modulación no farmacológica del sistema nervioso simpático
DESCRIPTION
Bloque: NUEVOS RETOS EN PREVENCIÓN Y TRATAMIENTO DE LA ENFERMEDAD CARDIOVASCULAR Ponente: Dr. Josep Redón Curso Medicina Cardiovascular que tuvo lugar el 8 y 9 octubre 2012 en Barcelona. Enlace: www.riesgocardiovascular.comTRANSCRIPT
NUEVOS RETOS EN PREVENCIÓN Y TRATAMIENTO DE LA ENFERMEDAD CARDIO VASCULAR
Dr. Josep Redón (Valencia)
Modulación no farmacológica del sistema nervioso simpático

Modulación no Farmacológica del Sistema Nervioso Simpático
Josep Redon. MD, PhD, FAHA Scientific Director Research Foundation and Research Institute INCLIVA. University of Valencia
Medicina Cardiovascular 2013 Master Course ESH
Barcelona, 8 de Octubre, 2012

Historical perspective of SNS and cardiovascular function
• 1664, Willis provided the first anatomic description
• 1840, Stelling correctly conclude that the vasomotor fibers were in sympathetic nerves from the CNS
• 1850, Brown-Sequard, Waller and Bernard laid the foundation for modern concepts of neural circulatory control
• 1920, Canon introduced the role of SNS in the concept of “fight and flight” response to stress
Historical perspective of SNS and cardiovascular function
• 1850, Brown-Sequard, Waller and Bernard laid the foundation for modern concepts of neural circulatory control
• 1946, Von Euler demonstrated the sympathetic transmitter, norepinephrine
• 1950s, pharmacologic intervention to modulate SNS overactivity in clinical conditions
• 1968 Hagbart and Vallbo, develop the clinical microneurography
• 1968, Engelman publish the first sensitive and specific plasma-chatecolamin assay

Sympathetic Nervous System: Methods for testing
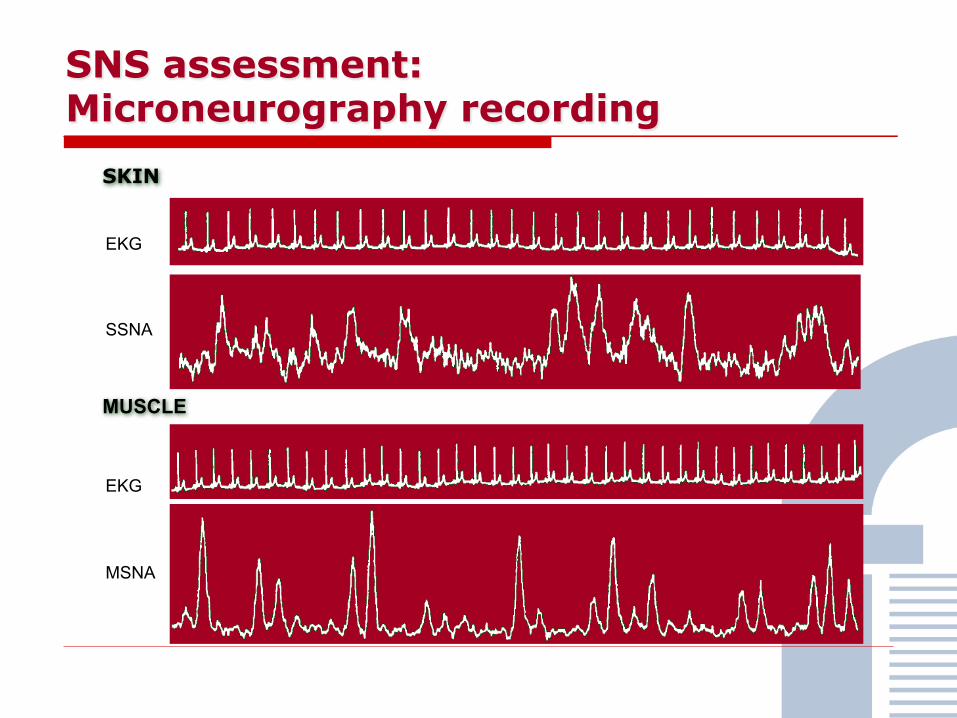
SKIN
MUSCLE
EKG
SSNA
EKG
MSNA
SNS assessment: Microneurography recording
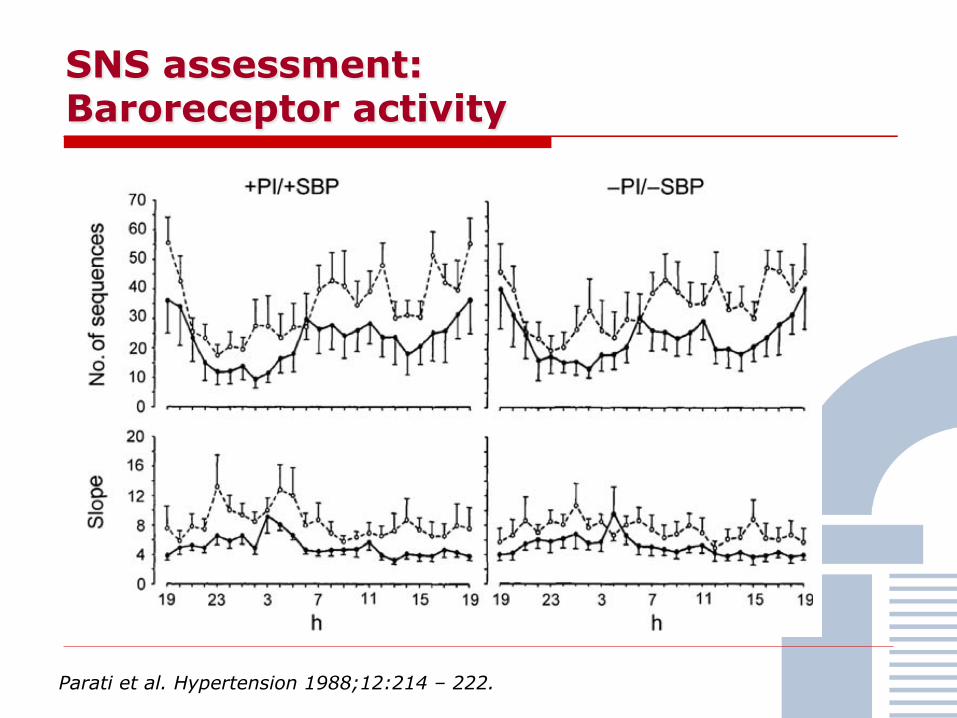
SNS assessment: Baroreceptor activity
Parati et al. Hypertension 1988;12:214 – 222.
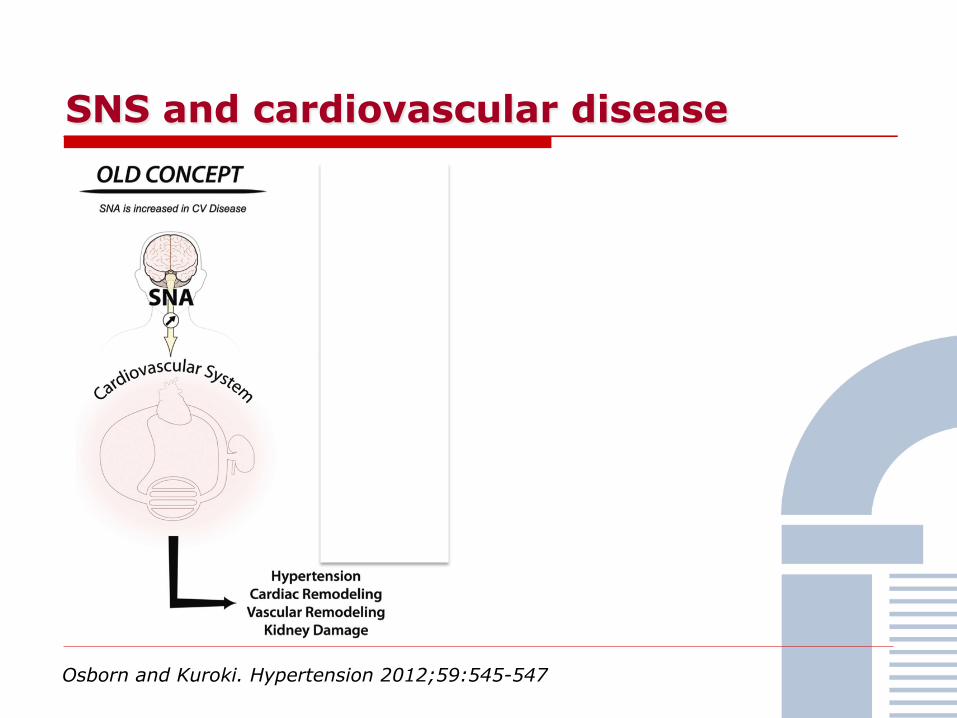
SNS and cardiovascular disease
Osborn and Kuroki. Hypertension 2012;59:545-547
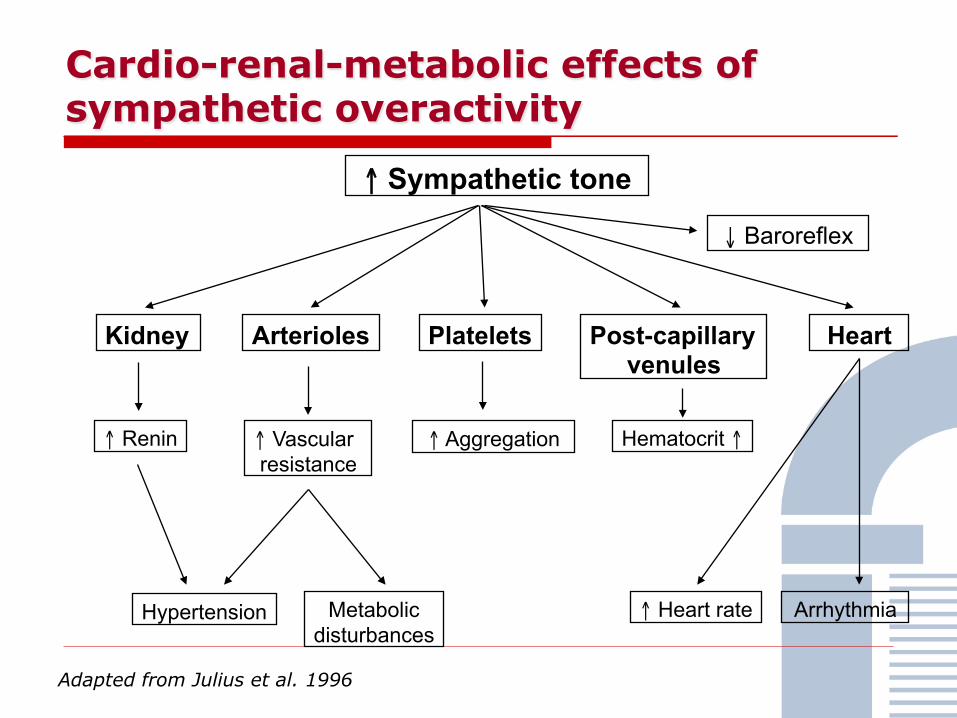
Cardio-renal-metabolic effects of sympathetic overactivity
Kidney
↑ Renin
Heart
↑ Heart rate Arrhythmia
↑ Sympathetic tone
Adapted from Julius et al. 1996
↓ Baroreflex
Hypertension Metabolic disturbances
Arterioles
↑ Vascular resistance
Platelets Post-capillary venules
Hematocrit ↑ ↑ Aggregation
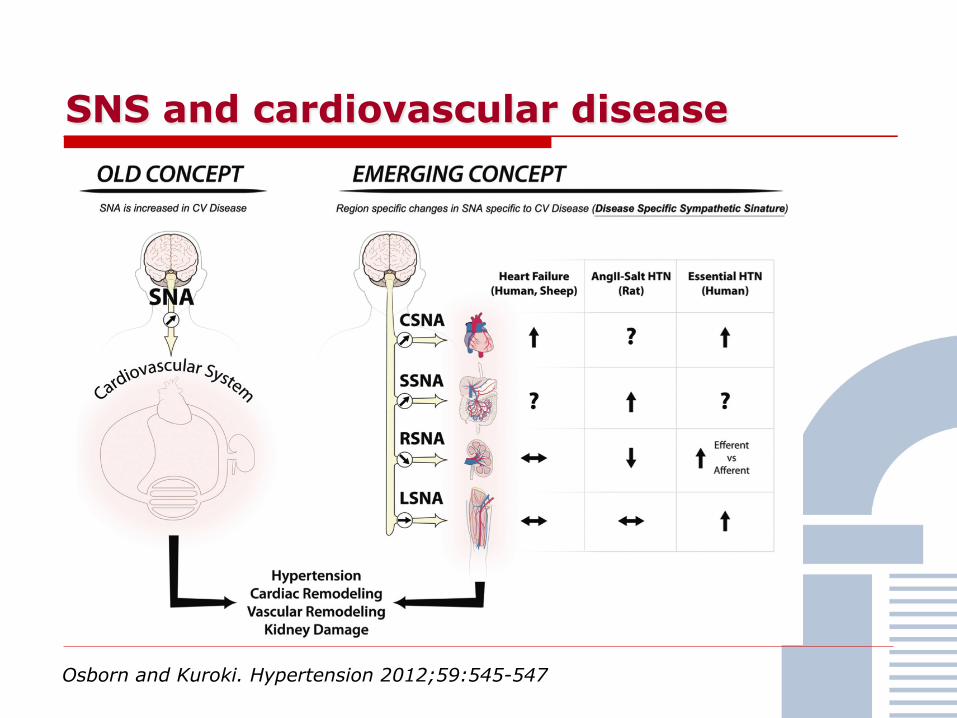
SNS and cardiovascular disease
Osborn and Kuroki. Hypertension 2012;59:545-547

Role of kidney in the sympathetic overactivity of hypertension

SNS and cardiovascular disease
• Heart failure • Essential hypertension
• Disorders of postural circulatory control causing syncope
• Psycogenic heart disease
• Heart disease attributable to mental stress and psychiatric illness

SNS in cardiovascular disease and associated conditions
• Heart failure • Essential hypertension
• Obesity and metabolic syndrome • Obstructive apnea syndrome
• Chronic kidney disease

**
** ** **
**
**
** ** ** **
Grassi G et al. Hypertension 1998;31:68-72
90
110
70
130
MAP (mm Hg)
60
70
50
80
Heart rate (bpm)
60
70
50
80
MSNA (bursts/min.)
Control subjects Stage I hypertension
Stage II/III hypertension Hyperaldosteronism
** p < 0,01
Overactivity of SNS in essential hypertension

Renal noradrenaline spillover in essential hypertension
Parati and Esler. Eur Heart J 2012;33:1058–1066

16 bs
/min
bs/1
00 h
b
C (n = 19)
OMS - (n = 14)
OMS + (n = 19)
C (n = 19)
OMS - (n = 14)
OMS + (n = 19)
*
* **
*
* **
Grassi et al. Nutr Metab Cardiovasc Dis 2007;17:473-481
MSNA MSNA
80
60
40
20
50
40
30
20
Sympathetic overactivity in the Metabolic Syndrome

Sympathetic overactivity and insulin resistance in obese hypertension
Grassi et al. J Hypertens 2004
0
15
30
45
60
25
40
55
70
L PO CO100
200
300
400
L PO CO0
1.2
2.4
3.6
MSNA MSNA
NE HOMA Index
bs/min
pg/ml
bs/100 hb
a.u. * * * * *
* *
* ** *
L n = 36 PO n = 20 CO n = 26
**
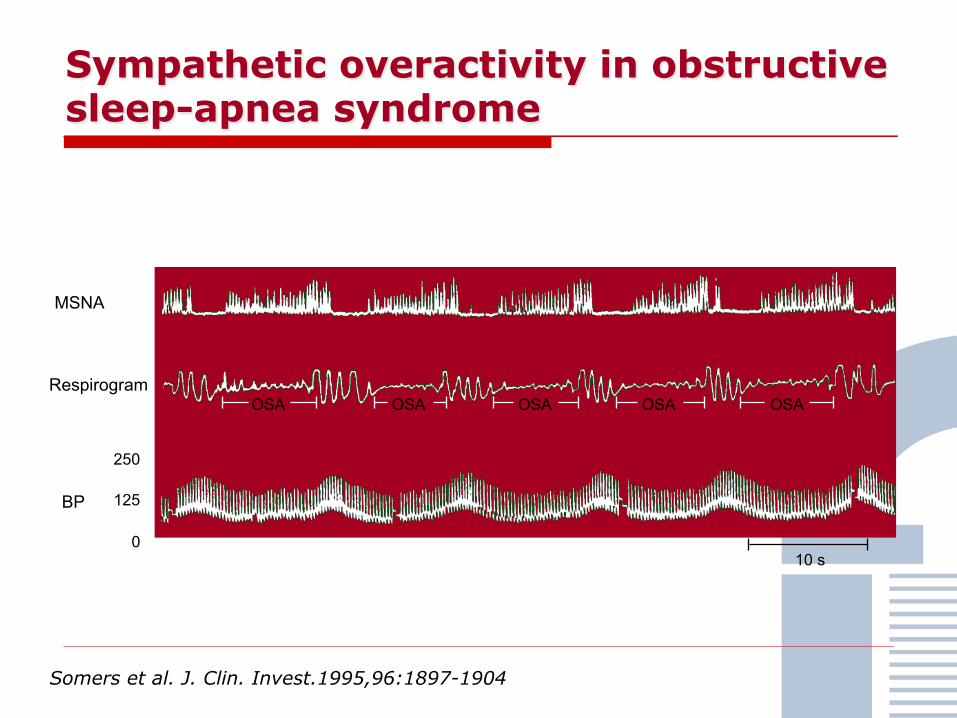
MSNA
Respirogram
BP
Somers et al. J. Clin. Invest.1995,96:1897-1904
250
125
0
OSA
10 s
OSA OSA OSA OSA
Sympathetic overactivity in obstructive sleep-apnea syndrome

Narkiewicz et al. Circulation 1998,98:772-776
Overactivity of the sympathetic nervous system in obstructive sleep-apnea

Sympathetic overactivity in early chronic kidney disease
Grassi et al. Hypertension. 2011;57:846-851
Quartiles of eGFR

Surgical ablation of SNS in hypertension
SPLANCHNICECTOMY FOR ESSENTIAL HYPERTENSION RESULTS IN 1,266 CASES Reginald H. Smithwick, M.D.; Jesse E. Thompson, M.D. JAMA August 15, 1953, Vol 152, No. 16
Many forms of therapy have been used in an effort to control hypertension. The principal ones may be classified under three headings: (1) diets low in sodium and fat, (2) drugs with a hypotensive or sedative effect, and (3) surgery. The form of surgical therapy that has been used most extensively is intervention on the sympathetic nervous system.
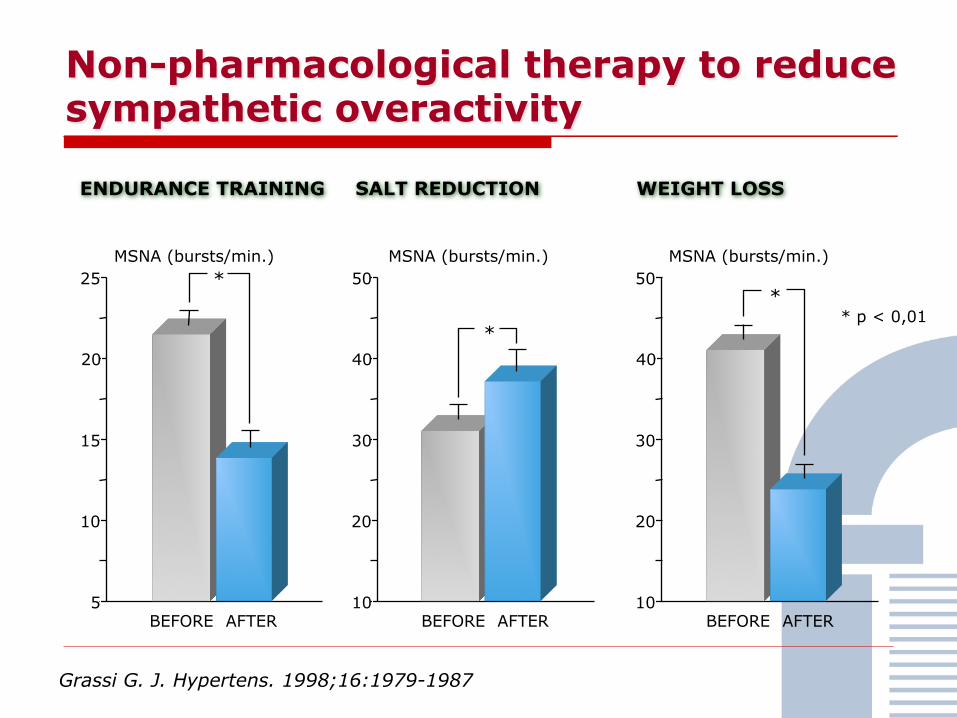
Non-pharmacological therapy to reduce sympathetic overactivity
Grassi G. J. Hypertens. 1998;16:1979-1987
25
15
10
5
MSNA (bursts/min.)
20
50
30
20
10
40
50
30
20
10
40
BEFORE AFTER
ENDURANCE TRAINING WEIGHT LOSS SALT REDUCTION
*
* *
* p < 0,01
MSNA (bursts/min.) MSNA (bursts/min.)
BEFORE AFTER BEFORE AFTER

Overactivity of the sympathetic nervous system in obstructive sleep-apnea
Before
After 1 month
After 6 months
After 1 year
10 s
Patient #1 Patient #2
Narkiewicz K et al. Circulation 1999
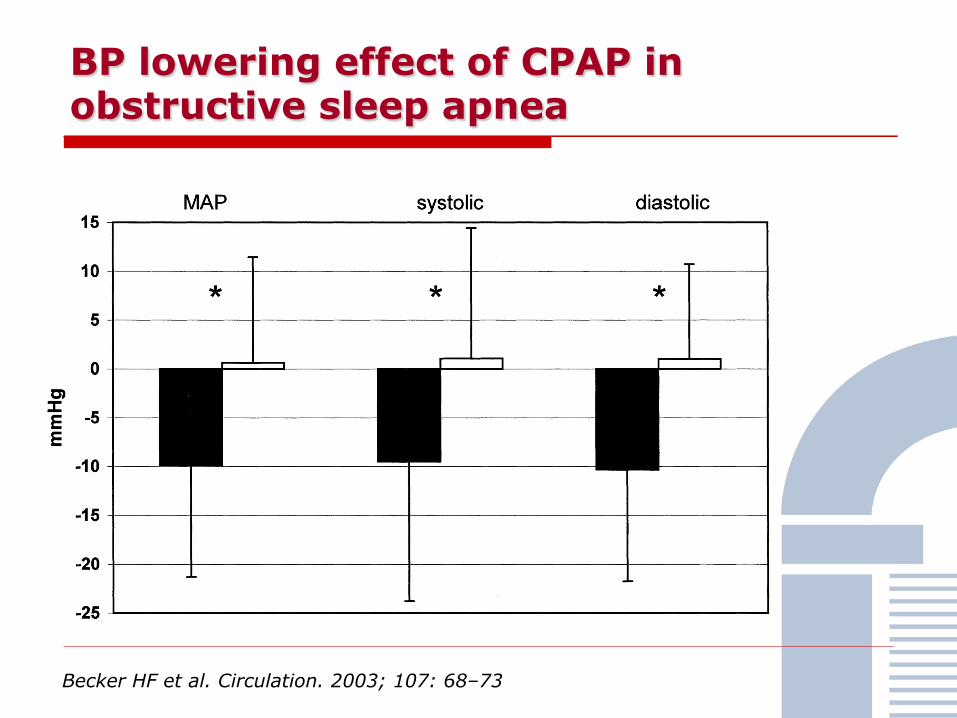
BP lowering effect of CPAP in obstructive sleep apnea
Becker HF et al. Circulation. 2003; 107: 68–73

Mechanisms frequently involved in resistance to reduce BP
Volume overload
Structural vascular changes
Sympathetic overactivity

Direct barroreceptor stimulation
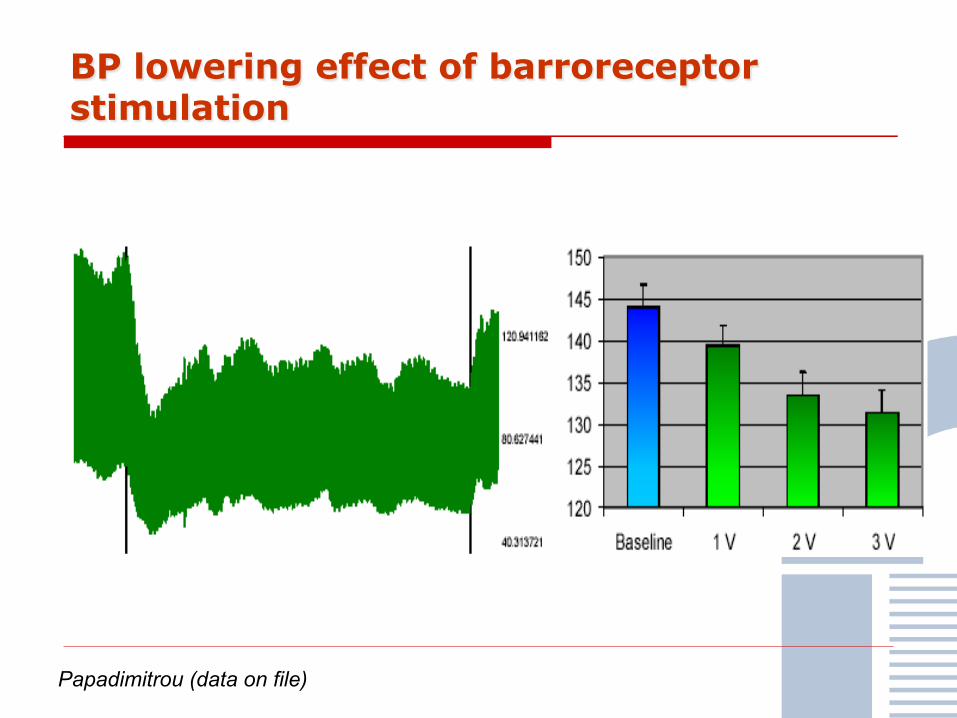
BP lowering effect of barroreceptor stimulation
Papadimitrou (data on file)
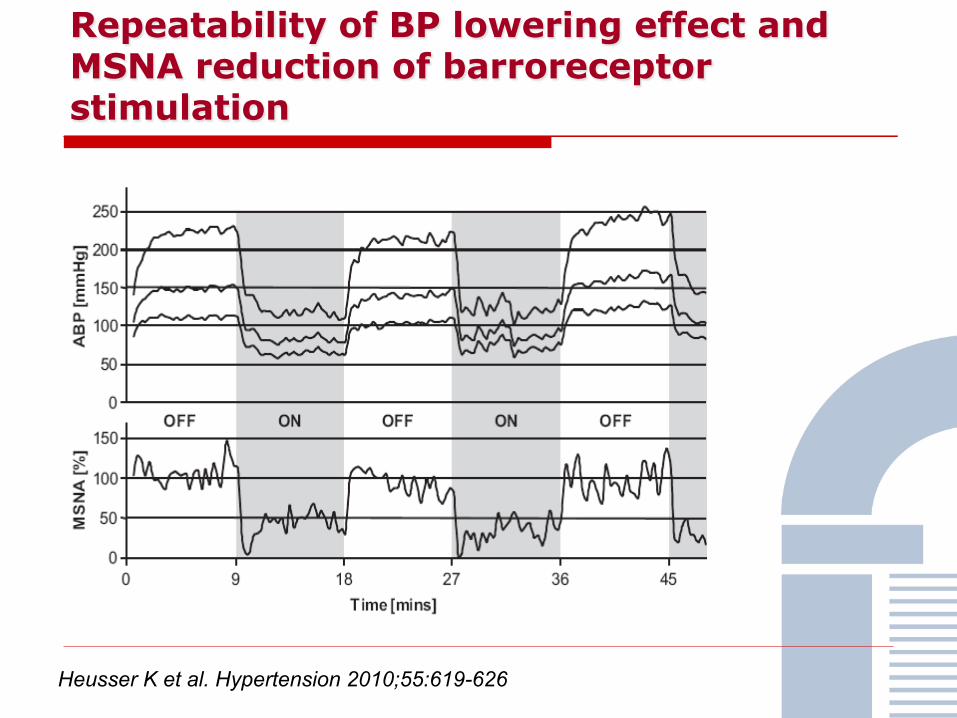
Repeatability of BP lowering effect and MSNA reduction of barroreceptor stimulation
Heusser K et al. Hypertension 2010;55:619-626
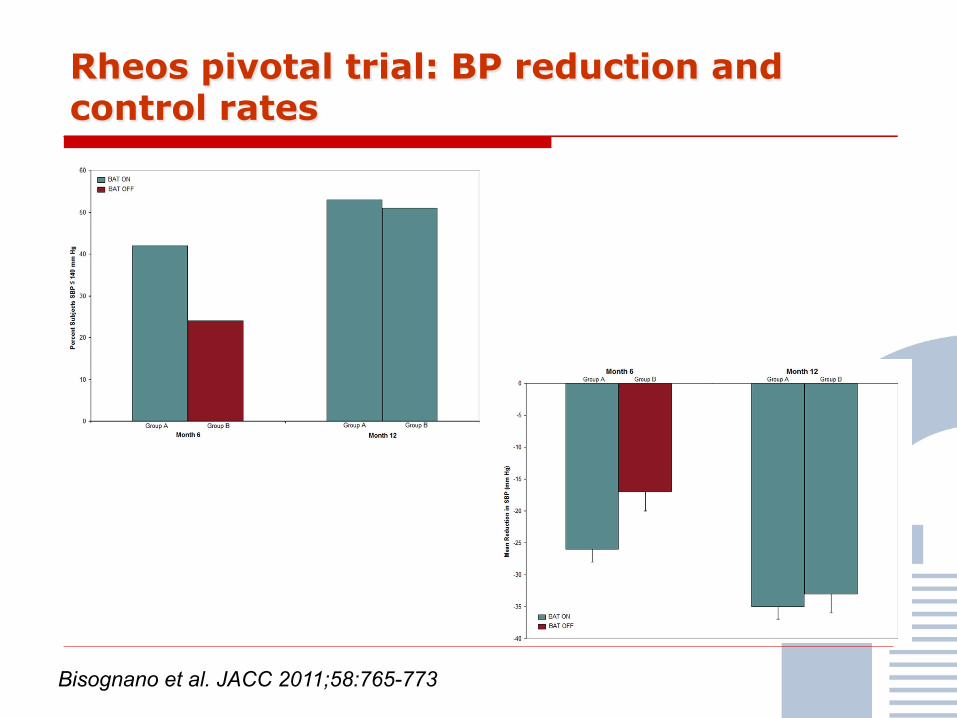
Rheos pivotal trial: BP reduction and control rates
Bisognano et al. JACC 2011;58:765-773

Renal sympathetic-nerve location
M Krum

Renal sympathetic-nerve ablation by using radiofrequency waves
M Krum
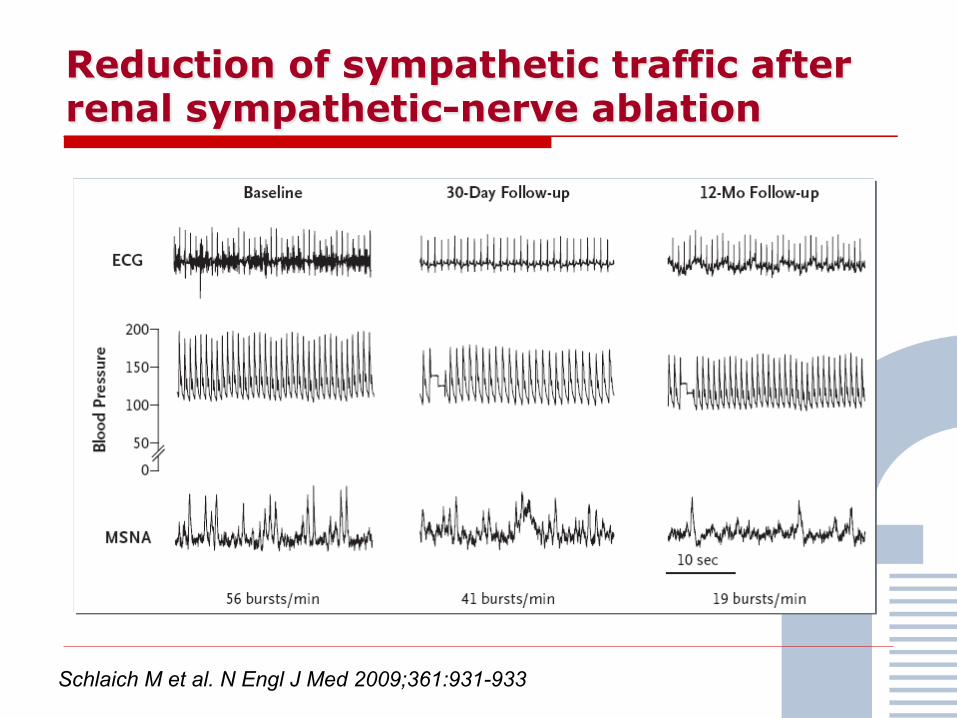
Reduction of sympathetic traffic after renal sympathetic-nerve ablation
Schlaich M et al. N Engl J Med 2009;361:931-933

Persistent BP reduction after renal sympathetic-nerve ablation
Krum H et al. Lancet 2009:373:1275-1282

Persistent BP reduction and changes in GFR after renal sympathetic-nerve ablation
Persu et al. Hypertension 2012;60:596-604

Persistent BP reduction after renal sympathetic-nerve ablation
Simplicity HTN-2 Investigators Lancet 2010;376:1903-1909

Persistent BP reduction after renal sympathetic-nerve ablation
Simplicity HTN-2 Investigators Lancet 2010;376:1903-1909
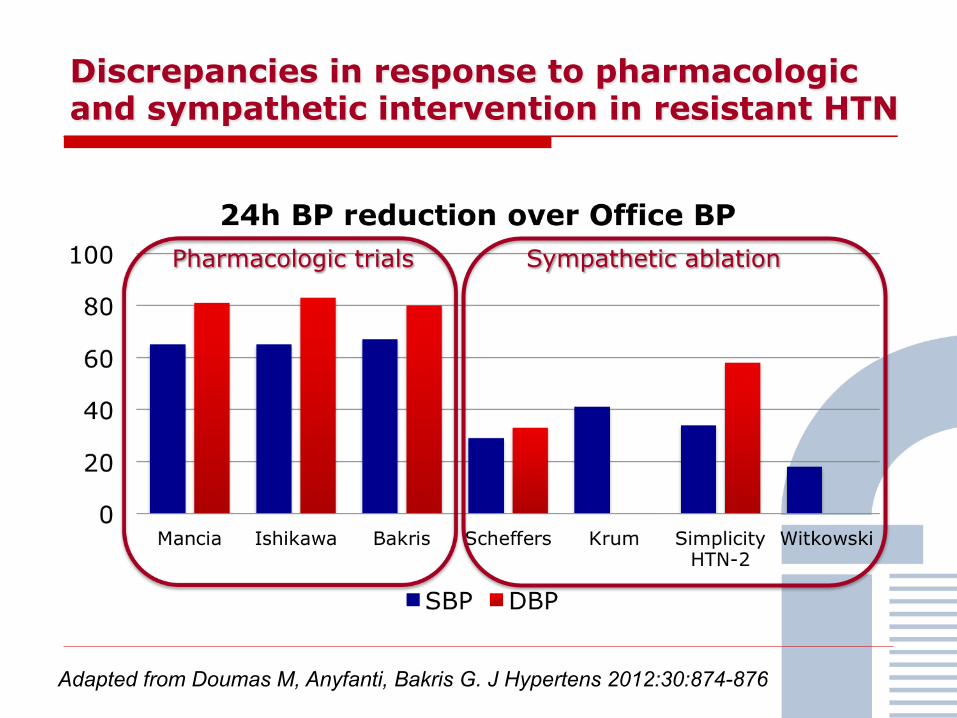
Discrepancies in response to pharmacologic and sympathetic intervention in resistant HTN
Pharmacologic trials Sympathetic ablation
Adapted from Doumas M, Anyfanti, Bakris G. J Hypertens 2012:30:874-876
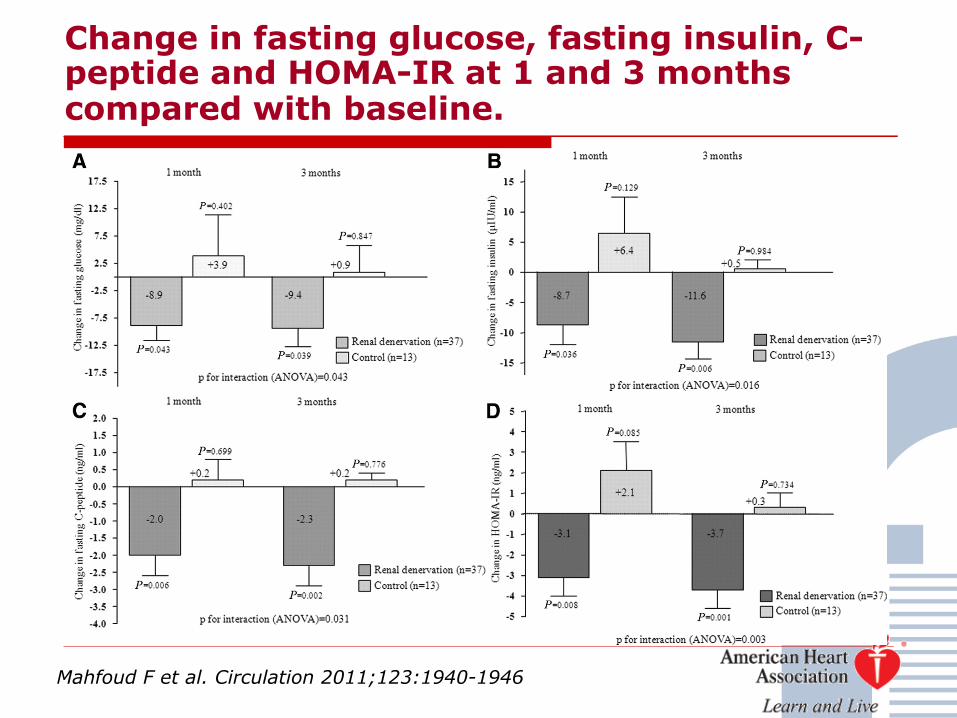
Change in fasting glucose, fasting insulin, C-peptide and HOMA-IR at 1 and 3 months compared with baseline.
Mahfoud F et al. Circulation 2011;123:1940-1946
Renal hemodynamics after renal denervation in resistant hypertension
Mahfoud F et al. Hypertension 2012;60:419-424
88 resistant hypertension patients Reduce Systolic BP RRI index independent of systolic BP No changes GFR measured with Cystatin C
First-in-man safety evaluation of renal denervation for chronic systolic heart failure: Primary outcome from REACH-Pilot study
Davies et al. Int J Cardiol 2012. Epub October 1st
7 patients (mean age 69years) with chronic systolic heart failure (mean BP on referral 112/65mmHg) on maximal tolerated heart failure therapy underwent bilateral renal denervation May–July 2011… Follow-up was weekly for 4weeks, and then monthly for 6months.
No significant haemodynamic disturbances were noted during the acute phase post renal denervation. Over 6months there was a non-significant trend to blood pressure reduction (Δsystolic −7.1±6.9mmHg, p=0.35; Δdiastolic −0.6±4.0mmHg, p=0.88). No hypotensive or syncopal episodes were reported. Renal function remained stable (Δcreatinine −5.7±8.4μmol/l, p=0.52 and Δurea −1.0±1.0mmol/l, p=0.33).
All 7 patients described themselves as symptomatically improved. The six minute walk distance at six months was significantly increased (Δ=27.1±9.7m, p=0.03).!
Unmet needs in knowledge about RDN therapy for refractary hypertension
§ Broad effect range and non-responders, How to identify the non-responders?
§ Monitoring the effect of the procedure, How do that?
§ Physiology of the BP-lowering effec, Why increases overtime?
§ Renoprotective effect of renal denervation, Does it exist?
Schmieder R, Redon J, Grassi G et al. J Hypertension 2012 (in press)

RDN in refractary hypertension
ESH Position Paper: Renal Denervation - an Interventional Therapy of Resistant Hypertension Roland E. Schmieder, Josep Redon , Guido Grassi, Sverre E. Kjeldsen, Giuseppe Mancia, Krzysztof Narkiewicz, Gianfranco Parati, Luis Ruilope, Philippe van de Borne, Costas Tsioufis Journal of Hypertension 2012 (May issue)

Unmet needs in RDN therapy for refractary hypertension
§ Randomized blinded studies § Use of 24-hour ABPM to enroll patients and to
assess BP reduction
§ Comparison of RDN efficacy and safety when using different procedures
§ Long-term maintenance of efficacy and safety § Impact in morbidity and mortality reduction
§ Cost-benefit balance studies
§ Standardized certification of RDN centres
Schmieder R, Redon J, Grassi G et al. J Hypertension 2012 (in press)

Today Recommendations in Renal Denervation
Schmider, Redon, Grassi et al. J Hypertens 2012;30:837-841
First step: Exclude ü False resistant hypertension (peudoresistance)
by using 24 hour ambulatory blood pressure monitoring (ABPM) and home BP monitoring.
ü Secondary arterial hypertension ü Causes which maintain high BP values and
might be removed (obstructive sleep-apnea, high salt intake, BP raising drugs, severe obesity)

Today Recommendations in Renal Denervation
Schmider, Redon, Grassi et al. J Hypertens 2012;30:837-841
Second step: Optimize ü Antihypertensive treatment with at least 3 (or
better 4) tolerated drugs including a diuretic and an antialdosterone drug (if clinically possible, e.g after re-evaluating renal function and the potential risk of hyperkaliemia)
ü Check for effective BP control using ABPM before giving indication for RND
Today Recommendations in Renal Denervation
Schmider, Redon, Grassi et al. J Hypertens 2012;30:837-841
Third step: Contraindications ü Anatomic contraindications due to unresolved
safety issues (avoid RDN in case of multiple renal arteries, main renal artery diameter of less than 4 mm or main renal artery length less than 20 mm, significant renal artery stenosis, previous angioplasty or stenting of renal artery)
ü eGFR should be > 45 ml/min/1.73m²

Today Recommendations in Renal Denervation
Schmider, Redon, Grassi et al. J Hypertens 2012;30:837-841
Overall ü Perform the procedure in very experienced
hospital centers, such as hypertension excellence centers
ü Use devices which have demonstrate efficacy and safety in clinical studies
Conclusions
ü Overactivity of the sympathetic nervous systemis in the core of cardiovascular and renal diseases
ü Advances in methods to assess the activity have permitted the accumulation of a large body of relevant information
ü Pharmacological modulation provide important resources to treat CV disease
ü Non-pharmacological intervention using invasive techniques provides a new dawn in the treatment of resistant hypertension and other CV diseases
ü Further research will provide more precise information for their clinical use