clube da hipÓfise ano vii · (hipopituitarismo) 2 – radioterapia (50–60%) convencional...
TRANSCRIPT

Futuro do Tratamento Clínico na
Doença de Cushing
Luíz Antônio de Araújjo
CLUBE DA HIPÓFISE – Ano VII 27/02/2013

Tratamento da D. Cushing
Transsphenoidal surgery is first-line
therapy in Cushing’s disease
Initial success rate 68–98% in patients with a microadenoma1,2
Remission rates lower (<65%) in patients with a
macroadenoma1
Relapse rate is 2–26% (after 6–240 months)2
1Biller BMK et al. J Clin Endocrinol Metab 2008;93:2454–2462; 2Tritos NA et al. Nat Rev Endocrinol 2011;104:279–289
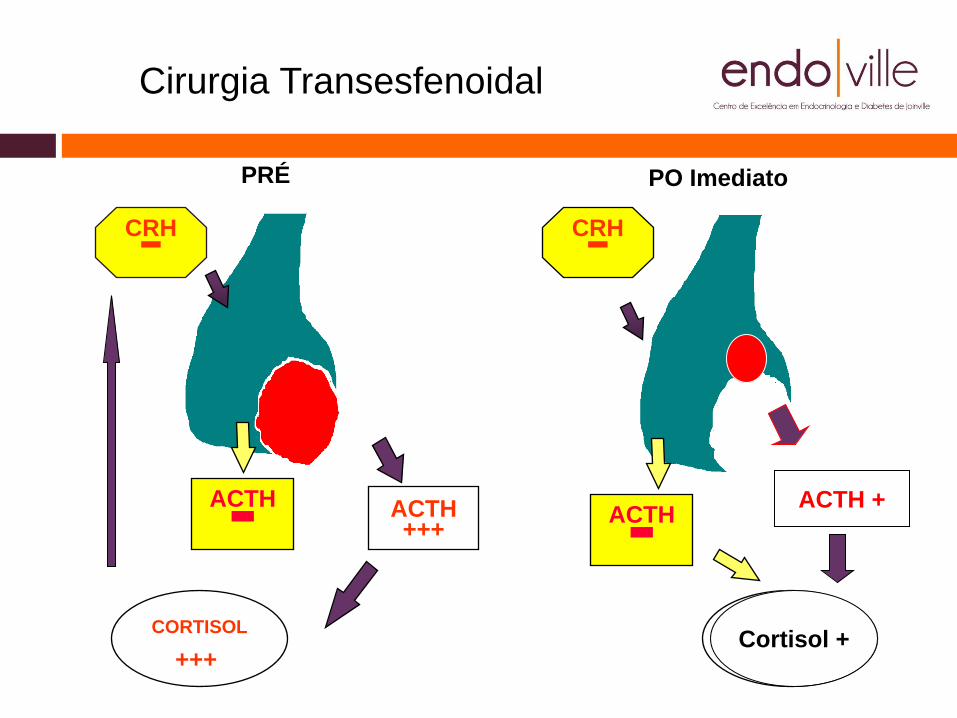
Cirurgia Transesfenoidal
PRÉ
ACTH +++
CORTISOL
+++
ACTH -
CRH - CRH -
ACTH -
CORTISOL
-
PO Imediato
ACTH +
Cortisol +
Conduta Persistência do
hipercortisolismo
Rescidiva
Recusa da
cirurgia
Contra
Indicação
cirúrgica
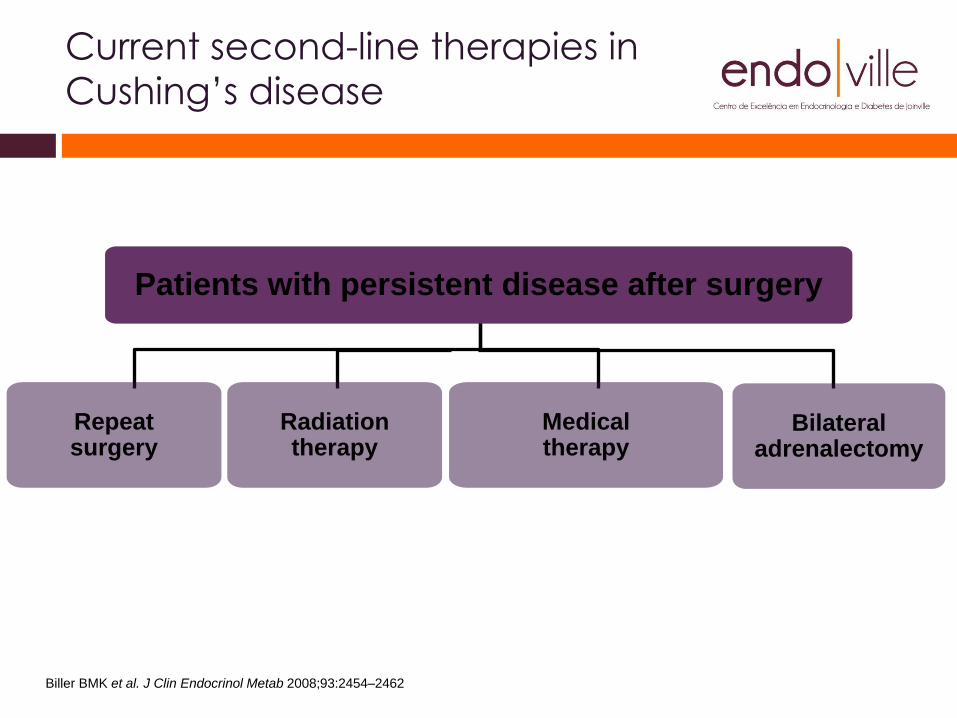
Biller BMK et al. J Clin Endocrinol Metab 2008;93:2454–2462
Current second-line therapies in
Cushing’s disease
Repeat surgery
Patients with persistent disease after surgery
Bilateral adrenalectomy
Radiation therapy
Medical therapy
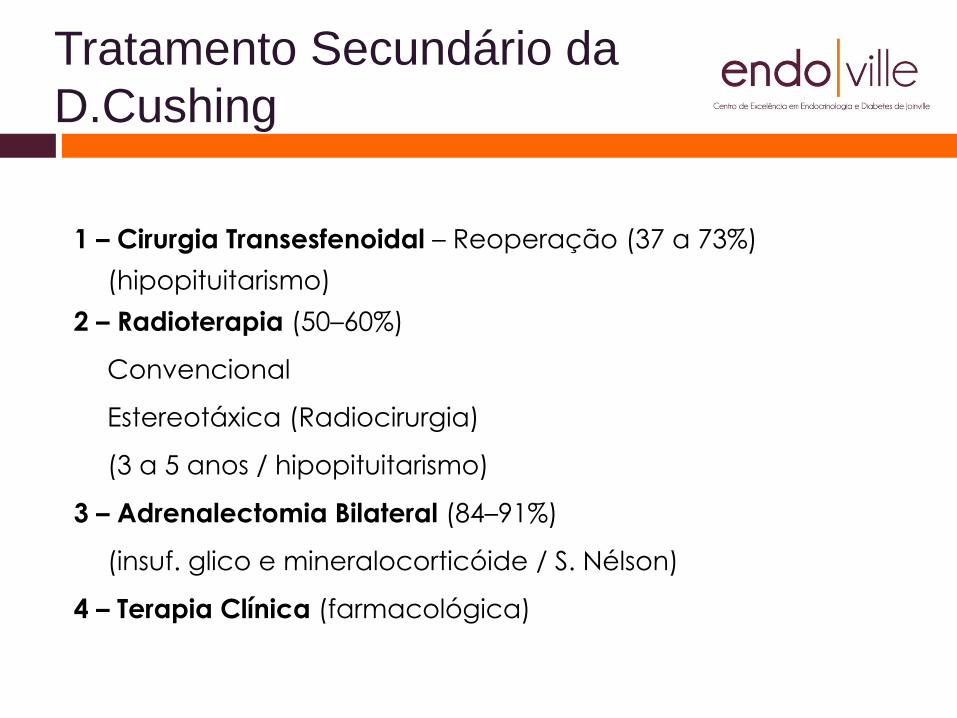
Tratamento Secundário da
D.Cushing
1 – Cirurgia Transesfenoidal – Reoperação (37 a 73%)
(hipopituitarismo)
2 – Radioterapia (50–60%)
Convencional
Estereotáxica (Radiocirurgia)
(3 a 5 anos / hipopituitarismo)
3 – Adrenalectomia Bilateral (84–91%)
(insuf. glico e mineralocorticóide / S. Nélson)
4 – Terapia Clínica (farmacológica)
Recentes Avanços na
Terapia Clínica
1 – Medicamentos de ação Central (ação sobre o tumor)
Cabergolina
Pasireotide
Outros: PPAR gama agonistas, ácido valpróico,
ciproheptadina, antagonistas da vasopressina.
2 – Medicamentos de ação periférica (bloqueio / Adrenal)
Cetoconazol
Metyrapone
Mitotane
Outros: fluconazol, aminoglutetimida, etomidate
LC1699
3 – Medicamentos Antagonistas do Receptor Glicocorticóide
. Mifepristone
Medicamentos de ação
Periférica
1 – Cetoconazol (400 a 1200mg / dia)
Retrospective study of 38 patients with active disease (17 had
previous surgery)
17 (45%) had normalized UFC; mean follow-up of 23 months
Treatment stopped in first week in five patients (13%) due to
clinical intolerance (GI symptoms) or biological intolerance
(elevated liver enzymes)
AEs included a moderate (<3xULN ) increase in γ-GT (8%),
nausea and diarrhea (5%), aspartate aminotransferase/alanine
aminotransferase 8xULN (3%)
Escape: 15%
1Castinetti F et al. Eur J Endocrinol 2008;158:91–
99;

Medicamentos de ação Central
1 – Cabergolina
Dose: 2 a 3,5 mg / semana
Resultados: Controlados = 35%
Parcialmente Controlados = 40%
Sem Resposta = 25%
Segurança = valvulopatia Mitral / Tricúspede
2 – Análogos de Somatostatina – Pasireotide (SOM 230)
Dose = 900 mcg BID SC; 30 mg 30/30 dias IM (LAR)
Segurança: hiperglicemia / DM, diarréia, náuseas, bradicardia,
insuf. Adrenal
Regulação: EMA (04/12); FDA (12/12)

Response at month 12 similar
to that at month 6
*Note: Responder was a patient with UFC ≤ULN who did not require uptitration
Fully controlled: UFC ≤ULN; partially controlled:
UFC >ULN, but had ≥50% reduction from baseline;
Uncontrolled: UFC >ULN and <50% reduction from baseline
Predetermined criterion for the primary efficacy endpoint was that the lower bound of the 95% CI
had to be greater than 15% for at least one of the dose groups: this was met for the 900 µg group
600 µg bid
(n=82)
900 µg bid
(n=80)
Overall
(n=162)
12 months
Fully controlled, n (%) 11 (13.4) 20 (25.0) 31 (19.1)
Partially controlled, n (%) 13 (15.9) 2 (2.5) 15 (9.3)
Uncontrolled, n (%) 58 (70.7) 58 (72.5) 116 (71.6)
Colao A et al. N Engl J Med 2012;366:914–924
Fully controlled: UFC ≤ULN; partially controlled: UFC >ULN but had ≥50% reduction from baseline; uncontrolled: UFC >ULN and <50%
reduction from baseline
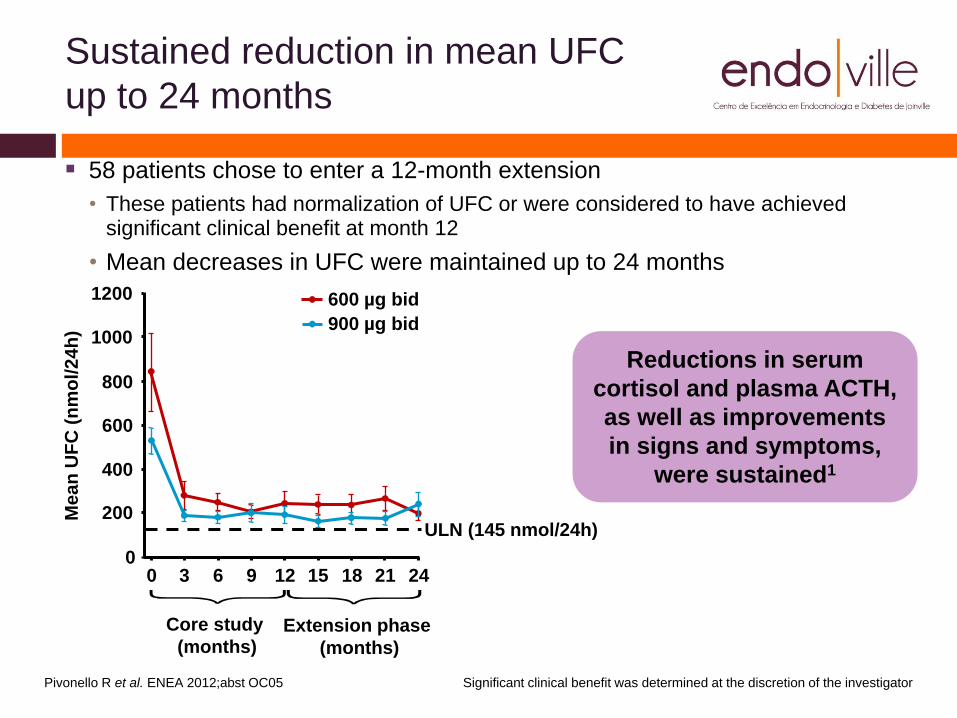
Sustained reduction in mean UFC
up to 24 months
Pivonello R et al. ENEA 2012;abst OC05
600
400
200
0
1200
1000
800
Mea
n U
FC
(n
mo
l/24
h)
0 3 6 9 12 18 15 21 24
600 µg bid
900 µg bid
ULN (145 nmol/24h)
Core study
(months) Extension phase
(months)
Reductions in serum
cortisol and plasma ACTH,
as well as improvements
in signs and symptoms,
were sustained1
Significant clinical benefit was determined at the discretion of the investigator
58 patients chose to enter a 12-month extension
• These patients had normalization of UFC or were considered to have achieved significant clinical benefit at month 12
• Mean decreases in UFC were maintained up to 24 months
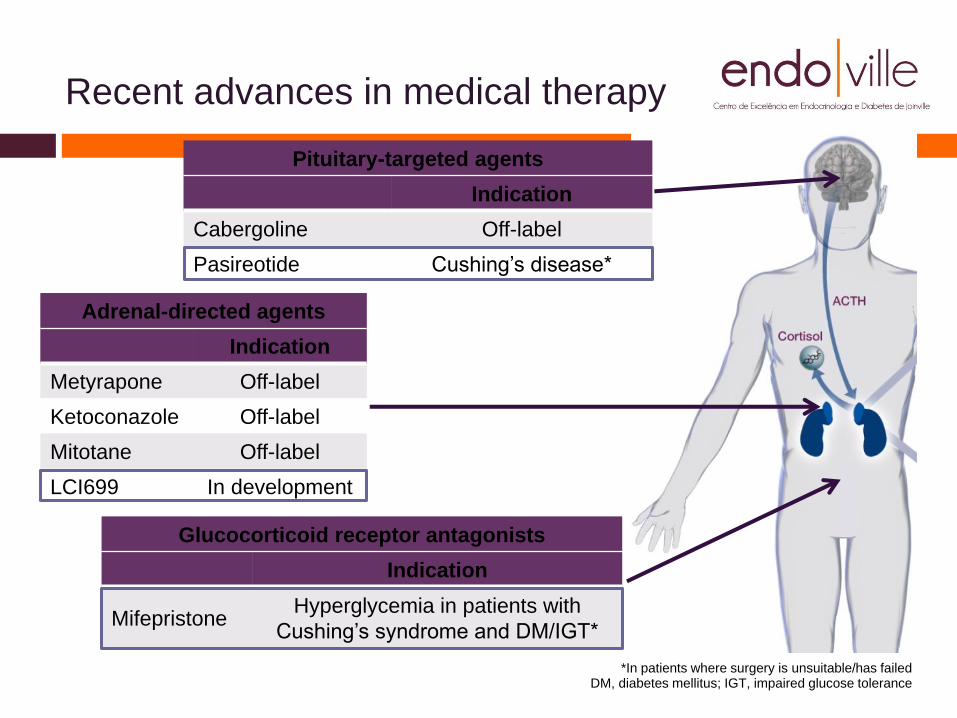
Recent advances in medical therapy
Pituitary-targeted agents
Indication
Cabergoline Off-label
Adrenal-directed agents
Indication
Metyrapone Off-label
Ketoconazole Off-label
Mitotane Off-label
Glucocorticoid receptor antagonists
Indication
Mifepristone Off-label
*In patients where surgery is unsuitable/has failed DM, diabetes mellitus; IGT, impaired glucose tolerance
Pituitary-targeted agents
Indication
Cabergoline Off-label
Pasireotide Cushing’s disease*
Adrenal-directed agents
Indication
Metyrapone Off-label
Ketoconazole Off-label
Mitotane Off-label
LCI699 In development
Glucocorticoid receptor antagonists
Indication
Mifepristone Hyperglycemia in patients with
Cushing’s syndrome and DM/IGT*

Tratamento Futuro
1 – Pasireotide LAR
Dose = 30 mg 30/30 dias IM (LAR)
2 - Pasireotide LAR + Cabergolina
Dose = 30 mg 30/30 dias IM (LAR) + 1 mg / semana
3 – Ácido Retinóico
Mecanismo de ação: Ação no tumor
4 – LC 1699
Mecanismo de ação: Inibidor da B hidroxilase
(esteroidogênese)
Dose: 4 -> 100 mg / dia

Obrigado pela Atenção
www.endoville.com.br
Agradecimentos:
Dra. Julia Appel
Equipe Endoville
Aos nossos pacientes