specific measures (44, 45), webelieve that the early detection of OSAS could contribute to betterperioperative management of these patients.
Our results indicate the need to assess the presence of symp-toms suggestive of OSAS in patients with thoracic aorta dissec-tion. Given the relative absence of sleepiness detected and thelack of specificity of other symptoms such as snoring, we believethat their presence should be additionally studied by simplescreening tests such as nocturnal pulsioxymetry or a limited sleepstudy and, when the patient is stable, with full polysomnography.
In summary, in this study, a high mean AHI was found inpatients with thoracic aorta dissection. We speculate that thecoexistence of OSAS may impose an additional risk of aorticdissection in predisposed patients or determine worse evolutionbecause of the increase in aortic transmural pressure implied.Because effective treatment for OSAS is available, we believeits diagnosis should be considered in the overall assessment ofpatients with aortic dissection.
1530 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003
similar age (56.4 [15.0] vs. 59.6 [14], p ! NS), years of arterialhypertension evolution (6.2 [7.6] vs. 6.1 [6.4], p ! NS), numberof hypertensive drugs (2.4 [1] vs. 2.1 [0.9], p ! NS), and yearsof snoring (18.8 [6.7] vs. 20 [14.1], p ! NS).
In the last imaging test performed before the sleep study,persistence of the aortic dissection was observed in 6 of the 10patients treated surgically and in all of those in whom surgerywas not performed. Four patients were considered to show pro-gression of their aortic disease: one with type A and three withtype B dissections. The latter three presented severe OSAS:Two showed progressive aortic dilation, and one presented evo-lution to dissection of an intramural hematoma.
DISCUSSION
The results of this study show an association between thoracicaortic dissection and OSAS. In particular, a higher AHI wasfound in patients with aortic dissection compared with a controlgroup of hypertensive patients.
Arterial hypertension is the main known risk factor for aorticdissection, and previous studies showed a high prevalence ofOSAS in hypertensive patients referred to a hypertension unit(12–14), which could justify our findings in a group of patientswith aortic dissection. However, the AHI found in our dissectionpatients, with seven suffering more than 30 apneas–hypopneasper hour of sleep, is higher than that previously reported inhypertensive patients. Furthermore, it was significantly higherthan that of a control group of hypertensive patients of similarsex, age, body mass index, and upper body obesity, all knownrisk factors for the development of OSAS (19–21). Isaksson andSvanborg (22) affirmed that OSAS is more common in patientswith poorly controlled hypertension, although this was not en-countered by other authors (14). However, apart from an AHIhigher than that reported by these authors, the aortic dissectionpatients in our study presented arterial hypertension of a numberof years of known evolution, number of drugs required for itscontrol, and blood pressure values on the day of the sleep studysimilar to those of the control group. Antihypertensive treatmentdiffered slightly between groups, and the frequency of "-blockers,a type of medication that some authors have suggested mightworsen OSAS (23), was somewhat higher in the group of patientswith dissection. However, this adverse effect has not been con-firmed in studies comparing the effects of "-blockers and placebo(24) or other antihypertensive drugs (25).
These facts raise the hypothesis that OSAS, besides favoringthe presence of arterial hypertension, could be a contributingfactor to dissection in some patients through the mechanicalstress on the aorta wall caused by repeated episodes of apneaand hypopnea. Inspiratory efforts against an occluded upperairway determine progressively negative intrathoracic pressures,which reach final mean peak values of approximately #60 cmH2O (8, 26). These negative pressures are transmitted to allintrathoracic structures and have been related to worsening ofleft ventricle function (27) and gastroesophageal reflux (28). Inan animal model, Peters and colleagues (29, 30) observed anincrease in systolic and diastolic aortic diameters during obstruc-tive apnea episodes. In parallel to this development of progres-sively negative intrathoracic pressures, a marked increase insympathetic activity and blood pressure is produced during ap-neas, which at the end of the obstructive event may doublethe basal systolic values (9, 31, 32). Upper airway obstructiveepisodes during sleep are known to be frequently asymptomatic(2) and may have been evolving for years before being clinicallydetected. Thus, it could be speculated that in our patients, thesudden rises in the transmural pressure of the aortic wall, re-
peated hundreds of times nightly over years, could have contrib-uted to dissection of the aortic wall, already weakened by factorssuch as diabetes, dyslipemia, or smoking. Apart from by thisincrease in the sheer forces, OSAS could contribute to this weak-ening of the aorta wall because various mechanisms have beensuggested relating it to arteriosclerosis development (33–35) andan increase in intima-media thickness of great arteries has beendemonstrated in OSAS patients (36).
Our study has several limitations. The sleep study was con-ducted several months after the aortic dissection had been diag-nosed; however, we believe that such a short period of time,together with the absence of significant changes in weight, sug-gests that the detected sleep-disordered breathing was presentat the time of the dissection. Furthermore, a case-control studydoes not permit us to elucidate whether OSAS is a risk factorfor aortic dissection. Although the main known variables forthe development of both entities had been controlled, otherconfounding factors may have existed to influence our results.A complementary alternative approach to our study would beto include OSAS as a prognostic variable in follow-up studies,including a greater number of patients with aortic dissection.
Despite these limitations, we believe that our findings mayhave repercussions on the management of these patients. Treat-ment of OSAS with nasal continuous positive airway pressureprevents obstructive episodes of the upper airway and, conse-quently, the development of intrathoracic negative pressures(26), sympathetic discharges, and their associated rise in bloodpressure (9, 37, 38), all of which are desirable in the aorticdissection patient. Furthermore, it has been demonstrated thatantihypertensive medication does not achieve optimum controlof blood pressure in hypertensive OSAS patients (25, 39), whichis achieved when nasal continuous positive airway pressure isadded (40). Although this study was not oriented toward as-sessing the evolution of patients with dissection, despite theshortness of follow-up, three of the four patients who showedaortic disease progression presented severe OSAS.
Thoracic aorta dissection frequently requires surgical treat-ment. OSAS is known to be associated with an increase in periop-erative morbidity and mortality (41, 42) because of a rise in thefrequency and duration of upper airway obstructive episodescaused by the use of analgesics, sedatives, and anesthetics (43).This may be particularly important in patients with aortic dissec-tion and OSAS undergoing surgery in whom, in addition to compli-cations secondary to OSAS per se, rises in transmural pressureduring upper airway obstructive episodes may have a particularlyadverse effect on the recently surgically repaired thoracic aorta.Because the anesthetic and postoperative management of thesepatients with OSAS benefits from specific measures (44, 45), webelieve that the early detection of OSAS could contribute to betterperioperative management of these patients.
Our results indicate the need to assess the presence of symp-toms suggestive of OSAS in patients with thoracic aorta dissec-tion. Given the relative absence of sleepiness detected and thelack of specificity of other symptoms such as snoring, we believethat their presence should be additionally studied by simplescreening tests such as nocturnal pulsioxymetry or a limited sleepstudy and, when the patient is stable, with full polysomnography.
In summary, in this study, a high mean AHI was found inpatients with thoracic aorta dissection. We speculate that thecoexistence of OSAS may impose an additional risk of aorticdissection in predisposed patients or determine worse evolutionbecause of the increase in aortic transmural pressure implied.Because effective treatment for OSAS is available, we believeits diagnosis should be considered in the overall assessment ofpatients with aortic dissection.
1530 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 168 2003
similar age (56.4 [15.0] vs. 59.6 [14], p ! NS), years of arterialhypertension evolution (6.2 [7.6] vs. 6.1 [6.4], p ! NS), numberof hypertensive drugs (2.4 [1] vs. 2.1 [0.9], p ! NS), and yearsof snoring (18.8 [6.7] vs. 20 [14.1], p ! NS).
In the last imaging test performed before the sleep study,persistence of the aortic dissection was observed in 6 of the 10patients treated surgically and in all of those in whom surgerywas not performed. Four patients were considered to show pro-gression of their aortic disease: one with type A and three withtype B dissections. The latter three presented severe OSAS:Two showed progressive aortic dilation, and one presented evo-lution to dissection of an intramural hematoma.
DISCUSSION
The results of this study show an association between thoracicaortic dissection and OSAS. In particular, a higher AHI wasfound in patients with aortic dissection compared with a controlgroup of hypertensive patients.
Arterial hypertension is the main known risk factor for aorticdissection, and previous studies showed a high prevalence ofOSAS in hypertensive patients referred to a hypertension unit(12–14), which could justify our findings in a group of patientswith aortic dissection. However, the AHI found in our dissectionpatients, with seven suffering more than 30 apneas–hypopneasper hour of sleep, is higher than that previously reported inhypertensive patients. Furthermore, it was significantly higherthan that of a control group of hypertensive patients of similarsex, age, body mass index, and upper body obesity, all knownrisk factors for the development of OSAS (19–21). Isaksson andSvanborg (22) affirmed that OSAS is more common in patientswith poorly controlled hypertension, although this was not en-countered by other authors (14). However, apart from an AHIhigher than that reported by these authors, the aortic dissectionpatients in our study presented arterial hypertension of a numberof years of known evolution, number of drugs required for itscontrol, and blood pressure values on the day of the sleep studysimilar to those of the control group. Antihypertensive treatmentdiffered slightly between groups, and the frequency of "-blockers,a type of medication that some authors have suggested mightworsen OSAS (23), was somewhat higher in the group of patientswith dissection. However, this adverse effect has not been con-firmed in studies comparing the effects of "-blockers and placebo(24) or other antihypertensive drugs (25).
These facts raise the hypothesis that OSAS, besides favoringthe presence of arterial hypertension, could be a contributingfactor to dissection in some patients through the mechanicalstress on the aorta wall caused by repeated episodes of apneaand hypopnea. Inspiratory efforts against an occluded upperairway determine progressively negative intrathoracic pressures,which reach final mean peak values of approximately #60 cmH2O (8, 26). These negative pressures are transmitted to allintrathoracic structures and have been related to worsening ofleft ventricle function (27) and gastroesophageal reflux (28). Inan animal model, Peters and colleagues (29, 30) observed anincrease in systolic and diastolic aortic diameters during obstruc-tive apnea episodes. In parallel to this development of progres-sively negative intrathoracic pressures, a marked increase insympathetic activity and blood pressure is produced during ap-neas, which at the end of the obstructive event may doublethe basal systolic values (9, 31, 32). Upper airway obstructiveepisodes during sleep are known to be frequently asymptomatic(2) and may have been evolving for years before being clinicallydetected. Thus, it could be speculated that in our patients, thesudden rises in the transmural pressure of the aortic wall, re-
peated hundreds of times nightly over years, could have contrib-uted to dissection of the aortic wall, already weakened by factorssuch as diabetes, dyslipemia, or smoking. Apart from by thisincrease in the sheer forces, OSAS could contribute to this weak-ening of the aorta wall because various mechanisms have beensuggested relating it to arteriosclerosis development (33–35) andan increase in intima-media thickness of great arteries has beendemonstrated in OSAS patients (36).
Our study has several limitations. The sleep study was con-ducted several months after the aortic dissection had been diag-nosed; however, we believe that such a short period of time,together with the absence of significant changes in weight, sug-gests that the detected sleep-disordered breathing was presentat the time of the dissection. Furthermore, a case-control studydoes not permit us to elucidate whether OSAS is a risk factorfor aortic dissection. Although the main known variables forthe development of both entities had been controlled, otherconfounding factors may have existed to influence our results.A complementary alternative approach to our study would beto include OSAS as a prognostic variable in follow-up studies,including a greater number of patients with aortic dissection.
Despite these limitations, we believe that our findings mayhave repercussions on the management of these patients. Treat-ment of OSAS with nasal continuous positive airway pressureprevents obstructive episodes of the upper airway and, conse-quently, the development of intrathoracic negative pressures(26), sympathetic discharges, and their associated rise in bloodpressure (9, 37, 38), all of which are desirable in the aorticdissection patient. Furthermore, it has been demonstrated thatantihypertensive medication does not achieve optimum controlof blood pressure in hypertensive OSAS patients (25, 39), whichis achieved when nasal continuous positive airway pressure isadded (40). Although this study was not oriented toward as-sessing the evolution of patients with dissection, despite theshortness of follow-up, three of the four patients who showedaortic disease progression presented severe OSAS.
Thoracic aorta dissection frequently requires surgical treat-ment. OSAS is known to be associated with an increase in periop-erative morbidity and mortality (41, 42) because of a rise in thefrequency and duration of upper airway obstructive episodescaused by the use of analgesics, sedatives, and anesthetics (43).This may be particularly important in patients with aortic dissec-tion and OSAS undergoing surgery in whom, in addition to compli-cations secondary to OSAS per se, rises in transmural pressureduring upper airway obstructive episodes may have a particularlyadverse effect on the recently surgically repaired thoracic aorta.Because the anesthetic and postoperative management of thesepatients with OSAS benefits from specific measures (44, 45), webelieve that the early detection of OSAS could contribute to betterperioperative management of these patients.
Our results indicate the need to assess the presence of symp-toms suggestive of OSAS in patients with thoracic aorta dissec-tion. Given the relative absence of sleepiness detected and thelack of specificity of other symptoms such as snoring, we believethat their presence should be additionally studied by simplescreening tests such as nocturnal pulsioxymetry or a limited sleepstudy and, when the patient is stable, with full polysomnography.
In summary, in this study, a high mean AHI was found inpatients with thoracic aorta dissection. We speculate that thecoexistence of OSAS may impose an additional risk of aorticdissection in predisposed patients or determine worse evolutionbecause of the increase in aortic transmural pressure implied.Because effective treatment for OSAS is available, we believeits diagnosis should be considered in the overall assessment ofpatients with aortic dissection.
Otros efectos de la presión negaQva intratorácica: 1.-‐ Reflujo esofágico 2.-‐ Hernia de hiato 3.-‐ Tos persistente 4.-‐ Afectación función ventricular izquierda/derecha 5.-‐ Nicturia 6.-‐ HTA 7.-‐ Edema pulmonar?

25
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS RaQonale y Discusión

26
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
RaQonale y Discusión
27
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
RaQonale y Discusión

28
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS RaQonale y Discusión

29
UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS
Conclusiones
1.-‐ Los cambios de presión intratorácicos en el SAOS son comunes y causan diferentes patologías 2. La repercusión sobre la Aorta, sobre los receptores natriuréJcos de la Aurícula I y sobre ambos Ventrículos, contribuye a patología cardiovascular secundaria al SAOS 3.-‐ No es infrecuente que los pacientes con SAOS severo se quejen de dolores torácicos inespecíficos 4.-‐ Se ha presentado un caso no descrito de fracturas costales producidas por Apneas durante el sueño (SAOS)

UN GRITO EN LA NOCHE: UNA COMPLICACIÓN NO DESCRITA DE SAOS