secuenciación terapéutica en cáncer de...
TRANSCRIPT

Secuenciacion terapeutica en cancer de pancreas
Andrés J. Muñoz Martín MD PhD
Servicio de Oncología Médica
Hospital General Universitario Gregorio Marañón

My disclosures
• Consultant or advisory role: Celgene
• Speaking: Celgene, Shire

• En los últimos siete años se ha modificado de forma significativa el tratamiento de primera línea de pacientes con cáncer de páncreas con la aparición de dos regímenes de quimioterapia: FFX y G-A
Se ha observado un incremento significativo de la supervivencia
Se han observado “largos supervivientes” (>2-3 años)
Se ha triplicado la tasa de respuestas
• En los últimos dos años se ha consolidado el tratamiento de
segunda línea basado en la combinación de FP y oxaliplatino o naliri y se ha introducido un nuevo concepto terapéutico “secuenciación”
Ensayos aletaorizados fase III en 3ª línea PANCRIT-1 (pacientes están
viviendo más y con buena calidad de vida)
En los últimos siete años en
cáncer de páncreas….

Primary Endpoint (OS) & Response Rate
Conroy T. N Engl J Med 2011;364:1817-25
mOS 11.1m FOLFIRINOX VS. 6.8 m G
mOS 8.7 m NP-G vs. 6.6 m G
Von Hoff DD, N Engl J Med. 2013;369:1691-1703
Diferencias de resultados…
Response rate 23% (29%) vs 31%

¿Son comparables los resultados de los dos estudios?
No
¿Por qué no son comparables? Las poblaciones incluidas son diferentes
¿Se podrían justificar las diferencias observadas?
Se podrían justificar…
¿Podemos esperar una comparación directa de los dos esquemas en un estudio randomizado?
Muy probablemente no…
MPACT vs PRODIGE

Características de las poblaciones
Estudio PRODIGE/ACCORD FOLFIRINOX
MPACT GZT+NBP
Edad (mediana y rango) 61 años (25-76) 63 años (27-86)
Pacientes ancianos >76 años No Si
Pacientes PS0 37% 16%
Pacientes PS2 1% 7%
Mediana de localizaciones metastásicas
2 3
Ca19.9 >59 LAN
(medida indirecta carga tumoral)
++ 42%
+++ 52%
MPACT
• Población con características clínicas más desfavorables en cáncer de páncreas: más jóvenes y más “sanos”
• Mayor número de pacientes recibieron tratamiento de 2ª línea en el estudio de FFX: FFX 47% vs G-NABP 40%, 2ª línea impacta en supervivencia

Tabernero et al. Beaujon Conference 2014
Pacientes ECOG 0-1 MPACT
Mediana de SG: 9,7 meses
Tabernero J et al, The Oncologist 2015;20:1–8

ASCO 2014: US Study Oncology Network, OS comparative study
First line chemo n Median OS
FOLFIRINOX 666 11.2 months
Gem + other drug 1567 7.0 months
Gem + nabpaclitaxel 184 10.2 months
Cartwright TH et al. J Clin Oncol 2014:32(15s):287s (Abs 4132)


YOSEMITE trial PhIIR, ESMO 2017 Related Adverse Events ≥ 15%
Overall Survival
Overall Survival by Region
Progression-Free Survival
There is accumulating evidence that the cell types within tumors are heterogeneous and that a
subset of the cells retain the property to self-renew and give rise to more differentiated progeny.
These cells, called Cancer Stem Cells (CSCs) or tumor initiating cells drive tumor growth and
metastasis and are more resistant to chemotherapy and radiotherapy than the remaining tumor cells.
The ability to characterize the CSCs through surface markers and functional limiting tumor dilution
assays, using minimally passaged human tumors, has enabled the identification of novel agents that
target the CSC population. One pathway which appears critical for the CSCs is the Notch pathway.
The pathway is comprised of 4 Notch receptors (1-4) and 5 ligands, Jagged (1-2) and delta-like
ligand (DLL1, 3 and 4). The DLL4 ligand contributes to CSC self-renewal and vascular
development. Demcizumab (DEM) is a humanized IgG2 antibody that binds to DLL4. In minimally
passaged human tumor xenografts, DEM was observed to have activity against a variety of tumors
including colorectal cancer, breast cancer, lung cancer, pancreatic cancer, melanoma and ovarian
cancer. The impact of treatment on the frequency of tumorigenicity was assessed using a limiting
dilution assay. In several models, using different chemotherapeutic agents, while the chemotherapy
alone decreased tumor volume, the frequency of tumor initiating cells was increased in the residual
tumor. In contrast, DEM alone decreased the frequency of CSCs and the greatest reduction was
observed when DEM was combined with GEM and nab-paclitaxel.
YOSEMITE: A 3 Arm Double-Blind Randomized Phase 2 Study of Gemcitabine, Paclitaxel Protein-Bound Particles for Injectable
Suspension (Abraxane®) and Placebo (GAP) versus Gemcitabine, Abraxane® and either 1 or 2 Truncated Courses of Demcizumab
Subject Disposition Placebo/
Placebo
Demcizumab/
Placebo
Demcizumab/
Demcizumab
Total
Intent to Treat 68 71 65 204
Safety Population 68 71 65 204
Ongoing 16 18 9 43
Discontinued 52 53 56 161
Reason for discontinuation
Progression
Death
AE
Withdraw Consent
Other Cancer Treatment
Investigator Decision
Other
34
5
3
0
0
2
8
28
4
5
4
0
5
7
34
3
5
1
1
2
10
96
12
13
5
1
9
25
RECIST Best Overall Response (n=204) Best Response Placebo/
Placebo
(N = 68)
Demcizumab
(N = 136)
P value
CR 0 1
PR 28 44
SD 20 56
PD 14 19
Response Rate (CR+PR) (95%
CI)
28 (41.2%) 45 (33.1%) 0.2815
Clinical Benefit (CR+PR+SD)
(95% CI)
48 (70.6%) 101 (74.3%) 0.5023
Conclusions •This was a randomized, double blind, 3 arm (1:1:1) study in subjects
with 1st-line metastatic pancreatic ductal adenocarcinoma.
•Two hundred and seven patients were randomized via an IWRS
system and 204 patients were treated.
•Patients were well balanced for the known prognostic factors between
the 3 treatment Arms.
•The efficacy outcomes were similar between Arm 1 vs. Arms 2 and 3
combined:
–Response rate: 41.2% vs 33.1% (p value = 0.2815)
–PFS: 5.49 mos. (95% CI:3.81-7.36) vs.5.52 mos.(95% CI:4.17-7.39) (HR = 0.93)
–OS: NR (95% CI:NR-8.97-NR) vs.13.24 mos.(95% CI: 9.79-16.53) (HR= 1.02)
• The efficacy outcomes were also similar when Arm 1 was compared
separately to Arm 2 and Arm 3.
•The most common AE’s in Arms 1, 2 and 3 respectively were:
–Nausea 61.8%, 53.5% and 63.1%
–Diarrhea 50.0%, 57.7% and 69.2%
–Anemia 39.7%, 60.6% and 53.8%
–Fatigue 50.0%. 43.7% and 56.9%
–Peripheral Edema 42.6% 54.9 and 52.9%
•The incidence of ≥ Grade 3 heart failure and pulmonary hypertension
were low and similar in all 3 treatment Arms. The incidence of ≥ Grade
3 bleeding was higher in the demcizumab arms.
–Heart Failure: 0/68 (0%), 4/71 (5.6%) and 1/65 (1.5%)
–Pulmonary Hypertension: 0/68 (0%), 1/71 (1.4%) and 0/65 (0%)
–Bleeding: 1/68 (1.5%), 7/ 71 (9.8%) and 4/65 (6.2%)
All Adverse Events ≥ 30%
Cancer Characteristics
Placebo/
Placebo
(N= 68)
Demcizumab/
Placebo
(N= 71)
Demcizumab/
Demcizumab
(N= 65)
Total
(N= 204)
ECOG PS
0
1
34
34
33
38
31
34
98
106
Region
US/Canada
Europe/Australia
20
48
23
48
19
46
62
142
CA 19-9
0-ULN
>ULN - < 59 X ULN
> = 59 X ULN
14
27
27
15
28
28
12
26
27
41
81
82
Background
Study Design Demographics
Placebo/
Placebo
(N= 68)
Demcizumab/
Placebo
(N= 71)
Demcizumab/
Demcizumab
(N= 65)
Total
(N= 204)
Age (Median) 62 63 66 63
Sex (M/F) 41/27 40/31 35/30 116/88
Number of Metastatic
Sites
0
1
2
3
> 3
1
27
23
12
5
0
26
24
18
3
1
23
28
8
5
2
76
75
38
13
Hepatic Metastases
Yes
No
72.1%
27.9%
74.6%
25.4%
75.4%
24.6%
74%
26%
NLR (Median) 3.2 3.8 3.4 3.5
Copies of this poster obtained through Quick Response (QR) code are for personal use only
and may not be reproduced without written permission from ASCO and the authors of this poster.
Study Schema
Primary Endpoint Secondary Endpoints Exploratory Endpoints
PFS
Survival Response
Safety
Biomarkers
Randomized: 207 pts Treated: 204 pts Data Cut: Nov 7, 2016
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Heart Failure
0 - 4 (5.6) 1 (1.5) 5 (2.5)
Pulmonary
Hypertension
0 - 1 (1.4) 0 - 1 (0.5)
Bleeding
1 (1.5) 7 (9.8) 4 (6.2) 12 (5.9)
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Nausea 42 ( 61.8) 38 ( 53.5) 41 ( 63.1) 121 ( 59.3)
Diarrhea 34 ( 50.0) 41 ( 57.7) 45 ( 69.2) 120 ( 58.8)
Anemia 27 ( 39.7) 43 ( 60.6) 35 ( 53.8) 105 ( 51.5)
Fatigue 34 ( 50.0) 31 ( 43.7) 37 ( 56.9) 102 ( 50.0)
Edema peripheral 29 ( 42.6) 39 ( 54.9) 34 ( 52.3) 102 ( 50.0)
Alopecia 30 ( 44.1) 33 ( 46.5) 28 ( 43.1) 91 ( 44.6)
Vomiting 27 ( 39.7) 32 ( 45.1) 25 ( 38.5) 84 ( 41.2)
Pyrexia 24 ( 35.3) 30 ( 42.3) 23 ( 35.4) 77 ( 37.7)
Decreased appetite
19 ( 27.9) 30 ( 42.3) 27 ( 41.5) 76 ( 37.3)
Neutropenia 21 ( 30.9) 24 ( 33.8) 25 ( 38.5) 70 ( 34.3)
Constipation 20 ( 29.4) 21 ( 29.6) 28 ( 43.1) 69 ( 33.8)
Abdominal pain 24 ( 35.3) 16 ( 22.5) 27 ( 41.5) 67 ( 32.8)
Asthenia 18 ( 26.5) 27 ( 38.0) 20 ( 30.8) 65 ( 31.9)
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Fatigue 22 ( 32.4) 20 ( 28.2) 27 ( 41.5) 69 ( 33.8)
Nausea 21 ( 30.9) 17 ( 23.9) 19 ( 29.2) 57 ( 27.9)
Anemia 15 ( 22.1) 19 ( 26.8) 17 ( 26.2) 51 ( 25.0)
Diarrhoea 10 ( 14.7) 18 ( 25.4) 22 ( 33.8) 50 ( 24.5)
Alopecia 12 ( 17.6) 16 ( 22.5) 13 ( 20.0) 41 ( 20.1)
Edema
peripheral 14 ( 20.6) 13 ( 18.3) 14 ( 21.5) 41 ( 20.1)
Vomiting 9 ( 13.2) 18 ( 25.4) 7 ( 10.8) 34 ( 16.7)
Asthenia 9 ( 13.2) 13 ( 18.3) 11 ( 16.9) 33 ( 16.2)
Decreased
appetite 5 ( 7.4) 16 ( 22.5) 11 ( 16.9) 32 ( 15.7)
Hypertension 6 ( 8.8) 11 ( 15.5) 12 ( 18.5) 29 ( 14.2)
Cubillo A1, Dean A2, Munoz A3, Hidalgo 1, Pazo Cid R4, Martin M5, Macarulla T6, Lipton L7, Harris M8, Manzano JL9, MaurelJ10, Gullen-Ponce C11, Tebbutt N12, Cooray P13, Sohal D14, Zalupski M15, Kolevska T16, Stagg R17, , Goldstein D18. 1Hospital Universitario HM Sanchinarro –
CIOCC, Madrid, 2St John of God Hospital Subiaco, Perth, 3Hospital General Universitario Gregorio Marañon, Madrid, 4Hospital Universitario Miguel Servet, Zaragoza, 5Hospital de La Santa Creu i Sant Pau, 6Vall d´Hebron University Hospital (HUVH) and Vall d’Hebron Institute of
Oncology (VHIO), Barcelona, 7Sunshine Hospital, Melbourne, 8Monash Medical Centre, Moorabbin Campus, 9Germans Trias i Pujol Hospital, ICO-Badalona, Barcelona, 10Hospital Clinic de Barcelona, Barcelona, 11Hospital Universitario Ramón y Cajal, Madrid, 12Austin Health,
Heidelberg, 13Box Hill Hospital, Melbourne, 14Cleveland Clinic, Cleveleand, OH, 15University of Michigan Cancer Center, Ann Arbor, MI 16Kaiser Permanente, Vallejo, CA, 17OncoMed Pharmaceuticals, Redwood City, CA 18Prince of Wales Hospital, Sydney, Australia.
This was a randomized, double blind, 3 arm (1:1:1) study in subjects with 1st-line metastatic pancreatic ductal
adenocarcinoma. The study was designed to randomize pproximately two hundred and one patients via an
IWRS system. Patients were randomized to one of the following 3 arms:
Arm 1 – Abraxane® and gemcitabine plus placebo (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus placebo (3 cycles) and then Abraxane® and gemcitabine until disease
progression
Arm 2 - Abraxane® and gemcitabine plus demcizumab (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus placebo (3 cycles) and then Abraxane® and gemcitabine until disease
progression
Arm 3 - Abraxane® and gemcitabine plus demcizumab (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus demcizumab (3 cycles) and then Abraxane® and gemcitabine until disease
progression.
The primary efficacy analyses compared Arm 1 to Arms 2 and 3 combined. Efficacy analyses comparing Arm 1
to Arm 2 and Arm 3 separately were also performed. The primary endpoint of the study was a comparison the
Investigator-assessed PFS between Arm 1 and Arms 2 and 3 combined. Secondary endpoints included a
comparison of response, survival, safety, immunogenicity and biomarkers. Gemcitabine was given by IV
infusion at a dose of 1000 mg/m2 on Days 1, 8 and 15 of each 28-day treatment cycle (or until toxicity
necessitated reducing or holding a dose). Abraxane® was administered by IV infusion at a dose of 125 mg/m2
over 30 minutes on Days 1, 8 and 15 of each 28-day treatment cycle. Demcizumab 3.5 mg/kg or placebo was
administered by IV infusion (prior to the administration of Abraxane® and gemcitabine) once every 2 weeks for
either one (1st course through Study Day 70) or two (2nd course begun on Study Day 168 and continued
through Study Day 238) 70 day courses. Patients who had two consecutive B-type natriuretic (BNP) values
>100 pg/mL or one value >200 pg/mL were unblinded by the Investigator through the IWRS system and if they
were receiving demcizumab they were started on an ACE inhibitor or carvedilol. Subjects were assessed for
disease status every 8 weeks and for safety at every visit and through 30 days following the termination visit.
The data cut-off for this analysis was November 7, 2016.
USA/Canada Europe/Australia
≥ Dem (N=94)
≥ Placebo N=48)
Time (months
Pro
bab
ility
(%
)
Time (months
Time (months
≥ Dem (N=136)
≥ Placebo N=68)
≥ Dem (N=136)
≥ Placebo N=68)
Pro
ba
bili
ty (
%)
Pro
bab
ility
(%
)
Dem vs. Placebo
Hazard Ratio: 0.930
95% CI (0.630-1.375)
Log-Rank p-value 0.7158
Kaplan Meier Medians
Demcizumab: 5.52 (4.17-7.39) months
Placebo: 5.49 (3.81-7.36) months
Dem vs. Placebo
Hazard Ratio: 1.018
95% CI (0.616-1.683)
Log-Rank p-value 0.9443
Kaplan Meier Medians
Demcizumab: 13.2 (9.79-16.53) months
Placebo: NR (8.97-NR) months
Dem vs. Placebo
Hazard Ratio: 0.80
95% CI (0.453-1.416)
Log-Rank p-value 0.4432
Kaplan Meier Medians
Demcizumab: 13.96 (10.3-16.5) mos
Placebo: 9.89 (7.1-NR) mos
0 1
0 2
0 3
0
4
0
50
6
0 7
0 8
0 90
1
00
0 3 6 9 12 15 18 21
0
10
2
0
30
4
0
50
6
0
70
8
0
90
1
00
0
1
0
20
3
0
40
5
0
60
7
0
80
9
0
10
0
0 3 6 9 12 15 18 21
0 3 6 9 12 15 18
Related Adverse Events ≥ 15%
Overall Survival
Overall Survival by Region
Progression-Free Survival
There is accumulating evidence that the cell types within tumors are heterogeneous and that a
subset of the cells retain the property to self-renew and give rise to more differentiated progeny.
These cells, called Cancer Stem Cells (CSCs) or tumor initiating cells drive tumor growth and
metastasis and are more resistant to chemotherapy and radiotherapy than the remaining tumor cells.
The ability to characterize the CSCs through surface markers and functional limiting tumor dilution
assays, using minimally passaged human tumors, has enabled the identification of novel agents that
target the CSC population. One pathway which appears critical for the CSCs is the Notch pathway.
The pathway is comprised of 4 Notch receptors (1-4) and 5 ligands, Jagged (1-2) and delta-like
ligand (DLL1, 3 and 4). The DLL4 ligand contributes to CSC self-renewal and vascular
development. Demcizumab (DEM) is a humanized IgG2 antibody that binds to DLL4. In minimally
passaged human tumor xenografts, DEM was observed to have activity against a variety of tumors
including colorectal cancer, breast cancer, lung cancer, pancreatic cancer, melanoma and ovarian
cancer. The impact of treatment on the frequency of tumorigenicity was assessed using a limiting
dilution assay. In several models, using different chemotherapeutic agents, while the chemotherapy
alone decreased tumor volume, the frequency of tumor initiating cells was increased in the residual
tumor. In contrast, DEM alone decreased the frequency of CSCs and the greatest reduction was
observed when DEM was combined with GEM and nab-paclitaxel.
YOSEMITE: A 3 Arm Double-Blind Randomized Phase 2 Study of Gemcitabine, Paclitaxel Protein-Bound Particles for Injectable
Suspension (Abraxane®) and Placebo (GAP) versus Gemcitabine, Abraxane® and either 1 or 2 Truncated Courses of Demcizumab
Subject Disposition Placebo/
Placebo
Demcizumab/
Placebo
Demcizumab/
Demcizumab
Total
Intent to Treat 68 71 65 204
Safety Population 68 71 65 204
Ongoing 16 18 9 43
Discontinued 52 53 56 161
Reason for discontinuation
Progression
Death
AE
Withdraw Consent
Other Cancer Treatment
Investigator Decision
Other
34
5
3
0
0
2
8
28
4
5
4
0
5
7
34
3
5
1
1
2
10
96
12
13
5
1
9
25
RECIST Best Overall Response (n=204) Best Response Placebo/
Placebo
(N = 68)
Demcizumab
(N = 136)
P value
CR 0 1
PR 28 44
SD 20 56
PD 14 19
Response Rate (CR+PR) (95%
CI)
28 (41.2%) 45 (33.1%) 0.2815
Clinical Benefit (CR+PR+SD)
(95% CI)
48 (70.6%) 101 (74.3%) 0.5023
Conclusions •This was a randomized, double blind, 3 arm (1:1:1) study in subjects
with 1st-line metastatic pancreatic ductal adenocarcinoma.
•Two hundred and seven patients were randomized via an IWRS
system and 204 patients were treated.
•Patients were well balanced for the known prognostic factors between
the 3 treatment Arms.
•The efficacy outcomes were similar between Arm 1 vs. Arms 2 and 3
combined:
–Response rate: 41.2% vs 33.1% (p value = 0.2815)
–PFS: 5.49 mos. (95% CI:3.81-7.36) vs.5.52 mos.(95% CI:4.17-7.39) (HR = 0.93)
–OS: NR (95% CI:NR-8.97-NR) vs.13.24 mos.(95% CI: 9.79-16.53) (HR= 1.02)
• The efficacy outcomes were also similar when Arm 1 was compared
separately to Arm 2 and Arm 3.
•The most common AE’s in Arms 1, 2 and 3 respectively were:
–Nausea 61.8%, 53.5% and 63.1%
–Diarrhea 50.0%, 57.7% and 69.2%
–Anemia 39.7%, 60.6% and 53.8%
–Fatigue 50.0%. 43.7% and 56.9%
–Peripheral Edema 42.6% 54.9 and 52.9%
•The incidence of ≥ Grade 3 heart failure and pulmonary hypertension
were low and similar in all 3 treatment Arms. The incidence of ≥ Grade
3 bleeding was higher in the demcizumab arms.
–Heart Failure: 0/68 (0%), 4/71 (5.6%) and 1/65 (1.5%)
–Pulmonary Hypertension: 0/68 (0%), 1/71 (1.4%) and 0/65 (0%)
–Bleeding: 1/68 (1.5%), 7/ 71 (9.8%) and 4/65 (6.2%)
All Adverse Events ≥ 30%
Cancer Characteristics
Placebo/
Placebo
(N= 68)
Demcizumab/
Placebo
(N= 71)
Demcizumab/
Demcizumab
(N= 65)
Total
(N= 204)
ECOG PS
0
1
34
34
33
38
31
34
98
106
Region
US/Canada
Europe/Australia
20
48
23
48
19
46
62
142
CA 19-9
0-ULN
>ULN - < 59 X ULN
> = 59 X ULN
14
27
27
15
28
28
12
26
27
41
81
82
Background
Study Design Demographics
Placebo/
Placebo
(N= 68)
Demcizumab/
Placebo
(N= 71)
Demcizumab/
Demcizumab
(N= 65)
Total
(N= 204)
Age (Median) 62 63 66 63
Sex (M/F) 41/27 40/31 35/30 116/88
Number of Metastatic
Sites
0
1
2
3
> 3
1
27
23
12
5
0
26
24
18
3
1
23
28
8
5
2
76
75
38
13
Hepatic Metastases
Yes
No
72.1%
27.9%
74.6%
25.4%
75.4%
24.6%
74%
26%
NLR (Median) 3.2 3.8 3.4 3.5
Copies of this poster obtained through Quick Response (QR) code are for personal use only
and may not be reproduced without written permission from ASCO and the authors of this poster.
Study Schema
Primary Endpoint Secondary Endpoints Exploratory Endpoints
PFS
Survival Response
Safety
Biomarkers
Randomized: 207 pts Treated: 204 pts Data Cut: Nov 7, 2016
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Heart Failure
0 - 4 (5.6) 1 (1.5) 5 (2.5)
Pulmonary
Hypertension
0 - 1 (1.4) 0 - 1 (0.5)
Bleeding
1 (1.5) 7 (9.8) 4 (6.2) 12 (5.9)
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Nausea 42 ( 61.8) 38 ( 53.5) 41 ( 63.1) 121 ( 59.3)
Diarrhea 34 ( 50.0) 41 ( 57.7) 45 ( 69.2) 120 ( 58.8)
Anemia 27 ( 39.7) 43 ( 60.6) 35 ( 53.8) 105 ( 51.5)
Fatigue 34 ( 50.0) 31 ( 43.7) 37 ( 56.9) 102 ( 50.0)
Edema peripheral 29 ( 42.6) 39 ( 54.9) 34 ( 52.3) 102 ( 50.0)
Alopecia 30 ( 44.1) 33 ( 46.5) 28 ( 43.1) 91 ( 44.6)
Vomiting 27 ( 39.7) 32 ( 45.1) 25 ( 38.5) 84 ( 41.2)
Pyrexia 24 ( 35.3) 30 ( 42.3) 23 ( 35.4) 77 ( 37.7)
Decreased appetite
19 ( 27.9) 30 ( 42.3) 27 ( 41.5) 76 ( 37.3)
Neutropenia 21 ( 30.9) 24 ( 33.8) 25 ( 38.5) 70 ( 34.3)
Constipation 20 ( 29.4) 21 ( 29.6) 28 ( 43.1) 69 ( 33.8)
Abdominal pain 24 ( 35.3) 16 ( 22.5) 27 ( 41.5) 67 ( 32.8)
Asthenia 18 ( 26.5) 27 ( 38.0) 20 ( 30.8) 65 ( 31.9)
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Fatigue 22 ( 32.4) 20 ( 28.2) 27 ( 41.5) 69 ( 33.8)
Nausea 21 ( 30.9) 17 ( 23.9) 19 ( 29.2) 57 ( 27.9)
Anemia 15 ( 22.1) 19 ( 26.8) 17 ( 26.2) 51 ( 25.0)
Diarrhoea 10 ( 14.7) 18 ( 25.4) 22 ( 33.8) 50 ( 24.5)
Alopecia 12 ( 17.6) 16 ( 22.5) 13 ( 20.0) 41 ( 20.1)
Edema
peripheral 14 ( 20.6) 13 ( 18.3) 14 ( 21.5) 41 ( 20.1)
Vomiting 9 ( 13.2) 18 ( 25.4) 7 ( 10.8) 34 ( 16.7)
Asthenia 9 ( 13.2) 13 ( 18.3) 11 ( 16.9) 33 ( 16.2)
Decreased
appetite 5 ( 7.4) 16 ( 22.5) 11 ( 16.9) 32 ( 15.7)
Hypertension 6 ( 8.8) 11 ( 15.5) 12 ( 18.5) 29 ( 14.2)
Cubillo A1, Dean A2, Munoz A3, Hidalgo 1, Pazo Cid R4, Martin M5, Macarulla T6, Lipton L7, Harris M8, Manzano JL9, MaurelJ10, Gullen-Ponce C11, Tebbutt N12, Cooray P13, Sohal D14, Zalupski M15, Kolevska T16, Stagg R17, , Goldstein D18. 1Hospital Universitario HM Sanchinarro –
CIOCC, Madrid, 2St John of God Hospital Subiaco, Perth, 3Hospital General Universitario Gregorio Marañon, Madrid, 4Hospital Universitario Miguel Servet, Zaragoza, 5Hospital de La Santa Creu i Sant Pau, 6Vall d´Hebron University Hospital (HUVH) and Vall d’Hebron Institute of
Oncology (VHIO), Barcelona, 7Sunshine Hospital, Melbourne, 8Monash Medical Centre, Moorabbin Campus, 9Germans Trias i Pujol Hospital, ICO-Badalona, Barcelona, 10Hospital Clinic de Barcelona, Barcelona, 11Hospital Universitario Ramón y Cajal, Madrid, 12Austin Health,
Heidelberg, 13Box Hill Hospital, Melbourne, 14Cleveland Clinic, Cleveleand, OH, 15University of Michigan Cancer Center, Ann Arbor, MI 16Kaiser Permanente, Vallejo, CA, 17OncoMed Pharmaceuticals, Redwood City, CA 18Prince of Wales Hospital, Sydney, Australia.
This was a randomized, double blind, 3 arm (1:1:1) study in subjects with 1st-line metastatic pancreatic ductal
adenocarcinoma. The study was designed to randomize pproximately two hundred and one patients via an
IWRS system. Patients were randomized to one of the following 3 arms:
Arm 1 – Abraxane® and gemcitabine plus placebo (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus placebo (3 cycles) and then Abraxane® and gemcitabine until disease
progression
Arm 2 - Abraxane® and gemcitabine plus demcizumab (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus placebo (3 cycles) and then Abraxane® and gemcitabine until disease
progression
Arm 3 - Abraxane® and gemcitabine plus demcizumab (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus demcizumab (3 cycles) and then Abraxane® and gemcitabine until disease
progression.
The primary efficacy analyses compared Arm 1 to Arms 2 and 3 combined. Efficacy analyses comparing Arm 1
to Arm 2 and Arm 3 separately were also performed. The primary endpoint of the study was a comparison the
Investigator-assessed PFS between Arm 1 and Arms 2 and 3 combined. Secondary endpoints included a
comparison of response, survival, safety, immunogenicity and biomarkers. Gemcitabine was given by IV
infusion at a dose of 1000 mg/m2 on Days 1, 8 and 15 of each 28-day treatment cycle (or until toxicity
necessitated reducing or holding a dose). Abraxane® was administered by IV infusion at a dose of 125 mg/m2
over 30 minutes on Days 1, 8 and 15 of each 28-day treatment cycle. Demcizumab 3.5 mg/kg or placebo was
administered by IV infusion (prior to the administration of Abraxane® and gemcitabine) once every 2 weeks for
either one (1st course through Study Day 70) or two (2nd course begun on Study Day 168 and continued
through Study Day 238) 70 day courses. Patients who had two consecutive B-type natriuretic (BNP) values
>100 pg/mL or one value >200 pg/mL were unblinded by the Investigator through the IWRS system and if they
were receiving demcizumab they were started on an ACE inhibitor or carvedilol. Subjects were assessed for
disease status every 8 weeks and for safety at every visit and through 30 days following the termination visit.
The data cut-off for this analysis was November 7, 2016.
USA/Canada Europe/Australia
≥ Dem (N=94)
≥ Placebo N=48)
Time (months
Pro
ba
bili
ty (
%)
Time (months
Time (months
≥ Dem (N=136)
≥ Placebo N=68)
≥ Dem (N=136)
≥ Placebo N=68)
Pro
ba
bili
ty (
%)
Pro
bab
ility
(%
)
Dem vs. Placebo
Hazard Ratio: 0.930
95% CI (0.630-1.375)
Log-Rank p-value 0.7158
Kaplan Meier Medians
Demcizumab: 5.52 (4.17-7.39) months
Placebo: 5.49 (3.81-7.36) months
Dem vs. Placebo
Hazard Ratio: 1.018
95% CI (0.616-1.683)
Log-Rank p-value 0.9443
Kaplan Meier Medians
Demcizumab: 13.2 (9.79-16.53) months
Placebo: NR (8.97-NR) months
Dem vs. Placebo
Hazard Ratio: 0.80
95% CI (0.453-1.416)
Log-Rank p-value 0.4432
Kaplan Meier Medians
Demcizumab: 13.96 (10.3-16.5) mos
Placebo: 9.89 (7.1-NR) mos
0 1
0 2
0 3
0
4
0
50
6
0 7
0 8
0 90
1
00
0 3 6 9 12 15 18 21
0
10
2
0
30
4
0
50
6
0
70
8
0
90
1
00
0
1
0
20
3
0
40
5
0
60
7
0
80
9
0
10
0
0 3 6 9 12 15 18 21
0 3 6 9 12 15 18
Related Adverse Events ≥ 15%
Overall Survival
Overall Survival by Region
Progression-Free Survival
There is accumulating evidence that the cell types within tumors are heterogeneous and that a
subset of the cells retain the property to self-renew and give rise to more differentiated progeny.
These cells, called Cancer Stem Cells (CSCs) or tumor initiating cells drive tumor growth and
metastasis and are more resistant to chemotherapy and radiotherapy than the remaining tumor cells.
The ability to characterize the CSCs through surface markers and functional limiting tumor dilution
assays, using minimally passaged human tumors, has enabled the identification of novel agents that
target the CSC population. One pathway which appears critical for the CSCs is the Notch pathway.
The pathway is comprised of 4 Notch receptors (1-4) and 5 ligands, Jagged (1-2) and delta-like
ligand (DLL1, 3 and 4). The DLL4 ligand contributes to CSC self-renewal and vascular
development. Demcizumab (DEM) is a humanized IgG2 antibody that binds to DLL4. In minimally
passaged human tumor xenografts, DEM was observed to have activity against a variety of tumors
including colorectal cancer, breast cancer, lung cancer, pancreatic cancer, melanoma and ovarian
cancer. The impact of treatment on the frequency of tumorigenicity was assessed using a limiting
dilution assay. In several models, using different chemotherapeutic agents, while the chemotherapy
alone decreased tumor volume, the frequency of tumor initiating cells was increased in the residual
tumor. In contrast, DEM alone decreased the frequency of CSCs and the greatest reduction was
observed when DEM was combined with GEM and nab-paclitaxel.
YOSEMITE: A 3 Arm Double-Blind Randomized Phase 2 Study of Gemcitabine, Paclitaxel Protein-Bound Particles for Injectable
Suspension (Abraxane®) and Placebo (GAP) versus Gemcitabine, Abraxane® and either 1 or 2 Truncated Courses of Demcizumab
Subject Disposition Placebo/
Placebo
Demcizumab/
Placebo
Demcizumab/
Demcizumab
Total
Intent to Treat 68 71 65 204
Safety Population 68 71 65 204
Ongoing 16 18 9 43
Discontinued 52 53 56 161
Reason for discontinuation
Progression
Death
AE
Withdraw Consent
Other Cancer Treatment
Investigator Decision
Other
34
5
3
0
0
2
8
28
4
5
4
0
5
7
34
3
5
1
1
2
10
96
12
13
5
1
9
25
RECIST Best Overall Response (n=204) Best Response Placebo/
Placebo
(N = 68)
Demcizumab
(N = 136)
P value
CR 0 1
PR 28 44
SD 20 56
PD 14 19
Response Rate (CR+PR) (95%
CI)
28 (41.2%) 45 (33.1%) 0.2815
Clinical Benefit (CR+PR+SD)
(95% CI)
48 (70.6%) 101 (74.3%) 0.5023
Conclusions •This was a randomized, double blind, 3 arm (1:1:1) study in subjects
with 1st-line metastatic pancreatic ductal adenocarcinoma.
•Two hundred and seven patients were randomized via an IWRS
system and 204 patients were treated.
•Patients were well balanced for the known prognostic factors between
the 3 treatment Arms.
•The efficacy outcomes were similar between Arm 1 vs. Arms 2 and 3
combined:
–Response rate: 41.2% vs 33.1% (p value = 0.2815)
–PFS: 5.49 mos. (95% CI:3.81-7.36) vs.5.52 mos.(95% CI:4.17-7.39) (HR = 0.93)
–OS: NR (95% CI:NR-8.97-NR) vs.13.24 mos.(95% CI: 9.79-16.53) (HR= 1.02)
• The efficacy outcomes were also similar when Arm 1 was compared
separately to Arm 2 and Arm 3.
•The most common AE’s in Arms 1, 2 and 3 respectively were:
–Nausea 61.8%, 53.5% and 63.1%
–Diarrhea 50.0%, 57.7% and 69.2%
–Anemia 39.7%, 60.6% and 53.8%
–Fatigue 50.0%. 43.7% and 56.9%
–Peripheral Edema 42.6% 54.9 and 52.9%
•The incidence of ≥ Grade 3 heart failure and pulmonary hypertension
were low and similar in all 3 treatment Arms. The incidence of ≥ Grade
3 bleeding was higher in the demcizumab arms.
–Heart Failure: 0/68 (0%), 4/71 (5.6%) and 1/65 (1.5%)
–Pulmonary Hypertension: 0/68 (0%), 1/71 (1.4%) and 0/65 (0%)
–Bleeding: 1/68 (1.5%), 7/ 71 (9.8%) and 4/65 (6.2%)
All Adverse Events ≥ 30%
Cancer Characteristics
Placebo/
Placebo
(N= 68)
Demcizumab/
Placebo
(N= 71)
Demcizumab/
Demcizumab
(N= 65)
Total
(N= 204)
ECOG PS
0
1
34
34
33
38
31
34
98
106
Region
US/Canada
Europe/Australia
20
48
23
48
19
46
62
142
CA 19-9
0-ULN
>ULN - < 59 X ULN
> = 59 X ULN
14
27
27
15
28
28
12
26
27
41
81
82
Background
Study Design Demographics
Placebo/
Placebo
(N= 68)
Demcizumab/
Placebo
(N= 71)
Demcizumab/
Demcizumab
(N= 65)
Total
(N= 204)
Age (Median) 62 63 66 63
Sex (M/F) 41/27 40/31 35/30 116/88
Number of Metastatic
Sites
0
1
2
3
> 3
1
27
23
12
5
0
26
24
18
3
1
23
28
8
5
2
76
75
38
13
Hepatic Metastases
Yes
No
72.1%
27.9%
74.6%
25.4%
75.4%
24.6%
74%
26%
NLR (Median) 3.2 3.8 3.4 3.5
Copies of this poster obtained through Quick Response (QR) code are for personal use only
and may not be reproduced without written permission from ASCO and the authors of this poster.
Study Schema
Primary Endpoint Secondary Endpoints Exploratory Endpoints
PFS
Survival Response
Safety
Biomarkers
Randomized: 207 pts Treated: 204 pts Data Cut: Nov 7, 2016
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Heart Failure
0 - 4 (5.6) 1 (1.5) 5 (2.5)
Pulmonary
Hypertension
0 - 1 (1.4) 0 - 1 (0.5)
Bleeding
1 (1.5) 7 (9.8) 4 (6.2) 12 (5.9)
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Nausea 42 ( 61.8) 38 ( 53.5) 41 ( 63.1) 121 ( 59.3)
Diarrhea 34 ( 50.0) 41 ( 57.7) 45 ( 69.2) 120 ( 58.8)
Anemia 27 ( 39.7) 43 ( 60.6) 35 ( 53.8) 105 ( 51.5)
Fatigue 34 ( 50.0) 31 ( 43.7) 37 ( 56.9) 102 ( 50.0)
Edema peripheral 29 ( 42.6) 39 ( 54.9) 34 ( 52.3) 102 ( 50.0)
Alopecia 30 ( 44.1) 33 ( 46.5) 28 ( 43.1) 91 ( 44.6)
Vomiting 27 ( 39.7) 32 ( 45.1) 25 ( 38.5) 84 ( 41.2)
Pyrexia 24 ( 35.3) 30 ( 42.3) 23 ( 35.4) 77 ( 37.7)
Decreased appetite
19 ( 27.9) 30 ( 42.3) 27 ( 41.5) 76 ( 37.3)
Neutropenia 21 ( 30.9) 24 ( 33.8) 25 ( 38.5) 70 ( 34.3)
Constipation 20 ( 29.4) 21 ( 29.6) 28 ( 43.1) 69 ( 33.8)
Abdominal pain 24 ( 35.3) 16 ( 22.5) 27 ( 41.5) 67 ( 32.8)
Asthenia 18 ( 26.5) 27 ( 38.0) 20 ( 30.8) 65 ( 31.9)
Placebo/
Placebo
(N=68)
Demcizumab/
Placebo
(N=71)
Demcizumab/
Demcizumab
(N=65)
Total
(N=204)
Fatigue 22 ( 32.4) 20 ( 28.2) 27 ( 41.5) 69 ( 33.8)
Nausea 21 ( 30.9) 17 ( 23.9) 19 ( 29.2) 57 ( 27.9)
Anemia 15 ( 22.1) 19 ( 26.8) 17 ( 26.2) 51 ( 25.0)
Diarrhoea 10 ( 14.7) 18 ( 25.4) 22 ( 33.8) 50 ( 24.5)
Alopecia 12 ( 17.6) 16 ( 22.5) 13 ( 20.0) 41 ( 20.1)
Edema
peripheral 14 ( 20.6) 13 ( 18.3) 14 ( 21.5) 41 ( 20.1)
Vomiting 9 ( 13.2) 18 ( 25.4) 7 ( 10.8) 34 ( 16.7)
Asthenia 9 ( 13.2) 13 ( 18.3) 11 ( 16.9) 33 ( 16.2)
Decreased
appetite 5 ( 7.4) 16 ( 22.5) 11 ( 16.9) 32 ( 15.7)
Hypertension 6 ( 8.8) 11 ( 15.5) 12 ( 18.5) 29 ( 14.2)
Cubillo A1, Dean A2, Munoz A3, Hidalgo 1, Pazo Cid R4, Martin M5, Macarulla T6, Lipton L7, Harris M8, Manzano JL9, MaurelJ10, Gullen-Ponce C11, Tebbutt N12, Cooray P13, Sohal D14, Zalupski M15, Kolevska T16, Stagg R17, , Goldstein D18. 1Hospital Universitario HM Sanchinarro –
CIOCC, Madrid, 2St John of God Hospital Subiaco, Perth, 3Hospital General Universitario Gregorio Marañon, Madrid, 4Hospital Universitario Miguel Servet, Zaragoza, 5Hospital de La Santa Creu i Sant Pau, 6Vall d´Hebron University Hospital (HUVH) and Vall d’Hebron Institute of
Oncology (VHIO), Barcelona, 7Sunshine Hospital, Melbourne, 8Monash Medical Centre, Moorabbin Campus, 9Germans Trias i Pujol Hospital, ICO-Badalona, Barcelona, 10Hospital Clinic de Barcelona, Barcelona, 11Hospital Universitario Ramón y Cajal, Madrid, 12Austin Health,
Heidelberg, 13Box Hill Hospital, Melbourne, 14Cleveland Clinic, Cleveleand, OH, 15University of Michigan Cancer Center, Ann Arbor, MI 16Kaiser Permanente, Vallejo, CA, 17OncoMed Pharmaceuticals, Redwood City, CA 18Prince of Wales Hospital, Sydney, Australia.
This was a randomized, double blind, 3 arm (1:1:1) study in subjects with 1st-line metastatic pancreatic ductal
adenocarcinoma. The study was designed to randomize pproximately two hundred and one patients via an
IWRS system. Patients were randomized to one of the following 3 arms:
Arm 1 – Abraxane® and gemcitabine plus placebo (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus placebo (3 cycles) and then Abraxane® and gemcitabine until disease
progression
Arm 2 - Abraxane® and gemcitabine plus demcizumab (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus placebo (3 cycles) and then Abraxane® and gemcitabine until disease
progression
Arm 3 - Abraxane® and gemcitabine plus demcizumab (3 cycles), Abraxane® and gemcitabine (3 cycles),
Abraxane® and gemcitabine plus demcizumab (3 cycles) and then Abraxane® and gemcitabine until disease
progression.
The primary efficacy analyses compared Arm 1 to Arms 2 and 3 combined. Efficacy analyses comparing Arm 1
to Arm 2 and Arm 3 separately were also performed. The primary endpoint of the study was a comparison the
Investigator-assessed PFS between Arm 1 and Arms 2 and 3 combined. Secondary endpoints included a
comparison of response, survival, safety, immunogenicity and biomarkers. Gemcitabine was given by IV
infusion at a dose of 1000 mg/m2 on Days 1, 8 and 15 of each 28-day treatment cycle (or until toxicity
necessitated reducing or holding a dose). Abraxane® was administered by IV infusion at a dose of 125 mg/m2
over 30 minutes on Days 1, 8 and 15 of each 28-day treatment cycle. Demcizumab 3.5 mg/kg or placebo was
administered by IV infusion (prior to the administration of Abraxane® and gemcitabine) once every 2 weeks for
either one (1st course through Study Day 70) or two (2nd course begun on Study Day 168 and continued
through Study Day 238) 70 day courses. Patients who had two consecutive B-type natriuretic (BNP) values
>100 pg/mL or one value >200 pg/mL were unblinded by the Investigator through the IWRS system and if they
were receiving demcizumab they were started on an ACE inhibitor or carvedilol. Subjects were assessed for
disease status every 8 weeks and for safety at every visit and through 30 days following the termination visit.
The data cut-off for this analysis was November 7, 2016.
USA/Canada Europe/Australia
≥ Dem (N=94)
≥ Placebo N=48)
Time (months
Pro
ba
bili
ty (
%)
Time (months
Time (months
≥ Dem (N=136)
≥ Placebo N=68)
≥ Dem (N=136)
≥ Placebo N=68)
Pro
ba
bili
ty (
%)
Pro
bab
ility
(%
)
Dem vs. Placebo
Hazard Ratio: 0.930
95% CI (0.630-1.375)
Log-Rank p-value 0.7158
Kaplan Meier Medians
Demcizumab: 5.52 (4.17-7.39) months
Placebo: 5.49 (3.81-7.36) months
Dem vs. Placebo
Hazard Ratio: 1.018
95% CI (0.616-1.683)
Log-Rank p-value 0.9443
Kaplan Meier Medians
Demcizumab: 13.2 (9.79-16.53) months
Placebo: NR (8.97-NR) months
Dem vs. Placebo
Hazard Ratio: 0.80
95% CI (0.453-1.416)
Log-Rank p-value 0.4432
Kaplan Meier Medians
Demcizumab: 13.96 (10.3-16.5) mos
Placebo: 9.89 (7.1-NR) mos
0 1
0 2
0 3
0
4
0
50
6
0 7
0 8
0 90
1
00
0 3 6 9 12 15 18 21
0
10
2
0
30
4
0
50
6
0
70
8
0
90
1
00
0
1
0
20
3
0
40
5
0
60
7
0
80
9
0
10
0
0 3 6 9 12 15 18 21
0 3 6 9 12 15 18
LAPACT G-NABP response rate: 31%

FRAGANCE (ECOG 2) ESMO 2017
Hidalgo et al. ESMO 2017

Outcome of Second-Line Treatment MPACT trial
Outcome of Second-Line Treatment Following nab-Paclitaxel + Gemcitabine
or Gemcitabine Alone for Metastatic Pancreatic Cancer
David Goldstein,1 E. Gabriela Chiorean,2 Josef Tabernero,3 Robert El-Maraghi,4 Wen Wee Ma,5 Michele Reni,6 Marian Harris,7 Robert Whorf,8 Jack Shiansong Li,9 Victoria Manax,9 Brian Lu,9 Alfredo Romano,9 Daniel D. Von Hoff10
1Prince of Wales Hospital, Sydney, Australia; 2University of Washington, Seattle, WA; 3Vall d'Hebron Institute of Oncology (VHIO), Barcelona, Spain; 4Simcoe Muskoka Regional Cancer Centre, Barrie, ON, Canada; 5Roswell Park Cancer Institute, Buffalo, NY; 6Ospedale San Raffaele, Milan, Italy; 7Dana-Farber Cancer Institute, Boston, MA; 8Florida Cancer Specialists, Bradenton, FL; 9Celgene Corporation, Summit, NJ; 10Translational Genomics Research Institute and HonorHealth, Scottsdale, AZ
INTRODUCTION
Abstract 333
• PC is a highly lethal malignancy, and mortality rates nearly equal incidence1
- ≥ 80% of pts are diagnosed with advanced disease (53% with metastatic
disease)2
• Over the past decade, treatment plans for most pts with MPC have consisted
predominantly of 1 line of therapy3,4
- This may be due, in part, to the aggressive nature of the disease4
- Improvements in 1L efficacy may permit the use of subsequent therapy
• nab®-Paclitaxel (nab-P) + Gem demonstrated superior efficacy vs Gem alone for all
endpoints examined in a phase III MPC trial, including OS, the primary endpoint
(median, 8.7 vs 6.6 mo; P < 0.001)5,6
• Feasibility and efficacy data are needed to guide 2L treatment decisions in MPC
• As nab-P + Gem has become a standard 1L therapeutic option for pts with MPC,3
an analysis of the regimen as part of a treatment plan is necessary
nab® is a registered trademark of Celgene Corporation.
• The current post hoc analysis investigated the feasibility and efficacy of 2L therapy
among pts from the MPACT trial
OBJECTIVE
STUDY DESIGN
• In the phase III trial, pts received nab-P + Gem or Gem alone as 1L treatment as
previously described5
- Pts were treated until disease progression, unacceptable toxicity, or pt or
physician decision
- Pts were followed until discontinuation of 1L therapy, after which only dates and
type of subsequent treatment(s) as well as date of death were collected
• After the closure of the MPACT trial (NCT00844649) in 2013, an observational
extension study was initiated to gather more survival information on pts who were
still alive (NCT02021500).
- The data collected from the extension study is included in this post hoc
evaluation
• The Kaplan-Meier method was used to calculate OS:
- Total OS: from initial randomization
- OS2: survival time from end of 1L therapy
• Multivariate analyses of total OS and OS2 were conducted using a Cox proportional
hazard model to evaluate 1L treatment and use of 2L therapy adjusted for other
prognostic factors (at the end of 1L treatment for OS2); a stepwise procedure was
performed to evaluate the treatment effect and identify the possible factors
associated with OS or OS2
- Total OS: In addition to 1L and 2L treatment effect, the potential influence of the
following prognostic factors was assessed:
Geographic region (North America and other), age, KPS, NLR, PC primary
location, stage at diagnosis, CA19-9 level, presence of liver metastases,
peritoneal carcinomatosis, previous Whipple procedure, presence of biliary
stent, presence of pulmonary metastases, number of metastatic sites
- OS2: The potential influence of the following factors was assessed:
Prognostic factors at baseline: geographic region (North America and
other) and number of metastatic sites
Factors at the end of 1L treatment: age, KPS, NLR, 1L PFS (≥ median and
< median)
RESULTS
Patients
• ≥ 40% of pts in each treatment arm received a 2L therapy (Table 1A)
• 5-FU or cape-containing regimens were the most common 2L therapies (> 75%;
Tables 1A and 1B)
• Pts who received 2L treatment had a better performance status at baseline
compared with those who did not receive 2L treatment (Table 1A)
• Pts treated with FOLFIRINOX as 2L therapy had better performance status at the
end of 1L treatment compared with all other regimens (Tables 2A and 2B)
1L, first-line; 2L, second-line; 5-FU, 5-fluorouracil; CA19-9, carbohydrate antigen 19-9; Cape, capecitabine; ECOG PS,
Eastern Cooperative Oncology Group performance status; FOLFIRINOX, leucovorin, 5-FU, irinotecan, oxaliplatin;
FOLFOX/OFF, leucovorin, 5-FU, oxaliplatin; Gem, gemcitabine; ITT, intent to treat; KPS, Karnofsky performance status; met,
metastatic; MPC, metastatic pancreatic cancer; nab-P, nab-paclitaxel; NLR, neutrophil-to-lymphocyte ratio; OS, overall
survival; PFS, progression-free survival; PFS1, progression-free survival during 1L treatment; PS, performance status; pt,
patient; PC, pancreatic cancer; ULN, upper limit of normal.
Variable
ITT Any 2L Therapy No 2L Therapy5-FU- or Cape-
Containing
nab-P
+ GemGem
nab-P
+ GemGem
nab-P
+ GemGem
nab-P
+ GemGem
n 431 430 170 177 261 253 132 135
Age, median, y 62.0 63.0 61.0 62.0 63.0 64.0 59.5 62.0
KPS, %
90 - 100
70 - 80
58
42
62
38
68
32
75
25
51
49
54
46
64
36
76
24
CA19-9
median, U/mL
≥ 59 × ULN, %
n = 379
2294
52
n = 371
2759
53
n = 152
2644
49
n = 162
2096
46
n = 227
1951
43
n = 209
3664
45
n = 120
2637
51
n = 125
2172
47
No. met. sites, %
1 - 3
> 3
86
14
85
15
88
12
88
12
85
15
84
16
88
12
89
11
NLR, %
≥ 5
> 5
n = 426
62
38
n = 426
65
35
75
25
73
27
55
45
60
40
74
26
72
28
Variable
5-FU or Cape Comboa FOLFIRINOX FOLFOX/OFF
nab-P +
GemGem
nab-P +
GemGem
nab-P +
GemGem
n 98 107 18 17 36 49
Age, median, y 59.0 62.0 53.5 56.0 58.5 64.0
KPS, %
90 - 100
70 - 80
67
33
76
24
72
28
76
24
53
47
67
33
CA19-9
median, U/mL
≥ 59 × ULN, %
n = 90
2601
51
n = 100
2206
48
n = 16
5539
56
n = 17
2368
53
n = 33
2650
53
n = 43
2005
43
No. met. sites, %
1 - 3
> 3
91
9
93
7
100
0
88
12
86
14
92
8
NLR, %
≥ 5
> 5
75
25
70
30
72
28
71
29
78
22
69
31
a 3 pts (2 in the nab-P + Gem arm and 1 in the Gem arm) received 2L FOLFIRI treatment.
Table 1A. Baseline Characteristics by 2L Therapy Received
Table 1B. Baseline Characteristics for Pts who Received 2L 5-FU- or
Cape-Containing Combinations
Reasons for 1L Treatment Discontinuation
• Pts with any 2L treatment: 59% and 74% in the nab-P + Gem and Gem-alone arms,
respectively, discontinued 1L therapy due to progressive disease
- 26% and 14% discontinued 1L therapy due to adverse events
Efficacy
• Pts with any 2L treatment: Total OS (from initial randomization) was significantly
longer with nab-P + Gem vs Gem (median, 12.8 vs 9.9 mo.; P = 0.015; Figure 1)
- Without 2L therapy: longer for nab-P + Gem (median, 6.2 vs 4.7 mo; HR 0.69;
P < 0.001)
• Pts who received a 5-FU- or cape-containing 2L therapy: Total OS was significantly
longer for those in the nab-P + Gem vs Gem-alone arms (median, 13.5 vs 9.5 mo; P
= 0.012)
• In the nab-P + Gem and Gem-alone arms, fewer pts received 5-FU or cape mono-
than combination therapy (34 vs 98 pts and 28 vs 107 pts, respectively)
- Fewer pts who received 5-FU or cape monotherapy had KPS 90 -100 (32%
and 36% for nab-P + Gem and Gem alone, respectively) compared with those
who received 5-FU or cape combination therapy (Table 2B)
• OS2 (from end of 1L therapy) for nab-P + Gem vs Gem alone
- With 2L therapy: median OS similar (6.7 vs 6.4 mo; P = 0.273; Figure 2)
- Without 2L therapy: longer for nab-P + Gem (median, 2.5 vs 1.6 mo; HR 0.67;
P < 0.001)
Variable
Any 2L Therapy No 2L Therapy5-FU-or Cape-
Containing
nab-P +
GemGem
nab-P +
GemGem
nab-P +
GemGem
n 170 177 261 253 132 135
Age, median, y 61.8 62.5 63.6 65.2 60.4 62.5
KPS, %
90 - 100
80
70
≥ 60
43
37
11
9
n = 176
48
34
10
8
n = 240
26
28
20
27
n = 222
22
32
19
27
43
38
8
11
45
35
12
8
CA19-9
median, U/mL
≥ 59 × ULN, %
n = 144
276
26
n = 131
380
32
n = 170
263
29
n = 121
1669
45
n = 112
276
28
n = 99
514
33
NLR
≥ 5 , % 74
n = 176
67
n = 236
59
n = 215
45 77 64
Variable
5-FU or Cape
Comboa FOLFIRINOX FOLFOX/OFF
nab-P +
GemGem
nab-P +
GemGem
nab-P +
GemGem
n 98 107 18 17 36 49
Age, median, y 59.8 62.5 54.4 56.2 59.5 64.7
KPS, %
90 - 100
80
70
≥ 60
47
38
6
9
48
35
11
7
50
39
6
6
59
12
29
0
44
31
6
19
35
51
10
4
CA19-9
median, U/mL
≥ 59 × ULN, %
n = 84
241
27
n = 76
547
33
n = 16
195
19
n = 10
401
20
n = 32
398
28
n = 33
261
30
NLR ≥ 5 , % 77 65 72 71 69 63
a Three pts (2 in the nab-P + Gem arm and 1 in the Gem arm) received 2L FOLFIRI treatment.
Table 2A. Pt Characteristics at End of 1L Treatment
Table 2B. Pt Characteristics at End of 1L Treatment for Pts who
Received 2L 5-FU- or Cape-Containing Combinations
Poster presented at the 2016 Gastrointestinal Cancers Symposium; January 21-23, 2016; San Francisco, CA
Figure 1. Total OS in Pts Who Received 2L Therapy
Events/nMedian, mo (95%
CI)
161/170 12.8 (10.9 - 14.2)
166/177 9.9 (8.9 - 10.9)
Pro
po
rtio
n o
f S
urv
iva
l
Time, monthsPts at risk
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
177Gem: 174 139 101 63 39 28 21 16 9 8 6 4 2 1 1 0 0
170 165 149 117 87 60 36 29 22 17 13 10 8 4 3 2 2 0nab-P
+ Gem:
HR 0.76
95% CI, 0.61 - 0.95
P = 0.015
Gem
nab-P + Gem
Events/nMedian, mo (95%
CI)
161/170 6.7 (6.1 - 7.9)
166/177 6.4 (5.3 - 7.7)
Figure 2. OS2 From End of 1L Therapy
Time, months
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Pro
po
rtio
n o
f S
urv
iva
l
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pts at risk
177 142 91 56 32 21 14 9 5 5 4 3 1 1 1 0 0 0Gem:
170 149 98 61 39 24 17 13 10 6 4 4 4 2 2 1 1 0nab-P
+ Gem:
HR 0.89
95% CI, 0.71 - 1.10
P = 0.273
Gem
nab-P + Gem
Covariate HR (95% CI) P value
Treatment group (nab-P + Gem vs Gem alone) 0.73 (0.63 - 0.85) < 0.001
2L therapy (with vs without) 0.47 (0.40 - 0.54) < 0.001
NLR at end of 1L (≥ 5 vs > 5) 0.60 (0.52 - 0.70) < 0.001
KPS at end of 1L
90 -100 vs ≥ 60
70 -80 vs ≥ 60
0.46 (0.37 - 0.57)
0.57 (0.47 - 0.70)
< 0.001
< 0.001
PFS, mo (≥ 4.4 vs < 4.4)a 0.78 (0.67 - 0.91) 0.002
Geographic region (North America vs others) 0.86 (0.74 - 1.00) 0.051
a In this study, the median PFS for the entire ITT population was 4.4 mo.
Table 3. Multivariate Analysis of OS2
Efficacy (continued)
• Factors significantly associated with longer total OS by multivariate analysis
include 1L treatment with nab-P + Gem vs Gem alone, use of 2L therapy, better
KPS at baseline (90 - 100 vs 70 -80), no liver metastases, baseline NLR ≥ 5 vs
> 5 (P < 0.001 for each), and lower CA19-9 at baseline (P = 0.005)
• Factors significantly associated with longer OS2 by multivariate analysis (Table
3) include 1L treatment with nab-P + Gem vs Gem alone, use of 2L therapy, NLR
≥ 5 vs > 5 at end of 1L therapy, better KPS at end of 1L therapy (P < 0.001 for
each), and PFS1 ≥ 4.4 mo vs < 4.4 mo (P = 0.002)
• The longest total OS values were for pts who received 1L nab-P + Gem and 2L
treatment with FOLFIRINOX (median OS, 15.7 mo; Table 4)
This study is supported by Celgene Corporation, Summit, NJ. The authors received editorial and production support in the
preparation of this poster from MediTech Media, Ltd, funded by Celgene Corporation. The authors are fully responsible for all
content and editorial decisions for this poster.
ACKNOWLEDGMENTS
DISCLOSURES
REFERENCES
Dr. David Goldstein - [email protected]
CORRESPONDENCE
CONCLUSIONS
• 2L treatment was feasible and beneficial for pts with MPC, with greater benefit
observed for those who received 1L nab-P + Gem vs Gem alone
• A limitation of this study is that no information was available about treatment
schedule or dose, safety, or efficacy (beyond survival) during 2L therapy
• Receiving 2L therapy was significantly associated with longer total OS, even after
adjusting for baseline characteristics
• 1L therapy may play a role in achieving optimal treatment benefit
- Total OS was significantly longer among pts who received 2L 5-FU– or cape-
containing therapies following 1L nab-P + Gem vs Gem alone
• Pts most likely to benefit from additional therapy include those with a longer PFS
during 1L treatment and lower NLR and better PS at the end of 1L treatment
• The current analysis supports the use of nab-P + Gem as an appropriate 1L therapy
onto which a treatment plan can be built
1. World Health Organization. GLOBOCAN 2012: Estimated cancer incidence, mortality,
and prevalence worldwide in 2012.
http://globocan.iarc.fr/Pages/fact_sheets_population.aspx. Accessed December 8, 2015.
2. Surveillance, Epidemiology, and End Results Program. SEER stat facts sheets: pancreas
cancer. http://seer.cancer.gov/statfacts/html/pancreas.html. Updated 2015. Accessed
December 8, 2015.
3. Abrams TA, et al. J Clin Oncol. 2014;32:(5 suppl) [abstract 4131].
4. Smyth EN, et al. Clin Ther. 2015;37:1301-1316.
5. Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703.
6. Goldstein D, et al. J Natl Cancer Inst. 2015;107(2).
Copies of this poster obtained through Quick Response (QR) Code are for
personal use only and may not be reproduced without permission from ASCO®
and the author of this poster.
DG: research funding, Celgene, Pfizer; consultant or advisory role (unremunerated), Celgene, Pfizer; EGC: research funding,
consultant or advisory role, Celgene; JT: consultant or advisory role, honoraria, Celgene; RE-M: consultant or advisory role, research
funding, Celgene; WWM: research funding, Celgene; MR: consultant or advisory role, honoraria, research funding, Celgene; MH:
nothing to disclose; RW: nothing to disclose; SC: stock ownership, Celgene; JSL, VM, BL, AR: employment, stock ownership,
Celgene; DDVH: consultant or advisory role, honoraria, Celgene; research funding, HonorHealth
Table 4. Survival Outcome Summary in Pts Who Received 2L Therapy
Variable n (%)
Median Duration, mo
OS
From 1L
Randomization to
First Dose of 2L Tx
From First Dose
of 2L Tx to Death
Any 2L therapy
nab-P + Gem
Gem
170 (39)
177 (41)
12.8
9.9
6.6
4.1
5.3
4.5
Othera
nab-P + Gem
Gem
38 (22)
42 (24)
10.9
11.3
6.3
4.5
3.2
4.8
5-FU- or Cape-Containing
nab-P + Gem
Gem
132 (78)
135 (76)
13.5
9.5
6.7
4.1
5.7
4.5
5-FU or Cape combo
nab-P + Gem
Gem
98 (58)
107 (60)
14.0
9.5
6.6
4.0
6.0
4.6
5-FU or Cape mono
nab-P + Gem
Gem
34 (20)
28 (16)
11.9
9.4
6.7
5.3
4.7
3.9
FOLFIRINOX
nab-P + Gem
Gem
18 (11)
17 (10)
15.7
7.2
8.4
4.0
7.2
3.5
FOLFOX/OFF
nab-P + Gem
Gem
36 (21)
49 (28)
13.7
9.8
5.6
4.1
6.4
4.5a Other than 5-FU- or Cape-containing Tx; median total OS for 1L Gem followed by 2L nab-P + Gem (n = 7) or nab-P
alone (n = 11) was 7.9 and 8.8 mo, respectively.
Choirean et al. Br J Cancer 2016

1516 1184 46 24 14 3 1 11
OFF vs FF as 2nd-line therapy for APC*
(CONKO-003)
OFF†
FF
Stratification: Presence of metastases, duration of 1st-line gemcitabine therapy (3, 3–6, or >6 months), KPS (70–80% or 90–
100%)
Primary endpoint: OS
Secondary endpoints: TTP, tolerability
• PD following gemcitabine 1st-line therapy
• KPS ≥70
• Measureable disease
100
80
60
20
0
40
Time (months)860 3 12 15 24 27 38336 9 18 21 30
076 34 6 5 1 1 0114 7 5 3 1184 20 3 3 2 2 129 7 2 2 2FF
OFFNo at risk
100
80
60
20
0
40
Time (months)No at risk
48189 120 3 6 3624 30 42 8654
FFOFF 21022 1576 59 37 46 5 3 01
Ove
rall
su
rviv
al (%
)P
rog
ressio
n-f
ree
su
rviv
al (
%)
OFF median 2.9 months (95% CI 2.4–3.2)
FF median 2.0 months (95% CI 1.6–2.3)
HR 0.68 (95% CI 0.50–0.94) p=0.019
OFF median 5.9 months (95% CI 4.1–7.4)
FF median 3.3 months (95% CI 2.7–4.0)
HR 0.66 (95% CI 0.48–0.91) p=0.010
R 1:1
Oettle et al. JCO 2014;32:2423-9
*>88% of patients had metastatic disease†OFF differs from FOLFOX (folinic acid, fluorouracil, and oxaliplatin) with respect to the
frequency of treatment administration: fluorouracil is administered weekly for the first 4 weeks,
and oxaliplatin is administered on Days 8 and 22 of a 6-week cycle
2ªL Oxaliplatino

mFOLFOX6 as 2nd-line therapy for MPC
(PANCREOX)
201 4 8 12 16
Times (months)
0
0.5
1.0
Ove
rall
su
rviv
al p
rob
ab
ility
mFOLFOX6
(n=54)
5-FU/LV
(n=54)
Median, mo 6.1 9.9
95% CI 3.2–8.0 6.7–16.9
HR (95% CI) 1.78 (1.08–2.93)
p value 0.024
= Canadian, multicentre, open-label trial
= 108 patients with APC previously treated with
gemcitabine-based therapy randomized to receive:
– mFOLFOX6
– 5-FU/LV
= No difference in PFS between treatment arms
– 3.1 vs 2.9 months
= Inferior OS with mFOLFOX6
– 6.1 vs 9.9 months
= mFOLFOX6 associated with more treatment-related
Grade 3/4 AEs
– 63% vs 11%
mFOLFOX6
5-FU/LV
Gill et al. JCO 2014;32(suppl):4022
2ªL Oxaliplatino
Gill et al. JCO 2016

NAPOLI-1: Study Design

NAPOLI-1: Efficacy results
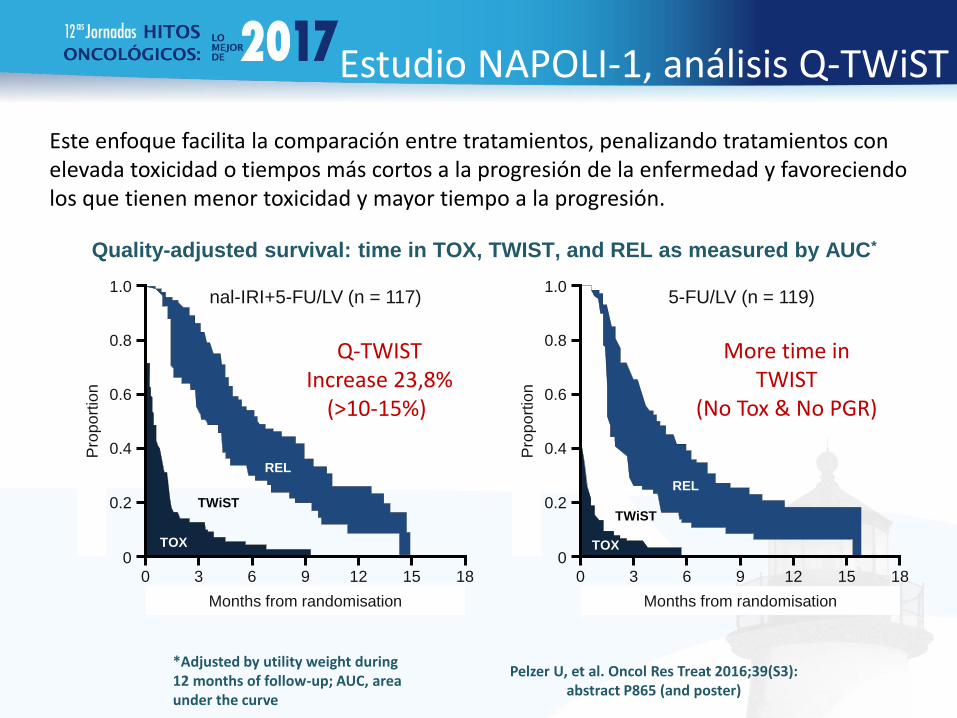
Este enfoque facilita la comparación entre tratamientos, penalizando tratamientos con elevada toxicidad o tiempos más cortos a la progresión de la enfermedad y favoreciendo los que tienen menor toxicidad y mayor tiempo a la progresión.
*Adjusted by utility weight during 12 months of follow-up; AUC, area under the curve
Pelzer U, et al. Oncol Res Treat 2016;39(S3): abstract P865 (and poster)
nal-IRI+5-FU/LV (n = 117) 5-FU/LV (n = 119)
Quality-adjusted survival: time in TOX, TWIST, and REL as measured by AUC*
Months from randomisation
Pro
po
rtio
n
0
0.2
0.4
0.6
1.0
0.8
0 3 6 9 12 18 15
REL
TWiST
TOX
Months from randomisation
Pro
po
rtio
n
0
0.2
0.4
0.6
1.0
0.8
0 3 6 9 12 18 15
REL
TWiST
TOX
Estudio NAPOLI-1, análisis Q-TWiST
Q-TWIST Increase 23,8%
(>10-15%)
More time in TWIST
(No Tox & No PGR)

Comparación de estudios (1)

Comparación de estudios (2)

Sonbol et al. Cancer 2017
PFS
FPIRI vs. FP: HR 0.64; 95%CI, 0.47-0.87; p=0.005
FPOX vs. FP: HR 0.81; 95%CI, 0.67-0.97; p=0.02
5 trials, 895 patients FPIRI: irinotecan formulations

Sonbol et al. Cancer 2017
OS
FPIRI vs. FP: HR 0.70; 95%CI, 0.55-0.89; p=0.004
FPOX vs. FP: HR 1.03; 95%CI, 0.64-1.67; p=0.9
5 trials, 895 patients

Potential treatment sequencing approach for MPC in 2017?
Nab-paclitaxel + gemcitabine
(if no neuropathy)
GemcitabineFOLFIRINOX
Nab-paclitaxel + gemcitabine
MM-398 + 5-FU/LV
OFF
Capecitabine
MM-398 + 5-FU/LV(depending on
prior exposure)
1st line
2nd line
3rd line
NOTE: Nab-paclitaxel is licensed for use in combination with gemcitabine as
1st-line therapy for patients with MPC
Nab-paclitaxel?(depending on
prior exposure)
mFOLFOX6 or CAPOX
Platinum-based tx(depending on
prior exposure)
Supported by RCT data
Supported by retrospective data or small, single arm trials
5-FU
No prospective randomized trial of 2L therapy after FOLFIRINOX providing risk/benefit ratio:

Designing a continuum of care in MPC
= 2nd-line MM-398 + 5-FU/LV provides a break from neurotoxicity, paving the way for subsequent 3rd-line treatment
= Prior exposure to irinotecan (with 1st-line FOLFIRINOX) could increase the potential for resistance to 2nd-line MM-398
1st line 2nd line 3rd line
Nab-paclitaxel +
gemcitabine
8.7 m
MM-398+
5-FU/LV
6.1 m
FOLFOX/OFF
Oettle & Lehmann, Lancet2016;387:507-8

Guía ASCO 2014
Recommendations
1. There are no agents recommended for the prevention of
CIPN
2. Treatment of existing CIPN, the best available data
support a moderate recommendation for treatment with
duloxetine
Loprinzi, Practice Update 2013: “The benefit from duloxetine, however, was not a home run; duloxetine decreased pain, more than was associated with the placebo, by 1 point on a 0-to-10 point scale”

Estudios observacionales retrospectivos de secuenciación

Outcome of Second-Line Treatment MPACT trial
Outcome of Second-Line Treatment Following nab-Paclitaxel + Gemcitabine
or Gemcitabine Alone for Metastatic Pancreatic Cancer
David Goldstein,1 E. Gabriela Chiorean,2 Josef Tabernero,3 Robert El-Maraghi,4 Wen Wee Ma,5 Michele Reni,6 Marian Harris,7 Robert Whorf,8 Jack Shiansong Li,9 Victoria Manax,9 Brian Lu,9 Alfredo Romano,9 Daniel D. Von Hoff10
1Prince of Wales Hospital, Sydney, Australia; 2University of Washington, Seattle, WA; 3Vall d'Hebron Institute of Oncology (VHIO), Barcelona, Spain; 4Simcoe Muskoka Regional Cancer Centre, Barrie, ON, Canada; 5Roswell Park Cancer Institute, Buffalo, NY; 6Ospedale San Raffaele, Milan, Italy; 7Dana-Farber Cancer Institute, Boston, MA; 8Florida Cancer Specialists, Bradenton, FL; 9Celgene Corporation, Summit, NJ; 10Translational Genomics Research Institute and HonorHealth, Scottsdale, AZ
INTRODUCTION
Abstract 333
• PC is a highly lethal malignancy, and mortality rates nearly equal incidence1
- ≥ 80% of pts are diagnosed with advanced disease (53% with metastatic
disease)2
• Over the past decade, treatment plans for most pts with MPC have consisted
predominantly of 1 line of therapy3,4
- This may be due, in part, to the aggressive nature of the disease4
- Improvements in 1L efficacy may permit the use of subsequent therapy
• nab®-Paclitaxel (nab-P) + Gem demonstrated superior efficacy vs Gem alone for all
endpoints examined in a phase III MPC trial, including OS, the primary endpoint
(median, 8.7 vs 6.6 mo; P < 0.001)5,6
• Feasibility and efficacy data are needed to guide 2L treatment decisions in MPC
• As nab-P + Gem has become a standard 1L therapeutic option for pts with MPC,3
an analysis of the regimen as part of a treatment plan is necessary
nab® is a registered trademark of Celgene Corporation.
• The current post hoc analysis investigated the feasibility and efficacy of 2L therapy
among pts from the MPACT trial
OBJECTIVE
STUDY DESIGN
• In the phase III trial, pts received nab-P + Gem or Gem alone as 1L treatment as
previously described5
- Pts were treated until disease progression, unacceptable toxicity, or pt or
physician decision
- Pts were followed until discontinuation of 1L therapy, after which only dates and
type of subsequent treatment(s) as well as date of death were collected
• After the closure of the MPACT trial (NCT00844649) in 2013, an observational
extension study was initiated to gather more survival information on pts who were
still alive (NCT02021500).
- The data collected from the extension study is included in this post hoc
evaluation
• The Kaplan-Meier method was used to calculate OS:
- Total OS: from initial randomization
- OS2: survival time from end of 1L therapy
• Multivariate analyses of total OS and OS2 were conducted using a Cox proportional
hazard model to evaluate 1L treatment and use of 2L therapy adjusted for other
prognostic factors (at the end of 1L treatment for OS2); a stepwise procedure was
performed to evaluate the treatment effect and identify the possible factors
associated with OS or OS2
- Total OS: In addition to 1L and 2L treatment effect, the potential influence of the
following prognostic factors was assessed:
Geographic region (North America and other), age, KPS, NLR, PC primary
location, stage at diagnosis, CA19-9 level, presence of liver metastases,
peritoneal carcinomatosis, previous Whipple procedure, presence of biliary
stent, presence of pulmonary metastases, number of metastatic sites
- OS2: The potential influence of the following factors was assessed:
Prognostic factors at baseline: geographic region (North America and
other) and number of metastatic sites
Factors at the end of 1L treatment: age, KPS, NLR, 1L PFS (≥ median and
< median)
RESULTS
Patients
• ≥ 40% of pts in each treatment arm received a 2L therapy (Table 1A)
• 5-FU or cape-containing regimens were the most common 2L therapies (> 75%;
Tables 1A and 1B)
• Pts who received 2L treatment had a better performance status at baseline
compared with those who did not receive 2L treatment (Table 1A)
• Pts treated with FOLFIRINOX as 2L therapy had better performance status at the
end of 1L treatment compared with all other regimens (Tables 2A and 2B)
1L, first-line; 2L, second-line; 5-FU, 5-fluorouracil; CA19-9, carbohydrate antigen 19-9; Cape, capecitabine; ECOG PS,
Eastern Cooperative Oncology Group performance status; FOLFIRINOX, leucovorin, 5-FU, irinotecan, oxaliplatin;
FOLFOX/OFF, leucovorin, 5-FU, oxaliplatin; Gem, gemcitabine; ITT, intent to treat; KPS, Karnofsky performance status; met,
metastatic; MPC, metastatic pancreatic cancer; nab-P, nab-paclitaxel; NLR, neutrophil-to-lymphocyte ratio; OS, overall
survival; PFS, progression-free survival; PFS1, progression-free survival during 1L treatment; PS, performance status; pt,
patient; PC, pancreatic cancer; ULN, upper limit of normal.
Variable
ITT Any 2L Therapy No 2L Therapy5-FU- or Cape-
Containing
nab-P
+ GemGem
nab-P
+ GemGem
nab-P
+ GemGem
nab-P
+ GemGem
n 431 430 170 177 261 253 132 135
Age, median, y 62.0 63.0 61.0 62.0 63.0 64.0 59.5 62.0
KPS, %
90 - 100
70 - 80
58
42
62
38
68
32
75
25
51
49
54
46
64
36
76
24
CA19-9
median, U/mL
≥ 59 × ULN, %
n = 379
2294
52
n = 371
2759
53
n = 152
2644
49
n = 162
2096
46
n = 227
1951
43
n = 209
3664
45
n = 120
2637
51
n = 125
2172
47
No. met. sites, %
1 - 3
> 3
86
14
85
15
88
12
88
12
85
15
84
16
88
12
89
11
NLR, %
≥ 5
> 5
n = 426
62
38
n = 426
65
35
75
25
73
27
55
45
60
40
74
26
72
28
Variable
5-FU or Cape Comboa FOLFIRINOX FOLFOX/OFF
nab-P +
GemGem
nab-P +
GemGem
nab-P +
GemGem
n 98 107 18 17 36 49
Age, median, y 59.0 62.0 53.5 56.0 58.5 64.0
KPS, %
90 - 100
70 - 80
67
33
76
24
72
28
76
24
53
47
67
33
CA19-9
median, U/mL
≥ 59 × ULN, %
n = 90
2601
51
n = 100
2206
48
n = 16
5539
56
n = 17
2368
53
n = 33
2650
53
n = 43
2005
43
No. met. sites, %
1 - 3
> 3
91
9
93
7
100
0
88
12
86
14
92
8
NLR, %
≥ 5
> 5
75
25
70
30
72
28
71
29
78
22
69
31
a 3 pts (2 in the nab-P + Gem arm and 1 in the Gem arm) received 2L FOLFIRI treatment.
Table 1A. Baseline Characteristics by 2L Therapy Received
Table 1B. Baseline Characteristics for Pts who Received 2L 5-FU- or
Cape-Containing Combinations
Reasons for 1L Treatment Discontinuation
• Pts with any 2L treatment: 59% and 74% in the nab-P + Gem and Gem-alone arms,
respectively, discontinued 1L therapy due to progressive disease
- 26% and 14% discontinued 1L therapy due to adverse events
Efficacy
• Pts with any 2L treatment: Total OS (from initial randomization) was significantly
longer with nab-P + Gem vs Gem (median, 12.8 vs 9.9 mo.; P = 0.015; Figure 1)
- Without 2L therapy: longer for nab-P + Gem (median, 6.2 vs 4.7 mo; HR 0.69;
P < 0.001)
• Pts who received a 5-FU- or cape-containing 2L therapy: Total OS was significantly
longer for those in the nab-P + Gem vs Gem-alone arms (median, 13.5 vs 9.5 mo; P
= 0.012)
• In the nab-P + Gem and Gem-alone arms, fewer pts received 5-FU or cape mono-
than combination therapy (34 vs 98 pts and 28 vs 107 pts, respectively)
- Fewer pts who received 5-FU or cape monotherapy had KPS 90 -100 (32%
and 36% for nab-P + Gem and Gem alone, respectively) compared with those
who received 5-FU or cape combination therapy (Table 2B)
• OS2 (from end of 1L therapy) for nab-P + Gem vs Gem alone
- With 2L therapy: median OS similar (6.7 vs 6.4 mo; P = 0.273; Figure 2)
- Without 2L therapy: longer for nab-P + Gem (median, 2.5 vs 1.6 mo; HR 0.67;
P < 0.001)
Variable
Any 2L Therapy No 2L Therapy5-FU-or Cape-
Containing
nab-P +
GemGem
nab-P +
GemGem
nab-P +
GemGem
n 170 177 261 253 132 135
Age, median, y 61.8 62.5 63.6 65.2 60.4 62.5
KPS, %
90 - 100
80
70
≥ 60
43
37
11
9
n = 176
48
34
10
8
n = 240
26
28
20
27
n = 222
22
32
19
27
43
38
8
11
45
35
12
8
CA19-9
median, U/mL
≥ 59 × ULN, %
n = 144
276
26
n = 131
380
32
n = 170
263
29
n = 121
1669
45
n = 112
276
28
n = 99
514
33
NLR
≥ 5 , % 74
n = 176
67
n = 236
59
n = 215
45 77 64
Variable
5-FU or Cape
Comboa FOLFIRINOX FOLFOX/OFF
nab-P +
GemGem
nab-P +
GemGem
nab-P +
GemGem
n 98 107 18 17 36 49
Age, median, y 59.8 62.5 54.4 56.2 59.5 64.7
KPS, %
90 - 100
80
70
≥ 60
47
38
6
9
48
35
11
7
50
39
6
6
59
12
29
0
44
31
6
19
35
51
10
4
CA19-9
median, U/mL
≥ 59 × ULN, %
n = 84
241
27
n = 76
547
33
n = 16
195
19
n = 10
401
20
n = 32
398
28
n = 33
261
30
NLR ≥ 5 , % 77 65 72 71 69 63
a Three pts (2 in the nab-P + Gem arm and 1 in the Gem arm) received 2L FOLFIRI treatment.
Table 2A. Pt Characteristics at End of 1L Treatment
Table 2B. Pt Characteristics at End of 1L Treatment for Pts who
Received 2L 5-FU- or Cape-Containing Combinations
Poster presented at the 2016 Gastrointestinal Cancers Symposium; January 21-23, 2016; San Francisco, CA
Figure 1. Total OS in Pts Who Received 2L Therapy
Events/nMedian, mo (95%
CI)
161/170 12.8 (10.9 - 14.2)
166/177 9.9 (8.9 - 10.9)
Pro
po
rtio
n o
f S
urv
iva
l
Time, monthsPts at risk
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
177Gem: 174 139 101 63 39 28 21 16 9 8 6 4 2 1 1 0 0
170 165 149 117 87 60 36 29 22 17 13 10 8 4 3 2 2 0nab-P
+ Gem:
HR 0.76
95% CI, 0.61 - 0.95
P = 0.015
Gem
nab-P + Gem
Events/nMedian, mo (95%
CI)
161/170 6.7 (6.1 - 7.9)
166/177 6.4 (5.3 - 7.7)
Figure 2. OS2 From End of 1L Therapy
Time, months
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45 48 51
Pro
po
rtio
n o
f S
urv
iva
l
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pts at risk
177 142 91 56 32 21 14 9 5 5 4 3 1 1 1 0 0 0Gem:
170 149 98 61 39 24 17 13 10 6 4 4 4 2 2 1 1 0nab-P
+ Gem:
HR 0.89
95% CI, 0.71 - 1.10
P = 0.273
Gem
nab-P + Gem
Covariate HR (95% CI) P value
Treatment group (nab-P + Gem vs Gem alone) 0.73 (0.63 - 0.85) < 0.001
2L therapy (with vs without) 0.47 (0.40 - 0.54) < 0.001
NLR at end of 1L (≥ 5 vs > 5) 0.60 (0.52 - 0.70) < 0.001
KPS at end of 1L
90 -100 vs ≥ 60
70 -80 vs ≥ 60
0.46 (0.37 - 0.57)
0.57 (0.47 - 0.70)
< 0.001
< 0.001
PFS, mo (≥ 4.4 vs < 4.4)a 0.78 (0.67 - 0.91) 0.002
Geographic region (North America vs others) 0.86 (0.74 - 1.00) 0.051
a In this study, the median PFS for the entire ITT population was 4.4 mo.
Table 3. Multivariate Analysis of OS2
Efficacy (continued)
• Factors significantly associated with longer total OS by multivariate analysis
include 1L treatment with nab-P + Gem vs Gem alone, use of 2L therapy, better
KPS at baseline (90 - 100 vs 70 -80), no liver metastases, baseline NLR ≥ 5 vs
> 5 (P < 0.001 for each), and lower CA19-9 at baseline (P = 0.005)
• Factors significantly associated with longer OS2 by multivariate analysis (Table
3) include 1L treatment with nab-P + Gem vs Gem alone, use of 2L therapy, NLR
≥ 5 vs > 5 at end of 1L therapy, better KPS at end of 1L therapy (P < 0.001 for
each), and PFS1 ≥ 4.4 mo vs < 4.4 mo (P = 0.002)
• The longest total OS values were for pts who received 1L nab-P + Gem and 2L
treatment with FOLFIRINOX (median OS, 15.7 mo; Table 4)
This study is supported by Celgene Corporation, Summit, NJ. The authors received editorial and production support in the
preparation of this poster from MediTech Media, Ltd, funded by Celgene Corporation. The authors are fully responsible for all
content and editorial decisions for this poster.
ACKNOWLEDGMENTS
DISCLOSURES
REFERENCES
Dr. David Goldstein - [email protected]
CORRESPONDENCE
CONCLUSIONS
• 2L treatment was feasible and beneficial for pts with MPC, with greater benefit
observed for those who received 1L nab-P + Gem vs Gem alone
• A limitation of this study is that no information was available about treatment
schedule or dose, safety, or efficacy (beyond survival) during 2L therapy
• Receiving 2L therapy was significantly associated with longer total OS, even after
adjusting for baseline characteristics
• 1L therapy may play a role in achieving optimal treatment benefit
- Total OS was significantly longer among pts who received 2L 5-FU– or cape-
containing therapies following 1L nab-P + Gem vs Gem alone
• Pts most likely to benefit from additional therapy include those with a longer PFS
during 1L treatment and lower NLR and better PS at the end of 1L treatment
• The current analysis supports the use of nab-P + Gem as an appropriate 1L therapy
onto which a treatment plan can be built
1. World Health Organization. GLOBOCAN 2012: Estimated cancer incidence, mortality,
and prevalence worldwide in 2012.
http://globocan.iarc.fr/Pages/fact_sheets_population.aspx. Accessed December 8, 2015.
2. Surveillance, Epidemiology, and End Results Program. SEER stat facts sheets: pancreas
cancer. http://seer.cancer.gov/statfacts/html/pancreas.html. Updated 2015. Accessed
December 8, 2015.
3. Abrams TA, et al. J Clin Oncol. 2014;32:(5 suppl) [abstract 4131].
4. Smyth EN, et al. Clin Ther. 2015;37:1301-1316.
5. Von Hoff DD, et al. N Engl J Med. 2013;369:1691-1703.
6. Goldstein D, et al. J Natl Cancer Inst. 2015;107(2).
Copies of this poster obtained through Quick Response (QR) Code are for
personal use only and may not be reproduced without permission from ASCO®
and the author of this poster.
DG: research funding, Celgene, Pfizer; consultant or advisory role (unremunerated), Celgene, Pfizer; EGC: research funding,
consultant or advisory role, Celgene; JT: consultant or advisory role, honoraria, Celgene; RE-M: consultant or advisory role, research
funding, Celgene; WWM: research funding, Celgene; MR: consultant or advisory role, honoraria, research funding, Celgene; MH:
nothing to disclose; RW: nothing to disclose; SC: stock ownership, Celgene; JSL, VM, BL, AR: employment, stock ownership,
Celgene; DDVH: consultant or advisory role, honoraria, Celgene; research funding, HonorHealth
Table 4. Survival Outcome Summary in Pts Who Received 2L Therapy
Variable n (%)
Median Duration, mo
OS
From 1L
Randomization to
First Dose of 2L Tx
From First Dose
of 2L Tx to Death
Any 2L therapy
nab-P + Gem
Gem
170 (39)
177 (41)
12.8
9.9
6.6
4.1
5.3
4.5
Othera
nab-P + Gem
Gem
38 (22)
42 (24)
10.9
11.3
6.3
4.5
3.2
4.8
5-FU- or Cape-Containing
nab-P + Gem
Gem
132 (78)
135 (76)
13.5
9.5
6.7
4.1
5.7
4.5
5-FU or Cape combo
nab-P + Gem
Gem
98 (58)
107 (60)
14.0
9.5
6.6
4.0
6.0
4.6
5-FU or Cape mono
nab-P + Gem
Gem
34 (20)
28 (16)
11.9
9.4
6.7
5.3
4.7
3.9
FOLFIRINOX
nab-P + Gem
Gem
18 (11)
17 (10)
15.7
7.2
8.4
4.0
7.2
3.5
FOLFOX/OFF
nab-P + Gem
Gem
36 (21)
49 (28)
13.7
9.8
5.6
4.1
6.4
4.5a Other than 5-FU- or Cape-containing Tx; median total OS for 1L Gem followed by 2L nab-P + Gem (n = 7) or nab-P
alone (n = 11) was 7.9 and 8.8 mo, respectively.
Pts who received a 5-FU- or cape-containing 2L therapy: Total OS was significantly longer for those in the nab-P + Gem vs Gem-alone arms
(median, 13.5 vs 9.5 mo; P = 0.012) And combo regimens >14 months…

• G-NP can face to FOLFIRINOX in the same group of patients (very fit or super-fit patients/without restrictions or limitations)? • Interesting “new” data (data from retrospective and randomized clinical
trials)
• 1st-line G-NP permits more 2nd - 3rd line treatment options than 1st-line FOLFIRINOX (1st-line treatment with G-NP does not compromise subsequent treatment options)
• In ECOG 2 patients (tumor load) G-NP is a new regimen with high efficacy
Conclusiones

• In second line setting the combination of naliri and 5FU is a new standard of care after gem combinations
• The combination of naliri and 5FU provides a break from neurotoxicity and paving the way of subsequent 3rd-line
Conclusiones