angioblastic meningioma with intraparenchymal hemorrhage
TRANSCRIPT

ANGIOBLASTIC MENINGIOMA WITH INTRAPARENCHYMALHEMORRHAGE
ismail H. Tekkok. M.D .. Mehmet Turgut. M.D .. Kadir Tabta. M.D .. Siileyman Saglam. M.D ..
Department of Neurosurgery, Hacettepe University school of Medidne,
Slhhiye 06100, Ankara, TURKiYE
Turkish Neurosurgery 2 : 165 - 169. 1992
ABSTRACT
We report the case of a 37-year-old female patient harboring a right tentorial meningioma with bicompartmental growth who deteriorated while awaiting elective surgery. Both radiological and operativefindings demonstrated intratumoral and intracerebellar hemorrhage. The tumor was removed totallyin two sessions and was an angioblastic type. We discuss the frequency. presentation and outcomeof such patients and point out to precautions that need to be taken.
KEY WORDS:
Angioblastic. Hemorrhage. Intracerebellar. Meningioma
INTRODUCTION
Meningiomas are slowly growing benigntumors having a gradual onset with a relatively chronic but progressive course (2). Hemorrhage. vascular changes. cerebral edema. highrate of malignancy and necrosis are factors heldresponsible of acute presentation of meningiomas (2,6.8). Acute presentation of a meningioma is so unexpected that most often ityields poor results (8).The purpose of this paperis to present a case who have bled whileawaiting surgery for a recurrent tentorial meningioma and to discuss the etiology. precautionsto be taken and outcome with a brief reviewof the literature.
CASE HISTORY:
A 37-year old female patient was first admitted in March 1988 with persistent headache oftwo months duration and a history of fourseizures. Concomittantly she had experiencedblurred vision. CT scan demonstrated an enhan
dng mass of 5 em diameter at right parietotemporal region. On March 3, 1988 a craniotomywas performed. A pink mass with moderate
consistency which was found to originate fromthe tentorium was removed gross totally. Thetumor bed was coagulated by bipolar and C02laser. The histopathological diagnosis was ameningioma with sarcomatous degeneration.The patient made an uneventful recovery. Toexclude any possibility of recurrence 50 Gy ofradiotherapy by a C060 source was also given.The patient stayed symptom- and recurrencefree at 6-monthly clinical and yearly CTfollowups.
In June 1991,while the neurological examination was completely normal. a contrast enhanced CT scan as well as an MR scan showedrecurrence on both sides of the tentorium.
Supratentorial growth measured 15x15mm andinfratentorial extension was 30x15 mm (Fig.1a).She was then hospitalized for surgery. Whileawaiting her operation day scheduled for 2 dayslater. she deteriorated suddenly with intensesweating, bradykardia and with decreased sensorium. A repeat CT scan with no contrast showed enlarging hyperdensity measuring 45x35 mm.in the posterior fossa. The fourth ventricle wasdistorted markedly towards left (Fig. 1b).
165
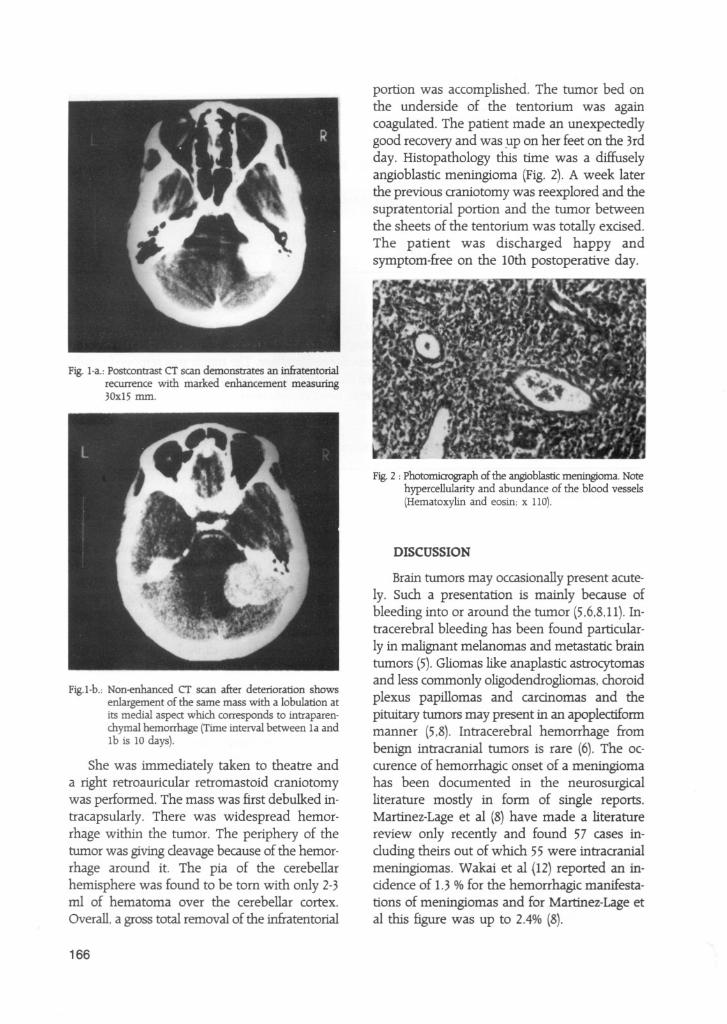
Fig. I-a.; Postcontrast CT scan demonstrates an infratentorialrecurrence with marked enhancement measuring30xl5 mm.
Fig.l-b.; Non-enhanced CT scan after deterioration showsenlargement of the same mass with a lobulation atits medial aspect which corresponds to intraparenchymal hemorrhage (Time interval between la and1b is 10 days).
She was immediately taken to theatre anda right retroauricular retromastoid craniotomywas performed. The mass was first debulked intracapsularly. There was widespread hemorrhage within the tumor. The periphery of thetumor was giving cleavage because of the hemorrhage around it. The pia of the cerebellarhemisphere was found to be tom with only 2-3ml of hematoma over the cerebellar cortex.
Overall. a gross total removal of the infratentorial
166
portion was accomplished. The tumor bed onthe underside of the tentorium was againcoagulated. The patient made an unexpectedlygood recovery and was ~p on her feet on the 3rdday. Histopathology this time was a diffuselyangioblastic meningioma (Fig. 2). A week laterthe previous craniotomy was reexplored and thesupratentorial portion and the tumor betweenthe sheets of the tentorium was totally exdsed.The patient was discharged happy andsymptom-free on the 10th postoperative day.
Fig.2 ; Photomicrograph of the angioblastic meningioma. Notehypercellularity and abundance of the blood vessels(Hematoxylin and eosin; x llO).
DISCUSSION
Brain tumors may occasionally present acutely. Such a presentation is mainly because ofbleeding into or around the tumor (5,6.8,11).Intracerebral bleeding has been found particularly in malignant melanomas and metastatic braintumors (5).Gliomas like anaplastic astrocytomasand less commonly oligodendrogliomas. choroidplexus papillomas and cardnomas and thepituitary tumors may present in an apoplectiformmanner (5.8). Intracerebral hemorrhage frombenign intracranial tumors is rare (6). The occurence of hemorrhagic onset of a meningiomahas been documented in the neurosurgicalliterature mostly in form of single reports.Martinez-Lage et al (8) have made a literaturereview only recently and found 57 cases including theirs out of which 55 were intracranialmeningiomas. Wakai et al (12) reported an inddence of 1.3 % for the hemorrhagic manifestations of meningiomas and for Martinez-Lage etal this figure was up to 2.4% (8).

There appears few points that deserve mentioning. Meningiomas with hemorrhage manifestthemselves during the fifth decade when the indden<;:eof cerebral stroke is already high whichmakes the initial diagnosis quite difficult onclinical grounds (8).No preponderance related tosex has been noted (6).The clinical presentationis almost always that of sudden deterioration ofsensorium accompanied by severe headacheand/or hemiparesis. The occurence of seizuresand the finding of papilledema are rarely encountered.
The value of CT as the emergency imagingmethod can not be overemphasized. Nonenhanced and enhanced CT scans are necessaryto visualize both the tumor and the hemorrhage(6).
Of the 55 cases reported to date (6.8). pureintratumoral bleed occurred in 2 (3.5%)and pureintracerebral in 6 (11%) cases. Intracerebral andintratumoral bleed with extension to
subarachnoid and/or subdural space accountedfor 17 (34%).Subdural space was involved alonein 4 (7%)while pure subarachnoid hemorrhageoccurred in 15 (28%). The rest were subject tocombinations of different locations as to hemor
rhage. Major reviews on the subject (6,8),noteda correlation between the location of the men
ingioma and the likelihood of hemorrhage. Convexity (38%), parasagittal (16%) andintraventricular location in the decreasing orderof frequency resulted in hemorrhagic onset in 55cases upto date. To our knowledge, our case appears as the first tentorial meningioma case tobleed.
Though angioblastic type would be the mostlogical histological type to bleed, meningothelia!meningiomas dominated the related literature(39%)(6).Only 9 (15%)cases of angioblastic meningioma cases with hemorrhage were reported(8).
The mechanism for production of hemorrhage is unknown. Goran etal (4) and Lazaro etal(7) stated that even nonangioblastic meningiomas may have more than one tissue pattern. As Goran etal (4),Modest eta! (9) an Nakaeta! (10) pointed out. the meningiomas assodatedwith hemorrhage showed an unusual vasculari-
ty near the site of hemorrhage and the-ruptureof these angiomatous vessels probably accountedfor the hemorrhage in nonangioblastic subtypes.A transformation to angioblastic subtype afterradiotherapy for sarcomatous meningioma mighthave been the case for our patient. but why thetumor bled infratentorially supports the view ofGoran eta! and Lazaro etal (4,7).
Anticoagulation (3). trauma (1,13) andhypertension (5)have all been implicated as contributory factors. Hamer (5)also speculated thathemorrhagic infarction due to compression of thebrain and of cortical veins leading to erosionmight be another cause (5).
The success rate of treatment depends onlyon prompt diagnosis. A high index of clinicalsuspidon is necessary. The overall mortality ofthe reported cases in the literature in up to 50%(8). in spite of easy availability of CT worldwide.The mortality figures for the angioblastic type hasbeen even higher. The fact that our patient wasa diagnosed meningioma patient contributedpositively to the outcome since she was takento theatre in few hours.
In conclusion, we have reported the case ofa female patient with a bleeding meningioma.We stress the fact that clinical suspidon isnecessary for prompt and accurate diagnosis ofsuch patients and that the preoperativeneurological state correlate well with theoutcome.
Correspondence: Ismail H. Tekkok, M.D.Hacettepe UniversitesiTIp Fakilltesi HastanesiNoro~iriirji Ana Bilim DahSIhhiye. Ankara 06100 - TURKiYEphone: 90-4-3108495Fax: 90-4-311 1131
REFERENCES:
1. Bingas B. Meese M: Subdurales Hamatom seltenerAtiologie (FaIImitteilung)_ Nervenarzt 37:175-177, 1966
2. El-BanhawyA. Walter W: Meningiomas with acute onset.Acta Neurochir (Wien) 10:194-206. 1962
3. Everett BA.Kusske JA. Pribham HW: Anticoagulants andintracerebral hemorrhage from an unsuspected meningioma. Surg Neurol 11:233-235. 1979
4_ Goran A. Ciminello VJ. Fisher RG: Hemorrhage into meningiomas_ Arch Neurol 13:65-69. 1965
167

5. Hamer J: Meningioma of the foramen magnum presenting as subarachnoid hemorrhage and cerebellarhematoma. Neurochirurgia (Stuttg) 22:189-193, 1979
6. Kohli CM, crouch RL: Meningioma with intracerebralhematoma. Neurosurgery 15:237-240, 1984
7. Lazaro RP, Messer HD. Brinker RA: Intracranial hemor
rhage assodated with meningioma. Neurosurgery8:96-101. 1981
8. Martinez-Lage JF, Poza M, Martinez M. Esteban JA. Antunez Me. Sola J: Meningiomas with hemorrhagiconset. Acta Neurochir (Wien) 110:129-132, 1991
9. Modesti LM, Binet EF, Collins GH: Meningiomas causing
spontaneous intracranial hematomas. Neurosurg45:437-441 1976
168
10. Nakao S, Sato S, Ban S, et al: Massive intracerebral hemor
rhage caused by angioblastic meningioma. Surg Neurol7:245-248. 1977
11. PalaogIu S, Ozgen T, Onol B: Acoustic neurinoma withintratumoral bleeding. J-Neurosurg Sd 34:65-67, 1990
12. Wakai S, Yamakawa K. Manaka S, et al: Spontaneousintracranial hemorrhage caused by brain tumor: its inddence and clinical sifnificance. Neurosurgery 10:437-444.1987
13. Ya~gil MG, So SC:Cerebellopontine angle meningiomapresenting as subarachnoid hemorrhage. Surg Neurol6:3-6, 1976