presentación de powerpoint 22 mayo 2015 j... · portal en la hepatitis c . j. aguilar reina ....
TRANSCRIPT

Evaluación no invasiva de la fibrosis y de la hipertensión
portal en la hepatitis C
J. Aguilar Reina
Emérito del Servicio Andaluz de Salud
Instituto de Biomedicina de Sevilla. Hospital Universitario Virgen del Rocío

“ Quien pueda reducir o evitar la fibrosis tendrá en su mano la posibilidad de curar las
enfermedades hepáticas”
Hans Popper

http://aeeh.es/what-i-do/enfermedades-hepaticas-consejos-practicos/

¿ Es necesario conocer la cuantía de la fibrosis hepática?
• Para indicar tratamiento • Para emitir pronóstico • Para iniciar seguimiento por hipertensión
portal • Para iniciar seguimiento por riesgo de
carcinoma hepatocelular
VHC
• Todo infectado es tratable
• Sólo si fibrosis > 2 (Metavir)
Futuros tratamientos de la fibrosis
Trasplantes y muertes

Bruguera M, 2005 Fondo de Imagen en Hepatología. AEEH
Aguilar Reina J, 2005 Fondo de Imagen en Hepatología. AEEH

Goodman, J Hepatol 2007;47:598

Valoración de la Fibrosis Hepática en Biopsias
• Regev A. Am J Gastroenterol, 2002: (Obtención de una biopsia de cada lóbulo mediante
laparoscopia) – Diferencias entre lóbulos: 24 % al menos 1 grado; 42 % al menos 1 estadio 14% de cirrosis en un lóbulo clasificados como F3 en el otro – Diferencias entre 2 pases por 2 patólogos : 0 - 4% en graduación, 6-10% en estadiaje – 14% de casos con cirrosis no diagnosticados

Inconvenientes de la biopsia
• Invasiva y con algún riesgo
• Costosa
• Errores de muestreo
• Interpretación subjetiva


Identificación de la Cirrosis Hepática (métodos incruentos)

Gaiani et al J Hepatol, 1997
Diagnóstico de cirrosis (ecografía)

Valor: 2 N: 113
S: 80% VPP: 66%
E: 92,3% VPN: 92,3
Macías et al , 2003

Ahmad et al. Virology Journal 2011
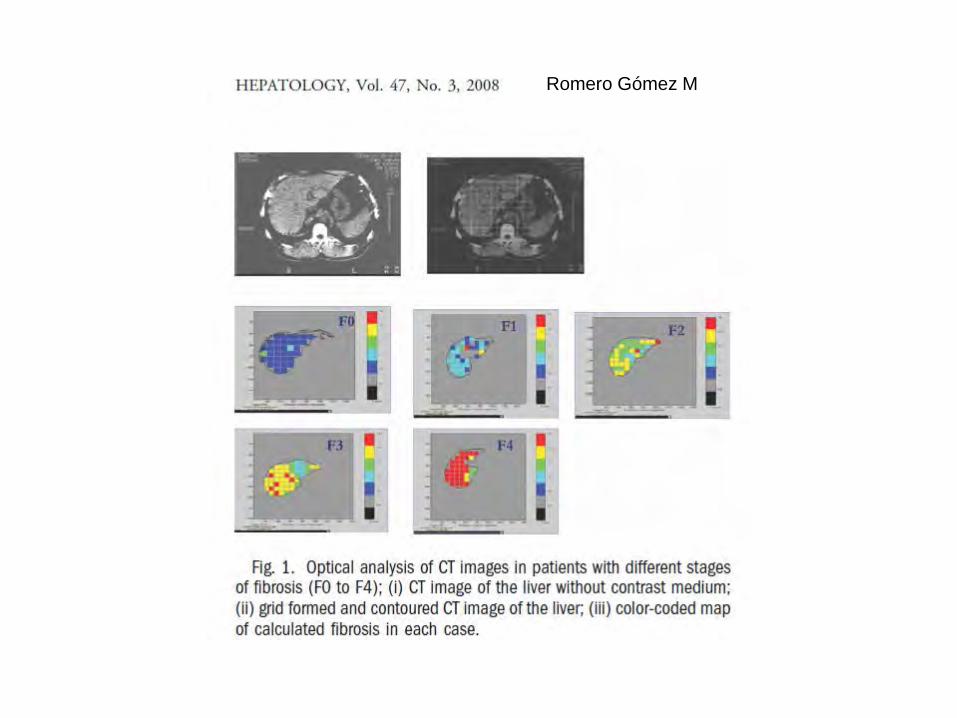
Romero Gómez M
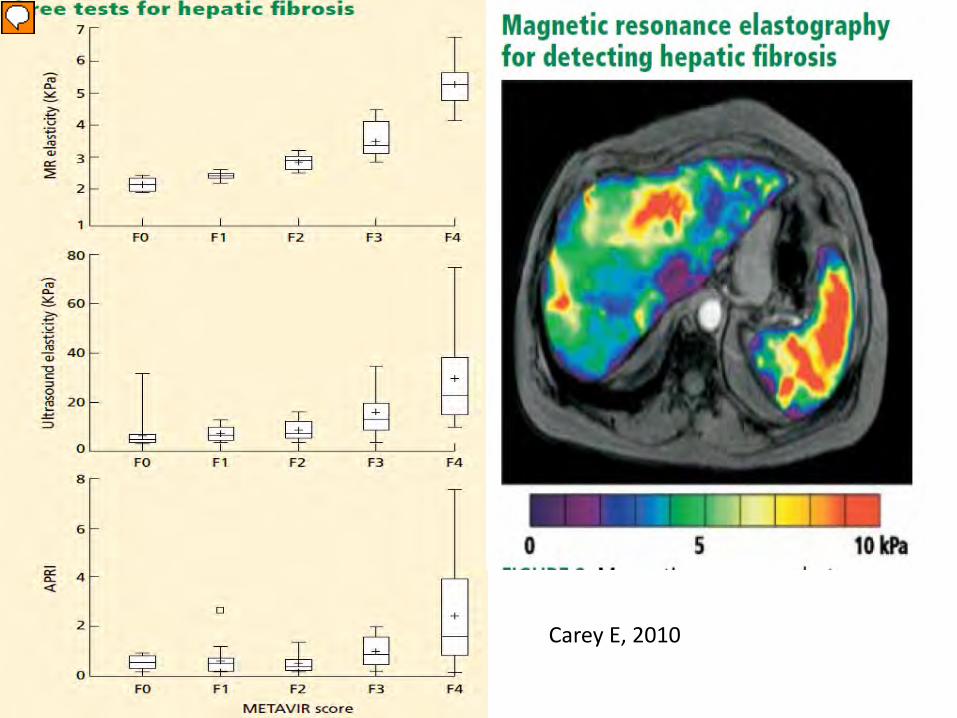
Carey E, 2010

Métodos serológicos
• Se basan en marcadores relacionados con: – Necroinflamación – Función hepática global – Hipertensión portal – Fibrogénesis – Reactantes de fase aguda – Resistencia a insulina – Edad
Pueden modificarse por:
•Patología extrahepática
•Factores genéticos
•Dudosa variación paralela a la de la fibrosis
Beaugrand. J Hepatol 2006
Además:
•Hay casos con enzimas normales
•¿Identifican fibrosis en respondedores?
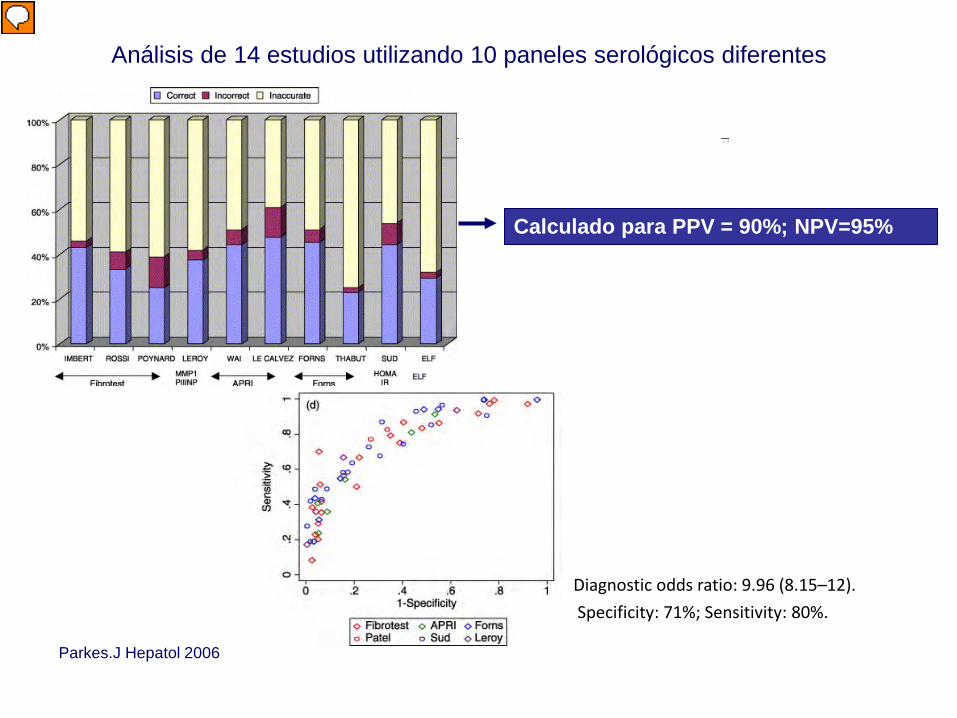
Parkes.J Hepatol 2006
Análisis de 14 estudios utilizando 10 paneles serológicos diferentes
Diagnostic odds ratio: 9.96 (8.15–12). Specificity: 71%; Sensitivity: 80%.
Calculado para PPV = 90%; NPV=95%

Fibrosis en pacientes con transaminasas normales
Schiffman et al. 2000
23%
39%
26%
6% 6%
sin fibrosis escasa portal puentes cirrosis
17% con fibrosis en puente.
Puoti,1997

Forns Fib-4
Halt-C
Edad ALT / AST gGT Colesterol Plaquetas Quick
0
2
4
6
8
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 0
25 %
50 %
75 %
100 %
37 % 48 %
Prob CH
39 %
72 %
0
2
4
6
8
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 0
25 %
50 %
75 %
100 % Prob CH
0
2
4
6
8
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 0
25 %
50 %
75 %
100 %
38 %
95 %
ASCITIS
Prob CH
Índices para la evaluación de la progresión de la enfermedad hepática
Solá R, 2008

Pacientes y Métodos
• Cálculo de los 3 índices en el momento de la biopsia y en un momento previo y/o posterior en el que contara con los datos analíticos necesarios
• Simulación, manteniendo los datos analíticos del momento de la biopsia y calculando los índices de FORNS y FIB4 como si el paciente, en ese momento, tuviera 1 año menos de edad y 1 y 10 años más
Biopsia
- 1 año Biopsia +1 año +10 años Aguilar Reina. AEEH 2009

FORNS (Antes) FORNS (Biopsia) FORNS (Después)
-2
0
2
4
6
8
10
94
8740
94
103100
494287
n = 131 n = 119 n = 85 APRI (Antes) APRI (Biopsia) APRI (Después)
0
2
4
6
8
26614240
46128426032
68
109
87
968
87
26
87
n = 132 n = 125 n = 86
FIB-4 (Antes) FIB-4 (Biopsia) FIB-4 (Después)
0
2
4
6
8
32
266089226140
4161
109
6887
87
26
60
87
n = 132 n = 125 n = 86
p: NS
* p< 0,05 * p< 0,05
* * *
* * *
Aguilar Reina. AEEH 2009

Acoustic radiation force impulse elastography or ARFI elastography
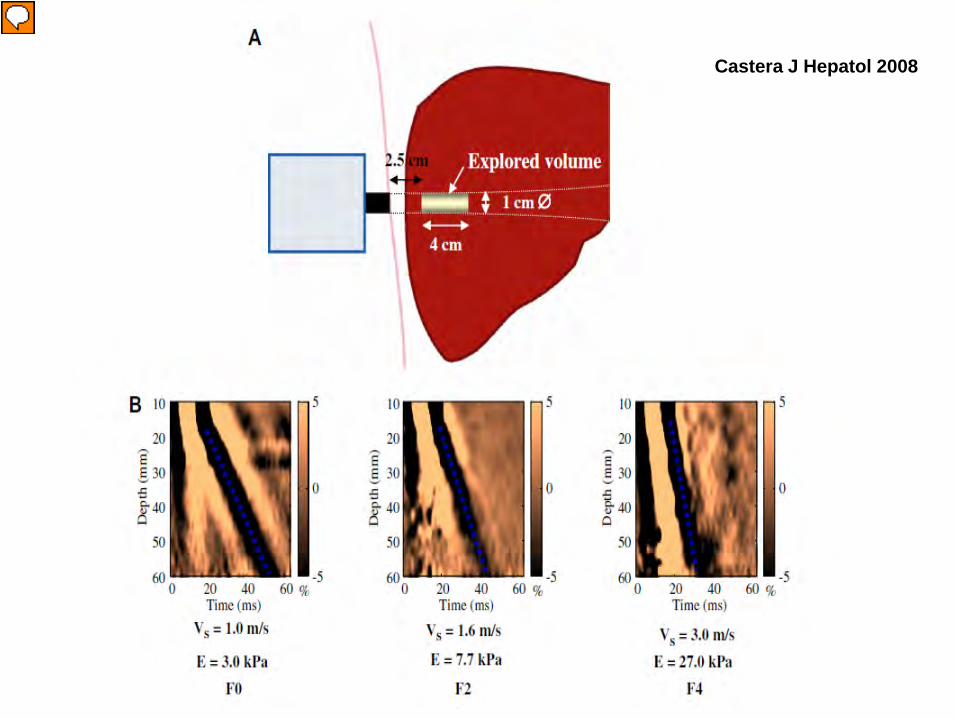
Castera J Hepatol 2008

CASTÉRA ET AL GASTROENTEROLOGY, 2005

In conclusion, Fibroscan is a reliable method for the diagnosis of cirrhosis in patients with chronic liver diseases, better at excluding than at predicting cirrhosis using a threshold of 14.6 kPa. False-negatives are mainly attributable to inactive or macronodular cirrhosis. ( Ganne – Carrié N HEPATOLOGY 2006;44:1511-1517.)


Factores que inducen mediciones erróneas (FS)
• Movimientos respiratorios • Estasis • Intensa actividad necroinflamatoria • Esteatosis • Factores anatómicos • Valsalva • Cirrosis macronodular • ¿ Uniformidad en puntos diferentes ?

P. Lebray. EASL 2010
Dos exploraciones (FibroScan) entre 1 día y 1 año
531 pares de FS
Múltiples etiologías
Sens
itivi
ty
0
0.2
0.4
0.6
0.8
1.0
0 0.2 0.4 0.6 0.8 1.0
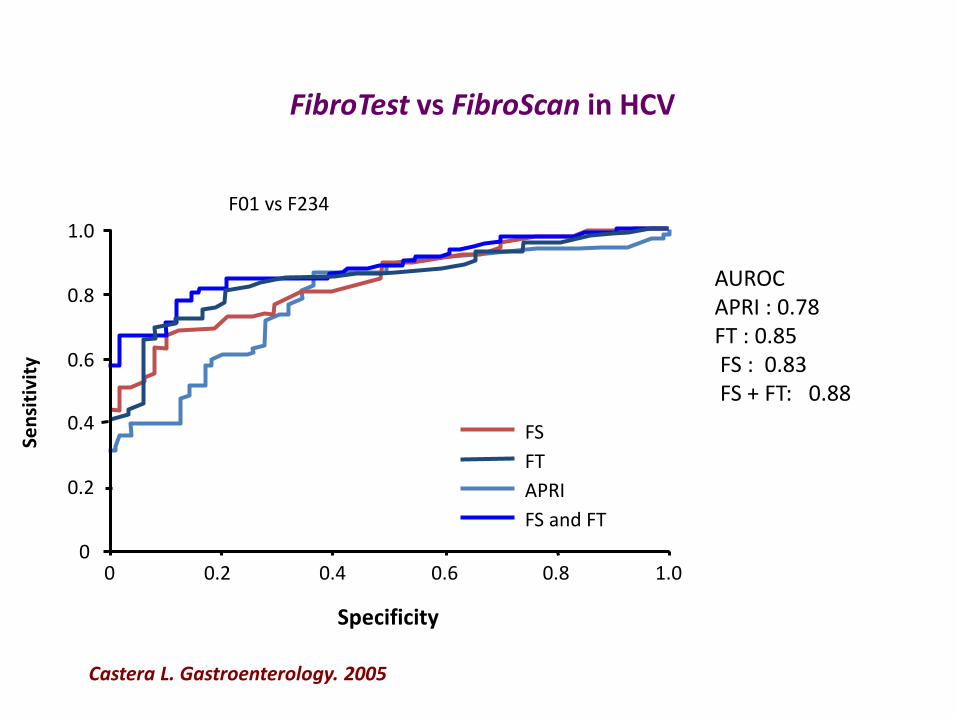
FS FT APRI FS and FT
F01 vs F234
AUROC APRI : 0.78 FT : 0.85 FS : 0.83 FS + FT: 0.88
Castera L. Gastroenterology. 2005
Specificity
FibroTest vs FibroScan in HCV

Infección VHC con transaminasas normales
Colletta Hepatology 2005
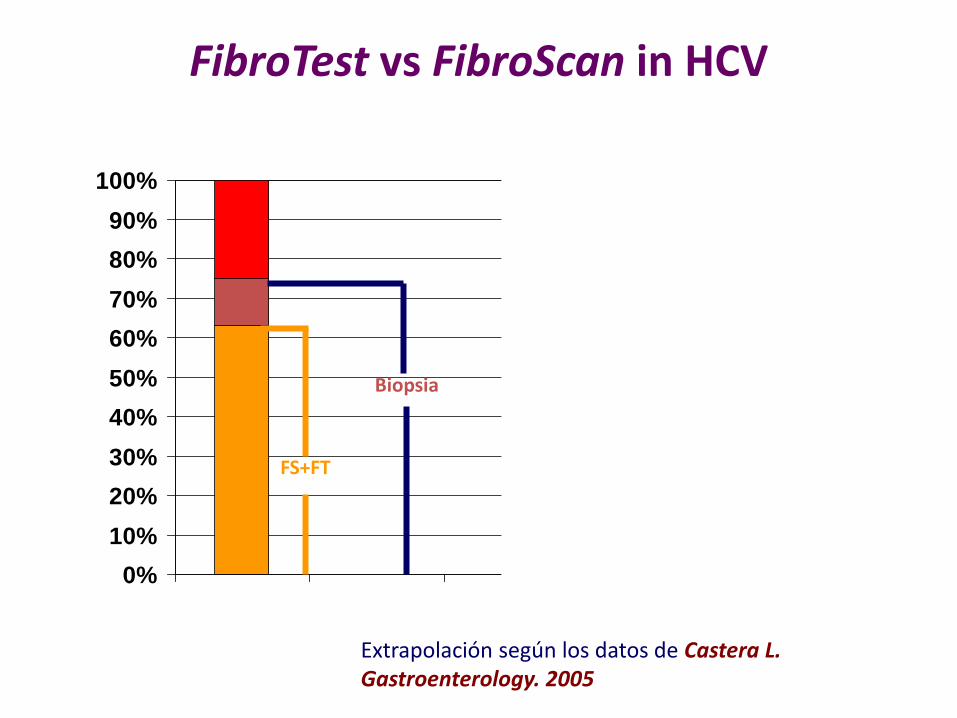
FibroTest vs FibroScan in HCV
0%10%20%30%40%50%60%70%80%90%
100%
FS+FT
Biopsia
Extrapolación según los datos de Castera L. Gastroenterology. 2005

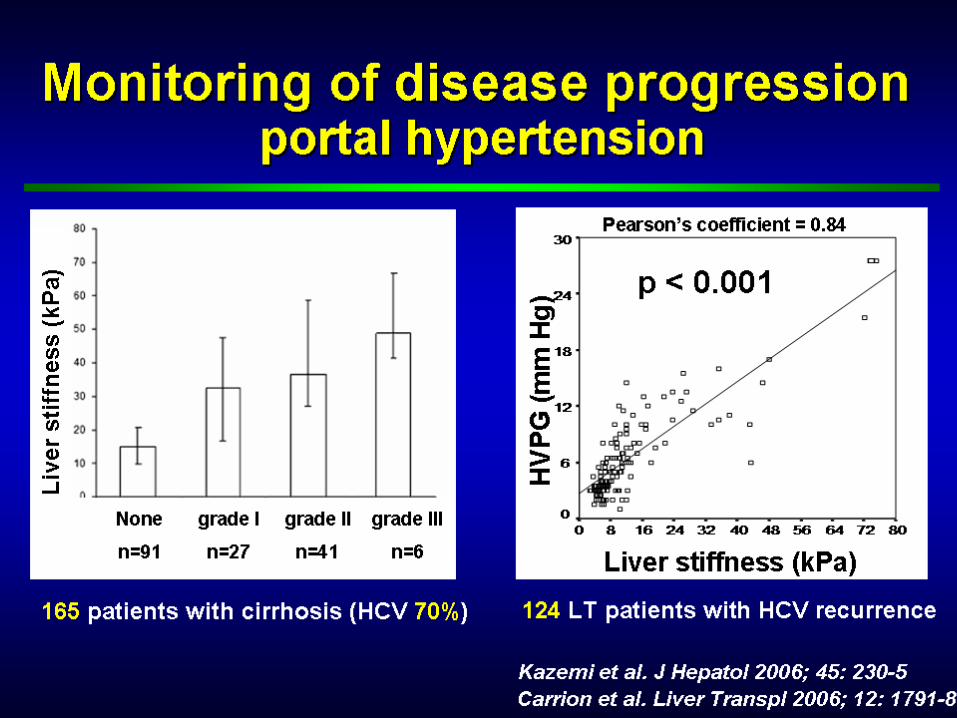
Identificación de hipertensión portal en pacientes con cirrosis


Pinzani M, EASL 2007 e series

Robic et al

A medida que aumenta la presión desciende la correlación
Vizzutti Hepatology 2017

Objetivos
Conocer:
– Si es posible la determinación de la elasticidad esplénica en la práctica clínica
– La relación entre los valores de elasticidad hepática y esplénica; y de ambas con la presencia de varices esofágicas
Aguilar Reina J. AEEH 2014

Conclusiones
• En la práctica clínica es posible el estudio de la elasticidad transitoria del bazo
• La elasticidad esplénica se relaciona mejor que la hepática con la presencia de varices esofágicas.
• Un algoritmo que incluya secuencialmente la medición de la elasticidad hepática y la esplénica puede fijar el momento en que es necesario iniciar el screening para descartar varices mediante endoscopia oral
Aguilar Reina, AEEH 2014

Fig. 4
Journal of Hepatology 2014 60, 1158-1164DOI: (10.1016/j.jhep.2014.02.024) Copyright © 2014 European Association for the Study of the Liver
Coleccia et al J Hepatol 2014

Pronóstico de complicaciones y supervivencia

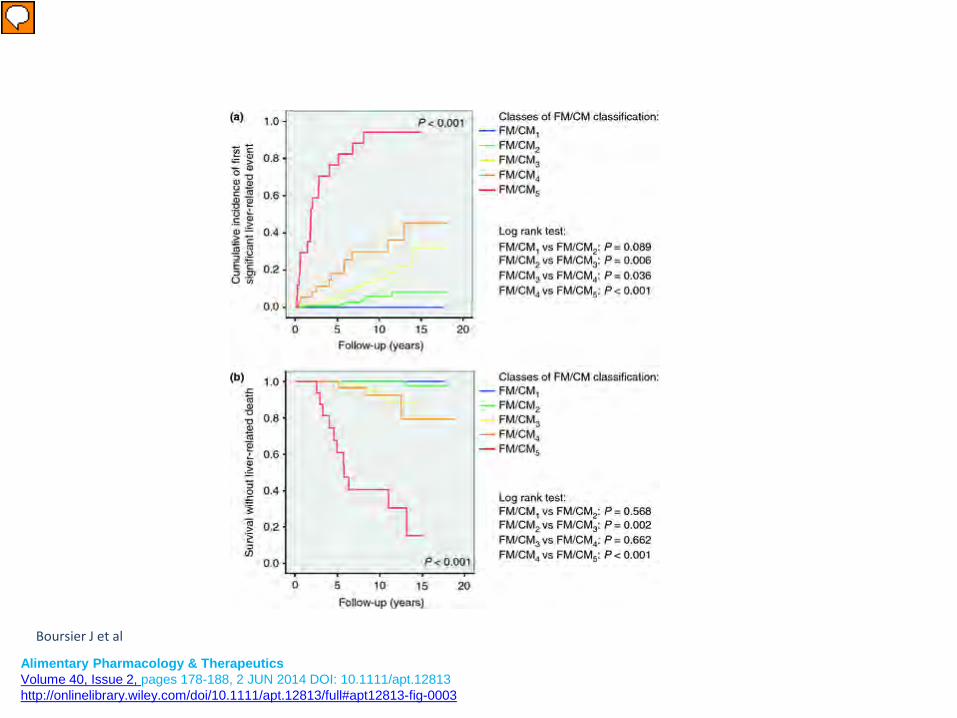
Combination of blood tests for significant fibrosis and cirrhosis improves the assessment of liver-prognosis in chronic hepatitis C
Alimentary Pharmacology & Therapeutics Volume 40, Issue 2, pages 178-188, 2 JUN 2014 DOI: 10.1111/apt.12813 http://onlinelibrary.wiley.com/doi/10.1111/apt.12813/full#apt12813-fig-0003
Boursier J et al

Delta=(follow-up result - baseline result) / time interval between baseline and follow- up measurements (year).
Whole cohort
Vergniol, Hepatology 2014

Elasticidad y carcinoma hepatocelular
Masuzaki, Hepatology 2009

Ledinghen, 2008

Conclusiones • La estimación de la fibrosis hepática debe hacerse inicialmente
y durante el seguimiento midiendo la elasticidad del hígado y mediante tests serológicos de libre uso.
• Se deben definir valores específicos de estos procedimientos, no referirlos a los de la biopsia
• La biopsia hepática está indicada si la evolución del paciente no se corresponde con los resultados, si hay discordancias mantenidas entre los valores de estos procedimientos o, si en algún momento hay dudas diagnósticas