sÈpsia abdominal greu - home | acadèmia de ciències … · 2016-05-13 · tractament antibiòtic...
TRANSCRIPT

Tractament antibiòtic empíric i dirigit. Durada. Desescalada.
Emili Díaz
Servei de Medicina IntensivaHospital Parc TaulíSabadell
SÈPSIA ABDOMINAL GREU

2
Pacient amb dolor abdominal, febre idolor a fosa ilíaca dreta
© Academy for Infection Management 2003 (All Rights Reserved)

3
Dades clíniques
• Noia de 22 anys que presenta dolor abdominal– inici agut– localitzat a fossa ilíaca dreta– no molt intens quan arriba a Urgències
• Exploració física no concluent– es realitza TC de abdomen

4
TC abdomen mostra apendix perforat

5
Es realitza cirurgia laparoscòpica
Area of gangrene/perforation
Pus/fibrin

6
Preguntes
• Quins patògens s’han de cobrir?• Tractaria aquesta pacient amb monoterapia o
combinació?• Quin o quins antibiòtics triaria?

7
Postoperatori
• Pacient va rebre 5 dies tractament antibiòticamb ciprofloxací i metronidazol– 2 dies parenteral, i desprès 3 dies oral
• Es va recuperar bé i va ser donada d’alta el dia3 postoperatori

SEPSIA INTRAABDOMINAL
2.- Durada
1.- Tractament empíric
3.- Desescalada

SEPSIA INTRAABDOMINAL
2.- Durada
1.- Tractament empíric
3.- Desescalada

Optimising anti-infective therapy: time to treatment
Adequate antimicrobial therapy should start within 1 hour
0.0
0.2
0.4
0.6
0.8
1.0Fractionof totalpatients
Time from hypotension onset (h)
Survival fractionCumulative effective antimicrobial initiation
Kumar A et al. Crit Care Med 2006;34:1589-96

Complicated intra-abdominal infection: results of randomised trials
n=633 n=1262
n=962n=379
DOR, doripenem; EPM, ertapenem; IMP, imipenem; MER, meropenem; mITT, modified intent-to-treat; M-mITT, microbiological mITT; MFX, moxifloxacin; PIPTAZ, piperacillin / tazobactam; TG, tigecycline
Solomkin JS et al. Ann Surg 2003;237:235-45;
Babinchak T et al. Clin Infect Dis 2005;41:S354-67; Malangoni MA et al. Ann Surg 2006;244:204-11;
Solomkin JS et al. Abs presented at ICAAC 2007
Success (%)
Success (%)
Success (%)
Success (%)
EPMPIPTAZ
TGIMP
MXFPIPTAZ
DORMER

Complicated intra-abdominal infection: trials were in lower-risk patients
mITT
Included in M-mITT
Apache II
Mortalitya
Appendicitis / cholecystitis
Doripenem
962
80%
<10 : 90%
3.0%
66%
Moxifloxacin
656
48%
Mean 6.4c
2.0%
60%c
Tigecycline
1642
77%
Mean 6.2b
2.5%
64%b
Ertapenem
633
63%
<15 : 92%b
4.9%
65%b
Babinchak T et al. Clin Infect Dis 2005;41:S354-67; Malangoni MA et al. Ann Surg 2006;244:204-11;Solomkin JS et al. Ann Surg 2003;237:235-45; Solomkin JS et al. Poster (Abs 487) presented at ICAAC 2007
aData for mITT populationbData for M-mITT population; cData for clinical efficacy population

Steinbach CL et al.Ann Clin Microbiol Antimicrob 2015;14:48
SPECTRUM ADEQUACY OF ANTIBIOTIC REGIMENS FOR SECONDARY PERITONITIS:A RETROSPECTIVE ANALYSIS IN
INTERMEDIATE AND INTENSIVE CARE UNIT PATIENTS
0102030405060
COMUNITARIA HOSPITALARIA
242 pacients. 654 microorganismes. Mediana 2 patògens, màxim 8.
n=88 n=154
%

Theunissen C et al. Intern J Infect Dis 2011;15:e769
MANAGEMENT AND OUTCOME OF HIGH-RISK PERITONITIS: A RETROSPECTIVE SURVEY 2005-2009
0
10
20
30
40
50
60
Narrow-spectrum* Broad-spectrum** Fluoroquinolone Aminoglycoside
COMUNITARIA HEALTHCARE HOSPITALARIA
93 pacients. 141 microorganismes. APACHE II 20
n=43 n=37
%
Perfil de resistència entre BGN
n=13*A/C o cefuroxime** 3-4ª gen cefalosporina, P/T, meropenem

TRACTAMENT EMPIRIC
Solomkin JS et al. Clin Infect Dis 2010;50:133-64

Guirao X et al. Rev Esp Quimioter 2009;22:151
RECOMENDACIONES EN EL TRATAMIENTO ANTIBIÓTICO EMPÍRICO DE LA INFECCIÓN INTRAABDOMINAL


Pharmacodynamic parameters(in vivo potency)
AUC:MIC
T>MIC
Cmax:MIC
Concentration
Time (hours)
MIC
AUC = Area under the concentration–time curveCmax = Maximum plasma concentration

Probability of developing resistance
Thomas et al. Antimicrob Agents Chemother 1998;42:521–527
AUC0–24h:MIC ³100
AUC0–24h:MIC <100
Days from initiation of therapy0 5 10 15 20
0
20
40
60
80
100Probability of remaining susceptible (%)
Data from 107 acutely ill patients with nosocomial RTIs treated with 5 different antibiotic regimens (ciprofloxacin, cefmenoxime, ceftazidime, ciprofloxacin plus piperacillin, ceftazidime plus tobramycin)
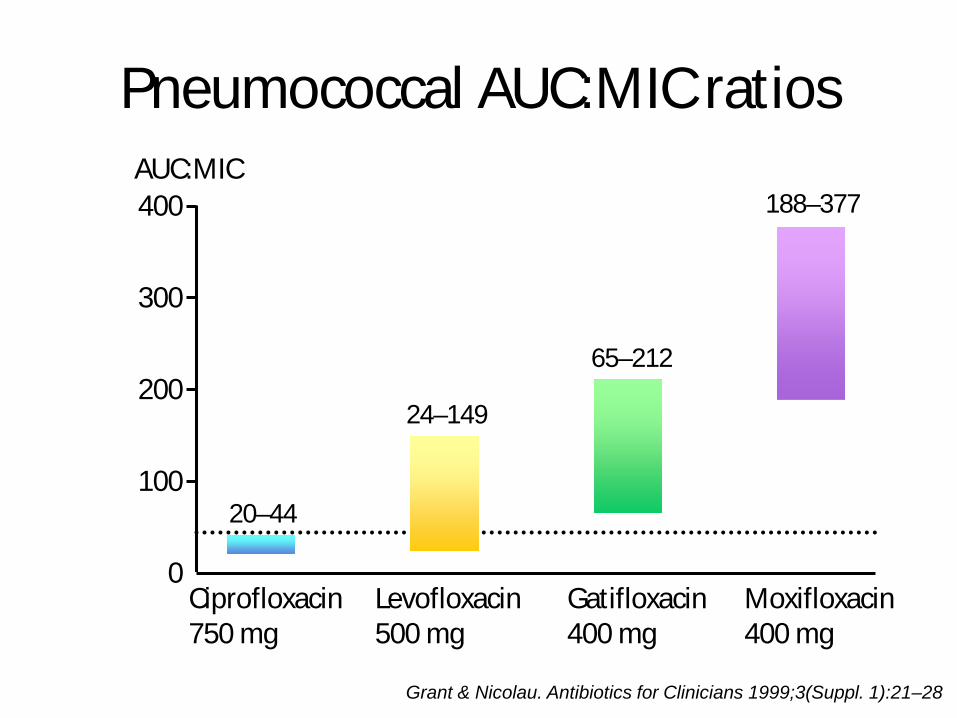
Grant & Nicolau. Antibiotics for Clinicians 1999;3(Suppl. 1):21–28
Pneumococcal AUC:MIC ratios AUC:MIC
0
100
200
300
400 188–377
65–212
24–149
20–44
Ciprofloxacin750 mg
Levofloxacin500 mg
Gatifloxacin400 mg
Moxifloxacin400 mg

Efficacy and safety of cefepime: a systematic review and meta-analysis
Yahav D et al. Lancet Infect Dis 2007;7:338
• 57 trials• Mortalitat de qualsevol causa: cefepime vs altres beta-lactams• Risk ratio 1.26 (IC 95%: 1.08-1.49)
• Revisió FDA• Risk Mortalitat en SSTI, neutropenia febril• No risc a pneumònia, infecció intra-abdominal i infec. urinària
Kalil AC. J Antimicrob Chemother 2011;66:1207

Cefepime therapy for monomicrobial Enterobacter cloacae bacteremia:Unfavourable outcomes in patients infected bycefepime-susceptible dose-dependent isolates
Lee NY et al. Antimicrob Agents Chemother 2015;59:7558
0
10
20
30
40
50
60
70
80
Mortalitat
CefepimeCarbapenem
Retrospectiu. 305 adults amb bacteriemia per Enterobacter cloacae SDD (susceptible dose dependent

SEPSIA INTRAABDOMINAL
2.- Durada
1.- Tractament empíric
3.- Desescalada
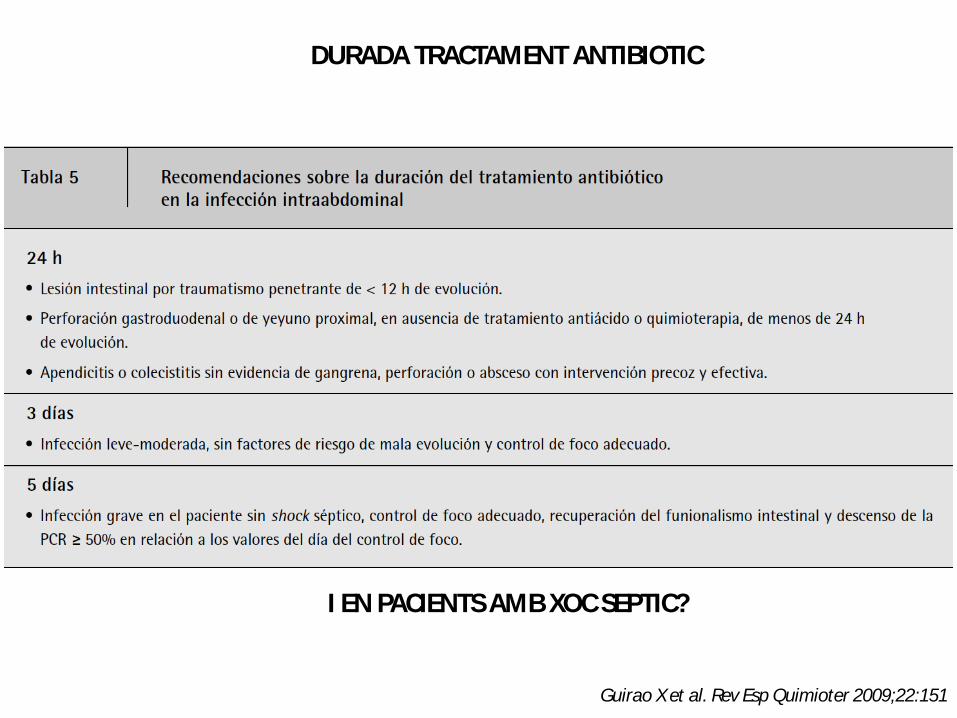
DURADA TRACTAMENT ANTIBIOTIC
Guirao X et al. Rev Esp Quimioter 2009;22:151
I EN PACIENTS AMB XOC SEPTIC?

FACTORS CLINICS PREDICTORS DE FRACAS DEL CONTROL DEL FOCUSPER INFECCIÓ INTRAABDOMINAL
• Retard en la intervenció inicial (>24 h)• Gravetat (APACHE II score >15)• Edat avançada• Comorbilitat i grau de disfunció orgànica• Baix nivell d’albúmina• Mal estat nutricional• Grau de afectació peritoneal l peritonitis difusa• Imposibilitat per aconseguir adequat desbridament o control
del drenatge.• Neoplàssia
Solomkin JS et al. Clin Infect Dis 2010;50:133-64

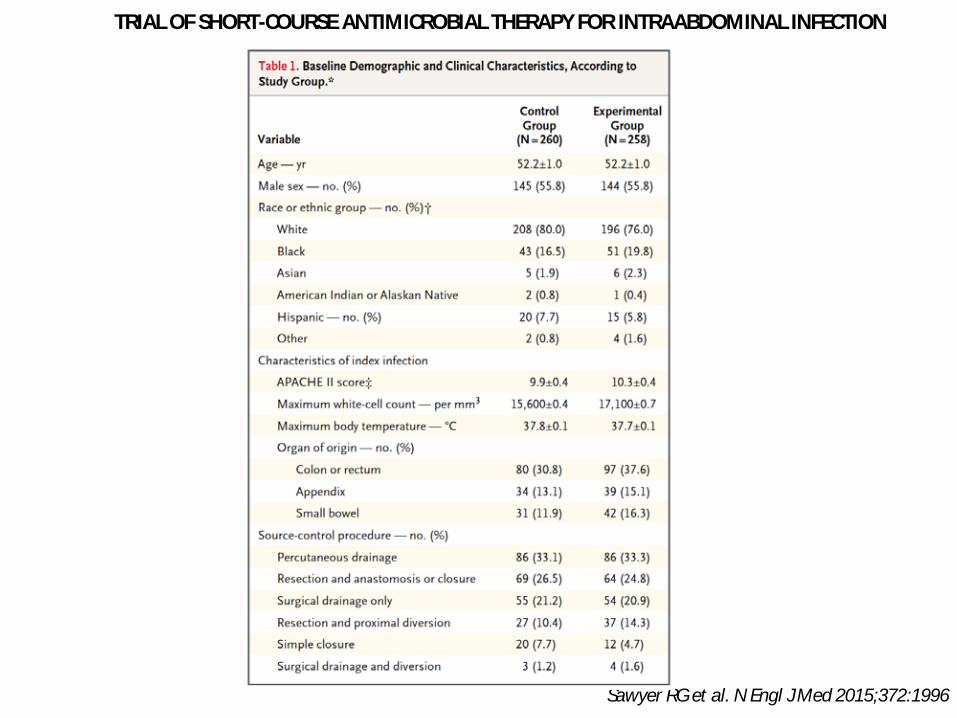
TRIAL OF SHORT-COURSE ANTIMICROBIAL THERAPY FOR INTRAABDOMINAL INFECTION
Sawyer RG et al. N Engl J Med 2015;372:1996
• 518 pacients• 2 tractaments:
• +2 dies (màxim 10) desprès resolució febre, leucocitosi, ili• 4+1 dies
• Outcome primari: compost de infecció ferida quirúrgica, infeccióintraabdominal recurrent o mort 30 dies
TRIAL OF SHORT-COURSE ANTIMICROBIAL THERAPY FOR INTRAABDOMINAL INFECTION
Sawyer RG et al. N Engl J Med 2015;372:1996

TRIAL OF SHORT-COURSE ANTIMICROBIAL THERAPY FOR INTRAABDOMINAL INFECTION
Sawyer RG et al. N Engl J Med 2015;372:1996

Maseda E et al. J Crit Care 2015;30:537
PROCALCITONIN-GUIDED THERAPY MAY REDUCE LENGTH OF ANTIBIOTIC TREATMENT IN INTENSIVE CARE UNIT PATIENTS
WITH SECONDARY PERITONITIS: A MULTICENTER RETROSPECTIVE STUDY
• 121 pacients• Retrospectiu. Daily PCT.• Stop antibiotic if: <0.5 ng/mL or 80% decrease peak concentration• (Bouadma et al. 5.4% abdominal source)
PCT NON-PCT p
ICU LOS (days) 5 5 NS
MORTALITY 9.6 13 NS
ATB (days) 5.1 10.2 <0.001
Procalcitonin guidance produced 50% reduction in antibiotic duration

SEPSIA INTRAABDOMINAL
2.- Durada
1.- Tractament empíric
3.- Desescalada

Per desescalar necessitem Microbiologia,
i a la peritonitis secundaria comunitaria sense
factors de risc no està indicada.

Cultius si:
• Health care-associated
• Pacients en risc: inmunodepressió, ATB, ...
Solomkin JS et al. Clin Infect Dis 2010;50:133-64



DE-ESCALATION OF EMPIRICAL THERAPY IS ASSOCIATED WITH LOWER MORTALITY IN PATIENTS WITH SEVERE SEPSIS AND SEPTIC SHOCK
Garnacho-Montero J et al. Critical Care 2016;20:83
• 403 patients with adequate antimicrobial therapy• Abdomen: 184• Antimicrobial treatment: Univariate
ANTIMICROBIAL TREATMENT
ALIVE DEATH p
ESCALATION 15,5 27,2 0.006
DE-ESCALATION 48,6 35,2 0.013
NO CHANGE 36 37,6 0.753
• De-escalation antimicrobial treatment and mortality: Multivariate• 0.54 (0.33-0.89) p=0.016

Montravers P et al. Critical Care 2016;20:83
CHARACTERISTICS AND OUTCOMES OF ANTI-INFECTIVE DE-ESCALATION DURING HEALTH CARE-ASSOCIATED INTRA-ABDOMINAL INFECTIONS
• 311 patients• Health care-associated intra-abdominal infections• De-escalation:
• Withdrawal of one agent (betalactam, aminoglycoside, fluoroquinolone, ancomycin, antifungal)• Narrowing spectrum of activity (betalactam)• and/or switch from combination to monotherapy.

Montravers P et al. Critical Care 2016;20:83
CHARACTERISTICS AND OUTCOMES OF ANTI-INFECTIVE DE-ESCALATION DURING HEALTH CARE-ASSOCIATED INTRA-ABDOMINAL INFECTIONS

CHARACTERISTICS AND OUTCOMES OF ANTI-INFECTIVE DE-ESCALATION DURING HEALTH CARE-ASSOCIATED INTRA-ABDOMINAL INFECTIONS
Montravers P et al. Critical Care 2016;20:83


40
Reingrès a l’hospital
• Pacient torna a l’hospital el dia 7 postoperatori amb febre i dolor abdominal – examen físic suggestiu de massa abdominal– leucos 15 000/µL– TC abdomen de nou

41
Abcès Postoperatori abscess

42
Seguiment
• Es realitza drenatge percutani– 200 mL pus– culture reveals Klebsiella oxytoca BLEE

PUNTS CLAU
• Tractament antibiòtic en infecció intraabdominal:
• Tractament empíric comunitari no és un problema.
• Vigilar factors de mala evolució.
• A pacients amb xoc sèptic, amb manca de dades, podria ser:
• +2 dies desprès de solucionar fracàsos orgànics, febre, leucos
• uns 7-10 dies pot ser suficient.
• Desescalar és possible, sobre tot en casos health care-associated.