nuevas drogas en cáncer de mama metastásico her-2 positivo€¦ · detención del ciclo celular y...
TRANSCRIPT

Nuevas Drogas en Cáncer de Mama
Metastásico HER-2 positivo
XX Congreso de la S.A.C. 2016

Clasificación molecular del Ca mama
HER-2 Basal-like Luminal A Luminal B Normal
Perou CM, Sorlie T, et al. Nature 2000; 406: 747
HER-2

HER-2: el comienzo de la historia

Vía de señalización HER-2
trastuzumab
sobreexpresado
ó amplificado
en ~ 20 %
Immune System
ADCC

SLP: 7.4 vs 4.6 (P= <0.001) SG: 25.1 vs 20.3 (p= 0.046)
QT
+HER
QT AC
+HER
AC Px
+HER
Px
RC 8% 3% 8% 4% 8% 2%
RP 42% 29% 48% 38% 34% 15%
RO 50% 32% 56% 42% 42% 17%
Ensayo pivotal H0648g

Dawood S, JCO 2010
HER2+
HER2+ MBC: worse survival
Prognosis of metastatic breast cancer by HER2 status and
trastuzumab treatment
13%
25%
Trastuzumab
No Trastuzumab
HER2+

Inh. Tirosin Quinasa (TKI): Lapatinib
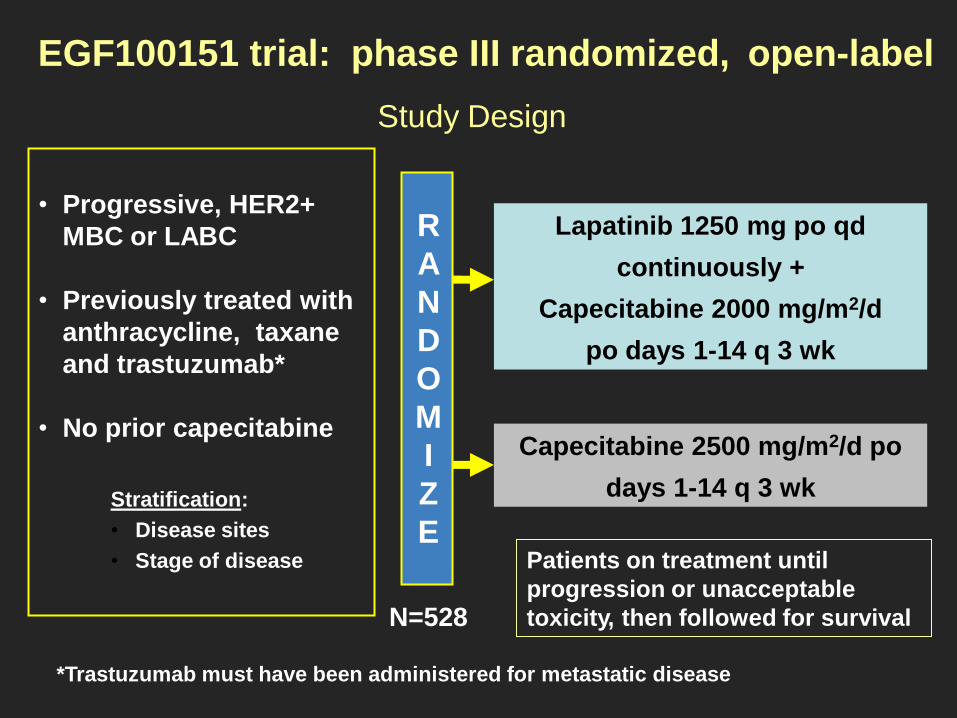
• Progressive, HER2+
MBC or LABC
• Previously treated with
anthracycline, taxane
and trastuzumab*
• No prior capecitabine
Lapatinib 1250 mg po qd
continuously +
Capecitabine 2000 mg/m2/d
po days 1-14 q 3 wk
Capecitabine 2500 mg/m2/d po
days 1-14 q 3 wk
Patients on treatment until
progression or unacceptable
toxicity, then followed for survival
Stratification:
• Disease sites
• Stage of disease
R
A
N
D
O
M
I
Z
E
*Trastuzumab must have been administered for metastatic disease
N=528
EGF100151 trial: phase III randomized, open-label
Study Design

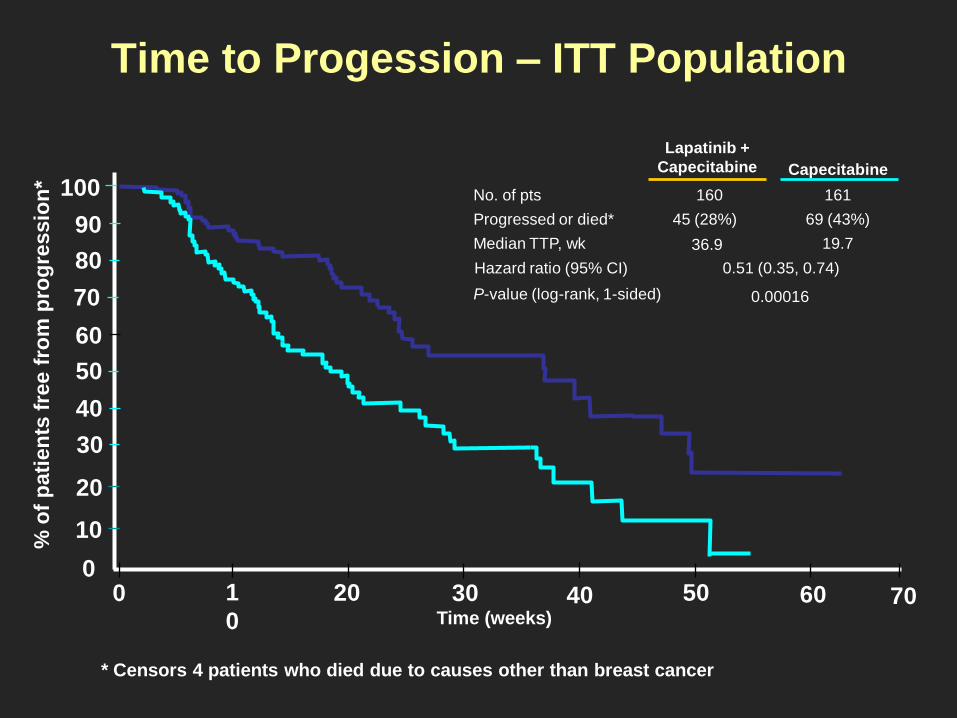
Time to Progession – ITT Population
70
10
20
30
40
50
60
70
80
90
0
100
Se cerró la randomización y sin diferencias significativas en SG (L+C se autorizó en 2ª línea)
1
0
20 30 40 50 60 0 Time (weeks)
Capecitabine
Lapatinib +
Capecitabine
0.00016 P-value (log-rank, 1-sided)
69 (43%) 45 (28%) Progressed or died*
19.7 36.9 Median TTP, wk
161 160 No. of pts
0.51 (0.35, 0.74) Hazard ratio (95% CI)
% o
f p
ati
en
ts f
ree f
rom
pro
gre
ssio
n
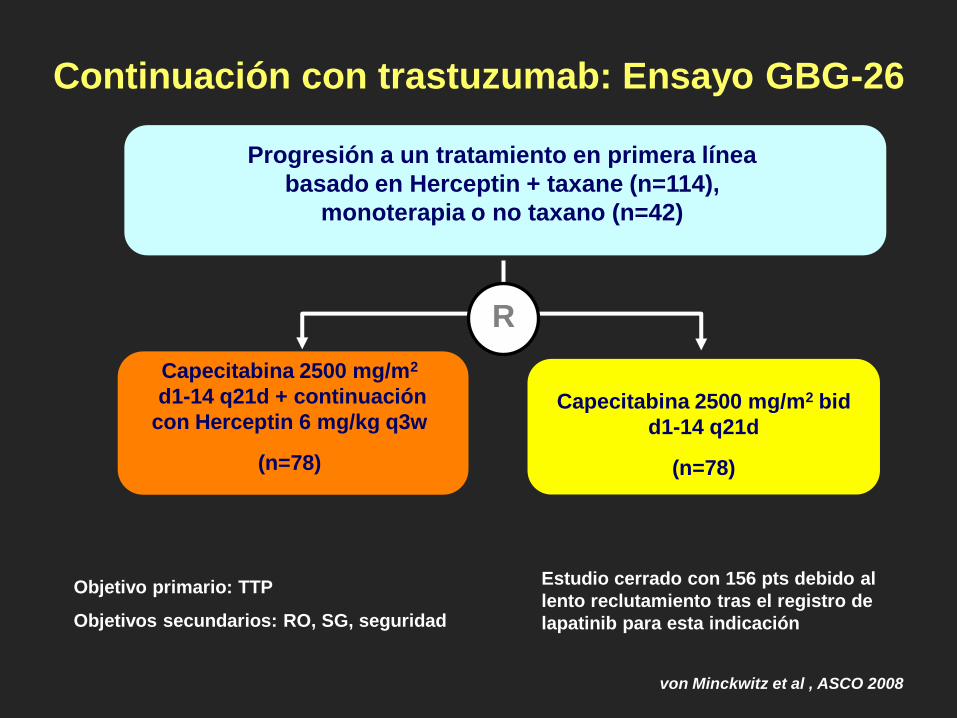
Continuación con trastuzumab: Ensayo GBG-26
von Minckwitz et al , ASCO 2008
Capecitabina 2500 mg/m2
d1-14 q21d + continuación
con Herceptin 6 mg/kg q3w
(n=78)
Progresión a un tratamiento en primera línea
basado en Herceptin + taxane (n=114),
monoterapia o no taxano (n=42)
Capecitabina 2500 mg/m2 bid
d1-14 q21d
(n=78)
R
Objetivo primario: TTP
Objetivos secundarios: RO, SG, seguridad
Estudio cerrado con 156 pts debido al
lento reclutamiento tras el registro de
lapatinib para esta indicación

Tiempo (semanas)
Probabilidad
TTP
24.3
(5.6 m)
36.9
(8.2 m)
120 10 0 20 40 50 60 70 80 100 30 90 110
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0 Herceptin® + Xeloda® (n=78)
Xeloda® (n=78)
Continuación con trastuzumab: Ensayo GBG-26
von Minckwitz et al , ASCO 2008
p= 0,034
HR= 0,69

HER2+RH+: HT + lapatinib or trastuzumab

RE+
65-75%
mTOR inhibitors
CDK 4/6 inhibitors
HER-2 la historia continúa: Presente
Nuevos fármacos según subtipo tumoral
Pertuzumab
TDM-1
Combinaciones AntiHER2
Triple negativo
15%
HER2+
15- 20 %
Nuevos citostáticos (Eribulina)
Sales de platino
Bevacizumab

Homodímeros Heterodímeros
Los dímeros HER2:HER3 inician la señal
mitogénica más potente
HER1:HER1
HER2:HER2 HER3:HER3
HER4:HER4 HER1:HER2 HER1:HER3
HER1:HER4
HER2:HER4
HER3:HER4
Tzahar et al. Mol Cell Biol 1996;16:5276–5287; Citri et al. Exp Cell Res 2003;284:54–65; Huang et al. Cancer Res 2010;70:1204–1214.
activar señalización intracelular
+ + + + + + + + + + + + + + + +
+
HER2:HER3
Precisan dimerizarse para

Control
Tratadas con gefitinib
0
20
40
60
80
100
120
140
No transfectadas Control Anti-HER3 siRNA
Cé
lula
s q
ue
su
fre
n a
po
pto
sis
(%
de
l to
tal)
p-HER2
0 1 4 12 24 48 96
p-HER3
Horas desde la adición de gefitinib
El bloqueo de la actividad de HER1
y HER2 por los TKi (p. ej., gefitinib)
da lugar a un aumento de la
actividad HER3
TKi = inhibidor de la tirosin quinasa; p-HER = HER fosforilado
Baselga et al. Cancer Cell 2002;2;93–95
Sergina et al. Nature 2007;445:437–44
HER3 ofrece una vía de escape para el Ca mama
Inhibicion HER1 y HER2 por TKi
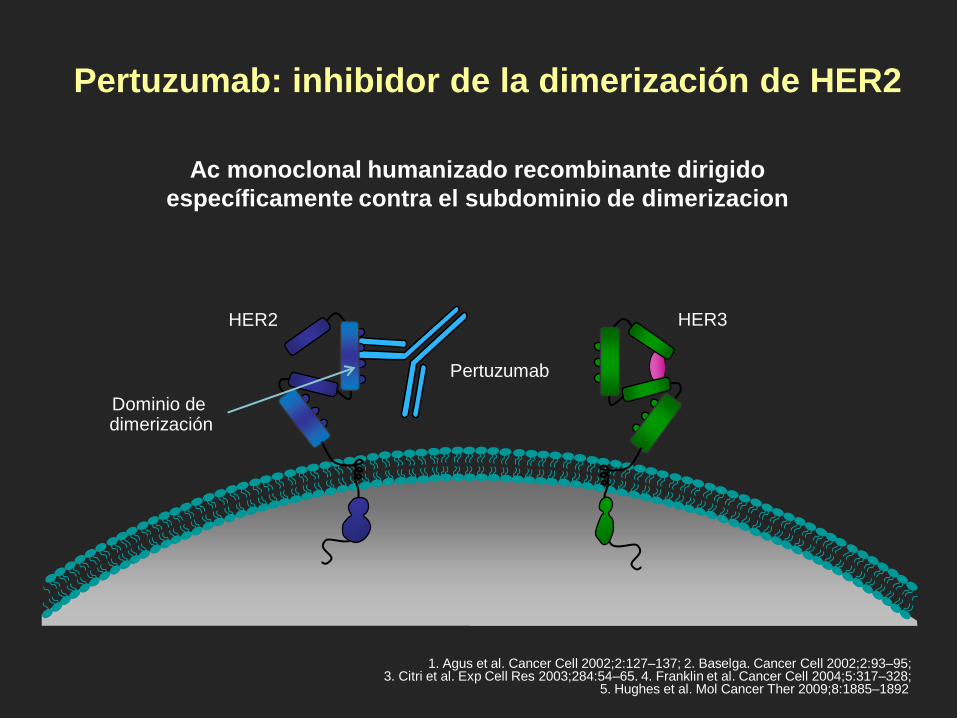
Pertuzumab: inhibidor de la dimerización de HER2
HER2
Dominio de dimerización
1. Agus et al. Cancer Cell 2002;2:127–137; 2. Baselga. Cancer Cell 2002;2:93–95; 3. Citri et al. Exp Cell Res 2003;284:54–65. 4. Franklin et al. Cancer Cell 2004;5:317–328;
5. Hughes et al. Mol Cancer Ther 2009;8:1885–1892
Pertuzumab
HER3
Ac monoclonal humanizado recombinante dirigido
específicamente contra el subdominio de dimerizacion

Trastuzumab y pertuzumab se unen a diferentes epítopos de
HER2 y presentan mecanismos de acción complementarios
HER2
Dominio de dimerización
Cho et al. Nature 2003;421:756–760; Fendly et al. Cancer Res 1990;50:1550–1558; Franklin et al. Cancer Cell 2004;5:317–328; Nahta et al. Cancer Res 2004;64:2343–2346; Scheuer et al. Cancer Res 2009;69:9330–9336
Pertuzumab
HER3
Trastuzumab
Subdominio IV
Trastuzumab inhibe la señalización de HER2
independiente de ligando y marca las células
para su destrucción por el sistema inmunitario
• Pertuzumab inhibe la dimerización de HER2 activada por ligando
• Pertuzumab marca las células para su destrucción por el sistema inmunitario
P + T causa un bloqueo más completo de la señalización dirigida por HER2

Diseño del estudio
• La randomización se realizó según la región geográfica y el tratamiento previo
(recibió o no recibió quimioterapia neo/adyuvante)
• Dosificación del estudio c3s:
- Pertuzumab/placebo: 840 mg como dosis de carga, 420 mg de mantenimiento
- Trastuzumab: 8 mg/kg como dosis de carga, 6 mg/kg de mantenimiento
- Docetaxel: 75 mg/m2, aumentando hasta 100 mg/m2 si se tolera
1ª Linea CMM HER2-positivo
con confirmacion central
(N = 808)
Placebo + trastuzumab
1:1
Docetaxel*
recomendado ≥6 ciclos
n = 406
n = 402
Pertuzumab + trastuzumab
Docetaxel*
recomendado ≥6 ciclos
*<6 ciclos permitido en caso de toxicidad inaceptable o EP; >6 ciclos permitido a valoración del investigador
PD
PD
- No se permitía
tto hormonal.
-Tto adyuvante
con IL>12 meses
90 % pts no trastuzumab
en adyuvancia

Objetivo principal: SLP por comité de revisión independiente
Mediana de seguimiento: 19,3 meses1
0 5 10 15 20 25 30 35 40
0
10
20
30
40
50
60
70
80
90
100
n en riesgo
402 345 267 139 83 32 10 0 0 Ptz + T + D
406 311 209 93 42 17 7 0 0 Pla + T + D
Tiempo (meses)
Pertuzumab + T + D: mediana 18,5 meses
Pla + T + D: mediana 12,4 meses
HR = 0,62
IC 95 % 0,51‒0,75
p < 0,0001
∆ = 6,1 meses
Su
perv
iven
cia
Lib
re d
e P
rog
resió
n
(%)
D: docetaxel; SLP: Supervivencia Libre de Progresión; Pla: placebo; Ptz: pertuzumab; T: trastuzumab 1-Baselga J, et al. N Engl J Med 2012; 366:109–119

Respuesta objetiva revisada de forma independiente
Pacientes con enfermedad medible al inicio del estudio
Placebo
+ trastuzumab
+ docetaxel
(n = 336)
Pertuzumab
+ trastuzumab
+ docetaxel
(n = 343)
Tasa de respuesta objetiva, n (%)
Tasa de respuesta completa, n (%)
Tasa de respuesta parcial, n (%)
233 (69,3)
14 (4,2)
219 (65,2)
275 (80,2)
19 (5,5)
256 (74,6)
p = 0,0011*
Enfermedad estable, n (%) 70 (20,8) 50 (14,6)
Progresión de la enfermedad, n (%) 28 (8,3) 13 (3,8)
Evaluación imposible o no
disponible, n (%) 5 (1,5) 5 (1,5)
* El resultado de la prueba estadística se considera exploratorio


SLP valorada por el comité de revisión independiente
en los subgrupos predefinidos
Todos
No Sí
Europa Norteamérica
Sudamérica Asia
<65 años ≥65 años
<75 años ≥75 años
Blancos Negros
Asiáticos Otros
Enfermedad visceral
Positivo Negativo
Desconocido
IHQ 3+ FISH-positivo
A favor de placebo A favor de pertuzumab
0 1 2 3 0,5
Estado RE/RP
Tipo de enfermedad
Raza
Grupo de edad
Región
Quimioterapia (neo)adyuvante previa
Estado HER2
808 0,63 0,52‒0,76
432 0,63 0,49‒0,82 376 0,61 0,46‒0,81
306 0,72 0,53‒0,97 135 0,51 0,31‒0,84 114 0,46 0,27‒0,78 253 0,68 0,48‒0,95
681 0,65 0,53‒0,80 127 0,52 0,31‒0,86 789 0,64 0,53‒0,78 19 0,55 0,12‒2,54
480 0,62 0,49‒0,80 30 0,64 0,23‒1,79 261 0,68 0,49‒0,95 37 0,39 0,13‒1,18
630 0,55 0,45‒0,68 178 0,96 0,61‒1,52
388 0,72 0,55‒0,95 408 0,55 0,42‒0,72
12 - -
721 0,60 0,49‒0,74
767 0,64 0,53‒0,78
n HR IC 95 %
RE: receptor de estrógenos; IHQ: inmunohistoquímica; FISH: hibridación in situ con fluorescencia; RP: receptor de progesterona
Enfermedad no visceral

PHEREXA study design (NCT01026142)
Herceptin (8 mg/kg→6 mg/kg) + Xeloda (1,250
mg/m2)
n = 224
• HER2-positive MBC (centrally confirmed)
• Prior taxane and Trastuzumab
• Progression during or after H-based therapy for MBC
N = 452
1
1
Herceptin (8 mg/kg→6 mg/kg) + Xeloda (1,000
mg/m2)
+ Pertuzumab (840 mg→420 mg)
n = 228
First pt included: Jan 30, 2010 Last pt included: Aug 12, 2013 Clinical cut-off: May 29, 2015
Arm A: H + X
(n = 224)
Arm B: H + X + P
(n = 228)
Events, n (%) 158 (71) 168 (74)
mPFS (months) 9.0 11.1
∆ (months) 2.1
HR (95% CI)a 0.82 (0.65–1.02)
Log-rank p-valuea 0.07
mFU (months) 28.6 25.3

T- DM1: fármaco conjugado (Ac - Qt)
• Trastuzumab dirige el agente
quimioterápico (DM1)
directamente hasta el interior de
las células neoplásicas
• DM1 es un maitansinoide, un
derivado del fármaco anti-
microtúbulos maitansina1
• DM1 se une directamente a los
microtúbulos para inhibir su
polimerización, causando la
detención del ciclo celular y la
consiguiente muerte celular2 por
apoptosis
DM1
1. Junttila TT, et al. Breast Cancer Res Treat 2011; 128: 347.

T-DM1 binds to the HER2
protein on cancer cells
Receptor-T-DM1 complex is
internalised into HER2-
positive cancer cell
Potent antimicrotubule
agent is released once
inside the HER2-positive
tumour cell
T-DM1. Mecanismo de Acción
Adapted from LoRusso PM, et al. Clin Cancer Res 2011.
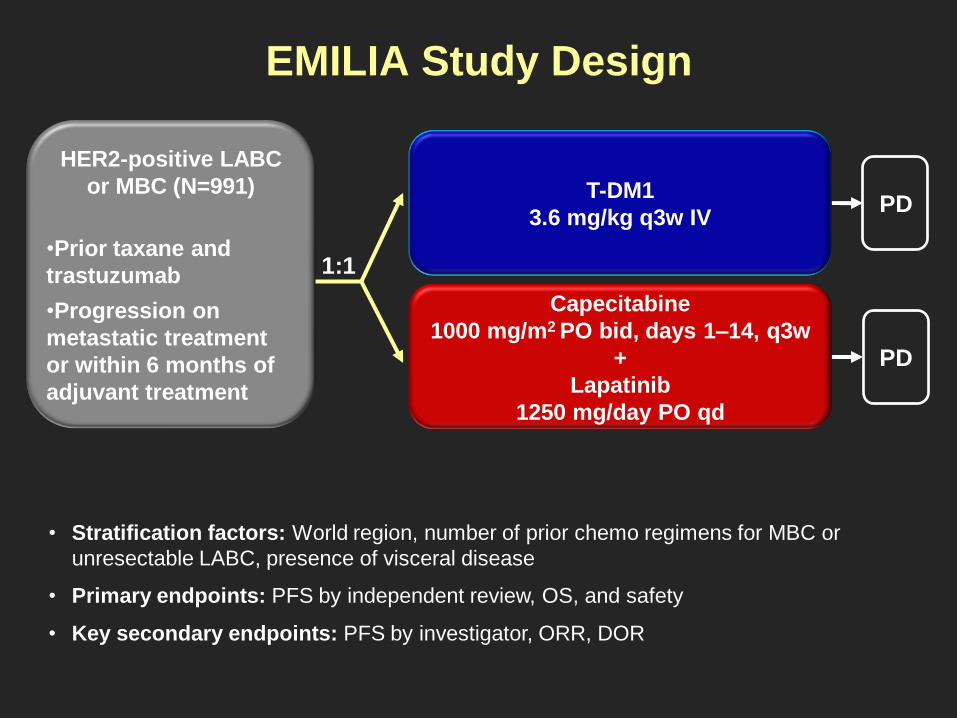
EMILIA Study Design
• Stratification factors: World region, number of prior chemo regimens for MBC or
unresectable LABC, presence of visceral disease
• Primary endpoints: PFS by independent review, OS, and safety
• Key secondary endpoints: PFS by investigator, ORR, DOR
1:1
HER2-positive LABC
or MBC (N=991)
•Prior taxane and
trastuzumab
•Progression on
metastatic treatment
or within 6 months of
adjuvant treatment
PD
T-DM1
3.6 mg/kg q3w IV
Capecitabine
1000 mg/m2 PO bid, days 1–14, q3w
+
Lapatinib
1250 mg/day PO qd
PD

Progression-Free Survival by Independent Review
496 404 310 176 129 73 53 35 25 14 9 8 5 1 0 0
495 419 341 236 183 130 101 72 54 44 30 18 9 3 1 0
Cap + Lap
T-DM1
No. at risk by independent review:
Median
(months)
No. of
events
Cap + Lap 6.4 304
T-DM1 9.6 265
Stratified HR=0.650 (95% CI, 0.55, 0.77)
P<0.0001
0.0
0.2
0.4
0.6
0.8
1.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
Pro
po
rtio
n p
rog
ressio
n-f
ree
Time (months)
Unstratified HR=0.66 (P<0.0001).

Overall Survival: Confirmatory Analysis
496 471 453 435 403 368 297 240 204 159 133 110 86 63 45 27 17 7 4
495 485 474 457 439 418 349 293 242 197 164 136 111 86 62 38 28 13 5
Cap + Lap
T-DM1
No. at risk: Time (months)
78.4% 64.7%
51.8%
85.2%
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n s
urv
ivin
g
Data cut-off July 31, 2012; Unstratified HR=0.70 (P=0.0012).
Median (months) No. of events
Cap + Lap 25.1 182
T-DM1 30.9 149
Stratified HR=0.682 (95% CI, 0.55, 0.85); P=0.0006
Efficacy stopping boundary P=0.0037 or HR=0.727

Objective response rate (ORR)
Duration of response (DOR)
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n p
rog
ressio
n-f
ree
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
Median, months (CI)
Cap +
Lap 6.5 (5.5, 7.2)
T-DM1 12.6 (8.4, 20.8)
P=0.0002
120 105 77 48 32 14 9 8 3 3 1 1 0 0 0 0
173 159 126 84 65 47 42 33 27 19 12 8 2 0 0 0
Cap + Lap
T-DM1
No. at risk
0
0
0
0
0
0
Time (months)
Pati
en
ts,
%
0
20
30
40
50
10
T-DM1
173/397 120/389
43.6%
30.8%
Cap + Lap
EMILIA trial: Results
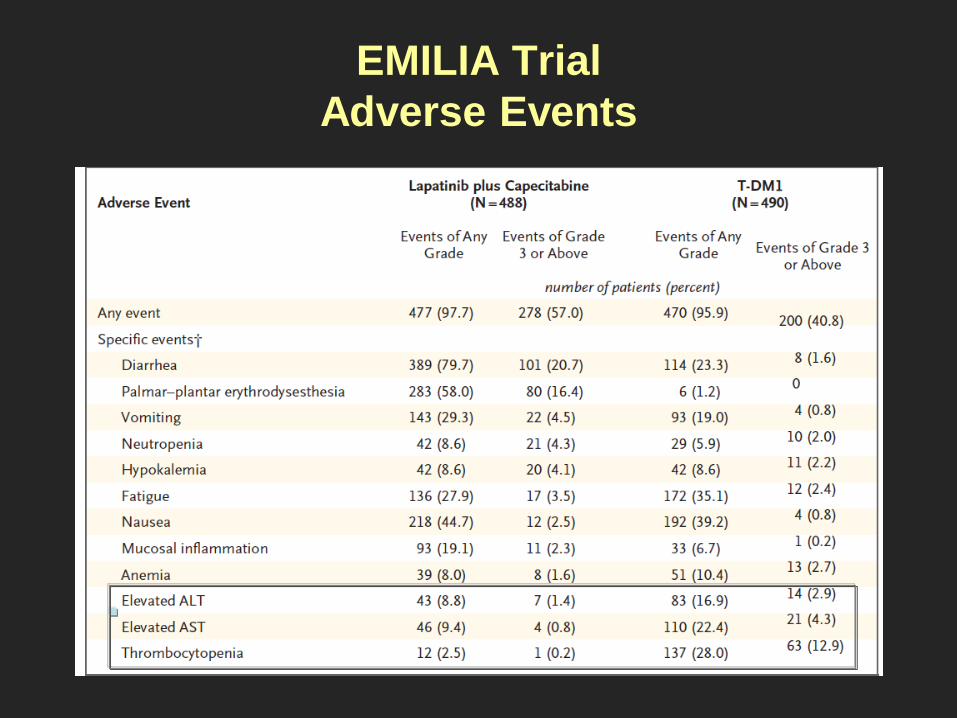
EMILIA Trial
Adverse Events

2
T-DM1c (optional
crossover)
TH3RESA Study Schema
• Stratification factors: World region, number of prior regimens for advanced BC,d
presence of visceral disease
• Co-primary endpoints: PFS by investigator and OS
• Key secondary endpoints: ORR by investigator and safety
PD
PD T-DM1
3.6 mg/kg q3w IV (n=400)
Treatment of
physician’s choice
(TPC)b
(n=200)
HER2-positive (central)
advanced BCa
(N=600)
≥2 prior HER2-directed
therapies for advanced BC
Prior treatment with
trastuzumab, lapatinib,
and a taxane
a Advanced BC includes MBC and unresectable locally advanced/recurrent BC.
b TPC could have been single-agent chemotherapy, hormonal therapy, or HER2-directed therapy, or a combination of a HER2-directed therapy with
a chemotherapy, hormonal therapy, or other HER2-directed therapy. c First patient in: Sep 2011. Study amended Sep 2012 (following EMILIA 2nd interim OS results) to allow patients in the TPC arm to receive
T-DM1 after documented PD. d Excluding single-agent hormonal therapy.
1

PFS by Investigator Assessment
Median follow-up: TPC, 6.5 months; T-DM1, 7.2 months.
Unstratified HR=0.521 (P<0.0001).
198 120 62 28 13 6 1 0
404 334 241 114 66 27 12 0
TPC
T-DM1
No. at risk: Time (months)
14 12 10 8 6 4 2
0.0
0.2
0.4
0.6
0.8
1.0
0
Pro
po
rtio
n p
rog
ressio
n-f
ree
TPC
(n=198)
T-DM1
(n=404)
Median (months) 3.3 6.2
No. of events 129 219
Stratified HR=0.528 (95% CI, 0.422, 0.661)
P<0.0001
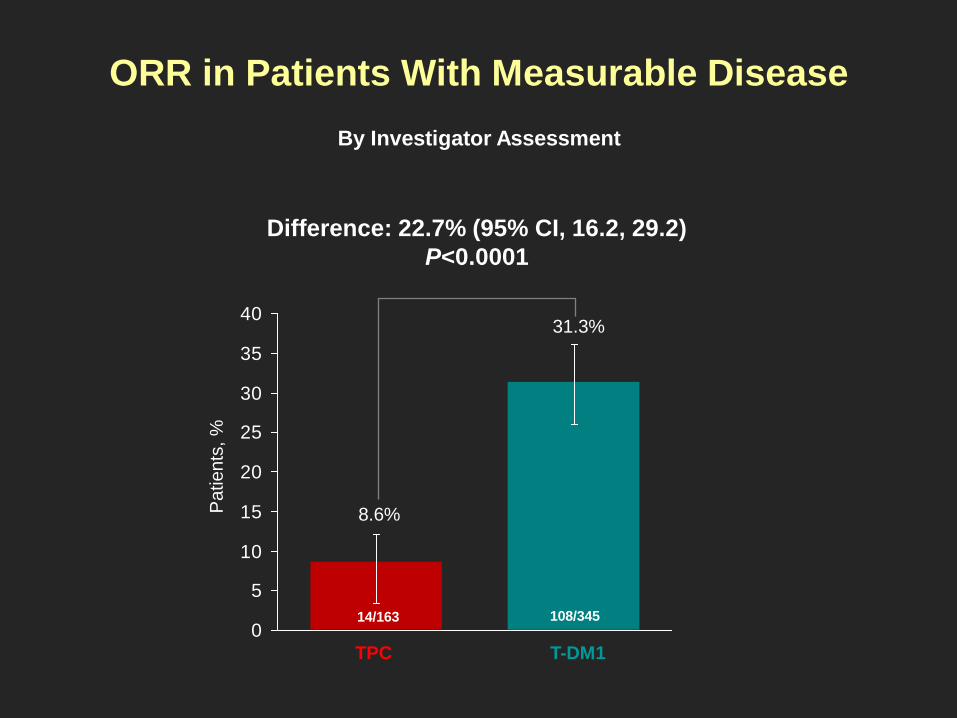
ORR in Patients With Measurable Disease
Difference: 22.7% (95% CI, 16.2, 29.2)
P<0.0001
Patients
, %
0
5
10
15
20
25
30
35
40
T-DM1 TPC
31.3%
8.6%
108/345 14/163
By Investigator Assessment

Final Overall Survival Analysis
TPC
T-DM1
No. at risk Time (months)
40 34 28 22 16 12 2
0.0
0.2
0.4
0.6
0.8
1.0
0
Pro
po
rtio
n s
urv
ivin
g
TPC
(n=198)
T-DM1
(n=404)
Median (months) 15.8 22.7
Stratified HR=0.68 (95% CI: 0.54–0.85)
P=0.0007 (Prespecifed crossing boundary: HR<0.748;
P<0.012)
4 6 8 10 14 18 20 24 26 30 32 36 38
0 6 39 62 80 107 168 198 150 131 122 115 93 68 66 59 51 28 16 1 0
0 25 132 179 226 280 388 404 368 347 321 298 251 207 192 167 164 84 54 12 2

Combinación de fármacos anti-HER2
• Treatment with lapatinib plus trastuzumab
resulted in complete tumor remission
– Effect was durable: no tumor relapse
observed after 8 mo post treatment
• Lapatinib induced accumulation of
inactive HER2 at plasma membrane
– Trastuzumab-mediated cytotoxicity
was higher with the addition of
lapatinib in MCF7/HER2 cells
• In vivo activity was consistent with in vitro
data demonstrating the Combination of
Lapatinib and Trastuzumab has
Synergistic Anti-tumor Activity.
Scaltriti, et al. Oncogene 2009;28(6):803-814, Konecny, et al. Cancer Res 2006;66:1630-1639; Xia, et al.Oncogene 2004;23: 646–653
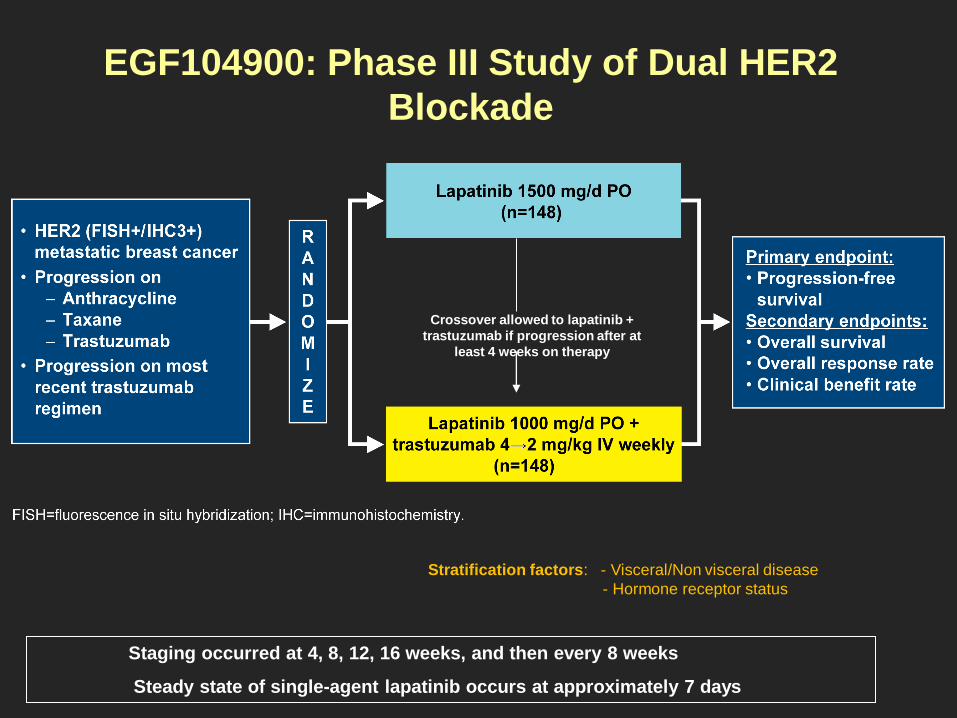
EGF104900: Phase III Study of Dual HER2
Blockade
Staging occurred at 4, 8, 12, 16 weeks, and then every 8 weeks
Steady state of single-agent lapatinib occurs at approximately 7 days
Crossover allowed to lapatinib +
trastuzumab if progression after at
least 4 weeks on therapy
Stratification factors: - Visceral/Non visceral disease
- Hormone receptor status
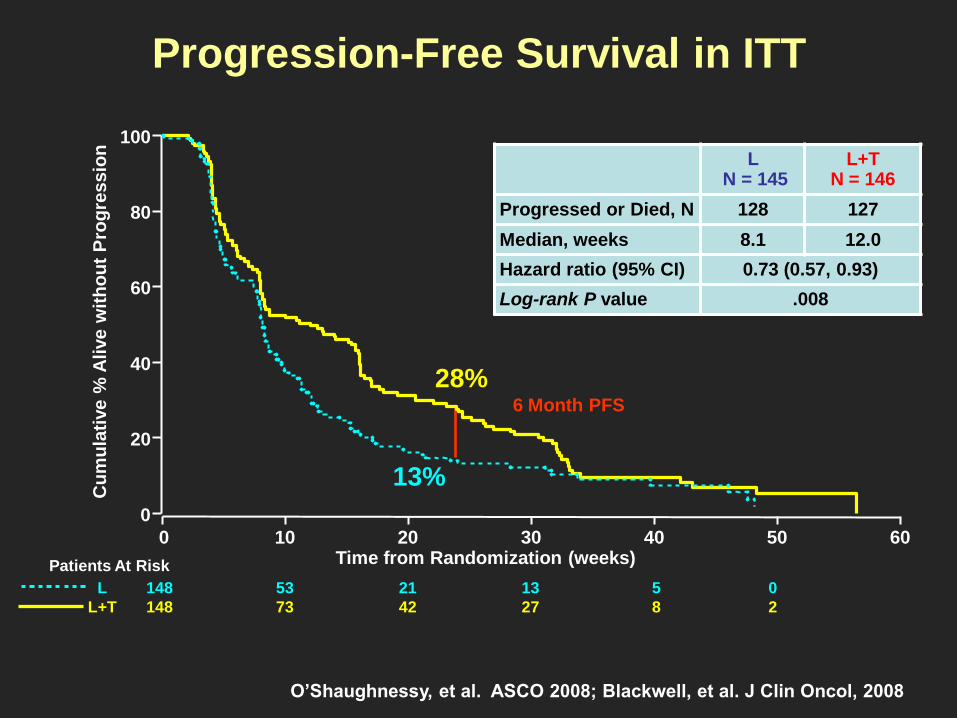
Progression-Free Survival in ITT
L N = 145
L+T N = 146
Progressed or Died, N 128 127
Median, weeks 8.1 12.0
Hazard ratio (95% CI) 0.73 (0.57, 0.93)
Log-rank P value .008
6 Month PFS
Cu
mu
lati
ve %
Alive w
ith
ou
t P
rog
ressio
n
Patients At Risk
148
148
L
L+T
53
73
21
42
13
27
5
8
0
2
13%
28%
0
20
40
60
80
100
0 10 20 30 40 50 60Time from Randomization (weeks)
O’Shaughnessy, et al. ASCO 2008; Blackwell, et al. J Clin Oncol, 2008

L N =145
L+T N =146
Died, N (%) 113 (78) 105 (72)
Median, months 9.5 14
Hazard ratio (95% CI) 0.74 (0.57, 0.97)
Log-rank P value .026 6 Month OS
80%
70%
12 Month OS
56%
41%
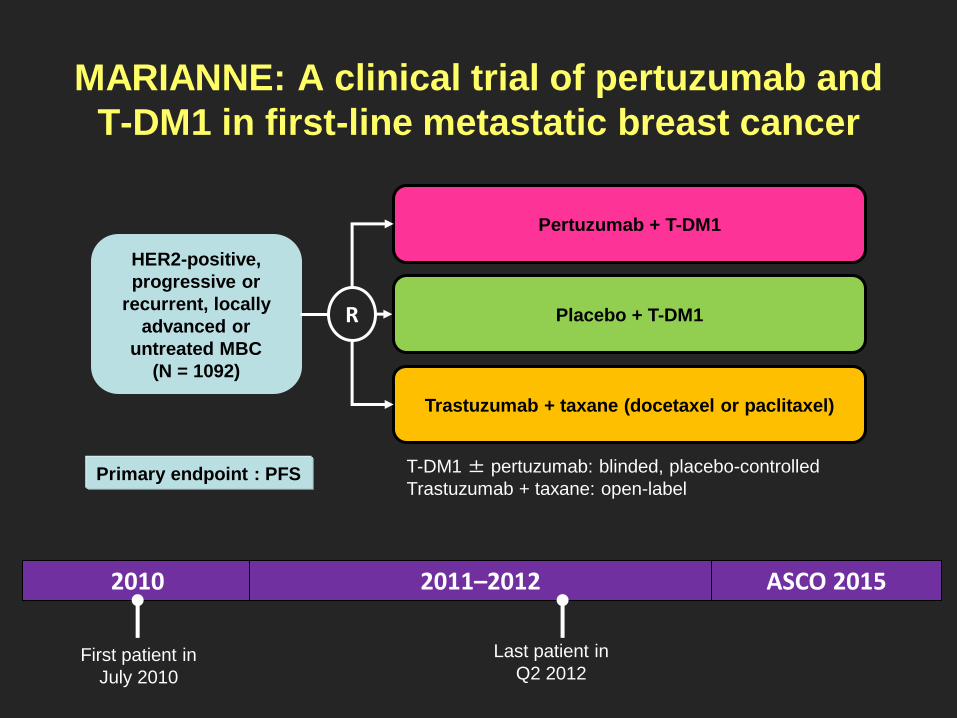
MARIANNE: A clinical trial of pertuzumab and
T-DM1 in first-line metastatic breast cancer
HER2-positive,
progressive or
recurrent, locally
advanced or
untreated MBC
(N = 1092)
Pertuzumab + T-DM1
Trastuzumab + taxane (docetaxel or paclitaxel)
R Placebo + T-DM1
2010 2011–2012 ASCO 2015
First patient in
July 2010
Last patient in
Q2 2012
T-DM1 ± pertuzumab: blinded, placebo-controlled
Trastuzumab + taxane: open-label Primary endpoint : PFS



Cross-Talk Between Signal Transduction
and Endocrine Pathways
Adapted from: Johnston SRD. Clin Cancer Res. 205;11:889s-899s.
Enfermedad HER-2 + y RH +
Crosstalk vías HER-2 y RE: resistencia endocrina
Habría que actuar sobre ambas vías para superar resistencia

Ensayo TAnDEM: Anastrozol +/- Trastuzumab
RESPUESTAS OBJETIVAS
RE+ con confirmacion central

EGF30008 trial:
Letrozol +/- Lapatinib en
CMM HER-2 positivo
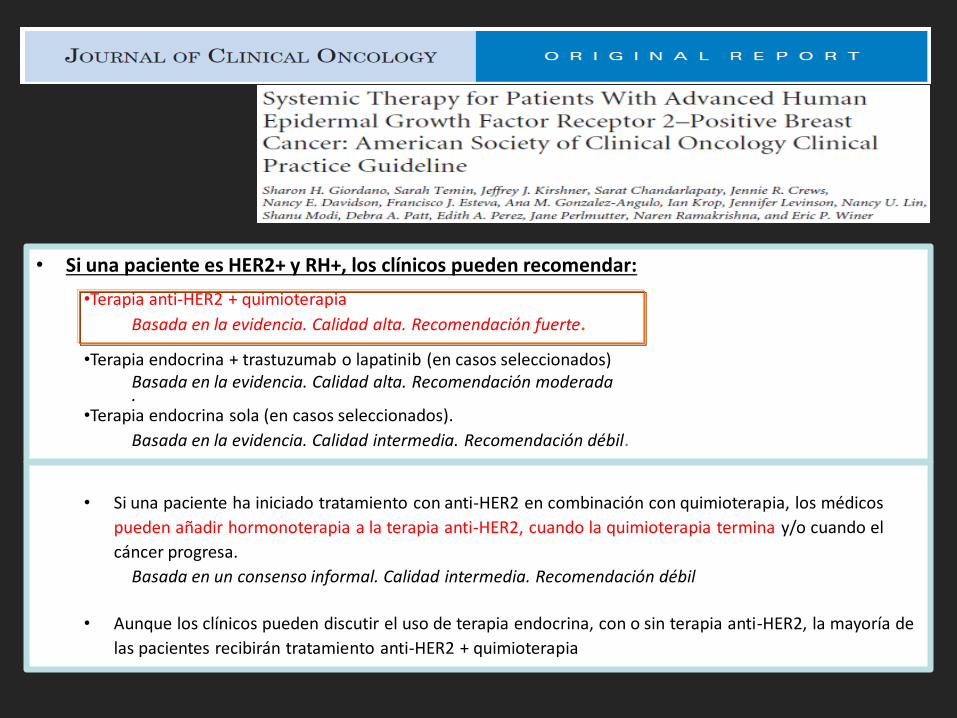
• Si una paciente es HER2+ y RH+, los clínicos pueden recomendar:
•Terapia anti-HER2 + quimioterapia
Basada en la evidencia. Calidad alta. Recomendación fuerte.
•Terapia endocrina + trastuzumab o lapatinib (en casos seleccionados) Basada en la evidencia. Calidad alta. Recomendación moderada .
•Terapia endocrina sola (en casos seleccionados).
Basada en la evidencia. Calidad intermedia. Recomendación débil.
• Si una paciente ha iniciado tratamiento con anti-HER2 en combinación con quimioterapia, los médicos
pueden añadir hormonoterapia a la terapia anti-HER2, cuando la quimioterapia termina y/o cuando el
cáncer progresa.
Basada en un consenso informal. Calidad intermedia. Recomendación débil
• Aunque los clínicos pueden discutir el uso de terapia endocrina, con o sin terapia anti-HER2, la mayoría de
las pacientes recibirán tratamiento anti-HER2 + quimioterapia

PERTAIN trial design (NCT01491737)

MAPK PI3K
p27-cdk2
cyclin D1
Alterations in downstream
molecules: PTEN downregulation,
increased Akt signaling, reduced
p27kip1
HER-2
Increased receptor signaling:
HER members, IGF-IR
Potential Molecular Mechanisms
of Trastuzumab Resistance
Disrupted antibody-
receptor interaction
Potential antineoplastic activity:
Inmune System
HER-2 la historia continúa: Futuro

HER-2 y vía PI3K-mTOR
Mutaciones activantes de PI3kCA y/o pérdida de expresión de PTEN
en un 20-50 % de pts con CMM HER-2 positivo

BOLERO-1 trial


Neratinib is an oral, irreversible TKI, targeting HER2,
HER4 and EGFR kinases
240 mg daily was the neratinib dose selected for phase
II trials: - diarrehea es the main toxicity

NALA trial

Fármacos conjugados: MM-302

HERMIONE study

Sistema inmunitario y terapia anti-HER2
Capacidad de los tumores para eludir la respuesta del sistema inmune


HER-2: el viaje continúa
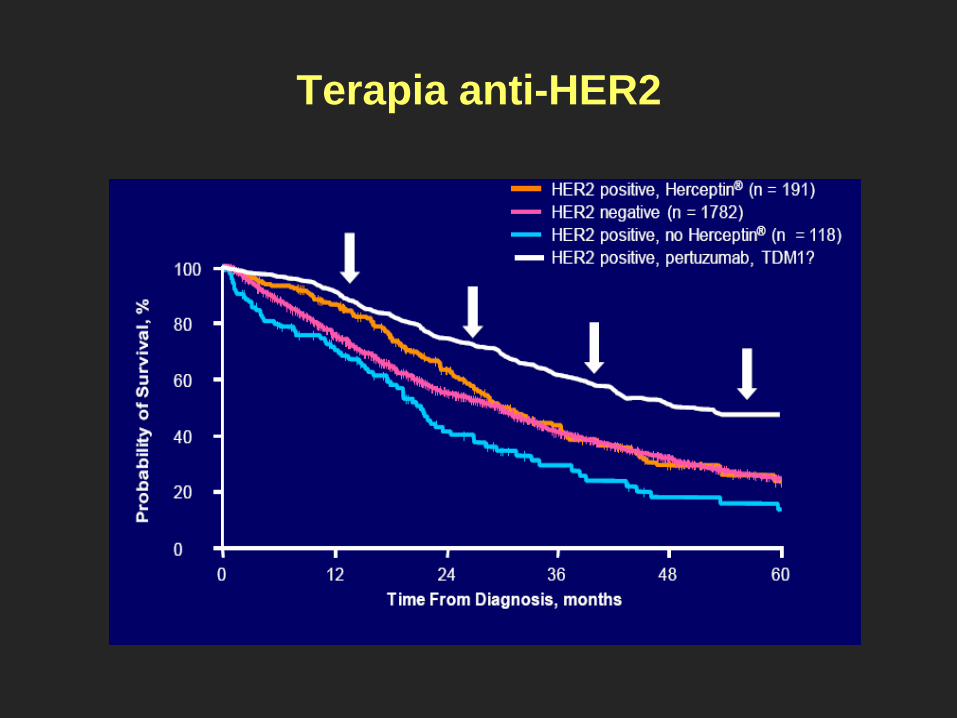
Terapia anti-HER2


Lapatinib puede sensibilizar las células ErbB2+
a subsecuentes tratamientos con trastuzumab (hallazgos in vitro)
• Lapatinib impide la fosforilación, proteolisis y degradación de ErbB2.
• Lapatinib induce la acumulación de las formas inactivas de ErbB2, aumentando
así la toxicidad celular mediada por anticuerpos.
K K K K Lapatinib
ATP
ErbB2
heterodimer
ErbB2
homodimer K K K K K K K K K K K K
trastuzumab
NK cell
FcR
K = kinase domain ADCC = antibody-dependent cell cytotoxicity Scaltriti M et al. Oncogene 2009; 28: 803-814.
Dimerización, fosforilación reducida e
inhibición de la señalización.
Acúmulo de receptores inactivos,
Estabilización de los dímeros, permite
aumento de la ADCC.

trastuzumab
TAM
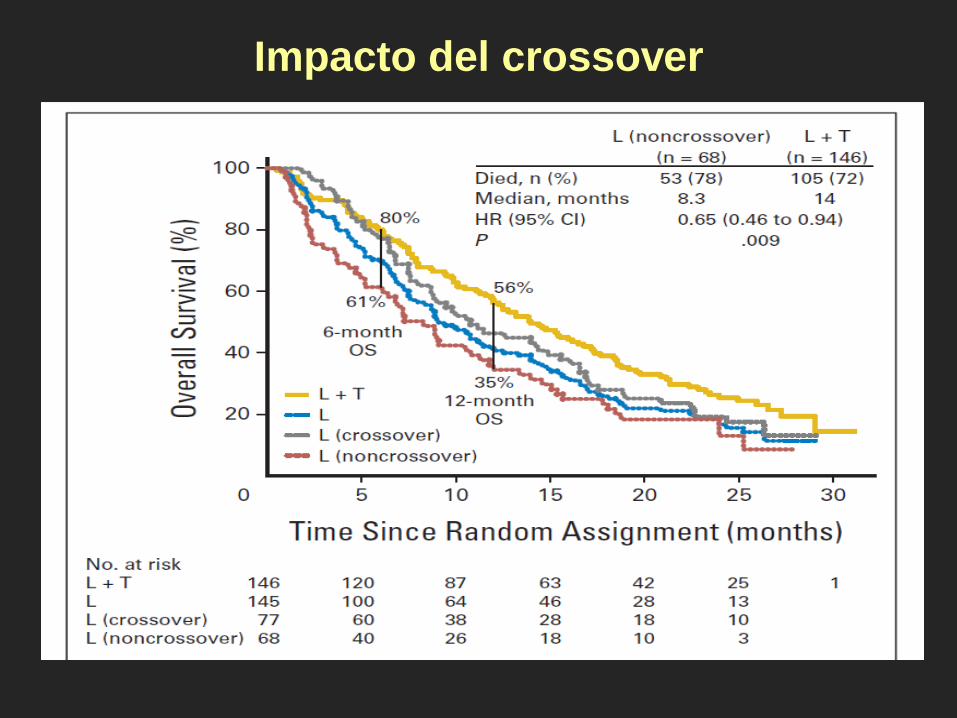
Impacto del crossover
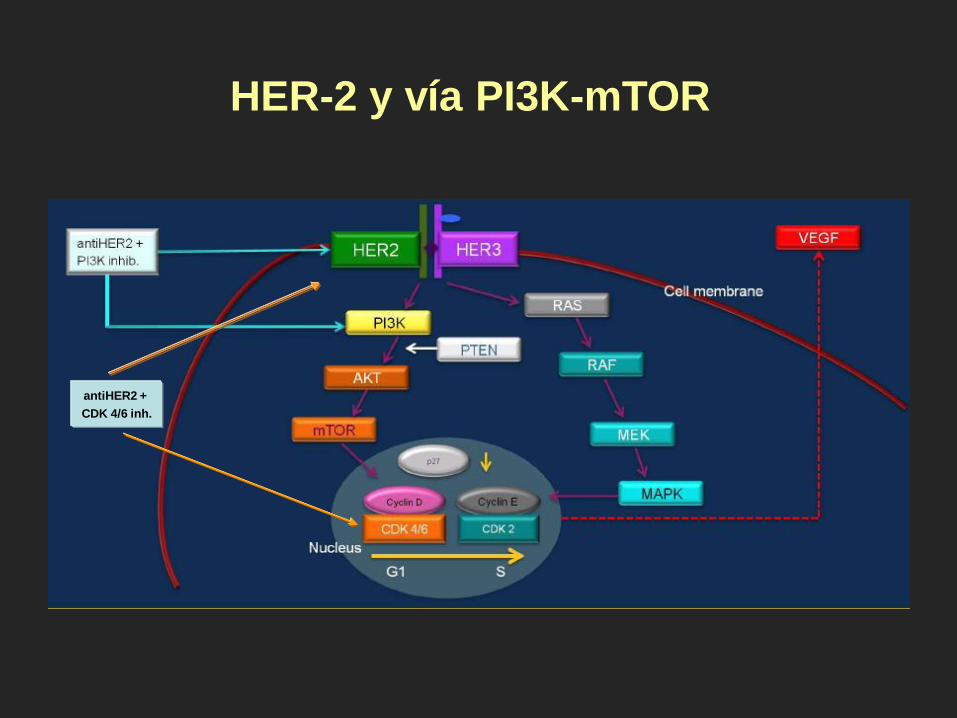
HER-2 y vía PI3K-mTOR
antiHER2 +
CDK 4/6 inh.



NCIC CTG MA.31 trial: results (PFS)
An open-label, randomized, phase III trial comparing taxane-based chemotherapy with
lapatinib or trastuzumab as a first-line therapy for women with HER2-positive MBC
Gelmon KA, et al. ASCO Annual Meeting Abstracts 2012;30:LBA671
Time to Progession – ITT Population
70
10
20
30
40
50
60
70
80
90
0
100
* Censors 4 patients who died due to causes other than breast cancer
1
0
20 30 40 50 60 0 Time (weeks)
Capecitabine
Lapatinib +
Capecitabine
0.00016 P-value (log-rank, 1-sided)
69 (43%) 45 (28%) Progressed or died*
19.7 36.9 Median TTP, wk
161 160 No. of pts
0.51 (0.35, 0.74) Hazard ratio (95% CI)
% o
f p
ati
en
ts f
ree f
rom
pro
gre
ssio
n*

RE+
65-75%
mTOR inhibitors
CDK 4/6 inhibitors
HER-2 la historia continúa: Presente
Nuevos fármacos según subtipo tumoral
Pertuzumab
TDM-1
Combinaciones AntiHER2
Triple negativo
15%
HER2+
15- 20 %
Nuevos citostáticos (Eribulina)
Sales de platino
Bevacizumab
Mayor conocimiento biológico de los
reecptores de la familia HER

Combination of Lapatinib and Trastuzumab has
Synergistic Anti-tumor Activity
• Treatment with lapatinib plus trastuzumab resulted in complete tumor remission
– Effect was durable: no tumor relapse observed after 8 mo post treatment
• Lapatinib induced accumulation of inactive HER2 at plasma membrane
– Trastuzumab-mediated cytotoxicity was higher with the addition of lapatinib in MCF7/HER2 cells
• In vivo activity was consistent with in vitro data demonstrating the combination as synergistic
Scaltriti, et al. Oncogene 2009;28(6):803-814, Konecny, et al. Cancer Res 2006;66:1630-1639; Xia, et al.Oncogene 2004;23: 646–653