ssc2 oral presentation m5724
TRANSCRIPT
Challenges In Dealing With Dengue Haemorrhagic Fever- LITERATURE REVIEW OF DENGUE VACCINE DEVELOPMENT
Learning Objectives•Be able to recognise how the burdens caused by dengue impact the healthcare system•Be able to understand the basic immunopathology in developing severe dengue and dengue shock syndrome•Be able to recognise the difficulties and challenges of developing dengue vaccines and doing clinical trials on population
A Bit Of Background……•Dengue is a mosquito-borne disease in tropical and sub-tropical regions caused by 4 serotypes (DENV 1–4) belonging to the family Flaviviridae1
•Dengue fever was first recorded in 17th century and in 1906 the presence of flavivirus and its transmission vector, Aedes mosquitoes were confirmed •It affects more than 100 countries and putting 40% of the world’s population at risk; no active treatment and effective prevention method available yet•Given the availability of licensed yellow fever and Japanese encephalitis vaccines, therefore dengue vaccine development is possible
Immunopathology•Theory: antibody-mediated DENV neutralisation in protection against infection; contributions of other immune mechanisms remains unclear1
•Homotypic antibodies confer life long immunity against reinfection with the same virus serotype•Short term cross-reactive antibodies are also produced against other serotypes•Antibody-dependent enhancement (ADE)- When heterotypic antibodies’ levels decline, the disease might be enhanced by facilitating the uptake of virions into FcyR-bearing cells •ADE may contribute to severe dengue and dengue shock syndrome especially in those with previous dengue infection
So, why do we still not have an effective vaccine
for dengue in the past 100 years?
Clinical Development Challenges1
1. Potential role of immune responses in the pathogenesis of severe dengue◦ 4 serotypes circulate globally and different from time to time
2. Lack of satisfactory animal models and immunological correlate◦ Dengue is a human disease; lack of susceptibility to infection or the absence of
human like expression of disease in animal studies
3. Challenges in the design and conduct of dengue efficacy studies◦ Lack of diagnostic algorithms in dengue detection and difficulties in making high
compliance from trial participants in long-term◦ For better efficacy studies, diversification of sites is needed
Potential Technological Approaches•Live-attenuated virus vaccines•DNA vaccines•Recombinant subunit vaccines•Purified inactivated virus vaccines•Virus-like particles vaccines•Virus-vectored vaccines•More……….
The World’s First Dengue Vaccine? A Phase III Study by Sanofi Pasteur Tetravalent Vaccine2
•Tetravalent dengue vaccine comprising four recombinant, live, attenuated dengue viruses (CYD-1–4) based on the yellow fever 17D vaccine strain •Preclinical evaluation:
1. both genotypic and phenotypic stability were demonstrated2. a controlled response with limited inflammatory cytokine production and
consistent type 1 IFN confirmed in vitro immunogenicity with good safety profile
3. non-human primates studies showed that one or more vaccinations conferred immunity against all serotypes, and almost complete protection against upon subsequent wild type challenge
•Phase I evaluation• A tetravalent formulation was used in 66 dengue naïve subjects in US and
demonstrated complete seropositivity against the 4 dengue serotypes after three vaccinations in a 0–3.5–12 month regimen• Results showed favourable safety profile and low levels of viremia, mainly
CYD-4 were observed after the first vaccination. Viremia was even lower after the second vaccination compared to the first, with more than 85% of subjects having no detectable CYD-1, 2, or 3 viremia • After receiving 3 vaccinations, all subjects seroconverted to all 4 WHO
reference dengue strains
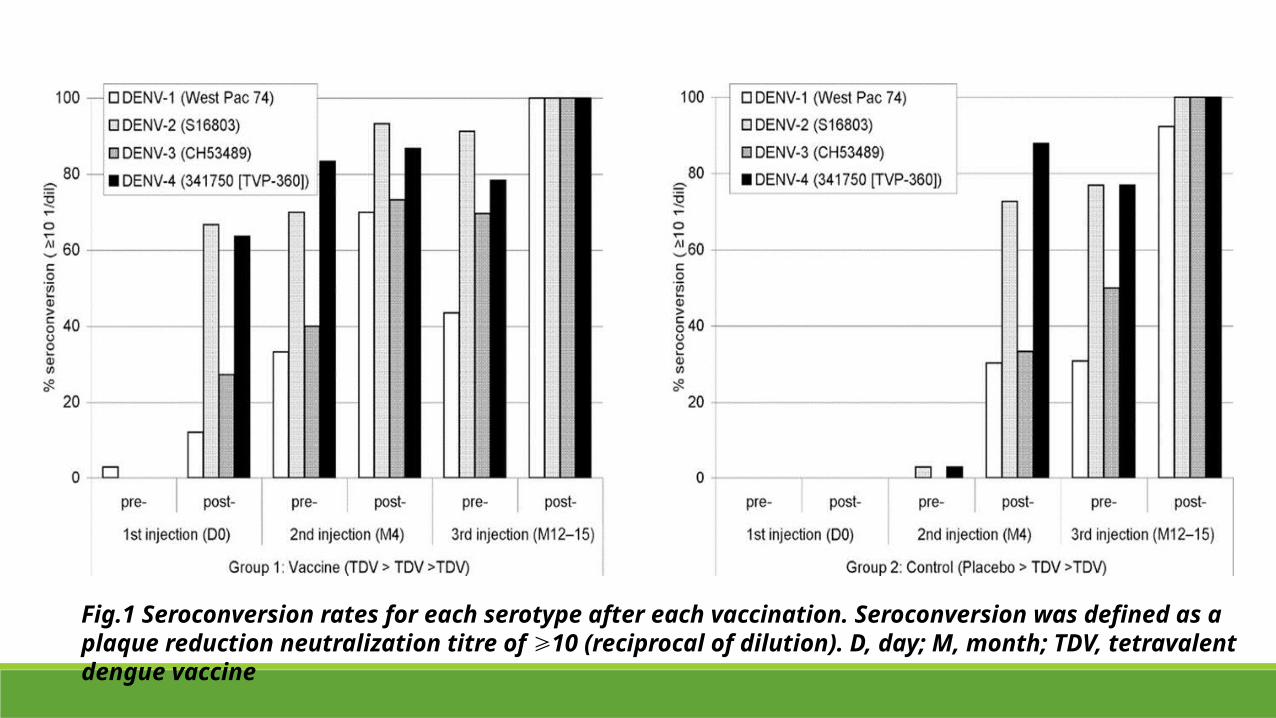
Fig.1 Seroconversion rates for each serotype after each vaccination. Seroconversion was defined as a plaque reduction neutralization titre of 10 (reciprocal of dilution). D, day; M, month; TDV, tetravalent dengue vaccine⩾
• Two other same tetravalent studies were carried out in a dengue endemic area (Philippines) and a non-endemic area (Mexico City) with enrolment of children (2-17 years old); results were consistent to the US study • Despite the differences in immunological status of the two
populations, results confirms that pre-existing flavivirus immunity does not adversely affect the safety of CYD-TDV
•Phase II evaluation• Objectives: To document the immunogenicity and safety of the tetravalent
vaccine candidates with the 0–6–12 month schedule in populations with different vaccination histories and investigating co-administration with another live virus vaccine in toddlers • A study in Peru included 2–11 years old with a history of YF vaccination earlier
received three TDV vaccinations or three control vaccinations at months 0–6–12; results were consistent with phase I study with good safety profile• Therefore, reactogenicity was neither increased by the presence of baseline
immunity to dengue and yellow fever, nor was it increased after the second or third vaccination than after the first
•Phase III evaluation• Randomised, observer-masked, placebo-controlled trials involving 31,144
children in the age group of 2-16 years old were carried out in 10 dengue endemic countries in Latin America and Asia (including Malaysia)3,4
• The injections of vaccine or placebo were done at 0,6 and 12 months with blood sampling and visits up to 25 months• Blood samples were taken from children with >38°C for 2 days to confirm
the presence of dengue after vaccination• Results showed the proportion of episodes and duration of hospital
admission due to virologically confirmed dengue were lower in the vaccine group than the control group
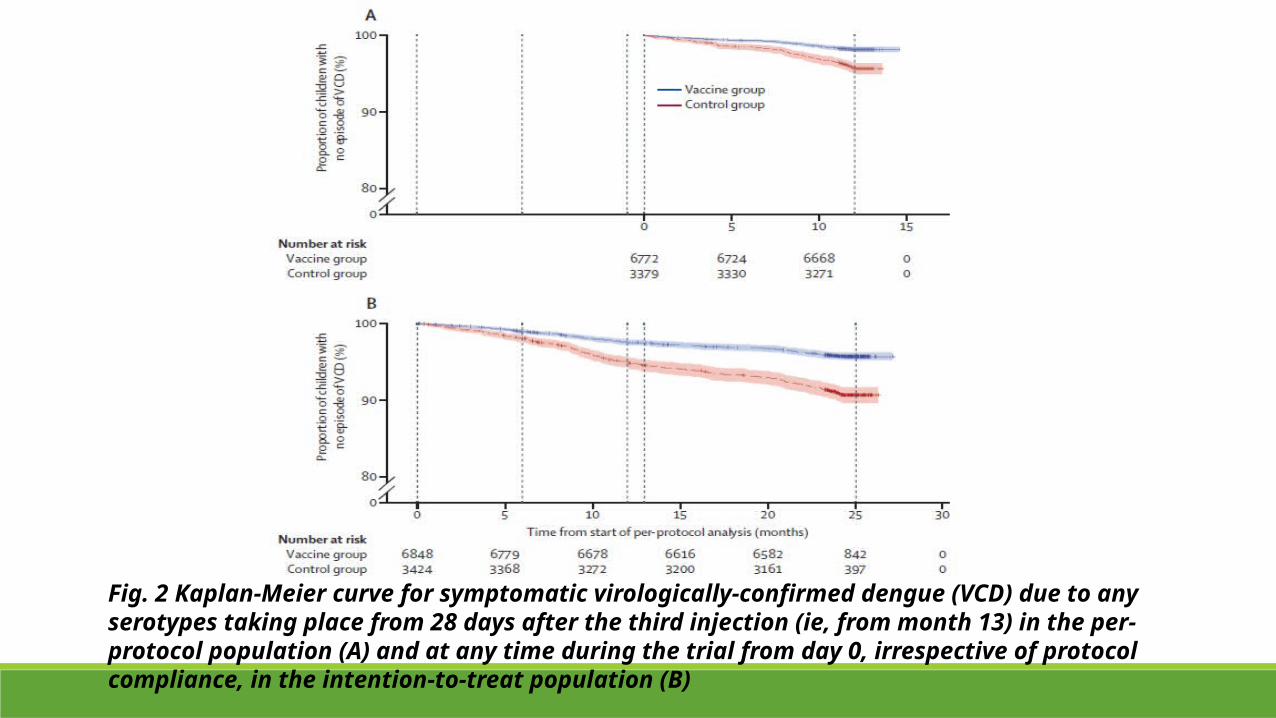
Fig. 2 Kaplan-Meier curve for symptomatic virologically-confirmed dengue (VCD) due to any serotypes taking place from 28 days after the third injection (ie, from month 13) in the per-protocol population (A) and at any time during the trial from day 0, irrespective of protocol compliance, in the intention-to-treat population (B)
Future……?•Interestingly, despite the presence of neutralising antibodies, studies also showed that there were certain efficacy against serotypes 1, 3 and 4 but not against serotype 2•Serotype 2 is the main dengue serotype that circulates in Asia, thus the efficacy is being questioned now•Nonetheless, CYD-TDV is proved to provide a certain degree of protection to severe dengue haemorrhagic presentation and therefore have a substantial effect on public health•Hopefully this vaccine will become the pioneer dengue vaccine in the market to reduce disease burden and further improvements on vaccine’s efficacy could be done in the future
References1. D. Wallace and et al (2013). "Challenges in the clinical development of a dengue vaccine."
Current Opinion in Virology(3): 352-356.
2. B. Guy and et al (2011). "From research to phase III: Preclinical, industrial and clinical development of the Sanofi Pasteur tetravalent dengue vaccine." Vaccine 29: 7229-7241.
3. L. Villar and et al (2015). "Efficacy of a Tetravalent Dengue Vaccine in Children in Latin America." The New England Journal of Medicine 372(2): 113-123.
4. M.R. Capeding and et al (2014). "Clinical efficacy and safety of a novel tetravalent dengue vaccine in healthy children in Asia: a phase 3, randomised, observer-masked, placebo-controlled trial." Lancet 384: 1358-1365.