presentación de powerpoint - svmefr.comsvmefr.com/wp-content/uploads/2018/04/dra.-calero.pdf · el...
TRANSCRIPT

Unidades de Coordinación de
Fracturas, desde el punto de
vista del Médico
Rehabilitador
Dra. Elena Calero Muñoz
Jefa del Servicio de Rehabilitación y Medicina Física
Xarxa Sanitària i Social Santa Tecla
Tarragona

OSTEOPOROSIS
FRACTURAS POR
FRAGILIDAD
GRAVÍSIMO PROBLEMA

INCIDENCIA

Fracturas de muñeca
• La más precoz1,2
• Primera señal de alarma de la "cascada osteoporótica"3
1.-International Osteoporosis Foundation. “The breaking spine”. Disponible en:
https://www.iofbonehealth.org/sites/default/files/PDFs/WOD%20Reports/2010_the_breaking_spine_en.pdf.
2.-Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359(9319):1761-7.
3.-International Osteoporosis Foundation. "It’s not just a broken wrist, it’s a warning sign". Disponible en: https://www.iofbonehealth.org/news/not-just-broken-wrist-it-is-warning-sign.

Fracturas vertebrales
• La más frecuente, afectando al 30-
50% de la población mayor de 50
años1
• La mayoría de las fracturas
vertebrales son consecuencia de
osteoporosis1
1.-International Osteoporosis Foundation. “The breaking spine”. Disponible en:
https://www.iofbonehealth.org/sites/default/files/PDFs/WOD%20Reports/2010_the_
breaking_spine_en.pdf
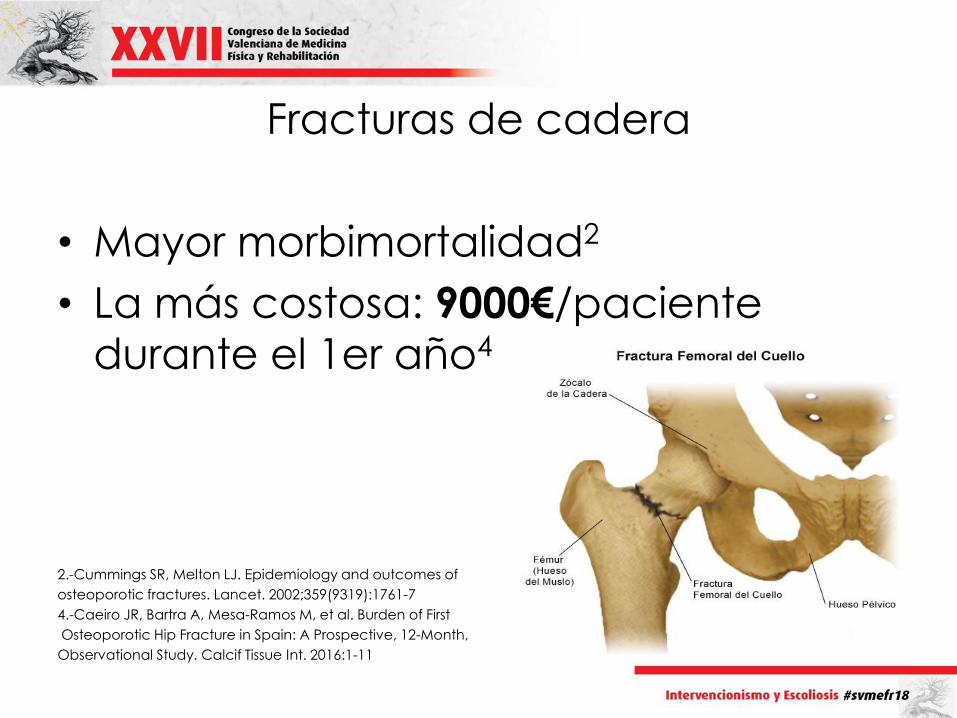
Fracturas de cadera
• Mayor morbimortalidad2
• La más costosa: 9000€/paciente
durante el 1er año4
2.-Cummings SR, Melton LJ. Epidemiology and outcomes of
osteoporotic fractures. Lancet. 2002;359(9319):1761-7
4.-Caeiro JR, Bartra A, Mesa-Ramos M, et al. Burden of First
Osteoporotic Hip Fracture in Spain: A Prospective, 12-Month,
Observational Study. Calcif Tissue Int. 2016:1-11
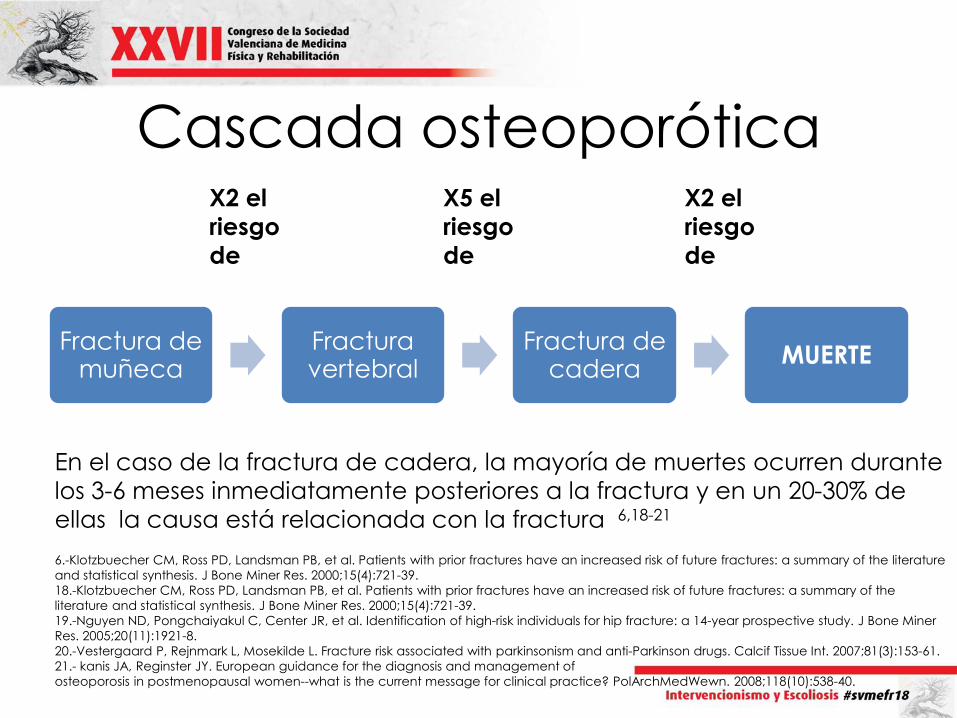
Cascada osteoporótica
Fractura de muñeca
Fractura vertebral
Fractura de cadera
MUERTE
X2 el
riesgo
de
X5 el
riesgo
de
X2 el
riesgo
de
En el caso de la fractura de cadera, la mayoría de muertes ocurren durante
los 3-6 meses inmediatamente posteriores a la fractura y en un 20-30% de
ellas la causa está relacionada con la fractura 6,18-21
6.-Klotzbuecher CM, Ross PD, Landsman PB, et al. Patients with prior fractures have an increased risk of future fractures: a summary of the literature
and statistical synthesis. J Bone Miner Res. 2000;15(4):721-39.
18.-Klotzbuecher CM, Ross PD, Landsman PB, et al. Patients with prior fractures have an increased risk of future fractures: a summary of the
literature and statistical synthesis. J Bone Miner Res. 2000;15(4):721-39.
19.-Nguyen ND, Pongchaiyakul C, Center JR, et al. Identification of high-risk individuals for hip fracture: a 14-year prospective study. J Bone Miner
Res. 2005;20(11):1921-8.
20.-Vestergaard P, Rejnmark L, Mosekilde L. Fracture risk associated with parkinsonism and anti-Parkinson drugs. Calcif Tissue Int. 2007;81(3):153-61.
21.- kanis JA, Reginster JY. European guidance for the diagnosis and management of
osteoporosis in postmenopausal women--what is the current message for clinical practice? PolArchMedWewn. 2008;118(10):538-40.

• Las estimaciones globales indican que el 40% de las mujeres y el 13%
de los hombres >50 años
sufrirá una fractura por
osteoporosis.8
• Debido al envejecimiento de la población, la incidencia se incrementará entre 2 y 4 veces durante las
próximas décadas.12-14 8.-European Commission. Report on Osteoporosis in the European Community: Action for Prevention
Luxembourg: Office for Official Publications of the European Communities. 1998: 1-114. Disponible en:
http://www.iofbonehealth.org/ osteoporosiseuropean-community-action-prevention.
12.-American Cancer Society. 1995.
13.-American Heart Association. 1995.
14.-Riggs BL, Melton LJ, 3rd. The worldwide problem of osteoporosis: insights afforded by epidemiology.
Bone. 1995;17(5 Suppl):505s-11s.

FRACTURAS
POR
FRAGILIDAD
9.-Lippuner K, Golder M, Greiner R. Epidemiology and direct medical costs of osteoporotic fractures in men and women in Switzerland. Osteoporos Int. 2005;16 Suppl 2:S8-s17.
10.-Johnell O, Kanis JA, Jonsson B, et al. The burden of hospitalised fractures in Sweden. Osteoporos Int. 2005;16(2):222-8.
11.-Kanis JA, Delmas P, Burckhardt P, et al. Guidelines for diagnosis and management of osteoporosis. The European Foundation for Osteoporosis and Bone Disease. Osteoporos Int. 1997;7(4):390-406.
• IAM +
• AVC +
• CÁNCER DE MAMA9-11

Los pacientes con una fractura previa tienen
un 86% más de probabilidad de sufrir
una segunda fractura durante el año siguiente.22
La 2ª fractura suele ocurrir dentro de los 6-8 meses23
22.-Kanis JA, Johnell O, De Laet C, et al. A meta-analysis of previous fracture and subsequent
fracture risk. Bone. 2004;35(2):375-82.
23..-International Osteoporosis Foundation. Capture The Fracture.
“About Capture the Fracture”. Disponible en: http://capturethefracture.org/slide-kits-reports.

Variación geográfica de incidencia de Fractura cadera
27.- Kanis et al, A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 2012 23:2239-2256 28.- Alvarez-Nebreda M.L y cols. Epidemiology of hip fracture in the elderly in Spain. Bone 2008; 42: 278-285
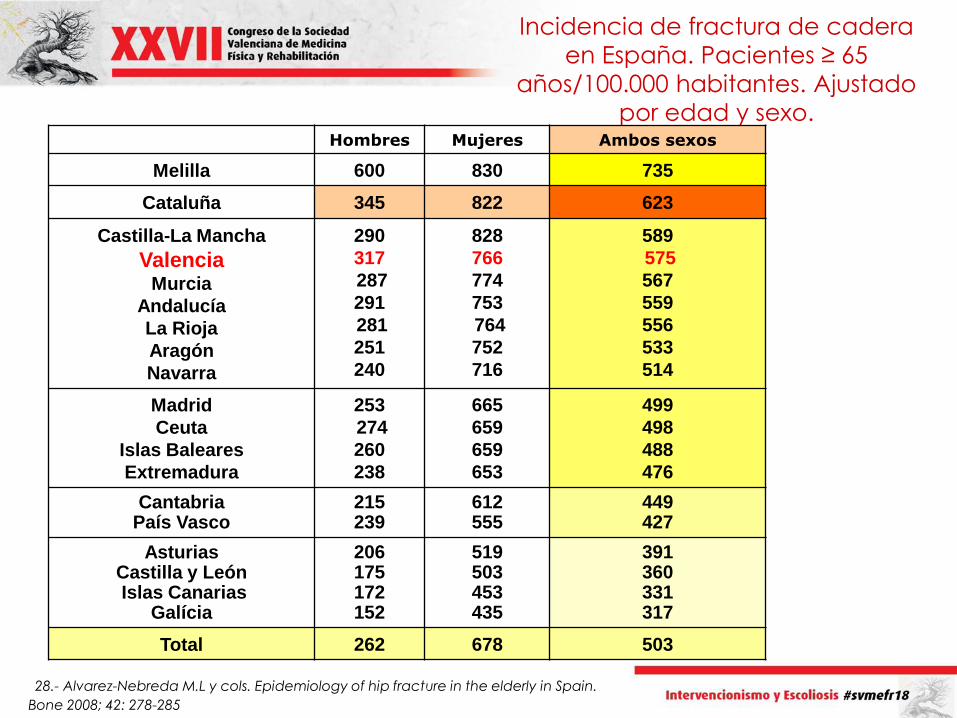
Incidencia de fractura de cadera
en España. Pacientes ≥ 65
años/100.000 habitantes. Ajustado
por edad y sexo. Hombres Mujeres Ambos sexos
Melilla 600 830 735
Cataluña 345 822 623
Castilla-La Mancha
Valencia Murcia
Andalucía
La Rioja
Aragón
Navarra
290
317
287
291
281
251
240
828
766
774
753
764
752
716
589
575
567
559
556
533
514
Madrid
Ceuta
Islas Baleares
Extremadura
253
274
260
238
665
659
659
653
499
498
488
476
Cantabria País Vasco
215 239
612 555
449 427
Asturias Castilla y León Islas Canarias
Galícia
206 175 172 152
519 503 453 435
391 360 331 317
Total 262 678 503
28.- Alvarez-Nebreda M.L y cols. Epidemiology of hip fracture in the elderly in Spain.
Bone 2008; 42: 278-285

LA MITAD DE LAS FRACTURAS DE CADERA PROVIENEN DEL 16% DE
PERSONAS QUE HAN TENIDO FRACTURAS PREVIAS.

CONSECUENCIAS

PROA (2011-12)
En España se estima una
población de riesgo para la
fractura de cadera de más
de 2 millones de personas7
GASTO GENERADO EN LA COMUNIDAD VALENCIANA:
7865€
durante el 1º año posterior a la misma38
7.-Avellana J, Fernández L. Guía de buena práctica clínica en geriatría. Anciano afecto de fractura de cadera.
Madrid: Ed. Elsevier; 2007.
38.-. Instituto de Información Sanitaria. Estadísticas Comentadas: La atención a la fractura de cadera en los hospitales del SNS [Publicación en Internet]. Madrid (Ministerio de Sanidad y Política Social; 2010). Disponible en: http://www.msps.es/estadEstudios/estadisticas/cmbdhome.htm
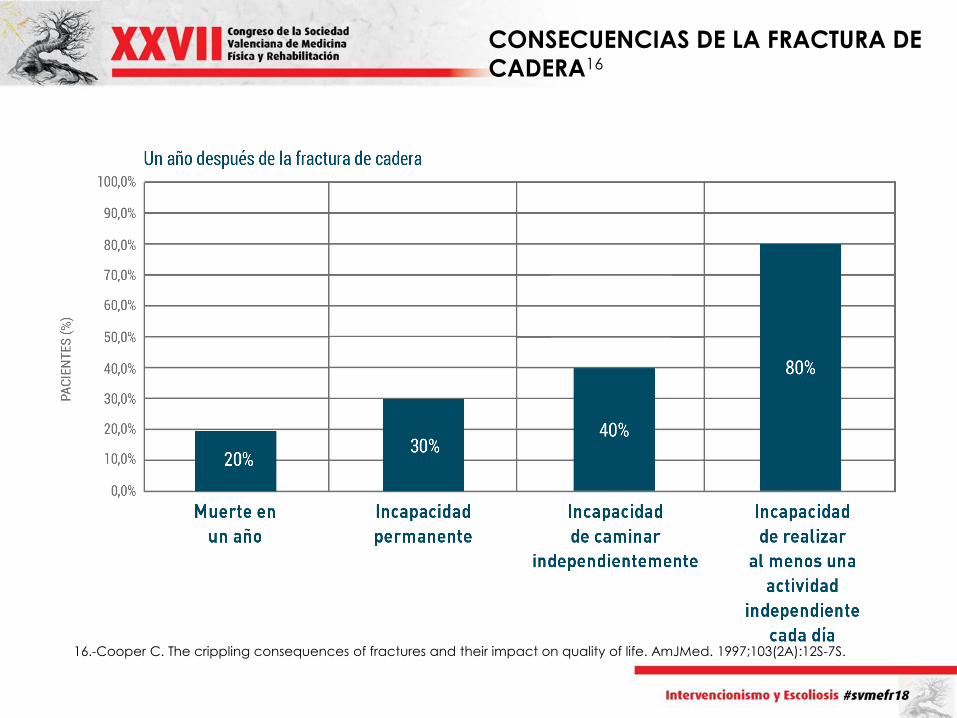
CONSECUENCIAS DE LA FRACTURA DE
CADERA16
16.-Cooper C. The crippling consequences of fractures and their impact on quality of life. AmJMed. 1997;103(2A):12S-7S.
La prevención secundaria de fracturas
por medios farmacológicos ha
demostrado ser altamente coste-
efectiva:25
– Reducción del riesgo de refractura en
un 39%
– Reducción del riesgo de muerte en
un 55%
– Reducción significativa de los costes
directos e indirectos asociados
25-Naranjo A, Ojeda-Bruno S, Bilbao Cantarero A, et al. Prevención secundaria de fracturas tras fractura de fémur en el área
norte de Gran Canaria: comparativa 2004-2014. Reumatol Clin. 2016;12(1):58-.

A pesar de los beneficios que conlleva
el tratamiento, las fracturas
actualmente están infratratadas,
y menos del 20% de pacientes con
fracturas previas recibe un tratamiento antirresortivo25
25-Naranjo A, Ojeda-Bruno S, Bilbao Cantarero A, et al. Prevención secundaria de fracturas tras fractura de fémur en el área
norte de Gran Canaria: comparativa 2004-2014. Reumatol Clin. 2016;12(1):58-.
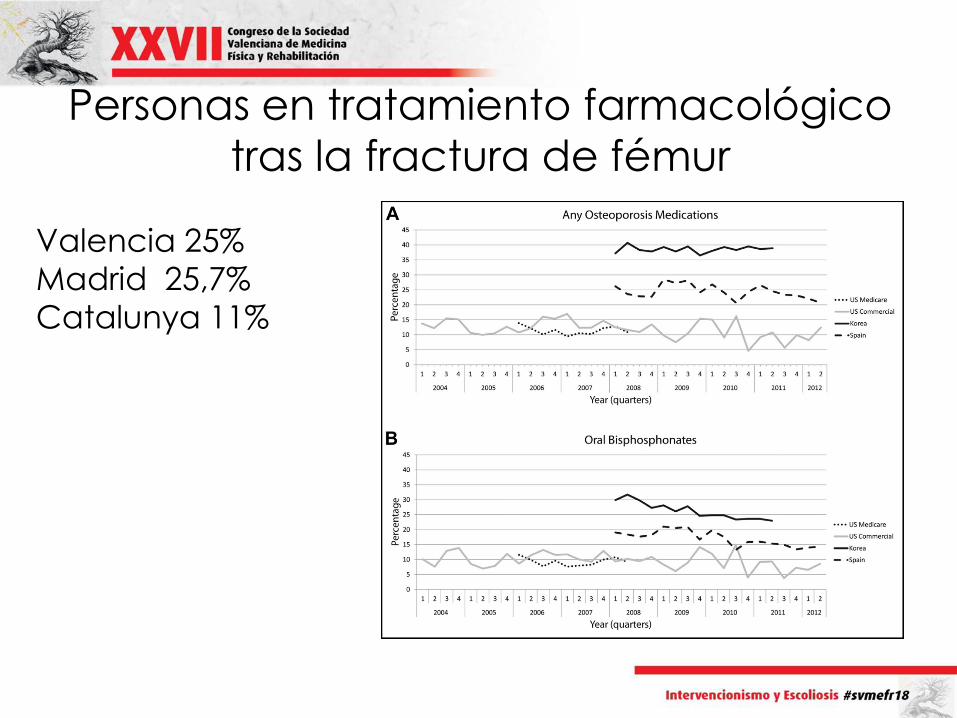
Personas en tratamiento farmacológico
tras la fractura de fémur
Valencia 25%
Madrid 25,7%
Catalunya 11%

CUMPLIMIENTO
• 50% pacientes no siguen los
tratamientos osteoporóticos prescritos
• Interrupción terapias: 50-70%

BAJO NIVEL DE ADHERENCIA

23

ABORDAJE SISTEMÁTICO QUE PERMITE
LA PREVENCIÓN SECUNDARIA DE
FRACTURAS (30,31) CREANDO SERVICIOS
MULTIDISCIPLINARES DE ATENCIÓN AL
PACIENTE CON FRACTURA
30.-McLellan AR, Gallacher SJ, Fraser M, et al. The fracture liaison service: success of a program for the evaluation and
management of patients with osteoporotic fracture. Osteoporos Int. 2003;14(12):1028-34.
31.-McLellan AR, Wolowacz SE, Zimovetz EA, et al. Fracture liaison services for the evaluation and management of patients with
osteoporotic fracture: a cost-effectiveness evaluation based on data collected over 8 years of service provision. Osteoporos Int.
2011;22(7):2083-98.

OBJETIVOS DE
LAS UCO(33)
• Identificar, evaluar, tratar y seguir al
enfermo afecto de fractura
osteoporótica
• Disminuir porcentaje de nuevas fracturas
• Reducir costes directos e indirectos de la
fractura
33.-IOF. Capture the Fracture. Disponible en: http://www.capturethefracture.org/fracture-liaison-services.

Coordinador
Internista/
Geriatra
Traumatólogo
Médico de familia
Médico de Urgencias
Gestor de
casos
Reumato
logo Rehabilita
dor
Asistente
social…

La comunicación entre hospital
y Atención Primaria es clave:35
• Ayudará al seguimiento de los pacientes
una vez consolidada la fractura
• Mejorará la adherencia al tratamiento que es baja en osteoporosis
• El abordaje integral del paciente hace posible la prevención de nuevas fracturas36
35.-Naranjo A, Ojeda-Bruno S, Bilbao Cantarero A, et al. Results of a model of secondary prevention for osteoporotic fracture coordinated by rheumatology and focused on the nurse and primary care physicians. Reumatol Clin. 2014;10(5):299-303.
36.-Akesson K, Marsh D, Mitchell PJ, et al. Capture the Fracture: a Best Practice Framework and global campaign to break the fragility fracture cycle. Osteoporos Int. 2013;24(8):2135-52.

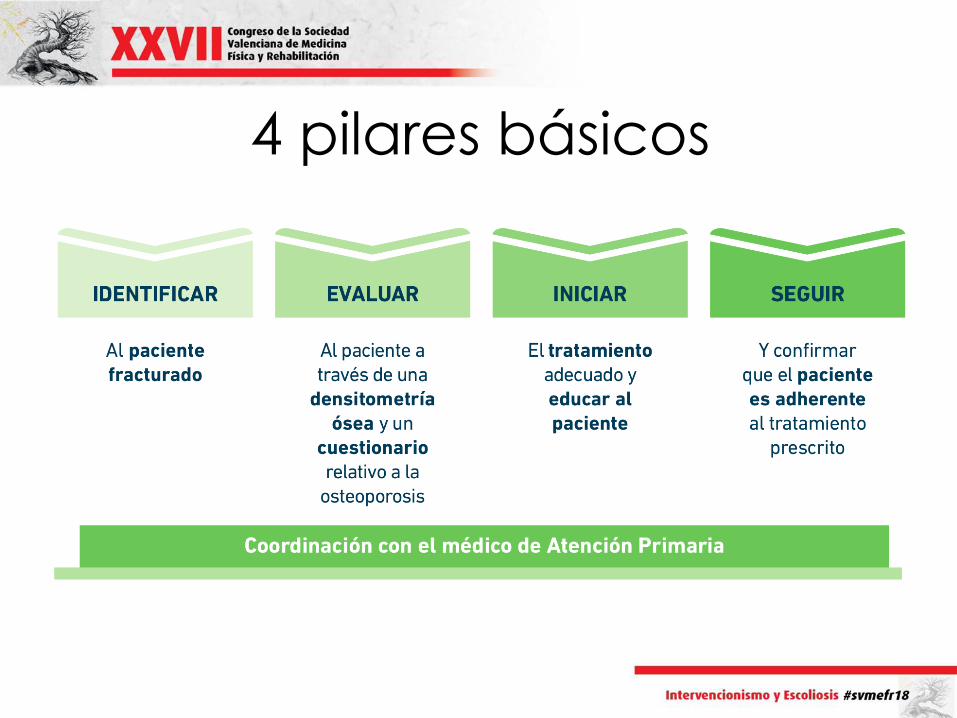
4 pilares básicos
UCO XARXA SANTA TECLA
- 2 hospitales comarcales (179 y 90
camas)
- 2 Sociosanitarios y 2 Residencias
- 6 centros de atención primaria


¿Dónde está
rehabilitación?
¡¡¡EN TODOS SITIOS!!!

• FORTALEZA (VENTAJA):
– ACCESO A TODOS LOS NIVELES
ASISTENCIALES
• DEBILIDAD (INCONVENIENTE):
– DISPERSIÓN

Fracturas de cadera
• Mayor morbimortalidad2
• La más costosa: 9000€/paciente
durante el 1er año4
4.-Caeiro JR, Bartra A, Mesa-Ramos M, et al. Burden of First
Osteoporotic Hip Fracture in Spain: A Prospective, 12-Month,
Observational Study. Calcif Tissue Int. 2016:1-11.
Equipo multidisciplinar
(Coordinado por Médico
Rehabilitador)
• Urgencias
• Servicio de traumatología
• Servicio de Int/Ger

Unidad ortogeriatría:
– Es la organización ideal
– Otras opciones: Internista
Responsable
- Traumatología: IQ

• Unidad ortogeriatría:
Geriatra/Internista prescribirá
Tratamiento farmacológico
Rehabilitación inicia terapia
Propia , valoración entorno…
• Atención primaria
• Médicos de residencia
• Rehabilitación:
Como coordinadores controlaremos los
resultados

• Perfil de laboratorio de osteoporosis/prequirúrgico de fémur
• Coordinación servicios trauma e interna
• Consulta virtual con reumatología para casos duda
• Información progresiva a todos los servicios implicados
• Recogida de datos para cumplir los criterios de calidad de la IOF

Hospital J23
• 383 camas
• Referencia en algunas especialidades e ítems para el resto de la provincia
• Ya disponía de Unidad de Ortogeriatría relacionada con su Sociosanitario
• La Dra. San Segundo, jefa de servicio de rehabilitación gestiona la coordinación de la UCO

• Integrará los servicios de
Reumatología,Rehabilitación y
Maxilofacial en el hospital
• Gestionará la integración de la
Atención primaria
• Recogida de datos para cumplir los
criterios de calidad de la IOF

CONCEPTOS BÁSICOS
• Patología con elevada carga
sociosanitaria
• Gran efectividad del tratamiento
farmacológico
• La atención protocolizada salva vidas
• La COORDINACIÓN la puede ejercer
perfectamente el Servicio de
Rehabilitación



¡¡¡GRACIAS POR VUESTRA
ATENCIÓN!!!

Referencias
1.-International Osteoporosis Foundation. “The breaking spine”. Disponible en: https://www.iofbonehealth.org/sites/default/files/PDFs/WOD%20Reports/2010_the_breaking_spine_en.pdf.
2.-Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359(9319):1761-7.
3.-International Osteoporosis Foundation. "It’s not just a broken wrist, it’s a warning sign". Disponible en: https://www.iofbonehealth.org/news/not-just-broken-wrist-it-is-warning-sign.
4.-Caeiro JR, Bartra A, Mesa-Ramos M, et al. Burden of First Osteoporotic Hip Fracture in Spain: A Prospective, 12-Month, Observational Study. Calcif Tissue Int. 2016:1-11.
5.-Consensus development conference: diagnosis, prophylaxis, and treatment of osteoporosis. Am J Med. 1993;94(6):646-50.
6.-Klotzbuecher CM, Ross PD, Landsman PB, et al. Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res. 2000;15(4):721-39.
7.-Avellana J, Fernández L. Guía de buena práctica clínica en geriatría. Anciano afecto de fractura de cadera. Madrid: Ed. Elsevier; 2007.
8.-European Commission. Report on Osteoporosis in the European Community: Action for Prevention Luxembourg: Office for Official Publications of the European Communities. 1998: 1-114. Disponible en: http://www.iofbonehealth.org/osteoporosiseuropean-community-action-prevention.
9.-Lippuner K, Golder M, Greiner R. Epidemiology and direct medical costs of osteoporotic fractures in men and women in Switzerland. Osteoporos Int. 2005;16 Suppl 2:S8-s17.
10.-Johnell O, Kanis JA, Jonsson B, et al. The burden of hospitalised fractures in Sweden. Osteoporos Int. 2005;16(2):222-8. 11.-Kanis JA, Delmas P, Burckhardt P, et al. Guidelines for diagnosis and management of osteoporosis. The European
Foundation for Osteoporosis and Bone Disease. Osteoporos Int. 1997;7(4):390-406. 12.-American Cancer Society. 1995.
13.-American Heart Association. 1995. 14.-Riggs BL, Melton LJ, 3rd. The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone. 1995;17(5
Suppl):505s-11s. 15.-De la Torre García M, Rodriguez Pérez J, Moreno Moreu N, et al. Estudio del impacto económico de las fracturas de
cadera en nuestro medio. Trauma Fund MAPFRE. 2012;23(1):15-21. 16.-Cooper C. The crippling consequences of fractures and their impact on quality of life. AmJMed. 1997;103(2A):12S-7S. 17.-Caeiro JR, Bartra A, Mesa-Ramos M, et al. Uso de recursos sanitarios y coste de la fractura de cadera en España:
estudio observacional, prospectivo PROA. XIX Congreso de la Sociedad Española de Investigación Ósea y Metabolismo Mineral, Santiago de Compostela 5-7 Noviembre 2014; póster LBA-3.

Referencias 18.-Klotzbuecher CM, Ross PD, Landsman PB, et al. Patients with prior fractures have an increased risk of future fractures: a
summary of the literature and statistical synthesis. J Bone Miner Res. 2000;15(4):721-39.
19.-Nguyen ND, Pongchaiyakul C, Center JR, et al. Identification of high-risk individuals for hip fracture: a 14-year prospective study. J Bone Miner Res. 2005;20(11):1921-8.
20.-Vestergaard P, Rejnmark L, Mosekilde L. Fracture risk associated with parkinsonism and anti-Parkinson drugs. Calcif Tissue Int. 2007;81(3):153-61.
21.- kanis JA, Reginster JY. European guidance for the diagnosis and management of osteoporosis in postmenopausal
women--what is the current message for clinical practice? PolArchMedWewn. 2008;118(10):538-40.
22.-Kanis JA, Johnell O, De Laet C, et al. A meta-analysis of previous fracture and subsequent fracture risk. Bone. 2004;35(2):375-82.
23..-International Osteoporosis Foundation. Capture The Fracture. “About Capture the Fracture”. Disponible en: http://capturethefracture.org/slide-kits-reports.
24.-Hernlund E, Svedbom A, Ivergard M, et al. Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos. 2013;8:136.
25-Naranjo A, Ojeda-Bruno S, Bilbao Cantarero A, et al. Prevención secundaria de fracturas tras fractura de fémur en el área norte de Gran Canaria: comparativa 2004-2014. Reumatol Clin. 2016;12(1):58-.
26.-Akesson K, Marsh D, Mitchell PJ, et al. Capture the Fracture: a Best Practice Framework and global campaign to break the fragility fracture cycle. Osteoporos Int. 2013;24(8):2135-52.
27.- Kanis et al, A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 2012 23:2239-2256
28.- Alvarez-Nebreda M.L y cols. Epidemiology of hip fracture in the elderly in Spain. Bone 2008; 42: 278-285
29 .-Kim SC, Kim MS, Sanfelix-Gimeno G, et al. Use of osteoporosis medications after hospitalization for hip fracture: a cross-national study. Am J Med. 2015;128(5):519-26.e1.
30.-McLellan AR, Gallacher SJ, Fraser M, et al. The fracture liaison service: success of a program for the evaluation and
management of patients with osteoporotic fracture. Osteoporos Int. 2003;14(12):1028-34.
31.-McLellan AR, Wolowacz SE, Zimovetz EA, et al. Fracture liaison services for the evaluation and management of patients with osteoporotic fracture: a cost-effectiveness evaluation based on data collected over 8 years of service provision. Osteoporos Int. 2011;22(7):2083-98.
33.-IOF. Capture the Fracture. Disponible en: http://www.capturethefracture.org/fracture-liaison-services.
34.-Curtis JR, Silverman SL. Commentary: the five Ws of a Fracture Liaison Service: why, who, what, where, and how? In osteoporosis, we reap what we sow. Curr Osteoporos Rep. 2013;11(4):365-8.
35.-Naranjo A, Ojeda-Bruno S, Bilbao Cantarero A, et al. Results of a model of secondary prevention for osteoporotic
fracture coordinated by rheumatology and focused on the nurse and primary care physicians. Reumatol Clin. 2014;10(5):299-303.
36.-Akesson K, Marsh D, Mitchell PJ, et al. Capture the Fracture: a Best Practice Framework and global campaign to break the fragility fracture cycle. Osteoporos Int. 2013;24(8):2135-52.
37.-Naranjo A, Ojeda-Bruno S, Bilbao-Cantarero A, et al. Two-year adherence to treatment and associated factors in a fracture liaison service in Spain. Osteoporos Int. 2015;26(11):2579-85.
38.-. Instituto de Información Sanitaria. Estadísticas Comentadas: La atención a la fractura de cadera en los hospitales del SNS [Publicación en Internet]. Madrid (Ministerio de Sanidad y Política Social; 2010). Disponible en:
http://www.msps.es/estadEstudios/estadisticas/cmbdhome.htm