dra. helena barrasa - seimc.org · efecto post-antibiótico. al aumentar la concentración de estos...
TRANSCRIPT


Dra. Helena Barrasa
Medicina Intensiva Hospital Universitario Araba, Vitoria.
PK/PD de daptomicina en el paciente crí3co
Introducción
PK/PD de daptomicina en el paciente crí3co
Introducción 3
I. TERAPIA ANTIMICROBIANA EN PACIENTES CRÍTICOS
Desde el descubrimiento de las sulfamidas y la penicilina, hace casi 90 años, se han desarrollado numerosos fármacos para tratar infecciones bacterianas. Aunque en aquel entonces estos nuevos medicamentos supusieron un descubrimiento que ayudó a curar muchas enfermedades hasta el momento letales, hoy en día el control de las infecciones bacterianas se ha convertido en un problema a la hora de seleccionar un antibiótico apropiado. La prescripción de un agente antibacteriano debe suponer una toma de decisión sobre cuál es el fármaco adecuado y la dosis e intervalos de dosificación correctos; para, de este modo, asegurar el éxito clínico, minimizar los efectos adversos y reducir la probabilidad de generación de resistencias.1
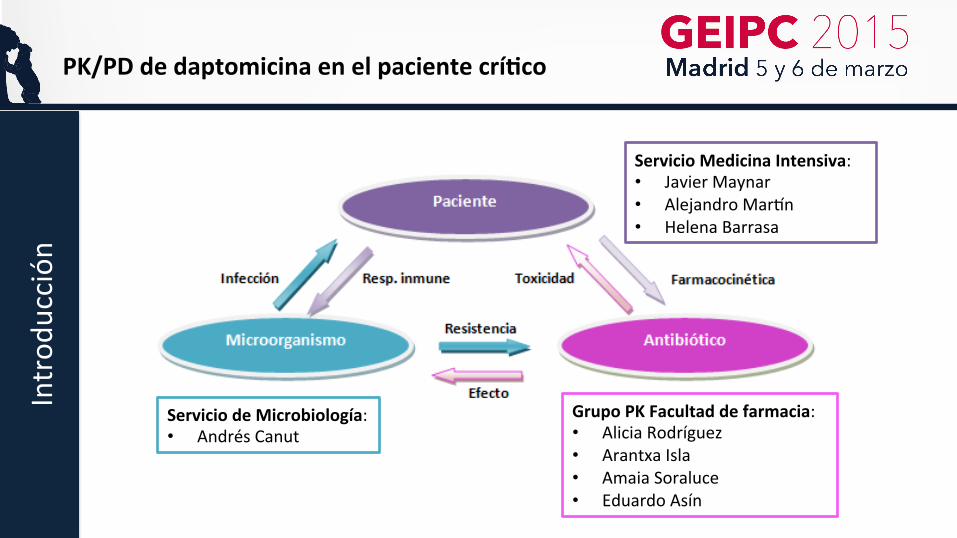
El uso adecuado de antimicrobianos debe tener en cuenta no sólo la susceptibilidad del agente infeccioso al antibiótico, sino también las complejas interacciones que se dan entre el fármaco, el paciente y el microorganismo (Figura 1). La diversidad en estas interacciones se traduce en una alta variabilidad en la relación dosis-respuesta.2
Esta variabilidad a menudo se ve aumentada en enfermos críticos, ya que, debido a los
cambios patológicos y a los factores relacionados con el manejo clínico durante el ingreso, la farmacocinética en estos pacientes se ve alterada. De esta forma, procesos tales como la absorción, la distribución, el metabolismo o la eliminación variarán mucho de un paciente a otro; además, el comportamiento cinético variará en función de la situación clínica del individuo, y es diferente al de otros grupos de pacientes.2 A modo de ejemplo, en la Figura 2 se
1 Graus S, Álvarez-Lerma F, Dominguez Gil A. Pharmacokinetic/pharmacodinamic índices: are we ready to use them in daily practice?Expert Rev Anti Infect Ther. 2007;5(6):913-916. 2 Carlos-Beltrán B. Farmacocinética y farmacodinamia de antimicrobianos: Utilidad práctica. Rev Chil Infect. 2004; 21 (Supl 1): S39-S44.
Figura 1.- Triángulo de Davis. Complejidad del proceso infeccioso y la respuesta al tratamiento farmacológico
Servicio Medicina Intensiva: • Javier Maynar • Alejandro Mar1n • Helena Barrasa
Servicio de Microbiología: • Andrés Canut
Grupo PK Facultad de farmacia: • Alicia Rodríguez • Arantxa Isla • Amaia Soraluce • Eduardo Asín
Introd
ucción
PK/PD de daptomicina en el paciente crí3co
Introd
ucción
PK/PD de daptomicina en el paciente crí3co
• Las infecciones que se dan en los Servicios de Medicina Intensiva (SMI) están asociadas a una alta morbilidad y mortalidad
• La precocidad en el inicio del tratamiento antibiótico, como el uso del antimicrobiano más adecuado son las intervenciones más importantes para reducir la morbi-mortalidad asociada a la infección
• La idoneidad de un tratamiento antibiótico no solo está condicionada por una adecuada selección del antibiótico, sino que también va a depender del régimen de dosificación utilizado
• Una mala utilización de los tratamientos antimicrobianos puede ser responsable de una ñtasa de fracaso terapéutico, un ñmortalidad, ñtoxicidad, incremento en los costes y aparición de resistencias
① Farmacocinética y Farmacodinamia
Farmacocinética:
ü Evolución de los niveles de un fármaco en el organismo a lo largo del tiempo.
ü Parámetros: Cmax, Css, Cmin, Vd, AUC…
Farmacodinamia: ü Cuantifica la actividad de un agente antimicrobiano, condicionada por
ü Las concentraciones que se alcanzan en el lugar de acción, dependientes del comportamiento farmacocinético
ü La sensibilidad del microorganismo al antibiótico, expresada como CMI.
PK/PD de daptomicina en el paciente crí3co Introd
ucción

Clasificación de antibióticos: PD a) Actividad concentración dependiente y
prolongado EPA. – Eficacia: Cmax/CMI y/o el AUC0-24/CMI. – Altas dosis, y el prolongado EPA è
intervalos de dosificación amplios (una dosis diaria).
– Ej. aminoglucósidos, fluoroquinolonas, metronidazol o daptomicina
b) Actividad tiempo dependiente y EPA mínimo o moderado.
– Parámetro (T>CMI).
– Ej. ß-lactámicos
c) Actividad concentración-independiente y prolongado EPA.
– Objetivo: optimizar la dosis – Parámetro: AUC0-24/CMI
– Ej. glucopéptidos, linezolid, tetraciclinas, clindamicina, azitromicina y glicilciclinas.
PK/PD de daptomicina en el paciente crí3co Introd
ucción
considered in earlier studies, and that many data retrievedfrom older literature established only the relationship be-tween Cmax/MIC and effect parameter. From a theoreticalpoint of view, most of the antibiotics should show a relation-ship with AUC and effect rather than Cmax.
Based on the PK/PD indices, antibiotics can be classifiedinto three categories that, by and large reflect their modes ofbacterial killing.28–30 The first category includes antibioticswhere the difference between the maximum effect andminimum effect is relatively large, and increasing concen-trations result in progressively increased killing. Therefore,these are also sometimes called concentration-dependentantibiotics, and include aminoglycosides and quinolones.For these antimicrobials, AUC/MIC describes their antibioticactivity best, and, mainly because AUC/MIC is closely corre-lated to Cmax/MIC, Cmax/MIC as well.31,32 On the other hand,time-dependent antibiotics’ activity, such as the β-lactams, isstrongly correlated with fT>MIC and as such, prolonging theduration of effective drug exposure should be the prioritywhen this antibiotic class is used.33,34 However, some anti-biotics such as the glycopeptides are more complex wherethey are found to display both concentration- and time-dependent kill characteristics.34 For these antibiotics, theratio of AUC0–24/MIC describes their antibiotic activity bestand higher thresholds are closely related to successful clinicaloutcome.35
Pharmacokinetic/PharmacodynamicConsiderations and the ResistanceDescriptors
Most of the earlier research on optimizing antibiotic dosingwas focused only on maximizing clinical and microbiological
cure and not on minimization of the emergence of antibioticresistance. To date, most of the data describing PK/PD and itsassociation with antibiotic resistance comes from preclinical,albeit advanced, PK/PD infection models. However, the anti-biotic exposure required for clinical efficacy and resistancesuppression is markedly different. For instance, the antibioticexposure–response relationship for clinical efficacy is mono-tonic or can also be described as a sigmoidal relationship inwhich no measurable antibiotic effect is expected at lowerdrug exposures while larger exposures are expected to aug-ment the bactericidal effect up to a certain threshold. Incontrast, the relationship between antibiotic exposure andthe selection of resistantmutants ismarkedly non-monotonicand has the shape of an inverted “U,”where resistant mutantsare amplified with initial antibiotic exposure and then slowlydecline with increasing exposure up to an optimal thresholdthat ultimately prevents resistance amplifications.36–39 Theinverted U-shape seems to follow a log normal distribution.40
In addition, Jumbe et al40 found that an AUC0–24/MIC of !110for levofloxacin, which was twice that was necessary foroptimal bactericidal effect, was required to suppress drug-resistant population of P. aeruginosa in a mouse thigh infec-tion model.41 This information, among other similar obser-vations, has indicated that themagnitude of the PK/PD indicesfor resistance suppression is generally different and higherthan the thresholds required for clinical success.37,42–44
Therefore, antibiotic dosing that only aims to optimize clinicalefficacy may potentially amplify resistance formation byselecting mutant bacterial strains with reduced drug suscep-tibility. With enhanced knowledge on antibiotic PK/PD overrecent years, important hypotheses and concepts, such as themutant selection window (MSW) and mutant preventionconcentrations (MPCs), have been proposed to provide
MIC
T>MIC
Cmax
AUC AUC
Concentration-dependent antibiotics (Cmax/MIC)e.g. Aminoglycosides, quinolones
Concentration- with/without time-dependence (AUC/MIC)e.g. Quinolones, aminoglycosides & glycopeptides
Time-dependent antibiotics (T>MIC)e.g. Beta-lactams
Cmin
Time (hours)
Fig. 1 The graphical illustration of fundamental pharmacokinetic and pharmacodynamic parameters of antibiotics on a hypotheticalconcentration–time curve. AUC, area under the concentration–time curve; Cmax, maximum drug concentration; Cmin, minimum drugconcentration; MIC, minimum inhibitory concentration; T>MIC, duration of time that drug concentration remains above MIC.
Seminars in Respiratory and Critical Care Medicine Vol. 36 No. 1/2015
Applying Pharmacokinetic/Pharmacodynamic Principles in Critically Ill Patients Abdul-Aziz et al.138
Down
load
ed b
y: IP
-Pro
xy O
sakid
etza
, Osa
kidet
za S
ervic
io V
asco
de
Salu
d. C
opyr
ight
ed m
ater
ial.
② Optimización del tratamiento antimicrobiano – Las propiedades PK/PD son el principal factor determinante de la eficacia
in vivo de los antimicrobianos
– Para poder diseñar los regímenes de dosificación es necesario conocer las características PK/PD de los antimicrobianos
– Cambios fisiopatológicos en pacientes críticos que alteran la PK/PD de los fármacos
PK/PD de daptomicina en el paciente crí3co Introd
ucción
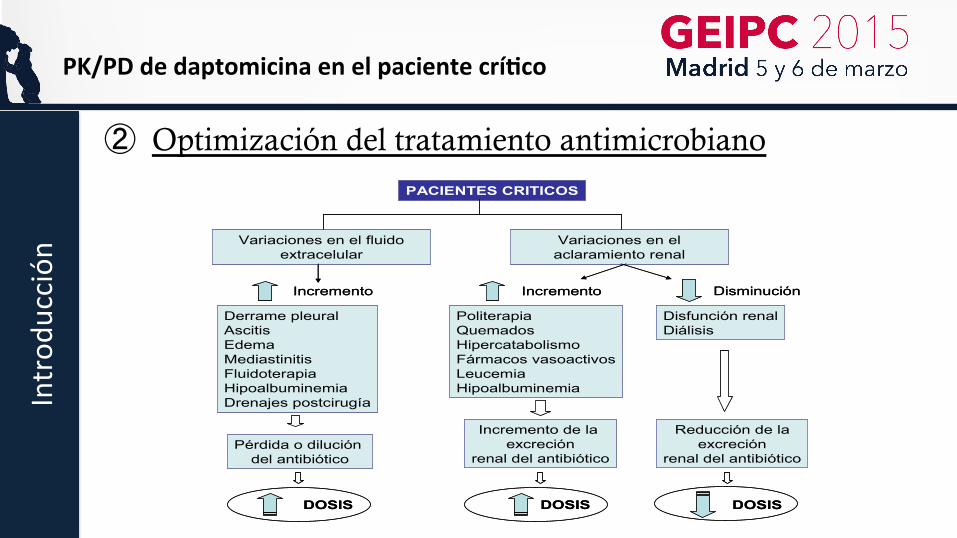
② Optimización del tratamiento antimicrobiano
PACIENTES CRITICOS
Variaciones en el fluido extracelular
Variaciones en el aclaramiento renal
Derrame pleuralAscitisEdemaMediastinitisFluidoterapiaHipoalbuminemiaDrenajes postcirugía
Incremento Incremento Disminución
Pérdida o dilución del antibiótico
PoliterapiaQuemadosHipercatabolismoFármacos vasoactivosLeucemiaHipoalbuminemia
Disfunción renalDiálisis
Reducción de laexcreción
renal del antibiótico
Incremento de la excreción
renal del antibiótico
DOSIS DOSISDOSIS
PACIENTES CRITICOS
Variaciones en el fluido extracelular
Variaciones en el aclaramiento renal
Derrame pleuralAscitisEdemaMediastinitisFluidoterapiaHipoalbuminemiaDrenajes postcirugía
Incremento Incremento Disminución
Pérdida o dilución del antibiótico
PoliterapiaQuemadosHipercatabolismoFármacos vasoactivosLeucemiaHipoalbuminemia
Disfunción renalDiálisis
Reducción de laexcreción
renal del antibiótico
Incremento de la excreción
renal del antibiótico
DOSIS DOSISDOSIS
PK/PD de daptomicina en el paciente crí3co Introd
ucción
② Optimización del tratamiento antimicrobiano
– Antibioterapia adecuada: • Régimen terapéutico con actividad demostrada in vitro frente al
microorganismo causal – Ej. el microorganismo aislado de la muestra clínica es sensible al tratamiento
empírico inicialmente prescrito
– Antibioterapia óptima: • Selección del antimicrobiano y el régimen de dosificación adecuados que
consiguen los mejores resultados clínicos con los mínimos efectos adversos para el paciente y el mínimo impacto en el desarrollo de resistencias.
PK/PD de daptomicina en el paciente crí3co Introd
ucción

Cómo citar este artículo: Canut Blasco A, et al. Análisis farmacocinético-farmacodinámico en microbiología: herramienta para evaluarel tratamiento antimicrobiano. Enferm Infecc Microbiol Clin. 2013. http://dx.doi.org/10.1016/j.eimc.2013.04.023
ARTICLE IN PRESSG ModelEIMC-964; No. of Pages 10
A. Canut Blasco et al / Enferm Infecc Microbiol Clin. 2013;xxx(xx):xxx–xxx 3
utilizan a altas dosis, y el prolongado EPA permite utilizar inter-valos de dosificación amplios (una dosis diaria). Ejemplos de estegrupo son:• Aminoglucósidos. Cmax/CMI ≥ 10-12.• Fluoroquinolonas. AUC24h/CMI ≥ 25-30 (infecciones no gra-
ves e infección respiratoria por Streptococcus pneumoniae),AUC24h ≥ 125 (infecciones graves y en inmunodeprimidos).
• Metronidazol. Índice PK/PD no establecido.• Daptomicina. AUC24h/CMI ≥ 666.
2. Antibióticos con actividad dependiente del tiempo y efecto post-antibiótico mínimo o moderado. El objetivo de la terapia esconseguir una larga exposición al antibiótico. Para los antibió-ticos incluidos en este grupo, el tiempo durante el cual lasconcentraciones permanecen por encima de la CMI (T > CMI) esel parámetro relacionado con la erradicación bacteriana y la res-puesta microbiológica. Este parámetro se denomina tiempo deeficacia. Cuanto menor es la semivida de eliminación, mayor esla frecuencia con la que hay que administrar estos antibióticos.Si la semivida es inferior a 2 h es difícil mantener un T > CMI porencima del 100% del intervalo de dosificación. En algunos casosla perfusión continua es la forma más efectiva de administrarestos antibióticos, especialmente si se requiere un valor alto deT > CMI. Los betalactámicos y los macrólidos son antibióticos quepertenecen a este grupo.• Betalactámicos. Penicilinas f T > CMI > 50% (el tiempo durante
el cual la concentración de fármaco libre está por encima dela CMI debe ser superior al 50% del intervalo de dosificación);cefalosporinas y aztreonam f T > CMI > 60-70% y carbapenemasf T > CMI > 30-40%.
• Macrólidos. f T > CMI > 40%.3. Antibióticos con actividad independiente de la concentración y
prolongado efecto post-antibiótico. Al aumentar la concentraciónde estos antibióticos la erradicación bacteriana aumenta sololigeramente, pero se consigue una prolongada inhibición del cre-cimiento. El objetivo en estos casos es optimizar la dosis, y elAUC24h/CMI es el parámetro relacionado con la eficacia. Este esel perfil de actividad de:• Glucopéptidos. Vancomicina: AUC24h/CMI ≥ 400.• Linezolid. AUC24h/CMI ≥ 100.• Tetraciclinas. AUC24h/CMI ≥ 15-25.• Clindamicina. Índice PK/PD no establecido.• Azitromicina. AUC24h/CMI ≥ 25.• Glicilciclinas. Tigeciclina: AUC24h ≥ 15-20.
Análisis farmacocinético/farmacodinámico en antibioterapia.Puntos de corte (breakpoints) farmacocinético/farmacodinámico
Para poder disenar los regímenes de dosificación de los anti-bióticos es necesario conocer sus características PK y PD. Además,hay que tener en cuenta que en pacientes críticos la dosificaciónse complica debido a los cambios fisiopatológicos que pueden alte-rar las características PK y, por tanto, la eficacia de los antibióticos.Se sabe que muchos regímenes de dosificación que han sido apli-cados a pacientes no críticos son poco apropiados para pacientescríticos13.
Los clínicos se enfrentan diariamente a la selección del régimende dosificación más adecuado para conseguir el objetivo PK/PD queasegure la máxima probabilidad de erradicación bacteriana y unaalta probabilidad de resolución de la infección. Son numerosas lasalteraciones patológicas que pueden modificar el comportamientoPK de los fármacos13, y el número de pacientes que pueden incluirseen estudios para conocer mejor estos cambios es muy limitado.Por ello, estrategias como la simulación de Montecarlo son de granvalor para guiar a los clínicos en la práctica diaria para una mejorselección de los tratamientos antimicrobianos.
Antibiótico
• Parámetros PK (distribución y varianza)Modelo PK:
Modelo PK/PD:
Sensibilidadin vitro:
CMI
Bacteria PacienteSimulación demontecarlo
Relación parámetros PK con CMI
• Covariables
Probabilidad de que el índice PK/PD (AUC24h/CMI, Cmax/CMI,T>CMI) alcance el valor relacionado con la eficacia
Figura 1. Relación entre todos los elementos necesarios para la simulación de Mon-tecarlo.
Simulación de Montecarlo. Probabilidad de alcanzar el objetivofarmacodinámico. Fracción de respuesta acumulada
La simulación de Montecarlo es una técnica matemática com-putarizada que permite «expandir» el tamano de una muestrapermitiendo ver todos los resultados posibles de las decisionesque tomamos y evaluar el impacto del riesgo, lo cual nos per-mite tomar mejores decisiones en condiciones de incertidumbre.Aplicada al análisis PK/PD, la simulación de Montecarlo consi-dera la variabilidad de los parámetros tanto PK como PD. Cadagrupo de parámetros se describe como una distribución de valorespara los cuales se asocia una probabilidad de inhibir al micro-organismo implicado. De esta manera podemos determinar laproporción de población en que se están alcanzando los índicesrequeridos para una CMI determinada. De ello se deriva que pue-den ser necesarias diferentes dosis para cada microorganismo,ya que su distribución de valores de CMI es variable. A ello seanade la variabilidad en las concentraciones de antibiótico alcan-zadas en el lugar de la infección, y la variabilidad PK individual.La simulación de Montecarlo permite combinar estas variabilida-des para disenar regímenes de dosificación que permitan alcanzaruna probabilidad de éxito determinada, basada en índices PK/PD.La simulación de Montecarlo se puede utilizar en antibiotera-pia con distintos fines: comparar antibióticos, definir criterios dedosificación o demostrar la validez de un antibiótico en una deter-minada situación (profilaxis, tratamiento empírico, insuficienciarenal, etc.).
En el contexto de la dosificación de antibióticos, los principa-les elementos para llevar a cabo una simulación de Montecarloson: a) un modelo PK robusto y bien definido con los correspon-dientes parámetros PK (distribución y varianza); b) un modelo decovariables que proporcione información sobre cómo cambian losparámetros PK en función de variables fisiopatológicas o varia-bles demográficas, y c) un modelo PD con una relación definidaentre los parámetros PK y PD. Así, la simulación de Montecarlo nospermite calcular la probabilidad de que con un determinado trata-miento antimicrobiano el valor del índice de eficacia (AUC24h/CMIo T > CMI) alcance el valor relacionado con la eficacia. Este valor deprobabilidad se conoce como probabilidad de alcanzar el objetivofarmacodinámico o probability of target attainment (PTA). Valoresde PTA > 90% se consideran indicativos de eficacia.
En la figura 1 se recoge un esquema con la interrelación entretodos los elementos necesarios para la simulación de Montecarloaplicada al análisis PK/PD.
③ Simulación de Monte Carlo – Modelo matemático
• Expansión muestraè resultados
– Tomar decisiones en condiciones de
incertidumbre
– Aplicada al análisis PK/PD:
determinar la proporción de
población en que se están alcanzando
el objetivo para una CMI determinada
PK/PD de daptomicina en el paciente crí3co Introd
ucción
④ Daptomicina
• Pertenece a la familia de los lipopéptidos. Actividad frente a Estafilococos, estreptococos (CMI ≤ 1mg/L) y Enterococos (CMI ≤ 4mg/L) , incluyendo especies resistentes a otros AB. Bactericida sin destrucción celular.
• Indicaciones aprobadas: – Tratamiento de infecciones complicadas de piel y tejidos blandos (4mg/Kg/día); tratamiento
de bacteriemia y endocarditis derecha por S. aureus sensible a meticilina (SASM) y SARM (6mg/Kg/día).
• Posibles indicaciones:
– Estudios en curso sugieren que puede ser una alternativa útil en osteomielitis, infecciones asociadas a dispositivos ortopédicos, infecciones asociadas a biopelículas e infecciones en pacientes inmunosuprimidos, en particular en pacientes onco-hematológicos, así como fármaco de 1ª línea en bacteriemia por SARM.
PK/PD de daptomicina en el paciente crí3co Introd
ucción
• Características farmacocinéticas:
• Efectos adversos: – Miopatía (Cmin> 24.3 mg/dL). Neumonia eosinofílica
• Características farmacodinámicas: – Actividad batericida rápida, potente y concentración dependiente. Prolongado EPA(6.8h). Parámetro:
AUC/CMI.
Papel de daptomicina en el tratamiento empírico y dirigido de infecciones por cocos grampositivos delpaciente crítico
J. Garnacho-Montero, et al.
27 15Rev Esp Quimioter 2011;24(1):13-24
calcio. Se postula que los oligomeros formados crean canalesde potasio en la membrana, conduciendo a la pérdida depotasio y despolarización de la membrana. La alteración de lasíntesis de las macromoléculas dependientes de potasio es lacausa de la muerte celular. Ello produce una escasa respuestainflamatoria, y aunque el mecanismo exacto es desconocido, esposible que haya menos fragmentos bacterianos inflamatoriosliberados por la daptomicina que por otros agentes bacterianos.Este es el mecanismo que no produce lisis celular y minimiza laliberación de toxinas bacterianas a la circulación. La acción dela daptomicina es rápidamente bactericida e independiente delinóculo bacteriano. La interacción directa con la membranasugiere que la daptomicina puede actuar independientementede la fase de crecimiento o actividad metabólica celular. Noestá indicada en caso de infecciones pulmonares pues esinactivada por el surfactante pulmonar10.
Su acción bactericida es concentración dependiente por loque el parámetro farmacocinético que correlaciona másestrechamente la eficacia antibacteriana de este antibiótico y,
por lo tanto, actúa como predictor de su farmacodinamiaantibacteriana es el relación entre el área bajo la curva (ABC) yla CMI. Sus propiedades farmacocinéticas se resumen en latabla 1. No se metaboliza por los microsomas hepáticoshumanos y no inhibe o induce al citocromo P45011, por lo queno existen descritas interacciones con otros fármacos.
Debe monitorizarse los niveles de creatinfosfokinasa (CPK)dado que puede ocasionar daño muscular con elevación de laCPK que revierte tras la suspensión del fármaco. No ocasionatoxicidad hepática o renal. Las dosis aprobadas de daptomicinason de 4-6 mg/kg. Sin embargo, estudios recientes handemostrado la eficacia y seguridad del fármaco cuando seemplea a dosis elevadas de 8 y hasta 10 mg/kg. En estosestudios, la duración media del tratamiento fue de 15 días, solose detectó como efecto adverso elevaciones de la CPK queafectaron a menos del 5 % de los pacientes12,13. Estaselevaciones se resolvieron tras suspender el fármaco. Losajustes de dosis en situaciones especiales, incluyendo ladepuración extra-renal14, 15, se resumen en la tabla 2.
PAPEL DE LA DAPTOMICINA EN EL TRATAMIENTOEMPIRICO Y DIRIGIDO DE LAS BACTERIEMIAS PORCATÉTER Y LA BACTERIEMIA PRIMARIA
La bacteriemia por catéter sigue siendo un problema gravecuya morbilidad y mortalidad es mayor cuando bacterias deelevada patogenicidad como S. aureus son responsables delepisodio. La administración temprana de antimicrobianos en elpaciente con bacteriemia contribuye a un pronóstico mejor y labacteriemia por SARM no es una excepción como se hademostrado recientemente en un estudio con diseño de casos ycontroles16. Pero además, en el caso de bacteriemia por SARMse da la particularidad que la tasa de fallo de tratamiento ymortalidad son mayores en episodios tratados con vancomicinacuando la cepa causante de la infección siendo sensible a lamisma presenta una CMI >1 mg/L3,4,17. En estos estudios ladeterminación de la CMI a vancomicina se realizó mediante elmétodo del E-test. En caso de bacteriemia por catéter nodebemos olvidar la importancia de la retirada precoz del mismodado que la demora más allá de 24 horas en su retirada seasocia de forma significativa a una mayor mortalidad18.
Las características farmacocinéticas y de mecanismos deacción de daptomicina, sobre todo su rápido poder bactericida,sirvieron para apuntar desde el inicio de su desarrollo clínico aque el antibiótico tuviera un papel importante en eltratamiento de bacteriemias por cocos grampositivos. Hay querecordar que daptomicina tiene un volumen de distribuciónbajo (0,1 ml/Kg) lo que nos indica que permaneceespecialmente en plasma y tejidos muy vascularizados.
En 2006 se publicó el trabajo que sirvió para la aprobaciónde daptomicina en bacteriemias y endocarditis derecha19. Setrata de un estudio multicéntrico, abierto, planteado como deno inferioridad (margen de diferencia 20%), para estudiar laeficacia y seguridad de la daptomicina en el tratamiento debacteriemias con o sin endocarditis causadas por S. aureus. Se
Tabla 1 Daptomicina: Propiedadesfarmacocinéticas
• Farmacocinética lineal, vida media 8-9 horas• Unión a proteínas plasmáticas 90-93%• Volumen de distribución bajo (0,1 ml/kg)• Excreción
Renal 78%Heces 6%
• No interactúa con el Citocromo P450• Inactivada por surfactante pulmonar• Penetración en meninges inflamada: 6%
Tabla 2 Dosificación de daptomicina.Situaciones especiales
• Dosis aprobada — Infección de piel y partes blandas: 4 mg/kg/d— Bacteriemia incluyendo endocarditis: 6 mg/kg/d
• Paciente crítico (dosis recomendada). 8-10 mg/kg/d(vigilar estrechamente CPK)
• Gran quemado: 10-12 mg/kg/d (primeras 4 semanas)• Obesidad mórbida: Dosis ajustada a peso real• Insuficiencia renal con aclaramiento de creatinina >
30 ml/min: Sin cambios• Insuficiencia renal con aclaramiento de creatinina <
30 ml/min Dosis requerida administrada cada 48 h• Insuficiencia renal en hemodiálisis: 4-6 mg/kg/48h.
Administración tras la hemodiálisis• Insuficiencia renal en HFVVC 4-6 mg/kg/d• Insuficiencia hepática leve-moderada: 4-6 mg/kg/día• Insuficiencia hepática grave (Child Pugh C): No hay
datos
1568 • CID 2010:50 (15 June) • Bhavnani et al.
M A J O R A R T I C L E
Daptomycin Exposure and the Probabilityof Elevations in the Creatine Phosphokinase Level:Data from a Randomized Trial of Patientswith Bacteremia and Endocarditis
Sujata M. Bhavnani, Christopher M. Rubino, Paul G. Ambrose, and George L. DrusanoInstitute for Clinical Pharmacodynamics, Ordway Research Institute, Albany, New York
Background. The objective of this analysis was to evaluate the relationship between daptomycin exposure andthe probability of an elevation in the creatine phosphokinase (CPK) level (hereafter, “CPK elevation”) in patientswith Staphylococcus aureus bacteremia with or without infective endocarditis.
Methods. Phase 3 data for patients with S. aureus bacteremia, with or without infective endocarditis, whoreceived intravenous daptomycin (6 mg/kg daily) and in whom pharmacokinetic data were collected were evaluated.On the basis of univariate logistic regression, the relationship between Bayesian post hoc exposure estimates andthe probability of a CPK elevation was evaluated. Time to CPK elevation was examined with Kaplan-Meier analysisand Cox proportional hazards regression.
Results. Significant relationships between the minimum concentration of drug (Cmin) and area under the plasmaconcentration time curve and probability of CPK elevation were observed in 108 evaluable patients. Of the 108patients evaluated, 6 (5.56%) demonstrated a defined CPK elevation, regardless of treatment relationship. Cmin
(breakpoint of 24.3 mg/L) was most significantly associated with CPK elevation (P p .002). The probabilities ofa CPK elevation with a Cmin !24.3 mg/L and !24.3 mg/L were 0.5 and 0.029, respectively. Increases in Cmin,evaluated as a continuous variable, were also significantly associated with CPK elevation (P p .01). StratifiedKaplan-Meier analysis and Cox proportional hazards regression demonstrated Cmin to be a significant predictorof time to a CPK elevation (P " .003). The probability of a CPK elevation was 0 and 0.01 after 7 days of treatmentin patients with a Cmin !24.3 mg/L or !24.3 mg/L, respectively. After 14 days, the probabilities were 0.5 and 0.025,respectively.
Conclusions. This analysis demonstrated that a daptomycin Cmin !24.3 mg/L was associated with an increasedprobability of a CPK elevation.
Clinical trials registration. Clinical trials.gov NCT00093067.
Daptomycin is a cyclic lipopeptide antibacterial agentwith in vitro activity against gram-positive bacteria, in-cluding methicillin-resistant Staphylococcus aureus. Inthe early 1990s, clinical trials for this agent [1] used a12-h dosing interval. After observing a signal of anadverse skeletal muscle effect at a dose level of 4 mg/
Received 6 October 2009; accepted 1 March 2010; electronically published 12May 2010.
Reprints or correspondence: Dr George L. Drusano, Institute for ClinicalPharmacodynamics, Ordway Research Institute, 150 New Scotland Ave, Albany,NY 12208 ([email protected]).
Clinical Infectious Diseases 2010; 50(12):1568–1574! 2010 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2010/5012-0003$15.00DOI: 10.1086/652767
kg administered every 12 h [2, 3], these trials werevoluntarily suspended. Subsequent studies in dogs re-ceiving daptomycin (75 mg/kg daily for 20 days) servedto demonstrate decreased skeletal myopathy and cre-atine phosphokinase (CPK) elevation when the dosewas administered once daily compared with 25 mg/kgevery 8 h [4], thereby supporting the study of once-daily dosing regimens in clinical trials that followed.Clinical studies of daptomycin administered daily dem-onstrated a lower incidence of elevations in the creatinephosphokinase (CPK) level (hereafter, “CPK eleva-tions”) [5, 6], thus supporting the findings in dogs [4].
After US Food and Drug Administration approval ofthis agent for the treatment of complicated skin andskin-structure infections attributable to gram-positive
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from
1568 • CID 2010:50 (15 June) • Bhavnani et al.
M A J O R A R T I C L E
Daptomycin Exposure and the Probabilityof Elevations in the Creatine Phosphokinase Level:Data from a Randomized Trial of Patientswith Bacteremia and Endocarditis
Sujata M. Bhavnani, Christopher M. Rubino, Paul G. Ambrose, and George L. DrusanoInstitute for Clinical Pharmacodynamics, Ordway Research Institute, Albany, New York
Background. The objective of this analysis was to evaluate the relationship between daptomycin exposure andthe probability of an elevation in the creatine phosphokinase (CPK) level (hereafter, “CPK elevation”) in patientswith Staphylococcus aureus bacteremia with or without infective endocarditis.
Methods. Phase 3 data for patients with S. aureus bacteremia, with or without infective endocarditis, whoreceived intravenous daptomycin (6 mg/kg daily) and in whom pharmacokinetic data were collected were evaluated.On the basis of univariate logistic regression, the relationship between Bayesian post hoc exposure estimates andthe probability of a CPK elevation was evaluated. Time to CPK elevation was examined with Kaplan-Meier analysisand Cox proportional hazards regression.
Results. Significant relationships between the minimum concentration of drug (Cmin) and area under the plasmaconcentration time curve and probability of CPK elevation were observed in 108 evaluable patients. Of the 108patients evaluated, 6 (5.56%) demonstrated a defined CPK elevation, regardless of treatment relationship. Cmin
(breakpoint of 24.3 mg/L) was most significantly associated with CPK elevation (P p .002). The probabilities ofa CPK elevation with a Cmin !24.3 mg/L and !24.3 mg/L were 0.5 and 0.029, respectively. Increases in Cmin,evaluated as a continuous variable, were also significantly associated with CPK elevation (P p .01). StratifiedKaplan-Meier analysis and Cox proportional hazards regression demonstrated Cmin to be a significant predictorof time to a CPK elevation (P " .003). The probability of a CPK elevation was 0 and 0.01 after 7 days of treatmentin patients with a Cmin !24.3 mg/L or !24.3 mg/L, respectively. After 14 days, the probabilities were 0.5 and 0.025,respectively.
Conclusions. This analysis demonstrated that a daptomycin Cmin !24.3 mg/L was associated with an increasedprobability of a CPK elevation.
Clinical trials registration. Clinical trials.gov NCT00093067.
Daptomycin is a cyclic lipopeptide antibacterial agentwith in vitro activity against gram-positive bacteria, in-cluding methicillin-resistant Staphylococcus aureus. Inthe early 1990s, clinical trials for this agent [1] used a12-h dosing interval. After observing a signal of anadverse skeletal muscle effect at a dose level of 4 mg/
Received 6 October 2009; accepted 1 March 2010; electronically published 12May 2010.
Reprints or correspondence: Dr George L. Drusano, Institute for ClinicalPharmacodynamics, Ordway Research Institute, 150 New Scotland Ave, Albany,NY 12208 ([email protected]).
Clinical Infectious Diseases 2010; 50(12):1568–1574! 2010 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2010/5012-0003$15.00DOI: 10.1086/652767
kg administered every 12 h [2, 3], these trials werevoluntarily suspended. Subsequent studies in dogs re-ceiving daptomycin (75 mg/kg daily for 20 days) servedto demonstrate decreased skeletal myopathy and cre-atine phosphokinase (CPK) elevation when the dosewas administered once daily compared with 25 mg/kgevery 8 h [4], thereby supporting the study of once-daily dosing regimens in clinical trials that followed.Clinical studies of daptomycin administered daily dem-onstrated a lower incidence of elevations in the creatinephosphokinase (CPK) level (hereafter, “CPK eleva-tions”) [5, 6], thus supporting the findings in dogs [4].
After US Food and Drug Administration approval ofthis agent for the treatment of complicated skin andskin-structure infections attributable to gram-positive
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from
PK/PD de daptomicina en el paciente crí3co Introd
ucción
I
Procedimientos en Microbiología Clínica
Recomendaciones de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica
Editores: Emilia Cercenado y Rafael Cantón
Coordinador: Andrés Canut Blasco Autores: Lorenzo Aguilar Alfaro Andrés Canut Blasco
Javier Cobo Reinoso Mª José Giménez Mestre
Alicia Rodríguez Gascón
ISBN-13: 978-84-616-4130-7
46. Análisis farmacocinético-
farmacodinámico en Microbiología: herramienta para evaluar el tratamiento
antimicrobiano
2 0 1 3 I
Procedimientos en Microbiología Clínica
Recomendaciones de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica
Editores: Emilia Cercenado y Rafael Cantón
Coordinador: Andrés Canut Blasco Autores: Lorenzo Aguilar Alfaro Andrés Canut Blasco
Javier Cobo Reinoso Mª José Giménez Mestre
Alicia Rodríguez Gascón
ISBN-13: 978-84-616-4130-7
46. Análisis farmacocinético-
farmacodinámico en Microbiología: herramienta para evaluar el tratamiento
antimicrobiano
2 0 1 3
I
Procedimientos en Microbiología Clínica
Recomendaciones de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica
Editores: Emilia Cercenado y Rafael Cantón
Coordinador: Andrés Canut Blasco Autores: Lorenzo Aguilar Alfaro Andrés Canut Blasco
Javier Cobo Reinoso Mª José Giménez Mestre
Alicia Rodríguez Gascón
ISBN-13: 978-84-616-4130-7
46. Análisis farmacocinético-
farmacodinámico en Microbiología: herramienta para evaluar el tratamiento
antimicrobiano
2 0 1 3
Author's personal copy
International Journal of Antimicrobial Agents 40 (2012) 313– 322
Contents lists available at SciVerse ScienceDirect
International Journal of Antimicrobial Agents
jou rn al h om epa ge: h t tp : / /www.e lsev ier .com/ locate / i jant imicag
Comparison of antimicrobial pharmacokinetic/pharmacodynamic breakpointswith EUCAST and CLSI clinical breakpoints for Gram-positive bacteria
Eduardo Asína, Arantxazu Islaa, Andrés Canutb, Alicia Rodríguez Gascóna,∗
a Pharmacokinetics, Nanotechnology and Gene Therapy Group, Faculty of Pharmacy, University of the Basque Country, 01006 Vitoria-Gasteiz, Spainb Microbiology Unit, Hospital Universitario de Álava, 01004 Vitoria-Gasteiz, Spain
a r t i c l e i n f o
Article history:Received 7 February 2012Accepted 8 June 2012
Keywords:Monte Carlo simulationMinimum inhibitory concentration (MIC)Pharmacokinetics/pharmacodynamicsStaphylococciEnterococciStreptococci
a b s t r a c t
This study compared the susceptibility breakpoints based on pharmacokinetic/pharmacodynamic(PK/PD) models and Monte Carlo simulation with those defined by the Clinical and Laboratory Stan-dards Institute (CLSI) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) forantibiotics used for the treatment of infections caused by Gram-positive bacteria. A secondary objectivewas to evaluate the probability of achieving the PK/PD target associated with the success of antimicrobialtherapy. A 10 000-subject Monte Carlo simulation was executed to evaluate 13 antimicrobials (47 intra-venous dosing regimens). Susceptibility data were extracted from the British Society for AntimicrobialChemotherapy database for bacteraemia isolates. The probability of target attainment and the cumula-tive fraction of response (CFR) were calculated. No antibiotic was predicted to be effective (CFR ≥ 90%)against all microorganisms. The PK/PD susceptibility breakpoints were also estimated and were com-pared with CLSI and EUCAST breakpoints. The percentages of strains affected by breakpoint discrepancieswere calculated. In the case of !-lactams, breakpoint discrepancies affected <15% of strains. However,higher differences were detected for low doses of vancomycin, daptomycin and linezolid, with PK/PDbreakpoints being lower than those defined by the CLSI and EUCAST. If this occurs, an isolate will beconsidered susceptible based on CLSI and EUCAST breakpoints although the PK/PD analysis predicts fail-ure, which may explain treatment failures reported in the literature. This study reinforces the idea ofconsidering not only the antimicrobial activity but also the dosing regimen to increase the probability ofclinical success of an antimicrobial treatment.
© 2012 Elsevier B.V. and the International Society of Chemotherapy. All rights reserved.
1. Introduction
The resistance rates of Gram-positive bacteria, in par-ticular meticillin-resistant Staphylococcus aureus (MRSA),vancomycin-intermediate S. aureus, vancomycin-resistant S.aureus, vancomycin-resistant enterococci (VRE) and multidrug-resistant Streptococcus pneumoniae, are a major public healthproblem worldwide. Among the interventions to mitigate thecurrent and future impact of antimicrobial resistance, the devel-opment of new generations of antimicrobials is one of the mostaccepted. Another recognised strategy to diminish antibioticresistance is optimisation of the dosing regimen of availableantimicrobials [1].
∗ Corresponding author. Present address: Laboratory of Pharmacy and Pharma-ceutical Technology, Faculty of Pharmacy, University of the Basque Country, Paseode la Universidad 7, 01006 Vitoria-Gasteiz, Spain. Tel.: +34 945 01 30 94;fax: +34 945 01 30 40.
E-mail address: [email protected] (A. Rodríguez Gascón).
To maximise the likelihood of a favourable clini-cal/microbiological response as well as to minimise the probabilityof exposure-related toxicity, pharmacokinetic/pharmacodynamic(PK/PD) modelling represents a very useful tool for dose decision-making. Use of Monte Carlo simulation provides an estimateof an antibiotic dosing regimen’s probability of achieving thetargeted pharmacodynamic exposure, given uncertainty in patientpharmacokinetics and the minimum inhibitory concentration(MIC) distribution of the bacterial population [2]. Based on MonteCarlo simulation, we showed differences in the probability ofsuccess of several dosing regimens of vancomycin, linezolid,daptomycin and tigecycline for the treatment of MRSA infectionsin four Western European countries owing to differences insusceptibility patterns [3]. Another application of PK/PD analysisand Monte Carlo simulation is the establishment of breakpointsbased on the likelihood of obtaining a targeted exposure [4].Pharmacodynamics is considered by regulatory agencies for thedevelopment of susceptibility breakpoints to be used by clinicalmicrobiology laboratories to categorise organisms as susceptibleor resistant. However, divergences between the probability ofpharmacodynamic target attainment and current susceptibility
0924-8579/$ – see front matter © 2012 Elsevier B.V. and the International Society of Chemotherapy. All rights reserved.http://dx.doi.org/10.1016/j.ijantimicag.2012.06.005
10
Tabla 4. Puntos de corte para cocos grampositivos obtenidos según el análisis PK/PD para los diferentes regímenes de dosificación.
ANTIBIÓTICO* POSOLOGÍA INDICE DE EFICACIA
VALOR A ALCANZAR
PUNTO DE CORTE PK/PD (mg/L)
TZP 4g/6h fT>CMI 50% 4
AMX 1g/6h fT>CMI 50% 2
1g/8h fT>CMI 50% 0,5
CFP 1-2 g/12 h fT>CMI 50% 1
1-2 g/8 h fT>CMI 50% 4
CTX 1g/8h fT>CMI 50% 0,5
2g/8h fT>CMI 50% 1
ETP 1g/12h fT>CMI 50% 1
1g/24h fT>CMI 50% 0,125
IPM 500mg/8h fT>CMI 50% 1
MEM 1g/8h fT>CMI 50% 2
CIP 400mg/8-12h AUC24h/CMI 125 0,125
LVX 500 mg/24 h AUC24h/CMI 125 0,25
VAN 1g/24h AUC24h/CMI 400 0,25
1g/12h AUC24h/CMI 400 0,5
1-1,5g/8h y 2g/12h AUC24h/CMI 400 1
1,5g/6h AUC24h/CMI 400 2
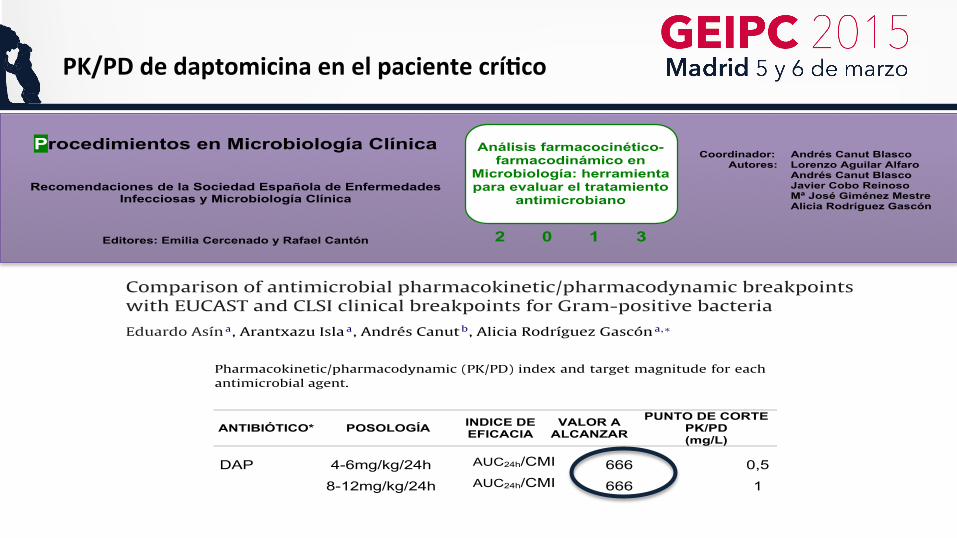
DAP 4-6mg/kg/24h AUC24h/CMI 666 0,5
8-12mg/kg/24h AUC24h/CMI 666 1
TGC 50mg/12h AUC24h/CMI 18 0,25
LZD 600mg/12h AUC24h/CMI 100 1 *TZP: piperacilina-tazobactam; AMX: amoxicilina; CFP: cefepima; CTX: cefotaxima; ETP: ertapenem; IMP: imipenem; MEM: meropenem; CIP: ciprofloxacino; LVX: levofloxacino; VAN: vancomicina; DAP: daptomicina; TGC: tigeciclina; LZD: linezolid. Tomado de: Asín E et al. Comparison of antimicrobial pharmacokinetic/pharmacodynamic breakpoints with EUCAST and CLSI clinical breakpoints for Gram-positive bacteria. Intern J Antimicrob Agents 2012; 40: 313-32.
10
Tabla 4. Puntos de corte para cocos grampositivos obtenidos según el análisis PK/PD para los diferentes regímenes de dosificación.
ANTIBIÓTICO* POSOLOGÍA INDICE DE EFICACIA
VALOR A ALCANZAR
PUNTO DE CORTE PK/PD (mg/L)
TZP 4g/6h fT>CMI 50% 4
AMX 1g/6h fT>CMI 50% 2
1g/8h fT>CMI 50% 0,5
CFP 1-2 g/12 h fT>CMI 50% 1
1-2 g/8 h fT>CMI 50% 4
CTX 1g/8h fT>CMI 50% 0,5
2g/8h fT>CMI 50% 1
ETP 1g/12h fT>CMI 50% 1
1g/24h fT>CMI 50% 0,125
IPM 500mg/8h fT>CMI 50% 1
MEM 1g/8h fT>CMI 50% 2
CIP 400mg/8-12h AUC24h/CMI 125 0,125
LVX 500 mg/24 h AUC24h/CMI 125 0,25
VAN 1g/24h AUC24h/CMI 400 0,25
1g/12h AUC24h/CMI 400 0,5
1-1,5g/8h y 2g/12h AUC24h/CMI 400 1
1,5g/6h AUC24h/CMI 400 2
DAP 4-6mg/kg/24h AUC24h/CMI 666 0,5
8-12mg/kg/24h AUC24h/CMI 666 1
TGC 50mg/12h AUC24h/CMI 18 0,25
LZD 600mg/12h AUC24h/CMI 100 1 *TZP: piperacilina-tazobactam; AMX: amoxicilina; CFP: cefepima; CTX: cefotaxima; ETP: ertapenem; IMP: imipenem; MEM: meropenem; CIP: ciprofloxacino; LVX: levofloxacino; VAN: vancomicina; DAP: daptomicina; TGC: tigeciclina; LZD: linezolid. Tomado de: Asín E et al. Comparison of antimicrobial pharmacokinetic/pharmacodynamic breakpoints with EUCAST and CLSI clinical breakpoints for Gram-positive bacteria. Intern J Antimicrob Agents 2012; 40: 313-32.
Author's personal copy
E. Asín et al. / International Journal of Antimicrobial Agents 40 (2012) 313– 322 315
A secondary objective of this study was to evaluate the probabil-ity of obtaining the PK/PD target with 47 dosing regimens of 13antibiotics used against Gram-positive bacteria.
2. Methods
2.1. Antimicrobials
Thirteen antimicrobials [47 intravenous (i.v.) dosing regimens]were chosen based on their routine use for treatment of Gram-positive infections. Table 1 lists all the dosing regimens studied.
Pharmacokinetic parameters were obtained from publishedpharmacokinetic studies. A search of the parameters was per-formed using the US National Library of Medicine’s ISI WebOf Knowledge combining the Medical Subject Heading (MeSH)‘pharmacokinetics’ or ‘population pharmacokinetics’ with eachantimicrobial’s International Non-proprietary Name (INN). Selec-tion of the different studies depended on the number ofparticipants, human race (Caucasian people) and age, year of publi-cation and pharmacokinetic model. Just one study was selected foreach antimicrobial, except for daptomycin for which two studieswere selected, reporting pharmacokinetic data for all regimens tobe studied. All parameters were expressed as mean and standarddeviation (S.D.) (Table 1).
2.2. Microbiology
MIC distributions for Enterococcus spp. (Enterococcus faecalisand Enterococcus faecium), Staphylococcus spp. [meticillin-resistantcoagulase-negative staphylococci (MR-CoNS), MRSA, meticillin-susceptible coagulase-negative staphylococci (MS-CoNS) andmeticillin-susceptible S. aureus (MSSA)] and Streptococcus spp.(Streptococcus pyogenes, Streptococcus agalactiae, Streptococcusanginosus, Streptococcus oralis and S. pneumoniae) were extractedfrom the British Society for Antimicrobial Chemotherapy (BSAC)database corresponding to bacteraemia isolates collected at hos-pitals from the UK and Ireland for every antimicrobial agent. Alldata were collected during 2009, except in the following cases:ertapenem (2007) and meropenem (2008) against enterococci andstreptococci.
2.3. Pharmacokinetic/pharmacodynamic analyses and MonteCarlo simulation
2.3.1. Probability of target attainment (PTA) estimationA 10 000-subject Monte Carlo simulation was conducted
for each antibiotic using Oracle® Crystal Ball Fusion Editionv.11.1.1.1.00 (Oracle USA Inc., Redwood City, CA). The PTA [19]is understood as the probability that a specific value of a PK/PDindex associated with the efficacy of the antimicrobial treatment isachieved at a certain MIC. Table 2 shows the magnitude or value ofthe PK/PD indices associated with the success of therapy for eachantimicrobial. The PTA was calculated over a range of doubling MICsbetween 0.002 mg/L and 512 mg/L using the following equations.
• For i.v. bolus-administered !-lactams:
f %T>MIC = Ln
✓D × (1 − PB) × (1 − exp(−n × (CLt/Vss) × !))
Vss × MIC × (1 − exp(−(CLt/Vss) × !))
◆
× Vss
CLt× 100
!
where f%T>MIC is the proportion of time that the free serum con-centration remains above the MIC at steady-state (%), Ln is thenatural logarithm, D is the dose of antibiotic administered (mg),PB is the fraction of drug bound to proteins in human serum
Table 2Pharmacokinetic/pharmacodynamic (PK/PD) index and target magnitude for eachantimicrobial agent.
Antimicrobial agent PK/PD index Magnitude
Amoxicillin [22] f%T>MIC 50Cloxacillin [22] f%T>MIC 50Piperacillin/tazobactam [22] f%T>MIC 50Cefotaxime [22] f%T>MIC 50Cefepime [22] f%T>MIC 50Ertapenem [22] f%T>MIC 30Imipenem [22] f%T>MIC 30Meropenem [22] f%T>MIC 30Levofloxacin [20] AUCSS/MIC 125Vancomycin [3] AUCSS/MIC 400Daptomycin [3] AUCSS/MIC 666Tigecycline [3] AUCSS/MIC 18Linezolid [3] AUCSS/MIC 100
f%T>MIC, percentage of time that the antimicrobial free serum concentrationremained above the MIC; MIC, minimum inhibitory concentration; AUCSS/MIC, ratioof the area under the antimicrobial concentration–time curve for 24 h divided by theMIC.
(%), Vss is the antimicrobial’s apparent volume of distribution atsteady-state (L), CLt is the total body clearance (L/h), ! is the dos-ing interval (h) and n is the dose number (fixed at 10). The subjectweight was fixed at 70 kg when necessary.
• For i.v. infusion-administered !-lactams:
t1 =MIC − fCmin,ss
fCmax,ss − fCmin,ss× tinf
t2 = Ln⇣
fCmax,ss
MIC
⌘× Vss
CLt
f %T>MIC = [(t2 + tinf ) − t1] × 100!
where fCmin,ss is the minimum serum concentration of unbounddrug (mg/L) at steady-state, fCmax,ss is the maximum serum con-centration of unbound drug (mg/L) at steady-state, tinf is theinfusion time (h), t1 corresponds to the time at which the con-centration reached the MIC during the infusion phase and t2corresponds to the post-infusion time at which the serum con-centration equalled the MIC in the elimination phase.
• For the rest of the antimicrobial agents:
AUCss
MIC= D × 24
MIC × ! × CLt
where AUCss is the area under the serum concentration–timecurve at steady-state over 24 h (mg h/L) [19].
Logarithmic transformation was applied to the mean and S.D.of all pharmacokinetic parameters to normalise their distributions,whereas protein binding was included following a uniform distri-bution (±10%).
2.3.2. Calculation of the cumulative fraction of response (CFR)CFR [19] is defined as the expected population PTA for a specific
drug dose and a specific population of microorganisms. It allowedus to calculate the probability of success for a treatment withoutknowledge of the clinical pathogen’s susceptibility and was calcu-lated taking into account the PTA for each MIC and the bacterialpopulation MIC distribution. A CFR ≥ 80% but <90% was associatedwith moderate probabilities of success, whereas a CFR ≥ 90% wasconsidered as optimal against that bacterial population [2].
PK/PD de daptomicina en el paciente crí3co
• Características farmacocinéticas:
• Efectos adversos: – Miopatía (Cmin> 24.3 mg/dL). Neumonia eosinofílica
• Características farmacodinámicas: – Actividad batericida rápida, potente y concentración dependiente. Prolongado EPA(6.8h). Parámetro:
AUC/CMI>666.
Papel de daptomicina en el tratamiento empírico y dirigido de infecciones por cocos grampositivos delpaciente crítico
J. Garnacho-Montero, et al.
27 15Rev Esp Quimioter 2011;24(1):13-24
calcio. Se postula que los oligomeros formados crean canalesde potasio en la membrana, conduciendo a la pérdida depotasio y despolarización de la membrana. La alteración de lasíntesis de las macromoléculas dependientes de potasio es lacausa de la muerte celular. Ello produce una escasa respuestainflamatoria, y aunque el mecanismo exacto es desconocido, esposible que haya menos fragmentos bacterianos inflamatoriosliberados por la daptomicina que por otros agentes bacterianos.Este es el mecanismo que no produce lisis celular y minimiza laliberación de toxinas bacterianas a la circulación. La acción dela daptomicina es rápidamente bactericida e independiente delinóculo bacteriano. La interacción directa con la membranasugiere que la daptomicina puede actuar independientementede la fase de crecimiento o actividad metabólica celular. Noestá indicada en caso de infecciones pulmonares pues esinactivada por el surfactante pulmonar10.
Su acción bactericida es concentración dependiente por loque el parámetro farmacocinético que correlaciona másestrechamente la eficacia antibacteriana de este antibiótico y,
por lo tanto, actúa como predictor de su farmacodinamiaantibacteriana es el relación entre el área bajo la curva (ABC) yla CMI. Sus propiedades farmacocinéticas se resumen en latabla 1. No se metaboliza por los microsomas hepáticoshumanos y no inhibe o induce al citocromo P45011, por lo queno existen descritas interacciones con otros fármacos.
Debe monitorizarse los niveles de creatinfosfokinasa (CPK)dado que puede ocasionar daño muscular con elevación de laCPK que revierte tras la suspensión del fármaco. No ocasionatoxicidad hepática o renal. Las dosis aprobadas de daptomicinason de 4-6 mg/kg. Sin embargo, estudios recientes handemostrado la eficacia y seguridad del fármaco cuando seemplea a dosis elevadas de 8 y hasta 10 mg/kg. En estosestudios, la duración media del tratamiento fue de 15 días, solose detectó como efecto adverso elevaciones de la CPK queafectaron a menos del 5 % de los pacientes12,13. Estaselevaciones se resolvieron tras suspender el fármaco. Losajustes de dosis en situaciones especiales, incluyendo ladepuración extra-renal14, 15, se resumen en la tabla 2.
PAPEL DE LA DAPTOMICINA EN EL TRATAMIENTOEMPIRICO Y DIRIGIDO DE LAS BACTERIEMIAS PORCATÉTER Y LA BACTERIEMIA PRIMARIA
La bacteriemia por catéter sigue siendo un problema gravecuya morbilidad y mortalidad es mayor cuando bacterias deelevada patogenicidad como S. aureus son responsables delepisodio. La administración temprana de antimicrobianos en elpaciente con bacteriemia contribuye a un pronóstico mejor y labacteriemia por SARM no es una excepción como se hademostrado recientemente en un estudio con diseño de casos ycontroles16. Pero además, en el caso de bacteriemia por SARMse da la particularidad que la tasa de fallo de tratamiento ymortalidad son mayores en episodios tratados con vancomicinacuando la cepa causante de la infección siendo sensible a lamisma presenta una CMI >1 mg/L3,4,17. En estos estudios ladeterminación de la CMI a vancomicina se realizó mediante elmétodo del E-test. En caso de bacteriemia por catéter nodebemos olvidar la importancia de la retirada precoz del mismodado que la demora más allá de 24 horas en su retirada seasocia de forma significativa a una mayor mortalidad18.
Las características farmacocinéticas y de mecanismos deacción de daptomicina, sobre todo su rápido poder bactericida,sirvieron para apuntar desde el inicio de su desarrollo clínico aque el antibiótico tuviera un papel importante en eltratamiento de bacteriemias por cocos grampositivos. Hay querecordar que daptomicina tiene un volumen de distribuciónbajo (0,1 ml/Kg) lo que nos indica que permaneceespecialmente en plasma y tejidos muy vascularizados.
En 2006 se publicó el trabajo que sirvió para la aprobaciónde daptomicina en bacteriemias y endocarditis derecha19. Setrata de un estudio multicéntrico, abierto, planteado como deno inferioridad (margen de diferencia 20%), para estudiar laeficacia y seguridad de la daptomicina en el tratamiento debacteriemias con o sin endocarditis causadas por S. aureus. Se
Tabla 1 Daptomicina: Propiedadesfarmacocinéticas
• Farmacocinética lineal, vida media 8-9 horas• Unión a proteínas plasmáticas 90-93%• Volumen de distribución bajo (0,1 ml/kg)• Excreción
Renal 78%Heces 6%
• No interactúa con el Citocromo P450• Inactivada por surfactante pulmonar• Penetración en meninges inflamada: 6%
Tabla 2 Dosificación de daptomicina.Situaciones especiales
• Dosis aprobada — Infección de piel y partes blandas: 4 mg/kg/d— Bacteriemia incluyendo endocarditis: 6 mg/kg/d
• Paciente crítico (dosis recomendada). 8-10 mg/kg/d(vigilar estrechamente CPK)
• Gran quemado: 10-12 mg/kg/d (primeras 4 semanas)• Obesidad mórbida: Dosis ajustada a peso real• Insuficiencia renal con aclaramiento de creatinina >
30 ml/min: Sin cambios• Insuficiencia renal con aclaramiento de creatinina <
30 ml/min Dosis requerida administrada cada 48 h• Insuficiencia renal en hemodiálisis: 4-6 mg/kg/48h.
Administración tras la hemodiálisis• Insuficiencia renal en HFVVC 4-6 mg/kg/d• Insuficiencia hepática leve-moderada: 4-6 mg/kg/día• Insuficiencia hepática grave (Child Pugh C): No hay
datos
1568 • CID 2010:50 (15 June) • Bhavnani et al.
M A J O R A R T I C L E
Daptomycin Exposure and the Probabilityof Elevations in the Creatine Phosphokinase Level:Data from a Randomized Trial of Patientswith Bacteremia and Endocarditis
Sujata M. Bhavnani, Christopher M. Rubino, Paul G. Ambrose, and George L. DrusanoInstitute for Clinical Pharmacodynamics, Ordway Research Institute, Albany, New York
Background. The objective of this analysis was to evaluate the relationship between daptomycin exposure andthe probability of an elevation in the creatine phosphokinase (CPK) level (hereafter, “CPK elevation”) in patientswith Staphylococcus aureus bacteremia with or without infective endocarditis.
Methods. Phase 3 data for patients with S. aureus bacteremia, with or without infective endocarditis, whoreceived intravenous daptomycin (6 mg/kg daily) and in whom pharmacokinetic data were collected were evaluated.On the basis of univariate logistic regression, the relationship between Bayesian post hoc exposure estimates andthe probability of a CPK elevation was evaluated. Time to CPK elevation was examined with Kaplan-Meier analysisand Cox proportional hazards regression.
Results. Significant relationships between the minimum concentration of drug (Cmin) and area under the plasmaconcentration time curve and probability of CPK elevation were observed in 108 evaluable patients. Of the 108patients evaluated, 6 (5.56%) demonstrated a defined CPK elevation, regardless of treatment relationship. Cmin
(breakpoint of 24.3 mg/L) was most significantly associated with CPK elevation (P p .002). The probabilities ofa CPK elevation with a Cmin !24.3 mg/L and !24.3 mg/L were 0.5 and 0.029, respectively. Increases in Cmin,evaluated as a continuous variable, were also significantly associated with CPK elevation (P p .01). StratifiedKaplan-Meier analysis and Cox proportional hazards regression demonstrated Cmin to be a significant predictorof time to a CPK elevation (P " .003). The probability of a CPK elevation was 0 and 0.01 after 7 days of treatmentin patients with a Cmin !24.3 mg/L or !24.3 mg/L, respectively. After 14 days, the probabilities were 0.5 and 0.025,respectively.
Conclusions. This analysis demonstrated that a daptomycin Cmin !24.3 mg/L was associated with an increasedprobability of a CPK elevation.
Clinical trials registration. Clinical trials.gov NCT00093067.
Daptomycin is a cyclic lipopeptide antibacterial agentwith in vitro activity against gram-positive bacteria, in-cluding methicillin-resistant Staphylococcus aureus. Inthe early 1990s, clinical trials for this agent [1] used a12-h dosing interval. After observing a signal of anadverse skeletal muscle effect at a dose level of 4 mg/
Received 6 October 2009; accepted 1 March 2010; electronically published 12May 2010.
Reprints or correspondence: Dr George L. Drusano, Institute for ClinicalPharmacodynamics, Ordway Research Institute, 150 New Scotland Ave, Albany,NY 12208 ([email protected]).
Clinical Infectious Diseases 2010; 50(12):1568–1574! 2010 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2010/5012-0003$15.00DOI: 10.1086/652767
kg administered every 12 h [2, 3], these trials werevoluntarily suspended. Subsequent studies in dogs re-ceiving daptomycin (75 mg/kg daily for 20 days) servedto demonstrate decreased skeletal myopathy and cre-atine phosphokinase (CPK) elevation when the dosewas administered once daily compared with 25 mg/kgevery 8 h [4], thereby supporting the study of once-daily dosing regimens in clinical trials that followed.Clinical studies of daptomycin administered daily dem-onstrated a lower incidence of elevations in the creatinephosphokinase (CPK) level (hereafter, “CPK eleva-tions”) [5, 6], thus supporting the findings in dogs [4].
After US Food and Drug Administration approval ofthis agent for the treatment of complicated skin andskin-structure infections attributable to gram-positive
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from
1568 • CID 2010:50 (15 June) • Bhavnani et al.
M A J O R A R T I C L E
Daptomycin Exposure and the Probabilityof Elevations in the Creatine Phosphokinase Level:Data from a Randomized Trial of Patientswith Bacteremia and Endocarditis
Sujata M. Bhavnani, Christopher M. Rubino, Paul G. Ambrose, and George L. DrusanoInstitute for Clinical Pharmacodynamics, Ordway Research Institute, Albany, New York
Background. The objective of this analysis was to evaluate the relationship between daptomycin exposure andthe probability of an elevation in the creatine phosphokinase (CPK) level (hereafter, “CPK elevation”) in patientswith Staphylococcus aureus bacteremia with or without infective endocarditis.
Methods. Phase 3 data for patients with S. aureus bacteremia, with or without infective endocarditis, whoreceived intravenous daptomycin (6 mg/kg daily) and in whom pharmacokinetic data were collected were evaluated.On the basis of univariate logistic regression, the relationship between Bayesian post hoc exposure estimates andthe probability of a CPK elevation was evaluated. Time to CPK elevation was examined with Kaplan-Meier analysisand Cox proportional hazards regression.
Results. Significant relationships between the minimum concentration of drug (Cmin) and area under the plasmaconcentration time curve and probability of CPK elevation were observed in 108 evaluable patients. Of the 108patients evaluated, 6 (5.56%) demonstrated a defined CPK elevation, regardless of treatment relationship. Cmin
(breakpoint of 24.3 mg/L) was most significantly associated with CPK elevation (P p .002). The probabilities ofa CPK elevation with a Cmin !24.3 mg/L and !24.3 mg/L were 0.5 and 0.029, respectively. Increases in Cmin,evaluated as a continuous variable, were also significantly associated with CPK elevation (P p .01). StratifiedKaplan-Meier analysis and Cox proportional hazards regression demonstrated Cmin to be a significant predictorof time to a CPK elevation (P " .003). The probability of a CPK elevation was 0 and 0.01 after 7 days of treatmentin patients with a Cmin !24.3 mg/L or !24.3 mg/L, respectively. After 14 days, the probabilities were 0.5 and 0.025,respectively.
Conclusions. This analysis demonstrated that a daptomycin Cmin !24.3 mg/L was associated with an increasedprobability of a CPK elevation.
Clinical trials registration. Clinical trials.gov NCT00093067.
Daptomycin is a cyclic lipopeptide antibacterial agentwith in vitro activity against gram-positive bacteria, in-cluding methicillin-resistant Staphylococcus aureus. Inthe early 1990s, clinical trials for this agent [1] used a12-h dosing interval. After observing a signal of anadverse skeletal muscle effect at a dose level of 4 mg/
Received 6 October 2009; accepted 1 March 2010; electronically published 12May 2010.
Reprints or correspondence: Dr George L. Drusano, Institute for ClinicalPharmacodynamics, Ordway Research Institute, 150 New Scotland Ave, Albany,NY 12208 ([email protected]).
Clinical Infectious Diseases 2010; 50(12):1568–1574! 2010 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2010/5012-0003$15.00DOI: 10.1086/652767
kg administered every 12 h [2, 3], these trials werevoluntarily suspended. Subsequent studies in dogs re-ceiving daptomycin (75 mg/kg daily for 20 days) servedto demonstrate decreased skeletal myopathy and cre-atine phosphokinase (CPK) elevation when the dosewas administered once daily compared with 25 mg/kgevery 8 h [4], thereby supporting the study of once-daily dosing regimens in clinical trials that followed.Clinical studies of daptomycin administered daily dem-onstrated a lower incidence of elevations in the creatinephosphokinase (CPK) level (hereafter, “CPK eleva-tions”) [5, 6], thus supporting the findings in dogs [4].
After US Food and Drug Administration approval ofthis agent for the treatment of complicated skin andskin-structure infections attributable to gram-positive
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from by guest on October 12, 2013
http://cid.oxfordjournals.org/Downloaded from
by guest on October 12, 2013http://cid.oxfordjournals.org/
Downloaded from
PK/PD de daptomicina en el paciente crí3co Introd
ucción
PK/PD de daptomicina en el paciente crí3co ObjeF
vo
Material y métodos
PK/PD de daptomicina en el paciente crí3co

① Población objeto de estudio
– Ingresados en el Servicios de Medicina Intensiva (SMI) del
Hospital Universitario de Álava
– Reciban daptomicina por sospecha infección por cocos gram
positivo multirresistentes
– Cumplan los criterios de inclusión, no presenten criterios de
exclusión y acepten formar parte del estudio
– Consentimiento informado
Material y m
étod
os
PK/PD de daptomicina en el paciente crí3co

③ Administración de daptomicina – Dosis habitual: 4-6 mg/Kg/día según indicación clínica
④ Toma de muestras – A tiempos previamente programados se tomaron muestras de sangre de
los pacientes, congelando inmediatamente el plasma obtenido a –20 °C.
⑤ Cuantificación – Los niveles plasmáticos totales de daptomicina se determinaron
mediante HPLC con detector UV.
Material y m
étod
os
PK/PD de daptomicina en el paciente crí3co

⑥ Análisis microbiológico – Identificar los microorganismos responsables de la infección
– Estudio de la sensibilidad a daptomicina (CMI)
⑦ Análisis farmacocinético – Parámetros farmacocinéticos en cada paciente
• Programa: WinNonlin
⑧ Análisis PK/PD – Índices que se relacionan con la eficacia del tratamiento:
• Relación AUC0-24/CMI>666
⑨ Simulación de Monte Carlo – Programe Oracle Crystal Ball
Material y m
étod
os
PK/PD de daptomicina en el paciente crí3co
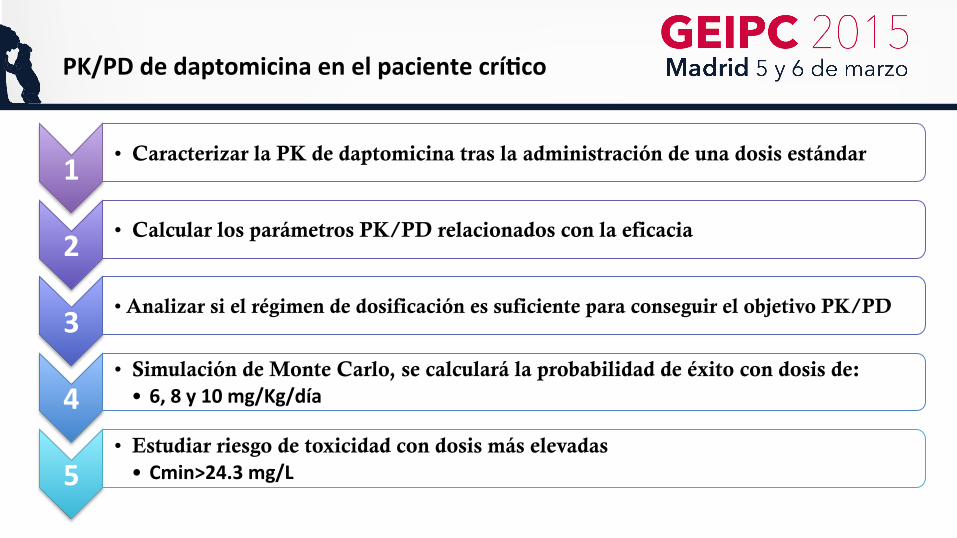
1 • Caracterizar la PK de daptomicina tras la administración de una dosis estándar
2 • Calcular los parámetros PK/PD relacionados con la eficacia
3 • Analizar si el régimen de dosificación es suficiente para conseguir el objetivo PK/PD
4 • Simulación de Monte Carlo, se calculará la probabilidad de éxito con dosis de: • 6, 8 y 10 mg/Kg/día
5 • Estudiar riesgo de toxicidad con dosis más elevadas • Cmin>24.3 mg/L
PK/PD de daptomicina en el paciente crí3co
Resultados y conclusiones
PK/PD de daptomicina en el paciente crí3co
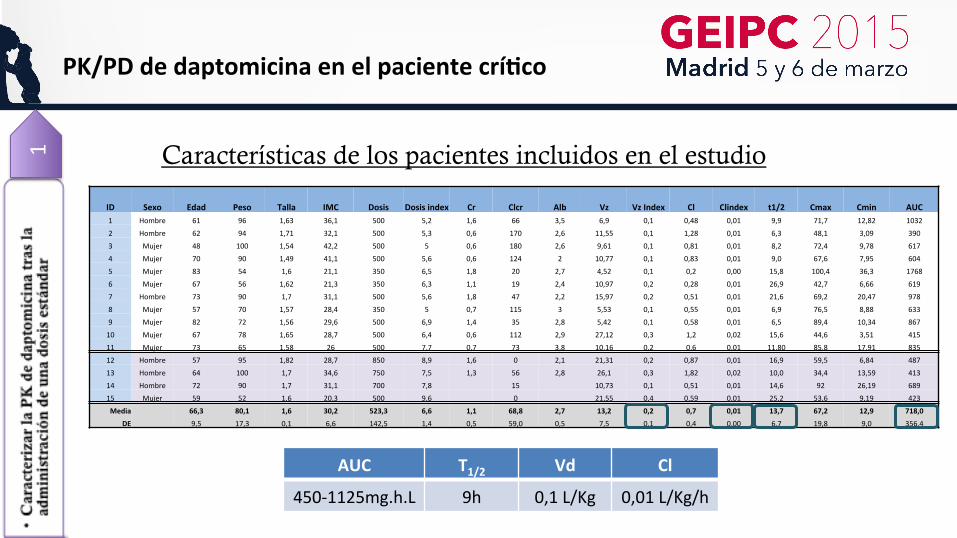
PK/PD de daptomicina en el paciente crí3co 1 Características de los pacientes incluidos en el estudio
AUC T1/2 Vd Cl
450-‐1125mg.h.L 9h 0,1 L/Kg 0,01 L/Kg/h
ID Sexo Edad Peso Talla IMC Dosis Dosis index Cr Clcr Alb Vz Vz Index Cl Clindex t1/2 Cmax Cmin AUC 1 Hombre 61 96 1,63 36,1 500 5,2 1,6 66 3,5 6,9 0,1 0,48 0,01 9,9 71,7 12,82 1032
2 Hombre 62 94 1,71 32,1 500 5,3 0,6 170 2,6 11,55 0,1 1,28 0,01 6,3 48,1 3,09 390
3 Mujer 48 100 1,54 42,2 500 5 0,6 180 2,6 9,61 0,1 0,81 0,01 8,2 72,4 9,78 617
4 Mujer 70 90 1,49 41,1 500 5,6 0,6 124 2 10,77 0,1 0,83 0,01 9,0 67,6 7,95 604
5 Mujer 83 54 1,6 21,1 350 6,5 1,8 20 2,7 4,52 0,1 0,2 0,00 15,8 100,4 36,3 1768
6 Mujer 67 56 1,62 21,3 350 6,3 1,1 19 2,4 10,97 0,2 0,28 0,01 26,9 42,7 6,66 619
7 Hombre 73 90 1,7 31,1 500 5,6 1,8 47 2,2 15,97 0,2 0,51 0,01 21,6 69,2 20,47 978
8 Mujer 57 70 1,57 28,4 350 5 0,7 115 3 5,53 0,1 0,55 0,01 6,9 76,5 8,88 633
9 Mujer 82 72 1,56 29,6 500 6,9 1,4 35 2,8 5,42 0,1 0,58 0,01 6,5 89,4 10,34 867
10 Mujer 67 78 1,65 28,7 500 6,4 0,6 112 2,9 27,12 0,3 1,2 0,02 15,6 44,6 3,51 415
11 Mujer 73 65 1,58 26 500 7,7 0,7 73 3,8 10,16 0,2 0,6 0,01 11,80 85,8 17,91 835
12 Hombre 57 95 1,82 28,7 850 8,9 1,6 0 2,1 21,31 0,2 0,87 0,01 16,9 59,5 6,84 487
13 Hombre 64 100 1,7 34,6 750 7,5 1,3 56 2,8 26,1 0,3 1,82 0,02 10,0 34,4 13,59 413
14 Hombre 72 90 1,7 31,1 700 7,8 15 10,73 0,1 0,51 0,01 14,6 92 26,19 689
15 Mujer 59 52 1,6 20,3 500 9,6 0 21,55 0,4 0,59 0,01 25,2 53,6 9,19 423
Media 66,3 80,1 1,6 30,2 523,3 6,6 1,1 68,8 2,7 13,2 0,2 0,7 0,01 13,7 67,2 12,9 718,0
DE 9,5 17,3 0,1 6,6 142,5 1,4 0,5 59,0 0,5 7,5 0,1 0,4 0,00 6,7 19,8 9,0 356,4
PK/PD de daptomicina en el paciente crí3co 3
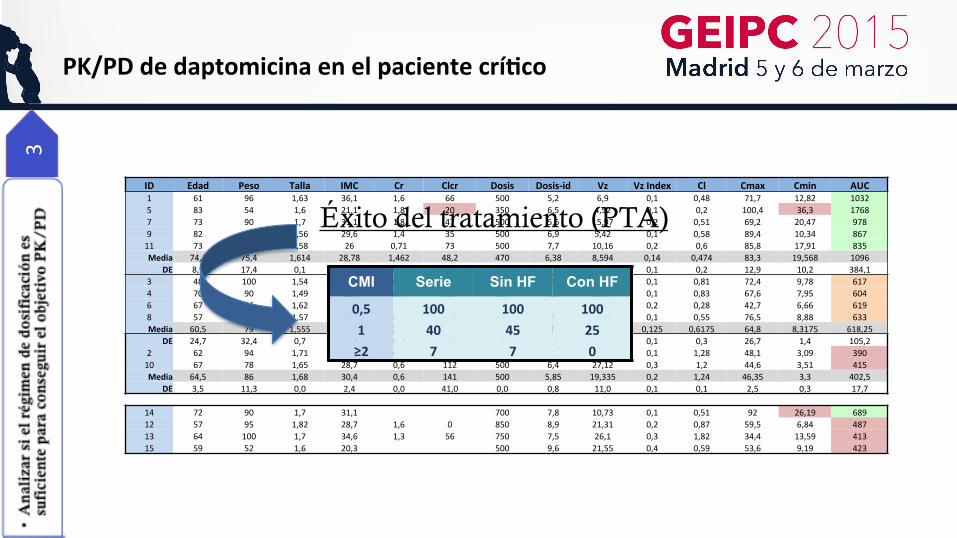
ID Edad Peso Talla IMC Cr Clcr Dosis Dosis-‐id Vz Vz Index Cl Cmax Cmin AUC 1 61 96 1,63 36,1 1,6 66 500 5,2 6,9 0,1 0,48 71,7 12,82 1032 5 83 54 1,6 21,1 1,8 20 350 6,5 4,52 0,1 0,2 100,4 36,3 1768 7 73 90 1,7 31,1 1,8 47 500 5,6 15,97 0,2 0,51 69,2 20,47 978 9 82 72 1,56 29,6 1,4 35 500 6,9 5,42 0,1 0,58 89,4 10,34 867 11 73 65 1,58 26 0,71 73 500 7,7 10,16 0,2 0,6 85,8 17,91 835 Media 74,4 75,4 1,614 28,78 1,462 48,2 470 6,38 8,594 0,14 0,474 83,3 19,568 1096
DE 8,9 17,4 0,1 5,6 0,5 21,8 67,1 1,0 4,6 0,1 0,2 12,9 10,2 384,1 3 48 100 1,54 42,2 0,6 180 500 5 9,61 0,1 0,81 72,4 9,78 617 4 70 90 1,49 41,1 0,6 124 500 5,6 10,77 0,1 0,83 67,6 7,95 604 6 67 56 1,62 21,3 1,1 44 350 6,3 10,97 0,2 0,28 42,7 6,66 619 8 57 70 1,57 28,4 0,7 115 350 5 5,53 0,1 0,55 76,5 8,88 633 Media 60,5 79 1,555 33,25 0,75 115,75 425 5,475 9,22 0,125 0,6175 64,8 8,3175 618,25
DE 24,7 32,4 0,7 15,2 0,2 64,0 176,8 2,1 3,0 0,1 0,3 26,7 1,4 105,2 2 62 94 1,71 32,1 0,6 170 500 5,3 11,55 0,1 1,28 48,1 3,09 390 10 67 78 1,65 28,7 0,6 112 500 6,4 27,12 0,3 1,2 44,6 3,51 415 Media 64,5 86 1,68 30,4 0,6 141 500 5,85 19,335 0,2 1,24 46,35 3,3 402,5
DE 3,5 11,3 0,0 2,4 0,0 41,0 0,0 0,8 11,0 0,1 0,1 2,5 0,3 17,7
14 72 90 1,7 31,1 700 7,8 10,73 0,1 0,51 92 26,19 689 12 57 95 1,82 28,7 1,6 0 850 8,9 21,31 0,2 0,87 59,5 6,84 487 13 64 100 1,7 34,6 1,3 56 750 7,5 26,1 0,3 1,82 34,4 13,59 413 15 59 52 1,6 20,3 500 9,6 21,55 0,4 0,59 53,6 9,19 423
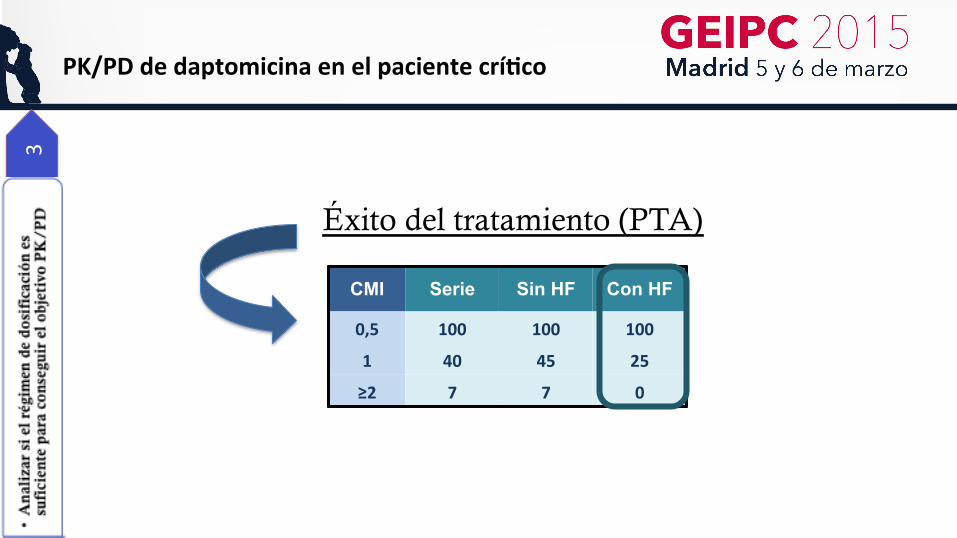
CMI Serie Sin HF Con HF
0,5 100 100 100 1 40 45 25 ≥2 7 7 0
Éxito del tratamiento (PTA)

PK/PD de daptomicina en el paciente crí3co 3 Aislamientos de Cocos Gram + en SMI HU Araba
Éxito del tratamiento (CFR)
Tasa de éxito (%) S. aureus 38 SCN 38 Enterococos 18
<5 % CMI ≥ 2
CMI50 CMI90 Puntos corte Distribución CMIs Sensibilidad 1 2 4 8 16
S. aureus 1 1 <=1 93 7 0 0 4,2
SCN 1 1 <=1 95 5
Enterococos 2 8 <=4 39 33 15 9 3
PK/PD de daptomicina en el paciente crí3co 3
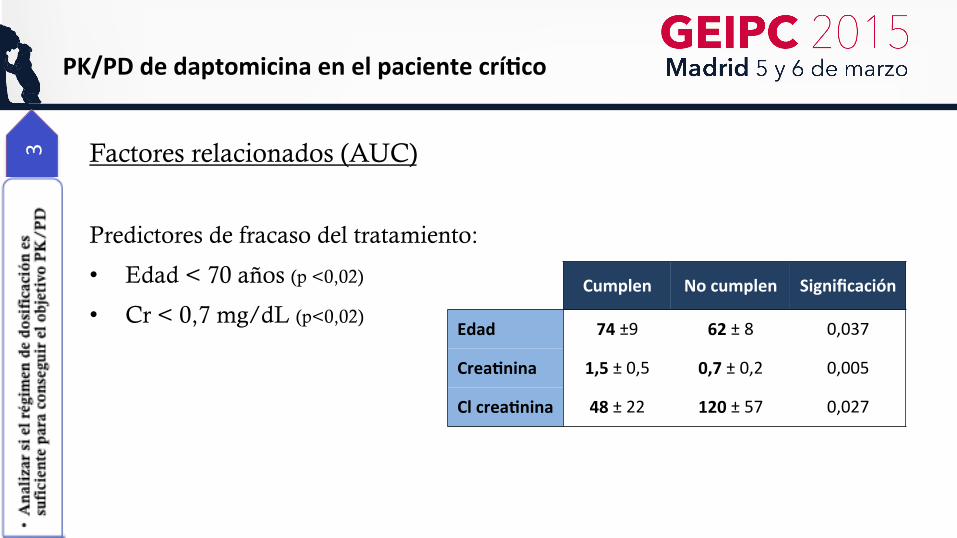
PK/PD de daptomicina en el paciente crí3co 3 Factores relacionados (AUC)
Predictores de fracaso del tratamiento:
• Edad < 70 años (p <0,02)
• Cr < 0,7 mg/dL (p<0,02)
Cumplen No cumplen Significación
Edad 74 ±9 62 ± 8 0,037
Crea3nina 1,5 ± 0,5 0,7 ± 0,2 0,005
Cl crea3nina 48 ± 22 120 ± 57 0,027
3
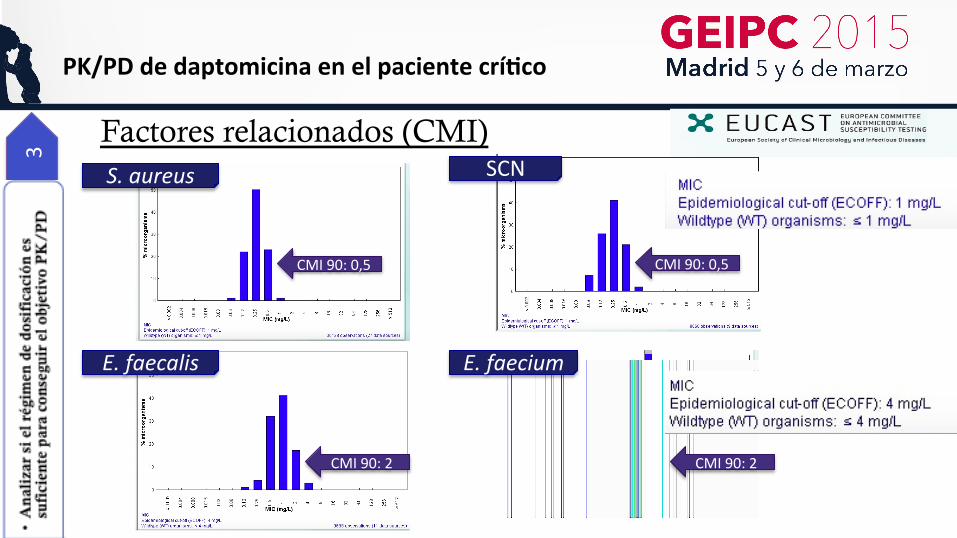
Factores relacionados (CMI)
S. aureus SCN
CMI 90: 0,5 CMI 90: 0,5
PK/PD de daptomicina en el paciente crí3co
E. faecalis E. faecium
CMI 90: 2 CMI 90: 2

PK/PD de daptomicina en el paciente crí3co 3 Factores relacionados (CMI)
CMI50 CMI90 Puntos corte Distribución CMIs Sensibilidad 1 2 4 8 16
S. aureus 1 1 <=1 93 7 0 0 4,2
SCN 1 1 <=1 95 5
Enterococos 2 8 <=4 39 33 15 9 3
PK/PD de daptomicina en el paciente crí3co 4
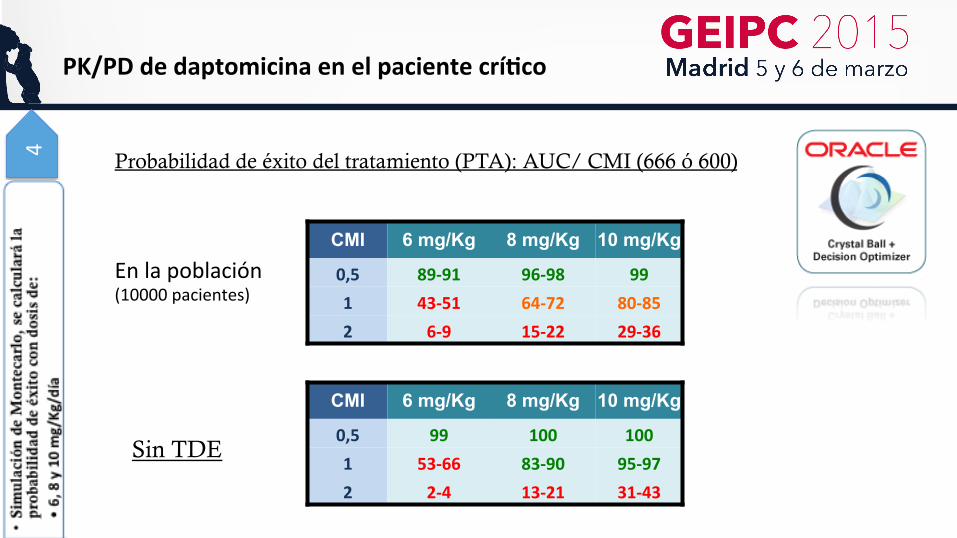
Probabilidad de éxito del tratamiento (PTA): AUC/ CMI (666 ó 600)
En la población (10000 pacientes)
CMI 6 mg/Kg 8 mg/Kg 10 mg/Kg
0,5 89-‐91 96-‐98 99 1 43-‐51 64-‐72 80-‐85 2 6-‐9 15-‐22 29-‐36
CMI 6 mg/Kg 8 mg/Kg 10 mg/Kg
0,5 99 100 100 1 53-‐66 83-‐90 95-‐97 2 2-‐4 13-‐21 31-‐43
Sin TDE
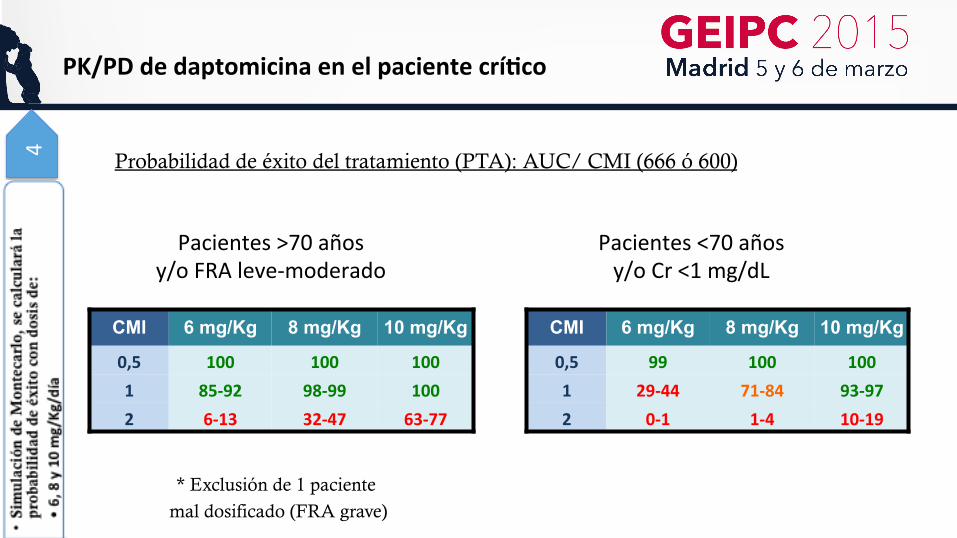
PK/PD de daptomicina en el paciente crí3co 4
Pacientes >70 años y/o FRA leve-‐moderado
Pacientes <70 años y/o Cr <1 mg/dL
CMI 6 mg/Kg 8 mg/Kg 10 mg/Kg
0,5 99 100 100 1 29-‐44 71-‐84 93-‐97 2 0-‐1 1-‐4 10-‐19
CMI 6 mg/Kg 8 mg/Kg 10 mg/Kg
0,5 100 100 100 1 85-‐92 98-‐99 100 2 6-‐13 32-‐47 63-‐77
* Exclusión de 1 paciente
mal dosificado (FRA grave)
Probabilidad de éxito del tratamiento (PTA): AUC/ CMI (666 ó 600)
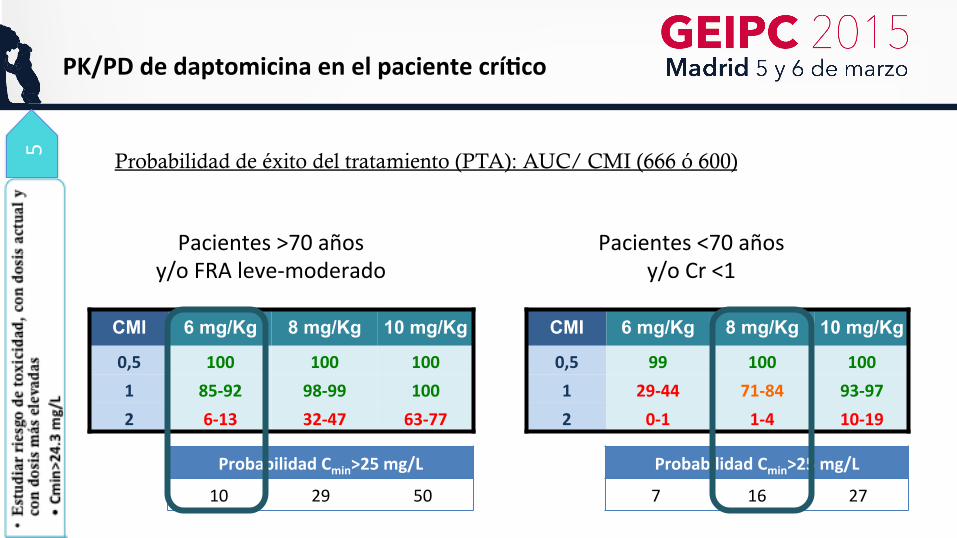
PK/PD de daptomicina en el paciente crí3co
Pacientes >70 años y/o FRA leve-‐moderado
Pacientes <70 años y/o Cr <1
5
Probabilidad Cmin>25 mg/L
10 29 50
Probabilidad Cmin>25 mg/L
7 16 27
CMI 6 mg/Kg 8 mg/Kg 10 mg/Kg
0,5 100 100 100 1 85-‐92 98-‐99 100 2 6-‐13 32-‐47 63-‐77
CMI 6 mg/Kg 8 mg/Kg 10 mg/Kg
0,5 99 100 100 1 29-‐44 71-‐84 93-‐97 2 0-‐1 1-‐4 10-‐19
Probabilidad de éxito del tratamiento (PTA): AUC/ CMI (666 ó 600)
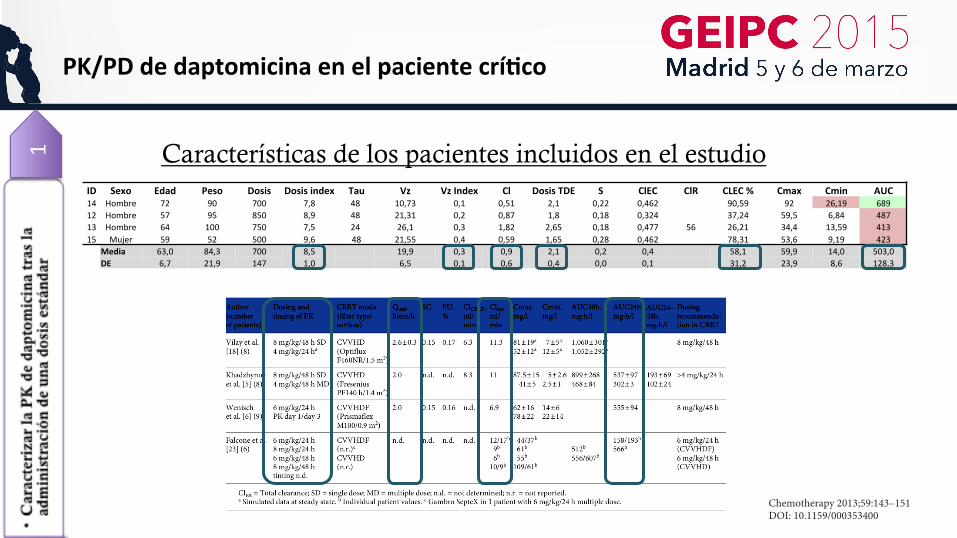
PK/PD de daptomicina en el paciente crí3co 1 Características de los pacientes incluidos en el estudio
ID Sexo Edad Peso Dosis Dosis index Tau Vz Vz Index Cl Dosis TDE S ClEC ClR CLEC % Cmax Cmin AUC 14 Hombre 72 90 700 7,8 48 10,73 0,1 0,51 2,1 0,22 0,462 90,59 92 26,19 689 12 Hombre 57 95 850 8,9 48 21,31 0,2 0,87 1,8 0,18 0,324 37,24 59,5 6,84 487 13 Hombre 64 100 750 7,5 24 26,1 0,3 1,82 2,65 0,18 0,477 56 26,21 34,4 13,59 413 15 Mujer 59 52 500 9,6 48 21,55 0,4 0,59 1,65 0,28 0,462 78,31 53,6 9,19 423
Media 63,0 84,3 700 8,5 19,9 0,3 0,9 2,1 0,2 0,4 58,1 59,9 14,0 503,0 DE 6,7 21,9 147 1,0 6,5 0,1 0,6 0,4 0,0 0,1 31,2 23,9 8,6 128,3
Once Daily Daptomycin PK in CRRT Chemotherapy 2013;59:143–151DOI: 10.1159/000353400
147
Results
Subject Demographics Baseline characteristics and individual clearance re-
sults of the 9 patients are shown in table 1 . Eight patients completed the study, and 1 patient died on the second study day for reasons unrelated to the study. Therefore, PK data of the third and fifth days are missing for this pa-tient. The total daily daptomycin dose ranged from 250 to 700 mg (mean 497 ± 145 mg). All patients were anuric (<50 ml of urine per day) during the study period; there-fore, no renal clearance was determined. In 8 patients, CVVHDF was used with predilution in 4 patients, and in 1 patient, CVVHD was performed.
PK Results PK parameters are presented in table 2 . Individual
plasma concentration-time curves are shown in figure 1 . No accumulation between day 1 and day 3 (AUC24h) and no further accumulation from the third to the fifth treat-ment day (Cmax and Cmin) occurred. The 90% confi-dence intervals of Cmax and AUC geometric mean ratios were not outside the bioequivalence zone of 0.8–1.25. Cl CRRT varied by up to 2.7-fold between patients, ranging from 2.5 to 6.7 ml/min (mean 4.5 ml/min). Mean CRRT clearance accounted for 48% (range 32–67%) of total dap-tomycin body clearance (mean 10.2 ml/min, range 6.1–18 ml/min).
Table 2. PK parameters
Day 1 Day 3 Day 5
mean ± SD GM mean ± SD GM GM ratio day 3/day 1
90% CI of GM ratio
me an ± SD GM GM ratio day 5/day 3
90% CI of GM ratio
Cmax, mg/l 65.8 ± 17.1 63.5 (30.5) 77.2 ± 31.3 72.1 (40.8) 1.13 0.83 – 1.54 66.9 ± 25.3 62.2 (44.1) 0.86 0.62 – 1.18 Cmin, mg/l 7.7 ± 4.1 6.8 (64.1) 13.1 ±8.3 10.7 (81.1) 1.58 0.86 – 2.9 15.6 ± 11.1 11.9 (106.2) 1.1 0.59 – 2.06 AUC a , mg∙h/l 611 ± 286 548 (55) 667.4 ± 367.6 588.2 (57.6) 1.07 0.70 – 1.65 FU, % 22 ± 8 fAUC24h, mg∙h/l 131.3 ± 43 fCmax, mg/l 15.7 ± 4.9 T 1/2 , h 10.6 ± 2.4 10.3 (23.1) 12.5 ± 2.3 12.3 (20.8) Total clearance, ml/min
10.5± 4 13.2 (32.3)
Values in parentheses represent coefficients of variation. CI = Confidence interval; FU = fraction unbound; GM = geometric mean; fAUC = AUC of free daptomycin; fCmax = free Cmax; T 1/2 = half-life . a Day 1: AUCinfinity; day 3: AUC24h.
Dap
tom
ycin
AU
C24h
(mg·
h/l)
1,200
1,000
1,600
1,400
800
600
400
200
0120 14020 40 60 80 100
Cmax (mg/l)
R2 = 0.91
a
Dap
tom
ycin
AU
C24h
(mg·
h/l)
1,200
1,000
1,600
1,400
800
600
400
200
0
Cmin (mg/l)
R2 = 0.94
0 5 10 15 20 25 3530b
Fig. 2. Individual total daptomycin AUC24h correlated to individual Cmax ( a ) and Cmin ( b ).
Down
load
ed b
y:
Unive
rsid
ad d
el P
ais
Vasc
o Bi
blio
teca
Cen
tral
15
8.22
7.22
8.15
4 - 1
0/1/
2013
9:5
2:56
AM
PK/PD de daptomicina en el paciente crí3co 3
CMI Serie Sin HF Con HF
0,5 100 100 100
1 40 45 25
≥2 7 7 0
Éxito del tratamiento (PTA)
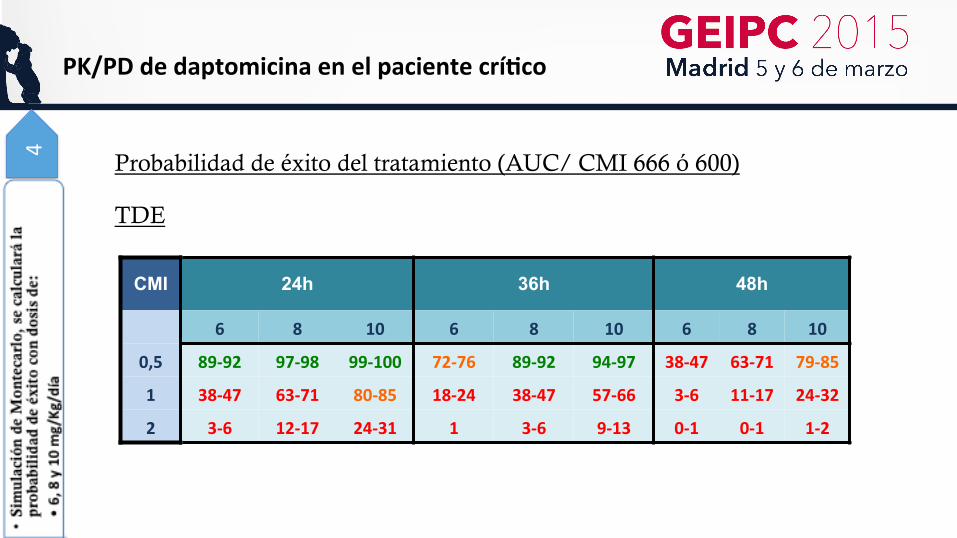
PK/PD de daptomicina en el paciente crí3co 4
Probabilidad de éxito del tratamiento (AUC/ CMI 666 ó 600)
CMI 24h 36h 48h
6 8 10 6 8 10 6 8 10
0,5 89-‐92 97-‐98 99-‐100 72-‐76 89-‐92 94-‐97 38-‐47 63-‐71 79-‐85
1 38-‐47 63-‐71 80-‐85 18-‐24 38-‐47 57-‐66 3-‐6 11-‐17 24-‐32
2 3-‐6 12-‐17 24-‐31 1 3-‐6 9-‐13 0-‐1 0-‐1 1-‐2
TDE
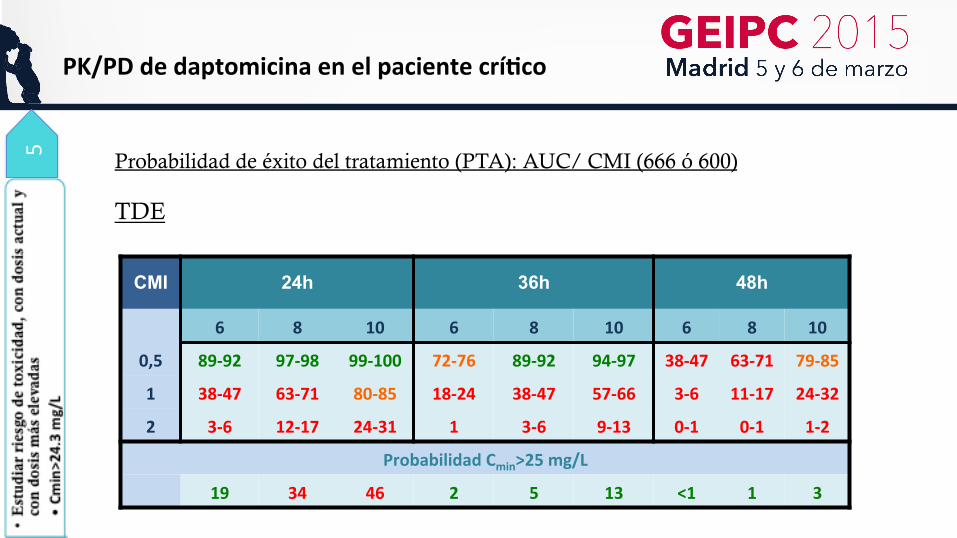
PK/PD de daptomicina en el paciente crí3co 5
CMI 24h 36h 48h
6 8 10 6 8 10 6 8 10
0,5 89-‐92 97-‐98 99-‐100 72-‐76 89-‐92 94-‐97 38-‐47 63-‐71 79-‐85
1 38-‐47 63-‐71 80-‐85 18-‐24 38-‐47 57-‐66 3-‐6 11-‐17 24-‐32
2 3-‐6 12-‐17 24-‐31 1 3-‐6 9-‐13 0-‐1 0-‐1 1-‐2
Probabilidad Cmin>25 mg/L
19 34 46 2 5 13 <1 1 3
TDE
Probabilidad de éxito del tratamiento (PTA): AUC/ CMI (666 ó 600)
Conclusio
nes
PK/PD de daptomicina en el paciente crí3co
① En nuestra serie la dosis pautada fue insuficiente para conseguir el objetivo PK/PD
en el 60% de los pacientes ü Más acusado en pacientes con hemofiltración
② Los factores relacionados con el éxito/fracaso del tratamiento:
ü CMI mayores en pacientes críticos
ü Función renal
ü Edad
③ La administración de dosis mayores incrementaría las posibilidades de cumplir el
objetivo PK/PD
④ Dosis mayores no se asocian a niveles séricos valle (Cmin) relacionados con mayor
riesgo de toxicidad ü Dosis más elevadas en pacientes jóvenes y/o bajos niveles de creatinina sérica
Conclusio
nes
PK/PD de daptomicina en el paciente crí3co
En TDE:
① No está claro el régimen de dosificación que optimice eficacia clínica con mínima
toxicidad.
② Aunque la eliminación de daptomicina por TDE es relativamente baja ésta se vuelve
significativa en situación de anuria (79% eliminación por filtración glomerular)
– Dosis mayores que en FRA??
③ En presencia de función renal residual, el aclaramiento total puede acercarse al de
pacientes sin FRA
ü Administración cada 24?
Limita
cion
es
PK/PD de daptomicina en el paciente crí3co
① Número reducido de pacientes
② Aclaramiento calculado por fórmula y no medido
③ Heterogeneidad en pacientes con hemofiltración
④ No poder analizar el impacto clínico por ser terapias empíricas en
la mayoría de los casos
⑤ Éxito infraestimado por no tener diluciones por debajo de 1mg/L.
Nos preguntam
os…
PK/PD de daptomicina en el paciente crí3co
① ¿Sería recomendable usar dosis más elevadas en pacientes críticos jóvenes y/o con niveles bajos de creatinina sérica?
– Calcular de forma sistemática Clcr para ajuste de antibióticos con filtración glomerular significativa
② ¿Deberíamos interpretar el antibiograma con más cautela? – Antibioterapia adecuada (sensible) vs antibioterapia óptima (régimen
dosificación)
③ ¿Cuál es el papel de la daptomicina para el tratamiento de infecciones en los que se sospeche microorganismos con CMI ≥ 2?.

¡Gracias por vuestra atención!