optimizaciÓn de tratamiento con taxanos · optimizaciÓn de dosis y esquema de tratamiento ....
TRANSCRIPT

OPTIMIZACIÓN DE TRATAMIENTO CON
TAXANOS
Mireia Margelí

ÍNDICE
•Introducción:
– Guías de tratamiento en enfermedad metastásica
– ¿De que taxanos disponemos?
•¿Que significa optimizar?
–Optimización de dosis y esquema de tratamiento
–Optimización según tratamiento previo
–Optimización en función de subtipos biologicos
–Optimización en pacientes de peor pronóstico
–Optimización según edad
–¿Existen biomarcadores?
• Nuevos taxanos
• Conclusiones
• Is there an optimal first-line or second-line CT and/or targeted therapy regimen?
– There is no single optimal first-line CT. No single agent has demonstrated
superiority; there are several active agents appropriate for first-line. The
evidence for efficacy is strongest for taxanes and anthracyclines.
Treatment selection should be based on previous therapy, differential
toxicity, comorbid conditions, and patient preferences. Specifically, drugs for
which clinical resistance has already been shown should not be reused
• What is the optimal timing, dose, schedule, and duration?
– Optimal duration is hard to quantify; longer planned duration CT prolongs
disease control compared with shorter but has to be balanced against
progressive toxicity
– CT should be continued until progression of the disease (toxicity – QoL)
• Should treatment regimen vary by tumor subtypes or clinical characteristics?
– Tumor type should not be used to dictate choice of first-line treatment.

Optimización de tratamiento con taxanos Perspectiva histórica
Paclitaxel
1994
Docetaxel
1996
Nab Paclitaxel
2005
EndoTAG-1?
Tesetaxel?
La introducción de paclitaxel en primera línea de tto. Incremento de OS de 23.6 a 26.1 m (Gronwald et al J Clin Oncol 2009)
OPTIMIZACIÓN DE DOSIS Y ESQUEMA
DE TRATAMIENTO

Primeros estudios con Taxanos

Optimización de dosis

Tabla comparativa entre taxanos
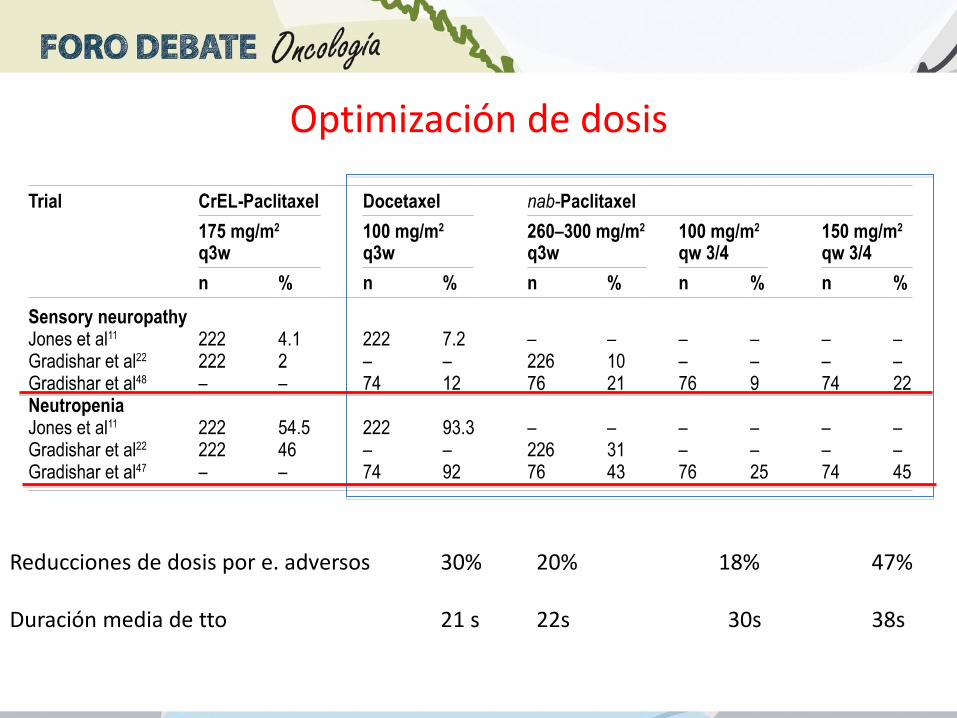
Optimización de dosis
Reducciones de dosis por e. adversos 30% 20% 18% 47% Duración media de tto 21 s 22s 30s 38s

Dosis de Nabpaclitaxel
Monoterapia vs Combinación
Journal of Cancer Research and Clinical Oncology
June 2011, Volume 137, Issue 6, pp 1005-1013
Date: 18 Dec 2010
A literature-based meta-analysis taxane-based doublet versus
single-agent taxane chemotherapy in patients with advanced
breast cancer
Hong-Bin Xu, Qing Xu, Ling Li
NO DIFERENCIAS EN OS
MÁS TOXICIDAD EN COMBINACIÓN
OPTIMIZACIÓN SEGÚN TRATAMIENTO PREVIO

Optimización según tratamiento previo
Tratamienro previo utilizado
Intérvalo libre de enfermedad
El Retratamiento con taxanos es posible Seleccionando un taxano diferente
Palmieri C (Nature Reviews Clin Oncol 2010)
Retratamiento
NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 7 | OCTOBER 2010 | 569
received prior paclitaxel, the RR was 13% and 20% for the
100 mg/m2 and 125 mg/m2 dose, respectively. For patients
previously exposed to docetaxel, the RR for both doses of
albumin-bound paclitaxel was 21%. The RR was only 7%
in those who received both taxanes as prior therapy (all
patients received the 100 mg/m2 dose). Of the patients who
received previous weekly taxane therapy, the proportion
of responders was greater at both dose levels for those who
had received docetaxel alone (30% and 27% for 100 mg/m2
and 125 mg/m2, respectively) than for those who had
received paclitaxel alone (0% and 17%, respectively).
However, there was no subgroup analysis on adjuvant or
metastatic patients where prior taxanes were given.
Docetaxel
The efficacy of rechallenging with docetaxel (100 mg/m2
every 3 weeks) following prior taxane exposure in the
metastatic setting has been published in two small studies
(Table 6 and Supplementary Table 3 online). The first
was a phase II study of 46 patients who had progressed
while or after receiving paclitaxel (135–250 mg/m2 for at
least two cycles).72 The median time from the last dose
of paclitaxel was 1 month. Following rechallenge with
docetaxel, overall RRs of 17.4% and 18.1% were observed
in the intent-to-treat and assessable popula tions, respec-
tively. The median duration of response was 29 weeks
and the median TTP and overall survival were 10 weeks and
10.5 months, respectively.
To determine the effect of taxane resistance on doce-
taxel rechallenge, the 44 assessable patients were divided
into those with primary resistance (n = 17), defined as
disease progression, and those with secondary resistance
(n = 27), defined as SD, PR or CR to paclitaxel before
disease progression. RRs were similar between the two
cohorts (17.6% and 18.5%, respectively). Further analysis
based on prior paclitaxel dose revealed an improved RR
in those who had received >175 mg/m2 paclitaxel than in
those who received <175 mg/m2 (31.2% versus 10.7%).
An improved RR was also seen in patients (74%) who
had previously received paclitaxel by 3 h infusion than in
patients treated with a 24 h infusion (25% versus 0%).
The second study was a single-center, retro spective
review of 24 patients previously treated with anthracycline-
based and paclitaxel-based regimens, who then received
docetaxel (75 mg/m2 every 3 weeks) until disease progres-
sion or the occurrence of unacceptable toxic effects.73 An
Table 6 | Taxane rechallenge
Study design and reference
n Prior ANC regimen (%)
Prior taxane regimen (%)
Time since taxane therapy (median), months
Second-line taxane treatment
Regimen mg/ m2 (n)
RR % (95% CI) Clinical benefit (%)
Median TTP (months)
Median OS (months)
Eff cacy of paclitaxel following ANCs and/ or taxane therapy in the metastatic setting
Phase II clinical
trial67
26 ANC-based
(33)
3 h Pac infusion
1 h Doc infusion
(100)
1–7 (1) Pac
120–140
(26)
27 (11.6–47.8) 61.5 RD = 6 (range:
1–13)
–
Multicenter
phase II trial:
subgroup analysis68
212 ANC-based
(72)
Pac or Doc 3–4
weekly regimen
(25)
2.7 Pac 80
(45)
15.6 – – –
Multicenter
phase II trial69
47 ANC-based
(93)
Doc (100) – Pac 80
(46)
17.4
1° resist* : 33.3
2° resist* : 9.7
26.1 11 weeks
(1–104
weeks)
–
Retrospective
single-center
cohort study70
82 ANC-based
(91)
Doc (100) 0.5–23 (2.9) Pac 80
(82)
19.5 (10.9–28.1)
1° resist‡: 8.3
2° resist‡: 24.1
– 3.7 (95% CI
2.75–4.72)
9.4
(95% CI
7.25–11.55)
Eff cacy of albumen-bound paclitaxel following ANCs and/ or taxane therapy in the metastatic setting
Open-label phase II
study71
181 ANC-based
(67)
Pac and/ or Doc
(100) in the
adjuvant or
metastatic setting
PD on treatment
for metastatic or
<12 months since
adjuvant treatment
Alb-Pac
100
(106)
Alb-Pac
125 (75)
14 (7.52–20.79)
16 (7.7–24.3)
26
37
3
3.5
9.2
9.1
Eff cacy of docetaxel following ANCs and/ or taxane therapy in the metastatic setting
Multicenter
phase II trial72
46 ANC-based
(89)
Pac 24 h infusion
or 3 h infusion
(100)
0.6–7.2 (1) Doc 100
(44)
ITT: 17.4 (7.8–31.4)
All: 18.1 (6.7–29.5)
1° resist§: 17.6
2° resist§: 18.5
50 2.3
(3–53 weeks)
10.5
(1.2–>30)
Retrospective
single-center
cohort study73
24 ANC-based
(100)
3 h Pac 175 or
Pac–cisplatin
(100)
– Doc 75
(24)
Overall: 25
Chemo-resist ||: 33
Chemo-ref ||: 20
62.5 9 (in cases
with response
or SD)
12.0
* 1° resist: progression within 6 months after adjuvant therapy or PD on treatment in metastatic setting; 2° resist: PD after treatment in metastatic setting after a documented response. ‡1° resist: PD on treatment in metastatic setting; 2° resist: PD after treatment in metastatic setting after a documented clinical response. §1° resist: no tumor response (PD); 2° resist: PD after treatment with
complete response, partial response or SD. ||Chemo-resist: chemoresistance to paclitaxel: recurrence after 12 months of the last dose of adjuvant chemotherapy response in the metastatic setting followed by recurrent disease; Chemo-ref: chemorefractory to paclitaxel: recurrence within 12 months of the last dose of adjuvant chemotherapy or PD while receiving treatment for metastatic disease. Abbreviations: ANC, anthracycline; Doc, docetaxel; ITT, intention to treat; OS, overall survival; Pac, paclitaxel; PD, progressive disease; RD, response duration; resist, resistant; RR,
response rate; SD, stable disease; TTP, time to progression. Full regimen details of these trials are outlined in Supplementary Table 3 online.
REVIEWS
nrclinonc_122_OCT10.indd 569 9/9/10 15:01:31
© 20 Macmillan Publishers Limited. All rights reserved10
Muchos pequeños estudios en metastásico,
evalúan retratamiento con taxanos
RR 18-31%
TTP 2.3-12 m
OS 9.1-26.7 m

Breast Care 2011;6:279–283Taxane Re-Challenge in Recurrent
Breast Cancer
281
overall response rate was 54.5% with combination therapy
and 40% with taxane monotherapy (p = 0.2) (table 2). Pa-
tients with a disease-free interval of < 1 year until recurrence
showed a response rate of 34.8%, those with 1–2 years, a rate
of 42.9%, compared to those with > 2 years having a response
rate of 63.3% (p = 0.04). Other factors influencing the re-
Table 2. Clinical response to first-line taxane-based therapy
First-line therapy CR, n (%) PR, n (%) SD, n (%) PD, n (%) Response unknown, n (%)
All (n = 74) 20 (27.0) 16 (21.6) 4 (5.4) 15 (20.3) 19 (25.7)Docetaxel (n = 39) 6 (15.4) 9 (23.1) 4 (10.3) 10 (25.6) 10 (25.6)Paclitaxel (n = 35) 14 (40.0) 7 (20.0) 0 (0) 5 (14.3) 9 (25.7)Monotherapy (n = 30) 6 (20.0) 6 (20.0) 1 (3.3) 7 (23.3) 10 (33.3)Combination therapy (n = 44) 14 (31.8) 10 (22.7) 3 (6.8) 8 (18.2) 9 (20.5)
CR = Complete response, PR = partial response, SD = stable disease; PD = progressive disease.
Table 3. Univariable analysis on response to first-line-therapy and overall survival according to patient characteristics
Parameter Patients, n CR/PR, n (%) Chi2, p Median overall sur-
vival, years (95% CI)
Log rank, p
Age< 50 40 21 (52.5%) 1.4 (0.5–2.3)≥ 50 34 15 (44.1%) > 0.1 1.3 (0.5–2.1) > 0.1
ER/PgR statusPositive 37 19 (51.4%) 1.5 (0.4–2.6)Negative 32 15 (46.9%) > 0.1 1.3 (0.8–1.8) > 0.1
HER2 statusPositive 11 7 (63.6%) 4.0 (1.9–6.1)Negative 50 26 (52.0%) > 0.1 1.3 (0.9–1.7) > 0.1
Triple (ER/PgR/HER2)-negative statusYes 24 12 (50.0%) 1.4 (0.4–2.4)No 33 19 (57.6%) > 0.1 1.5 (0.4–2.4) > 0.1
Taxane as (neo-)adjuvant chemotherapyDocetaxel 39 19 (48.7%) 1.3 (1.0–1.6) > 0.1Paclitaxel 35 17 (48.6%) > 0.1 1.2 (0.0–2.5)
Disease-free interval until recurrence≥ 2 years 44 17 (38.6%) 0.9 (0.7–1.1) 0.002> 2 years 30 19 (63.3%) 0.04 4.0 (1.9–6.1)
Visceral metastasisPresent 40 25 (62.5%) 1.0 (0.7–1.4)Not present 34 11 (32.4%) 0.01 2.4 (1.1–3.7) 0.04
Taxane as first-line therapyDocetaxel 39 15 (38.5%) 2.4 (1.1–3.7)Paclitaxel 35 21 (60.0%) 0.06 1.0 (0.5–1.4) > 0.1
CR = Complete response, PR = partial response, CI = confidence interval, ER = estrogen receptor, PgR = progesterone receptor.
Fig. 1. Overall
survival of patients
receiving taxane
re-challenge as first-
line therapy.
Fig. 2. Overall
survival of patients
receiving taxane
re-challenge as first-
line therapy
according to the
length of the disease-
free interval.
sponse rate were the presence of visceral metastasis (p = 0.01)
and the type of taxane used (p = 0.06), whereas age, type of
taxane used for (neo-)adjuvant treatment, and hormone and
HER2 receptor status were not predictive (table 3). However,
there was no difference in response rates in relation to the
type of taxane that was used for re-challeng (table 2).
Fig. 3. Overall
survival of patients
receiving taxane re-
challenge as first-line
therapy according to
the presence of vis-
ceral metastasis.
Fig. 4. Overall
survival of patients
receiving taxane re-
challenge as first-line
therapy according
to the type of taxane
used in this setting.
Do
wnlo
ad
ed b
y:
77
.224.8
8.9
- 5
/3/2
015
10:3
2:2
7 P
M
Original Art icle · Originalarbeit
Breast Care 2011;6:279–283 Published online: August 19, 2011
DOI: 10.1159/000330946
Prof. Dr. Gunter von Minckwitz
German Breast Group
c/o GBG Forschungs GmbH
Martin-Behaim-Str. 12, 63263 Neu-Isenburg, Germany
Tel. +49 6102 7480-411, Fax -111
© 2011 S. Karger GmbH, Freiburg
1661-3791/11/0064-0279$38.00/0
Accessible online at:
www.karger.com/brc
Fax +49 761 4 52 07 14
www.karger.com
BreastCare
Re-Challenging Taxanes in Recurrent Breast Cancer in Patients Treated with (Neo-)Adjuvant Taxane-Based Therapy
Xinrong Guo a Sibylle Loibl a Michael Untch b Volker Möbusc Kathrin Schwedler d Peter A. Fasching e Jana Barinoff f Frank Holmsg Christoph Thomssen h Dirk M. Zahm i Rolf Kreienberg k Maik Hauschild l Holger Eidtmann m Sascha Tauchert n Keyur Mehtaa Gunter von Minckwitza for the German Breast Group and AGO-B Study Group
aGerman Breast Group, bHelios Klinikum Berlin-Buch, cFrauenklinik, Klinikum Frankfurt-Höchst, dUniversitäts-Frauenklinik Frankfurt, eFrauenklinik des Universitätsklinikums Erlangen, Friedrich-Alexander Universität Erlangen-Nürnberg, Erlangen, fFrauenklinik, Horst-Schmidt-Kliniken, Wiesbaden, gBarbaraklinik, Hamm, hUniversitäts-Frauenklinik Halle, iGera, kUniversitäts-Frauenklinik Ulm, lFrauenklinik Rheinfelden, mUni-Frauenklinik, Kiel, nCaritasklinik St. Theresia, Saarbrücken, Deutschland
Schlüsselwörter
Docetaxel · Paclitaxel · Adjuvant · Rezidivierter Brustkrebs
Zusammenfassung
Hintergrund: Docetaxel und Paclitaxel gehören zu den
aktivs ten Substanzen in der Behandlung des Mam makar-
zinoms. Da sie heute häufig bereits zur adjuvanten Be-
handlung eingesetzt werden, können Effektivitätsdaten von
früheren Studien mit Taxan-naiven, metastasierten Patien-
tinnen nicht mehr als zuverlässig angesehen werden. Pati-
enten und Methoden: Für die Taxane Re-Challenge Kohor-
tenstudie haben wir Teilnehmerinnen 6 prospektiver Taxan-
basierter (neo-)adjuvanter Studien mit rezidivierter Erkran-
kung identifiziert und Daten zur weiteren Behandlung
gesammelt. Bei 106 (27,8%) von 381 Patientinnen mit einem
Rezidiv oder einer Metastase wurde erneut ein Taxan in der
ersten oder späteren Behandlung eingesetzt. Ergebnisse:
Taxane wurden in der Erstlinie bei 74 Patientinnen ange-
wandt und zeigten eine Ansprechrate von 48,6% (inklusive
Komplettremissionen in 27,0%). Die Ansprechrate war vom
krankheitsfreien Intervall (< 1 Jahr: 34,8%; 1–2 Jahre: 42,9%;
> 2 Jahre: 63,3%; p = 0,04) und dem Vorhandensein viszera-
ler Metastasen (vorhanden: 62,5%; nicht vorhanden: 32,4%;
p = 0,01) abhängig. Patientinnen ohne viszerale Metastasen
und mit einem krankheitsfreien Intervall > 2 Jahre überleb -
ten am längsten. Hormon- und HER2-Rezeptorstatus waren
für das Ansprechen nicht prädiktiv, jedoch sprachen tripel-
negative Tumoren in 50.0% auf die erneute Taxan-Therapie
an. Die Gesamtansprechrate auf ein erneutes Taxan in der
späteren Linie betrug 28.2%. Schlussfolgerung: Der Wieder-
einsatz von Taxanen erscheint effektiv und steht somit als
sinnvolle Option für mit Taxanen (neo-)adjuvant vorbehan-
delte Patientinnen zur Verfügung.
Keywords
Docetaxel · Paclitaxel · Adjuvant · Recurrent breast cancer
Summary
Background: Docetaxel and paclitaxel are among the most
active substances for the treatment of breast cancer. As
both drugs are used today in adjuvant regimens, efficacy
data from pivotal trials in the metastatic setting in taxane-
naive populations cannot reliably be used as references.
Patients and Methods: The Taxane Re-Challenge Cohort
Study identified participants from 6 prospective (neo-)ad-
juvant taxane-based studies w ith recurrent disease and
collected data on their subsequent treatment. Out of 381
recurrent patients, 106 (27.8%) were re-challenged w ith a
taxane-based treatment as first- or later-line therapy for re-
current disease. Results: Taxanes were used as first-line
therapy in 74 patients and showed a response rate of 48.6%
(including complete responses in 27.0%). The response rate
was dependent on the disease-free interval (< 1 year: 34.8%;
1–2 years: 42.9%; > 2 years: 63.3%; p = 0.04) and visceral
metastasis (present: 62.5%; not present 32.4%; p = 0.01).
Patients without visceral metastasis and with a disease-free
interval of > 2 years achieved the longest overall survival.
Hormone and HER2 receptor status were not predictive;
however, triple-negative tumors responded in 50.0%. The
overall response rate of later-line taxane-based treatment
was 28.2%. Conclusion: Re-challenging taxanes appears to
be effective and therefore represents a reasonable option in
this population.
Down
loaded
by:
77.224
.88.9 -
5/3/20
15 10:
32:27
PM
Guo X Breast Care 2011
EN PACIENTES CON TAXANOS EN ADYUVANCIA/ NEOADYUVANCIA RR 48.6% EN PRIMERA LÍNEA RR 28.2% EN SEGUNDA LÍNEA Y POSTERIORES

Estudio Fase II 181 p pretratadas con taxanos (mediana 3 líneas previas)
ORR 14-16% PFS 3-3.5 m OS 9.1-9.2 m
Blum JL Clin Breast Cancer 2007
CA013: nab-Paclitaxel Treatment in Taxane- Refractory Metastatic Breast Cancer
Nab®-paclitaxel 100 mg/m2 qw3/4
n=106
Nab®-paclitaxel 125 mg/m2 qw3/4.
n=75
2 cohortes de pacientes *
100 mg/m2 125 mg/m2
Grado 3
%
Grado 4
%
Grado 3
%
Grado 4
%
Neutropenia
(sin G-CSF)
14 4 31 3
Fatiga 5 0 12 0
Neuropatía
sensorial
8 0 19 0

Nab-paclitaxel in Metastatic Breast Cancer
Patients Failing Solvent Based Taxane (Tiffany)
Cerrado precozmente por falta de reclutamiento

Optimización según subtipo biológico
• ¿Los diferentes subtipos biológicos responden de forma diferente a tratamiento con taxanos?
• Análisis multivariante de 3332 mujeres incluidas en estudios de neoadyuvancia. – Tto más largo, mayor dosis acumulada de antras y taxanos, adición de
Capecitabina. BENEFICIO EN EL GLOBAL DE PACIENTES
– Tto más prolongado de taxanos, más beneficio de RH+
– Tto más corto con más altas dosis de taxanos en TN
– HER2 positivo no influencia de número de ciclos o dosis acumulada de taxanos
Von Minckwitz G et al. Breast Cancer Res and Treat 2011

G. von Minckwitz et al. / Critical Reviews in Oncology/Hematology 85 (2013) 315–331 325
Fig. 4. Multivariate analysis showing the association between pathological complete response and (a) treatment characteristics, and (b) treatment characteristics
stratified by HR and HER2 status, both after adjustment for age, tumour size, grade, type, HR and HER2 status, as applicable. Findings are from a pooled
analysis of individual patient data from 3332 women included in seven neoadjuvant studies conducted in Germany [119].
*Effect as estimated for HER2-positive patients.
HR, hormone receptor; HER2, human epidermal growth factor receptor-2; pCR, pathological complete response.
Adapted with kind permission from Springer Science + Business Media B.V.: von Minckwitz et al. [119], http://dx.doi.org/10.1007/s10549-010-1228-x.
Von Minckwitz G et al. Breast Cancer Res and Treat 2011

GeparSepto: Phase III Neoadjuvant Trial of nab-P
vs sb-P Regimens in Early Breast Cancer
Initial Study Design
Untch et al. SABCS 2014; oral S2-07

Untch et al. SABCS 2014; oral S2-07

Untch et al. SABCS 2014; oral S2-07

Untch et al. SABCS 2014; oral S2-07

Primary endpoint: ORR in ITT population
Secondary endpoints: PFS, OS, ORR (crossover), toxicity
Subgroup analyses: BRCA1/2 mutation, basal-like subgroups, HRD biomarkers
TNT: Carboplatin vs Docetaxel in Advanced TNBC or BRCA1/2+ BC
Tutt A et al. SABCS 2014; Abstract S3-01

Tutt A et al. SABCS 2014; Abstract S3-01

OPTIMIZACIÓN EN PACIENTES DE MAL PRONÓSTICO
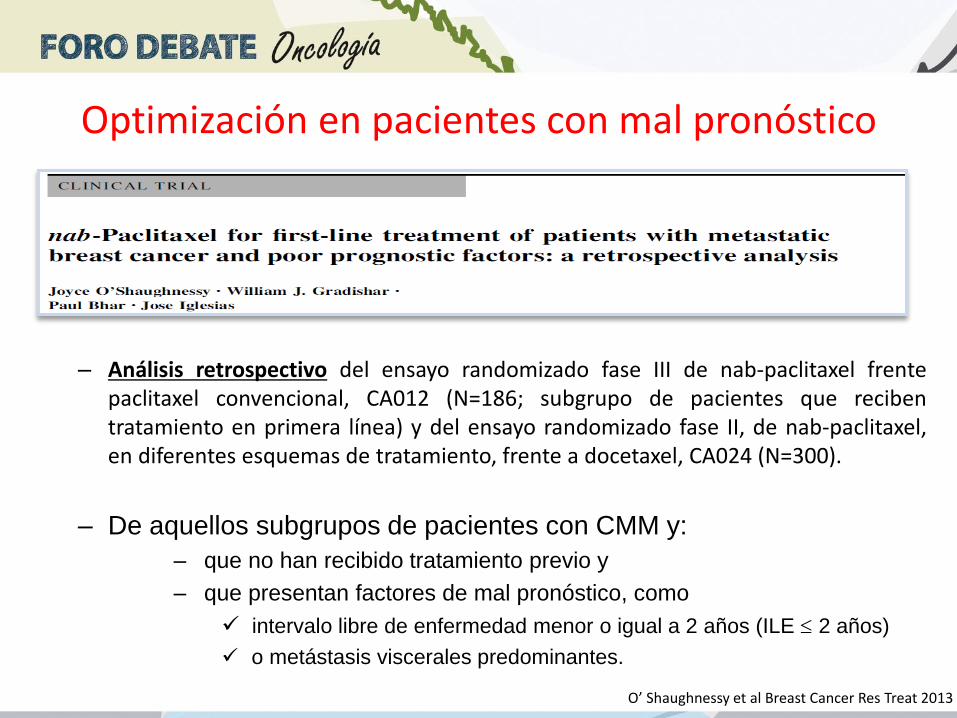
– Análisis retrospectivo del ensayo randomizado fase III de nab-paclitaxel frente paclitaxel convencional, CA012 (N=186; subgrupo de pacientes que reciben tratamiento en primera línea) y del ensayo randomizado fase II, de nab-paclitaxel, en diferentes esquemas de tratamiento, frente a docetaxel, CA024 (N=300).
– De aquellos subgrupos de pacientes con CMM y:
– que no han recibido tratamiento previo y
– que presentan factores de mal pronóstico, como
intervalo libre de enfermedad menor o igual a 2 años (ILE 2 años)
o metástasis viscerales predominantes.
Optimización en pacientes con mal pronóstico
O’ Shaughnessy et al Breast Cancer Res Treat 2013

O’Shaughnessy et al. Breast Cancer Res Treat (2013) 138:829–837.
Datos de respuesta
Optimización en pacientes con mal pronóstico
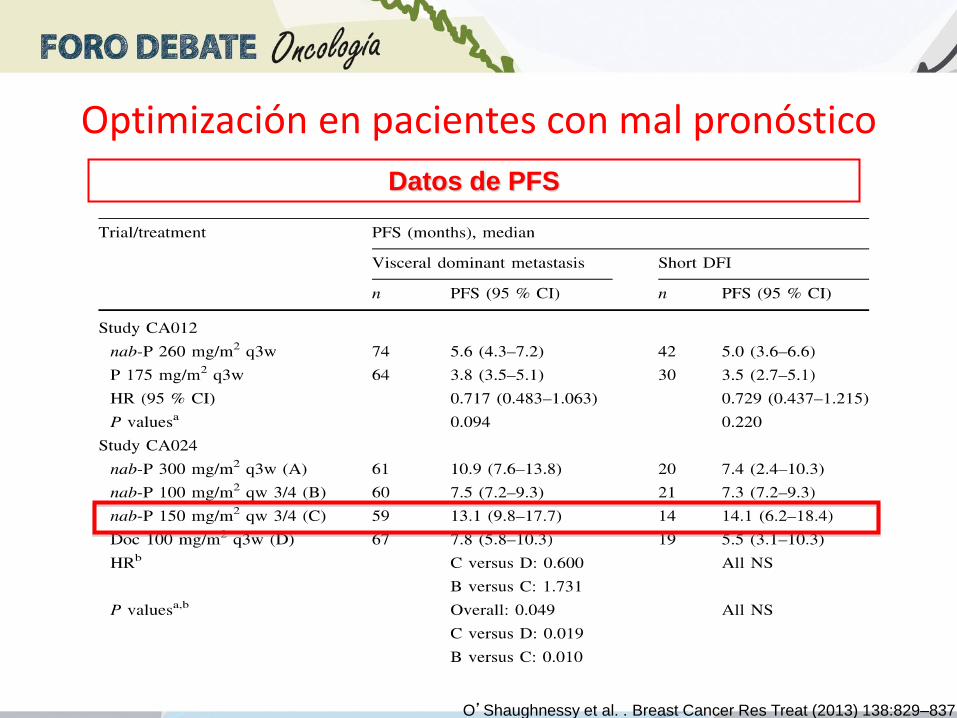
Datos de PFS
Optimización en pacientes con mal pronóstico
O’Shaughnessy et al. . Breast Cancer Res Treat (2013) 138:829–837.
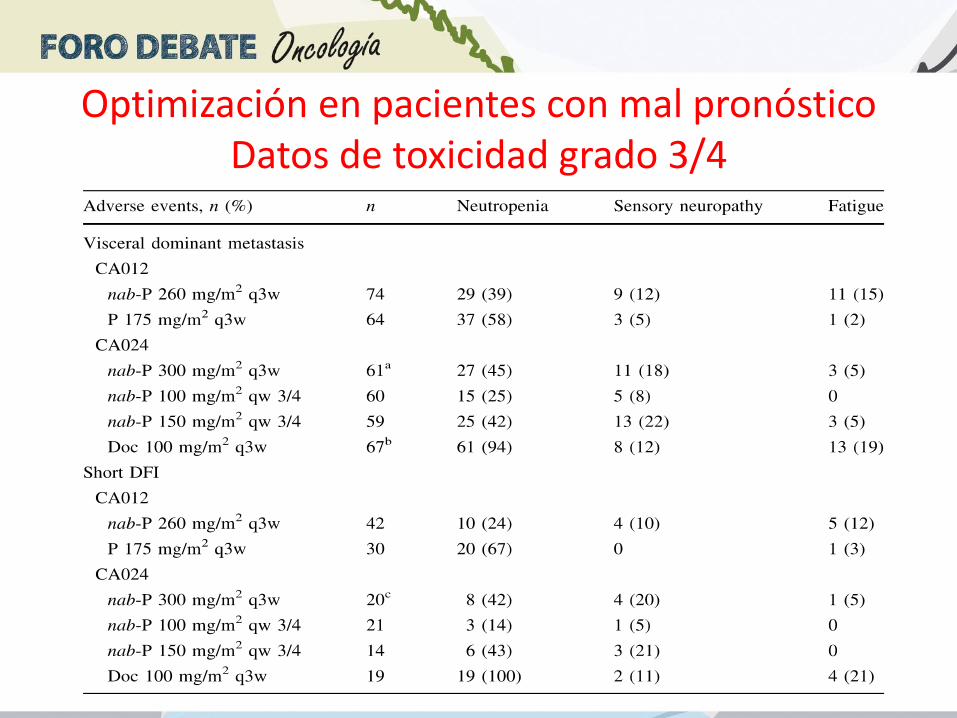
Optimización en pacientes con mal pronóstico Datos de toxicidad grado 3/4

EDAD Y TAXANOS
EFICACIA
CALIDAD DE VIDA MAS EFECTOS ADVERSOS MENOR TOLERABILIDAD COMORBILIDADES MEDICACION CONCOMITANTE
RETRASOS DE TRATAMIENTO REDUCCIONES DE DOSIS TRATAMIENTOS INACABADOS
Estudios farmacológicos de disminución de aclaramiento de paclitaxel y docetaxel an ancianos
Optimización de tratamientos con taxanos según EDAD
All patients <60 years
60-65 years > 65 years
Loibl S et al Breast Cancer Res 2008
Esquemas semanales de paclitaxel (diferentes fase II)
Menos neutropenia Astenia, Neurotoxicidad
Wildiers H, Cancer Treat Reviews 2004

• 139 pacientes con cáncer de mama metastásico. 89% en 2ª y 3ª línea de
tratamiento
– 71 ≥ 65 años (grupo 1)
– 68 < 65 años (grupo 2)
• Reducción de dosis
– Grupo 1: en 56% de pacientes la dosis de paclitaxel se redujo a 60-65
mg/m2 (en la mayoría por fatiga)
– Grupo 2: en 12% de pacientes la dosis de paclitaxel se redujo a 60-65
mg/m2 (en la mayoría por fatiga)
• Eficacia: OR similar en ambos grupos (28%), beneficio clínico 58% vs 51%
• Toxicidad:
– Grupo 1 más neutropenia (14% vs 6%), más fatiga, anemia y
trombocitopenia. Neuropatía periférica (grado 1-2) aumento con el número
de ciclos, pero similar en ambos grupos.
Gruszfeld AIJ et al. J CLin Oncol 2014
Optimización de tratamientos con taxanos según EDAD
Weekly nab-paclitaxel is safe and effective in ≥65 years old patients with
metastatic breast cancer: A post-hoc analysis
Aapro M et al The Breast 2011

Optimización según marcadores predictivos de respuesta
NO VALIDACIÓN PROSPECTIVA
ALGUNOS MÁS PREDICTIVOS DE UN FENOTIPO CLÍNICO QUE UN MARCADOR PREDICTIVO

44 patients with metastatic breast cancer treated with nabpaclitaxel.
Prospective study
- Expression of SPARC in tumor cells (integrating staining intensity and
percentage of positive tumor cells
- Expression in stroma based on staining intensity
- SPARC serum levels before first and secons cycle of nabpaclitaxel and at
progression
NO ASSOCIATION betwen expression of SPARC in primary or metastatic tumor
tissue or in serum and any clinical end-point
EFFICACY OF NABPACLITAXEL DOES NOT SEEM TO BE ASSOCIATED WITH
EXPRESSION OF SPARC IN TUMOR TISSUES OR SERUM
FOR INTERNAL USE ONLY
Not to be Shown to Physicians or Other Customers.
Not to be Used in Sales/Promotional Detailing
Schneeweiss A et al. Anticancer Research 2014
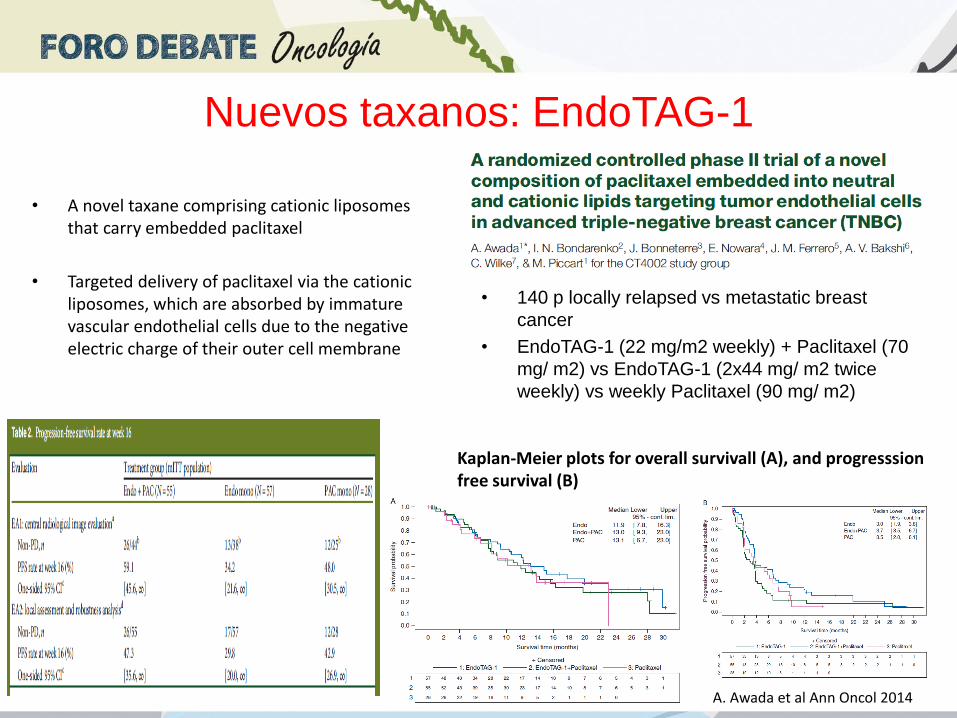
• A novel taxane comprising cationic liposomes that carry embedded paclitaxel
• Targeted delivery of paclitaxel via the cationic liposomes, which are absorbed by immature vascular endothelial cells due to the negative electric charge of their outer cell membrane
• 140 p locally relapsed vs metastatic breast
cancer
• EndoTAG-1 (22 mg/m2 weekly) + Paclitaxel (70
mg/ m2) vs EndoTAG-1 (2x44 mg/ m2 twice
weekly) vs weekly Paclitaxel (90 mg/ m2)
Kaplan-Meier plots for overall survivall (A), and progresssion free survival (B)
A. Awada et al Ann Oncol 2014
Nuevos taxanos: EndoTAG-1

Nuevos taxanos: EndoTAG-1
A. Awada et al Ann Oncol 2014

Nuevos taxanos: Tesetaxel
• Taxano oral semisintético
• No asociado a reacciones de hipersensibilidad, y neuropatía no prominente
• Severa neutropenia, estudios con mortalidad, frenaron su aprobación por FDA
• Estudio fase II en primera línea de metastásico (Seidman A Proc ASCO 2012)

Conclusiones • Los taxanos (docetaxel, paclitaxel y nabpaclitaxel) constituyen
unos de los agentes más activos en cáncer de mama
• Un alto porcentaje de nuestras pacientes habrán recibido taxanos de forma adyuvante/ neoadyuvante
• En cáncer de mama metastásico, el retratamiento con taxanos supondrá una alternativa de tratamiento de entre las múltiples opciones
• En ese caso es importante su optimización considerando: tratamientos previos recibidos, edad, carga tumoral, subtipo biológico, perfil de efectos adversos previo