factores pronÓsticos para la resecabilidad · factores pronÓsticos para la resecabilidad dr....
TRANSCRIPT

FACTORES PRONÓSTICOS PARA
LA RESECABILIDAD
Dr. Javier Sastre
Servicio de Oncología Médica
HC San Carlos (Madrid).

Factores pronósticos preoperatorios: Resultados a 10 años de seguimiento MSKCC (612 pts, 1985-1994)
Primario N+
ILE < 1 año
CEA > 200 ng/ml
Número de lesiones > 1
Lesiones hepáticas > 5 cm
Tomlinson JS, JCO 2007
Low CRS: 0-2
High CRS: 3-5
MEJORÍA EN LAS TÉCNICAS RADIOLÓGICAS PARA SELECCIÓN DE
PACIENTES
MEJORÍA DE LAS TÉCNICAS QUIRURGICAS Y CUIDADOS
POSTOPERATORIOS
APARICIÓN DE REGÍMENES DE QUIMIOTERAPIA MAS EFICACES

Paul Brousse Hospital: 2047 patients (Apr 1988–Dec 2003)
0
200
400
600
800
1000
1200
1400
1307
535
205
205
Unresectable
Initially unresectable
Resectable
Chemotherapy: 1512 (74%)
14%
86%
28%
72%
Resection: 740
Updated from: Adam R, et al. Ann Surg 2004;240:644–658
COLORECTAL LIVER METASTASES
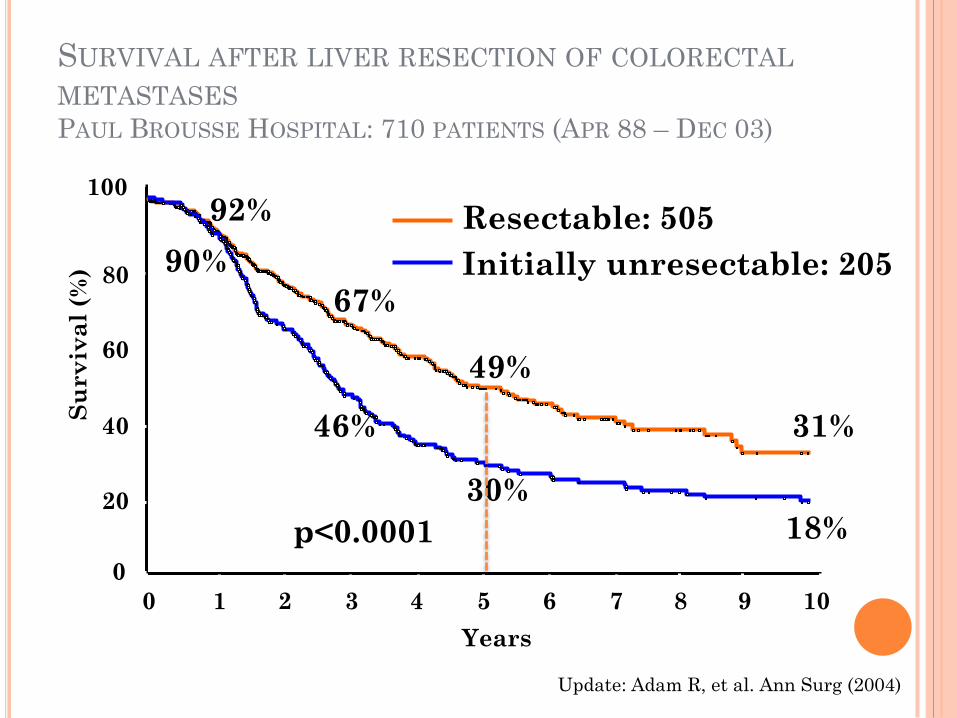
Resectable: 505
Initially unresectable: 205
Years
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10
Su
rv
iva
l (%
)
92%
49%
31%
67%
p<0.0001
90%
30%
46%
18%
Update: Adam R, et al. Ann Surg (2004)
SURVIVAL AFTER LIVER RESECTION OF COLORECTAL
METASTASES PAUL BROUSSE HOSPITAL: 710 PATIENTS (APR 88 – DEC 03)
0
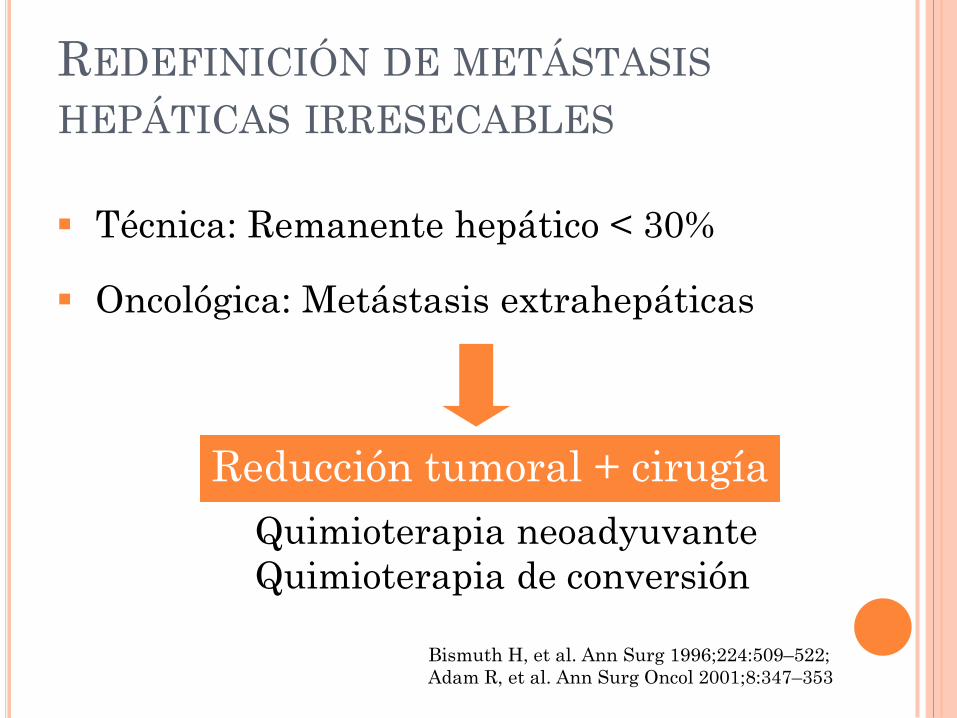
REDEFINICIÓN DE METÁSTASIS
HEPÁTICAS IRRESECABLES
Técnica: Remanente hepático < 30%
Oncológica: Metástasis extrahepáticas
Reducción tumoral + cirugía
Quimioterapia neoadyuvante
Quimioterapia de conversión
Bismuth H, et al. Ann Surg 1996;224:509–522;
Adam R, et al. Ann Surg Oncol 2001;8:347–353

30% synchronous metastases
Additional ~50% will develop metastases
30–35% ‘liver only’ metastases
75–90% not resectable 10–25% candidates for
SURGERY
Aim: R0 resection
250,000 CRC cases/year (Europe)
Chu, et al. Clin Colorectal Can 2006; Kemeny, et al. NEJM 1999;
Kemeny, et al. Oncologist 2007; Leichman. Surg Oncol Clin N Am 2007;
Leonard, et al. JCO 2005; Tomlinson, et al. JCO 2007; Van Cutsem, et al. EJC 200;
Initially
resectable
Borderline
resectable
ESCENARIOS DE PACIENTES CON METÁSTASIS
HEPÁTICAS PARA CONSIDERAR EL
TRATAMIENTO

PRESENTACIONES CLÍNICAS DE PACIENTES
CON METÁSTASIS HEPÁTICAS DE CCRM
Resecable sin factores
de riesgo si:
Metacrónica > 12m
Primario N-
CEA < 200 ng/ml
Única < 3cm o
unilobares
Resecable con
factores
de mal pronóstico:
Tamaño > 3 cm
Sincrónica
Bilobar
Inicialmente
irresecable o
resecabilidad
bordeline
RESPUESTA AL TRATAMIENTO SISTÉMICO


THE NEW EPOC STUDY: FOLFOX/XELOX +
CETUXIMAB VS FOLFOX/XELOX EN KRAS
WT CON METÁSTASIS RESECABLES
272 pacientes randomizados
Análisis de futilidad con 45% de eventos (cierre del
estudio prematuro)
mPFS
(meses)
HR
FOLFOX-C 15.2
1.56 (1.01-2.41) FOLFOX 24.2
Conclusión: La adición de cetuximab a FOLFOX perioperatoria en
pacientes con metástasis resecables K-RAS WT no es beneficiosa.
Primrose JN, ASCO 2013 Abstract 3504.

Resection rate of metastases and tumor response
Response rate
,9,8,7,6,5,4,3
Resection r
ate
,6
,5
,4
,3
,2
,1
0,0
Studies including all patients with mCRC (solid line) (r=0.74, p=0.001)
Studies including selected patients (liver metastases only, no extrahepatic disease) (r=0.96, p=0.002)
Phase III studies in mCRC (dashed line) (r=0.67, p=0.024)
Folprecht G, et al. Ann Oncol (2005).

Tasa de RESPUESTAS en pacientes seleccionados
con enfermedad metastásica confinada al hígado
Estudio Población Esquema RC (%) RP (%) RO (%)
BOXER
Inicialmente irresecable + SINCRONICO
XELOX + BVZ
9
69
78
NCCTG Inicialmente irresecable
FOLFOX 2.4 47.6 50
Abad Inicialmente irresecable
FUOXIRI 2.4 66.6 69
CELIM Inicialmente irresecable
FOLFOX + CET 68
CELIM Inicialmente irresecable
FOLFIRI + CET 57 (70 WT)
PLANET Resecables alto riesgo o
irresecables
FOLFOX + PAN
FOLFIRI + PAN
73
67

46 pacientes
Tratamiento neoadyuvante con oxaliplatino
+capecitabina+bevacizumab
RO: 78%
Tasa de resecabilidad: 40%

BOXER: Progression-free survival (PFS) and overall survival (OS) for all eligible patients (n = 45).
Wong R et al. Ann Oncol 2011;22:2042-2048
© The Author 2011. Published by Oxford University Press on behalf of the European Society for
Medical Oncology. All rights reserved. For permissions, please email:
Datos inmaduros Mediana de seguimiento 12m
86%
50%

OLIVIA: STUDY DESIGN
Criteria for unresectability
Patients had to meet at least one of the following criteria:
no upfront R0/R1 resection of all hepatic lesions possible
less than 30% estimated residual liver after resection
disease in contact with major vessels of the remnant liver
FDG-PET was performed to exclude extrahepatic metastases
Previously untreated
unresectable
colorectal cancer
with metastases
confined to the liver
N=80
Bev + mFOLFOX-6
Bev + FOLFOXIRI Stratification factors
• Centre
• ECOG performance status
• No. of metastatic lesions
Randomizatio
n
1:1
ECOG, Eastern Cooperative Oncology Group

BASELINE CHARACTERISTICS
Variable
Bev + FOLFOXIRI
(n=41)
Bev + mFOLFOX-6
(n=39)
Male/female, % 71/29 46/54
Median age (range), years 63 (32–77) 57 (28–80)
ECOG performance status (0/1), % 63/37 77/23
Criteria for unresectability,* %
No upfront R0/R1 resection of hepatic lesions
possible 80 80
Less than 30% estimated residual liver after
resection 63 59
Disease in contact with major vessels of remnant
liver 37 44
Primary tumour site, %
Colon 71 69
Rectum 20 23
Colorectal 10 8
Disease stage at diagnosis, %
Locoregional/metastatic 27/73 18/82
Primary tumour in situ, % 61 69
ITT population. Percentages may not add up to 100% due to rounding; *Based on manual medical science review of case report
forms

RESECTION AND RESPONSE RATES
Variable, n (%)
Bev +
FOLFOXIRI
(n=41)
Bev +
mFOLFOX-6
(n=39)
Difference
(%) P value
Resection rate
R0/R1/R2* 25 (61.0) 19 (48.7) 12.3 0.271
R0/R1 21 (51.2) 13 (33.3) 17.9 0.106
R0 20 (48.8) 9 (23.1) 25.7 0.017
Overall response rate 33 (80.5) 24 (61.5) 18.9 0.061
ITT population; *Only 2-stage hepatectomy

PROGRESSION-FREE SURVIVAL: ALL PTS
ITT population; analysis performed 15 March
2013
0 3 6 9 12 15 18 21 24 27 30
33 Time (months)
Su
rv
iva
l p
ro
ba
bil
ity
(%)
Bev +
FOLFOXIRI
Bev + mFOLFOX-
6
1.0
0.8
0.6
0.4
0.2
0.0
0.9
0.7
0.5
0.3
0.1
No. at
risk: 39
41
37
38
16
27
24
31
8
22
2
19
1
4
33
37
2
9
0
2
0
1
12.0 18.8
0
0
Median (95% CI)
18.8 mo (12.4–21.0)
12.0 mo (9.5–14.1)
log-rank test p=0.0009
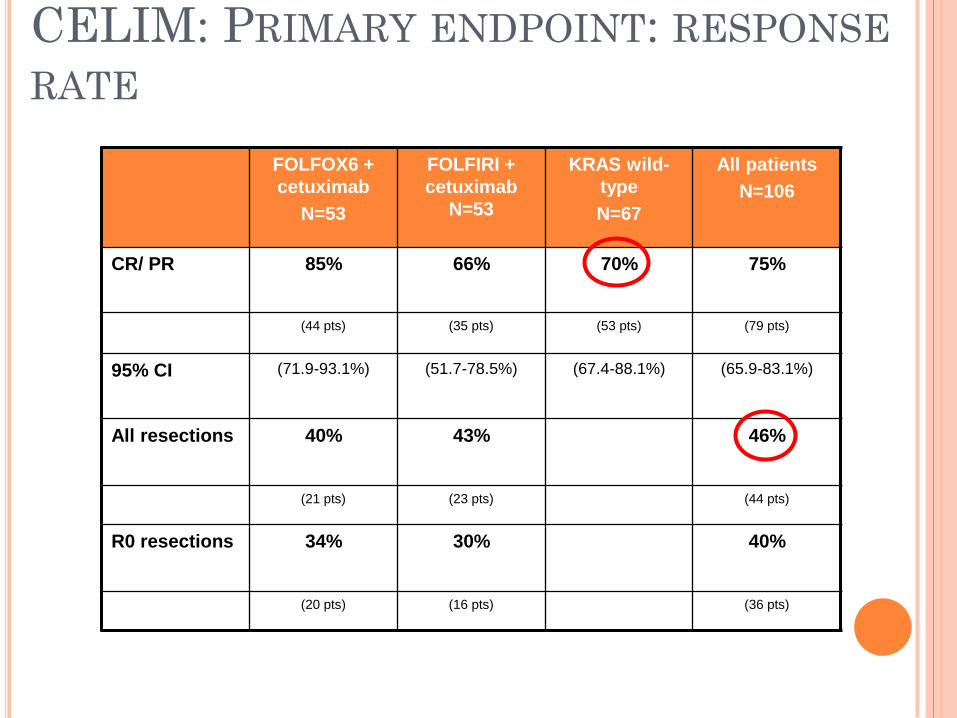
CELIM: PRIMARY ENDPOINT: RESPONSE
RATE
FOLFOX6 +
cetuximab
N=53
FOLFIRI +
cetuximab
N=53
KRAS wild-
type
N=67
All patients
N=106
CR/ PR 85% 66% 70% 75%
(44 pts) (35 pts) (53 pts) (79 pts)
95% CI (71.9-93.1%) (51.7-78.5%) (67.4-88.1%) (65.9-83.1%)
All resections 40% 43% 46%
(21 pts) (23 pts) (44 pts)
R0 resections 34% 30% 40%
(20 pts) (16 pts) (36 pts)

Criterios de inclusión
1. Metástasis sincrónicas
2. Inicialmente
irresecables evaluadas
por al menos 3
cirujanos y un radiólogo
3. No tratamiento previo

(A) Overall survival curves and (B) Kaplan-Meier progression-free survival for the intent-to-
treat population in the cetuximab plus chemotherapy and chemotherapy-alone treatment
arms.
Ye L et al. JCO 2013;31:1931-1938
©2013 by American Society of Clinical Oncology
RESECTION RATE: 28% vs 13% in favour of cetuximab

Abad et al. Presented at the 16th World Congress on Gastrointestinal Cancer, June 25-28, 2014, Barcelona (Spain); Abstract nº PD-0006
PLANET STUDY
RESPONSE RATE AND RESECTABILITY
†percentages calculated over the total number of patients with surgical resection in each group; ORR: Objective response rate (not confirmed*); *patients resected before response confirmation
WT KRAS population ACCORDING TO
RAS STATUS
(n = 38 / 39 / 77) (n = 38 / 39 / 77) (n = 17 / 23 / 40) (n = 27 / 26 / 53) (n = 4 / 7 / 11)
Abad et al. Presented at the 16th World Congress on Gastrointestinal Cancer, June 25-28, 2014, Barcelona (Spain); Abstract nº PD-0006

VALIDACIÓN DEL SCORE MSKCC
RESULTADOS A 10 AÑOS (1996-2007)
CRS score n mOS (m) 5-Year OS Log-rank
0-2
3-5
80
80
43m
18m
41%
13%
p < 0.01
0-1
2-3
4-5
39
96
34
-
27m
15m
72%
21%
4.6%
p < 0.01
Ivanecz A et al. Hepato-Gastroenterology 2009
Criterios de resecabilidad:
1. Resección macroscópicamente completa con preservación de
25-40% de parénquima hepático.
2. Ausencia de comorbilidades de contraindiquen la
intervención.

Carácterísticas de los pacientes nº (%)
Mts sincrónicas
> 3 metástasis
Mts > 5 cm
Lesiones extrahepáticas
QT preoperatoria
Bevacizumab preoperatorio
Cetuximab peoperatorio
QT adyuvante
3.015 (50.0)
1.046 (17.4)
1.103 (18.3)
417 (6.9)
2.249 (37.3)
382 (17)
127 (5.6)
2.820 (46.8)
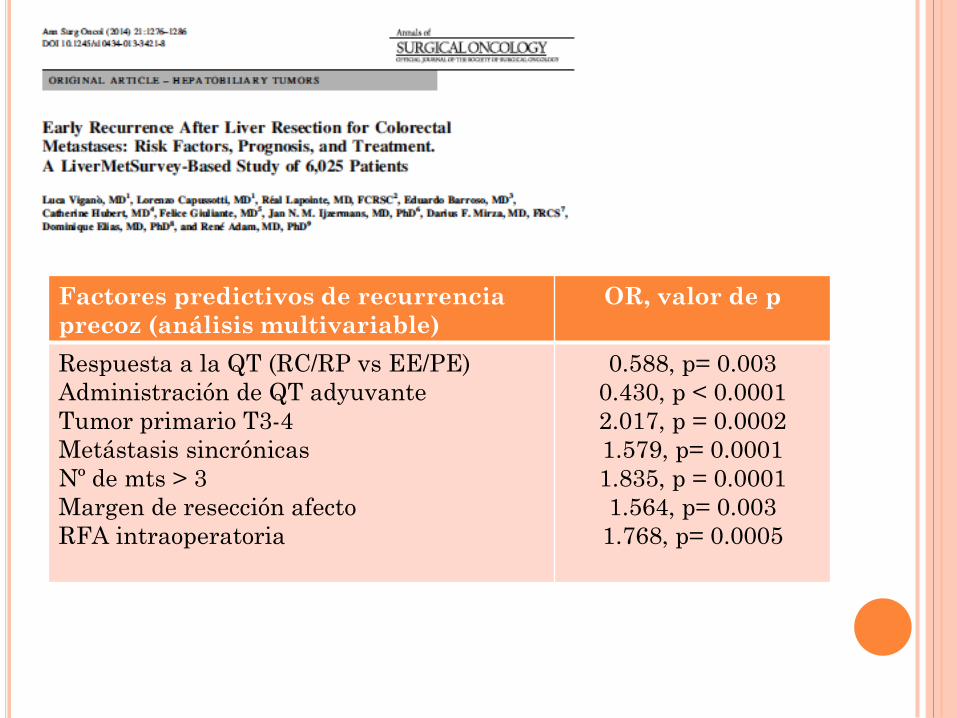
Factores predictivos de recurrencia
precoz (análisis multivariable)
OR, valor de p
Respuesta a la QT (RC/RP vs EE/PE)
Administración de QT adyuvante
Tumor primario T3-4
Metástasis sincrónicas
Nº de mts > 3
Margen de resección afecto
RFA intraoperatoria
0.588, p= 0.003
0.430, p < 0.0001
2.017, p = 0.0002
1.579, p= 0.0001
1.835, p = 0.0001
1.564, p= 0.003
1.768, p= 0.0005

LIVER RESECTION FOR MULTIPLE
METASTASES AFTER CHEMOTHERAPY:
OVERALL SURVIVAL
Adam R, et al. Ann Surg (2004)
30% 37%
Stabilization: 39
Progression: 34
Downsizing: 58
Log-rank: p<0.0001
20
40
60
80
100
0 1 2 3 4 5
63%
12% 8%
44%
95%
55%
Years
(%)
92%
0

EQUIPOS MULTIDISCIPLINARES
Cirugía General y Digestiva (7)
Radiodiagnóstico (4)
Anatomía Patológica (1)
Medicina Nuclear (2)
Oncología Médica (2)
Oncología Radioterápica (2)
Gastroenterología (1)
¡¡SESIONES DE TOMA DE
DECISIONES CON CARÁCTER
SEMANAL!!

CONCLUSIONES (I)
Los criterios clínicos clásicos del MSKCC nos dan
información del riesgo de recidiva de los
pacientes con mts hepáticas de CCR, pero no se
consideran a día de hoy criterios de
irresecabilidad
La enfermedad extrahepática irresecable y la
imposibilidad de un remanente hepático del 30%
son los criterios actuales de irresecabilidad
Los pacientes se deben clasificar en
Resecables sin criterios de riesgo
Resecables con criterios de riesgo
Borderline o irresecables
CONCLUSIONES (II)
Los pacientes con mts resecables sin criterios de
riesgo son candidatos a recibir quimioterapia
postoperatoria
Los pacientes con mts resecables con criterios de
riesgo deberían recibir quimioterapia
perioperatoria sin agentes biológicos
Los pacientes con mts borderline o irresecables
deben recibir quimioterapia + agente biológico,
preferentemente anti-EGFR si RAS wt
El trabajo en equipos multidisplinares es
fundamental para el manejo de estos pacientes.