i) .“”- .. - 148.206.53.84148.206.53.84/tesiuami/uam20685.pdf · caz en el dian6stico temprano...
TRANSCRIPT

., , ~ _ ” -..,.I) -.._ - _--. .“”- lil “ . ._._, . .... , ... .,. .
. .
UNIVERSIDAD AUTONOMA METROPOLITANA
PLANTEL IZTAPALAPA
, MEDICINA I V
//;íCANCER CERVICQ UTERINO
ALUMNOS 2
.,&ANA ROC10 VICTORIA ROMERO 86228042 MIGUEL ANGEL RODRIGUEZ CAMPA 86333373
PROF.- ALFONSO MARTINEZ ORTIZ
Juba 90.
MARCO NEDICQ
UNIVERSIDAD AUTONOMA METROPOLITANA
PLANTEL IZTAPALAPA
MEDICINA I V
CANCSR CERVICO UTERINO
ALUMNOS : DIANA ROC10 VICTORIA ROMERO 86226042 MIGUSL ANGEL RODRIGUEZ CAMPA 86333373
POFRe- ALFONSO MARTINEZ ORTXZ
" . - s . . . . . ,.., , . . . . , - . ., ~ , , , , , , , ,.,. 1~~ ...... ;. _",.e- r .,
.-
..
r -.
- ..
--. - .. . ..
. i.
~ ..
.-.
...
~ ..
. . I
. .
.. .
. .
.
L "
I N P I C E PAG .

E l cáncer cervicouterine constituye un problema de salud de
importante magnitud en nuestro pals, que se manifiesta por ui)
na tendencia ascendente como causa de mortalidad y de gran
trascendencia social a l afectar a las mujerss en su etapa mds
productiva y relevante dentre del núcleo familiar.
Por fertuna, l a acceskbilidad del útero y las caracterfstic -
,,. .
as bioldgicas de l a evoiuci6n de esta patología, as í cemo e l
desarrollo de técnicas diagndsticas y terape6ticas, hacen vu1 - nerable e l padecimienta s i &stas meaplican oportunamente en
sus etapas incipientes o preciínkas.
Es indudable e l valer de l a citelogía exfeliativa en e l dia - gnostico del cáncer cervical. Su alto grado de sensfbilidad y
especifidad, aunad@ a su sencillez y bajo costo relativo ori-
ginan que en l a actualidad sea censiderado el método más efi-
caz en e l dian6stico temprano del cáncer invasor del cérvix,
as í como de sus precursores: e l carcinema ill '11 y las displ
asias.
Las autores de numeresos estudios en diversos países coinc
iden en afirmar que l a implantacih de programas masives de J
deteccih con e l método citoibgice, que aseguren coberturas
impertantes de l a peblacih en riesgo, y se apeyen en un sic4
tema adecuado de tratamiento y contrel de l a patología cervi-
ca1,contribuyen censiderablemente a l control del cáncer ervi - ceuterino, que se ref le ja en l a reduccib de las tasas de mer - talidad per esta causa.

De l a s muchas responsabilidades asumidas por e l ginecblo-
go moderno, quizá ninguna es tan importante como l a detección
de l a s neoplasias l o mas temprano y osortuno posible.
2h es t e trabajo se c r i t i c a n va r i o s métodos diagndsticos
corrientemerite empleados; s i se comprenden todas sus l i m i t a - ciones y sus ventajas y s e u t i i i z q n apropiadamente, podría
s e r pos ib l e aproximarse a l a meta de aue "nadie debería mor iP
de carcinoma de cérv ix .
La introducción de l a c i t o l o g i a en l a prác t i ca ginecoló-
g i c a ha cambiado s ign i f i cat ivamente l a deteccibn de cáncer c e r
v i c a l . Este cáncer, actualmente se diagnostica en estadios
c l í n i c o s mucho más tempranos. Además l a c i t o l o g i a es capav de
detectar a l o s precursores de l c b c e r invasor: e l carainoma i n
s i t u y l a d i sp las ia ; por l o tanto es indudable su va l o r en l a
deteccidn c i t o l 6 g ~ c a ; s in embargo, es ta sentencia no se ha cum
p l i d o en poblaciones que en su t o t a l i d ad han s ido examinadas
por es te método una vez a l ano. Bryans y colaboradores (4) en
un extenso programa de detec,ción c i t o l ó g i c a en Columbia B r i t& - -
n i ca , mostraron que l a inc idenc ia de l Carcinoma c e r v i c a l inva-
so r fue de 3.5 X 100,000 mujieres estudiadas, comparado con l a
tasa de 24.1 X 180,000 en poblaciones de mujeres no estudiadas
Unil~garainoma c e r v i c a l no se desarro l la en un.,año; por l o tanto
l o s cánceres c l í n i c o s que se presentaron en l a población estu-
diada previamenze por c i t o i o g í a , indican l a tasa de f a l s o s ne-
ga t i vos de e s t e método. A causa de es ta c i f r a , l a inc idenc ia
de carcinoma invasor de l c e r v i x nunca puede ba j a r a cero.
-
-

DATOS ANATOMICOS DEL TRACT0 GENITAL FEMENINO
El tract0 genital femenino astd compuesto por l a vulva, l a va - gins, e l dterc, las trompas de falapio y les evarios.
.
, .
.
. .
. .
. <
RECTO
VAGINA
Lp vulva, que representa la parte externa, es una estructura e
compleja formada por los siguientes e1ementes:l) mente de venus
, 2) labies mayores, 3 ) labies Rencores, 4) cl ftcr is , 5)vestfbu-
Is, 6 ) meate urinario, 7 ) orificia, vaginal, 8) hiaicn
vfrgenes) y 9) glándulas vulvwaginales.
MONTE DE VENUS
ES un mntfculo de g ma, cubicrte , : el y situ
(en las
d F r e -
ima de l a sfnfhsis pubiana, en l a parte más inferier de l a pare
cd abdeminal anterior.
-3 -

~
. ..
I
” .
<. .
LABIOS MAYORES
Sen dos pliegues lengitudinales salientes, fermados por tejid@
ad ipsa recubierto de pie& que en sus partes externas se encue - ntran cubiertos de vello. Durante l a pubertad se desarrollan c?
nsiderablemente y despugs de! esta etapa se extienden hacia atrá - s, en direccidn a l perinee; s i se separan en l a parte pasterior
se puede observar una comisura ligeramente saliente, llamada ha - r qu ill a.
LABIOS MENORES
Son dos pliegues Be direccidn anteroposterier que se observan i)
a l separar les labios mayores. En l a parte anterior se subdivid - en y cubren con una horquilla e l glande del C l f t Q r i S , farmando
una cubierta llamada capuchbn, mientras que l a otra ho j i l la pas - apor debajo del glande para formar, con l a del lado epueste, e l
f reni l le del cl íteris. La piel que cubre los labios menores est* - S provista de follculos piloses, pero es muy rica en glándulas
sebáceas.
CLITORIS
Es un pequeña brgane, eriktil de forma cilindrica, que está for-
- 4 -

mads por un glande, un cuerps y dos raíces; e l glande de aproxi - madamente ti a 8 nun de didmetro, es l a única porcidin visible de
6rgano desde e l exter iw .El c l í ter is está formado por tejids
erkctil en e l quo abundan canales venesos rodeados de gran can-
tidad de fibras musculares lisas.
VESTrBULQ
SE llama vestíbule a l a excavacib navicular que se observa a l
separar los labios de l a vulva; en é l se encuentra el s r i f ic io
vaginal y per delante de este e l meato urinario. En l a mujer v i
rgen, e1 ~ r b f i c i e vaginal se encuentra parcialmente 9ClU idQ per
e l himen, que es una membrana farmada per tejido caneetivo f i r -
me y cubierta por un epitelio plano estratificado que frccuntem
ente tiene forma lunar o semilunar, pero tambian puede ser crib
iforme; en casos anermales puede permanecer imperforado y ocasi
mar retencibn del f lu jo menstrual.
-
- -
-
MEATO URINARIO
Es e l pequen@ ori f ic io externo de l a uretra, de forma triangul
ar 6 de hendedura. Frecuentemente se e-bserva a cada lado del me
ato una pequefia depresi6n en l a que se encuentran las llamadas
- -
- 5 -

glándulas meneres del vestfbdla. La uretra, en su posición prox - imal, se encuentra revestida por epitelio de transicibn; su per - cidn distal está cubierta per epitelio plano estratificado no Q
c$rneo.
GLANDULAS VULVOVAGINALEC O DE BARTHOLIN
Son glándulas arracimadas, dispuuestas en lbbulos que se encuen - tran a cada lado del or i f ic io vaginal, especialmente durante e l
coito, su funci6n censiste en secretar mucasidad para lubricar
e l s r i f i c io y e l conducto vaginal. El C@ndUCtQ principal de l a
glándula está cubierts, por epitelio de transicinn.
TROMPA DE FALOPIO &#@PODEL UTERO
CAVIDAD ENDOMETRIAL FIM5RIAS CUERPO UTERINO CERVIX
VAGINA
.- I .
. ,,
VAGINA
La vagina es un conducto musculomembranoso que une l a vulva a
a l btero y se relaciona anathicamente con l a vejiga por delani
e y cen e l recta hacia atrás ; mide entre 9 y 10 cm de longitud
y se dirige hacia arriba y hacia atrás desde su extremidad vul-
var hasta su extremidad uterina. E l extremo superimr, a l di lat - arse, forma e l f b rn ix en e l cual hace pretrlsién l a porcidn vag
inal del cervix uterine, e portio; las areas demarcadas por e l - f ' 6rnix y p w e l cgrvix fornaao%os fasndos de saco vaginales later - ales, anterior y posterior, siende eke último e l más profunds y
el s i t io donde se acumulans las cklulas exfoliadas y las secreci - enes de las glándulas utcrinas; e l fendo de sac@ vaginal pester - ior tiene también interksequirúrgico por constituir una vfa fác - il de acceso a l a cavidad abdominal. En l a mujer virgen l a muce
sa de l a pared anteriar de l a vagina presenta una serie de arru
gas transversales y un pliegue central longitudinal que l e dan
e l aspecto de "árbol de l a vida"; en l a multfpara, cuyo conduct - o vaginal está claramente distendide ne hay pliegues. La pared
de l a vagina esta fermada por tres capas: l a mucosa que tapiza
- -
e l canal vaginal es l a más interna; por debajo de l a mucosa se
encuentra l a túnica muscular formada por dos capas de músculo &
l iso; l a capa fibrosa es l a más externa de tedas y 4 -17-
por te j ide conectius pehians.
L .
. "
., ,
. .
. <
UTERO
E l 6tere es un lbrgane hueco, de gruesas paredes musculares, s i t
uade en l a pelvis entre l a vejiga per delante y el recto por de - tras, sostenido per una serie de ligamentoa y por hojas del per - itoneo que se reflejun y se extienden hacia los lados del 6tero
y se conocen c-e paramtrios dereche e ircquierdo. Tiene forma
de pera o de pi rk ide invertida; en l a nulípara mide alrededu
de ocho o nueve centfmetros de longitud, seis centímetros en su
parte d s ancha y unos cuatre centfiactros de espesor. Se encuen - tra inclinado hacia adelante y hacia abajo.
E l btero esta fumado de dos partes: e l cuerpe y e l cuello. En
l a mujer pre*ber y en l a saclnop&usica, e l cuerlw, es muy pequeño
pero durante l a edad reproaluctiva suele ten- pulpmen aumentado
a consecuencia de l a eatimúacibn ovQrica."
La pared del atere est& formada por delgadas capas de nñsculo
liso capaces de aumentar considerableumnte su peso y tanafie du-
rante e l enbaraso. La Wrcibn superier del cuerpo se denomina
fondo o fundus; e l hgu lo que marca a une y otro lade e l erigen
aparente de l as trompas recibe e l nombre de cuerne. E l c&rvix o
es una estructura tubular de aproximadamanta cuatro centímetros
de longitud y trea centímetros de diámtro; de su longitud total - (3-

. .
cerca de l a mitid se encuentri cerca de l a vaqini y constituye
1 i pertie, e perción va9inii del cérvix; e l resta est i ecuíto
per l a pared vaginii y se centinóa cen e l cuerpo del dtera.
US reiacienes anitómicis del c d n i x sen con ii vegiga anteriuc - mente y c m wnbos urcteres hacia los lados.
Las paredes del 6tere fuman una cavidad que sigue l a f o rm del
cuerpo uterine; es cbnica, su base corresponde a l fend. y e l
vCrtice a l esteurn interne u ar i f ic ie cervical interne. La cavi-
dad del cuerpo uterino se cbnece coii). cavidad endometrial y se
cemunica cen e l can81 endocervical hacia abaja, La abertura del
canal endecervical en l a v8jiAa se c m e e c « w osteuffl extern. u
u b f i c i r aervici l &%terne, y elbpinte de transicibn del canal e - ndocervical y l a cavidad endemetrial es e l osteum interne men-
cion ado.
La mucesi del cuerp uterine recibe e l nombre de endometrio; e l
egite l ie endocervicil recubre e l aanal correspondiente. El estr - 0 ~ 1 esta ferrnado per tejido conective. U túnica muscular, for-
mada par fibras musculares lisas, entrecrumdas, recibe e l neut-
bre de Biiametrio. La tónica serese está formada por e l peritene
o que cubre tedo e l cuerpe uteririm;-
Las trampas de falopie miden entre eche y doce centímetros de
large par tres a cinc. centfmetras de d i h t r e , Sus extremos pr
oximaies se cemtinóm can ci cuerpo uterino, mientras que íos
-
- - 9-

..
.
. .
distales con su perci6n fimbriada se abren libremnte dentre de
l a cavidad abdeminal. A t d a su lengitud l a trwpa presenta un
estreche canal gue asegura l a csmunicacibn directa entre l a v b
gina y l a cavidad abdominal (de impertancia para l a dliscainc
cibn de infecciones e de tumeres malignos).
Les avaries, une derecho y une izquierdo, sen estructuras wei -
des que miden alrededer de cuatre H r des por des centht res .
Se lecalizan anatemicumnte en l a vecindad de l a perci6n fim-
briada de las treapas, aunque ne directamente centigues a l a luz
tubaria. Les evarios a l iyual que las trorapas se encuentran 80s
tenides dentre de l a pelvis per medie de repliegues peritutb.ít
les.
-

..
. ..
* .
- .
EL UTERQ Y LAS TRBDMPAS DE FALfbBIO
L.S ovarios, e l ótere y sus trempas, y l a vagina constituyen les
$r,rcganes internos de repr.ducci(in en l a mujer. Les wvaries se en-
cuentran en l a pared pesterior de l a pelvis, sostenidos por e l
ligamente susgenserie del @vario (que lleva les Vasos), e l ligamen - to ovb ico y una extensidn del ligamento ancho. Ea esta vista, los
ovaries han side fraccionados hasta una psici6n hwizmntai para
esclarecer sus relaciones cnn las treinpas o tubas uterinas. Las
ttowpas o tub*s,uterinas sen extensimes laterales del titer., re-
vestidas de epitelio columnar ciliado sestemdole pwr tejide cenecti
vo y músculo liso. US centraccienes rltmicas de este másculo ayu-
dan a l $vule en su viaje hacia l a cavidad uterina, y las c(5lulas
de recubrlipiento l o mantienen nutricionalmente. La trompa muestra
tres porcienes bien definidas: l a fimbria, que encierra l a s u p r f i - tie antcrier y superior de1 ovario, **atrapa*@ e l 6vuie expulsade y
1s mueve rápidamente hacia su interior; l a ampolla o perci&n nias
ancha de l a trompa y e l istmo, cuya luz se estrecha cenforme pena-
tra en l a pared uterina. E l óters es una estructura en ferma de pe
r a cuy0 cuello (cervix) entra en l a porcibn superior de l a vagina
y cuy@ cuerpe/fona¡o est$ flcrxienade (anteflexih) e inclinado ha-
cia adelante (anteversibn) sobre l a vejiga. La fiexiQn e inclina-
ci$n hacia atrás (retr,flexi(ln/retroversibm) es frecuente, parti-
-
-
- \ \ -

cularncnte en mujeres que ya han dade a luz. Esta última posici6n
del dtero ("inclinada"), s i es importante, puede conducir a una va - riedad de molestias, desde darlor hasta infertilidad. La situacibn
tambidn predispone a un ligero deslizamiento del útero dentre de
l a vagina (prolapse), ya que este pone a i dtero más e menos en e l
e je del cuelle y l a vagina. La pared del btero, como puede obser-
varse, es en su mayorfa d scu lo l i so (miornetriel recubierto cen
una capa glandular de greser variable (endmetrie) que es extrema
r
c
-
.
* ,
. .
.
damente sensible a las hormonas estr6qens y progesterena. En el
lugar donde el cervix penetra en l a vagina, se forma un canal e
fesa alrededor de d l ifendo de sac8 ar fornix vaginal). Esta &ea f
fibroelástica se expande considerablemente durante e l ceito. Justa - mente a l lade del cervix e cuerpo del útero, para e l ureter. en su
camine hacia l a vejiga, my cerca de l a arteria uterina (una rela-
ciQn importante para e l cirujano gincc6logo). Debido a l a potencia - lmnte precaria posici6n del útere, e1 sastdn ligamentario de esta
estructura es crucial. E l ligamente ancho, una capa de peritoneo,
en fmna Be s I b M a sobre e l btere, sus trampas y les Bvarias, j u r
ga e l papel de sost& mas importante, en asociaci6n con otros.

. .. ,-1
.. . c.
., . ,'. .. .
c
L.
P-
CI
r' -. r-
C..
c-
I
c
UTERQ Y TRBHPAS DE FALLOPIO
Utera: a) fendo
b) cuerw
c) cueil., canal cervical
d) aavidad utarina (endometrio)
e) miematrie
Trampas de Falopi*:
f ) istmo
g) ampolla
h) fimbria
Estructuras relacionadas: i) ligamento anche (peritoneo)
3) ligamento redonde
k) ligamente ovkice
1) ligamente suspcnserie del vario
a) arteria uterina
a. vesical superior
O ) avarie
p) vayina p?) fend. de saco
q) uretere
-13-
_L_1_L.
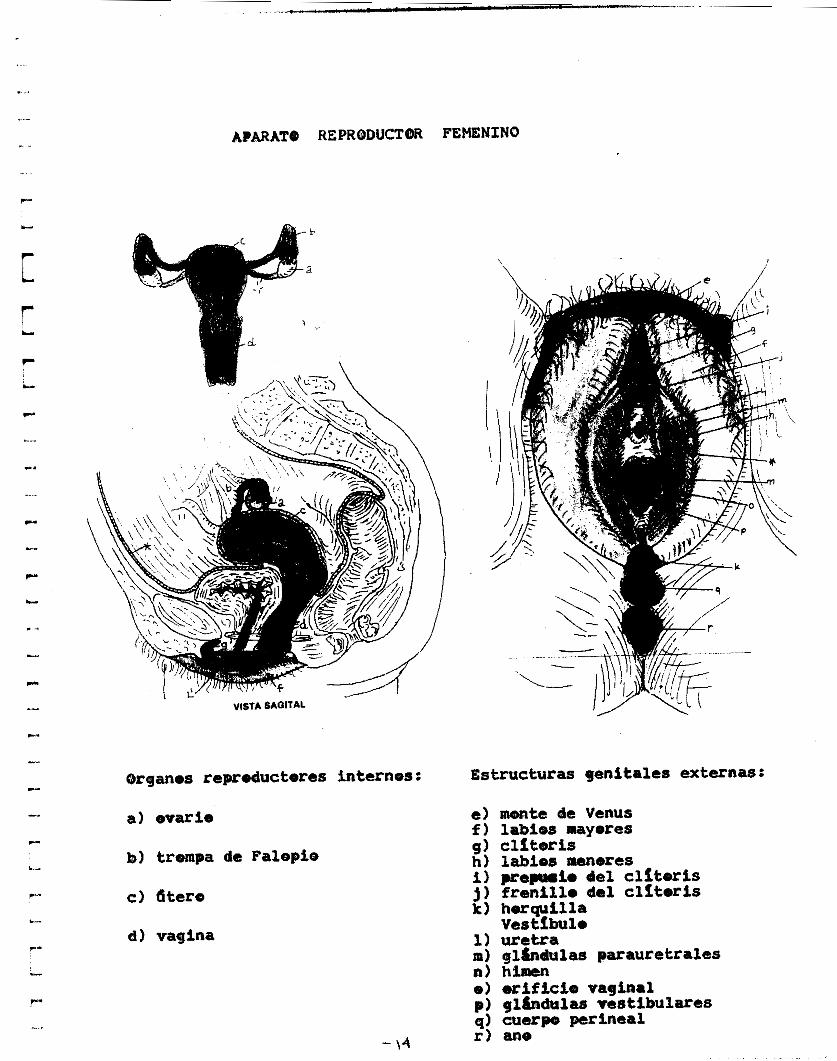
AIARATTO REPReDUCTM FEMENINO
b
a . c
cBrganes reprducteres internos:
a) ovario
b) trompa de Falepie
c) 6tero
d) vagina
- \4
Estructuras jenitales externas:
e ) mente ae Venus f ) labies mayores g) ClftcPriS h) labios menores i) prepwio del c l f ter is j) franil ie del c l f ter is k) herquilla
Vestíbule 1) uretra ni) oi&adulas parauretrales n) himen e ) u i f i c i e vaginal p) gllndulas vestibulares 9) cuarpa, perineal r) ane

E]. aparate reprducter femenina esta fermado gor partes inter-
nas y externas. E l &gane primarir de este aparate es e l evarie,
e l cual prduce las c6luias germinales femeninas (bvuies) y se-
creta las hermenas estrQSenes y pregesterana. US estrkenos son
l a principal harmma femenina y es respemsablc, entre @tras cesas,
de las características sexuales secundarias (desarrelle ale turnas,
ensanchamiente de las caderas, crecimiente del vei le Pbice, etc.
asf cemo del desarrelle de las glgndulas y cenductes del tract. rz-
prducter en l a pubertad, EI evarie, a l igual que e l testlcuim, se
origina en l a pared pesterior del abdomen (a un lade de les riiit
nes) durante e l atesarrelle fetal tcmprane. Tanibi6n desciende a l e
large de esa p a r d cele e l testfcule, pure es interrumpido tempra-
namente en su camine, per un par de l&ganbsntos hacia e l ffarie y
e1 dtero y es detenido en l a pelvis, úkere sirve c m lugar de
implantaci6n y nutxicibn de1 nueve embrih ; las tubas uterinas e
trompas de Falopie sen e l vehícule para l a cenduccibn del hueve - fertiiiaado e ne- hacia e l dtere. La vagina, una vaina fibrmtuscu-
lar, recibe e l semen preveniente del pene, le transmite a l dtero y
actda came canal del porte, del dtere a l exterior, para e1 recida
nacide. A pesar de que les @varies y les testículos cempwten un - e
rigen c d n , es1 c m las estructuras genitaies externas aascuii-
na8 y fedninas, e l dtere, sus trompas y los des tercies superleres
- \5 - - ~

.." -. .
*. ,
-. .
i-
r- 1..
.--
._I
.-.
de l a vagina se originan de un sistema de conductas my diferentes
a ZWI del VU&.
El monte da Venus y los labios mayores canparten una estructura cz
d n r a1 tejlde fibroso y adiposo. Los labies menawes d S PcqUQñOs
y pigmentades confuibuyen a formar e l capuchb del cl fter is hacia
l a parte anter ia y en l a parte pes te r i s se unen a les labiss me-
yores feriaando una horquilla. La hendidura entre las labios menores
es el v e s t h ~ l o y recibe enSf&c&os de l a uretra corta, l a vagi-
na y los pqueflos conductss de cuatre glcndulas. Las erif icios de
l a uretra y l a vagina se abren aquf: nernulmcnte se encuentran co-
lapsados y cerrados. E l himen es una c a y de aucasa que cubre col^
pleter e incompletamente e l csrificio vaginal en l a mujer ndbil. A
menudo se pueden ebservar restas de él en l a mujer sexualmente ac-
tiva. E l cuerpo perineal, por debajo de l a piel, en e l lugar indi-
cado, es una masa fibremuscular que sirve cem tendbn certral a un
ndmero de ~ s c u l o s purineales tealos los cuales ayudan a estabilizar
y dar sostbn a las estructuras petrineales y a l titer..
C I T O L O G I A E X F O L I A T I V A
La citelegfa es una ciencia, rama de l a bieiogía que -.mo e
su ncimbre l e indica se encarga del tratado de las células. La
citolegía diagnbstica es e l &te de l a interpretaciba de las
cglulas del cuerpb humana, descamadas empentáneamente de las
superficiees epiteliales u obtenidas de los tejidas mediante
diversos procedimientos clínices.
HISTORIA
La descripcibn del contenido celular del calostro hecha per
Denn& en 1838 fue seguida de las de Pouchet en 1847, quién RH
ncienb l a aparicibn de células en l a secreci6n vaginal. En 18 - 43 Walshe encontré tejidos malignes en espute, y Tessenbach en
lavados gástrices hacia 1882. En 1853 Donaldson rec@neci$ chi1 - ulas malignas en líquidos de derrames de cavidades, mientras
que b a l e , en 1860, las recenecid en e l esputo. S in embargo,
l a apiicaci6n de l a citología en problemas diagnésticos se ha
basade en e l trabaje de George )apanicolacñr, realizade en col - aberaci6n cam Stockard en 1917 que aiencien6 los cambios c í c l i - ces ebservados en las cblulas exfeliadas del epi-lie vaginal
, dands fundamente para e l use subsecuente del mét@dQ para ce - necer l a funcih hermonal. En 1928, Papanicolaou describi6 e l
papel del fretis vaginal dn e l diagn6stice del cáncer, y en19
43 €1 y Traut publicaron su trbajs clásica E l diagnbstice del
cáncer uterine por medio del frotis vaginal.
FUNDWENTO
Come un mbtode diagnibtico l a citología se basa en e l heche

,.,. ,... . .
de que las cdlulas exfoliads o colectadas de una superficie o
colectadas de una superficie, reflejan muchas de las caracter'
ísticas del tejido del cual previenen.
La exfoliacidn espentánea de las células es el resultado d¿
continue crecimienta del epitelio, cuyas células más superfic - iales son centinuamente descamadas y rempiazadas per células
m8s jovenes. Las células descarnadas meden acumularse en las
diversas cavidades del cuerpa , cemo suceden en l a vagina, de
dende pueden obtenerse para e l examen micrescopico.
Aplicacidn
En l a actualidad , l a tconica citelbgica se aplica pkincipa - lmente en e l diagnhtico oportuno del cdncer, especialmente
en e l trctat genital femenino . S in embargo e l rn6tsdo puede se
r usado para etres prspbsites,
Las ventajas de l a citologfa exfoliativa para diagnbstics
son las siguientes : - En l a mayoría de les casos se puede obtener especímenes a
decuades con un rnfnime, de mblestias para e l paciente.
- En algunes sitios, el uso de l a citología puede hacer in:
ecesaria l a biobsia.
- Las técnicas de bbfencih de las muestras usualmente re%
ieren de POCC equipa de bajo csste.
- La c i tb logh puede revelar anormalidades celulares en eta
pas tempranas del cáncer cuande a6n no sen aparentes a l a
exploración clínica, i o que significa un me#er pronhtico pa-
r a l a paciente.
- \a -

- La considerable sensibilidad del método para ref le jar al;
eraciones en el esjrddo hermana1 unida a l bajo costo y a l a f a - cilidad de hacer exhenes seriados hacen de l a CitQlOgf8 e l
método ideal para estudios a largo plazo.
Desafortunadamente , l a citcslegfa diagnbstica tiene también
limitacisnes y desventajas pues si se desconocen e ne se teun
an en cuenta, fácilmente se puede abusar del d t sdo con res-
tados negativas. E l primer pase es centar con una histeria c l ’ - fnica adecuada que propercione dates erientadores relacionado
s con e l padecimiente y les antecedentes de l paciente; el sig
uiente, es l a ebtencibn y fi jacibn adecuada de los especfmen-
es para estudio; ecacienalmente l a f a l l a en e l diagn6stico ac - urre per l a inaccesibilidad de un kgano para hacer una toma
directa, & bién, s i e l material ne se obtiene del s i t io adecu .. ado Q no se siguen las instrucciones para una fijaci6n cerrec
ta, E l manejo y process que se da a l es&cfraen en e l labmat?
rio también es importante ya que se puede alterar l a calidad
del material y disminuir las pesibilidades de emitir un diagn*
fiestice cerrecte. Otro problema es l a necesidad de hacer un
cuidadese escrutinio micr@scopicp de l a totalidad de lamuesta
, pues ecasionalmenteun hallazge anormal permite hacer e l dia - gnbstico inmediatamente pero en l a mayoriade los cases es neg
esario examinar tatalmente les especimenes para llegar a un
diagndstico definitivo; esta actividad requiere tiempo y fre-
cuentemente resulta mmltona.
-
Per 6itimo existen faltas inherentes a l método. Laopinibn #
-\3-

f inal del observador es una cembinacibn de l a informacih der - ivada de l a histmria c l h i c a del aspecto general del frotis y
de l a apariencia individual de las c&lUlaS o de los grupcps ce - lulares; s in embargo en e l diagn6stico del chcer nunca s - p:
ude estar seguro de que un informe negativo no se deba a una
lesi6n innaccesibae o a una toma de muestra inadecuada; t a l
informe negativo can ausencia de sospecha clínica, excluye ua - a investigacibn ulter im que podría pejudicar a l paciente.
E l informe positivo tiene tambih sus limitaciones, pues - e
1 tipo y l a diferenciacibn del tumor a menudo se estiman cit6 - lbgicaniente, pero puedan ser confundidos con tumores que muez
tran varios grades de diferenciacien. E 1 s i t io geegráfico
del turner piede ubicarse cuando l a toma de l a muestra es dire
cta, no así cuando e l material procede de cglulas exfoliadas.
Laprecencia o ausencia de invasi6n no se puede asegurar c i t - ologicamente, aunque e l aspecto y distribución de las células
pueden sugerirlas. Por ta l motivo, a un diagnbstico positivo
siempre debe seguir l a confirmación histoibgica antes de que
e l paciente se someta a una cirugia mayor o a una radioterapia

Li
c
.. .
."
. , -
I
c
..- 1 .
L
i-
c
L"
-.

Li
r ._ I .I
-22-
t t
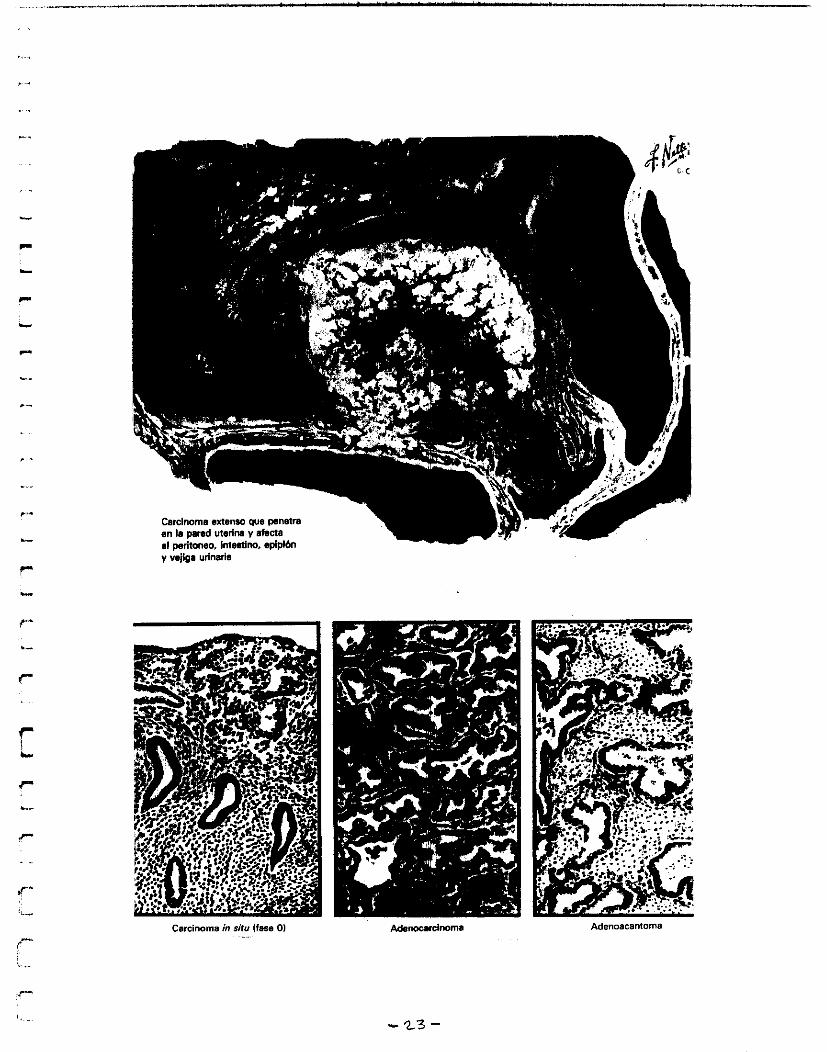
y wjipa urinaria
carcinoma in *it" (fase o1 Adenoacantorna
- 2 3 -

I
p"
- P
P
L
P
L
F
. ..
r -
. ..
I -
- 2 4 -
L.
r i i
L
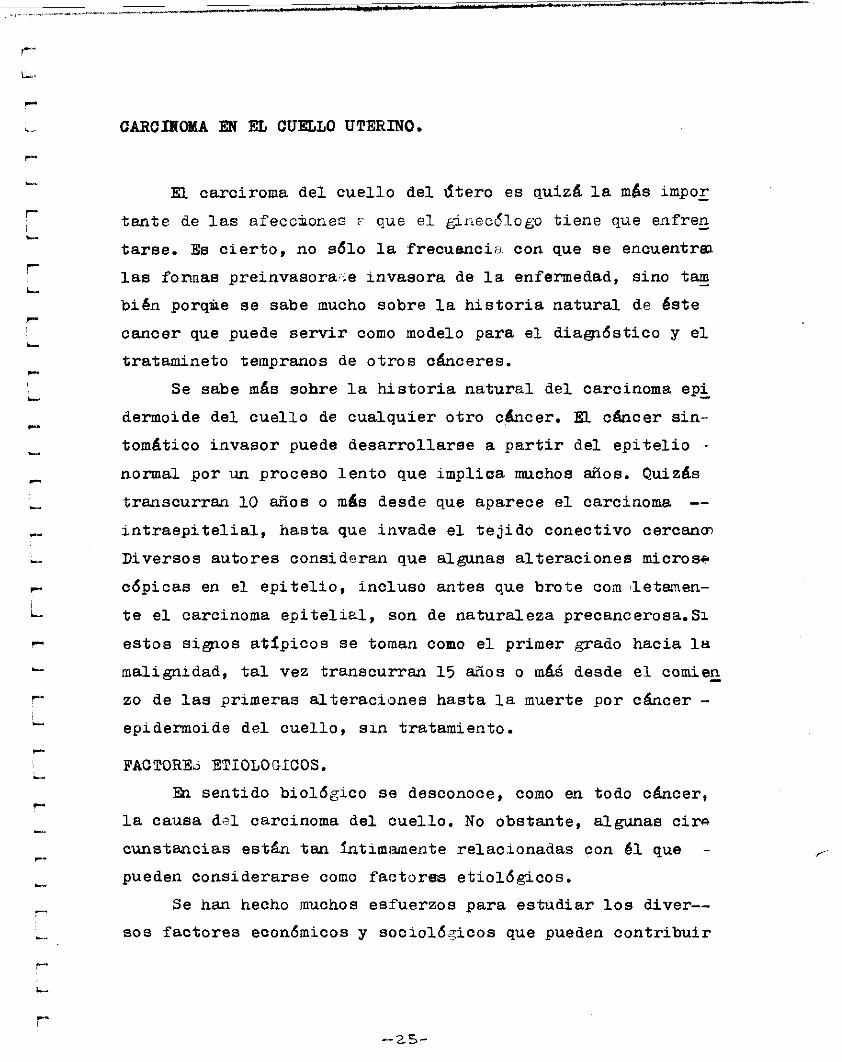
CARCIBOMA EN EL CUELLO UTERINO.
EL carciroma d e l c u e l l o del ú t e r o e s quizá i a m8s impox
t a n t e de l a s afeccjiones i que e l ginecdlogo t i e n e que enfren - t a r s e . Es c i e r t o , no sdlo l a frecuanciii. con que s e encuentra2
las fonnas preinvasora,5e in.vasora de l a enfermedad, sino tam - b i 6 n porqke s e sabe mucho sobre l a h i s t o r i a n a t u r a l de é s t e
cancer que puede s e r v i r como modelo para e i diagfidstico y e l
tratamineto tempranos de o t r o s cánceres.
Se sabe más sohre l a h i s t o r i a n a t u r a l del carcinoma epi
dermoide d e l c u e l l o de cua lquier o t r o c h c e r . EL c h c e r s i n -
tom4tico i n v a s o r puede d e s a r r o l l a r s e a p a r t i r del e p i t e l i o -
normal por un proceso l e n t o que i m p l i c a muchos años. Quizás
transcurran io a ñ o s o más desde que aparece e i carcinoma -- i n t r a e p i t e l i a l , hasta que invade e l t e j i d o conect ivo cercana,
Diversos autores consideran que algunas a l t e r a c i o n e s microsa
cdpicas en e l e p i t e l i o , i n c l u s o a n t e s que b r o t e corn 'letamen-
t e e l carcinoma e p i t e l i r t l , son de natura leza precancerosa.Si
e s t o s sisas atfpicos s e tornan como e l primer grado hacia l n
malignidad, t a l vez transcurran 1 5 años o m46 desde e l comien - zo de l a s primeras a l t e r a c i o n e s hasta l a muerte p o r cáncer - epidermoide d e l c u e l l o , s i n tratamiento.
FACTOREd ETIOLOGICOS. En sent ido b i o l ó g i c o s e desconoce, como en todo cáncer ,
l a causa d e l carcinoma del cue l lo . No obstante , algunas c i r n
cunstanc ias e s t & t a n íntimamente re lac ionadas con 61 que -
pueden cons iderarse como factores e t i o i ó g i c o s .
Se han hecho muchos es:Euerzos para e s t u d i a r los diver--
so8 f a c t o r e s económicos y s o c i o i 6 . ~ i c o s que pueden c o n t r i b u i r
-2s-

. .-
r-
L
c
P-
L
c
a ’ l a frecuencia var iab le de l c&ncer ce rv i ca l . Todos co inc ida
en que e l cáncer c e r v i c a l es relat ivamente raro en l a mujer
judfa; Wynder y colaboradores indican que su frecuencia es - aproximadanente l a octava par te de l a que se observa en gru-
pos s imi lares de genita les. Rothman y colaboradoses, en una
r e v i s i ón de e s t e tema, basada en e l riqulsimo material. de l - hosp i ta l Mount Sinai , de Nueva York, encuentran que e l c&n-- c e r de l cue l l o uter ino es nuesre veces más frecuente en muje-
r e s na judías que en l a s judfas. %I i o que se r e f i e r e al car _.
cinoma endometrial no s e observan d i f e renc ias de frecuencia
en ambos grupos.
La baja frecuenaia del. cáncer c e r v i c a l uter ino en muje-
r e s judías ha hecho sospechar que e l c o i t o con un varón s in
c i rcuncis ión puede actuaren a l m a forma como in f luenc ia cau
sa l , quizá a base de poca h ig iene de l pene, y se sospecha de
i s importancia que pudiera tener e l esmegma, según señala .
Fischer. Se ha observado recientemente e l desarro l lo del -- c‘ncer c e r v i c a l en algunas cepas de ratones sometidos a est&
muiación durante 1 4 meses por l o menos con esmegma humano.
Wynder y colaboradores han publicado una amplia r e v i s i ón so-
bre l a importancia de diversos fac tores extraños y han l l e g a - do a i a conclusión de que ]-a carcinogénesis puede considerar - se solamente como resulatdo de var ios estimulos endógenos y
exógenos. Hay que tener siempre presentes fac tores como pro-
miscuidad sexual, Circuncisión incompleta y f a l t a de adheren - c i a a l a doctr ina mosaica, que impide e l contacto sexual. du-
rahte una semana después de l a mentsruacibn. Sin embargu Jo-
nes y colaboradores no han observado d i f e renc ias notables en
e l c4ncer c e r v i ca l , sea cual sea e l estado de c ircuncis ión - de l compaiiero. ih un informe muy importante de l a universidad
-26-

de Kadrás, Rewell ha comprobado igdal f recuenc ia de cáncer - c e r v i c a l en musulmanes (varones con c i r c u n c i s i ó n ) e hind6es ( s i n c i r c l u i c i s i b n ) . L i l i e n f e l d y Graham estudiaron rigurosa-
mente l a supuesta r e l a c i ó n e n t r e c i r c u n c i s i d n y cáncer c e r v i - cal demostrando que había un 34.4 $ de desacuerdo e n t r e l a - información de 2 1 3 varones a c e r c a de &u c i r c w c i s i ó n y l a - verdadera s i t u a c i ó n del prepucio según demostraba e l examen.
En resumen, solo caben suposiciones a c e r c a de l a supuesta r e - lac ión e ti o16 gi c a.
Por o t r a p a r t e , durante l a &tima década una media doce - n a de estudios importantes han examinado l a r e l a c i ó n entre -
e i c o i t o o e i matrimonio y e i cáncer c e r v i c a l . Todos los es-
tudios concuerdan en que e l r i e s g o d e l cáncer c e r v i c a l sumen - ta con e l matrimonio temprano o e l primer c o i t o a edad teme-
prana . Rotkin ha estudiado e l problema nuevamente y sus re7
su i tados parecen i n d i c a r que de los 1 5 a l o s 20 años e s e l - período s u s c e p t i b l e en que l a primera r e l a c i ó n sexual y las
s i g u i e n t e s predisponen u l ter iormente al cáncer. El tiempo - medio d e l periodo de l a t e n c i a entre e l primer c o i t o y e l des -
cubrimiento de cáncer fue de unos 30 arios. Ponen de r e l i e v e
l o s f a c t o r e s sedalados p o r diversos a u t o r e s , como pobreza, -
por ejemplo; c o i t o , casami!ento y embarazos tempranos; Rewell
tambdn s e n a l a que en l a I n d i a l o más f recuente e s que las - mujeres s e casen entre los 1 4 y 1 5 años, y que en e l l a s e l - c á n c e r s e descubre unos diez años a n t e s que en l a edad acos-
tumbrada.
Durante anos s e ha t e n i d o l a impresión de que las muje--
r e s con h i j o s t i enen mucha mayor tendencia a s u f r i r cáncer - c e r v i c a l que l a s o l t e r a . Indudable:nerite, l o s datos más impre - s ionantes a i respec to fueron l o s proporcionados por Gagnon,
-. 21-

quien, en una rev i s ión de l a s h i s t o r i a s y c e r t i f i c ados de - defunciiín de no menos de 13 O00 monjas canadienses, no logró descubrir un s o l o caso de c h c e r ce rv i ca l . Por o t r a parte, - un estudio más rec i ente de Tome sobre un n h e r o s im i l a r de
mujeres c é l i b e s reve l6 s e i s casos de carcinoma del cue l lo , - aunque este dato representa, frecuencia extraordinariamente - baja. Considerando nuestra experiencia con algunos hospita--
l e s catb i icos , y l a de var ios autores de f i l i a c i o n e s r e i i g i o - sas similares, no descubrimos uno solo di: t a l e s casos hasta
que finaimente ocurrió uno.
Sin embargo, l a monja que l o su f r í a provenfa de c i e r t a
casa que aceptaba muchachas jóvenes, y e l in te r roga tor io di-
rec to efectuado de esta mujer jóven, que colaboraba bien,re-
ve16 que en su v ida pasada habfa tenido contactos sexuales.
Por l o tanto, es muy probable que e l tener h i j o s per se
no es acontecimiento causal importante, sino más bien l a ex-
pos i c ión sexual. "1 este sentido, e l carcinoma epidermoide - de l cue l l o puede considerarse una enfermedad venérea.
Estudios epidemioi6gicos han culpado diversas o t ras c i r - cunstancias que se acompañan de carcinomas cerv i ca l es de po-
co o mucho pe l i g ro . La demostración epidenioiógica es esen--
c i a1 y básicamente circunrbt;ancial. Por l o tanto, debe u t i l i ?
zarse e l sentido comb al i .nterpretar l a in fomacibn. Asl l a
in fomac ibn de l cuadro s iguiente r e su l t a muy interesante, p-
r o es una cosa muy d i ferante admitir una o más de estas ca--
r a c t e r l s t i c a s como causa de l a enfernedad. Se t r a t a es te pun - t o en un trabajo sobre r e l ac i ón entre tabaco y carcinoma de
cuel lo . Sus conclusiones son ineteresantesr I* Los resultados
indican que habfa una a s o c i a c ~ ó n s i g n i f i c a t i v a entre e l em--
p l eo del tabaco en rapé, el. tabaco mascado, o ambos, y e l --.

cánc(?r do los g e n i t a e s femeninos, y que los cigarri l los no- guardaban r e i a c i d n con l a enfermedad estudiada’! Hecho i n t e r - - s a n t e , s e consideraba seriamente que e l rapé y e l mascar tsc
baco pudieran t e n e r alguna r e l a c i ó n con l a causa. ¿Puede - c r e e r s e que e l tomar rapé y nascar tabaco son a r e n t e s cau - saLes? Tampoco cabe admitir que e l a c u d i r a los s e r v i c i o s
r e l i g p o s o s PO s i mismo e v i t e , como si di jeramos, l a enferme-
dad, segun s u b i e r a deducirse de l a información del cuadro.
Grupos de poco p e l i g r o
Mujeres musulmanas (kmet y colaboradores, Wynder y colabora-
dores , 1954) Mujeres amish
Mujeres judias (Haenme1 y Hil lhouse, 1959;kenaway,1948) Mujeres advent i s tas del sépt imo d í a (Lemon y colaboradores,
1954; Wynder y colaboradores, 1959) Mujeres inmigrandee i r l a n d e s a s ( H a e n s ~ e l , 1961)
Mujeres inmigrantes italianas (Haenseel, 1961)
Mujeres pro$estantes y católicas que acuden regularmente a
los s e r v i c i o s r e l i g i o s o s (Naguib y colaboradores, 1966)
Mujeres de s i t u a c i o n economica alta (Dorn y C u t i e r , 1959) Mujeres de medio rural. (Levin y colaboradores , 1960)
Grupos de gran p e l i g r o
Mu j e r e a . de Puerto Rico (Haenseel y Hillhouse 1959) Inmigrantes mexicanas (Haenszel)
Mu j e r e s negras
Reclusas de una p r i s i ó n femenina ( P e r e i r a ) (Haenszel y Hil lhouse )
-29-

P r o s t i t u t a s ( R o j e r l ) P a c i e n t e s de una c l í n i c a de enfremedades venéreas (Greene)
kíujeres de n i v e l económico b a j o (Dorn y C u t l e r )
Mujerees de medio urbano.
Los datos epidemioldgicos , como s e ha dicho, implican
una exposic ibn sexual temprana, especiaimente con compderos
d i v e r s o s , como causa e t i o l d g l c a importante. E s t o , naturalmen - t e ha hecho sospechar que pudiera i n t e r v e n i r un agente i n f e c
c ioso . En al& momento s e ha sospechado semen, esmegma, tri - comonas, CUamydias y condilomas. Coppleson y colaboradores
han presentado pruebas que sugieren que e l agente e t i o l d g i c o
e s e l DNA d e l espermatozoide.
Al p a r e c e r , e l v i r u s d e l Herpes simple de t i p o 2 s e re-
l a c i o n a claramente con e l c á n c e r c e r v i c a l , pero & no s e ha
comprobado si e s una r e l a c i ó n de causa y e f e c t o más que l a - i n c i d e n t d de un agente i n f e c c i o s o comilui en mujeres sexual--
mente a c t i v a s .
TIPOS ANATOMOPAMLO GICOS.
Hay dos t i p o & p r i n c i p a l e s de c h c e r c e r v i c a l , que nacen - respectivamente de las dos c l a s e s de e p i t e l i o que recubren
e i c u e l l o , Se recordará que e l e p i t e l i o que t a p i z a l a super-
f i c i e ex terna o vaginal de l a porcidn vagiuiai de l c u e l l o pey
t e n e c e a i a variedad pavimentosa e s t r a t i f i c a d a , que s e c o n t f - nua con e i e p i t e l i o pavimentoso e s t r a t i f i c a d o de l a vagina.
De 61 nace e l carcinoma de cdlulas pavímentosas o epidermoi~:' - de. P o r o t r a p a r t e , e l e p i t e l i o c i i i n d r i c o del conducto c e r - v i c a l o r i g m a al adenocarcinoma de l c u e l l o . Las l e s i o n e s de
c é l u l a s escanosas corresponden a un 90 5 de l t o t a l de los -

cánceres c e r v i c a l e s , aunque en l o s úl t imos &os los adenocax
cinomas const i tuyen una proporción cada vez mayor. Ambas t i e - nen malignidad mayor que e l carcinoma d e l cuerpo uter ino . Es d i f i c i l dec id i r c u a l de l o s dos t i p o s de carcinoma c e r v i c a es más maligno; no o b s t a n t e , e l adenocarcinoma, por o r i s n a r - s e con f r e c u e n c i a i n s i d i o s m e n t e en e i i n e t r i o r d e l conducto
comporta quizás un pron6sti .co mas desfavorable. Se ha comprobado que algunos tumores t i enen componentev
c e l u l a r e s de ambos t i p o s , adenomatoso y palno, y s e han c l s , s i f i c a d o de carcinoma adenoescamoso o adenoepidermoide del - c u e i i o . Ta les tumores pareoen t e n e r un pronóstico m4s s e r i o
que l o s tumores puramente de c é i u i a s p lanas o e l adenocarci-
noma. Los sarcomas de l c u e l l o u t e r i n o s e han encontzsdo muy -
raras veces y s e han observado unas c u m t o s melanomas prima-
r i o s . También es raro e l sarcoma b o t r i o i d e o , que en ocasio--
nes puede a f e c t a r e l c u e l l o pero, como se ha comentado, en - la mayoria de los casos e l d e a a r r o i i o primario ocurre en l a
vagina.
ANATOHOPATOLOGIA MACROSCOPICA.
Etapa Precifniaa.
No hay a l t e r a c i o n e s a n a t o m o p a t o l b ~ c a s características - que ayuden a i d e n t i f i c a r un carcinoma i n t r a e p i í z e l i a l d e l cue - 110 por e x p i o r a c ~ 6 n macroscbpica. De hecho, algunos casos d e
c e r v i c i t i s a r ó n i c a crean un aspecto m4s anormal que un c u e l l o con carcinoma i n t r a e p i b e l i a l .
- 3 d -

. --- ._._I_ ---
Primeros ea tadios . En sus fases m4s tempranas, e l cágcer c e r v i ca i se pre*r-e
senta i a más de l a s veces, como una pequeña l e s i ó n que as i en - t a a n i v e l de l o r i f i c i o externo o próximo a Qi, es decir , en
l a unión de l o s dos t ipos de e p i t e l i o ce rv i ca l . Aparece como
una pequeña zona endurecida y granulosa, que a l a palpación
s e perc ibe como un l i g e r o sa l i en te en r e l ac i ón con l a super-
f i c i e vecina. Ai examen con. e l espécuio, l a super f i c i e en -- cuestión se presenta granulosa y l igeramente prominente, san - grando a l menor contacto. A veces 1a:muperf icie puede ha l l a r - se cubierta en es ta temprana fase por excreencias finamente
papilares. Las porciones vecinas de l cue1l.o pueden s e r norma - l e s , pero es m4s frecuente que sean asiento de una afección
crónica infiamato r ia .
De hecho como en e l carc:inoma i n t r a e p i t e l i a l , suele re- su l t a r imposible d i s t ingu i r por simple inspección e l cáncer
invasor i n i c i a l de lesionesi benignas como erosiones y ever--
s i ones.
Estadio moderaelamente avanzado.
Desde su asiento primi.tivb, e l cáncer se propaga hasta
que abarca l a mayor parte o l a t o ta l i dad de uno de l o s la--
b i o s del cue l l o , o porciones de ambos. A medida que avanza,
muestra una de sus dos ca rac t e r í s t i cas pr incipales. Puede - p r i v a r l a tendencia papi lar , creciendo l a neo formación sobre
l a super f i c i e principalmente; de aquf que l a l e s i ó n a fecte
l a forma de c o l i f l o r , constituyendo l a variedad eve r t i da o
exof i t i ca. Por
super f i c ia l , o
dose l a l e s i ó n
induración muy
o t r a parte, quiz4 no se produzca formacidn - és ta tenga I.ugar en perueña medida, extendién - en l o s t e j i d o s c e r v i c a l e s y produciendo una
firme, a veoes pétrea, aunque practicamente
- 3 2 -

._ F-
L
r L
i-
i-
r- L..
P
-
L
siempre hay alguna uiceración. Este t i po se denomina inver-
t i d o o endof f t i co .
La i n f i l t r a c i ó n puede a f e c ta r desde e l p r inc ip io e l fon - do
pa r t i c i pa r en e l l a .
de l saco vaginal vecino, y l o s l igamentos anchos pueden -
Estadio Avanzado
sus a t i n a s fases, e l desarro l la de l proceso cancer2 so provoca una destrucción cada vez mayor de l cue l l o , al que
reemplaza entonces una cavidad excamada y ulcerada, de paré-
des ásperas y f r i ab l e s ; de aquf que de no hacerse un examen
extremadmente del icado, se produzca una hemorragia franca.
Las paredes vaginaies prdximas a i cue l l o son res i s tentes y - se hal lan induradas a consecuencia de l a i n f i l t r a c i ó n cance-
rosas. EL l igamento ancho :muestra también extensa i n f i l t r a +
c idn no sólo como resultado de i a e.:tensión de l cáncer, sino
como consecuencia de i n f i l t r a c i ó n inf iemator ia, secundaria a
l a l e s i ó n ulcerosa sépt ica de l cuel lo .
En los casos en que l a p ro i i f e rac idn es exo f i t i ca , s e - forma una masa de aspecto de c o l i f l o r que puede ocupar cas i
toda l a vagina. En esta variedad l a i n f i i t r a c i ó n macroscópi-
ca de l o s t e j i d o s vecinos pueden s e r asombrosamente escasa,.
atin en e l caso de qhe l a t;umoración c e r v i c a l sea de gran t a
maña. si progreso u l t e r i o r de i a enfermedad se carac te r i za
porque va invadiendo y destruyendo cada vez nuevas estructuw
ras, i n f i l t r ando en grado crec iente l o s ligamentos ancfios, - con bloqueo de un uréter o de l o s dos, y afectando con fre--
cuencia v e j i g a o recto. A menudo se producen trayectos f i s t u
l o s o s entre cua1esquYk-a de estos órganos y la vagina.
-
-
- 33-

c--
,afermedad metastática.
A medida que avanza l a enfremedad, hay m e t á s t a s i s en l o s
g a n e i o s i i n f á t i c o s p é i v i c o s y f inalmente en los gangi ios a6r t i c o s y d i s t a n t e s .
En l a enfremedad avanzada, también aparecen m e t 4 s t a s i s - en pulmones, hígado, t e j i d o óseo y cerebro.
Con e l empleo c r e c i a n t e de l a quimioterapia y técnicas- para r a d i a c i ó n nuevas, s e ban observado cada vez con mayor - f recuenc ia m e t á s t a s i s en s i t i o s "raros", por ejemplo p i e l , -
p r a r e n a i e s y meninges. La causa más común de l a muerte en p a c i e n t e s con c 4 n c e r cervical . e s l a obs t rucc i6n u r e t r a 1 por e l
c á n c e r p é i v i c o en crecimiento con l a cons iguiente i n s u f i c i e n - c i a r e n d . También e s común que haya s e p s i s , i n s u f i c i e n c i a - r e s p i r a t o r i a , hemorragia e i n s u f i c i e n c i . a hepát ica .
Desde hace a ñ o s s e sabe q.ue s e puede d e s c u b r i r c é l u l a s
tumorales en e l t o r r e n t e v a s c u i a r , especialmente después de
c u a l q u i e r traumatismo que s u f r a e l tumor, % todo c a s o , e l - descubrimiento dd c é l u l a s malignas en l a sangre no implica -
necesariamente que s e producirán m e t 4 s t a s i s c l í n i c a s . Por i o
t a n t o , t i e n e poco v a l o r pr"16stico en p a c i e n t e s que rec iben
t ra tamiento o s i n 61.
Tiene que admit irse c i e r t o grado de r e s i s t e n c i a o s e n s i - b i l i d a d de l huésped p a r a que las c é l u l a s c i r c u l a n t e s puedan
c r e c e r y formar un foco m e t a s t á t i c o ; de todas maneras, pare-
c e que una b a c t e r i e m i a de c É l u l a s tumorales t r a n s i t o r i a no - e s rara en muchas enfermedades neopiás icas .
c
c
I
P
L
_...
e
-34-
ANATOMIA PATOLOGICA NICROSCOPICA DEL CARCINOMA EPIDERMOIDE.
Pato genia
Como antes dij imos, se sabe m's sobre l a evoiución d e l -
carcinoma epidermoide del cue l l o que de l a de cualquier o t ro
cáncer. A pesar de e l l o , aún es motivo de controvers ia l a se -
cuencia exacta de l a transformación neopiásioa en cuel lo .
Uno de l o s hal lazgos importantes en e l carcinoma micros - tópico i n i c i a l es 4a constancia de su or igen en l a unión es-
c m o c i i í n d r i ca.
J b l a s prepfiberes, l a porción vaginal d , . l exocervix es-
t a compuesta de estroma ce r v i ca l s in glfmdulas, cubierta por
e p i t e l i o escamoso nat ivo o maduro.
i%i endocervix, que anatómicamente corresponde a i condug
t o que se encuentra por a r r i ba del o r i S i c i o c e r v i c a l externo
y abajo del interno, se encuentra cubierto de e p i t e l i o c i l i r i - dr ico , q.ue no s610 recubre l a super f i c i e de l conducto sino -
también l a s g l h d u l a s endocervicales, que se encuentran en - e l estroma.
Antes de l a menarquia, l a unión entre e l e p i t e l i o esca-
moso del exocervix y e l e p i t e l i o c i i i n d r i c o del endocervis -
sue le s e r precis?. Sin embargo con e l c recmiento del cue l lo
durante ia menarquia, y en especia l con l a eversidn f i s i o i ó -
g i ca del endocervix durante e l embarazo, e l e p i t e l i o c i l f n d r i - co y l a s gl.&ndulas del endocervix salen hacia e l exocervix - anatómico.
Este e p i t e l i o c i l f n d r l c o que se encuentra ahora en e l - exocervix está expuesto al medio ambiente vaginal. Por in--
f luenc ia de éste , debido probablemnte en -, parte al PH,
e l e p i t e l i o c i l f n d r i c o exocervical es substituido graduaimen - t e por e p i t e l i o escamoso.
-3s -
La zona anatómica del cue l l o en l a que ocurre se drnomina zcr. - na de transformacidn y es ah í donde por primera vez se obser
van l a s anormalidades e p i t e i i a l e s c i i f ndricas, consideradas
precursoras de l carcinoma invasor.
A pesar de l o s años de intenso estudio por muchos inves - t igadores, aún se discute l a forma exacta en que ocurre este
proceso. Hoy en dia, l a t e o r í a más aceptada es e l concepto - de l a metaplasia.
Todavía suc i ta controvers ia p r ec i sa r cu4l es l a cé lu la
exacta que pa r t i c i pa en e l proceso de metaplasia, pero eo--
ppleson y Reid señalan que esta cé lu la c i l f n d r i c a en s í , t a l
vez aunada a l a s cé lu las de l estroma subyacente que son tram - formadas directamente en ” c é lu l as basales neoescamosas“ . Por
debajo de gruposde estas cé lu las se forman una nueva membrara
basal y de esta manera “ e l e p i t e l i o escamoso metap16sicor‘ ha
sust i tuido a l e p i t e l i o c i l f nd r i co . Aún no se sabe qon seguri - dad s i l a s propias cé lu las c i l í n d r i c a s se di ferencian nueva-
mente en cé lu las e p i t e i i a l e s escanosas o s i son sustituidas
por una p rb l i f e r a c i ón ds una cE1ul.a. indiferenciada de l estral - ma endocervical denominada ‘I cé lu las de reserva o aé iu las - subc i l f ndricas” .
El proceso de l a metaplasia es especialmente ac t i vo des
pués de iü eversión del e p i t e l i o c i i f n d r i c o que ocurre durm - t e l a menarquh y e l primer embarazo. Es un proceso f i s i o i ó -
g i co normal cuyo resultado puede ser nuevo e p i t e l i o escamoso
b i en diferenciado, que cubre e l exocervix.
Los fac tores m a l ca ra c t e r i zados denominados en l a “ r e s - puesta del huéspedr1 pueden e v i t a r e l desarrol lo c l í n i c o de -- una neoglasia ce rv i ca l , a pesar de l a combinaci6n de a l t o -- r i esgo que piantean l a s circunstancias.
- 36 . -

r-
L
P
L
L
c
L
Sin embargo esta t e o r í a se :ajusta muy bien a l a s observacio-
nes epidemioiógicas de que e i c o i t o a edad temprana (durante
e i período posmenarquía de metaplasia ac t i va ) y múl t ip les - compañeros sexuales (exposic ión a un agente carcinógeno tram - misib le ) son factore.:. de a l t o r iesgo de cáncer ce rv i ca l .
No obstante, cualquiera que sea l a cé lu la o e l origen, - pruebas f irmes sugieren que l a neoplasia del cue l l o s e o r i g i - na de una cé lu la a is lada más que de d l t i p l e s s i t i o s . Park y
Jones al estudiar mujeres que fueron heteroc igotos para l a .-
forma A y B deshidrogenasa gLucosa-6-fosfat0, encontraron qve
e l t e j i d o canceroso tenfa ~ ~ 3 1 0 forma A o B. Ya que l o s genes
de es ta enzima se encuentran en e l cromosoma-X,el resiultado-
puede expl icarse por e l desar ro l l o de una masa tumoral a par
tir de una c é lu l a simple que fue act ivada por u:ia u o t r a f o r
ma de esta enzima.
- -
h v a s i d n temprana de l estroma
Es d i f i c i l e l diagnóstico delos grados tempranos de in-
vasión de l estroma, ya que posiblemente l a s glándulas sean - sust i tuidas de l todo por brotes de l tumor s i n que haya una -
invasión verdadera. S i is estructura de l a glándula s e con-
serva bien y e s l i s a , no hqy invasión. S i e l contorno es gri - sáaeo y confuso, probablemite l a invasión por parte de l es--
troma. Casi siempre Bas c é lu l as escamosas invasoras parecen
más maduras con citoplasma e o s ino f f i i c o aumentado cuando se
comparan con l a e cé lu las indi ferenciadas de t i po basal de -- carcinoma i n s i tu . Los co r t e s tangenciales, l a invasión de -
l a s glándulas, y una mala preparación de l t e j i d o suelen d i f i - c g i t a r en extremo es te diagnóstico.
L
L
c
-3%-
Carcinoma invasor
i gua l que sucede en caso de que e l carcinoma asiente
en o t r o punto, e l diagnóstico de esta a fecc ión a n i v e l del - cue l l o se basa en dos caracQer fs t icas pr incipales; 1)una ex-
pos ic ión o arquitectEra anormal, 2) anomalías en l a s cé lu las
que l o constituyen.
Eh tanto que en l a supe r f i c i e e p i t e i i a i normal l a s c é i u
l a s e p i t e i i a l e s s e encuentran claramente separadas de l es tro - ma por l a membrana basal, en e l cheer es ta 6l t ima se destru - ye; de aqul que e l e p i t e l i o se introduzca en e l estroma, al ii
pr inc ip i o a manera de pequeños botones, más tarde en forma u
de la rgas colwnnas que crecen profundamente en qquel, seme--
jando l a forma en que l a s ra f c es de un árbol se introducen - en l a t i e r r a . En toda8 l a s fases excepto l a s m's tempranas - puede hacerse un diagnóstico f i m e con un pequeño aumento, fu
puesto que é s t e pone da manif iesto i a desordenada y anormai
invasió i i de l estroma por el. e p i t e l i o . Es ese carácter inva--
sor, junto con l a propagación de l a s ce iu ias a través de l o s
i i n f á t i c o s , e l causante de l a s cualidades t í p i c a s que t rad i3
cionalrnente s e asocian a l a malignidad, a saber:la i n f i l t r a ;
c i ón l o c a l , las metástasis y l a s r e c id i vas después de l a -- ext i rpac ión incompleta.
En tanto que e l e p i t e l i o normal es ta const i tuido por cé - i u i a s di ferenciadas de t i p o a d d t o , l a s de l cáncer muestran
un grado va r i ab l e de inmadurez. Hist916gicamente asto se po-
ne de r e l i e v e por l a b spa r i dad de l tamaño c e lu l a r y de los
núcleos, hipercromatoais, mi tos is normales o patoidgicas y - ca r r i o r r ex i s.
Aunque se han propuedto a través de l o s años var ias c l a - s i f i c a c i óne s d e l carcinoma c e r v i c a i de cé lu las escamosas y -

i
P
L
actualmente is mayoria de l o s anatomopatóiogos dividen e l C-
cinoma epidemoide d e l c u e l l o en t r e s t i p o s r 1) célula gran*
de , quera t in izaüa ; 2) c é l u l a grande, no querat in izada y 3) - c 6 l u l a pequeña. Los cánceres querat in izados e s t á n compuestos
de c é l u l a s grandes con n o t a b l e pleomorfismo, re la t ivamente - pocas m i t o s i s , y fonnación de p e r l a s escamosas. Los tumores
no q u e r a t i n i z a n t e s de c6lul .as grandes se c a r a c t e r i z a n por c-
i u i a s con pleomorfismo moderado y m i t o s i s f r e c u e n t e s , y gran - des núc leos que suelen contener macronuciéoios. La variedad - d e l carcinoma c e r v i c a l de c é l u l a s pequeñas e s t 4 compuesto de
una lámina monótona de c é l u l a s pequeñas i n d i f e r e n c i a d a s s i n
p e r l a s de querat in ina . Las m i t o s i s son f recuentes .
En un es tudio l a s enfermas con tumores no querat inizadw
de c é l u l a s grandes evolucionaron mejor que los tumores que-
t i n i z a n t e s y e l peor í n d i c e de supervivencia s e obervd en mu - j e r e s de c h c e r de c é l u l a s pequeñas.Swan y Roddick pudieron
conf irmar e s t o s ha l lazgos en p a c i e n t e s tratadas con radiac ión
pero no en ias que s e hizo cirugía en i a s que no Encontraron d i f e r e n c i a en l a supervivencia e n t r e los t r e s t i p o s histoló-
g i c o s . Gunderson y colaboradores no encontraron d i f e r e n c i a s
de supervivencia en 175 p a c i e n t e s tratadas por r a d i a c i ó n y
o t r o s han señalado ambos t i p o s de resul tados . En consecuen--
c ia , cabe c o n c l u i r que atin e s i n c i e r t a l a importancia pronós - tics de e s t a c las i f icac ibn.
L a c l a s i f i c a c i ó n de Broders , que c o n s i s t e en designar - d i v e r s o s grados numérbcos según l a d i f e r e n c i a c i ó n c e l u l a r , .-
también s e u s a con f recuenc ia . Los tumores de p a d o I son - l o s me jor d i f e r e n c i a d o s y los del grado IV los más i n d i f e r e n - ciadoa. Nuevamente, l a im&lortancia p r o n ó s t i c a de esta clasi-
f icación e s motivo de controvers ia . Desde e s t e punto de v is -
t a pronóst i co e s mucho más importante l a etapa de de l a en-
fermedad que d e l t i p o c e l u l a r o l a d i f e r e n c i a c i b n .
-39-

ADENOCARCD.TOMA Y CARCINOMA ADENOESCAMOSO D'EL CUELLO
EI adenocarcinoma c e r v i c a l es menos comh que l a varie-
dad de cé lu las escamosas. Segihestudios rec ientes, correspon - de aproximadamente ai io$ de l t o t a l de l o s cánceres cervica-
l e s . Aunque por l o general s e i n i c i a dentro del conducto c e r - v i c a i , l a l e s i ó n primaria puede asentar en e l o r i f i c i o ex te r - no o próxima a éi, formando en etapas avanzadas W a ve,Teta--
c i ón de gran tamaño a n i v e l de l a supe r f i c i e vaginal de l cue - 110. A pesar de l o bcho , es más t í p i c o que e l proceso afec-
t e en proporción c rec i ente e l cue l l o y los t e j i d o s vecinos - s i n producir l e s i ones ex temas en l a supe r f i c i e vaginal.
~ icroscdpicamente se c'a acI;eriza por l a disposic ión @an - dular abfpica tan d i s t i n t i v a de l adenocarcinoma, en notable - contraste con e l aspecto y d is t r ibuc ión ordenada de l a s g l h - duias c e r v i ca l e s nowaies. En algunos casos e l ppartaniento
de l o normal es mod rado; e.n o t ros l a disposic ión @andular
anoi-mai es intr incada y a t f p i c a en extremo. Los mismos pa--
dos de var iacidn se apl ican a:.,las cé lulas. En algunos adeno-
carcinomas, e l e p i t e l i o glandular puede es tar formado en su
mayor parte por una so l a capa celular , y conservar dichos -- elementos l a forina c i l í n d r i c a adulta de l e p i t e l i o c e r v i ca l -
normal. En o t ros puede ha l l a r se formado por múlt ip les capas,
y es pos ib l e que l l eguen a invad i r tan amplianiente e l conduc - t o que en zonas ais ladas parezca que e l carcinoma pertenece
a l a variedad epidermoide sól ida.
Tomando como base estas var iaciones en laL- mismal famila de tumores, se han popularizado d i s t in tos sistemas de grada-
c ión h is to ibg i ca , siendo e l más myileado e l de Broders. La - variedad menos indi ferenc iada constituye e l grado I; aquella
en que el proceso e s .n4xima, e l grado I V , d e s i w n d o los gra dos I1 y I11 l a s variedades intermedias.
-40-

Quizilbash y F r i ede l l y McKay han descr i to l a s altera-
c iones neopiásicas i n i c i a l e s dentro de l a s glándulas del en-
docervix, y se r e f ' i r i e r o n a e l l a s como adenocarcinoma i n sL tu en e l cuel lo . Suelen ser' cambios foca les ,y a d i f e renc ia - de sus contral tartes de cé lu las escamosas, aún no se estudia
b i en su h i s t o r i a natural.
dn ocasiones, l o s tumores que surgen del cue l l o conten-
drán elementos mali6gos del, e p i t e l i o tanto escamoso como g l ~
duiar. Cuando se i d e n t i f i c a n claramente l o s elementos escamo
sos pueden denominarse carcinomas adenoescamosos. S in embar-
go en muchos casos, e l componente epidermoide esta mal di fe-
renciado s in formación de j ier las de queratinina, y Juiian y
colaboradores han recomendado que estso tumor,es se c l a s i f i 3 q
quen separadamente como carcinoma adenoepidermoide. Las p a t
c i en t e s con estos tunores combinados t ienen al parecer peor
pronóstico que l a s enfermas con adenocarcinomas o con cáncer
de cé lu las escamosas únicamente. Cuando se observa es te pa-
tr6n h ia to lóg i co , es importante tener t e j i d o endometrial por
d i l a tac i ón y raspado o biopsia, para comprobac s i hay invaei
s ión de l cuerpo uterino. S i es ta afectando, debe eonsiderar-
se e l tratamiento comb.inado que incluye radiacibn además de
h i s t erectomfa.:.
.,
En ocasiones, se observan otros t i pos h i s t o i óg i cos de - cáncer del cue l lo . El. sarcoma, e l adenoide de cé lu las bas&-
l e s , y e l melanoma pueden surg i r en forma primaria en e l cue
110, y s610 en raras ocasiones se observa cáncer metast&tico
de o t r o s s i t i o s o linfomas.
CARACl'ERISTlCAS GLINICAS DTL CARCINOMA CERVICAL
La edad media de l a s pacientes con carcinoma sintomátia
co de l cuelLo es de aproximadaraente 45 años. En contraste, -

l a s enfermas con carcinoma Ln t r a ep i t e l i a l t ienen en promedio
32 años y no es raro e s t e diagnóstico en adolescentee o j ó v ~ nes en l o s primeros &os de l a segunda decada de vida. EL - carcinoma i n t r a e p i t e l i a i es cas i sie,npre asintomático, y e l
diagnbstico se establece a l inoaento de un f r o t i s c e r v i c a l - rea i i zado como estudio sisterntico .
El. dolor no constituye un sintoma de l carcinoma c e r v i c a
hasta l a s a t i m a s Pases de l a enfreiaedad. % descoiioriiniento
de e s t e hecho cap i t a l es uno de l o s obst&culos m&s graves - que se encuentran en l a campaña tendiente de l reconocimiento
prematuro de l cáncer. En l a mayorfa de los casos, e l primer
síntoma es l a hemorragia, l i g e r a por l o general. S i por su - edad l a paciente s e encuentra aim en período reproductor, e s t e sangrado adopta tfpicamente la variedad intermenstrual.
Pueden producirse después de l co i t o , esfuerzos v i o l en tos o * de una defecation d i f í c i l . Es ca rac t e r f s t i ca sobre todo l a - hemorragia "por contacto", que sigue a l c o i t o o a un simple
examen pé lv ico . Por desgracia, en muchos casos de hemorragia
no se produce hasta que l a enfermedad está arraigada y se ha
extendido a l o s l i n f á t i c o s ; de aquf que hasta una paciente - intrr l igente y a l e r t a puede e s ta r condcnada a muerte antes c p
se presenten l o s síntomas. Más a h s i e l tumor está l o c a l i z a - do en e l endocervix, hay propensi6n a que l a hemorragia spa%
rezca más tardiamente porque l a l e s i ón está en un s i t i o más
pro t e gi do.
A veces.puecle notarse un f l u j o anormal, por l o general
acuoso, aún antes de que aparezca l a hemorragia especialmen-
t e en caso de adenocarcinoma. Sin embargo, tarde o temprano
e l f l u j o aparece teñido de sangre. A medida que progresa l a
enfermedad, tanto l a hemorragia como e l f l u j o áe hacen más - pers is tentes y profusos, ali propio tiempo de l a ulceracibn,
cada vez mayor, y l a in fecc ión secuhdaria van conf ir iendo a
- 4 2 -

u---.----
L.
r .
I..
C"
I
il ,,;.
producto de secresidn un o l o r cada vez más desagradable. ñLg d::n presentarse o t r os sfntomas como i r r i t a b i l i d a d ves ica l , - d bido a que e l proceso va tomando e l tabique vesicovaginai,
con l a correspondiente sensación de molest ia r e c t a l , que se
ext iende hac ia l a parte poster ior . El do lo r gravat ivo, peno-
so constituye por i o general un síntoma destacado, que puede
hacerse severo a medida que avanza l a afeccibn. a do lor per - s i s t en t e en l a reg ión lumbcsacra en espec ia l cuando se acom-
paiiade i infedema de i a pierna, es un s igno de muy mal pronbg
t i c o . La " t r i ada t e r r i b l e " , do lor sacro, l infedema un i l a t e ra l
y obstrucci6n '..citzrsteral un i la te ra l , i nd i ca una enfermedad - m u y avanzada, po r l o general incurable. Es pos ib l e que se - produzcan f i s t u l a s en v e j i g a o recto , haciendo más t e r r i b l e
e l padecimiento. La m f i i t r a c i 6 n l a t e r a l crec iente obstruye
l o s uréteres, siendo i a uremia i a causa ihbtima de muerte - quizá en el gru;io mayor de casos. M A R C O I N G E N I E R I L
DIAGNOSTICO DEL CANCEñ CERVICAL
En &os rec i entes se :han revisado completanente nuestra
métodos de va lorac ión de consul to f lo en i o que se r e f i e r e . BL
diagn6stico de c4ncer uter ino, especialmente cazv ica l . De he
cho se i n s i s t e en l a importancia de preguntar cuidadosamente
s i había hemorragias de contacto, considerar e l aspecto ma-- - croscópico de l cue l lo , e l v a l o r de l a palpación y o t r os méto - dos que aiiora hemos de considerar simplemente secundarios.
F r o t i s de Papanicolaou
El desa i r o l l o de un método c i t o i ó g i c o prec iso para es%
d i a r mujeres asintomáticas con cue i i o de aspecto cornpietamel'
t e normal nos ha permltido en muchos casos e l diagnóstico de
P
-43 -
c h c e r temprano l a r g o tiempo antes que hubiera síntomas o -
anomaifas patoh5gicas manifiestas. poda mujer sexualmente a c
t i v a debe prac t i carse un f r o t i s para cáncer, que no es c a r o ,
y que como aclaramos sinceramente a nuestras enfermas, es lw. mejor invers ión que pueden kacer. No obstante hay que tomar
una h i s t o r i a completa sobre hemorragia intermentrual o por - contacto, palpar cuidadosamente e l cue l l o y exp lorar lo con - e l esrPjo. "onde hay una i e e i bn v i s i b l e en e l cue l l o , se debe
obtener una b i ops i a además de un f r o t i s , tenga o no l a l e s i ó n
aspecto de c h c e r . De hecho, l a s c é lu l as necrót icas e i n f l a k
matorias de un cáncer invasor ulceroso pueden d i f i c u l t a r o
impos i b i l i t a r e l diagnóstico c i t o l ó g i c o de una l e s i ó n muy -- evidente. Papanicolaou y Tsaut introdujeron inicialmente l a
t é cn i ca de l a c i t o l o g f a en l a aed ic ina c l ín i ca . Las muestras
de c é lu l as ex f :> l iadas o raspadas de l a supe r f i c i e de l cue l lo
y de l a vtiggina s i r v en como microbiopsias, en l a s que e l c i t o - patóiogo estudia los múlti.pies procesos de l a salud y l a en-
fermedad. Aunque suelen provenir de l a supe r f i c i e de órganos
como e l cue l l o , estas muestras r e l l e j a n con prec i s ión proce-
sos más profundos. Abarcan una Brea para e x h e n más amplia F
de l o que suelen pennii&vlo l a s biopsias, no extirpan t e j i d o
v i a b l e y no producen procesos in f iamator ios o de reparación
o e s muy pequerio.S& han descr i to muchas tecnicas para obtena
muestras c i t o i ó g i c a s , e l denominado f r o t i s Papanicolaou. s in importar e l procedimiento u t i l i z ado , es necesario recordar
va r i o s pr inc ip ios ; 1) l a técnica para obtener muestras debe
s e r óptima a f i n de l o g r a r l a s c e l d a s que proporcionan l a - información an&s prec i sa d e l transtorno en invest igac ión; 2)
l a muestra debe f i j a r s e inmediata y adec admente para perm&
tir l a mejor interpretacrbn, y 3 ) es necesario informar a i -
-,
-44 -

c i topató iogo de cualquier hal lazgo o h i s t o r i a c l í n i c a poco - comfmes, asf como senalar le c u d q u i e r pregunta o preocupaciái
espec í f i ca , % consecuencia, s i e l ob j e t o es hacer un estudiD
para d iagnost icar cheer ce rv i ca l , hay que obtener una bue-
na muestra de l área de l a unión escamocilíndrica de l cue l lo ,
pero s i s e desea va lorar e l estado hormonal de una paciente,
es p r e f e r i b l e hacer un raspado de l a pared l a t e r a l de l a va-
gina. Para proporcionar la, in te rpre tac ión m's prec i sa y ú t i l
de l a muestra, es importan.te enumerar algunos datos de l a pet. - c i en t e como laedad, ú l t ima. meiiei6,ruación, t i p o de anticoncep4
t i v o ( s i emplea alguno) y diagnóst.!.cos y tratamientos p r e v i a
por ejemplo b iops ia o radioterapia.
La técnica que hemos u t i l i z ado para l a detección de l .:-
cáncer c e r v i c a l incluye l a . de obtener muestras de l fon.do co-
mún vaginal, e l exocerv ix y e l conducto endocervical. hk cue - iio se expone y se elimina. suavemente e l exceso de secresióri
Se u t i l i z a e l extremo redondeado de una espátula de p l ás t i co
o de madera para obtener un poco de mater ia l
g m a l poster ior . Después s e usa e l o t r o extremo para raspar
e l cue l l o en 360 . Por úIt;imo, un ap l icador cubierto con al-
godón humedecido en solución sa l ina s e introduce en e l con-
ducto endocervical y se hace g i r a r para obtener una muestra
de l endocervix. Cuando s e han tomado l a s muestras, s e disemi
nan l o más rápidamente poe:ible en un portaobjetos y se fijan
de insiediato en alcohol e t S l i c o a l 95 $. Algunos autores re-
comienda una p ipe ta pequeria prov i s ta de un bulbo de caucho
para obtener una muestra endocervical, pero Shingleton y co-
laboradores encuentran que son igualmente e f i caces e l ap l i ca
dor cubierto en un extremo con algodón y l a aspiracidn endo-
de l f 6 rn i x va -
-
-
-45-

c
ce rv i ca l . Cuando se sabe que hay d i sp las i a c e r v i c a l u o t r a - anormalidad, puede ser út i l . usar dos o t r e s portaobjetos y - para i a in te rpre tac ión diagnostica r em i t i r separadamente cadi
muestra en un portaobjeto, a f i n de proporcionar una disemi*
nación c e lu l a r más amplia. Los f i j ado r e s comerciales en ae-
r eoso l o e t a s son bastantes sa t i s f ac to r i o s , s i e l f r o t i s no
s e de ja secar a i a i r e hasta después de l a f i j a c i ón . Una vez
que se f i j a , puede secarse e l portaobjetos para env iar lo a i
l abo ra to r i o de c i to log fa .
Originaimerite se propuso un sistema de gradación para - i nd i c a r e l diagnós .ico de i .a c i t o : o g í a c e r v i c a l de l a c lase
I a l a V, se& l a gravedad de l a anomalfa. S i no se observg
ban cé lu las anormales, e l CLiagnnSstico correspondfa a l a c ia=
I, y s i habfa c é lu l as que smgerfan cheer invasor franco, se
indicaba una l e c tu ra c l ase V. Muchos c i topató iogos informan
actualmente un diagnóstico en términos h i s t o l6g i cos como "be - ni;;no", " d i sp i as i a moderada", o "carcinoma de c é lu l a s esta.-
masas", e indiaan su inh$ryiretación de l o que hubiera mostra. - do una b iops ia con base an l a muestra c i t o lbg i ra .
La técnica de l f r o t i s de Papanicolaou es relativamente
barata, indolora, y prec i sa para e l diagnóstico de d i s p l a s i a
c e r v i c a l y cáncer. como t a l , e s i d e a l en e l diagnóstico de - grandes grupos para descubrir una neoplas ia c e r v i c a l asinto-
mática temprana. La in f luenc ia de l o s grogramas de se lecc ión
en i a frecuencia de l cáncer c e r v i c a l y l a d i sp ias ia ha s ido -
estudiada. en muchos s i t i o s de l mundo.
Muy pocos laboratorios; de c i t opa to l og f a están conscien-
t e s de estas negativas faisias, por l a simple razón de que - l a s pacien.tes con f r o t i s negativos normalmente no s e contro-
l a n después, de ninguna. maner;.. Sia embargp, es pos ib l e ca l -
-

cu lar e l promedio de ne::a.tivas f a l s a s de l o s dcztos obtenidos
en estudios repet idos , y al@mos de ellos poe ejemplo e l de
S i l b a r y Woodruff han desarrollado c i f r a s de negativas fal--
sas de o t r a forma. De éstos y o t ros estudios s e ha obtenido
una c i f r a aproximadamente 204a de neAativas f a i s a s para l a c i ._
t o l o g f a e x f o l i a t i v a .
Esto no s i g n i f i c a que l a c i t o l o g f a e x f o l i a t i v a no sea - procedimiento d e va lor , pero quiere d e c i r que l o s g i n e c o i b p
deber& tomar en cuenta. e s ta pos ib i l i dad en e l empleo de l mé , .-
todo c i t o ibg i co . a problema de l a s negativas f a l s a s es une.
de l a s p r inc ipa l e s razones para r e a l i z a r un estudio anual,
pero s i l a paciente t i ene dos o a& mejor t r e s pruebas ne,F-
t i v a s Fn u11 período de t r e s años, l a evoiucidn l e n t a del cán - ter de l cue l l o uter ino indican que no es necesario un f r o t i r
subsecuente anual. sino que puede r e a l i z a r s e cada t res , cuats,
arios.
Sin embargo, l a s ¿pacientes de " a l t o riesgo" por tener
una o más ca rac t e r l s t i cas ep idemio lbg~cas mencionadas o que-
han tenido f r o t i s anormales en años anter iores , dehen some-
t e r s e a exhenes cuando menos una vez a l allo. También hay - que recordar que un f r o t i s <cerv ica l de Papanicolaou no es e l
único be:ieficio médico de una v i s i t a anual c t l ginecoiógo.
Desde un punto de v is ta tebr ico , e l empleo frecuente de
un e x h e n c i t o i d g i c o con in t e r vá i os adecua.dos pudiera dismi-
nu i r l a muerte por esta enfermedad, descubriéndola. más tern--
prano y en etapa curable. La pos ib i l i dad de cont ro la r e l CELL - ter de cue l l o uterino por ce iecc ibn c i to i6g i ca . ahora es de - plena catualidad. HL&O un tiempo, cuando aparecí6 e l método
c i t o i 6@co , en oue parecfa como s i e l problema de l cáncer -
c e r v i c a l se pudiera resolver proporciomdo estudios c i told*.
g icos anunciando su disponibi l idad, y pensándose y esperarido
que todas l a s mujeres h ic i e ran l o necesario para s e r examina - das q a c i a s a l o s medios que normalmente ut i l i zaban como ser - v i c i o médico regular. Parece comprobado que e ra ingenuo espe - r a r un contro l amplio y e f h a z de l cáncer de l cue l l o en esta
forma.
Esto no s i g n i f i c a que una población l imi tada de mujeres
no pueda l o g r a r protecci6n con este método, y hay muchos in-
fames publicsdos de grugot3 de pacientes p w t i c u i a r e s que lo
confirmati. Con e l paso de l tiempf.> y e l aunento de l número de
f r o t i s repet idas, ha disminuido netariente l a proporci6n de - descubrimientos a .iiediaa que los carcinomas en l a poblucidn
s e han ido extirpando. Aunque es te enfoque procede, cabe se-
5alar. que, en téminos de (control d'-e una comunidad y de l t o
t a l de energfa gastada en proporcidn de l o s cánceres descu-
b i e r tos , se t r a t a de una t 'écnica poco e f i caz . Irn estudio de
Kashgarian y colaboradores acerca de l a d isponib i l idad públ - i ca de l a c i t o l o g f a uter ina en e l condado Shelby de Memphis,
Tennessee, en un proyama adecuado, demostró que, ihcluso en - t r e aquel las mujeres que s'e sienten impulsadas por l a propa-
ganda a buscar un f r o t i s o r i g ina l , después de un periodo de
cinco arios dki esfuerzo de .propaganda muy considerable y pro-
longado so lo dejd l a quintis. parte de l a pi;blacibn dcsezndo - e f e c Luar ex&menes anuales repetidos, incluso cuando t a l e s - examenes eran to talnente gratuitos.
f o r l o tanto e l problema primario en e l contro l publico
de l cancer c e r v i c a l no es de tecnica n i d isponibi l idad de mv - dios, sino mas b ien de organizaci.6n y motivaci6n de dicha co -- munidad.
- 4 8 -

Prueba de S c h i l l e r
Se basa en que e l ep i t , e l i o canceroso no contiene glucó-
geno y, por tanto no capta. e l yodo como e l e p i t e l i o normal - de l cue l lo , o de l a vagina, que son r i c o s en giucógeno. As1
l a ap l i cac ign de una solución de yodo (de S c h i l l e r a l 0.3% -
de Lug01 a l 56) 2uede mostrar e p i t e l i o normal de c o l o r caobm
mientras l a s zonas de displ.:isict y cancer quedan s i n t e f i i r ;y
ne tamerite l i m i ta.das.
por desm:racia, e l e p i t e l i o c i l l n d r i c o >- diversos cuadrm
in f lamator ios benignos quiza tampoco se tinan,Jo que conduce
una "prueba p o s i t i v a de S c h i l l e F , y e l empleo más l i b e r a l n
de f r o t i s y b iops ias ha l imi tado hasta c i e r t o punto l a u t i l i - zación de es te método. > in embar@, t i e n e Zran va lor espec ia - mente cuando LOS f r o t i s son pos i t i v os y l a s b iops ias son dudo - sas; s i el. f r o t i s se vulve pos i t i v o d.espues de h i s t e r ec tomh
por un cáncer i n s i tu , sefiala l a necesiadd l ó g i c a de una b i o c
s ia .
-. - . _-__ - - - - "1 .Hallazgos colposcópicos normal es.
A. E p i t e l i o esc&mosos o r i g ina l . Se obserara en cue l l o y va
S n a un e p i t e l i o o r i ¿ - i n a l l i s o , rosado y s i n rasgos pro - pios. No ex is ten v e s t i g i o s de e p i t e l i o c i l l n d r i c o que-
pueden i d en t i f i c a r s e , a s i como e p i t e l i o que secreta mo-
co, hendiduras abier.tas o auis tes de Naboth
B. Ep i t e l i o c i l i nd r i c o . Es una capa de e p i t e l i o simplela&
ta l que produce moco, que se extiei4fle entre e l endome4
t r i o por a r r iba y e l e p i t e l i o escamoso oric&nal o e l - e p i t e l i o metaplásico por abajo. Lz super f i c i e cubierxa
con e p i t e l i o c i l i n d r i c o es i r r e g u l a r con pápi las gran-
der; de estroma y hentiiduras profundas. l a colposco-
p i a despues de l a prueba de ácido acé t i co t i ene estruc - tura t l p i c a semejante a uvas.
-43-

L
c
c
L.
r.
c
L
c.
L..
.._
... ..
E l e p i t e l i o c i l f n d r i c o puede e s ta r presente en e l endo-
c e r v i x sobre una porción o toda l a vagina.
C. Zona de transfonnaci6ri. Es l a supe r f i c i e entre e l ep i t e - l i o plano o r i g i na l y el e p i t e l i o c i l l n d r i c o con d i f e ren - t e s graüos de madurez que pueden iden t i f i ca r se . Los com -
ponentes una zona normal de transformación puede es tar
a is lados de l e p i t e l i o c i l i n d r i c o que l e rodea por ep i t e - lie plano metaplástico, "aberturas giandulares" y quis-
t e s de Naboth. En l a s zonas de transformacidn normales
no s e enc entran a l a colposcopia estructuras que hagan
pensar en neoplasia c e r v i ca l .
11. Hallazgos colposcópicos anormales.
A. Zona A t i p i c a de transfomaci6n.Una zona dP transforma - c ión en l a cual ex i s ten ha l lazgos colposcópicos que - hacen pensar en neoplas ia c e r v i ca l .
1. E p i t e l i o blanco- despues de l a prueba con ácido a6
c é t i c o se observa con e l colposcopio una zona anor
mal foca l . E l ep:ttelio blanco es un f enheno trail-
s i t o r i o que se observa en l a supe r f i c i e de mayor - d+nsi dad nuclear.
-
2. Pun t i l l e o - anormalidad coiposcópica f o c a l en l a - que s e observan cap i la res de manera punteada.
3. Blosaico - anormal-idad colposc6pica f o ca l en l a que
e l t e j i d o semeja un inosoico. Los campos del mosai-
co están separados s o r bordes enrojecidos.
4. Leucoplaquia - anormalidad colposcdpica f o ca l en - La que hiperqueratos IS y paraqueratosis parecen u-
na p laca blanquecina elevada. Esta p laca blanqueci
na se i d e n t i f i c a antes de l a ap l icac ión dr. acid0 - ace t i c 0 .

. - _I--
5. Vasos Sanpineos anormales - anormalidad colpos-
cópica f o ca l , en l a que los vasos sangulneos no
son puntileados, como mosaicos o con pequenisi--
mas ramificaciones, sino que son vasos i r r egu ia - r e s con cursos sinuosos que parecen comas, tira-
buzones o espagueti.
B. Sospecha de cáncer invasor. Es e l cáncer que en l a
exploraci6n c l l n i c a no puede observarse.
111. Hallazgos colpóscópicos insa t i s f ac to r i o s .
Casos donde l a unión p lanoc i l indr i ca no puede observar - se.
TV. Otros Hallazgos colposc6picos
A. Vag inocerv ic i t i s . Es un molde colposcópico di fuso de
hiperemia en l a oue l o s vasos sanguineos parecen - arreglados en forma. di fusa semejante a l pu i i t i l l eo - vascular.
B. Erosión Verdadera. Es una supe:.f icie s i n e p i t e l i o p r 2
vo c ada generalmente por traumat i smo . 6. E p i t e l i o a t r6 f i co . Es un e p i t e l i o plano con carencia
de estr6gerios en que e l molde vascular se i d e n t i f i c a
pronto por e l adelgazamento r e l a t i v o de l e p i t e l i o - plano suprayacente.
D. Condiloma, papiloma. Son l e s i ones e x ó f i t i c a s que pue - den es ta r dentro o fuera de l a zona de transformación
- 5 1 -

I .
P-
-.. c
c_
r-
C..
r-
L.
_I - P
L
r
L
c
L.
r -
- 5 2 -

Colposcopia
El colposcopio es un instrumento grac ias a l cual puede
observarse e l cuellm en plena l u z con aumento de 10 a 40.
La técnica de exámen es rápida; requiere practicarnente e l - mismo tiempo que l a inspección de l cue l l o a simple v is ta .
Después de obtener muestras para cittblosfa, puede l impiarse
e l cue l l o con un hisapo d? algodón, enfocarse e l eolposcopio
y estudiar cuidadosamente todo e l cue l l o , primero con iluwi-
nación normal, luego con f i l t r o verde para mejolrr l a visibi-
l i d a d de l a s imágenes vasculares. &l cue l l o s e asea adicio--
nalrnente con una solución de acido acé t i co a l 3% que proporo
ciona una .nejor d i f e renc iac ión de l e p i t e l i o c i i l n d r i c o de l a
zona de transformaci6n. P o r último pueae t eñ i r s e con solución
de Lug01 para delinear. &rea,s negativas a l giucógeno.
Los ha1 ~ a z g o s colposcó,icos pueden d i v i d i r s e en var ias
ca tegor las u t i l i z ando l a
dad Estadounidonse para Colposcopia y Pa to l og l a Cerv ica l .
erminoiogia adoptada por l a so c i eh
Hay va r i o s estudios que comparan l a prec is idn diagnósti - ca de l a colposcopia con l a de l a c i t o l o g í a . Los resultados
presentan que dependen principalmeate de l a experiencia de - l o s autores con cada una de l a s tecnicas. Ut i l i zando ambas -
mejora l a ,precisión diagnóstica, porque l a s ventajas d~ ambcs
metodos se complementan.
E l p r inc ipa l inconveniente de l a coiposcopia es que só-
l o permite examinar l a par te v i s i b l e de l cuel lo. Por l o tanb
s i no puede v i sua l i za r se l a unión p lanoc i l lndr i ca , e l exilmen
colpocópico es poco s a t i s f a c t o r i o y hay que con f i a r solo en
l a c i t o l og i a . Esta s i tuac ión ex i s t e en e l 1 5 6, aproximada-
mente, de l a s mujeres premenopausicas.
Po r o t r a parte, l a c i t o l o g l a t i ene e l inconveniente de que -
-53-

L..
c
c _
r-
L
c
L
c
c
LI
c
no ind i ca precisamente donde nacen l a s c e lu l as svspechosae - d e l cue l lo . Po r colposcopia suele poderse l o c a l i z a r l a zona
sospechosa, va l o ra r sus dimensiones y su gravedad,y tomar - b iops ia d i r e c ta para es tab lecer e l di;.gnóstico h is to lbg ico .
La corre lac i6n entre los datos c i t o l ó g i c o s , colposc6picos e
h i s t o l óg i cos permite un tratamiento más racional de l a enfer - ma que fiando solamente a l método.
Aunque l a colposcopia ya fue creada por Hinse1.mm en
1 9 2 5 , y ha s ido ampliaqente! u t i l i z a d a en Europa y en América
del Sur para diagn6stico de l e s i ones cerv i ca l es , ha tardado
en l o g r a r popularidad en Estados Unidos, probablemente por
e l desarro l lo más temprano de medios diagnósticos para c i tp-
l o g i a .
En los Li t imos años las tecnieas c i to16g icas se han ido
perfeccionando tanto que 82) presentan cada vez mas problemas
a l descubr i r i , pequeiias zonas sospechosas en e l cue l l o por i n - ves t i gac ión c l in i ca . Las b iops ias a c i e gas en casos de s i to-
l o g l a sospechosas o pos i t i va , en l a s cuales no s e descubre - una l es ibn , puede tener por consecuencia un diagnlbstico hist-
t o l ó s c o negat ivo fa lso . Po r o t r a parte, procedeer directa--
mente a l a conización basándose en una so l a muestra c i to16g i
ca sospechosa originaráun nfunero muy elevado de conizaciones
innecesarias, que no dejan de tener morbilidad. Es pre fer ia-
b l e u t i l i z a r e l colposcopio para buscar l a zona de biopsia.
-
Con e l descubrimiento de l es iones cada vez in&s semprh=!
nas durante l a se lecc ión sistemática y e l estudio de l a s po-
blaciones, e l colposcopio est$. adquiriendo un lugar cada vez
más importante en e l tratamiento x's moderno de pacientes con
c .i t 010 ?:la ano m a l .
-54-

-- 65-
Estas son a l v a s de las caracteristicas del Cblposccpio cuando onpaado Ccn otros en el nercado:
- optica supeiior que p x m e claridad. hasta e l borde misrm de1 r x m p visual.
- Tiene un sistem Tri-Optiw, el cual elimina l a necesidad de dividir el p d s de ha- en- e l exanrinadDr y e l visor para fotografía.
- ndemas del anpiio canp visuai, ia profiindidad del misrrr, es excelente. ü s t d no enantrará esto aun si io omrpara mn cualquier otro aziposccpio VendIda a myor predo. prácticas ya qm es muy dificil expresarla w n nomiros.
üsteü se dara cuenta de su superioridad hadendo exdnaciionos
- Nueva distancia focal de 2 8 h
- IiimrinacFbn superior del capo visual (3011 una luz de intensidad ajustable la cual provee el 25 por ciento mas de luz que e l rrejor CblpscopiO decpies del nuestm
- Nueva canara Polaroid Sanar SLR om aditamento para acercar la ha-.
- Capacidad para fotografía an canaras Polaroid y Oe 35m. Canbiar de un slstem a l otro imm3 menoc de M IIdnUto.
- La camara foingrafica se p& dejar posidonada en e l B l p s a p i o sin que esto interfiera am e l operador o mientras se tcrrian nuestras.
- El ajuste horizmtal es 2 pulgadas mas grande quo en cualquier otro b l p o s ~ u l o cual permite hacer e l enfoque mas f a d m t e .
- E l tubo de enseibnza es disponible am la mism seleccih de 04-s de ltmk- que e l observador y e l examinador puedan ver exactammte la ndsnia imp.
- E l film esta amvenienerrente integra& a l Cblposapio.
- E l mta je se ofrece en cuatro m r a s diferentes: para nesa wn bram de pimte; mntura para pared an brazo de pi- o base mdante para uso pesado wn brazo de piwte.
- pdemac de estas hay muchas otras caracteristicas ~IE hacen gue nuestro BJposcq>io sea superior y mudio mas practim a otros en su clase.
- Gran e d a - Si usted aprpara cualquier otro Cblposwpio an la mima capacidad, usted enwntrara una gran e w n d a a l omprar e l nuestro. opinion, m o debe verlo y -10 wn otros m3oelos.
base &te ligera; &ut7
En nuestra
-rge Garamy vice PXeSident international Madceting

LAPAROSCWIA
LO laparoscopia es una tecnica utilizada por varias especiaA
idades médicas cp » : ginecolegfa, cirugia y gastrrnterología.
Desde su intreduccibn clínica en los inicies de este siglo
l a laparescopia ha llegado a jugar un papel impmtante, Ha si-
do utilizada en gastranterología para evaluar enfermedades de
hfgade, permitiendo l a visuaiizaci6n directa del hfgade y l a
biopsia directa de defectos focales.; desde e l advenimiente de
l a tomograffa cemputarizada (CT) su papel ha disminuido . Los
cirujanes se hen advecado en l a laparascapia en lugar de l a
laparetaniia en pacientes selectes , cmo en e l caso de evalum
ción de dafio metastatid
de hfgade. Puede ayudar a evitar l a laparetomia innecesaria o
puede ayudar a determinar kt neaissidad de operacib. En l a g i - necmlogía es su area da mayiyor aplicación. Es ú t i l para e1 diag
ndstico da infertilidr¿, amunalfas cong&nitas, endemetriesis y
más recientemente , para recuperar hu vo para fertiiizaci6n
i i i ( 8 .
(hepático) y evaluación de abseses 1
E l equipo es variable dependiendo de l a especialidad en l a
que se va a utilizar. Come en otras areas,' l a introduccih de
fuentes luainasas de fibra-6ptica ha rnejuade l a iiumunaci6n
y eliminade e1 riesgo de quemaduras debido a una fuente de luz
-51-

caliente. Existen una gran variedad de modelos de laparescopies
, con alguna variacien en e:L angula de visi6n. También se re*&< - ere una fuente de gas para insuflacidn de l a fiao&dad abdominal
y un menitor para estimar presibn entre e l abdomen y l a canti-
dad de gas infiltrado. Los acceshrios varian cen las indicacion
es; pruebas, forceps para bibpsias, equipo para cauterie, ins-
trumentos ligantes para amarre de tubes * instrumentos monitcrri
sadores de presibn para medicibn de presiencs intravasculares,
sen algunes ejemplos de accesorios para laparascopia.
-
-
Elpracedimiente puede ser realizado bajo anestesia lecal cr ge - neral: los examenes sencillos de diagnbstico sen frecuentemente
hechos bajo anestesia lwal en e l sits de insercibn y sedacih
intravenesa suplemental; los prwedimientos mas largos y l a may
@ria de de los precedimientes terapeutkes sen hechas baBe mes
tesia general. E l s i t io de insercibn es usualmente apenas aril,
ba deabajo del ombligo y requiere sela una muy pequefia incisión
tlcm). La cavidad abdeminal es distendida cen 2-4 L de gas para
prevenir daño a las viceras cuando e l instrumento es insertade
y para prevenir una completa visualizacibn del contenido abdemi - nal.(El gas mas frecuentemente usado es Ce2 y en mener frecuem
cia e l Ne2&% se utilizara aire, so la una pqqueña cantidad (ie
201111) intravascular bastaria para causar una embelea fatal ; el
- S8-

(b2 ne se utiliza perque evitaría e l us, de cauterio. Ne2 es u t i - lizade mas frecuentemente cen anestesia local pwque es nenes &
rritante para e l peritonean 1. Despi&s de l a induccibn de pnaurn - aperitonrum, e l instrumento es insertado, y se l l w a a cabs una
inspeccibn. Se puede inspecc:ionar y probar, con biopsias tema-
das si se requiere; e l periteneum, l a superficie serosal del
intestine, les organos pelvicos, e l hígado, l a vesícula b i l iar
y frecuentemente e l apéndice, También se pueden llevar a cabo
maniabras terapdticas. Despu6s de del procedimiento, alge del
aj86 infiltrado se escapa per e l area; 1. que queda es sistemáti
camente abs8rbj.de y excretado en las horas siguientes a e l pro-
cese.
-
Les resultados del precedimiento sen exelentes. Es d í f i c i l de - terminar de manera exacta BU razbn de exactitud en e l us@ diay
nbstice per8 se habla del 96% de exactitud, con 72% de pacienb
es que evitaron l a laparatomía. E l use de l a laparoscopia segui - r& jugando un papel importante en obstetricia y ginecelegfa.
-F9-

.._ e..
L
L
L
c
L_
c
L
P
L_
P
L
r-
i.
Colpomicroscopia
EI. coipomicroscopio proporciona una ampi i f i cac i6n mayor
que e l colposcopio. El e p i t e l i o c e r v i c a l s e t i ñ e vi ta lmente
con hematoxi l ina de Meyer o azul de t o l u i d i n a y pueda obser-
v a r s e l a h i s t o i o g í a s u p e r f i c i a l de l e p i t e l i o cervical. Como
e s t e campo de v i s i 6 n e s l i m i t a d o , y i a profundidad de foco
no e s mucha, e l método resul tado complicado y no t a n popular
que pueda emplearse si-st em4t icamente.
S i desea información a d i c i o n a l sobre e s t a t e c n i c a , e l
l e c t o r debe c o n s u l t a r l a e x c e l e n t e r e v i s i ó n de Wilbanks.
BlopsisL
!\ ( Nuestra p r e f e r e n c i a personal e s obtener una b i o p s i a di-
r i g i d a con colposcopio cuando e l f r o t i a de Papanicolaou e s
a n o r m a l o so hay una l e s i ó n c e r v i c a l p e r c e p t i b l e a simple
vista o con e l colposcopio. Debe recordarse que e l anatomo-
patóiogo ~610 puede b a l o r a r e l m a t e r i a l que s e l e proporcio-
n a y e s muy importante obbener porciones adecuadas de t e j i d o
aunque l a b i o p s i a en ocas iones r e s u l t e técnicamente d i f í c i l .
Para e s t e f i n , s e cilspone (&e v a r i o s instrumentos d i s t i n t o s
para b iops ias . Extirpan una porción pequeña de t e j i d o y l a
hemorragia s u e l e s e r m i n i m y fác i l de contener con presión
o l a a p l i c a c i ó n de n i t r a t o de plata o de so luc i6n de Monsel. Cuando no s e dispone de un e s p e c i a l i s t a entrenado en
co lposcopia , s e adopta ampliamente l a t e c n i c a de l a b i o p s i a mfLLtiple de t b l a d r o , con dos bocados de l a pinza a las 12 y
6 horas d e l r e l o j -que son los sit ios mas f r e c u e n t e s de p r i n -
c i p i o de una neoplas ia - o con cuatro mordidas de l a pinza a,
las 1 2 , las t r e s , l as s e i s y a las nueve d e l r e l o j de l a c i r
cunferenc ia c e r v i c a l a n i v e l de l a unión p l a n o c i l i n d r i c a . -

Sin embargo, no es un método muy s t i t i s fac tor io para va lo rar e l cue l lo . S i l b a r y Woodruff señalaron que con l a b iops ia en los
cuatro cuadrantes se pasaron por a l t o 11 de 185 (6s) carcinomas
invasores. Por tanto, a menas que estas b iops ias en sacabocado
tomadas más o menos al azar muestran un cáncer invasor, suele
s e r neceshrio obtener una b iops ia circunferencia1 amplia deno - minada b iops i en cono a f i n de e s ta r seguros de no pasar por al
t o un foco de cáncer invasor. -
Lo dicho antes no s e ap l i ca a l o s casos m4s avanzados, en
los cuales cualquier parci6n de l t e j i d o extraido de cualquier
parte de l a l e s i ó n macroscópica demostrará cáncer, y generalmen - t e nada más que cáncer. incluso en l o s casos más avanzados s e
recomienda l a b iops ia para d.eterminar e l t i p o anatomopatoi6gico
exacto de l a l es ión , tambien para el iminar l o s raros casos en
l o s cuales l e s i ones como l a teberculosis c e r v i c a l pueden e s t i m
l a r e l cuadro macroscópico de l cáncer. Aunque tenemos e l mayor
respeto para los métodos c i t o l ó g i c o s , es eaeo que e l tratamien-.
t o se establezca antes de obtener b iops ias de confirmación.
-
Gonización de l cuello
Cuando es imposible v i sua l i z a r l a uni6n escamocilindrica
con e l colposcopio, l a i e s i 6n se extiende a l i n t e r i o r de l conduc
t o y no es pos ib l e v e r l o s l.imite8 superiores, o no concuerdan
e l f r o t i s , l a valoración col.poscópica, y l a b iops ia d i recta , es
t á indicado prac t i car una b iops ia en cono. S i no se dispone de
un colposcopio y no hay 1esi.ones macroscbpicas en e l cue l l o n i
zonas s in t inc i6n en l a grueba de S ch i l l e r , también está ind i ca
do hacer una conizaci6n diagn6stica. Esta t écn ica se ha denomi
nado con frecuencia “cono con cuch i l l o f r i o “ para d i f e r enc ia r l a
de una conización ca l i en t e , que se pracGica en trastornos i n f l a
matorios cor1 e l ec t rocauter io , carboniza e l t e j i d o y resu l ta i na
decuada para estudio c l topato i6g ico . La conización d i a a o s t i c a
-
-
- -
- -
- 6 \ -

e s fit11 no s o l o para estab lecer e l diagnostico de carcinoma i n
s i tu , sino es además muy importante para descartar un cáncer
invasor, pues sieinpre hay que recordar que e l carcinoma i n S i tu
suele e x i s t i r en l a p e r i f e r i a de un cáncer invasor verdadero.
Una b i ops i a c e r v i c a l en cono impl ica simplemente ex t i rpa r
una p ieza de t e j i d o c e r v i c a l en foriua cónica que incluya toda
l a zona de anormalidad. Desde e l punto de v s t a de l laborato - r i o , l a s dos princiGaies necesidades son l a s siguientes: i) te-
n e r l a seguridad de que e l t e j i d o se ex t i rpa de manera que r e - v e l a l a mucosa endocervical coma e l e p i t e l i o plano del cue l l o
vaginal, y l a porción necesaria subyacente de l estroma y &&du
l a s ; 2) preparar un número de bloques y co r ta r lo su f i c i ente , a
n i v e l e s var iab les , para tener l a seguridad de oue no se de j e
inadvert ida una pequeña zona, de carcinoma i n t r a e p i t e l i a l . La
primera de estas precauciones parece evidente, ya aue a s i e l ana - tomopatóiogo puede va lo rar n.o s o l o l a l e s i ó n i n s i t u sino tam - bién l a pos ib i l idad ,de invasion temprana. Po r l o que se r e f i e r e
a l segundo punto, debemos insist ir qn que un informe anatomopa-
t o i ó g í c o basado en un s o l o c.orte puede s e r causa de grave e r r o r
diagnóstico en etapas muy tempranas de l cáncer.
-
Desde l a ins t i tuc i ón de l a colposcopia mas o menos como es-
tudio de rut ina para l a valoracion de anormalidades cerv i ca l es ,
l a mayor par te de l o s cen-trcis ha observado una disminución impor
tante en e l númer; de biopsi.as diagnósticas en cono como se ha
comentado, S t a f l y uattinglgr practicaron sólo 80 conizaciones en
una s e r i e de 1410 pacientes turnadas para valoración coiposcópi-
ca por c i t o i o g i a c e r v i c a l ariormai.
en quienes l a valoración coi.posc6pica no fue s a t i s f a c t o r i a , ne-
ces i taron conización diagnóstica.
-
Cincuenta y cuatro (4.3$),
RI pacientes embarazadas l a morbilidad por hemorrag-a (9.4%)
y parto prematuro (7.4)96) complicó l a b iops ia en cono entre 180
pacientes que dieron a conooer Averet te y co l . La valoración
- 6 2 -
....
r-
L
L-
r
L
coiposcópica de pacientes embarazadas con f r o t i c de Papanico-
l aou anormales ha elimrnado c a s i por com l e t o l a necesidad de
l a b iops ia en cono en e s t e grupo. Lurain y Gallup, Talebian
y colaboradores y De P e t r i l l o y colaboradores han comunicado
resultados excelentes usando colposcopia para va lo rar a pacien - t e s embarazadas.
CLASIFICACION CLINICA DEL CANCER CERVICAL.
Es obv io que para un estudio camparativo de los informes,
e s tad i s t i cos y los resultados terapeuticoc de l cancer c e r v i c a l
se neces i ta un sistema uniforme de c l a s i f i c a c i ó n por etapas pa
r a ii,ue l o s grupos de pacientes sean similares. Ya que muchas
enfermas con cáncer cervical. se tratan con rad io te rap ia y nun-
ca se someten a laparotomia exploradora o b iops io de g a n e i o s
l i n f á t i dos , e l sistema de c i a s i f i c a c i ón por etapas debe s e r
c i i n i c a mas que qu i rú ra co , para i n c l u i r a l a s pacientes t r a - tadas con todas l a s modalidmies. Se han propuesto var ias ela-
s i f i c a c i one s a traves de 1 0 2 1 apos, pero l a internacional adop-
tada por l a Federación internacional de Ginecologfa y Qbs t e t r i
c i a (FIGO) se usa amp1iameni;e hoy en día. En e l sistema de '<
c l a s i f i c a c i ó n por etapas uti. i izado en e l informe h u a i de l o s
Resultados d e l Tratamiento de l Carcinoma de l Utero JC publicado
bajo e l pa t roc in io de l a Federación internacional. Las pacien
t e s se c l a s i f i c a n antes de someterlas a n i n e tratamiento u t i
l i zando s610 l a s técnicas di .agn6s~icas disponibles comunmente,
como b iops ia , examen ba jo anestesia, cistoeoopia, proctoscopia
rad iogra f fas , pielograma intravenoso y enema de bario. Para
estab lecer l a etapa de una naciente dentro de l a c ias id i cac i6n
internac ional no se permite l a laparotomia exploradora con b i o
p s i a de ganplios l i n f á t i c o s y l i n f a g i o g r a f í a , dos técnicas de
uso comun algunas partes. E l l o no s i g n i f i c a , por supuesto,
que no deban hacerse es tas pruebas diagnosticas n i oue no se
-
-
- -

consideren l o s resultados a l planear e l tratamiento. Sino,
simplemente, que no pueden considerarse en l a c l a s i f i c a c i ón o f i
c i a l por etapas de las pacientes con cáncer ce rv i ca l . -
Se ha reconocido ampliamente que hay un e r r o r imp l i c i t0 en
es t e sistema c l i n i c o de c l a s i f i c a c i on por etapas. V e n Nagel ha,
encontrado que e l e xwen c l i n i c o s610 da un 7596 de precis ion
cuando se compara con l a c l a s i f i c a c i ó n por etapas en exáaenes
bajo anestesi. En un grupo de 123 pacientes que se sometieron
posteriormente a l a c l a s i f i c a c i ón por etapar quirúrgicas, e l
examen c l i n i c o l a establec io correctamente s610 en e l 54% de l a s
ocasiones, y e l examen bajo anestesi en e l 74% de l a s pacientes
E l l o depende en g r a n parte de l a s metástasis en ganglios i i n f& -
t i c o s pé l v i cos que sólo pued.en diagnosticarse mediante laparoto
mis, y ya que eetos hal lazgos no in f luyen actualmente en e l t r a
tamiento, se aonsidera que l a laparotomia exploradora no es un
método necesario o sistemático para la c l a s i f i c a c i ó n por etapas.
Meiga y Brunschwig han sugerido un sistema q u i d r g i c o para l a
c l a s i f i c a c i 6n por etapas de iJacientes tratadas en forma prima - r i a con cirugxa rad ica l , pero no se ha u t i l i z ado extensamente.
- -
Toda paciente con c h c e r c e r v i c a l debe someterse a l a va lo
raci6n d i a e ó s t i c a adecuada y se r c l a s i f i c ada fomalmewte antes
de i n i c i a r e l tratamiento. Una vez establecida l a etapa, es PO
s i b l e que no se cambie a medida que sukgen nuevos acon8ecimien-
t o s en e l curso del tratamiento o de l a v i g i l a n c i a U t e r i o r .
-
-
TRATAMIENTO DEL CARCIñOKA IHTRBEPITELIAL.
EL tratamiento de l carcinoma i n s i t u del cue l l o est4 l e j o s
de haberse estandarizado y en l a decis ión terapéutica inf luyen
muchos factores. Aunque l a rad ioterapia rara vez se usa, es un
tratamiento e f i c a z y puede considerarse para enfermas que quiza
no to leren l a c i rug ia por su estado médico y su edad.
- 6 4 -

Clas i f i cac i ón por etapas quirurgicas de l carcinomsc cerv i ca l
se& Melga - Brunschwig.
Clase O
Carcinoma i n s i tu , también denominado carcinoma preinvasor
o i n t r a e p i t e l i a l , o microcarcinoma.
Clase R El carcinoma se h a i l a estrictamente l imitado a l cuel lo.
Clase Ao; DespuBs de una b iops ia po s i t i v a para carcinoma i n f i l t r a n t e
no se descubre tumor c e r v i c a l en l a p ieza qu idwg ica .
Clase B
B1 carcinoma se extiende partiendo del cue l lo para abarcar
l a vagina, exceptuando su t e r c i o in f e r i o r . El carcinoma se
extiende por e l cuerpo. Puede a f e c t a r parte a l t a de vagi-
na y cuerpo. La extensión vaginal, l a uterina, o ambas,
pueden ser directamente o por metástasis.
Clase C
E l carcinoma ha afectado t e j i d o s paracervicales, paravagi-
nales, C ambos, por extensi6n d i rec ta por vasos l i n f á t i c o s
o en ganglios intrat isu lares . Hay metastasis vaginal, exten-
si6n d i recta , o ambas, en e l t e r c i o i n f e r i o r de vagma.
Clase D
Vias y gangi ios i i n f á t i c o s afectados mas a l i a da l a s r e - giones paracervical 3 paravaginal. Ello incluye todos los vasos l i n f á t i c o s , gangl ios, o ambos, en l a p e l v i s verdade-
ra, excepto en l a forma correspondiente a l a c lase C. Me-
t a s t a s i s en ovar io o trompa.
-- h s-
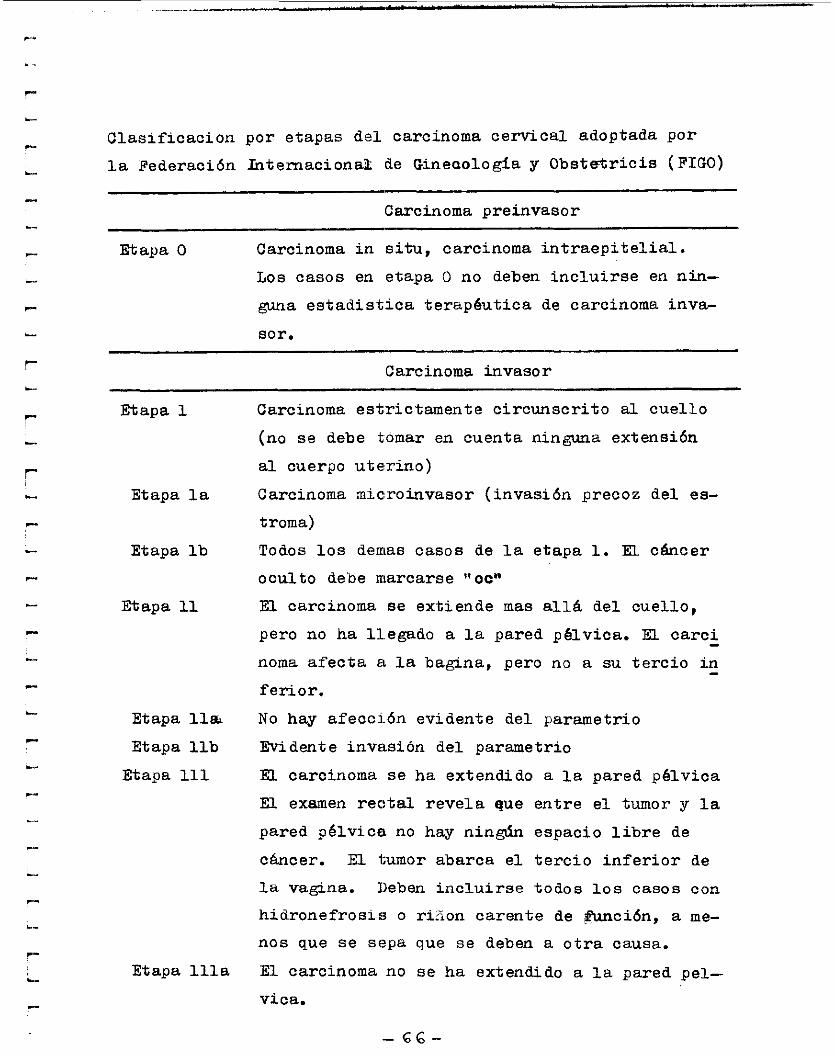
Clas i f i cac ion por etapas de l carcinoma cerv i ca l adoptada por
l a Federación Internaciona2 de Gineaología y O b s t d r i c i s (FIGO)
Carcinoma preinvasor
Etapa O Carcinoma i n s i tu, carcinoma i n t r a e p i t e l i a l .
Los casos en etapa O no deben i n c lu i r s e en nin-
guna e s t ad i s t i c a terapéutica de carcinoma inva-
sor.
Carcinoma invasor
Etapa 1
Etapa l a
Etapa l b
Etapa 11
Etapa lla Etapa llb
Etapa 111
Etapa l l l a
Carcinoma estrictamente c ircunscr i to a l cue l l o
(no se debe tomar en cuenta ninguna extensión
a i cuerpo uter ino)
Carcinoma microinvasor ( invasión precoz de l ea-
t roma)
Todos l o s demas casos de l a etapa 1. El cáncer
oculto debe marcarse r t ~ ~ n
E l carcinoma se extiende mas a l l á del cuel lo ,
pero no ha l l egado a l a pared péiv ica. EL ca rc i
noma a f e c ta a l a bagina, pero no a su t e r c i o i n
feriar.
No hay a fecc ión evidente del parametrio
Evidente invasi6n del parametrio
El carcinoma se ha extendido a l a pared p é i v i c a
E l examen r e c t a l r e v e l a que entre e l tumor y l a
pared p é l v i c a no hay nin& espacio l i b r e de
c h c e r . E l tumor abarca e l t e r c i o i n f e r i o r de
l a vagina. Deben i n c lu i r s e todos los casos con
h idronefros is o ririon carente de gunción, a me-
nos que se sepa que se deben a o t r a causa.
E l carcinoma no se ha extendido a l a pared pei-
vica.
- -
- 6 6 -

Etapa lllb Extensión a l a pared pé lv ica , h idro f renos is o
riñón carente de función.
EL carcinoma se ha extendido mas a l l á de l a
p é l v i s verdadera o ha afectado clinicamente l a
mucosa de l a v e j i g a o e l recto. Un edema vesi-
cuioso en s i no permite i n c l u i r e l caso en l a
etapa iV .
Etapa 1 V
Etapa 1Va Extensi6n de l a neoplas ia a los órganos adya - c a t e s .
Etapa 1Vb Extensión de l a neoplasia a órganos distantes.

j - c
L
-- i L
r .- *-
& l a s pacientes t i p i c a s que han completado su fami l i a y
no ob jetan l a histerectomia, l a intervención qu in í rg i ca acepta - b l e para e l carcinoma i n s i t u debe s e r l a histerectomia t o t a l ,
con cuidado de ex t i rpar todo e l cue l l o y conservar en l a s muje
r e s jovenes uno o ambos ovarios. La inteHenci6n puede p rac t i
carse por l a s vias abdominal o vaginal. La valoraci6n preope-
r a t o r i a cuidadosa mediante l a oolposcopia y l a prueba de Schi4:
l l e r delinean l a extensión de l a l e s i ó n y determinan l a varia-
c i ón en l a cantidad de l a cúpula vaginal , s i acaso alguna, que
debe extirparse.
- -
S i l a paciente desea conservar su potencial de reproduc-
atón u ob je ta l a histerectomia por cualquier motivo, pueden
pract icarse conización, cauterizaci6n o c r io te rap ia , como a i - ternat ivas a l a histerectomia. Los pros y contras de estos
métodos se comentan despúés y es importante que l a paciente
pa r t i c i pe an esta decisión, que se l e debe exp l i car l o mas c l a - ramente pos ib le .
Conieación
La conización como tratamiento s e ha empleado mas que l o s
o t r os dos métodos simples y fue usada primero en lugar de his-
terectomia para preservar l a f e r t i l i d ad . Muchos estudios en
l a s decadas de los dncuentas y a l p r inc ip io de l o s sesentas,
antes de que aumentara e l empleo d e l colposcopio para de l inear
cuidadosamente los i f m i t e s de l a l es ión , mostraron que l a coni
zación t en ia una f a l l a de aproximadamente 20% como pudo compro
barse por los f r o t i s subsecuentes a l a conización, o por $umo-
rea residuales en piezas quirúrgicas de histerectomia. Estu - d i o s mas rec ientes , por ejemplo de Er i ege r y McCormack, han de - mostrado una frecuencia menor (9%) de enfermedad residuai des-
pués de l a conizacibn, debido a exploración preoperator ia cui- dadosadel cue l :~o y a que no ex i s t e duda en cuanto a l a exten -
- -
-68 -
s ión de l a s lesiones.
Una de l a s ventajas de l a conización es que conserva l a
f e r t i l i d a d . Sin embargo, l a conización por s i mismo p u d e te-
n e r e fecto adverso sobre l a función reproductiva. MarVicar y
Wi l locks estudiaron cerca de 632 pacientes que sufr ieron c o d -
zacion con anterioridad. Eiicontraron una frecuencia de f e r% i -
l i d a d de 64 $, pero aunque quedaron embarazadas, 24 $ presenta - ron aboryo o parto greniaturo. Otro estudio de Kullander y S jo
be rg demostraron excelentes porcentajes de f e r t i l i d a d despues
de l a conizaci6n cerca de 83 $, pero de nuevo se presentaron
aborto y parto prematuro en 21 $ de l o s casos. Ut i l i zando co-
mo t e s t i g o s l o s antecedentes de l o s embarazos de l a paciente
antes de l a conización, B j e r r e y colaboradores señalaron un 17. 1 $ de aborto4 espontaneos despues de l a biops ia en cono en com
paración con e l 11.6 $ antes de l a conización. La frecuencia
de premadurez fue identAca en ambos grupos.
-
-
La pr inc ipa l complicación de l a b iops ia en cono es l a he-
morragia. V i l lasanta y Uurkan señalaron que en su s e r i e un lO$
de 200 pacientes tuvo hemorragia posoperatoria que necesit6
transmsibn de sangre en e l 3.5 % de l o s casos. En ocasiones,
hay in f e cc i ón pé l v i ca y estenosis cerv ica. Eh pacientes embara
zadas hay e l p e l i g r o de inducir e l parto. -
Cauterizaci6n y c f i oc i rug ia .
El trataniei i to de a t i p l a c e r v i c a l y carcinoma in t raep i t e i.-
l i a s l por cauter izacion o congelacion se ha desarrol lado mas r e
cientemente y t i ena l a granventaja de que puede r ea l i z a r se en
pacientes externas.
-
Los resultados a l a r go plazo no es pos ib le va lo rar los a h ,
pero s i pal timos de f r o n t i s pos i t i v os pers is tentes después de l
trataniento, Wilbanks y cola,boradores encoritraron que con caute -
. - ...
- c
ii
c - P
L_
P
i-
i
L
...
r L
c
r i z a c i ón l a a t i p i a fue curada en 84 $ de l a s pacientes.
Existen muchos defensores de l a c r i o c i rug i a para t rabar neo - p las i as i n t r a e p i t e l i a l e s de cue l l o uterino. Creasman y colabora,:!
dores publicaron un a r t i cu l o sobre l a pers i s tenc ia de l tumor en
p iezas quirúrgicas histerectomizadas de 75 pacientes con b iops ia
que mostró caccinoma i n s i t u o d isp ias im severa. Con l a congela-
c ión doble, 82 $ de l o s e pecimenes no mostraron tomor residual,
pero s i se empleo una s o l a congelaci6n hubo pers i s tenc ia d e l tu-
mor de 48 $ en l a s p iezas qui.nirgicas extraidas, Kaufman e Irwin encontraron un 5.8 $ de fracasos en 238 pacientes tratadas con
c r i o t e rap ia después de uAL raspado endocervical negativo, pero un
20 $ de f racasos en 48 mujeres en quienea e l respaldo del endo - c e r v i x mostró cé lu las anormales. Como i o s e n d a Townsend, e l t a
malo de l a l e s i ó n tambien se re lac iona directamenTe con e l indi-
c e de ex i t o s de l a c r io te rap ia . Sevin y colaboradores han publ i
cado ocho casos de carcinoma invasor de l cue l l o despues de cr io-
c i rug ia de l misino. Probablemente dependieron de una valoración
pretratamienGe inadecuado y tambien fracaso de l método, pero es
importante no o l v i da r l a os:tbJidad de pers i s tenc ia o recurren-
c i a de una neoplas i epite1ia:L despues de e$te o cualo ider o t r o
tratamiento, incluyenco l a histerectomio por carcinoma i n s i tu .
-
-
-
Ha hahido muchas controversias, algunas de e l l a s acaloradas
sobre los me*itos r e l a t i v o s ide l a cauterizacion y l a congelacion
Sin embargo, en base a l o s datos publicados en un interesante es
tudio comparati o de M i l l e r y Eis t e in concluimos "no se comprobó
a i f e r enc ia n i en e l número de curaciones sintomáticas n i en e l de
curaciones ob je t ivas" .
-
BI res..imen, l a s pruebas rec i entes parecen mostrar que momo tratamiento d e f i n i t i v o y con menos problemas cie cont ro l pos t e r i o r
e l método de e l ecc ión sigue ,siendo l a nisterectomia ya sea abdo-
minal o vaginal. Sin embargo, para l e s i ones de bordes definirlos o cualido es de grimordial importancia preservar l a f e r t i l i d a d ,
l a conizaci6n, cauterización o congelación pueden emplearse como
métoaos de substitución. Sin importar e l metodo seleccionado,
tanto l a paciente eomo e l medico deben es ta r de acuecdo sobre e l
periodo prolongado de v i g i l anc ia .
que ocurrió una vez en e l cue l l o puede iresentarre de nuevo, so-
bre todo s1 hay una zona de transformación ac t i va , y l a unica ga - ran t i a contra e l desar ro l l o de un cancer invasor es l a vigilan- c i a continua.
La transformacibn neoplásica

R E S U M E N La c i t o l o g i a e x f o l i a t i v a representa e l método más práct ico
para l a detección temprana del cáncer cerv ica l . Aunq.ue e l ind i
ce de f a l s a negat iv idad es extraordinariamente a l t o (10 - 20 q6)
en una so la muestra, é s t e puede s e r considerablemente disminuí-
do por medio de r epe t i c i ón de l o s f r o t i s c i to lóg i cos .
Eh presencia de c i t o l o g i a anormal se debe l l e v a r a esto l a
evaluación u l t e r i o r del cérv ix . La prueba de S c h i l l e r der4 re-
sultados conf iab les s o l o en un bajo porcentaje de pacientes en
r iesgo. Con l a técnica de l a b iops ia c e r v i c a l c i ega de cuatro
cuadrantes e l e r ror diagnóstico estimado es por encima del 20 $.
Sin embargo, cuando se u t i l i z a l a prueba de S c h i l l e r para d i r i -
g ir l a s b iops ias cerv i ca l es y cuando l o s especfmenes de b iops ias
mfi l t iples se examinan con numerosos cor tes histo16gicos, se
puede obtener mayor certeza. La conización del C 6 r V i X represen
t a un método conf iab le de evaluación ce r v i ca l , pero su costo
es elevado y e l índ ice de complicaciones es importante, en espe
c i a en l a s gestantes. La coiposcopia es un método práct ico,
barato, conf iable , de ba ja niorbilidad, excelenta para evaluar e l
c é r v i x de mujeres cuya c i t o l o g i a es anormal. De acuerdo a l o s
h@l laagos colposcópicos l a s pacientes se dividen en 3 grandes
grupos$ 1) Normales.- Sólo se recomiai ia contro l cito16gico: sólo en l o s
casos en qe l a c i t o l o g i a se presente repetidamente sopechosa o
se transforme en pos i t iva , esta indicada &a conización.
2 ) Coiposcopia " insatisfactoria".- La c o n i z a c i h está indicada
para descartar neoplasia s i l a c i t o l o g i a es p o s i t i v a o peresis-
ten tement e sospechosa.
3) Anormales.- Siempre e s t á indicada l a b iops ia ba jo control
colposcópico; s i l a l e s i ó n se extiende dentro de l c a n a andocer
v i c a l está indicada l a conización; S i e l diagnóstico de l a b iog
-
-
-

s i a d i r i g i d a es de d i sp las i a l e v e o moderada, se puede ap l i c a r
un tratamiento conservador; cuando se t r a ta de d isp las ia severa
o carcinoma i n s i t u se puede ap l i c a r e l tratamiento d e f i n i t i v o
( conización t e r a p k t i c a , histerectomia) s in necesidad de coni-
zación diagnostica;. cuando e l diagpóstico es de carcinoma mi - croinvasor, l a conizaci6n diagnóstica está indicada para eva - l ua r exacta.mente l a extensián y profundidad de l a invaeión.
ih e l caso de cáncer invasor, e l tratamienfio dependerá de l es-
t ad i o c l i n i c 0 de l a enfermedad.
Uno de l o s usos más va l iosos de l a colposcopia es l a cer-
t e z a diagnóstica y m w j o de l a s pacientes embarazadas con c i -
t o l o g l a anormal. Las pacientes embarazadas son excelentes can
didatos para l a evaluación coiposcópica de un Papanicolaou a - normal, ya que l a eversión f i s i o l ó g i c a que se presenta en es te
estado permite muy bien l a visuaLizaci6n de l a unión escamo-
columnar completa. ih esta€! pacientes, cuanto l a b iops ia d i r i
g ida por colposcopia encuentra d isp las ia severa o carcinoma i n
s i tu , e l tratamiento d e f i n i t i v o puede posponerse hasta después
de l pai%o, ev i tándoles los r iesgos de l a conización en estado
de gestación.
-
-
-13-

B I' B L I O G R A F I A
- STAFG, A. ERIERICH ,J.R.E. G. & MATTYNGY, RF. Detection of cervical Neoplasia - Reducfmq the risk of error; Clinical Obstetrics & Ginecoloqy. pp 16 - 22; 238-260. June 1973.
- DR. GRETCHE HINDERSMAN PRACTICA Privada de Obstetricia y Ginecoloqía, Pruebas sistema- ticas de Papanicolaou. Mundo Médico pp. 81 - 85. Junio 1986.
- DR HOWARD W. JONES, DRA. GEORGEONNE SEEGAR. .Tratado de Ginecoioqfd . pp 299 - 332.
- MEHRAN M. The impact of diagnostic ultrasound on the prediction intrauterine growth retardation in devolopinq countries. Int. J. Ginecoloqy - Obstetrics Vol. 26 1988 pp 315 - 378.
- FRANK H. NETER Coleccidn Ciba de ilustraciones Médicas. Tomo I1 Sistema Reproductor.
- WEBSTER JHON G. Encyclopedia of Medical Devices.
- DR. PINO JUAREZ VERGARA, DRA, E MEZA BAND. Cáncer Cérvico Uterino, Histología Normal y Citología Exfoliativa. pp 13-15 y 19-22.
- WYNN W I T / LAWRENCE M. ELSON Anatomfa Cromodindmica pp 96-98. Ferndndez Editores.
- CANCER. A Journal of the American Cancer Society -' 'Vol 64 pp 2069- 2075, 2104 - 2109.
Vol 61 pp 679-687.
Human Papillomaviruses and the Pathogenesis of Cervical Neoplasia
A Study by In Situ Hybridization
JEAN W. GUPTA. PHD:.t KAORU SAITO. MD,S AKEMl SAITO. MD,S YA0 S. FU, MD.S AND KEERTl V. SHAH, MD. DRPH'
in a previous topographic shdy ofcenial conization specimens, cvndylommus changes were commonly present III direct contact with inhaepitheüd neophsh d were 8iwaya bated dist8J (ectocervial side) to the neoptuh. Viral DNA was detected by ir sita hykidintba using "S-hbekd nick mmhted DNA probn in 50 of '10 asea (71%) which bid adequate IesiOW: HPV-16 in 30, HPV-18 in ten, HPV-31 III six, d multipk types in fwr cases. HPV4/I1 detected wly once, in a multipk infeaiOii. As a ni*,
s positive cervix contained a single v h s type, d the same v i m type m a found in mudyiwiitcui d neophetic ueas. Thc results s-t that the neoplutic process is initiated in the M of condyloma toward the endocervix d, once established, extends proximally toward the cervical cand. Capsid aotigen was detected b 19 aseq hdicntiw that a proportion of the h-e lesions is potentiilly infecüom.
Cancer 64:2104-2110, 1989.
UMAN PAPILLOMAVIRUSES (HPV) of the genital tract H have been recovered from tissues showing a wide spearum of pathologic lesions as well as from histoiogi- cally normal tissues.' HPV-6 and HPV-I I have been as- sociated predominantly with condylomas and HPV-I6 and HPV-18 with high-grade intraepithelial neopiasias and invasive cancers.' HPV-31 is associated with both mild and severe lesions.' Cervical intraepithelial neoplasia (CIN) frequently coexists with condylomatous changes in affected cenices.'" We have examined ceMcai conization specimens removed for the diagnosis and treatment of high-grade cervical lesions in an attempt to define the role of human papüIomavinises in the pathogenesis of ceMcai cancer. in an earlier report, the topographic relationship of condylomatous changes to CIN was studied by an ex- amination of 101 conization specimens! More than 90% of CIN and condyloma lesions were found within, or trans$rrssing, the transformation zone. Seventy-five per-
2 104
cent ofthe tissues contained both CIN and condylomatous lesions. Condylomatous changes were invariably distal (toward the ectocervical side) to CIN and in a majority of cases were in direct contact with CIN.
In this report, we describe the virologic correlation of the topographic findings. Paraffin sections of the coniza- tion specimens were examined for the prevalence and dis- tribution of HPV DNA by in silu hybridization, a tech- nique which is well suited to correlate the morphologic features of the lesions with the presence and type of HPV DNA. The sections were also examined for HPV capsid antigen. We found that despite the high frequency ofcon- dylomatous changes assoCiated with the high-grade lesions in cervical conization specimens, HPV-6 and HPV-I I were virtually absent in these tissues. HPV-16, HPV-18, and HPV-3 I were identified from a majority ofthe lesions. As a Nk, the areas with different grades of seventy in a conization specimen displayed the same HPV type. Also, about a fourth of the tissues contained HPV capsid an- tigen, an indication that some of these lesions were po- tentially infectious.
Materials and Metbods
Coniralion Specimens
In the topographic study described previously> 101 conization specimens removed between 1981 and 1983 for ceMcaI dysplasia and carcinoma in situ at the Uni- ver& of California, Los Angeles (UCLA) Medical Center.
r
- t t t t C c -
1
t ( S
a c I
S
I
3
I t 2
I S
t I
\
I
1
t t
\
c c
-
-
-

No. IO HPV AND CERVI<:AL NEOPLASIA Gupta el a/. 2105
TABLE I. Rcqwney ofDe<ation of Human Rpülomavinu DNA d Canid Antinen in Gmid Conization T k u s
No. mcd No. &tive 1%) ~
HPV DNA 70 u) (71%) HPV ppvd pnIig.cn 67 19 (28%)
HPV DNA and iaIig.cn 70. 17 (24%)
Only HW pnIig.cn 67
HPV DNA or in&m 70. 52 (74%)
Only HPV DNA 70 33 (47%) 2 (3%) -
H P V humin papillmavinis. Sixtylcvcn tisuer tmtcd for capsid anIig.cn
were analyzed. The ages of the women ranged from 20 to 89 years (mean age, 36). These specimens were recut (233 blocks, one-three blocks per cone) to obtain paraffin sections for in situ hybridization, immunoperoxidase test and hematoxylin and eosin (HdrE) staining. Pathologic diagnosis was made by criteria desCnbed previously6 and is based on the most severe lesion found in the examined sections.
in Situ Hybridization
Serial sections on sepanite slides were hybridized with 35Slabeled, nick translated whole genomic HPV DNA probes. pBR vector DNA probe served as a negative con- trol. Viral DNA probes of HPV-á+I I (mixed), HPV-I6 and HPV- I8 (all.prepared from clones kindly supplied by Dr. H. zur Hausen) and HPV-31 (from a clone kindly supplied by Dr. A. Lorinn) were employed. Sections of tissues known to be positive for HPV-6, I 1 and 16 were included in each test as positive controls. Hybridization was performed as described previously: with the following modifications. Paraffin sections were cut onto organosi- lane-treated siides'; this treatment almost completely pre- vented loss of sections during the procedure. Sections were treated with a reduced concentration (IS &mi) of Pro- teinase K solution at 37°C for 15 minutes. The reduction of Roteinax K concentration improved the preservation of morphologic features while still allowing adequate
probe penetration of the tissue. Slida were hybnáized overnight insiead of for 2 days. The final hi&-tcmperaturc washes at 55OC were performed with 0.25 X SSC instead of 0.5 x SSC. The increased stringency reduced nonspe- cific background hybridization as well as cross-hybridiza- tion between related HPV and permitted distinction be- tween HPV-16 and HPV-31. Hybridized sections were scored for the presence and type of HPV DNA, intensity and location (neoplastic or condylomatous ana) of signal, hybridization pattern (diffuse, focal or mixed), and for basal cell hybridization. No attempt was made to distin- guish between HPV-6 and HPV-I 1.
Test for Capsid Antigen
The immunoperoxidase test for capsid antigen was performed using anti-BPV polyclonal antibody (Dako Corp., Santa Barbara, CA) and the anti-rabbit igG ABC kit (Vector Laboratories, Burlingame, CA) as described? This polyclonal antibody prepared by immunization with disrupted viral capsids recognizes capsid antigens of all HPV.
Results
Sections from one to three blocks of each conization specimen were examined for these studies. Tissues avail- able forthis study from 31 ofthe 101 conization specimens contained only normal epithelium, or no epithelium, or mere traces of atypical epithelium. They were uniformly negative for HPV DNA and capsid antigen and are ex- cluded from further analysis. Ofthe 70 tissues which dis- played adequate pathologic lesions and were examined for HPV DNA, 67 were also tested for HPV capsid an- tigen. Human papillomavirus DNA and HPV capsid an- tigen were detected, respectively, in 71% and 28% of the tissues (Table I). Evidence o f HPV infection by the pm- ence of either DNA or antigen was demonstrable in 74% o f the tissues. Only HPV DNA and only HPV antigen were detected, respectively, in 47% and 3% of the tissues.
TABLE 2. DirVibution of Human Papillomavinis Typs by Moat Sevm Lepion REnt
HPV type No. of No. of DN k
D W O S i S ' FBSJ positive (a ) 6/11 16 18 31 Multiplet
Condyloma only 5 3 O I I O I CIN I 2 I O I O O O CIN II 14 lO(71) O 2 5 I 2 CIN 111 49 36 (73) O 26 4 5 I
Tntal 7n 5nr7ir O M 10 6 4 _ _ _ _ ~ ~ ~~~ ~~ ~ ~~
H W . human ppiuomawus; CM. emspl intncpthclipl neoplas¡r * The most severe laion in the hybriduÍd d o n s . t The multiple infdom wre: HW-18 and HW-31 in a condyloma:
HPV-611 I uid HPVJI, and HPV-16 and HPV-18 in two cssco ofCIN I t and HW- I6 and HW-18 in one CIN Ill. -

2106 CANCER November I S 1989 vol. 64
Distribution ofHuman Papillomavirus Types by Lesion Pathologic Features
Almost all conization specimens contained lesions o f different grades of severity. The pathologic diagnosis of a tissue was based on the most severe lesion Seen in the hybridized sections. The most frequent diagnosis was CIN 111, which accounted for 49 of the 70 (70%) cases (Table 2). Human papillomavirus DNA was found at about the same frequency in tissues with a CIN 111 diagnosis as in lower grade lesions. A single HPV type was de- in 46 of the 50 HPV-positive tissues; HPV-I6 in 30, HPV- I 8 in ten, and HPV-31 in six tissues. The HPV-6/11 was not detected in any of the cases which were infected with a single HPV type. Four tissues showed double infections (Table 2). In the study, HPV-6/1 I was identi6ed only once, present along with HPV-3 I in a CIN I1 lesion. Both HPV-I6 and HPV-31 appeared to be more frequent in CIN I11 lesions, relative to HPV-18.
Both condylomatous cells and CIN coexisted in most of the tissues. In most instances, there was either a gradual transition from condylomatous cells to CIN or condy- lomatous cells were contiguous to CIN. As a rule, in a DNA-positive ceMx a single viral type was locahed in both pathologic types. In 13 DNA-positive cases, there were separate discrete lesions in the tissues which were more than two histologic grades apart. The results of HPV typing and capsid antigen tesis for each of these lesions are shown in Table 3. In five cases, the same HPV type was present in both lesions and in two additional cases at least one HPV type was found at both sites. In four cases, only one site was DNA-positive. In Case 79 and probably
TABLE 3. Virologic Findingr in Cavs Showing Discrele Area Two or More Hi?.IoI&e Odes Ame
Condyloma or atypical
condvlomala CIN I1 or CIN 111
No. Case DNA AP DNA Ap
I 4 HPV-I6 - N- ... . .- - HFV-3 I - HPV- I8 3 18 HPV-18
4 20 HPV-I6 - HPV-I6
2 9 NCS
5 26 HPV- I8 - HPV- I8 6 33 HW-I6 - NS 7 39 HPV-16t18 - HPV-18 8 66 N s - HPV-18
NCS' 9 61 HPV-I6 IO 70 HPV-I6 - HPV-I6 I I 78 H P V W I t31 t HPVJI 12 79 HPV-I6 - HPV-18 13 91 HPV-16 - HPV-I6
-
H P V human ppübmvinu; Al: antigen. *An HPV typ n a repremu in the pobamidc<sted in uiu
twe by nonrviiyat hybridization (unpubürhrd diu).
FIGS. IA AND 18. A condyloma in a conization opcimen. (A) H & E, X312. (B) focal hybridization with HPV-16, X312. This specimen also displayed HPV capsid antigen.
Case 67, different HPV were present at the two sites. Thus, the data suggested that in a majority of the cases, histo- logically diverse and spatially discrete lesions in a tissue were caused by the same HPV type. In these 13 cases, viral capsid antigen was detected in one of CIN and eight of the condylomatous lesions.
Characteristics of Hybridization
Hybridization was seen only in the altected epithelium and never in the normal epithelium adjacent to the lesion or in the stroma. Intensity of hybridization signal ranged from banly deteciable over background to extremely strong. It is probable that very faint signals were masked by the background, which varied from test to test. Lesions associated with HPV-3 I and with mixed infections showed relatively stronger signals.
Two distinct patterns of hybridization, focal and diffuse, were evident. The focal pattern was d t e d with signals of moderate to high intensity, and with antigen-positive. lowgradc lesions (Figs. IA and 18, and 2). It occurred
No.
(H an
nt cr flc al
hi N di h: ai ir al
5
L
o1
lT
ti ii I< fi

No. 10 HPV AND CERVICAL NEOPLASIA Gupra 91 01. 2107
TABLE 4. com*iion of Hybridization Panmi and Human Paoillomavirus T we
FIG. 2. Faal hybridization in a CIN I lesion with HPV-31 probe (Hematoxylin stain, x400). This specimen alza diwlayed HPV capsid antigen.
near the epithelial surface, with the signal strength in- creasing toward the surface. This pattern probably re- flected productive viral infection. The diffuse pattern usu- ally displayed faint signals distributed uniformly through- out the depth of the epithelium and was associated with high-grade antigen-negative lesions (Figs. 3A and 38). Many tissues displayed a focal pattern in one area and a diffuse panern in another (Fig. 4). The diffuse pattern of hybridization was relatively more frequent with HPV-I6 and HPV-18 infections than with HPV-31 and multiple infections (Table 4). Basal cell hybridization was seen in about one third ofthe DNA-positive cases and was found relatively more frequently in HPV-I8 infections (Table 5). It was usually associated with CIN 11 or CIN Ill lesions.
Dislribution of Capsid Aniigen
The presence of capsid antigen is indicative of produc- tive v i ~ s infection. The antigen was detected most often in condylomatous areas, infrequently in CIN I or CIN II lesions and rarely in CIN 111 lesions. The antigen was found in 28% of all tissues, 35% of DNA-positive tissues
TOUI DNA HPV type
Dsttem cases 6/11 16 18 31 Multiple Hybridization positivc
Focal 16 O a 4 3 I Mired 17 O 9 1 3 4 muse 17 o I 3 5 0 O Total 50 O 30 IO 6 5
HPV human papillomavirus.
and 11% of DNA-negative tissues (Table 6). Productive infection was found in a significant proportion of tissues infected with HPV-16. HPV-18 and HPV-31.
Discussion
Overall, this study investigated the role of HPV infec- tion in the pathogenesis of cervical neoplasia. In the to- pographic analysis reported earlier? 68% of CIN lesions were found to be in direct contact with condyloma or atypical condyloma. Condylomatous areas were always located distal to the C IN areas, and koilocytosis was pres ent in 90% and 78%. respectively, of CIN K I N I1 and CIN 111. This observation confirmed the results ofprevious investigators that in a cervical lesion the les severe patho- logic type is located distal to the more severe pathologic
A major aim of the current study was to examine if condyloma and CIN were different manifestations of the same underlying process. The in siiu hybridization test was an excellent tool for this purpose because it allowed localization of genome to specific cells and therefore per- mitted a correlation between presence of vinis and cellular pathology.'3-" The test for capsid antigen was useful in two ways. First, it determined to what extent these high- grade lesions were still producing full viral particles. Sec- ond, the number of antigen-positive DNA-negative tissues gave some indication of the extent to which infections
type.'Gl2
TABLE 5. Correlation %tween Frequency nf Basal Cell Hybridization and Human Papillomavirus Typcs
Total DNA HPV type
hybridization caws 6/11 16 18 31 Multiple
Present 11 O 7 6 3 I Absent 33 O 2 3 4 3 4
Total 50 O 30 10 6 5
HPV human papillomavirus
basalcell Positive

--7 .. ., 2108 CANCER November I5 1989 Vol. 64
hos. 3A ANO 3B. A CIN 111 !esion h y b r i d ¡ with HPV-18 probe. (A) Low power view (hematoxylin stain, XIS6). (B) Higher magnification, displaying Faint, d i b hybridization (hematoxylin stain, X W ) .
with HPV types not represented in the probe panel were involved in cervical neoplasia.
Sixty-three of 70 tissues which had adequate pathologic features contained high-grade lesions (CIN I1 01 CIN Ill)
and most of them also contained condylomatous cells. Virologic evidence for the presence of HPV was obtained in 53 of the 70 (74%) specimens. The two specimens which contained capsid antigen but no HPV DNA very likely reDresented infection with HPV tvoes not included in the probe panel. They constituted aGUt a tenth ofaü antigen- positive tissues The 20 specimens (29%) with adequate pathologic types in which HPV DNA was not detected may represent infedon with HPV types not included in the probe panel or low copy numbers of HPV types in- cluded in the probe panel, The 70% rate of detection of HPV DNA in high-grade cervical lesions is in the range of detection rates in other studies in which tissues are examined with a similar panel of proba either by in sifu hybridization or by Southern hybridization.'"2
Despite the presence of condylomatous a l l s in most of the DNA-positive specimens, HPV-6/1 I was virtually absent from these tissues. Forty-six (92%) of the DNA- positive h u e s contained a single viral type. Among thesc, HPV-16, HPV-18, HPV-31. and HPV-ó/II accounted - 'Iac is íocil llcu tkc sad below (he- for, respectively. 30, ten, six, and zero specimens. The
mamxyün 6% ~250). finding of the predominance of HPV-I6 and HPV-18 in
Flo. 4. WII d8 CIN II-CIN 111 laion hy- to M HPV-IO
Ni
Al DI
LT U CI CI
th st
K tt el si t> tr O
a: tl tt le H V
si d b
fc 11
e P
H
C
g O
r I L
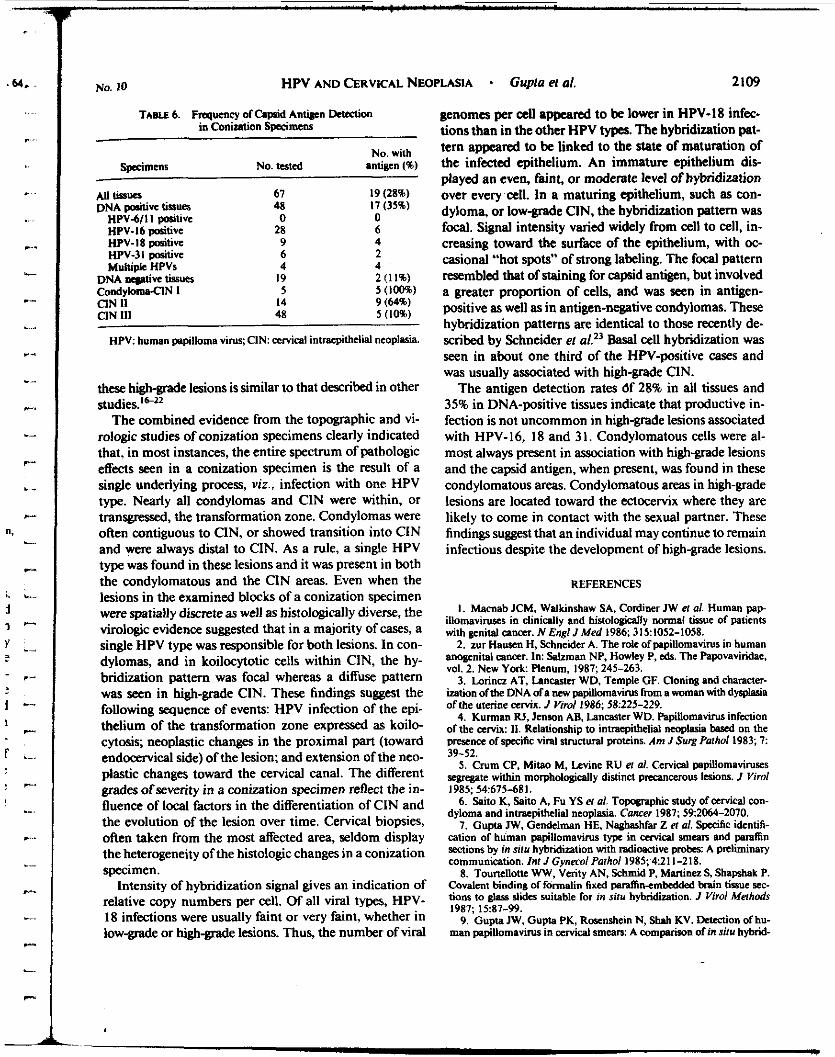
No. 10 HPV AND CERVICAL NEOPLASIA Gupia el al. 2109
TABU 6. Frequency ofClpiid Anlieen DMtion in Conintion Specimens -
No. with Spcimas No. tacd intipcn (%) -
All Iissuer 67 19 (28%) DNA @¶¡Ve t¡SSUa 48 17 (33%)
HPV-611 I positive O O
HPV-I8 positive 9 4 HPV-31 positive 6 2 Muhipk HPVs 4 4
HPV-I6 @tive 28 6
DNA ur@it¡W IissUts 19 2 ( I 1%) CondylomsClN I 5 3 ( l o w CIN I1 14 9 (64%) CIN 111 48 5 (10%
HPV: humn papillama virus; CIN: cervical intraepitheli neoplasia.
these high-grade lesions is similar to that described in other studies.’”’2
The combined evidence from the topographic and vi- rologic studies of conization specimens clearly indicated that, in most instances, the entire spectrum of pathologic effects seen in a conization specimen is the result of a single underlying process, vi,?., infection with one HPV type. Nearly all condylomas and CIN were within, or transgressed, the transformation zone. Condylomas were often contiguous to CIN, or showed transition into C IN and were always distal to CIN. A s a rule, a single HPV type was found in these lesions and it was present in both the condylomatous and the CIN areas. Even when the lesions in the examined blocks of a conization specimen were spatially discrete as well as histologically diverse, the virologic evidence suggested that in a majority of cases, a single HPV type was responsible for both lesions. In con- dylomas, and in koilocytotic cells within CIN, ihe hy- bridization pattern was focal whereas a diffuse pattern was seen in high-grade CIN. These findings suggest the following sequence of events: HPV infection of the epi- thelium of the transformation zone expressed as koilo- cytosis; neoplastic changes in the proximal part (toward endocervical side) of the lesion; and extension of the neo- plastic changes toward the cervical canal. The different grades of severity in a conization specimen refleci the in- hence of local factors in the differentiation of CIN and the evolution of the lesion over time. Cervical biopsies, often taken from the most affected area, seldom display the heterogeneity of the histologic changes in a conization specimen.
Intensity of hybridization signal gives an indication of relative copy numbers per cell. Of all viral types, HPV- 18 infections were usually faint or very faint, whether in low-grade or high-grade lesions. Thus, the number of viral
genomes per aU appeared to be lower in HPV-18 infec- tions than in the other HPV types. The hybridization pat- tern appeared to be linked to the state of maturation of the infected epithelium. An immature epithelium dic played an even, faint, or moderate level of hybridization over every cell. in a maturing epithelium, such as Con- dyloma, or low-grade CIN, the hybridization pattern was focal. Signal intensity varied widely from cell to cell, in- creasing toward the surface of the epithelium, with oc- casional “hot spots” of strong labeling. The focal pattern resembled that of staining for capsid antigen, but involved a greater proportion of cells, and was seen in antigen- positive as well as in antigen-negative condylomas. These hybridization patterns are identical to those recently de- scribed by Schneider el al.” Basal cell hybridization was seen in about one third of the HPV-positive cases and was usually associated with high-grade CIN.
The antigen detection rates óf 28% in all tissues and 35% in DNA-positive tissues indicate that productive in- fection is not uncommon in high-grade lesions associated with HPV-16, 18 and 31. Condylomatous cells were al- most always present in association with high-grade lesions and the capsid antigen, when present, was found in these condylomatous areas. Condylomatous areas in high-grade lesions are located toward the ectocervix where they are likely to come in contact with the sexual partner. These findings suggest that an individual may continue io remain infectious despite the development of high-grade lesions.
REFERENCES
I . Macnab JCM, Waikinshaw SA, Cordiner JW el al. Human pap illomavims in clinically and histologically normal tipsue of patienu with pcnital cancer. N Engl JMed 1986: 3151052-1058.
2. zur Hausm H, Schneider A. The role ofpapillomavirus in human anogcnital canar. In: %&man NP, Hmley P, eds. The Papovaviridae, vol. 2. New Yo*. Plenum, 1987,245-263.
3. Lorinn AT, Lancaster WD, Temple GF. Cloning and character- ¡ration ofthe DNA ofa llcw papillomawuS from a woman with dysplasia ofthe uterine a m x . J Vim1 1986: 58~225-229.
4. Kurman RJ, Jason AB, Lancaster WD. Papillomavirus infection ofthe aMx: 11. Relationship io intraepithelial neoplasia bavd on the p m n a ofspccihc viral structural proteins. Am J Surg Pniholl983,7 39-52.
5. Crum CP, Mitao M, Levine RU el ai. Cervical papillomaviruses segregate within morphologically distinct PRcancemus lesions. J Viro¡ 1985: 54675681.
6. Sito K, Saito A, Fu YS et ai. Topographic study ofarvical con- dyloma and intraepithclial neoplasia. Cancer 1987: 592064-2070.
7. Gupta JW, Gendelman HE, Naghashfar Z el al. Spaific identifi- cation of human pspillomavirus type in cmical smears and mlñn sations by in silu hybridization with radioactive probes: A Preliminary communication. In1 J Gpmoi Pathol1985; 421 1-218.
8. Tourtellonc WW, Verity AN, Schmid P, Manine2 S, Shapshak P. Covalent binding of formalin fixed wraffin~mbedded bnin tissue scc- tioni to glass slider suitable for in situ hybridization. J Virol Mefhods 1987; 1987-99.
9. Gupta JW, Gupta PK, Roscnshein N, Shah KV. Dnstion ofhu- man papillomavirus in -cal smears: A wmparison of in sifu hybrid-

I ) .
.. .
I .. .. .
r.
.- L
C.
L..
I
.- c
._ w..
I
r .. ....
c . L.
r.
....
....
C.
*"
L_
I,-.
r-
L
c.-
....
._..
.__ c
.... *.
21 10 CANCER November 15 1989 Vol. 64 -
ization, immunocytochemistry andcytopathology. Acta Cyid 1987: 31: 387-396.
IO. Reagan JW, Patten F Jr. DysplaJia: A basic rraction to injury in the uterine cervix. Ann NYAcadSci 1962: 96662682.
I I . Johnson LD. The histopathologic approach 10 early m i c a l ne& plasia. Obsiel C ~ d SUN 1969: 24135-761.
12. Wielenga G, Old JW, von Haam E. Squamous carcinoma in situ of the uterine cervix: 11. Topography and clinical comlations. Cancer 196% 18:1612-11621.
13. Stoler MH. Broker TR. In riru hybridization detection of human papillomavim DNAs and messenger RNAs in genital condylomas and a cervical cancer. Hum Pachol 1986; 17:1250-1258.
14. Crum CP, Nagai N, Levine RU, Silverstein S. In situ hybridization analysis of HPV-I6 DNA sequences in early cervical neoplasia. Am .I Paihd 1986; 123174-182.
15. k k m a n e AM, Myemon D. Daling J, Kiviat NM. Fenoglio CM, McDnugall JK. Detation and localization of human papillomaviru DNA in human genital condylomas by in silu hybridization With bio- tinylated probes. JMed Virol 1985; 16265-273.
16. Fuchs PG. Girardi F, pñstcr H. Human papiilomavinu DNA in normal, mnaplartic, pnneoplastic and neoplastic epithelia ofthe ceMn uteri. Inr JCacer 1988: 41:4,l45.
17. Reid R, G m n b M, JenJon AB el d. Sexually transmitted pap-
illomavid infections: I. The anatomic diatnbution and patholoQc @ of neoplanic lesions nmisted with diaerent viral typcs. Am J Obsta Gplecol 1987: 156212-222.
18. Millan DWM, Davis JA, TorM TE, Campo MS. DNA sequenas of human papillomaviw t p I I, 16, and 18 in IeJiono of the uterine cervix in the wesf of Scotland. Br Med J 1986: 29393-96.
19. Wilnyruki SP, &rssn S. Walker J, Liao SY, Pcailman LF. Hu- man papillomaviwcs and cervical canm Anal* of hinopathologic fcatum ayoOated with d i b n t viral types Hum Paibol 1988: 19697- 704.
20. Lonna AT, Temple GF, Kumian RI, J a s o n AB, LancaNr WD. Oncogenic &tion of e ü c human papillomavim t p with cer- vical neopluia. J Nail Cancer Ins1 1987; 79671477.
21. Gupta I, Pilotti S, Rilkc F, Shah K. A d t i o n of human pap. illomavim typc 16 with neopla5tic laions oíthc vulva and other genital rites by in silu hybridmtion. Am JPalhol1987: 127:206-215.
22. Caussy D, Orr W, Daya AD. Roth P, Reeves W, Itawls W. Eval- uation of methods for detation human papilbmavinis deoxyribonu- cleotide sequences in clinical specimens. JClin Microbid 1988: 26236- 243.
23. Schneider A, OltersdorfT, Schneider V, GisJmann L. Distribution pattern of human papillomannu 16 genome in cervical neoplasia by molecular in silu hybridization oftiJsue d o n . Ini J Cancer 1987; 39 717-721.

Adenocarcinoma del Cérvix Asociado al Uso de Anticonceptivos Orales. Presentación de i caso. Dr. Alfonso Torres-Lobatón' Dra. M c d a Hernández Gonzücz" Dra. Guadaiupe Rojo-Herren' * * Dr. Avissai Alcántara-Vázquez" Dr. G c d o Mota-Cieafucgos' * * *
I Resumen I ~ ~ ~~
Se presenta el caso de una paciente de 30 años de edad con diagnóstico de adenocarcinoma invasor del cénrix en estadio Ib, el cual fue manejado con histerectomía total más Iinfadenectomía pélvica. Se menciona que la pacienre tenía el antecedente de emplear de los 17 a los 20 años contraceptivos orales y que conraba con los siguientes factcfes de riesgo para el desarrdlo de ccincer cérvico-uterino: proceder de medio socioscondmiw bajo. inicio a los 15 años de la acfividad sexual. embarazo antes de los 20 arios. multiparidad, y no contar con estudio previo de papanicolaou. Se llevan a cabo consideraciones acerca del efecto inductor o promotor de los contraceptivos orales, en la etiología del adenocarcinoma cervical que se estd observando en mujeres @venes, los cuales podrían actuar en forma aislada o en combinacidn con otros factores. Se trara de documentar esta relacidn. con observaciones que presentan a los contra ceprivos orales asociados a la hiperplasia de las células de reserva del endocérvix, misma que se ha visto evolucionar a displasia glandular, a adenocarcinoma in situ y a adenocarcinoma invasor. Se senala que la paciente en estudio mostrd un tumor de menos de 4 cms. de diámetro y ausencia de meidstasis gan- glionares, factores considerados como de buen prondstico; cabe esperar en ella su curacidn.
r Summarv 1 A 30 years da female with a history of oral contraceptwe use presented an invasive aaenmarcinoa of me C ~ N I X , srage Ib. tne treatment was total nysierecromy win pslvic node resecrion She had oral contraceptives from 17 to 2ü years of age sne was also noted to have cenam risk lacrors for cervical cancer such as she came from a low socio~wnomic envi ronmer. sraned sexual activity at 15 years sne was also mulrparous and firsr became pregnanr before 20 years of age She had no previous cpofogy sruay There is some evidence thaf oral conrracepfives may play some role in the etiotogy of cervical adenocarcinoma in young women, eitner aione or with omer facrors The evtdence for mts IS rhat me reserve cell hyperplasia of me endocerv*. asK)cIa- tea wnrh ora! conrraceptrve use nas been observed to develop into glandular dysplasia adenocarcinoma in situ as well as invasive carcmoma The prognosis for rne parnent is good because of mall size 01 the tumor and the abscense of lymph node metastases
rPalabns ciave I Adenocarcinoma, cérvix. anticoncepiivos
El adenocarcinoma del cérvix ocupa el segundo lugar entre los cánceres de esta estructura anat6mi- ca con una frecuencia global de un 60/0,'.~ misma
rt
* Jefe del Servicio de Gineoologia. Unidad de Oncologia. * * Servicio de Patologia.
* * * Servicio de Gineco-obstetricia. MBdico Residente Unidad de Oncdogia. ...*
Hospital General de MBxico. S.S. Dirección: Or. Balmis 148 MBxico. D.. C.P. 06820
que según estudios epidemiol6gicos recientes, tien- de a incrementarse en algunas regiones de los Esta- dos Unidos de Norieamérica, donde su frecuencia ac- tual, fundamentalmente a expensas de mujeres de menos de 35 años de edad, ha alcanzado cifras has- ta de un 18%.3,4
Si bien es cierto algunos de los factores involucra- dos en su posible etiología concuerdan con los del carcinoma epidermoide del &rvix, como el inicio tem- prano de la actividad genital. la promiscuidad sexual
43

y las infecciones cervicales por algunos tipos de vi- rus,5 y otros factores con un cierto predominio en clases sociales altas, en pacientes nulíparac, en obe- sas y diaMticas. recuerdan a los factores de riesgo asociados al cáncer endometrial en cuya etiología se ha demostrado una clara influencia horm0nal.2~~~~
A partir de 1986, se han reportado casos clínicos en forma aislada o en pequeñas series de pacientes jóvenes con adenocarcinoma del cérvix, quienes ha- bían tomado contraceptivos antes de los 20 años de edad por 1 o más años, lo cual está relacionado el incremento anotado en la frecuencia del adenocarci- noma cervical, con el empleo 10 años antes de con- traceptivos orales.4J
En esta publicaci6n se muestra un caso de ade- nocarcinoma del cérvix en una paciente de 30 aiios de edad, quien tenia el antecedente de empleo de anticonceptivos orales y quien fue atendida en la Uni- dad de Ginecologia del Servicio de Oncologia del Hospital General de México, S.S. Se analizan los as- pectos etiopatogénicos. anatomoclinicos y terapéuti- cos correspondientes y se llevan a cabo considera- ciones al respecto.
Preaente~lón del caso
L.M.R. de 30 años con exp. 89/1112. residente en el Edo. de MBxico y procedente de medio socimo- nómico bap. Antecedentes de menarca a los 13 años, ritmo de 30x3, eumenorreica hasta hace 2 años en que inició con hipermenorrea y dismenorrea. Vida c8- xual activa a los 15 años con un compai7ero sexual. GestasVIII, parasVI, aborto I, cesáreas I. Primer par- to a los 17 años, &ea por presentacan peivica con salpingoclasia a los 26 años. Utiliz6 de los 17 a los 20 años contraceptivos orales. Nunca se le había efec- tuado papanicolaou.
Un mes antes de su ingreso a la Unidad, present6 metrorragia abundante en una ocasi6n. lo que moti- vó consulta en medio hospitalario de su localidad. de donde 89 canalizada al Servicio con diagnóstico de adenocarcinoma del cérvix.
La expioraci6n física mostr6 al paciente en buen estado nutricional, con una cicatriz media infraumbi- lical; la exploración ginecd6gica arrojó como datos positivos la presencia de una lesi6n neoplásica exofi- tica de 3.5 x 3.5 cm limitada al cuello uterino. 4.4
Con un diagn6stico de adenocarcinoma de cérvix en estadio clínico Ib, radiografía del tórax sin eviden- cia de meastasis y ex8menes preoperatorios dentro de la normalidad, se sometió a histerectomia con lin- fadenectomía peivica conservando ambos anexos. La evoluci6n postoperatorio fue satisfactoria y la pieza quirurgica 8-89-4000 report6 adenocarcinoma del cérvix moderadamente diferenciado, sin tumor eq bor- de vaginal ni metástasis ganglionares (Figura 1 y 2). La paciente asiste a sus controles sin evidencia de enfermedad.
FlüURA 1
I

Comontirio
En 1986, R.K. Peters y cds7 destacaron el incre- mento observado en la frecuencia del adenocarcino- ma del Cervix en mujeres jóvenes del Condado de los Angeles California. Este fue atribuido al uso de anti- wnceptivos orales, al demostrar en este tipo de pa- cientes la asociación de adenocarcinoma in situ e in- vasor del cérvix. M.P. Hopkins y cok del Centro MB- dico de la Universidad de Michigan? informaron en 1987 una frecuencia para esta lesión del 16.8%, ha- ciendo notar que el 45% de las pacientes que conta- ban con 45 años de edad o menos tenian el antece- dente de emplear anticonceptivos orales. Otras auto- res? han llegado a idbnticas conclusiones.
En cuanto al mecanismo a través del cual los con- traceptivos orales influyen en el desarrollo del cáncer endocervical, se han reportado evidencias de diver- sa indole que muestran una clara influencia hormo- nal ejercida por estos agentes en las células colum- nares del endocérvix y en las células subcdumnares o de reserva de esta estructura. Algunos autores’ su- gieren que en la adolescencia, el epitelio del cérvix en su zona de transformación de epiletio columnar a epitelio escamoso. es especialmente susceptible al efecto de los cancerigenos ambientales, por lo que el efecto inductor o promotor generado por estos agentes bien sea en forma aislada o en combinación con otras factores, podría llevarse a cabo precisamen- te en esta etapa de la vida de la mujer.
Por otra parte, desde el punto de vista experimen- tal se ha demostrado que los progestagenos admi- nistrados a dosis altas, desencadenan en ciertos ma- míferos el desarrollo de adenocarcinomas cervicales similares a los de los humanos.3
El empleo de contraceptivos orales se ha visto aso- ciado a hiperplasia microglandular del endcdrvix, pa- tologia que también se ha llegado a observar duran- te el embarazo y que no es considerada como pre maligna. Sin embargo, existen reportes que señalan su asociaci6n con la hiperplasia de las cBlulas de re- serva del cérvix la que puede evolucionar a displa- sia glandular, a adenocarcinoma in situ y adenocar- cinoma invasor.
La paciente presentada en este estudio tenia los siguientes factores de riesgo para cáncer cervico- uterino: el proceder de medio socioecon6mico bajo,
inicio a temprana edad de la actividad sexual, multi- paridad y el no contar con un estudio previo de pa- panicdaou. Todos los factores. sobre todo los men. cionados en segundo y tercer lugar, son considera- dos en la actualidad de alto riesgo para el desarrollo de esta enfe~nedad.~
El hecho de que la neopiasia se haya diagnostica- do a la edad de 30 años y no a los 45, como ocurre para esta etapa clinica en las pacientes que acuden al Servicio con cancer c8rvicuuterino invasor limita- do al cérvix,’ sugiere la participación de otro u otros elementos en su posible etiologia. por lo que el ante- cedente de haber utilizado durante’más de 3 años anticonceptivos orales, permite establecer una rela- ción causa-efecto, como se ha mencionado pre- viamente.
Para esta paciente, resulta atractivo el plantear la muencia de los siguientes eventos en la historia na- tural de su enfermedad: 1, inicio temprano de la acti- vidad genital; 2, embarazo en la segunda década de la vida; 3, empleo de contraceptivos orales durante 3 años por lo menos; 4, multiparidad; 5. periodo de lactacia de 10 años y 6, presencia de adenocarcino- ma cervical invasor.9
En cuanto al tratamiento instituido a esta enferma, la histerectomia con linfadenectomia p4ivica consti- tuye la terapéutica de elección para pacientes de 40 años o menos, en las que resulta fundamental con- servar el funcionamiento ovárico, ya que el otro prc- cedimiento. considerado también de elección y que es la radioterapia, termina prematuramente con la fun- ci6n ovárica. lo que trae como consecuencia un cli- materio a edad muy temprana.
La pieza quirijrgica reportó un adenocarcinoma del cérvix de 3.5 cms moderadamente diferenciado, sin tumor en bordes de sección y sin methtasis ganglio- nares, lo cual permite inferir una evoluci6n a largo pla- zo sin actividad tumoral.
Si bien es cierto que al adenocarcinoma cervical se le ha atribuido, en términos generales, un pronós- tico menos favorable que al carcinoma epidermoi-
el caso en particular presenta como factores de buen pronóstico, el contar con una lesión menor de 4 cms y el carecer de ganglios metasthsicos. M.P. Hopkins y cdc4 obtuvieron curaciones del orden de 88% en 34 pacientes, con reporte de ganglios nega- tivos para metástasis; por su parte J.S. Befek y colsl0
45
Admanminomi del ctrrk. T-Lobztón A,, Hcmindcz-Gonzílcz M.. Rojo-Hwen G.. Alrinnrr Vízqucr A,, Mora-Cicnhicgm G . -
alcanzaron, en lesiones de 4 cms, curaciones del or- den de 69%.
I. Torres LA. Cruz TF. Plata NP et ai Cancer &rviwuterino 1983.1984. Experiencia de la Unidad de Oncología. Hospitd General de M B x i c o , S.S. Cancercdcgia 1988; 3 4 617-622.
2. Brinton LA. Karen T. Tashima H el a i Epidemiology o1 Cervi- cal Camer by wll type. Cancer Res. 1987; 47: 1706-1 71 1.
3. Valente PT, Hanlani P. Endocervical Neoplasia in Longterm Users d oral Contraceptives: Clinical and Patholwic Observa.
, lions. Obstet and Gynscol. 1986; 67: 695.704. 4. Hopkins PM. Patrick S. Robert9 AJ: Prognostic features and
46
treatment of endocervical Adenmrcincma of the cervix. Gym cd Oncd. 1987; 27: 6475.
5. Menu- J. YaronSchfflw O. Liventon S, elal. HerpesvirusType 2 in Adenocarcinoma of the uterine cervix: A possible associa- tion. Canm. 1981: 48: 1497-1499.
6 Milson I. Gostafr berg L Primary adenocarcinoma o1 [ne Liter. ne C B N I ~ Cancer 1983. 52 942.947
7 Peters KR. Chao A. Macr MT. Bemstein L h noerson EB In. creased frequency of adenocarcinoma of the uterine carvix id young w a n e n in Los AngdesCounty. JNCl19BB; 76: 425428.
8. Chumas CJ. Beth N. Mann JW. et al. Microglandular Hyper- plasia of the uterine ceMx. Obsfet G y d . 1985; 66 406409.
9. Torres LA. Roman BE. MaRinez MR. Cruz TF. CAncer cervi- couterim. Evidencias a favor de una etiología multifactorial. GI. nec Obstet Méx. 1987; 55: 214.
10. Berek SJ, Castaldo WT. Hacker FN, et a i Adenocarcinoma of the uterine cervix. Cancer 1981: 48: 2734.2741
i

Second Primary Cancer After Treatment for Cervical Cancer
Late Effects After Radiotherapy
HANS H. STORM. MD
U s 4 data horn tk pprhlioii-bawd W s b Cancer Re&try. ik relative risk (RR) of second priaury -r M useued 24,970 w0-n wilh invasive cervlal mcer (1943-1982) d 19,4470 women rrHh eird.oii ir situ of lk cervix. Tk aulyris was s h t i f k d to treatment with (+) and *ilLout (-) ndhlba . For dl prhuks combid , I RR + = 1.1 (95% mfdcrc htcnil (a) = 1.06-1.18)diRR- = 13(95%CI = 1 . 1 3 - 1 . ~ ) ~ o b a c r v e d . f i r r i n v w i v c c e ~ l e i a e m u d i RR+ = 35 (95% Ci = 1.4-7.2) d RR- = 1.1 (95% Ci = 0.7-1.6) fdl0wi.o in situ cancer. T k amll oven11 excesa of second primuy is m u n t e d for by 80 incruse of some -rs such as Iwg. W d e r , d i eo~~yrrenl dnreue In others such as h i . Allhough mot stalisticslly dinefist from .oiiimdbld tk RR iarrased with lime since treatment among irndbied invisive emhl -1 ).lints in o r p i s cbse to and i t in~ermediite distance from lbe m i x , remchiag a maximum after 30 or more y a n of follow-up (RR = 1.9; 95% Ci = 1.4-2.5). Altogether. for tbcse eles i n cxms of 64 ases per 10,oOO women prr y a r wen imikitabie to ndhtion amhug survivors of 30- y a n . The bilkst risks immg lomg-term s d v m were observed for the foliowing: otber gaita1 organs (RR = 58; 95%
stonicb (RR = 2J; 95% CI = 1.1-4.7) d rectum (RR = 2.4; 95% Ci = 1.146). A s i p l R a i t deAcit of risk for breast cancer (RR = 0.7.956 Ci = 0.6-0s) M okcned for 10- y a n , my k imibutsbie to lbe dCa of o v U t a ibbtim by ndiotknpy. I1 is spenilted that the mme decl iIS0 my expLin lht observed dcfleita of kiio tumors (RR = 0.6; 95% Ci = 0.4-1 .O) d skim m~lioonis (RR = 0.6; 9% Cl = 03-10). It b cmclded Ibat cancers itidbutable lo rdbtiai. i p u t from m t e Iioiiympbocytic ieukrmts, l ed to ippeu lale (IO or more ye in after ndiotknpy), d that <be risk remiins denled for mom than 30 y a n .
Cancer 61xÍ79488,1988.
CI = I a-13.0) H e r (RR = 55;95% CI = 2a-95), ~ V C ~ ~ S S W (RR = 3.3 95% a = 0.4-12.0~
SUBSTANTIAL PART of our knowledge on the carci- A nogenicity to humans of ionizing radiation derives from populations irradiated for medical purposes.' The results of these studies are corroborated by those of atomic bomb s~rvivors?~ although there are some dis- crepancies. Whereas high to moderate levels of exposure
From the Danish Cancer Registry, Institute oiCanar Epidemiol- ogy, Danish cuK?cr Society. Copnha&%n.
SuppoRed by a lcsepIch grant h m the Danish Canar Society, which also suiupponr the Danish Cancm Rcgistiy.
The authon thank Mis. Hew Ni&n for thorough pmfmading, prepamtion oftabla and typing thc tat; MIS. Aase Lami for drawing the fisurrs; Mr. Ni& Chri>tnisni for wnducting the computer anaiy- e, and Un. Elizabeth Hsssltine for her skilled editing. The authors also thank DI. Ok M d a Jcnsen and Dr. John D. Lbice Ir. Radiation Epidemiology Branch, NCI, for valuable criticism during p-tion of the manuscript.
Addreda for reprints: Huis H. Síorm, UD, Danish Cancer Registry, Institute of Cnocer Epidcmidogy under thc auwh Cancer Society. L.ndil;ronasr.de 66,4th Boor DK-2100, Copenhasen, Denmark.
Ampted forpublimtion Aue.ust 31,1981
to ionizing radiation increase the risk of cancer,' con- troversy still exists about the carcinogenicity of expo- sures to low-level ionizing radiation.'
Leukemia is the most prominent radiation-associated cane+' although its induction appears to be a complex function of dose, involving inactivation of bone marrow cells at high Radiation-induced solid tumors are of greater numerical significance than leukemia' and, in contrast to leukemia, appear decades afier radiation ex- posure, with a temporal pattern of incidence (ie., age at diagnosis) that seems to follow the natural incidence.' The excm risk does not appear to decline with time, as it does for leukemias, bur few irradiated populations have been foliowed beyond 30 years.
The majority of cervical cancer patients in Denmark are treated with radiotherapy,''." and most as a benefit of treatment survive for a long time, as in other coun- tries.'* An international coUaborative study by Hutchi- soni3 on irradiated cervical patients, withan extended
679

680 CANCER February I S 1988 Vol. 61
TABLE I Numkr of Women by Age at Dtagnmis. Total 'lumber of Womcn (1943-1977). and Women-Yenrs a1 Risk for Second hmary Cancer Development í 1943-1982) A h irradiated or Not Irradiated Cervical Cancer or Canar In Situ of the Cenia in Denmark
Invasive In siru
Radiotherapy No radiotherapy Total Radiotherapy No radiotherapy Told
No. of women 20160 4810 24970 567 18903 19470 Women-yr at risk since diagnosis
<I yr 18292.0 4246.4 22538.4 554.6 18827.6 19382.2 1-9 97294.3 29927.6 127221.9 4206.5 139930.1 I44 136.6
10-19 58895.8 18303.8 77199.6 2051.1 3 1548. I 33599.2 20-29 23969.4 5425.7 29395.1 186.6 669.2 855.8 30+ 4646.6 485.4 5132.0 5.6 7.1 12.7 All 203097.9 58388.7 26 1486.6 7004.2 190982.0 197986.2
No. of women by agc at diagnosis <35 yr 1953 35-44 5151
723 IS69
2676 66 6720 183
45-54 5849 1281 7130 I64 55-64 4170 672 4842 75 65+ 2232 744 7574 61
664 739 188 249
follow-up,l' showed no increased risk of leukemia, in contrast to a larger and more recent study." Excess risks also have been observed for solid tumors in organs close to and at intermediate distance from the cervix.ls How- ever, information on long-term survivors (20 or more years) has so far been limited in large part to results from the Connecticut Tumor Registry.16
The current study reports the results of an extension of follow-up through 1982 of cervical cancer patients diagnosed in Denmark between 1943 and 1977; the previous follow-up was through 1976.'" Emphasis is placed on the risk of second primary solid cancers among long-term survivors, since the present report is based on more woman-years accrued among 30+ years survivors than any previous publication o f cervical cancer patients.
Materiala Ud Methods
Danish Cancer Registry
The study is b a d on incidence data collected rou- tinely by the national Danish Cancer Registry between 1943 and 1982. The Registry receives notification from hospital departments, pathology institutes, and practic- ing physicians. Reports on carcinoma in siru and severe dysplasia of the CCMX have been requested since 1968.'' Unreported cases are identified by means of annual linkages with the ~tional death register." The Cancer Reeistry is tumor-baJcd, with each tumor linked to the unique personal identification number provided to all Danish inhabitants. AU tumors M coded and clpsyfied in accordance with a modified version of the seventh revision of the Intmnationai Classification which allow a distinction baween sarcomas and carci- nomas
Multiple primary cancers in the same person are de- fined as tumors that arise in different organs, and these are notified as new primary cancers or as separate tumors with different morphologic characteristics." The registry is known to be complete regarding invasive tumors,2°*'1 although there is some underreporting of multiple primaries, estimated to be approximately 16% depending on site of first cancer?'
Study Population
All women with either invasive carcinoma (24,970) or carcinoma in situ of the cervix uteri (19.470) diagnosed between 1943 and 1977 were included if the woman survived at least I month from the day of diagnosis (Table 1). Altogether, 460,000 person-years were ac- crued. A total o f 2313 second primary cancers (ex- pected, 2045) were identified 1 or more years &r the initial cancer diagnosis by means of record linkage within the registry and were distributed according to site, notified treatment, and time since cervical cana%. Nonmelanoma skin cancers were not considered in this study. Most cervical cancers (98%) but fewer of the sec- ond primaries (88%) were histologically verified.
The study population was subdivided into four CD-
horts: invasive or in situ c e r v i d cancer and, within each of the two, with or without radiation, the latter including cases without information on radiotherapy. classiñca- tion of invasive and in situ cervical cancers by the Cancer Registry was shown in an d i e r study to be ~0rrect.l~ A comparison of regism information and hos- pital record information showed that 98% of 2156 cer- v i d cancer patients notified and coded as irradiated had in fact undergone radiotherapy, whmps 24% of 423 cases classified by the Registry as not irradiated had in
Nc
fa< mt
h> ar b! hi
di h
W
W
1.
fi ti b t F
5
i ( I

- *
I.
i Bf i a *-
c
- .._
.._ - >
j
Y ,
.<I j
._
F' , u '
SECOND PRIMARY CANCER AFTER TREATMENT Storm 68 I No. 4
fact received radiotherapy as part of the primary treat- ment (Table 2).
The Same data were used to estimate the frequency of hystcnctomies and oophorectomies among irradiated and noninrrdiated cervical cancer patients as classified by the Cancer Registry. Among irradiated patients 9 1% had an intact uterus and 89% intact ovaries, compared with 4% and 21%. mpectively, among those nonirra- diated, among the nonirradiated women, a further 18% had one ovary left. Altogether, 39% of the nonirradiated women thus probably had intact ovarian function.
A random Sample of 4 1 patients classified by the Reg- istry on the basis of a histologic diagnosis as irradiated for in siru cervical cancer were selected for recoding of the notified information. One patient (2%) was found to have had invasive cervical cancer. The majority, 3 I pa- tients (76%), were irradiated for an in s i fu lesion, whereas nine (22%) were not. However, 19 (48%) of in situ patients were classified according to the Interna- tional Federation of Gynecology and Obstetrics (FlGO)I2 as Stage I (a or b) or even Stage 11 by the reporting clinician, who thus disagreed with the patho- logic classification.
Follow-Up and Analysis
Follow-up information on vital status is available from the Cancer Registry records." Woman-years at risk were calculated from the date of diagnosis of the cervical cancer until the date of diagnosis of the second primary cancer, death, or December 31, 1982, which- ever occurred first. Expected numbers of second pri- mary cancers were obtained by multiplying age, sex and calendar time-specific incidence rates by appropriate women-years, using a modified version of the program developed by Monson?' Relative risks (RR) were mea- sured as the ratio of observed to expeaed numbers of incident cancers. Tests of significance and confidence interval (CI) of the RR were calculated assuming a Pois- son distribution?' Tests for trend over time from 10 to 30+ years were canied out utilizing programs for a pro- grammable calc~lator,~' using midpoints of follow-up intervals and 35 years for the 30+ year category. The absolute risk attributable to radiation was calculated as the difference between the observed and expected num- bers divided by the woman-years at risk.
Results
Table 3 shows the overall pattern of risk one and more years after cervical cancer or carcinoma in situ accord- ing to initial treatment with or without radiation. Among irradiated (+) and nonirradiated (-) women with invasive cervical cancer, significantly increased
TABLE 2. Vdidity of Clusifiation (%) According to Radiotherapy in thc Din¡& cinar Rsutry
Ciruification according io hosmul rem&
No CLirUfication in Ridiothcrnpy ndiothcrapy Total no. of
cancer @svy record (5) ptimía (5)
Irradiated 97.1 2.3 2156 (100) No1 irradiated 23.9 76.1 423 (100)
risks are observed for cancer of the lung (RR+ = 2.6; RR- = 2.4). other genital organs (vulva and vagina pre- dominantly; RR+ = 1.9; RR- = 3.2), bladder (RR+ = 2.9; RR- = 2.5) and connective tissue (RR+ = 1.5; RR- = 2.3). Kidney cancer rates are increased among nonirradiated patients (RR- = 2.6). Imspective of treatment, nonsignificantly (NS) increased risks are ob- served for second primary cancer of the esophagus, small intestine, rectum, and bone. Significantly de- creased risks are seen for cancer of the uterine corpus (RR+ = 0.6; RR- = 0.1) and ovary (RR+ = 0.5; RR- = 0.5). The risk of breast cancer is significantly de- creased among irradiated cervical cancer patients (RR+ = 0.7); similarly significantly decreased risks are Seen for melanoma (RR+ = 0.6) and brain tumors (RR+ = 0.6) after irradiated invasive cancer.
Among women with in situ cervical cancer, increased risks are seen for cancer of the lung (RR+ = 2.2 [NS]; RR- = 2.1), other genital organs (RR+ = 14.3; RR- = 7.1) and bladder (RR+ = 4.7; RR- = 1.3 [NS]). The only overall excess of cancers of the lymphatic and hae- matopoietic tissus (due to acute leukemias) is observed after irradiated in siru cervical cancer (RR+ = 3.5). Sig- nificant deficits of breast (RR- = 0.8). corpus uterine (RR- = 0.2), and ovarian cancer (RR- = 0.7) are seen after nonirradiated carcinoma in situ.
Table 4 shows the trend in RR for cancers at selected sites among long-term survivors irradiated (+) and not irradiated (-) for invasive cervical cancer. The RR for stomach cancer increases significantly with time since irradiation of the cervical cancer (x2 trend = 9.1; P = 0.001). The RR for colon cancer is 10% to 40% higher among nonirradiated than among irradiated women throughout the follow-up period, although none of the RR is significantly different from unity. The RR for rectal cancer is similar in irradiated and nonirradiated patients, with a significant increase in risk with time for irradiated women only (xz trend = 16.9; P = 0.0002). An increasing RR (x2 trend = 11.2; P = 0.004) for pan- creatic cancer is Seen among irradiated cervical cancer patients, however not present if including follow-up years 1 to 9. The overall increase in risk fG this cancer

I- . ~
. .. . -. . - 1
682 CANCER February 15 1988 Vol. 61
T A B U 3. ObSe~ed and O ~ W N C ~ to Expected Ratio of Second Primary Cpnocr 1944-1982 at Lmst I Year ARer CeMcal Cancer and Carcinoma In Situ of the Cervix 1943-1977. According io Notified Treatment With and Without Radiation
Invasive cervical canwr Carcinoma in situ cervix utcnt
No rddiotherapy* Radiotherapy No radiothera~ - Radiotherapy Second primary cancer
(ICD.7 code no.) ObSeNed OIE observed O/E observed OIE Obamed OIE
Buccal cavity and pharynx
E-phapua ( I 50) I5 I .6 3 Stomach I Is I ) 75 I .o 16
Colon (133) 131 I .o 29 1.1 4 1 . 1 30 0.8 Small inicstine (152)
Rmum(i54) 85 1.2 17 I .2 I 0.5 I4 0.7 Liver and pllbladdcr( I 55) 30 0.9 5 0.7 2 2.1 9 I .o Pancreas (I 57) 48 1 . 1 I2 I .4 4 3.3 16 I .4 Lun6 ( I 61) I70 2.66 42 2.4# 5 2.2 77 2.16 Brcpst ( I To) 207 0.76 69 0.9 10 I .o I55 0.81
54 0.66 3 0.16 2 0.7 8 0.21
1.1 5 1.3 O - 10 1.5 - I 0.5 - 13 I .o - O
(140-146) 18 I .8 O 1.3 O
6 I .7 I 1.3 O -
ovary ( 175) 47 0.56 10 0.57 3 1.1 28 0.7W Uterine wpus (172)*
29 I .9( IO 3.21 6 14.36 37 7.16 Kidney I 180) 35 I .o 21 2.66 I I .o 9 0.7 Other genital (176)
2.56 5 4.71 I6 1.3 - 23 I .o
Bladder [ I 8 I) 104 2.96 20
- 13 0.6 Melanomi (IW) I 3 0.61 R Brain(IO3) 20 0.61 10 I .2 O Thymid t 194) 8 0.9 I 0.5 I 4.2 I 0.2
2.1 I 2.3 O - I I .4 - 5 0.6
bne( I%a) 5 Connective tisue (197B 26 IS! 9 2.31 O
1.1 O
Lymphatic and hematopoietic tisues (200-204) 59 0.9 I n 1.2 7 3.5n 29 1 . 1
All sites ( 140-204 except 191 othcrskinand 171 cervi.i\ 1338 1.16 349 1.36 58 1.611 568 1.1
O/E ~*dcrved io expected ratio. Inilihks radiotherapy unknown.
t Includes severe dyrplaua of the cervix. t Includes uterus unspceificd.
disappears 20 or more years after a nonirradiated pri- mary. The risk for lung cancer increases consistently (RR = 1 . 3 4 3 ) imspective of primary treatment. in mntmt, breast cancer risk remains consistently
below expectation (RR = 0.5-0.9). but significantly so only if the cervical cancer was irradiated. After a nonir- radiated cancer of the cervix, deficits of second primary Corpus uterine cancer (RR 0.3) and of ovarian cancer (RR 0.6) are observed. The overall deficits of corpus uterine and ovarian cancers disappear 20 or more years after an irradiated primary, and a significantly increas- ing tRnd in risk by time is seen for both sites (X' trend corpus - 9.9: P = 0.001; x' trend ovary = 7.2: P = 0 . 0 0 . The risk of other genital cancers (predomi- nan@ cancera of the vulva and the vagina) is signifi- can* incnased, especially among long-term survivors who irnived radiotherapy, and the RR increases signifi- can@ with time (x' trend = 10.9; P = 0.ooOS). The hcrraned RR of bladder cancer after either an irradiated or a amirradiated primary W significantly different from unity only if the cervix received radiation. The risk
5 Includes own siic-spific sarcomas II P< 0.0s. TP<O.OI. 6 P < 0.001.
among these patients also increases significantly with time since irradiation (x2 trend = 26.0; P < O.oooO1).
When one combines all second primary cancers close to (bladder, rectum, ovaries, vulva-vagina, pelvic bones, connective tissue of the pelvis) and at intermediate dis- tance from (kidney, ureter, colon, small intestine, stom- ach, pancreas, liver, peritoneum, retrope&oneum) the cervix of irradiated women (Fig. 1), the RR increases substantially and significantly with time (x' trend = 225.6; P < O.oOo1). The excess number of tumors at these sites amounts to 64/10000 women-years and 17/10,OOO women-years among irradiated and nonina- diated women, respectively, 30 or more years after ini- tial treatment. The relative risks over time are not sta- tistically different from those of the nonirradiiated pa- tients (x2 = 9.6; 8 df, P = 0.30). The RR increases significantly with time for nonirradiated patients also (x' trend 25.1; P < 0.0001). However, the RR- start from a higher level at the outset (RR = I .O) for nonirra- diated than for irradiated and ends at a lower level (30+ years: RR- = 1.3; RR+ = 1.9) (Fig. I).
No. 4
secar (1'
Stom
Col0
Red
Pam
i u n
BRí
Cor
ov; Ott
Bla
M<
BE
C<
-
-
di
a E
C I
<

NO. 4 SECOND PRIMARY CANCER A m n TREATMENT * Sform 683
TABLE 4. o b s e d and Eapsied Second Rimary Canan of Sc*aed Sita. Lon&Tcmi SuMvh8 Irndkld and Not Irradiated* Cervical Qnar htients
Yr U n a aMcal cancer
10-19 20-29 M+ Second primary cancer
(IcD7 d e no.) O Et OlEt O E OIE O E OIE
Stomach ( IS I )
Colon (153)
Rmum (154)
P n n m ( I S7)
Lung (162)
BrraJt(170)
Corpus uteri (172)
Ovary(175)
Other genital (176)
Bladder ( I8 I )
Melanoma ( 190)
Brain (193)
Connmive tirsue (197)
2.5. 2.8 0.7 1.2 2.4# 2.7 2.0 0.0 I .9 5.3 0.7 0.8 2. I 0.0 I .o 0.0 5.88 0.0 5.511 4.6 0.0 0.0 0.0 0.0
1 N I N I N I N I N I N I N I N I N I N I N 1
28 9 42 14 29 7
13 6 43 16 78 27 23 13 2
5 IO 6
34 7 5 3 5
25.2 4.5
44.5 10.3 24.8 S.8 15.2 3.6
24. I 7.5
104.2 31.1 32.0 9.3
30.2 8.6 5.1 I .2
12.8 3.3 8.0 2.8
11.1
1.1 2.0 0.9 I .4 I .2 1.2 0.9 I .7
2.15 0.75 0.9 0.7 0.2$ 0.411 0.6 2.0 4.99 2.711 2. I 0.6 1.1 0.5
1.81
14 O 29 6 25 4 9 2
20 6 28 7
16 I 14 2 8 I
32 2 2 I 4
14.0 I .O 2. I 0.0 28.9 I .o
5.3 1.1 14.5 1.7t 2.7 1.5 10.3 0.9 I .9 1.1 14.9 I .3 3.4 I .8 S2.4 0.51 11.2 0.6 15.9 I .o 3.7 0.3 14.7 1 .o 3. I 0.6 3.0 2.6t 0.6 1.7 8.3 3.911 1.6 1.3 4.0 0.5 I .o I .o 5.3 0.8
9 I 6 I 9 I 6 O 7 2 8 I 7 O 3 O 5 O
I2 I O O O
3.6 0.4 8.3 0.8 3.7 0.4 2.9 0.3 3.7 0.4 11.9 I .2 3.3 0.3 3.1 0.3 0.9 o. I 2.2 0.2 0.9 o. I 1.1
~~
N 6 3.3 I .8 O I .2 0.0 O o. I I 8 5.5 I .4 7 2.1 2.6t 2 0.6 3.3 N 4 I .5 2.1 2 0.5 3.1 O o. I 0.0
0 ObXNed, E CXpCCtCd; O/E ObXrVCd IO CX-d d o ; 1: im- dialed: N no1 irradiated.
Includes irradiated unknown. t F@um are based on two decimal point calculations.
Soft tissue sarcomas occur in excess in both irradiated and nonirradiated women (Table 3), and the RR in- creases with time since diagnosis among those who re- ceived radiation (x2 trend = 3.5; P = 0.03) (Table 4). Almost 90% of the sarcomas are located at sites close to or at intermediate distance from the cervix (Table 5), which is not significantly different (x2 = 2.66) from the distribution among women in the Danish Cancer Regis- try material as a whole (70%).
Table 6 presents the data on women treated for carci- noma in siiu and followed for more than 10 years. The findings are similar to those in patients with invasive cervical cancer: elevated RR are seen for lung cancer (RR+ = 1 .E [NS]; RR = 2.3). other genital cancer (RR+ = 11.8; RR- = 4.9) and bladder cancer (RR+ = 4.7; RR- = 1.4 [NS]). The RR for second primary breast cancer among nonirradiated carcinoma in situ patients is as expected (RR = 1 .O), whereas a decreased risk (RR = 0.5 [NS]) is observed after irradiation.
When one combines all irradiated patients, with both invasive and in situ cervical cancer, 15 acute nonlym-
t P < 0.05 5 P < 0.01. IP<O.oOl
phocyiic leukemias (ANLL) are observed, with 7.3 ex- pected (RR = 2.1; 95% C1 = 1.2-3.4); five ANLL oc- curred among nonirradiated patients during the first 19 years of follow-up, with 6.7 expected (RR = 0.81; 95% CI = 0.2-1.7). The leukemia risk by time among irra- diated women is shown in Figure 2. A significantly in- creased RR of 3.5 (95% CI = 1.3-7.6) for ANLL is observed 1 to 4 years after primary treatment; the RR then decreases and no case is observed beyond 15 to 19 years. The RR for chronic lymphocytic leukemia (CLL) remains constant at the expected level for the entire follow-up period (20+ years; RR = 0.9).
Discussion Studies of multiple primary cancers may point to
common exogenous and endogenous risk factors for the first and the second primary cancer, to genetic suscepti- bility or to an etiologic role of treatment for the first ~ancer.~~J~-*' Ce rvical ' cancer patients are probably those mOSt extensively studied over the years with re- spect to second cancer de~eloprnent."~~~-'~*-~' A Par-

684 . CANCER February IS 1988 Vol. 61
TABLE 5. Morphologic Findin@ of Second Primary Sarcoma 10 or More Yeam Aftcr Irradiated Invasive Cancer o f t k Cervix, According to Distance From the Cervix and Treatment With or Without Radiation, Compared With Incident Soft Tisnue
Sarcomas Amom Women in Denmark 1978-1982
Irradiated Denmark 1978-1982
Site relative to cervix’ Site relative to ceMx
Morphologic features Close Intermediate Distant Clm Intermediate Distant
Sarcoma NOS 1 I - 64 13 32 Leiomyosarcoma 5 2 I 103 33 I2 Carcinosarcoma I - - 32 3 4 Fibmsareoma, fibrous histiocytoma
(malignant) 2 - - 64 5 29 47 I I2 Myxolanama. lipovumma - - -
An&sarmma I I - 13 7 8 Other specified sarcomas I - I 49 3 91 All sarcomas
No. Percent
I I 65
4 24
2 372 I2 60
65 IO
188 30
‘ C l o x female genital organs, unnaty bladder, mtum, pento- ncum-mmpntomum and connective tisue of plvis, intcrmediaie.
ticular feature is the risk related to therapy among women followed for more than 20 to 30 years, since only limited information from uniform registration schemes has previously been available for such long-term SUM-
VOTS. ’~ This study examines irradiation as a dichoto-
NO. OF CANCER CASES (+) 216 r2a l(H U (-) 52 u 23 4
m 4
s
2
I ! L 1 -e lo-I* ?a-= ao+ TIME SDWX flRn TRE*lUENi (YEARS)
I , I
FlO. I . AtVibuPMe I¡& (AR) pr 10,OOO woman-yM (WY) and rclativc nak (RR) with 93% mnhdena intervals for developing a sec. onday prinuty unta 8t any Yle close to or at immdule diamnce from the d a by time Once hirt tmtment among women irradiated (+) or not imdiaud (4 tor d c d einar.
kidney, u e r , descending colon, small intestine, stomach, pa- and liver, distant: all other sites.
mous variable as reported to the Registry; no account could be taken of other known risk factors for cancer, operating among cervical cancer patients.”
Overall, no major difference between irradiated (RR = 1. I ) and nonirradiated (RR = 1.3) invasive cervical cancer patients is observed although a somewhat steeper increase in risk over time is observed for irradiated pa- tients. However, one fourth of the “nonirradiated” group probably received radiotherapy, limiting the va- lidity of using this group for comparison. Furthermore, due to the smaller number of long-term survivors among nonirradiated, confidence limits of the RR are wider than among irradiated, thus rendering compari- sons difficult. A valid comparison group could be non- irradiated carcinoma in situ patients, who also show no difference in RR ( I . 1) from the irradiated invasive group; however in siru patients in Denmark have not been followed for a sufficiently long period for compari- son with long-term survivors of invasive cervical cancer. Time trends in RR combined with risk differences be- tween irradiated and nonirradiiated groups for specific sites were therefore chosen to evaluate the possible influ- ence of irradiation on the observed risks.
The extended follow-up provides further information on the long-term hazards of radiation, inasmuch as pn- viously demonstrated excess and decreased risks per- sist.” The risk attributable to radiation for cancer in organs close to or at intermediate distance from the cer- vix increases with time to 64/1oooO women yeam, as daes the RR (to 1.9; 95% CI = 1.4-2.5) (Fs I). The attributable risk only changes slightly if the uterus is not included in the calculation. Intmstingly, the attribut- able risk increases from a lower level at the OUM to
No.
lev Ca
do an thi th
ct
I
or
ce O‘
di 9. T ic e a r’ a E t z 1
4
I
!

--’ I ...
rs .e
I 1- ..“ ,
- I-
D ?
e t --
r.
. . ” ,
r_.
L,..
,... ,
.... r
F. ,
L.
SECOND PRIMARY CANCER AFTER TREATMENT storm 685 No. 4
levels comparable to those published on data from the Connecticut Tumor Registry.”
Other genital organs, uterus, and ovanes receive large doses of radiation3’ during treatment of cervical cancer, and it is thus not surprising that the risk for cancer at these organs increases with time since exposure and that there is a significant excess of cancer of “other genital organs.” Adjusting for uteri and ovary at risk does not change the RR appreciably after an irradiated invasive cervical cancer (RR uterus = 0.7; 95% CI = 0.5-0.9; RR ovary = 0.6; 95% CI = 0.4-0.7), whereas the deficit disappears in the nonirradiated group (RR uterus = 3.3; 95% CI = 0.7-9.7; RR ovary = 2.2; 95% C1 = 1.0-4.0). These findings are at variance with those from Connect- icut,m where cancers of the ovaries and uterus are above expectation after radiotherapy; however, the time trends are similar to those in the current study. The discrepant results for the RR may be due to a more conservative attitude towards accepting new primary cancers in organs close to or adjacent to the cervix in Denmark than in Connecticut.18*u The same adjustment for uten and ovary at risk for nonirradiated in situ patients (61% uteri and 88% ovanes intact)I0 changed the RR uterus to 0.3 (95% CI = O. 1-0.6) and the RR ovary to 0.8 (95% C1 = 0.5-i.2), which agree well with previous findings.”
The urinary bladder receives radiation doses compa- rable to those of female genital organs” when a woman is treated with radiotherapy for cervical cancer. A signif- icantly increasing trend in nsk by time and a signifi- cantly increased RR for bladder cancer among long- term survivors are seen only among irradiated invasive cervical cancer patients. This indicates that radiation
TABLE 6 Obse~ed and fipmed Second Pnmary C a n a Among Sei& Pstlenu With Carcinoma In Siiu ofthc Cervix
Uten Foilowcd for 10 or More Yean According to Trcatmcnt With or Without Radiation
Irradiated Not irradiated Seeond primary w a r
(ICD7 code no.) O E O F 0 E O F
Stomach(151) O 0.6 0.0 6 4.2 1.4 Colon (153) 3 1.5 2.0 10 12.4 0.8 Rectum (154) I 0.8 1.3 4 6.7 0.6 Panmas (157) 2 0.5 3.9 7 4.2 1.7 Lung (162) 2 1 . 1 1.8 29 12.4 2.3t Brega ( 170). 2 4.1 0.5 50 50.7 1.0 Corpus uim (172) 2 1.3 1.6 3 13.9 O.2t Ovary (175) o 1.1 0.0 9 11.8 0.8 Other gmital(l76) 2 0.2 11.8. 8 1.6 4.9# Bladdrr(181) 2 0.5 4.7 6 4.3 1.4 Melanoma (190) O 0.4 0.0 4 5.5 0.7 Brain (193) O 0.5 0.0 3 5.4 0.6 Connectiwtissue(197) O 0.2 0.0 O 2.1 0.0
*P < 0.05. f P < 0.01. # P < 0.001.
OBSERVED NO OF CMES
W 6 4 2 3 cu 2 1
R R C
5
4
3
2
1
C
I 7.6
2 2
*NU
c u
1 I I I 1-4 5-8 10-14 15-le
TIME SINCE FIRST RADIATION TREATMENT (YEARS)
FIG. 2. Relative risk (RR) and 95% confidmcc interval for acute nonlymphocytic leukemia (ANLL) and chronic lymphobktic leuke- mia (CLL) among women trratcd for cervical canar, by time since fim radiation treatment
plays a part in the increased risks, and the findings cor- roborate well with those of other^.^'^'^." However, ex- c e s s ~ ~ of bladder cancer are observed after both invasive and in situ cancers, irrespective of treatment. Cigarette smoking, which is an identified risk factor for both cer- vical cance332 and bladder cancer,)’tM may play an addi- tional role.
The rectum also receives high doses,)’ and radiation may induce some of the rectal cancer excess observed, as seen in studies of women treated for benign gynecologi- cal disease’.’ and cervical No excess risk of rectal cancer was observed among atomic bomb survi- vors’ or spondylitis patients,” in whom radiation doses would be lower. In the current study also, the findings for nonirradiated women are similar to those for irra- diated patients although not attaining statistical signifi- cance.
During radiotherapy for ceMcal cancer, different sec- tions of the colon receive widely varying radiation doses from high levels (7000 rad) to low levels (4QO rad). In this study the colon was not subdivided into anatomical
686 CANCER February 15 I988 Vol. 61
sections; in contrast to the rectum, no increased risk was observed (RR = 1.0). Increased mortality from colon cancer has been observed both among spondylitis pa- tients)' and among people treated for metropathia hem- morrhagica? in which radiation doses are lower than after treatment for invasive cervical cancer.
It has been ~peculated'~ that the low colon cancer risk can be explained by the fact that low social class is a risk factor for cancer of the c ~ M x ' ~ and high social class colon cancer.38 The low risk observed among nonirra- diated in situ patients (RR = 0.8) supports this explana- tion, but not the consistently highest risk (10%-40%, Table 4) among nonirradiated invasive cervical cancer patients through all periods. However, the increased risk seen among nonirradiated as compared to irradiated pa- tients with invasive cervical cancer, is probably due ei- ther to chance or, although speculative, to an interaction of endogenous estrogen production with the colon cancer risk among those with functioning ovarie~.'~
An increasing trend in risk by follow-up is observed for both pancreatic and stomach cancer after an irra- diated primary, reaching a maximum after more than 30 years of follow-up. This is in agreement with obser- vations on irradiated spondylitis patients3' although the radiation doses are lower (99-300 rad):) and in other studies on irradiated cervical cancer patient^?^,^^ Stom- ach cancer and pancreatic cancer also were increased in the Connecticut however, no observation was made after 20 to 29 years of follow-up. Since overall elevations of risk also are observed among nonirradiated patients, cigarette smoking, which has been related to both stomach" and pancreatic cancer,'6 may be respon- sible in part for the increased risks, even among irra- diated patients.
The lung cancer excesses observed among both irra- diated and nonirradiated patients (Table 3 and 4) and to some extent the excesses of esophageal (Table 3) and stomach cancer, also may be explained by risk factors in common with cancer of the cervix, i.e.. smoking and social class.'2 The excess of lung cancer agrees well with the hypothesis of ~molon&''~~~ as Seen in other studies of cervical cancer patients."." However, the pattern of risk over time is at variance with the observations of h i c e et
where the RR declined to normal levels after 20 years of observation. In our study, the RR remains con- sistently elevated throughout the follow-up period, indi- cating an effect on all patients and not an effect related to misclassification of lung metastasis after the primary cancer. Kleinerman et al." attributed a five times higher RR of lung cancer among irradiated than nonirradiated cervical cancer patients to differences in social class and Stage of disease being associated. which should in turn be related to radiotherapy; although plausible, this is not Corroborated by the results from Denmark.
One of the most striking findings is the significant deficit of breast cancer after an irradiated invasive ceM- cal cancer (RR = 0.7), a deficit that is apparent throughout the follow-up. No deficit is observed IO or more years after diagnosis of nonirradiated carcinoma in sifu (RR = l.O), whereas a slight hut nonsignificant deficit is observed after a nonirradiated invasive cervical cancer. Ovarian function may be assumed to be intact for all (in situ) or a large proportion (invasive) of the two nonirradiated groups. Surgically and radiation-induced menopause have been shown to reduce breast cancer risk,''.'' and radiation seems to be etiicient in this re- spect even if women are irradiated at ages older than 50 years? The younger a woman is at artificial menopause, the lower the breast cancer risk".? although age has not been considered in this anaiysis, our previous follow-up showed the lowest risk for breast cancer after irradiation at young ages." Endogenous estrogens have been related to increased breast cancer risk." whereas exogenous n trogens given as replacement therapy increase the risk only slightly, if at A s in other s t~dies '~ .~~-" our findings point to a protective effect of cervical cancer irradiation on breast cancer, probably due to destruction of the ovaries. In addition, cervical cancer patients have risk profiles, e&, early age at first birth, low social class, that would result in lower breast cancer rates compared to the general population."
Other cancer deficits among irradiated women are those of skin melanoma (RR = 0.6) and brain tumors (RR = 0.6). Exogenous estrogens and reproductive fac- tors may influence the development of melanoma," and a protective effect of bilateral oophorectomy has been described!6 Breast cancer was found in excess after ma- lignant melanoma in one study" but not in another.q Meningiomas and breast cancer may share hormonal risk since meningiomas constitute a substan- tial proportion of brain tumors, ovarian ablation may influence the deficit.
The excess of connective tissue sarcomas is present among both irradiated and nonirradiated invasive cer- vical cancer patients followed for more than 20 years (Table 4); however, a significantly increased risk is Seen only among irradiated women. Several reports of radia- tion-induced soft tissue sarcomas have been pub- l i~hed, ' .~ .~ ' all showing a clear relation between the site of the sarcoma and the therapeutic fields. However, the relative excess of 19% (Table 5) observed for sarcoma development close to or at intermediate distance from the radiotherapy fields is not statistically significantly different from the expected distribution in the female population. Wagone? showed a ratio 3: I for leiomyo- Sarcomas and carcinosarcomas among women irra- diated for gynecologic disorders. In the cumnt study, the overall distribution by morphologic features of soft
N<
ti! Wi
is ri fc b e: e: t< d Ji
C
tl I!
I
a t t I 1
1 (
I
!

No. 4 SECOND PRIMARY CANCER A ~ E R TREATMENT Srorm 687
tissue sarcomas was no different from that among women in Denmark.”
Although a significantly i n c d RR (3.5) for ANLL is observed only during the first 5 years of follow-up, the risk continues to be slightly elevated (nonsignificantly) for 19 years. No excess is seen of CLL, which has never been assoCiated with radiation.’ Surprisingly, in most early leukemias were not observed in exccss after radiotherapy for cervical cancer, in contrast to the result of studies of patients who m i v e smaller doses of radiation to the bone marrow?d In other large- scale studies of cervical cancer patient^,'^.",'^ an in- creased risk was observed, although it was much smaller than predicted on the basis of radiation dose to the marrow.
It has been argued that very high doses of radiation inactivate or kill cells in the bone marrow. The results of a recent case-control study among cervical cancer pa- tients in Denmark’ are in line with this hypothesis, as is the analysis of medically irradiated populations.” The highest RR (12.9) for ANLL is observed among in sifu patients. An explanation to the high risk among irra- diated in siru patients compared to invasive, could be that the bone marrow receives lower doses, if in siru cancers are treated with hrachytherapy alone as is often seen for invasive Stage I cancers, or with reduced exter- nal-beam therapy. If so, less inactivation or cell killing in the bone marrow is likely, and a higher leukaemogenic potential of the radiation a possibility. The analysis on leukemic risk would have benefitted if numbers of leu- kemia and quality of notifications allowed differentia- tion between carcinoma in sifu, Stage l cervical cancer and other m e s .
Generally, in studies of cervical cancer patients, in- cluding population-based studies, the overall risk of sec- ond primary cancer is very close to that of women with- outcancer(RR= 1.1,’5RR= 1.4,)0presentRR= 1.1). Several caveats must be kept in mind when interpreting the current data and comparing them with others. These include differences in the definition and classification of second primary cancers; lack of correction for organs at risk:6 underreporting,2* and decreasing autopsy rates52 also may mask true risks. In addition, a substantial study size and long follow-up are needed in order to demon- strate the relatively small increased risks of second pri- mary cancer related to radiotherapy. A further problem is associated with validity of exposure information.
In conclusion then, by preventing death from cancer of the cervix, radiation for ceMcal cancer over a 35-year period in Denmark has influenced the risk of second cancer both directly, by increasing the risks of bladder, other genital, rectal, and connective tissue cancers, ANLL, and perhaps stomach and pancreatic cancers, and indirectly, possibly through some hormonal mecha-
a
nism, by decreasing the risks of cancers of the breast and perhaps brain, skin melanoma, and colon cancer. The role of radiation in these excmes and deficits will be addressed in d&l in case control studies both nation- ally and internationally,” in which aciual organ doses will be taken into account” and controlling for the in- fluence of confounding factors is possible. However, follow-up for life of irradiated populations is warranted to evaluate fully the long-term carcinogenic risk of radi- ation.
REFERENCES
I . Boia JD. Cinar following medical irradiation. Cancer 1981; 47:1081-1090.
2. Schull WJ. Atomic bomb survivors: Patterns of canar risk. In: B o k ID Ir, Fraummi IF Ir, eds. Radiation C u c i n ~ n m s : Epidemi- ology and Biological Significance. New York Raven Press, 1984; 21-36.
3. Darby SC. Nakashima E, Kat0 H. A patallel analysis of cancer monality among atomic bomb suMvors and patients with ankylosing spondylitisgkn x-ray therapy. JNafl Cancer Inst 198% 75:I-Zl.
4. Unitcd Nations Scientific Committee on the EK& of Atomic Radiation. Ionizing radiation: Sources and biological dfau. In: Offi- cial Records ofthe General Auembly, ThinySeventh W o n , suppl. no. 45. New York United Nations, 1982.
S. National Academy of Sciences Advisory Committee on the Bic- logical Eñens of Ionizing Radiations. The &cas on populations of exposure to low levels of ionizing radiation. Washington, DC National Academy Rers 1980.
6. lchimm M, Ishimam T, Bel* JL. lncidena of leukemia in atomic bomb survivors belonging to a fixed w h a in Hiroshima and Nagasaki, 1950-1971: Radiation doze, ycan &r wpouire, age at exposure, and typ of leukemia. Jpn Radiar Res 1978; 19262-282.
7. Smith PG, Doll R. Late dfau of x-irradiation in patients treated for mctropathia hacmorrhsgica. Br JRadiol 1976; 49224-232.
8. Wagoner JK. Leukemia and other miliSiipncin following radia- tion therapy for gynecological disorders. In: Boia ID Ir, Fraumcni JF Ir, eds. Radiation carcinognicsis: Epidemiology and biological sinifi- cana. New York Raven Rcsr, 1984; 153-159.
9. Storm HH. Boia JD Ir. Leukaemia after &cal cancer irradia- tion in Denmark. inr J €pidemio/ 1985; 14363-368.
IO. Storm HH, Jcnscn OM. Secondary primary canars among 40518 womcntreatcdforcanaror~inomainsifuofllicanixuten inDenmark 1943-1916.111: DayNE,BoiaJDJr,edr.SemndCanar in Relation to Radiation Tnatment for Cewical Canar (IARC Sci publ. no. 52). Lyon: International Agency for Rcscnrch on Cancer, 1983: 59-69.
I I . Storm HH, Ewcnz M. Scmnd war following cancer of the female genital system in Denmark 1943-1980. Nafl Cancer Insf Monogr 198% 68331-340.
12. Pettcru>n F. Bj8rkbolm E. Staging and rcporüng of arvical carcinoma. Sernin Oncol1982; 9287-298.
13. Hutchison OB. Leukemia in patients with cancer ofthe arvix uUn tnatcd with radiation: A report wvcring the 6rslS yean of an intemationai audy. J Natl Cancer Inst 1968; 40.951-982.
14. Boia ID, Hutchison OB. Leukemia in women followingradic- therapy for aMcal cancer Ten-year follow-up of an international study. JNaflCancerInrt 1980; 65:115-129.
IS. Bois I D Ir, Day NE, Andervn A el a/. Semnd canars follow- ing radiation treatment for aMcal cancer An intrrnationai whbora- tion among canm registries. J Natl Cancer imf 198% 14995-975.
16. Curtis RE, Hoover RN, Klcinrrman RA, lbwcy EB. Second cancer following cancer ofthe female genital aynem in Connecticut. Nat/CancerInst Monogr 198% 60113-137.
17. Clemm- I. Statistical studies in the I*iology of d ¡ a n t neoplasms: 111. Denmark 1958-1962. Acta Pafhol Microbid Scand [Supp/] 1969.

CANCER February 15 1988 Vol. 61 - 688
18. Jcrika OM, Storm HH, Jcnm H. Cancer ngistration and the study of multiple primary canccn in Denmark 1943-1980. NalI Cancerlmt Monogr 1985; 60245-251.
19. Danish Cancer ReButry. Cancer incidmce in Denmark I981 and 1982. Dan& Cancer Sonay, Copenhagen, 1985.
20. Storm HH. Complnenes of cancer regklration in Denmark 1943-1966 and cliicacy of record linkage praedum In1 J Epidemiol (in pma).
21. 0stcrlind A, Jcnsen OM. Evaluation ofcaocer in casts in 1977 Preliminary evaluation of regklration of cancer casts by the Cancer Registry and National Patient Registry. Ugeskr Laeger 1986; 1472483-2488 (in Danish).
22. Storm HH. L y w E, Wründ A, Jmscn OM. Multiple primary cancers in Denmark 1943-80: lnüucnce of poaslbk undcrreponing and sugpatcd risk facton. Yak JBidMed 1986; 58547459.
23. Monson RR. Analysis of dat ive survival and proportional mortality. Comput Biomed Res 1974; 7325-332.
24. Rothman KI, Boice JD Ir. Epidemiologic analysis with a m grammable calculator. -on: Epidemiology Rcsourq 1982: 30-31.
25. Schoncnfeld D. Multiple primary canan. In: Schottenfeld D, Fraumeni IF Jr. Cdr Cancer Epidemiology and Prevention. Philadel- phia: Saundcn, 1982; 1025-1035.
26. Boia JD Jr, Storm HH. Cunis RE el al. Introduction to the study of multipk primary canccn NalI Cancer INI Monogr 1985; 683-9.
27. Storm HH, Jenscn OM, Ewe* M el ai. Summary: Multiple primary canan in Denmark, 1943-1980. Nall Cancer Ins1 Monogr 1985:68411-430.
28. Sarensen B. Late mults of radium therapy in cervical carci- noma. Ac~a Radld 1958: (Supil) 16995-100.
29. Dickson RS. Late mulu of d u m treatment of carcinoma of the cervix. Clin Radio/ 1972; 23528-535.
30. Kkinemun RA, Cuflis RE, Boice JD Ir, Flannery JT, Frau- mcni JF Ir. Second c a n m foliowing radiotherapy for mica l cancer. J NaII Cancer Ins1 1982; 691027-1033.
31. Clarke EA, Krciger N, Spcngler RF. Ssond primary cancer following treatment for cervical cancer. Can Med Assoc J 1984: 131553-556.
32. Keky JL, Hildreth NG. B W and gynecological cancer epide- miology. BaaRaton,FL:CRCPrcss, 1983: 117-141.
33. Stovdl M. Organ dosca from radiotherapy ofcancer ofthe uter- ine cervix. in: Day NE, bin JD Ir. eds. Second Cancer in relation to radiation treatment for cervical cancer (IARC Sci publ. no. 52). Lyon: international Agcncy for Raeardi on Cancer, 1983: 131-135.
34. Lynge E. Storm HH, Jenxn OM. Evaluation of trends in soli tissue sarcoma according to dipsnaatic criteria and consumption of phenoxy herbicida. Cancer 1987: M):1896-1901.
35. Lockwood K. On the etiology of bladder tumours in Keben- havn-Frcdenkskg! An inquiry of 369 psticntsand 369 controls. Acla Patho/ Microbid Scad [Supp/) 1961: 51:1-166.
36. Doll R, Pelo R. Mortality in relation 10 smolrino: Twenty yean obseivationonmakBrituhdMonBrM~J1976;21525-1536.
37. Smith Po, Doll R. Mortality among paticnu with ankyloYng spondylitis aRcr a Einglymtment coune with x-ray* Br Med J 1982; 284449460,
38. Schottcnfcld D. Winawcr SJ. L~QC intestine. In: Schoncnfeid D, Fraumeni IF Jr, cds. Cancer epidemiology and prevention. PhiL, delphk Saunden, 1982; 703-727.
39. McMichacl AJ, P O W JD. Reproduction. end-nous and ex- ogenous sex hormones, and colon can- A review and hypothesis 3 Not/ Cancer Ins1 1980: 651201-1207.
40. Hacnslcl W. Correa P. Developments in the epidemiology oí stomach cancer in the past decade. Cancer Res 197% 353452-3459.
41. Winkelstein W Jr. Smoking and cancer of the uterine cervix Hypoth& Am 3 Epidemid 1977; Ioó:257-259.
42. Winkelstein W Ir, Schillitoe U. Brand R. Johwn KK. Funher comments on cancer of the cervix, smoking and berprvinu infection. Am JEpidemid1984; 1191-8.
43. Trichopoulos 0, MacMahon B. Cole P. Menopause and b m cancer risk. J Nall Cancer Ins1 1972; 48:605-6 13.
44. Feinleih M. Breas cancer and artificial menopsuse: A cohort studv. 3 NaI1 Cancer Ins< 1968: 41:315-339.
45. HOUY EA. weis NS. LHIM. CurPneous melanoma in relation to exogenous hormones and reproductive fanon 3 Nad Cancer I ~ I 1983: 70827-831.
46. Gallagher RP, Elwood JM, Hill Gü, Coldman Al. Threlfdl WJ. Spinelli 11. Repmductive facton, oral contraceptives and risk of maüg- nant melanoma: Western Canada melanoma study. BrJ Cancer 1985: 52901-907.
47. Tucker MA, Boia JD Jr. HoiTman DA. Second cancer follow- ing cumncous melanoma and cancen of the brain. thyroid. connective tissue. bone and eye in Connecticut. 1935-1982. .Vai/ Cancer INI Monogr 198% 68: 161 - I89
48. &ierlind A. Olxn JH. Lyngc E. Ewe* M. Semnd cancer rol- lowng cutaneous melanoma and canccn of &e brain. thyroid, COD ncctiveiissue. boneandeye in Denmark. 1943-1980. S a t l C a n c r r l ~ i Monogr 1985: 68361-388.
49. Schoenbeg BS. Christine BW. Whisnant JP. Nervous system ncoplarmr and primary malignancies of other rites Thc unique ars00- ation betuun meninpicomas and brrast cancer. \;woloXy 1975: 25:705-7 12.
50. Pinkston JA. Sckinc I. Postirradiation LZrmmi (malignant fi- brous histiocytoma) folloWng ccrvia cancer. Cancer 1982 49434- 438.
5 I. Kim JH, Chu FC. Woodward HQ et al. Radiation induced SOR tissue and tone wcoma. Radidom 1978: 129MI-508.
52. Storm HH, Andenen J. PerrrntsOe of auropaia in cancer po tienuin Denmarkin 1971-1980. UgrskrLarger 1986.1~.1I10-1 I14 (in hnish ) .

The Use of Magnetic Resonance Imaging and Spectroscopy in the Assessment 07 Patients With Head and Neck
and Other Superficial Human Malignancies
W. GlLLlES MCKENNA, MD. PHD,. ROBERT E. LENKINSKI. PHD,t ROBERT A. HENDRIX. MD,S KATHERINE E. VOGELE. BA.7 AND PETER BLOCH, PHD'
The proper demarcation of d i d tissue is important for radiation thenpy phnlng and trritwiit. The volume to he irrndmted is vsuplly identified on radiographs or on x-ray computed tomography (cr) soetions. Magnetic resonance (MR)-derived images of the proton Ti. relwtion times in prmul *el elements, typically 0.5 nun* or less, provide si@antiy sharper differentiation between nMm;il and diseased tissue. The T2 vdws in tissuc depend on tbe tissue composition, histologic condition, and phys- iologic environment within the tumor. Furthermore, for many tumors the histogram of R v d a s h.s a dear biphasic distribution suggesting thpt R m p s may he Usctol for the identifiation of necrMic or hypoxic regions within tumors. The distribution of T2 values witbin the tumor bed shorn the geneml pattern that the T2 vdues are elevated with a range greater than that seen in normal muscle. Ehrted T2 values are not by themselves dingamtic of mliginacy; however, they demonskate the heterogeneity of ihe microenvironment present within a tumor. The spatid distribution of R vplnes is he¡¡ explored as a method for computer wsishnce in the delineation of the target volnme for treatment pbo¡n& In addition, M R P-31 spectroscopic eximinntiws were performed on 30 patients with squimws cell car- cinomas of the head and neck. Although hampered by m d e contamination in Some P-31 spectra o b l 8 k d with surface coil profile localintion techniques, significant trends cm still be appredated ia our datu. These trends include the following (1) the P-31 specbufrom millgnint tissue have well-resolved spectral lines in the upfieid region that corres& to Pi, pbsphomomester (PME), and phosphodiester (PDE) not usuilly seen in normal muscle; (2) the PDE/B-ATP and PME/B-ATP ratios are greater tbia unity In nU a s ; and (3) most of the tumors have bigher PME peaks than PDE peaks. The P-31 speebi from patients treated with ionizing radiation changed during and after tbenipy. Some of the c h g c s emld be associated with alteration of the tumor metabolic activity or synthesis and breakdown of lipoproteins. These studies suggest that mngnetic resotmm imaging (MRI) and magnetic resonmce speftmseopy (MRS) studies my be useful for both radiotberapy treatment phoning and the noninvasive momking of patients both hefore and during treatment.
Cancer 61:2069-2075, 1989.
HE EFFECnVE TREATMENT Of tUmOrS by radiaUOn T therapy depends on accurate delineation of the ma- h a n t tissue. Failure to treat the entire volume infiltrated by a tumor will result in local recurrence. There also is evidence to suggest that local failure may result from the pmnce of heterogeneous, hypoxic regions within a tumor v-kme. Additionally, one of the assumptions underlying fractionated radiotherapy is that it allows the reoxygen-
ation of hypoxic tumor tissue to take p W but the kinetics and scope of such reoxygenation have not been studied extensively in human tumors. Magnetic resonance im- aging (MRi) and magnetic resonance spectroscopy (MRS) offer the oncologist new methods with which to nonin- vasively study the extent and metabolism of tumors and to follow the changes that occur in tumors as they undergo treatment. A prospective study was initiated ofpatients with head
and neck and other superhcial malignancies before and
whether MRi and MRS can be used to dan and follow
- From the Dcparimcnis of *Radiation Oncology, tRadiolugy, and
$Otorhinolqngobgy, Hospital ofthe Univenity ofPennsylvania, Phil- .dclohic hnwlvanh.
Our goal in these studies was to - - - --,- -~~
&\ad, for npnnts: W. Gillin McKenna MD, PhD, Dmrtmerd Of Radiation Oncolw, Hospital ofthe Univmity ofp~nrylvania, MMJ spnioc Sheet, Philadelphia, PA 19104.
Accepted for publication May 26, 1989.
therapy. We used MRI to study whether iKtter definition of tumor volumes can be we can develop automated computerized methods for doing so
I..
2069

an, + :din f
V I , -. 207 I .<. NONINVASIVE MONITORING OF RADIOTHERAPY PATIENTS * McKenna et ai. ,: pto. 10 .. . , ...
Results
Analysis of T2 Distribution in Patients
Figure I shows both the quality of the T2derived image for a histologically confirmed liposarcoma in the thigh of
natient and the tissue heterogeneity within the tumor &. The T2 distribution throughout the entire tumor and n o i d surrounding tissue shown in Figure 2 was obtained by evaluating the T2 values in 17 contiguous axial d o n s 7.5 mm apart. The means of the derived T2 values for normal muscle and the liposarcoma were 35 and I 10 ms, respectively, with all of the T2 values of normal muscle king less than 45 ms. The maximal values of the T2 values within the tumor volume were found at the center ofthe tumor volume. The range ofvalues ofthe T2 values for the tumor volume shows a broad peak extending from 311 ?o 180 ms.
In Figures 3A and 3B, the T2 distribution within the tumor and normal volume, respectively, are shown for a patient with a T2NO squamous cell carcinoma of the floor of the mouth. Once again, the T2 distribution shows a mean value higher than that of adjacent normal tissue and the range of values also is large (35 to 95 ms). In Figures 3C and 3D, this is compared with the distribution seen in a patient with a benign branchial cleft cyst that was found to have an extensive lymphoid infiltrate and a I rge cystic component at surgery.
Figure 4 shows the regional T2 distribution in multiple axial slices through a large soft tissue sarcoma. In this case, we show the change in the distribution of the T2 values in serial cuts through the tumor volume at 7.5- mm intervals, not the integral value throughout the tumor volume. Position I is defined as the most inferior part of the tumor volume and position 16 as the most superior
FIG. 3. Ibe TZ distribution within squamous ccll carcinoma of the Boor of the mouth (A). The mean value and range of values ir mter thanthatseeninadjnanf ~ rma l t i s~~ (B ) .AJ imi l s rpa t t~n~~ found in a patient with a nonmalignant branchial cleR cyst with lymphoid tissue (C); however, mmpMsd with n d adjaant tisue (D), the T2 distribution within the ben i IsUon s- a normal pius a sndc abnormal twional Ti.
n I-)
ninLI1
FIG. 4. The regionai distribution of TZ in a SOR tissue sxoma. The TZ -ms arc shown in 16 axial sliar xpratcd by 7.5 mm. Slice I mmponds to the moat inferior imaged d o n and slice 16 the most superior. The nominnl cmvsl ponions of slica 6 thmugh IO show the bgm n u m h of regionally clevited T2.
part. This illustrates the changes that are seen in com- paring one region of the tumor to another. Note that the largest T2 values are seen close to the center of the tumor volume (positions 6 through IO), although the values at the edges of the tumor mass remain elevated above nor- mal. Furthermore, there appears to te several components of the T2 distribution, including one which is elevated to higher levels and Seen most clearly in the central part of the tumor volume. Of course, it is possible that some of these components represent edema in surrounding normal tissues rather than the presence of malignant tissue per se. The analysis of this possibility will await better cor- relation of T2 maps with resected specimens after surgery.
Analysis of "P Spectra
Figures 5A and SB show "P spectra for two patients who had T3NO squamous cell carcinoma of the lower lip. The tumors masses in both of the patients were large
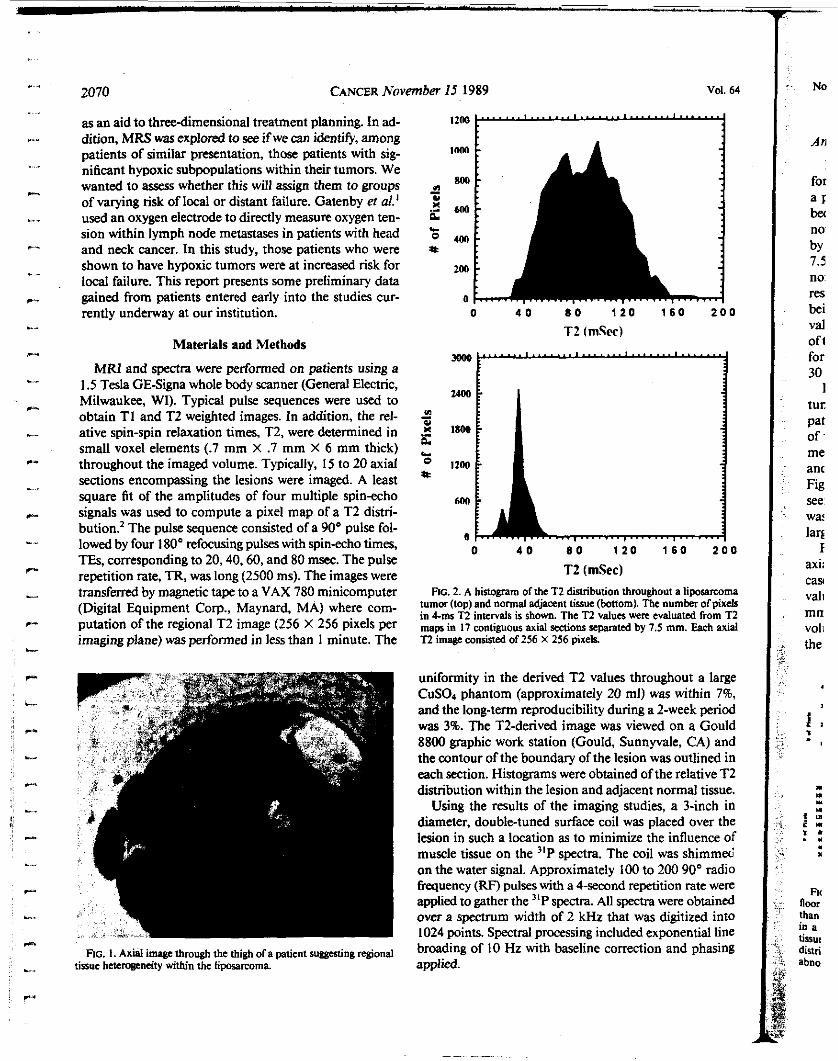
2070 CANCER November 15 1989 Vol. 64
as an aid to three-dimensional treatment planning. In ad- dition, MRS was explored to see if we can identi@, among patients of similar presentation, those patients with sig- nificant hypoxic subpopulations within their tumors. We wanted to assess whether this will assign them to groups of varying risk of local or distant failure. Gatenby m al.' used an oxygen electrode to directly measure oxygen ten- sion within lymph node metastases in patients with head and neck cancer. In this study, those patients who were shown to have hypoxic tumors were at increased risk for local failure. This report presents some preliminary data gained from patients entered early into the studies cur- rently underway at our institution.
Materials and Methods
MRI and spectra were performed on patients using a 1.5 Tesla GE-Signa whole body scanner (General Electric, Milwaukee, WI). Typical pulse sequences were used to obtain T I and T2 weighted images. In addition, the rel- ative spin-spin relaxation times, T2, were determined in small voxel elements (.7 mm X .7 mm X 6 mm thick) throughout the imaged volume. Typically, 15 to 20 axial sections encompassing the lesions were imaged. A least square fit of the amplitudes of four multiple spin-echo signals was used to compute a pixel map of a T2 distri- bution? The pulse sequence consisted of a 90' pulse fol- lowed hy four 180" refocusing pulses with spinecho times, TEs, corresponding to 20,40,60, and 80 msec. The pulse repetition rate, TR, was long (2500 ms). The images were transferred by magnetic tape to a VAX 780 minicomputer (Digital Equipment Corp., Maynard, MA) where com- putation of the regional T2 image (256 X 256 pixels per imaging plane) was performed in less than 1 minute. The
FIG. I . Axial image through the thigh ofa patient suggesting r*onal tissue hctnogcneity within the Liposarcoma
o 4 0 8 0 1 2 0 1 6 0 2 0 0
T2 (mSec) Flc. 2. A histogram ofthe T2 disvibution throughout a lipoaamma
tumor (top) and normal adjacent tissue (bottom). The numbcr ofpixels in 4ms T2 intervals is shown. The T2 values wcre evaluated from T2 m a p in 17 contiguous axial d o n s separated by 7.5 mm. Each axial i2 image consisted of 256 X 256 pixek
uniformity in the derived T2 values throughout a large CuS04 phantom (approximately 20 mi) was within 796, and the long-term reproducibility during a 2-week period was 3%. The T2-derived image was viewed on a Gould 8800 graphic work station (Gould, Sunnyvale, CA) and the contour of the boundary of the lesion was outlined in each section. Histograms were obtained of the relative T2 distribution within the lesion and adjacent normal tissue.
Using the results of the imaging studies, a 3-inch in diameter, double-tuned surface coil was placed over the lesion in such a location as to minimize the influence of muscle tissue on the "P spectra. The coil was shimmeti on the water signal. Approximately 100 to 200 90" radio frequency (RF) pulses with a 4-second repetition rate were applied to gather the "P spectra. Ail spectra were obtained over a spectrum width of 2 kHz that was digitized into 1024 points. Spectral processing included exponential line broading of IO Hz with baseline correction and phasing applied.
~
c_
- No
An
for a r bec no by 1.5 no res be¡ Val oft for 30
1 tur
of me an< Fig see war lar$
I axi: cas vali mn vol1 the
pat
1,
rn I. I II ,I
6 - r . . " . Fn
than in a lissu< distn abno
nWr
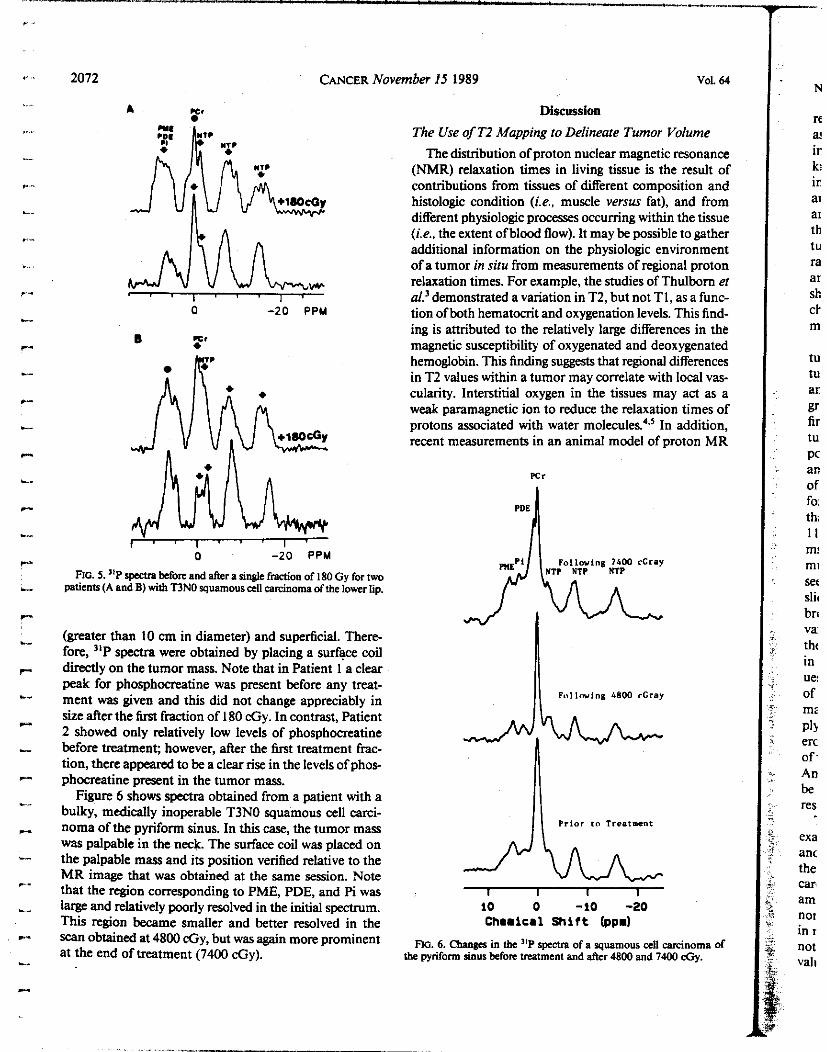
I .
2072 CANCER Novc
U* A
O -20 PPM
B :' IC."
o -20 PPM
FIG. 5. "P s q befon and after a single fmdon of 180 Gy for two patients (A and B) with T3NO squamous cell caarcinoma of the lower tip.
(greater than 10 cm in diameter) and superficial. There- fore, "P spectra were obtained by placing a surface coil directly on the tumor mass. Note that in Patient 1 a clear peak for phosphocreatine was present before any treat- ment was given and this did not change appreciably in size after the fust fraction of I80 &y. In contrast, Patient 2 showed only relatively low levels of phosphocreatine before treatmen$ however, after the fust treatment frac- tion, there appeared to he a clear rise in the levels of phos- phocreatine present in the tumor mass.
Figure 6 shows spectra obtained from a patient with a bulky, medically inoperable T3NO squamous cell carci- noma of the pyriform sinus. In this case, the tumor mass was palpable in the neck. The surface coil was placed on the palpable mass and its position verified relative to the MR image that was obtained at the same session. Note that the region corresponding to PME, PDE, and Pi was large and relatively poorly resolved in the initial spectrum. This region became smaller and better resolved in the Scan obtained at 4800 &y, but was again more prominent at the end of treatment (7400 &y).
?mber 15 1989 vol. 64
Discussion
The Use of TZ Mapping to Delineate Tumor Volume The distribution of proton nuclear magnetic resonance
(NMR) relaxation times in living tissue is the result of contributions from tissues of different composition and histologic condition (i.e., muscle versus fat), and from different physiologic processes occurring within the tissue ( ie . , the extent ofhlood flow). It may be possible to gather additional information on the physiologic environment of a tumor in situ from measurements of regional proton relaxation times. For example, the studies of Thulbom et al'demonstrated a variation in T2, but not T1, as a func- tion ofhoth hematocrit and oxygenation levels. This find- ing is attributed to the relatively large differences in the magnetic susceptibility of oxygenated and deoxygenated hemoglobin. This finding suggests that regional differences in T2 values within a tumor may correlate with local vas- cularity. Interstitial oxygen in the tissues may act as a weak paramagnetic ion to reduce the relaxation times of protons assoCiated with water molecules?.' In addition, recent measurementS in an animal model of proton MR
Pci
I\ Pi lor to Treatment
10 O -10 -20 Chamical Shif t (ppd
Flo. 6. Ckws in the "P spcira of a squamous cell carcinoma of the pyiform sinus before irratment and a k r 4800 and 7400 &y.
N
re
ir ki ir ai ai
th tu ra ar sh Ck m
a!
tu tu ar gr fir tu PC an of f0i
th: 11 m! mi see Slil
bri va: thc in
of mi PIS erc of- An be res
Ue:
exa anc the can am nor in I
not val,
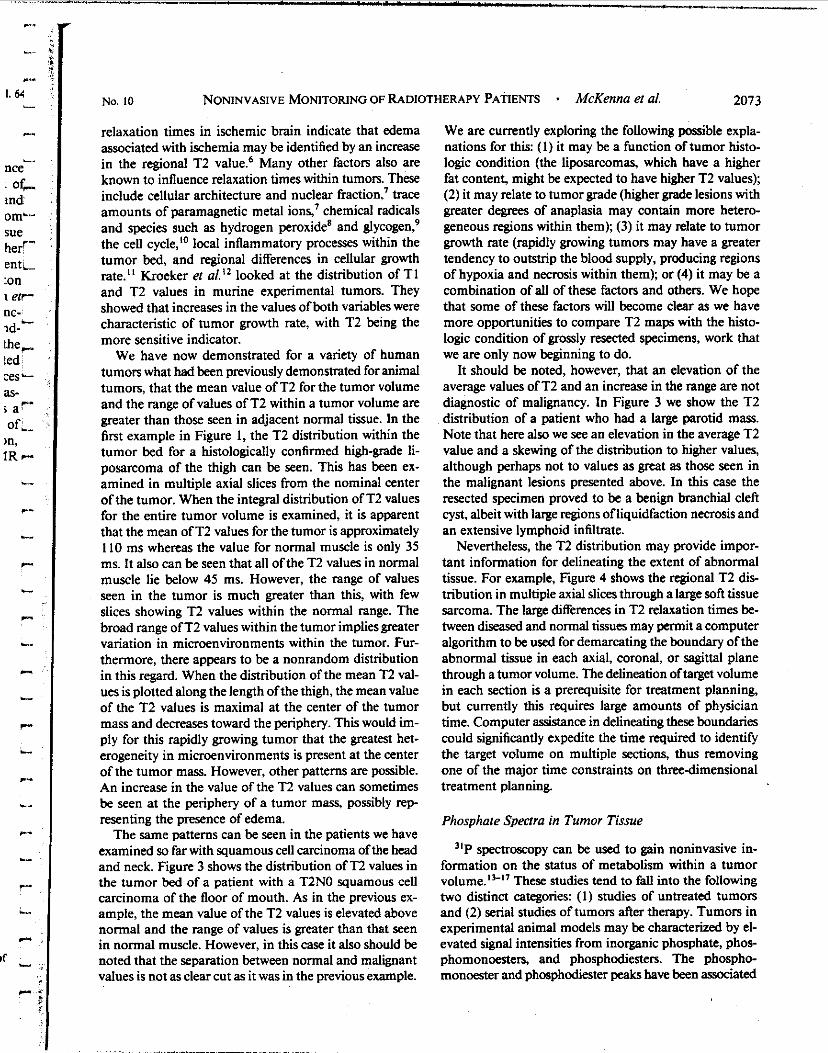
c
- C.
1. 64
,-.. -_
nce oc-
md omL- sue her'- ent, ton 1 err- nc-_ id- the, ted Les- as- E ar of,
)n, IR P-
c
c
c
I
- r-
b..
c
..- r-
L
n
L
c
If
c
No. 10 NONINVASIVE MONITORING OF RADIOTHERAPY PATIENTS * McKenna et ai. 2073
relaxation times in ischemic brain indicate that edema associated with ischemia may be identified by an increase in the regional T2 value! Many other factors also are known to influence relaxation times within tumors. These include cellular architecture and nuclear fraction? trace amounts of paramagnetic metal ions: chemical radicals and species such as hydrogen peroxide' and glycogen? the cell cycle,l0 local inflammatory processes within the tumor bed, and regional differences in cellular growth rate." Kroeker et a/.!* looked at the distribution of T I and TZ values in murine experimental tumors. They showed that increases in the values ofboth variables were characteristic of tumor growth rate, with T2 being the more sensitive indicator.
We have now demonstrated for a variety of human tumors what had been previously demonstrated for animal tumors, that the mean value of T2 for the tumor volume and the range of values of T2 within a tumor volume are greater than those seen in adjacent normal tissue. in the first example in Figure I, the T2 distribution within the tumor bed for a histologically confirmed high-grade li- posarcoma of the thigh can be seen. This has been ex- amined in multiple axial slices from the nominal center ofthe tumor. When the integral distribution of T2 values for the entire tumor volume is examined, it is apparent that the mean of T2 values for the tumor is approximately I10 ms whereas the value for normal muscle is only 35 ms. it also can be seen that all ofthe T2 values in normal muscle lie below 45 ms. However, the range of values seen in the tumor is much greater than this, with few slices showing T2 values within the normal range. The broad range o fT2 values within the tumor impliesgreater variation in microenvironments within the tumor. Fur- thermore, there appears to be a nonrandom distribution in this regard. When the distribution of the mean T2 val- ues is plotted along the length ofthe thigh, the mean value of the T2 values is maximal at the center of the tumor mass and decreases toward the periphery. This would im- ply for this rapidly growing tumor that the greatest het- erogeneity in microenvironments is present at the center of the tumor mass. However, other patterns are possible. An increase in the value of the T2 values can sometimes be seen at the periphery of a tumor mass, possibly rep resenting the presence of edema.
The same patterns can be seen in the patients we have examined so far with squamous cell carcinoma of the head and neck. Figure 3 shows the distribution of T2 values in the tumor bed of a patient with a T2NO squamous cell carcinoma of the floor of mouth. As in the previous ex- ample, the mean value of the T2 values is elevated above normal and the range of values is greater than that seen in normal muscle. However, in this case it also should be noted that the separation between normal and malignant values is not as clear cut as it was in the previous example.
We are currently exploring the following possible expla- nations for this: ( I ) it may be a function of tumor histo- logic condition (the liposarcomas, which have a higher fat content, might be expected to have higher T2 values); (2) it may relate to tumor grade (higher grade lesions with greater degrees of anaplasia may contain more hetero- geneous regions within them); (3) it may relate to tumor growth rate (rapidly growing tumon may have a greater tendency to outstrip the blood supply, producing regions of hypoxia and necrosis within them); or (4) it may be a combination of all of these factors and others. We hope that some of these factors will become clear as we have more opportunities to compare T2 maps with the histo- logic condition of grossly resected specimens, work that we are only now beginning to do.
It should be noted, however, that an elevation of the average values of T2 and an increase in the range are not diagnostic of malignancy. In Figure 3 we show the T2 distribution of a patient who had a large parotid mass. Note that here also we see an elevation in the average T2 value and a skewing of the distnbution to higher values, although perhaps not to values as great as those seen in the malignant lesions presented above. In this case the resected specimen proved to be a benign branchial cleft cyst, albeit with large regions ofliquidfaction necrosis and an extensive lymphoid infiltrate.
Nevertheless, the T2 distribution may provide impor- tant information for delineating the extent of abnormal tissue. For example, Figure 4 shows the regional T2 dis- tribution in multiple axial slices through a large soft tissue sarcoma. The large differences in T2 relaxation times be- tween diseased and normal tissues may pmnit a computer algorithm to be used for demarcating the boundary of the abnormal tissue in each axial, coronal, or sagittal plane through a tumor volume. The delineation oftarget volume in each section is a prerequisite for treatment planning, but currently this requires large amounts of physician time. Computer assistance in delineating these boundaries could significantly expedite the time required to identify the target volume on multiple sections, thus removing one of the major time constraints on three-dimensional treatment planning.
Phosphaie Spectra in Tumor Tissue
spectroscopy can be used to gain noninvasive in- formation on the status of metabolism within a tumor volume."-" These studies tend to fail into the following two distinct categories: (1) studies of untreated tumors and (2) serial studies of tumors after therapy. Tumors in experimental animal models may be characterized by el- evated signal intensities from inorganic phosphate, phos- phomonoesters, and phosphodiesters. The phospho- monoester and phosphodiester peaks have been associated

2074 CANCER November I5 1989 Vol. 64
with the extent of cell membrane biosynthesis and deg- radation." Phosphocreatine (PCr) is a high energy storage product used by some tissues to maintain ATP levels when demand exceeds the capacity for generation from oxi- dative phosphorylation. Therefore, the presence and height of this peak may give some indication of the quality of oxygenation within a tumor volume. Okunieff et showed that the PCr/Pi levels in C3H murine fibrosar- coma and spontaneous mammary caminomas trans- planted in mice were modulated by the inspired oxygen concentration. In addition, they demonstrated lower PCr/ Pi ratios in larger tumors that are likely to have a greater hypoxic component. This strongly suggests that changes in the PCr levels during therapy may possibly be used to follow tumor reoxygenation. The levels ofthe high energy phosphates of nucleoside triphosphates tend to be more constant and maintained in tissues until death. N g and coworkersm have used "P spectroscopy to study the growth of animal tumozx and their response to therapeutic agents, chemotherapy, radiation therapy, and hyperther- mia They concluded that tumors became less metaboli- cally active as they grew larger and that tumor tissues were more hypoxic than normal tissues. They also claim to have seen rapid spectral changes in tumors in response to therapy, and at least in their experimental system these changes appeared to be specific for the type of therapeutic intervention.
With the development of relatively high-field, whole- body scanners, many studies have been conducted on the application of )'P spectroscopy to the study of intact hu- man tumors.'3M23 These studies indicate that the MR spectra of the tumors show marked changes in response to therapy. For example, the studies conducted on neu- roblastomas by Maris and Chance" indicated that the level of phosphomonoester peak was a sensitive indicator of tumor regrrssion. Most of these studies used surface coils as the only method of localization, so it is likely that the observed spectra were reflections only of the hulk or average metabolic properties of the tumors. This may be disadvantageous when studying relatively heterogeneous lesions.
In Figure 5 we compare the spectra, before and im- mediately after starting treatment, of two patients had large T3NOMO squamous cell carcinomas of the lower lip (Fig. 5A). in one patient the peak for PCr was large before any treatment was given, whereas in the other patient the peak for PCR was small relative to the other peaks in the spectrum. One interpretation of this result is that, in these two patients with an essentially identical clinical presen- tation, one had a tumor that had a greater hypoxic frac- tion, as manifested by the much lower levels of PCr present in the tumor tissue. Consistent with this hypothesis is the fact that the calculated pH for the tumor tissue of this patient was 0.3 to 0.4 units lower than in the other, which
would be consistent with an accumulation of acidic prod- ucts of metabolism in the tumor tissue. However, it is of interest in this patient that after a single 180 cGy fraction there appeared to be a rapid rise in the PCr peak. If our original interpretation of this spectrum was correct this would imply rapid reoxygenation of hypoxic tumor tissue.
The situation becomes more complex as we follow pa- tients further into treatment. in Figure 6 the spectra are shown of a patient with a medically inoperable T3NO squamous cell carcinoma of the pyriform sinus. These spectra were obtained before radiation treatments were initiated, after 4800 cGy when an approximately 50% regresion of the tumor was seen and after 7400 cGy when the tumor had shrunk to approximately 15% to 20% of its original volume. in this case the original spectrum shows a relatively high peak for PCr, implying that the tumor was relatively well oxygenated, however, a large and poorly resolved shoulder is seen in the region where the peaks for phosphomonoesters, phosphodiesters, and inorganic phosphate are located. This implies the presence of a significant necrotic and heterogeneous component. At 4800 &y, this component is both reduced and better resolved. At 7400 &y, this shoulder region is again larger and poorly resolved. There are many possible explanations for this result, ie., damage to normal tissue and its vas- culature seen at the end of therapy, selection and growth of radioresistant clones during treatment despite overall continued shrinkage of the tumor mass, or simply a sam- pling error of this relatively insensitive and poorly local- ized "P spectra. This latter problem can be partially over- came by the use of onedimensional phase encoded spec- troscopy,2' a technique that allows spectroscopic information to be acquired from I-cm slices through the tumor volume, which can in turn be tied to the tumor image. We will be pursuing this route with our patients in the future. it also should be noted that there is an in- trinsic limitation to the information that can be derived from "P spectroscopy because of the relatively large voi- umes (e.& 30 mi) from which the spectra must be col- lected. This places an intrinsic limitation on the infor- mation that can be gathered from heterogeneous tumors since it averages over too large of a volume. Additionally, as the tumor shrinks it will tend to volume average in- formation from adjacent normal tissue (often muscle with a high PCr concentration). It is possible that some of these problems may be overcome by using proton spectroscopy. This may offer the possibilities of not only sampling from a smaller volume, but also of obtaining information on other useful metabolites for following the response of tu- mors to therapy such as la~tate.2~
Summary These initial studies demonstrate areas where MRI and
MRS may be useful for the management of patients with

No. 10 NONINVASIVE MONITORING OF RADIOTHERAPY PATIENTS * McKenna et d. 2075
head and neck and other malignancies. The displacement of T2 values in tumors to higher values than are seen in normal tissue may be useful both as a measure of the heterogeneity of microenvironments within a tumor vol- ume and for the development of computer algorithms to outline tumor volumes for three-dimensional treatment planning in a way that is practical and economical of physician time. In addition, it is now possible to obtain from MRS serial information about tumor metabolism under therapy in a way that is benign and noninvasive, offering us (for the first time) the ability to assess the true role of tumor metabolism in determining the outcome of therapy in human cancers. From this information may come new insights into treatment strategies for these dif- ficult patient management problems.
REFERENCES
I. Gatenby RA, Kesdcr HB, R m b l u m JS B ai. Oxygen disvibution in squamous all carcinoma melaslas%: Relationship to outcome of ra- diation therapy. Ini JRadial Oncol Bid Phys 1988 14:831-838.
2. Brcger RK, Webrü FW. Charles C, MacFall JH, Haughton VM. Reproducibility of relaxation and spin density paramaen in phantoms and the human brain measured by M R imaging at 1.5 T. Magn Reson Med 1986; 3:649-662.
3. ihulbom KR. Waterton JC, Matthewx PM. Radda G. Ox$CMtion dependence of the transverse relaxation time on water pmtons in whole Mwd at high fields, Biochem Eiophys Acta 1982: 714265-270.
4. Hausicr R, Nasck F. I(crmagnstische relaxation und korciation ion systcm wasynaumtoff. Zeii FNaiwf1965; 20:1668-1675.
5. Krynicki K. Proton spin-iattia relaxation in pure water bstwecn O'and 100" C. Phyiivs 1966; 32167-173.
6. Horikawa Y, Nawc S, Tanaka C, Hirakawa H, NSkawa H. Proton N M R relaxation in ischemic brain edema. Siroke 1986; 171 149-1 152.
7. Shah SS. Rande SS, Phadke RS, W u r i SR. Significance ofwafer proton spin-iattia relaxation times in normal and malignant tissuaand their subnllvlar fraaions: Pan I and 2. Magn Reson Imaging 1982: I: 91-104.
8. Bloch P. The influence of hydrogen peroxide on the TI and T2 of water pmtons. Procmdings of thc Radiation Research Saiq, 35th An- nual Mcning, Atlanta, Georgia, 1987.
9. Gore JC, Brown MS, Mizumoto CT, Annilage IM. Influence of glycogen on water pmton relaxation times. Magn Reson Med 1986; 5 463-466.
IO. Beail PA, Haziewwd CF, Rao PN. Nuclear magnaic resonance
patterns of intradlular water as a function of H e L ail cycle. Science 1976; 192:904-907. I I. Hollis DP, Saryan LA, EBskston PA, Moms HP. Nuclear ma~netic
-nam studies of cancer wrrlationship among spin-ipnia &tion tima, grourth rate, and water mntent of Monis hepatomis. JNal Cancer Inri 197% 541469-1472.
12. Krwker RM, stewvt O., Bronskill MJ, Hcnkelman RM. Con- tinuous distributions of NMR nla?ation tima applied to tumors bcfore and after therapy with x-rays and cyclophosphamide. Magn Reson Med 1988: 624-36.
13. Maris JM, Chance B. Magnetic resonance spscimwpy of nM- olarms. In: Krcnel HY, ed. Magnetic Resonance Annual. New York &ven, 1986; 213-235.
14. Glickson JD. Evanochko WT. Sakai Ti. NP TC. In vivo nmr ~prrUmop, oftumon. in: ~ u p t a R1, cd. NMR spcMaropy ofcciis and Organism% Boca Raton: CRC Reps. 1987: 99-134.
15. Gnffiths JR. Suverns AN, llles RA. Gordon RE, Shaw D. "P NMR investigation of d i d tumors in thc living rat. Biok-I Rep 1982: 2719-725.
16. Schiffer LM. Braunrhweipr PG,Glickeron JD. Evanochko WT. Ng TC. Reliminuy observations on thc codation ofpdifnative phr- nomena with in vivo "P NMR spmmscop) añcr tumor chcmotherap) Ann Ni' AcadSci 1986: 158270-276.
17. Sostman HD. A m i y IM. Firher JJ. NMR in cancer. high molution spxmxopy in tumon M a n Reson /mag 1984; 2265-278.
18. Cohcn JS. Phospholipid and cnerg) melabolkm of cancer cells monitored by "P magncuc mnanrc rpcuoocopy: Poasiblc clinical Yo. nihcana. Muw Clin Pmc 1988,631 199-1207.
19. Okunicff P. Ramuy J. Tokuhiro T. Hiuig B n al. Estimation of tumor or)gcnaiioa and metabolic rate using "P MRS: Comlaiion of longitudinal relaxation mth tumor grovth rate and DNA synthesis. Ini J Radia Onwl &o1 Phys 1988 141 18s-I 195.
20. Ng TC. Major AW. Mcancy TF, Thomas FJ. "P MRS nudy of humantumon in~n r t o r ad i auon thcmpyunnga 1.5TMRlsyjtcm. SMRM Absir 1986, 516.
21. Semmln W, Gadcmann G. von Kaick. Zabel HJ, Lorenz W. I n vivo "P specmxopy of human tumors and their m n s c to therapy usinpa 1.5 Tnla wholc body scanncr. S.WRM Abur 1986; 39.
22. Niedcckn AC. Muller S. AYC WP ei ai Earnmiry bone Iumors: Evaluation by "P MR spnrce~opy. Radiology 198% 157167-174.
23. Balcnau D. Arnold DA. Segebartb C. Luytcn PR. den Hollander JA. PJ' MR evaluauon of human brain respanu to therapy. SMRM Absrr IY86; 41.
24. Ros B. Helsper JT. Cox J. Young I, Kcmpf R. htmsarroma and othcr nmpiasms of bnc: Magnnic resonance spcclmmpy Io mon- nor therapy. Arch Su@ 1987; 1221464-1468.
25. Solak CH. F m a n DM. Monitoring lactic x i d production in mted failw~ngthcmmulatedcchospaualloaliraDonucbNquc. Rcvnled at thc Sociny of Magnnic Rmnancc in Medicine. 61h Annual Mming New York New York. 1987.

Sexual Behavior, Venereal Diseases, Hygiene Practices, and Invasive Cervical Cancer in a High-Risk Population
ROLAND0 HERRERO, MD,'.t LOUISE A. BRINTON. PHD.t WILLIAM C. REEVES, MD.* MARIA M. BRENES. ES.* FRANCISCO TENORIO, MD.5 ROSA C. DE BRITTON. MD.11 EDUARDO GAITAN. MD.7 MARlANA GARCIA, MS.* AND WILLIAM E. RAWLS. MD#
A case-eontrol study of 759 women with Lvasive cervical cancer and 1430 controls in four Latin American countries evaluated risk in relation to sexma1 behavior, histories of speck venereal diseases, and hygiene practices. Early age at first sexual iatercoune and increasing number uf sexual partners were associated with significantly incrmsed risk even miter adjustment for their mutual effects. Risk iirrawd to a twofold excess among women repwtiq first intercourse at 14 to IS years of age conpied with M+ yeus. The number of steady sexual pibcrs was a more important prediietor of risk thin the number 01 nonsteady partners, puticuiarly hefore age 30, pnssihly reflecting the need for prolunged or repeated exposum to a tnnsmissibk agent, a düierent methods of protfftioa against s e x d l y tnosmined d i v w s or pregnancy. Reported frequency of intercourse w a s not generally associated with risk, except among women reporting incread frequencies before 20 years of age. Histonca of gonorrhea or crab lice we* ns.wxhted with increased risk, but hist& ofutber venereal di- were not signifinat predictors. No consistently increased risks were detected for women reporting specifir hygiene or douching habits, except the practice of washing the genitalia inhcquently during menstruation. These results provide support for a period of incrmsed susceptibility to areinogena during adolescence, and suggest that this my be an importiat determinant of the high iacikaee of cervical cancer in Latin America.
Cancer 65:380-386,1990.
HE CAUSE of invasive cervical cancer has been the T subject of numerous studies over the last 50 years. However, most of the epidemiologic research has been done in developed countries where cervical cancer inci- dence has declined significantly in the last three decades.' Latin America is still a high-risk area for invasive cervical cancer? but few studies have analyzed the role of specific factors in this region.34
SupponedinpanbymntrpetNOICP41026andgrantROICA-42042 from the National Cancer Institute, National Institutes of Health, and by a grant from the National Canar Institute of Canada.
Unidad Nacional de Canamlogin. Caja CoJtamcens de %uro Social, San Josc, Costa Ria.
t Environmental Epidemiology Branch, National Canar Institute, Bethexin. Miryhnd.
#Gorga# Memod Laboratory. Panama City. Republic of Panama. $Hospital de Oncdogji Nacional, Instituto Mexicano de Scguridad
I Instituto Oncologico Nacional. Panama, Republics de Panama. 1 Division de Epidemiolosia. Instituto Nacional de Canmlwa. L b
pth Colombia. Y Mokcular Vimlw and Immunolw. Dewment of Pathology,
Mc Master Uniwnity, Hamilton, Ontario. Can& A d d m for reprint% Rolando Hemm, MD. Environmental €pide-
mbkw B~-acsh N i i i o d C a m Institute. Exenitiw ñ u Nonh. Room 443, Buhedi. MD 20892.
Amp<ed for puMition July 14. 1989.
Social. Mexico Cily, Mexico.
Cervical cancer may represent a late sequela of a sexually transmitted disease>' and early age at first sexual inter- course, increasing number of sexual partners, low socio- economic status, and nonparticipation in screening pro- grams are established risk factors? Other suggested facton include number of pregnancies?" smoking,".'2 histones of specific venereal diseasesi3 use of oral contra~eptives,'~ and the male partner's sexual
In a previous analysis o f the same study population 10 be described in this article.I8 we noted a strong relation between human papillomavirus (HPV) types 16/18 and risk of cervical cancer, but the Occurrence of viral DNA was not associated with sexual behavior. This unexpected finding, which suggests an effect of sexual practices in- dependent of infection or measurement of this specific virus, renewed our interest in the relation of sexual activity to risk, particularly with respect to possible modes Of
transmission of infectious agents. Venereal diseases have been associated with risk ofcer-
vical cancer?" but no specific infection transmitted ve- nereally has been identified consistently as a causal agent. In addition, the possible role of personal hygiene in tho cause of cervical cancer has been s~ggested,~ but Ud available studies yield contradictory results.
380

*,. ,
. r-.
... c
I -._
c-
.-. ,
L..
c
L
._-
I
c
.... c
...- r"
.". F-
4lY er- 'lo-
D r s b i . , 4 r 1
- ! to 1
on- i nd ; 4ACI i .ed- i in- fic -- ity of'-'
er- ve- - nt. beC.
ies '
3,
3,
-..
he- L. I j
- :
No. 2 CERVICAL CANCER IN LATIN AMERICA Herrero et ai. 38 I
To determine the reasons for the h@ incidence of cer- vical cancer in Latin America, with emphasis on sexual characteristics, we conducted a case-control study in four countries. We obtained detailed information on past and current sexual behavior. hygiene practices, tobacco and alcohol exposure, medical, reproductive, and screening history, and presence of HPV DNA as measured by in situ hybridization studies of ceMcal samples.
Materials and Methods
Newly diagnosed cases of invasive cervical cancer were ascertained before treatment in four Latin American study sites: Bogota, Colombia; Costa Rica; Mexico City, Mexico: and Panama between January 1986 and June 1987. Eli- gible patients were younger than 70 years of age and had lived in the study area for at least 6 months. The six study hospitals were the major cancer treatment centers in the study sites.
in Bogota and Mexico City, two age-matched (5-year groups) hospital controls were selected for each case; in Costa Rica and Panama, one hospital and one community control were chosen. Potential controls with a hysterec- tomy or history of cancer were replaced. Hospital controls were selected randomly from admission lists excluding patients with neoplastic, endocrine, nutritional, psychi- atric, selected circulatory, gynecologic, or smoking-related diagnoses. In Costa Rica and Panama, hospital controls were selected from inpatients at the primary referral hos- pitals that served patient areas of residency. In Bogota, they were chosen from eight tertiary level government hospitals and in Mexico City from three social security hospitals serving the population from which the patients were derived. Community controls were selected ran- domly from current census listings of the corresponding patient counties of residency. Eligible controls who refused to participate were not replaced.
A personal interview, lasting an average of 60 minutes, was conducted with each participant to obtain detailed information on demographic, socioeconomic, reproduc- tive, occupational, and medical history, as well as dietary, sexual. hygienic, and contraceptive practices. Interviewers who were trained uniformly under strict supervision ad- ministered the questionnaire in private settings.
During the 18-month study period, 766 eligible patients were identified and an interview was obtained from 759 patients (99.1%). Of 1532 eligible hospital controls, 1467 were interviewed (95.8%). Nonresponse among patients and controls was due to death (three patients, zero con- trols), refusal (zero patients, 41 controls), language and hearing problems (two patients, ten controls), mental in- competence (one patient, eight controls), and change of residency (one patient, six controls). Histologic infor- mation was available for 728 patients (96%). of whom
92% had squamous carcinomas and 8% had adcnocarci- nomas. Thirty-seven (2.5%) controls reported no prcv¡ous sexual experience. compared with zero patients. The 37 virgin controls were excluded from analysis in order to adjust simultaneously for number of sexual partners and age at first intercourse. The final group consisted of 759 patients and 1430 controls.
To assess the presence of HPV, a ceMcal swab was obtained from 755 patients (99.6%) and 1325 controls (95.4%). We used cotton tipped applicators to collect cell samples from the neoplastic lesion (patients) and the cer- vical os (controls). Swabs were eluted in phosphate buf- fered saline, frozen as soon as possible, and maintained at -2OOC until tested. Assays were conducted by the filter in situ hybridization method as reported in detail else- where.'* All autoradiographs were studied independently by three observers blinded to case-control status, and specimens that were recorded as positive by at least two observers were considered positive.
To estimate the risk of invasive cervical cancer asso- ciated with various factors, odds ratios were calculated as approximations of relative risks (RR). Unconditional le- gistic regression was used to adjust for potential con- founding variables," deriving maximum likelihood esti- mates of RR and 95% confidence intervals (CI). Tests for trends in the logistic analyses were obtained by categoriz- ing the exposure variable and treating the scored variable as continuous. The results of conditional logistic regressionz2 were similar to the unconditional analysis, and the latter have been chosen for ease of presentation.
Results
Patients and controls were similar regarding age, race, and religion. The mean age was 46.5 years for both pa- tients and controls. Most of the participants were mestizos (65.7% of patients, 64.9% of controls) or white (30% of patients, 29.8% of controls), and Catholic (87.1% of the patients, 89.4% of controls). No major differences were seen by calculating the RR with the use of only hospital or community controls; therefore, both types of controls were combined in the analysis.
Apart from the sexual variables, the most important risk factors identified in the current study were the fol- lowing (Table I): detection of HPV types 16/18 DNA, increasing interval since last Pap smear, increasing num- ber of pregnancies, and a smaller number of household fadities (the socioeconomic status estimator related most strongly to risk in this study). interval since last Pap test, number of pregnancies, and socioeconomic status were correlated with the sexual behavior variables and exerted confounding effects. The occurrence of HPV DNA, al- though associated with the highest relative risk, was not correlated with sexual behavior and, when included in
1 't
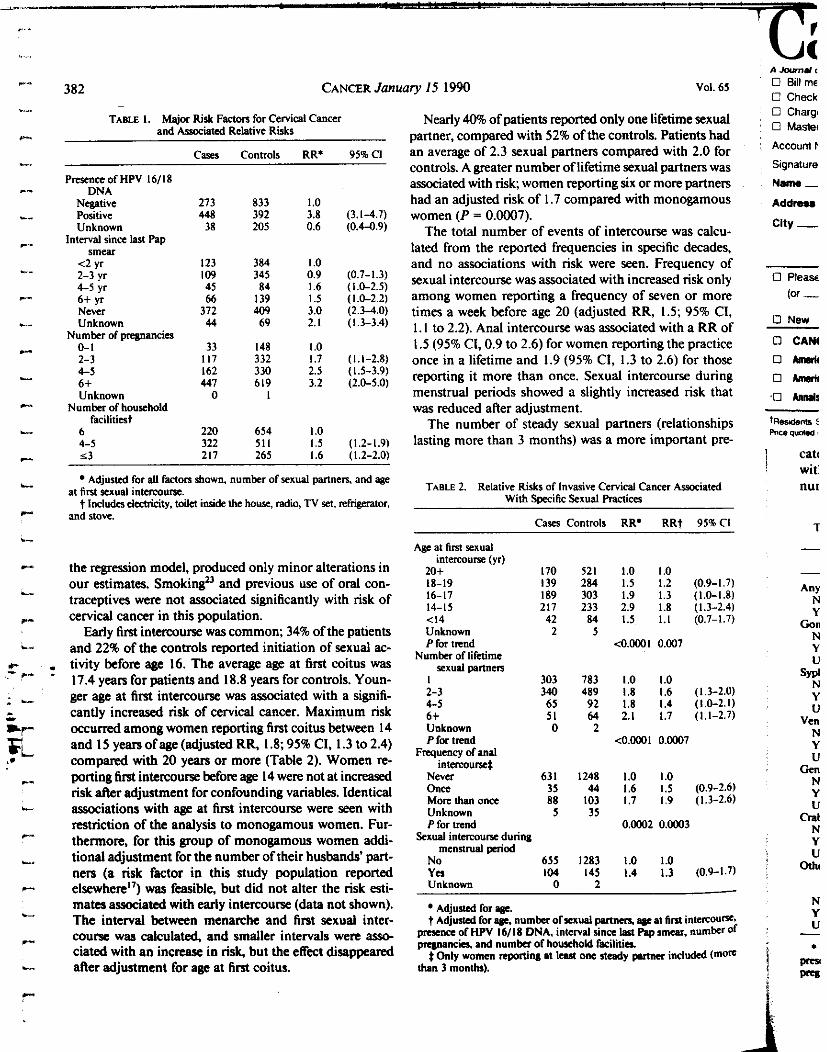
382 CANCER Jam
TABLE I, Major Risk Factors for Cervical Cancer and Awciated Relative Risks
CWS
PresenceofHPV 16/18 DNA
Negative Positive Unknown
smear interval sinn last Pap
<2 yr 2-3 yr 4-5 yr 6 f yr Never Unknown
273 448 38
123 109 45 66
372 44
Controls RR* 958C1
833 1.0 392 3.8 (3.1-4.7) 205 0.6 (0.44.9)
384 I .o 345 0.9 (0.7-1.3) 84 1.6 (1.0-2.5)
I39 1.5 (1.0-2.2) 409 3.0 (2.3-4.0) 69 2.1 (1.3-3.4)
Number of pregnancies 0-1 33 148 I .o 2-3 I I7 332 1.7 (1.1-2.8) 4-5 I62 330 2.5 (1.5-39) 6f 447 619 3.2 (2.0-5.0) Unknown O I
Numbn of household facilitiat
6 220 654 1.0 4-5 322 511 1.5 (1.2-1.9) s3 217 265 I .6 I I .2-2.0)
aty I5 1990 Vol. 65
Nearly 4090 of patients reported only one lifetime sexual partner, compared with 52% of the controls. Patients had an average of 2.3 sexual partners compared with 2.0 for controls. A water number oflifetime sexual partners was associated with risk; women reporting six or more partners had an adjusted risk of 1.7 compared with monogamous women (P = 0.0007).
The total number of events of intercourse was calcu- lated from the reported frequencies in specific decades, and no associations with risk were seen. Frequency of sexual intercourse was associated with increased risk only among women reporting a frequency of seven or more times a week before age 20 (adjusted RR, 1.5; 95% CI, 1. I to 2.2). Anal intercourse was associated with a RR of 1.5 (95% CI, 0.9 to 2.6) for women reporting the practice once in a lifetime and 1.9 (95% CI, 1.3 to 2.6) for those reporting it more than once. Sexual intercourse during menstrual periods showed a slightly increased risk that was reduced after adjustment.
The number of steady sexual partners (relationships lasting more than 3 months) was a more important pre-
Adjusted for all fadors shown. number of sexual partners, and age
t Includeselafnaty. toikt inside the how, radio, TV XI, refrigerator, at first sexual intncoune.
and stove.
TABLE 2. Relative Risks o í Invasive Cervical Cancer A~ocialed With Specific Scrual Practices
Cases Controls RR* RRt 954bCl
the regresion model, produced only minor alterations in our estimates. Smoking” and previous use of oral con- traceptives were not associated significantly with risk of cervical cancer in this population.
Early first intercourse was common; 34% of the patients and 22% of the controls reported initiation of sexual ac- . tivity before age 16. The average age at first coitus was
* 17.4 years for patients and 18.8 years for controls. Youn- ger age at first intercourse was associated with a signifi- cantly increased risk of cervical cancer. Maximum risk occurred among women reporting first coitus between 14 and I5 yearsofage(adjusted RR, 1.8; 95% C1,l.3 to 2.4) compared with 20 years or more (Table 2). Women re- porting first intercourse before age 14 were not at increased risk after adjustment for confounding variables. Identical associations with age at first intercourse were seen with restriction of the analysis to monogamous women. Fur- thermore, for thio group of monogamous women addi- tional adjustment for the number of their husbands’ part- ners (a risk factor in this study population reported elsewhere”) was feasihle, but did not alter the risk esti- mates associated with early intercourse (data not shown). The interval between menarche and first sexuai inter- course was calculated, and smaller intervals were aso- ciated with an increase in risk, but the effect disappeared afier adjustment for age at fint coitus.
Age at first sexual internurse (yr)
20+ 170 521 1.0 1.0 18-19 139 284 1.5 1.2 (0.9-1.7) 16-17 189 303 1.9 1.3 (1.0-1.8) 14-15 217 233 2.9 1.8 (1.3-2.4) <I4 42 84 1.5 1.1 (0.7-1.7) Unknown 2 5 P for trend <0.0001 0.007
Numbn oilifelime P X U ~ p r i n r n
I 303 783 1.0 1.0 2-3 340 489 1.8 1.6 (1.3-2.0) 4-5 65 92 1.8 1.4 íl.0-2.1) 6+ S I 64 2.1 1.7 (1.1-2.7) Unknown O 2 P for trend <0.0001 0.0007
Frequency of anal internunet
Never 631 1248 1.0 1.0 Once 35 44 1.6 1.5 (0.9-2.6) More than once 88 103 1.7 1.9 (1.3-2.6) Unknown 5 35 P for trend 0.0002 0.0003
Sexual intmOurx during mennnial period
No 655 1283 1.0 1.0 Y a 104 145 1.4 1.3 (0.9-1.7) Unknown O 2
Adjuued for v. t Adjwted for p~c. number o i x r u i l partners, age al hrn intercou*~
prrrenx of HPV 16/18 DNA. inlerval J i n a lp<l Pap smear, number Of Prcyinck and number of household facilitia
t Only women reunting at leut one study pltnn included (morn than 3 monthah
A*#‘ O Billms C Check O Chargt O Masiei
Account P
Signature
Nanw - Addmu
city -
o p l e ~
(M - O New
o CAW
O A n r k
ohmfil 0 h n * S

No. 2 CERVICAL CANCER IN LATIN AMERICA - Herrero et al. 383
TABLE 3. Rditivc Risks* of Invasive Cmrpl Cinar Accordin8 10 Number of Stcsdv and N o n n d v Sexual Rnnen
Nonsteady sexual panncn Steady uaud
mnnen O 1-2 z 3
I I .o 1.2 I .4
2 l.7t 1.5 1 . 1 (3031783) (84175) (25/41)
Numbers in parentheses are caxs/mntmls (unknowns excluded). Adjusted for age, age at finl internurse, pmence of HPV 16/18
DNA, intmal Pna kt Pap smear, number of pregnancies. and number of household facilities.
t 95% CI = 1.3-2.3. t9S%Cl = 1.5-3.0. 695% CI = 1.0-3.8.
dictor of risk than the number of nonsteady partners (Ta- ble 3). Risk increased with the number of steady partners in each category of nonsteady partners. However, for each category of steady sexual partners the risk did not rise with a greater number of nonsteady partners. The total number of sexual partners at specific decades of life was
TABLF 4 Relatwc Risks oflnvavvc Cervical Cancer Associated
- With Histoncr of Specific VcncMJ D8-s
Cases Controls RR*
Any venereal di-
Gonorrhea
N o Yes
N o Yes Unknown
Syphilis N o Yes Unknown
Venereal warn N o YCS Unknown
GeniIal herpes N o YCS Unknown
Crab lice N o YCS Unknown
Other venereal di- ( n o n wec i fi ed)
N o Y a
676 1333 I .o 83 97 I .8
727 1408 I .o 30 18 3.3 2 4
743 1407 I .o 15 21 I .3
I 2
745 1392 I .o 13 36 0.9
I 2
730 1405 I .o 28 23 2.2
I 2
744 1415 1 .o 12 13 1.4 2 7 Unknown - -
95% CI
(1.2-2.5)
(1.7-6.4)
(0.6-2.7)
(0.5-1.8)
(0.1-6.5)
( 1 , 2 4 2 )
(0.6-3.5) __
Adjusted for age, number of sexual partners, age at lint intmourse, pmence of HPV 16/18 DNA, interval Pna last Pap smear, number of presnancics and number of household facilities.
not related to risk, but a greater number of sieady patiners before age 30 was associated with increasing risk (data not shown).
The risk assOciated with having had a venereal disease was 1.8 (95% CI, 1.2 to 2.5) (Table 4). The two specific diseases ass0ciaied with risk were gonorrhea (adjusted RR, 3.3) and crab lice (RR, 2.2). A history of these two diseases was approximately ten times more common among women with six or more sexual partners than among mo- nogamous women. Histories of syphilis, genital warts, herpes, and other (unspecified) venereal diseases were not associated with significant increases in risk among the few women reporting these diseases. Women reporting a his- tory of more than one venereal disease were at the same risk as those reporting only one.
A slightly increased risk was associated with bathing less than once a day (Table 5). An increased risk (RR, I .7; 95% CI, I . I to 2.6) was noted for women who washed their genitals more than twice a day. In contrast, women reporting frequent washing of their genitals during men-
TmL f 5 Relative Risks of Invsslve Cenical Cancer Associated With Spccihc Hygunc Practices
Cases Controls RR' 95% CI
Bathing z once a day <once aday Unknown
Frequency of washing genital areat
Never 5 once a day Twice a day > twice a day Unknown P for trend
Frequency of washing pnital area during menstmal period
<once a week 1-7 t ima a week > once a day Unknown P for trend
Use of sanitary napkins during menstm- ation
N o Yes Unknown
Use oftampons during menstruation
N o Y a
534 225
O
20 I 343 I45 70 O
95 190 474
O
308 450
1
745 13
I
1114 315
I
47 I 627 248
80 4
139 293 997
I
508 92 1
I
1392 31
I
I .o 1.3
I .o 1 . 1 1 . 1 I .7
0.04
1.0 0.9 0.6
O.wO7
I .o I .o
I .o 0.9
(1.0-1.6)
(0.9-1.5) (0.8-1.5) (1.1-2.6)
(0.6-1.3) (0.5-0.9)
(0.8-1.3)
Unknown (0.5-1.9)
AdjUaed for age, number of sexual parinera, age at ñnl intercourse, pmence ofHPV 16/18 DNA, interval piace last Pap smear, number of pregnancies and number of household facilities.
t Separate occasions from gmeral bathing.

384 CANCER January I5 1990 Vol. 65
stnial periods were at significantly decreased risk. Those women reporting this practice more than once a day had an adjusted RR of 0.6 (95% Ci, 0.5 to 0.9) compared with less than once a week. No particular feminine hygiene product used during menstrual periods was assoCiated with risk, including tampons, sanitary napkins, cloths, and various other products.
A marg¡nally significant 40% risk was seen for women reporting regular use of vaginal douches for 2 months or more compared with women who did not douche, but there were no consistent trends for age at initiation, fre- quency, or duration of douching (Table 6).
Di s eu s s i o n
in concordance with the notion that coitus is a prereq- uisite for the development of cervical carcinoma, none of the patients reported themselves as virgins, compared with 2.5% of age-matched controls. Early age at first sexual intercourse was associated with increased risk of invasive cervical cancer, independent of number of sexual partners and other confounding factors. The highest risks were seen among women reporting first intercourse at ages 14 and 15, whereas those who initiated sexual activity before 14
TABLE 6. Relative Risks of Invasive Cervical Cancer Associated - With Douching Practices
CaseS
U r of vaginal douche for 2 months or more
Never used 513
Regularly I14
Never used 513 231 29 21-30 55 <21 29 Unknown I P for trend
Never u x d SI3 <I a w k 14 1-2 a w k 38 >2 a week 51 Unknown I P for iwnd
Never used 513 S I 2 43
Not regularly 131
Agc nvtcd using?
Frequency of use?
Months of regular u s ?
Controls RR’
960 I .o 270 1.1 198 I .4
960 I .o 54 I .3 80 I .8 63 I .o
I 0.31
960 I .o 40 1.8 86 1.1 71 1.6
I 0.04
960 1.0 55 1.7
95% CI ___
(0.8-1.5) (I. 1-1.9)
(0.8-2.3) (I .2-2.8) (0.6-1.6)
(1.0-3.3) (0.7-1.8) (I .0-2.4)
KI 20 38 59 1.7 (1.0-2.7) 121-240 23 40 1.5 (1.0-2.7) a240 10 40 0.7 (0.8-2.8) Unknown O 4 (0.3-1.4)
KI 20 121-240 a240 Unknown
38 59 1.7 (1.0-2.7) 23 40 1.5 (1.0-2.7) 10 40 0.7 (0.8-2.8) O 4 (0.3-1.4)
P for trend 0.35
Adjwcd (or .A n u m b oíxaud pnnm, a8c at ñni inicrmursc. prcsnce of HPV 16/18 DNA, inmil since laü Plp smear, numba of prrlnmnciea 8nd number of household frilitia
t Nonmguh usn cacludcd.
years of age were not at increased risk. This finding may be a reflection of social or behavioral charactexistics of this group of early starters, which we were not able to determine.
Most epidemiologic studies of cervical cancer have re- ported increased risk for women who initiated sexual ac- tivity during adolescence?c28 and it has been hypothe- sized that the adolescent cervix is particularly susceptible to the effect of coitwrelated carcinogens?9sM Areas of atypical metaplasia are seen among sexually active ado- lescents more often than among virgins.” However, it is not clear if the effect of age at first intercourse is due to a particular vulnerability of the young cervix or to the fact that women who start sexual activity earlier have longer exposure to coitus-related in an attempt to evaluate this issue, risks were considered in relation to age at diagnosis and latency periods. To the extent that such an analysis was possible in an age-matched study, we found no evidence of an effect of longer exposures that could explain the association with age at first intercourse, and the effect of the latter was evident regardless of age at diagnosis.
Number of lifetime sexual partners was associated with a significant trend of increasing risk, with women who reported six or more partners having an adjusted RR of 1.7 compared with monogamous women. However, risk was elevated for 2 to 3 partners, primarily reflecting a difference between monogamous women and nonmon- ogamous women. This finding is in agreement with other report^,^'*"-'^ and has been interpreted as evidence for an important role of sexually transmitted agents. Two previous studies of preinvasive and invasive cervical neo- plasia did not show an independent effect of early inter- course after adjustment for number ofsexual partne13.”5.’~ However, two recent studies showed that independent ef- fects of both factors do Our results support independent effects of early ages at first intercourse and numerous sexual partners.
The number of steady partners (relationships lasting more than 3 months) dated more to risk than the number of nonsteady partners, and this effect was more apparent for the persons who had multiple steady partners at young ages. Possible explanations for this finding include the need for more pmlongd or repeatad exposure to a partner who carries a transmissible agent. Alternatively, it could be related to more frequent use. of condoms with non- steady rather than steady partners, as suggested by a recent study of the transmission of human immunodeficiencY virus (HIV).* Although we found that use of condoms was associated with a slight reduction in risk and that usage was more frapuent among women with nonstdy partners, this did not explain the difference in effect be- tween steady and nonsteady partnea AdditiOndlY, we studied whether differential use. of other methods Of con-
No.
tmc rest m wit1
F
rele and inte rep<
S
to c infe infe mis pen thai plai mis onl: sub for
C
rese
por
pro!
gen
epit trar o f t fon HOT effe for the üth, the¡
S the Am ass< WiLl
rep Pro
Cral like
I rela SOCi
Prai
re01
it p
i gen
1 gen
i

.-_- , ..I^-
c -
. .. No. 2 CERVICAL CANCER IN LATIN AMERICA * Herrero el al. 385
trsception or ftepuency of intercourse could explain the results, but then remained a stronger effect of steady partnm. A recent studylo also failed to find an assoCiation with nonsteady partners.
Frequency of intercourse has been studied by several -hers, most of whom have concluded that it is not relevant to risk of cervical ~ a n c e r . ~ ~ . ~ ~ , ~ ~ ~ ~ ~ in this study, and in concordance with other authors,"" frequency of intercourse was a significant risk factor only for women reporting frequent intercourse before age 20, again sup porting the hypothesis of a vulnerable period.
Several possible carcinogenic mechanisms have been proposed to explain the relation of risk of cervical cancer to coital factors. The one that is accepted most is that an infectious agent, possibly HPV, is transmitted from an infected male to his partner. Under this premise, iftrans- mission occurs with a single exposure, we would not ex- pect the number of steady partners to be more important than total number of sexual partners. An alternative ex- planation is that the infectious agent is not always trans- misible, because of cyclic shedding, and is transmitted only after repeated exposure. A recent study on female subjects" suggests that there is such a cyclic pattern for HPV.
Other hypotheses consider the possibility of carcino- genic constituents of the human semen; it has been sug- gested that basic proteins from human semen can alter epithelial and subepithelial cells and induce neoplastic transformation.4 A recent study showed that protamine of human and animal origin produces neoplastic trans- formation of human cervical epithelial cells in v i m . 4 7 However, the general lack of evidence in regard to an effect of frequency of intercourse provides little support for this mechanism. The evidence of increased risk with the practice of anal intercourse may be a reflection of other aspects related to sexual behavior of the women or their partners, or to hygiene practices.
Specific venereal diseases are usually correlated with the incidence and mortality From cervical cancer! in Latin America, gonorrhea and crab lice were the two diseases associated with cervical cancer, whereas herpes, genital warts, and syphilis were not related, although few women reported these diseases. No specific mechanisms have been Proposed for a direct carcinogenic effect ofgonorrhea and it probably represents general venereal exposure, as do crab lice. In addition, these two diseases are probably most likely to be remembered by patients.
It has been suggested that hygiene practices may be related to risk of cervical cancer:' but no consistent as- sociations with risk have been established for specific practices!'" In our study, the frequency of washing the genitals was associated with increasing risk, which may reflect inrreased sexual activity. Frequent washing of the gental area during menstrual periods, however, was as-
sociated with reduced risk. in concordance with other studia,I0 the type of feminine hygiene products used dur- ing menstrual penods was not associated specifically with risk.
Vaginal douching, which alters the vaginal milieuzb or causes initation," has long been reported as a risk factor for cervical cancer.u A recent study did not find any re- lation,1° whereas another showed i n d n g risk with fre- quency and duration of use of various douching prepa- rations, excluding water or vinegar." The current study does not show any consistent associations of douching practices with risk of invasive cervical cancer.
The participation rates in this study were almost loogb for both patients and controls. Although questions arise regarding recall biases assoCiated with.the sexual variables, the correlation of number of sexual partners with reported histories of venereal diseases provided an indirect form of validation. Furthermore, the interviewers were in- structed to stress the confidentiality of the information and to administer the interviews in an appropriate setting.
in conclusion, age at first sexual intercourse and num- ber of steady sexual partners exerted independent effects on risk of cervical cancer. The high incidence of cervical cancer in Latin America is probably influenced by the lack of adequate cytologic screening programs and the high prevalence of early sexual activity. This factor may also explain partially the high incidence ofcervical cancer in low Socioeconomic groups in developed countries, as suggested by a recent study!9 Furthermore, effects with the number of constant sexual partners before 30 years of age and frequent intercourse at early ages suggest in- creased susceptibility of the cervix during adolescence, and emphasize the need for additional research on the means of transmission of putative causal agents.
REFERENCES 1. Lkvesa SS. DaCnPtive epidemiology of canm of the uterine anix.
Obstefrics and Gynerdogy 1984; 63605412. 2. Restrepo HE, Gonzalw 1. RobeN E, Litvak J. Epidcmiologia y
mntml del cancer del cuello uterino en America iatina y el Caribe. Bo/ OfSanif Panam 1987; 102578-593.
3. Z u l w L. Cancer de ceMx y w faom de riq+: Ea\udio de cpy>s y mnmla. Rev Colombiana Obsrer Ginad 1982; 23:219-232.
4. Carreras O. Algunos aspectos egidcmiologicos del &noma cer- vimutcnno. R e Cuhna Obsrei Ginmd 1981; 7:376-383.
5. Reeves WC, Brena MM, LkBritton RC, Valdes PF, ioplin CFB. Cervical Cancer in the Republic of Panama. Am J Epidemid 1984; I19 7 14-724.
6. Duque E, Cuello C, Aristirabal N, Haenvel W, ñotero S, Coma P. PIcmaliiant lesions of the in women of Cali, Colombia. J Nod Cancer Ins1 1979; 63953-963.
1. KcJJler 11. Human aMcal canar as a venereal di-. Cancer Res 1976: 36783-791.
8. Beral V. Cancer of the cervix: A sexually transmitted infection? Lnncel 1974: 1:1037-1040.
9. Brinton LA, Fraumeni JF. Epidemiology of uterine ces-vkd -. JChron Dis 1986: 391051-1065.
IO. Brinton LA, Hamman RF, Huagins GR n al. Sexual and repro ductive risk fnctors for invasive squamous all cmical eamer. 3 Nafl Cancer Ins1 1987; 7923-30.

386 CANCER January IS 1990 Vol. 65
I I . Winkebtan W.CigarrttcsmoLingandcanceroftheutrrinecervix. BanbwyRep 1986; 23329-341. 12. World Health O~nizationllnternational Agency for Research
on Cancer. Epdemiological studies of cancer in humans. In: IARC Monograph on the Evaluation of the Carcinogenic Risk of Chemic& to Humans Tobaao Smoking. Lyon. France: International Agency for Rexarch on Cancer, 1986; 199-308. 13. Fcncglio CM, Fcrenny A. Etiologic factors in cervical neoplasia.
Semin Onml1982: 9349-372. 14. Piper JM. Oral contraceptiva and cervical cancer. Gynecol Onml
1985; 22:l-14. 15. ' Lunzunegui MV, King MC, Coria CF, Charlet J. Male influenas
on cervical canal risk. Am J Epidemiol 1986; 123:302-307. 16. Buckley JD, Harris RW, Doll R, Vesey MP. Williams FT. Case-
control study ofthe husbands ofwomen with dysplasia or carcinoma of the cervix uteri. Lancer 1981; 21010-1014. 17. Brinton LA. Reeves WC, Brenes MM el al. The male factor in
the etiology ofcervical cancer among sexually monogamous women. Int J Cancer 1989: M199-203. 18. Reeves WC, Brinton LA, Garcia M et al. Human papillomavirus
infection and cervical cancer in Latin America. N Engl J Med 1989 320143741 19. Guijon FB. Pnnskevas M, BNnham R. The arsociation of vxually
transmitted d- with cnvical intraepithelial neoplasia: A caScontrol study. Am JObsler Gynecd 1985; 151:185-190. 20. Jayant K. Notani PN, Gadre VV, Gulati SS, Shah PR. Personal
hygiene in groups with varied cervical cancer rates. Indian J Cancer 1987: 2447-52. 2 I. Breslow NE, Day NE. Statistical methods in cancer m a r c h The
analysis of cay«intml studies. IARC Monogr Eva1 Carcinog Risk Chem Hum 1980 1:192-246. 22. Lubin JH. A computer program for the analysis of matched case-
control studies. CompulBiomedRes 1981; 14138-143. 23. Herrero R. Brinton LA, Reeves WC el a/. Invasive cervical cancer
and smokingin Latin America. JNal1Cancer Ins1 1989 81:205-211. 24. Tems M, Wilson F, Smith H. Spring E, Nelson JH. The rela-
tionship ofcoitus to carcinoma o f the cervix. Am J Public Healrh 1967; 57840447. 25. Stewan HL. Dunham W, Casper J el a/. Epidemiology ofcancers
of uterine cervix and corpus, breast. and ovary in Israel and New York City. J Nail Cancer Inst 1966 37 1-95. 26. Graham S. Schotz W. Epidemiology of cancer of the cervix in
Buffalo, New York. J Nafl Cancer Inst 1979: 6323-27. 27. Fujimoto I, Nemoto H, Fukuda K, Masubuchi S, Masuhuchi K.
Epidemiologic study of carcinoma in siiu of the cervix. J Repmd Med 1985; 30535-540. 28. La Vnrhia C. Francerhi S, Decarli A n a/. Sexual factors, venercal
diseases, and the risk of intraepithelial and invasive cervical neoplasia. Cancer 1986; 58935-941. 29. Rotkin ID, Cameron JR. Clusters of variables influencing risk of
cervical cancer. Cancer 1968: 21:663-671.
30. Rotkin ID. Relation of adolescent coitus to cervical cancer risk.
3 I. Singer A. The uterine cervix from adolmnce to the menopause.
32. La Vecchia C. The epidemiology of cervical neoplasia. Biomed
JAMA 1962; 179486491,
Br Jobstel Gynaecol 1975; 8281-99. .~
Pharmacolher 1985; 39425433. 33. Marlin CE. Marital and coital facton in cervical cancer. Am J
Public H d I h 1967: 57803-814. 34. Tems M, Fítzpatrick W. Nelson JH. Comparative epidemiology
of inwive carcinoma of the cervix, carcinoma in situ. and cervical d y s plash. Am J Epidemiol 1980 112253-257.
35. Harris LW, Brinton LA, Cowdell R H el d. Chancteristicd of women with dysplasia or carcinoma in silu of the cervix uteri. Br J Cancer 1980 42359-369. 36. Herity B, Murphy IF. üaly L, Moriany MI. Studies of the epi-
demiology of preinvasive and invasive carcinoma of the uterine cervix in Ireland. I r Med J 1985; 78177-182. 37. dc GraaiT J, Stolte LAM, Janssens J. Marriage and childbeanng
in relation to cervical cancer. Eur J Obslel G y n d Reprcd Biol 1977: 7307-312. 38. Faill E, Simmons ME. Kamcert JB. Factors associated with ha
andlow riskofcervical neoplasia. JNalICancerImI 1981:6663l-á36. 39. Raves WC. Brinton LA, Brenes MM, Quiroz E, Rawls WE,
DcBritton RC. CaJe control study of cervical cancer in H m m Province, Republic of Panama. In1 J Cancer 198% 365560.
40. Centen for Disease Control. Antibcdy to human immunodeh- ciency virus in female prostitutes. MMWR 1987: 36157-161. 41. Rotkin ID. A comparison review of key epidemiological studies
in cervical cancer related to current m h e s for transmissible agents. CancerRes 197); 331353-1367. 42. Rotkin ID. Adolescent coitus and cervical cancer: Auociations
ofrelated events with increased risk. Cancer Res 1967: 27:603-617. 43. Peters RK, Thomas D, Hagan Do. Mack TM, Hendenon BE.
Risk factors for invasive cervical cancer among latinas and non-latinas in Los AngelesCounty. JNall Cancer Ins1 1986; 711063-1077. 44. Tems M, Oalmann MC. Carcinoma of the m i x : An epidemi-
ologicstudy. JAMA 1960: 174:1847-1851. 45. Reeves WC. Arwemena JR. Garcia M el al. Genital human pap
illomaviws infection in Panama City prostitutes. JInfecl Dis 1989: IM): 599-603. 46. Singer A, Reid BL, Coppleson M. A hypothesis: The role of a
high-risk male in the etiology of cervical carcinoma Am J Obsta Cynm/ 1976 126110-115. 47. French PW. Coppleson M. Reid EL. Effects of- protamine
on human cervical epithelial cells and BHK 21 cells in vitro. I R Sw Med 1987: 80434-437. 48. Smith FR. Etiologic factors in carcinoma of the cervix. Am J
Obstei Gynecol 1931; 21:18-25. 49. Mant D, Vessey M, Loudon N. Social clari differences in sexual
tehaviour and cervical cancer. Communily Med 1988: 1052-56.
Si rth Phil SW shoi to c The not
Si carb x 11 b e 9 a co title theii in tt whe auth ackr of 1k on a nghi plus
Tt mat1 and Stan relat iCuF lenh
c: Mar Amr LiPF BE& MD to tt editi con (UM plica
Fa shou whic nam and thesi by I: man tion! its fi
Mitomycin C Adjuvant Chemotherapy After Wertheim 's Hysterectomy for Stage IB Cervical Cancer
V. SIVANESARATNAM. MBBS. FRCOG. FICS. FACS,'t AND P. JAYALAKSHMI, MBBS. MPATH. MRCPATHSS
hhta undergoing dial a m g i d tre8tmeat for Stmgc IB d IU cervical arcloomi are i t hlgh risk of develop& I d rewrmce and/or dlitint metashses when ame M owre of the fobwing fxtors are present: pnsom of whseitk pelVic lymph Warr 8 we piimUy po.Vtb, full-tbklmu hlmol hdoa of the cervix, cllnially undetected PyimCMiI extensbo, iad Iymphitie/vueiihr chinael perwitloo in the cervix by hmDl cella. cireimmi oith cervix 8 p p M to be kbivisp iikc 8 systemic dirare. w o r e , syatemk wiaurea shnuld be mnsidmd its ther8py. The 8 i t h a report the ini(hl eXperknce 4 t h tbe use of mitomycin C M 8 sh#ie 8gent 8djuvMt in 16 patknta with is eudaomi of the cervix who had o o d ~ Wertheim ndK.l byaterectomy d were tbn&t to be in tbis high-tisk group. Fourteen of the patients in dlve and Ires of d h after duntiws of follov-irp mng¡ng from 16 to 38 months, the discisclrrc surVinl8t 8 medhn folh-up or 29 nwtb be¡llg 87.5%. @IC ptkd quucd di- tinuation of adjivnat chemotherapy b u s e of severe marrow toxidtr, hnwever, in view of the prrreaec of a multipk risk factors, pelvieimdIntloo WM glvea inatead. She dkd 13 molitb Inter from disseminited disease. A second pitieat died 6 moatha Inter from congestive ardir Idlure.
Cancer 64:r)8-800,1989.
ERTHEIM'S RADICAL HYSTERECTOMY is today an accepted method for the management of Stage IB
and early Stage IIA carcinoma of the ceMx. It is partic- ularly appropriate in the young patient in whom many years of ovarian and coital function can be preserved. However, then are a group of patients undergoing such therapy who might already have exirapelvic micrometas- tases and thus are at "high risk" of developing recurrences. These patients include those with a large primary tumor,l3 those with clinically undetected parametrial tumor exten- sion,' thost with lymphatic/vascular channel permeation in the ceMx,"' and those with histologic evidence of me- tsstases to peivic lymph nodes!.'
Although the use of adjuvant pelvic irradiation does decrease the incidence of local pelvic recurrence, the de- velopment of distant metastaJcs gives no imptovement in the overall survival." The use ofsysiemic adjuvant che- motherapy in this select group of high-risk cases thus a p pcars to be logical.
Fmm tbe Dcpr<mcnts of Wmetria and Gynvcolooy and Wa-
t Rofaoi. Had sad Senior Consulunt. o-. -lor M o t & ' V. Sivamuatnun, FRCOO. Fla FACS. Had
and Senia Conudmnl, Department of Oimmria id Gynwsolqy. F d i y of Medicine. Univemiiy of MiLm 59100 KWL Lumpur.
Accepted fo? publiation March 7, 1989.
thoiow. Fruhy of Medicine, Unimsity of M.Ly* KWL Lumpur.
798
This report describes our preliminary results with the use of mitomycin C as a single agent adjunct to surgery on the above high-risk cases.
Materids and Methods
Sixteen consecutive patients who had undergone a Weriheim radical hysterectomy at the University Hospital Kuala Lumpur, Malaysia, for Stage 1B carcinoma of the ceMx were found &r surgery to have one or more of ihe foUowiw high-risk f&om ( I ) metastatic pelvic nodes, (2) lymphatic/vascular channel permeation, (3) hill- thickness tumor invasion of the ceMx, and (4) micm ropic parametrial tumor extension. The pmperative evaluation of the patients included chest radiograph, in- travenous urography, and where neceSSary a cystoscopic examination. A full intraabdominal exploration was per- formed in all patients before commencement ofdefinitive surgery. None had palpably enlarged or suspicious para- aortic nodea The peritoneal washingc in all cases showed no malignant cells.
Chemotherapy was initiated between 7 and IO days &r surgery. Mitomycin C at a dosage of IS mum' was administered intravenously at intervals of 3 weeks for five course% Aü but one patient completed the scheduled bve course% The latter developed scvm marrow depression after two courses, making continuation of therapy inad-
No. 4
visable. stcad. WP;
smears, aminatie puted t<
Four cervix : (Table 15 o fü in dian tastases Histolc vadede V d but on' sion w Fou
dence These from 1 tient d had fL lymph pearec The o multii vasior i d l y vic nc them1 seven fusior 13 m( meta!
A I for I Pmsi sever these chao and a and 1 TI
Pletii aRer vere f i c
h w VaSC
e n d

--
. . --r CHEMOTHERAPY AFTER HYSTERECTOMY SivaneJaratnam el al. 199 NO. 4
d b l e . She was then given whole pelvic irradiation in- stead.
~ 1 1 patients were closely followed with vaginal vault mam, colposcopy, abdominal and pelvic ultrasound ex- amination, chest radiograph, and where ncceSSary com- puted tomography (Cr) scan evaluation.
Results
Fourteen patients had squamous cell carcinoma of the a& and two others had adenosquamous carcinoma (Table I). The primary tumor size was less than 3 cm in 15 of them. In the remaining patient it measured 4 cm in diameter. In the three patients with pelvic node me- - it was bilateral in one patient, involving six nodes. Histologic examination showed that the tumor had in- vaded almost the full thickness ofthe ceMx in ten patients. Vascular/lymphatic channel permeation was seen in all but one and microscopic evidence of parametrial exten- sion was present in another.
Fourteen of the 16 patients are alive and without evi- dence of disease after a median follow-up of 29 months. These patients have been followed for periods ranging from 16 to 38 months. Two other patients died. One pa- tient died 6 months after surgery from cardiac failure; she had full-thickness invasion of the cervix by tumor and lymphatic channel permeation by tumor cells, and a p peared to have tolerated the five courses reasonably well. The other, who had an adenosquamous carcinoma, had multiple high-risk factors, viz., full-thickness tumor in- vasion of the ceMx, lymphatic channel permeation, clin- ically undetected parametrial extension, and bilateral pel- vic node melastases (six positive nodes). Mitomycin C therapy was discontinued after two courses because of severe bone marrow depression. After appropriate trans- fusions, she was given whole pelvic irradiation. She died 13 months later from disseminated disease (lung and brain metastases).
A majority of patients experienced nauses and vomiting for 1 to 2 days after administration of drugs. Myelosup pression was present in four patients (25%) resulting in a severe drop in hemoglobin and platelet counts; one of these patients developed petechial hemorrhages. These changes were observed after two cou~ses in one patient and after the fifth course in three others. AU required blood and platelet transfusion. Three patients complained of breathlessness on com-
pletion of therapy. In one patient this occurred 3 months after completion of therapy and was accompanied by se- vere anemia, thrombocytopenia, and bilateral pleural ef- fusion. She was thought to have mitomycin C-induced vasculitis with pulmonary infarction. AAer prolonged hospitalization of 3 months she appeatrd to have m v - ered from the toxic effecis of the drug. Another had facial
T d Rcnimd Dead (n = 16) (n - I) (n - 2) - ~
HUtola~ic typc Squimous ctU arcinom Lule all kemtiauing iugc cell nonkcntinizing
Adcnosquunout arcinom
<2 cm 2-3 cm >3 cm
UniliterPI BilitrrpI
Rimuy tumor a k @os)
pelvic mode metpRlsQ
Full thickness invasion of ihe m i x (histologic)
Lymphatic channel permeation Vascular permeation ppramcuial extension Duntioo o l lollow-up (mo)*
<IO 10-15 16-20 .. -~ 21-25 25-30 31-35 35-40
* Median suMval.29 mo.
puffiness and difficulty in breathing. A chesi radiograph showed mediastinal widening. A CT scan demonstrated a lobulated mass in the anterior mediastinum. At anifxior mediastinotomy, the thymus gland was eniarged and a thymectomy was performed. She remains well. In the third patient the breathlessness was transient. Moderate alo- pecia occurred in two patients. Transient elevation of m m glutamic oxaloacaetic transaminase (SGOT) and serum glutamic pyruvic transaminase (SGPT) levels was present in one patient.
Diseussioa
SuMval in patients with carcinoma of the cervix mated by radical surgeq is influenced by several factors. A large. primary growth, undetectad paramarial tumor extension, the presence of tumor in lymphatic/vascular channels of the cervix, and histologic evidence of pelvic node metaE tases are features that influence prognosis in such pa- tients.'"
Although the overall 5-year survival rates after radical surgery or radiotherapy for Stage IB disease is 75% to 85%,89 when metastases to pelvic nodes are present this drops to 48.5% if between one and four peivic nodes ace positive, and to 19% if five or more nodes are involved. Where undetected parametrial extension exists, the 5-year

CANCER Augurt I5 1989 Vol. 64
suniVd ir only 508.1 m e presence oflymphaticlvmh pnnution the survival rats to 60% to 70%:''
l.lter. in our view, is an ominous finding even in the o~~ ofpelvic node metastases; even with postoperative pelvic imdiation in such cases many have been reported IO recur.'O
When whole pelvic irradiation is added to radical sur- wry there is a high risk of morbidity and mortality." The use of postoperative pelvic irradiation does decrease the incidence of local pelvic recurrence, but the development of distant metastases is not prevented, resulting in no im- provement in overaü s ~ M v d . 8 ~
Gynecologic oncologists have today accepted cytotoxic chemotherapy as a useful adjunct to surgery in the man- agement of ovarian cancer. Its use in the management of those patients undergoing radical hysterectomy for early cervical cancer is not yet established. Cervical cancer can no longer be considered to be a pelvic disease spreading slowly by local infiltration and lymphatic spread; from a small primary lesion spread to pelvic and upper abdominal lymphatics have been seen, and frequently, vascular channel tumor permeation has been observed, suggesting that spread by the blood stream is possible. It is thus seen to be behaving as a systemic disease, a pattern of spread that requires systemic measures. In view of the poor prog- nosis when the above high-risk factors are present, it is fair to assume the possible presence of micrometastases not only within the pelvis, but at extrapelvic sites as well at the time of surgery. Adjuvant chemotherapy in such a situation can be expected to increase cure rate over what can be achieved with local therapy alone.
We had recently reported our experience with cisplatin in combination with bleomycin and vinblastine used as an adjunct to radical surgery in these high-risk patients and found a disease-free survival rate of 86.4% at a median follow-up of 23 months." Cisplatin combination drugs are, however, costly. Mitomycin C, a cheaper drug, used as a single agent or in combination with bleomycin, has been used in the therapy of advanced or recurrent squa- mous cell carcinoma of the cervix. Responses of up to 22% and 93% have been rep~rted."~" In the current study the use of mitomycin C as a single agent adjuvant in I6 patients has shown a disease-free survival rate of 87.5% 'at a median follow-up of 29 months, a rate similar to survival ratea reported in patients with negative pelvic
In one of the two patients who died, adjuvant chemotherapy was discontinued after two courses, and despite full pelvic irradiation the patient died from pul- monary and brain metastases, supporting our earlier comment on the drawback ofadjuvant pelvic irradiation. The other patient died from acute congestive cardiac faii- un 6 months later. A few casm of severe congestive cardiac
failure have been reported after mitomycin C adminii i tration in patients previously treated with Our patient ülushates that mitomycin C by itself can rarely i have cardiotoxic effects. Doroshowl* had demonstrated i that mitomycin C may enhance superoxide and hydrogen 1 peroxide formation in the rat heart. This finding might ~
explain the toxic effect of mitomycin on the heart. Al- though such therapy is not without risks, the preliminary results do show the usefulness of the drug as an adjunct to radical surgery in patients with high-risk factors present and merits further study.
REFERENCES
I . PivaMS,ChungWS.~osticsignifimaofarvicnllnionsize and pclvic node metatasa in cervical &noma Obsiet Gyncol1975; 507-5 IO.
2. Buckley CH, Bepnh CS, Fox H. Pathological prognostic indicaton io cervical m a r with paRiculnr rdmna to pticnts under the age of 40 yean BrJ Obsiet Gynmd 1988; 9547-56.
3. Sidhu O, Koss Uj. Barbcr HRK. Relation of histological factors to the mpons of Stage 1 cpidumoid Caronoma of the c e M x to surgical matment Obsrn Gynecol 1970; 35329-339.
4. F r i a OH, Wnom L. Blood 4 invasion in mar of the d x . Cancer 1962; 151269-1274.
5. üarber HRK, Sommm SC, Ronrrdam H et al. Vascular invasion as a prognostic factor in Stage IB canar of the &. Obsrei G y m d 1976; 52343-348.
6. Martinbeau PW, Kjomad KE, ivcrscn T. Stage IB &noma of the cervix. The Nom@an Radium Hospitll: ti. Results when pelvic nodes involved. Obsfet Gynml 1982; tWZI5-218.
7. Fulla AF, EUiot N, KoJoloff C el al. Lymph node metaRara from carcinoma of the d x : Stage IB and I i A implications for pmgnosU and treatment GynccdOncd 1982; 13164-171.
8. HaLins WJ, Ford JH Ir, Lutz MH et al. Radical hyitemtomy and dv i c IymphSdcKMmy for the management ofearly invasive canm of the cervix. G y n d Oncd 1976; 4278-290.
9. Morley OW, Seksi IC. Radical plvic surgery venus radiation for Stage I minoma of the arvix (cxclusivc of microcarcinoma). Am J Obsiet G y d 1976; 126785-789,
IO. Shingleton HM, Orr JW. Rimary surgical and combined mat- mcnt. in: Sinpcr A, Jordan J. & Canar of the Cervix: Diagnosis and Treatment. London: Churchill Livingnone, 1983; 76-100.
I I . Dirhc S. Radiotherapy of cervical canar. Clin Obsief C y m d 1985; 12203-227.
12. Sivanannlnam V, Scn OK, Jayalakshmi. Adjuvant cytotoxic chemotherapy follOmng Wmheim radieal hysterrctomy for ceMcal canar. A u f NZ JObsret Gynecol1987; 22231-233.
13. niigpn T, Vana RB. 8.lduc-i L, Blesing J. Chemotherapy in the management of advanad or rrcumnt d c a l canar and endo- mnrislrcamri. Cancer 1981; 48658-665.
14. Miyamota T. T i wK Y, Watinpbe M, Tensimi T. EWvenar of a ysvcntiPl combination of bleomycin and mitomydn-C on an ad- vanced emial mm. Cancer 1978; 41:403-414.
with extensive lymph node mclmkses Am J Obsfn Gpwcd 1972; I 1 4 954-962.
16. Crcceh RH. Caulino RB. Shah MK e) u/. An eü&w low dose mitomycin regimen for h m o d and chemotherapy refractory ptimu withm*utiticbrrrdaaxr.Conen1983;5I:IOK1040.
17. B u d u AU, Legba s$ Tashima CK et d. Mriuaynn and mi- tomycin C POiaiMc synerjcmic toxicity. C a m T r a Rep 1978; 6 1 1005-1008.
18. Domsbow IH. Mitomyeid enhatmi rupmride and hyd- pemxideformationintherathmn. JPlilm<imlExpTher 1981:218: 206-211.
IS. mu a, ch.oi Ys, su sc. Flu@& of utmne ceMcal mm
vi
T 2: chemoth tentidy neurotoi which n festation such as 1 pnesthe toxicity include Buctuat nomic 4
adverte and syn neurop sureme
ASSe &mat
-

-
The Demonstration of Human Papillomavirus 7 6 Genomes in the Nuclei of Genital Cancers Using Two Different
Methods of in Situ Hybridization
ELKE-INGRID GRUOENDORF-CONEN, MD,' AND SABINE CREMER. MW
Biopsy specimens of 16 invasive genital cancers (two vuivai arcinomas, two archmu of the vngitu, and 12 cervix d w m u ) were examined for the presence and dlitrlbntion of human paplbmivina (HPV) DNA by in r i m hybrldiutioa with 'H-likkd and bbünylited DNA probes of HPV 6, HPV 11, and HPV 16. None of the tumors reacted with HPV 6 or HPV 11. Using in situ hybridbation with 'H- iabeled DNA probes nine of the 16 nnms &ive positive results with HPV 16. Only three of the nine wen positive for HPV 16 by in situ hybridbatioa with biotinylited probes. Cnrrently, the method of in situ hyiwidlrrtlon with commerciai blotlnyiated probes is kss sensitive than in situ hybridlrrtiw with 'H-libeled HPV DNA.
Cancer 65:23&241,1990.
N RECENT YEARS, mounting evidence has associated I human papillomaviruses (HPV) with genital cancer and its precursors. Human papillomaviruses have been detected in more than 80% of biopsy specimens from gen- ital cancers.' Although different types of HPV have been observed in Benita1 cancerous and precancerous lesions, HPV 16 and HPV LE are most oAen associated with high- grade neoplasias. This implies that these types may have a high oncogenic potential.
The use of cloned DNA in hybridization experiments proved to be the most sensitive method for detecting virus infection in clinical specimens. When cellular morpho- logic type is to be correlated with the presence of viral nucleic acid, in siiu hybridization on tissue sections is indispensable. This technique permits localization of vi- rus-infected cells within a biopsy sample.'.'
Although labeling of the HPV DNA probe with radio- active nucleotides is still the method of choice, major pro- gress has been made in the incorporation of biotinylated nucleotides into the DNA strands, followed by detection with enzyme-coupled avidin and a staining reaction. However, opinions are contradictory with regard to the sensitivity of in situ hybnduation with biotin-labeled
Fmm UK *apr<mnit of h a t o l o g y al the Medid Faculty of the R W " . Arhcn: and thc tr>cpr<ment oiGynssology at the ONUdt HOapiUl ofthe Mcdial S c h d Hannowr. Hannover, Federal R-MK
Supported by a DeuWhe Fonchungq#meiMeM grant No. Gr.641. Mdrar br nrpnitc U b i @ GniBmdoñconm. MD, HiuIkünik
der Msduinixim FakulUi, an der RWTH Aachrn. F'auwekStnBe. D 5100 A.ebm. Fedenl RepuMK of Germany.
AcecDIsd for publition July 21, 1989.
-
of ocnnuiy.
probes as compared with the sensitivity of methods using isotope-labeled pr~bes .~ ' In this study, two different in sifu hybridization methods using 'H-labeled or biotin- labeled DNA probes are compared in disclosing HPV DNA sequences in frozen tissue samples of female genital cancers.
Materials and Methods
We determined the presence and localization of viral DNA in female genital lesions using different methods of in situ hybridization with labeled DNA of HPV 6, HPV I I, and HPV 16. Sixteen genital cancers were studied. The deep-frozen tumor tissues were received from the Department of Gynaecology at Hannover. Federal Re- public of Germany. We examined 12 cervix carcinomas. two vulva carcinomas, and two carcinomas of the vagina. For comparison of the different in situ hybridization tech- niques, parallel sections of each tissue sample were sub jected to both procedures. We performed method I using HPV 6, HPV 1 I , and HPV 16 DNA nick translated with 'H-TTP as probes. The different HPV clones were gen- erously provided by Dr. Lutz Gissmann/Heidelbeg. For method 2 we used the "PathoGene" DNA probe assay for identification of human papillomavirus types 6/1 I and 16 in tissue sections (Enzo Diagnostics, Inc., New York).
In Situ Hybridization With 'H-Labeled Human Papilloma Virus DNA
Frozen d o n s ofabout 5 wn were mounied on slides. dried in air, and fixed in methanokglacial acetic acid 3: I (v/v) for 3 minutes. ARer heat denaturation in boiling
No. :
pho chi1 Sub con on t in : rins chlr met the! emi 43" for P
in € bat1
stai and O f < t o t
In : Hu.
S to s for eth:
buf con coli eac Ute diu tail anc inc soli roc mn
ish on! for 3-a in 1 an< slic her
of < I 1 tes
Was
que
I
L

HPV 16 IN GENITAL CANCERS WJO. 2
hate-buffered saline (PBS) for I5 pconds slides were Ph-. . gilled in iced water and fixed in methanol for 3 minutes. Subsequently 50 hl of denaturated labeled DNA solution eonmining IO' cpm per slide and a coverslip were placed on the d o n s which were incubated for 20 hours at 65OC in a moist chamber. After incubation, coverslips were rinsed with 2x ssc ( ix ssc contains 0.15 mol/l sodium chloride (NaCI) and 0.01 5 mol/l sodium citrate) fixed in methanol for 3 minutes and air dried. The slides were then dipped into a 1 : I dilution of Kodak nuclear track emulsion (Eastman Kodak Co., Rochester, NY) kept at 43T . AAer having been dried in air, they were exposed for 20 days at -20°C.
After exposure, the slides were developed for 4 minutes in Eukobrom, developing was stopped in an acetic acid bath for 2 minutes, then normal photographic fixation, washing, and airdrying followed. The sections were stained with hematoxylin and eosin, mounted in Eukitt, and covered with a glass slip. Labeling appears in the form of dark grains, dispersed or in clusters, strongly limited to the nuclei of epithelial cells.
In Situ Hybridizaiion Wirh Bioiin-Lnbeled Human Papilloma Virus DNA
Sections of about 6 pm of frozen specimen were applied to adhesive pretreated slides, fixed by soaking in acetone for 10 minutes, and airdried. After dehydration in ethanol, slides were dried at room temperature. Subse- quently 1 drop ofdenaturated biotinylated HPV DNA in buffered NaCI/ethylenediamine tetraacetic acid (EDTA) containing 40% formamide, 8% hybridization enhancer, coloring and a coverslip were placed on the sections of each slide. The slides were then incubated for 4 to 5 min- utes at 92°C and for 25 minutes at 37OC. Coverslips were discarded and 0.5 ml ofa post hybridization solution con- taining 20 mmol/l phosphate buffer, 260 mmol/l NaCI, and 40% formamide were applied to every specimen and incubated for 10 minutes at 37°C. The posthybridization solution was then tapped off and slides were washed at room temperature with IO mmol/l PBS containing 5 mmol/l EDTA.
A total of 0.5 ml of streptavidin-biotinylated horserad- ish peroxidase complex in buffered NaCl was dropped onto each specimen and slides were incubated at 37°C for 15 minutes. After washing, 0.5 ml of a mixture of 2% 3-amino-9-ethylwbazole (AEC) and hydrogen peroxide in 0.05 mol/l acetate buffer was applied to each specimen and slides were incubated at 37°C for 15 minutes. The slides were then washed in buffer and counterstained with hematoxylin.
The appearance of a red precipitate within the nuclei of epithelial cells indicates the presence of either HPV 6/ I I or HPV 16, or both, in the biopsy specimen being tested.
Gn@endor/-Conen and Cremer 239
Results We examined biopsy spechens of 16 women with
genital cancer for the presence of HPV DNA in these lesions using two different methods of in siru hybridiza- tion. All cases studied represented invasive, poorly dif- ferentiated squamous cell carcinomas. The results of in siiu hybridization are shown in Table I .
Nine of the 16 invasive cancm gave positive results with HPV 16 using an in siru hybridization technique with tritium labeled DNA probes of HPV 6, I I and 16. Three of the nine were positive for HPV 16 using in siiu hybridization with biotinylated probes. These tissue spec- imens gave especially strong positive signals with radio- actively labeled HPV 16 DNA. None ofthe tumors reacted with HPV 6 or I1 DNA.
The specific hybridization signals were seen to varying extents within nuclei of cells in the tumor strands. in some cases, positive labeling was confined to only a few nuclei which were grouped within the invasive tumor tissue (Fig. I). The intensity of nuclear staining varied considerably from cell to cell within these HPV I&@tive cell clusters. Tumor strands of other cases showed extensive areas in which nearly all tumor cells contained nuclei with strong positive signals (Figs. 2 and 3). Morphologically these areas could not be differentiated from those without labeling. They did not contain conspicuous cytoplasm or cyto- plasmic halos similar to the cells that stain in condylomas or in bowenoid papulosis.
Diseussion The well-established close relationship between HPV
and genital cancers has rendered the in siiu hybridization
TABU I . HPV In Siru HybndUation RnulU in Genital Cancers
In siru hvbridization with
Biotinylatcd DNA 'H DNA
Age Cancer HPV HPV HPV HPV Sample (yr) diagnosis 16 6/11 16 6/11
O - cmix + O O
HI - cervix + O
O H2
O 43 cervix - O
H3
O H4 42 Cmix + O HS 51 c m i x + O H6 65 cervix + O + O
88 Vagina + O + O O
H7
O H8
O H9
O HI0
O HI I 41 c m i x
O HI2 HI3 78 CeMx HI4 42 Vulva + O + O
O O
HI5 41 cervix HI6 78 Vagina
- - - - -
- O 83 Cmix 57 Vulva + O 36 CeMx + O
O O 47 CeMx - O
O O
- - - - - - - - - - - - -
HPV human papillornavinis.
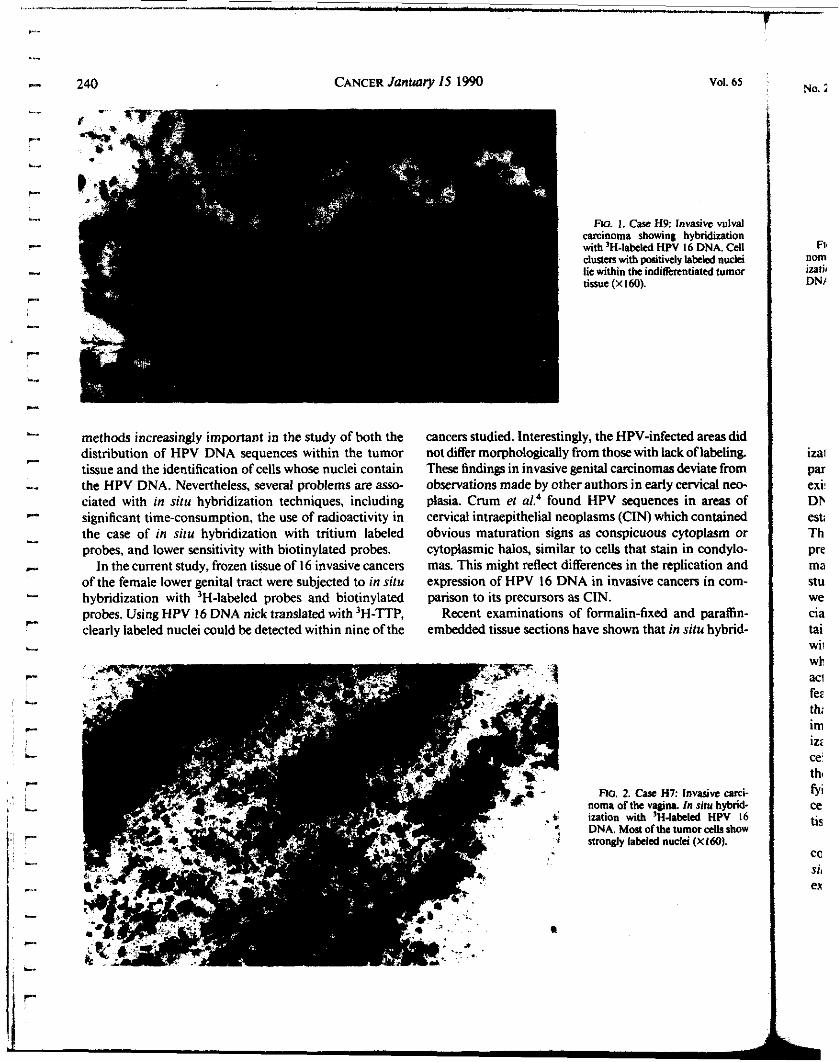
240 CANCER January 15 1990 Vol. 65
RG. 1. Case H9: InvaUvc vulval carcinoma showing hybridization with 'H-labeled HPV 16 DNA. Cell clusten with paaitively labled nwki lie within the indiUnentiatal tumor tissue (X160).
methods increasingly imporiant in the study of both the distribution o f HPV DNA sequences within the tumor tissue and the identification of cells whose nuclei contain the HPV DNA. Nevertheless, several problems are asso- ciated with in silu hybridization techniques, including significant time-consumption, the use of radioactivity in the case of in situ hybridization with tritium labeled probes, and lower sensitivity with biotinylated probes.
In the current study, frozen tissue of 16 invasive cancers of the female lower genital tract were subjected to in situ hybridization with 'H-labeled probes and biotinylated probes. Using HPV 16 DNA nick translated with 'H-TTP, clearly labeled nuclei could be detected within nine of the
cancers studied. Interestingly, the HPV-infected areas did not differ morphologically from those with lack oflabelin& These findings in invasive genital carcinomas deviate from observations made by other authors in early cervical neo- plasia. Crum el al.' found HPV sequences in areas of cervical intraepithelial neoplasms (CIN) which contained obvious maturation signs as conspicuous cytoplasm or cytoplasmic halos, similar to cells that stain in condylo- mas. This might reflect differences in the replication and expression of HPV 16 DNA in invasive cancers in com- parison to its precursors as CIN.
Recent examinations of formalin-fixed and paraffin- embedded tissue sections have shown that in situ hybrid-
Flc?. noma c ization DNA. I annsi:
Cye H7: Invasive Enro- Y vagina. In situ hybnd- th 'H-labeled HPV 16 it of the tumor cclh show kled nuclei (Xlóü).
No. 1
Fi, nom izati< DN/
ira1 Par ex¡' DE est; Th pre ma stu we cia tai Wii
Wb
aci fez th; irn iz2
thg ce
fYi ce tis
ca si, ex

re&--or
NO. 2 HPV 16 IN GENITAL CANCERS Gru@endo$Conen and Cremer 24 I
w. 3. C a s H7: Invasive carci- noma ofthe vagina. In siri: hyhrid- a t ion with biotinylated HPV 16 DNA (X160).
ization with radioactive and biotinylated probes are com- parable in sensitivity, although contradictory opinions also exist? The method of ir! siiir hybridization with 'H-labeled DNA. which requires frozen tissue sections, has been well established in our laboratory over a period of I O years. The theoretical sensitivity of this method is such that the presence of approximately 20 viral genomes (approxi- mately IO grains) should be detectable? In our current study we compared the results of this method with those we obtained with biotin-labeled probes using a commer- cial detection kit. Only three of the nine HPV 16-con- taining tumors were positive with in siiu hybridization with biotinylated probes. These were the tissue specimens which gave especially strong positive signals with radio- actively labeled HPV 16 DNA. However, the morphologic features in biotin-treated sections were better preserved than in those which were 'H-DNA treated. This is a very important observation, for it is the aim of in situ hybnd- ization to correlate the presence of viral sequences with cell morphologic type. In the case ofbiotin-treated sections the lack of radioactive background was especially satis- fying. Positive signals were restricted to the nuclei oftumor cells, whereas the nuclei of the surrounding connective tissue and of infiltrating lymphocytes were negative.
Currently, the method of in sirir hybridization with commercial biotinylated probes is less sensitive than in sirir hybridization with 'H-labeled HPV DNA. Further experimentation focused on improved sensitivity of the
avidin-biotin- based in siru hybridization techniques are required. A s rapid, less complicated and nonradioactive methods, these should have increasing application in fur- ther studies of HPV-dependent cancers.
REFERENCES
I . Zur Hauxn H. Papillomavinixs in human cancer. Cancer 1987; 591692-1696.
2. Gnirwndorf-Conen El. In siru hybridization with papillomavirus DNA in genital Inions. In: Peto R, zur Hausen H, eds. Viral Etiology ofCervical Canm(Banbury Rw~i 2 I) . Cold Spring Harbor, N Y : Cold Spring Harbor Laboratory, 1986 724.
3. Ortrow R, Manias D, Clark B, Mragaki T, Twiggs L, Faras A. Detection ofpapillomannirspecific sequences in human genital tumon by in situ hybridization. Banbury Rep 1986; 21:253-258.
4. Cnim CP, N.@ N, Lcvine RU, Silvmein S. In silir hybridization analysis of HPV 16 DNA sequences in early amcal neoplasia. Am J Parhol 1986 123174-182.
5. Gissmann L. Dun1 M, Oltmdorf T, Daterilz K. Human papii- lomaviruses and cervical cancer. In: Steinberg BM. Brandsma JL, Taich- man LB, eds. Cancer Cells: V. Papillomaviruses. Cold Spring Harbor, N Y : Cold Spring Harbor Laboratory, 1987; 275-280.
6. Syjanen S, PaMnen P, Syjanen K. CompIlnson of in siru DNA hybridization pmlocols using "Slabeled and biotin-labeled probes in detection ofhuman papillomavinis DNA xquennr. In: Steinberg BM, Brandsma JL. Taichman LB. eds. Cancer Cells: V. Papillomaviruses. Cold Spring Harbor, Ny. Cold Spring Harbor Laboratory, 1987; 329- 336.
7. Wells M, Griffiths S. Lewis F. Bird CC. Demonstration of human papillomavinis typs in paraffin promsed tissue from buman anogenital laions by in siru DNA hybridization. JPorhol 1987; 15277-82.
8 . GnisrendoñE-I, zur Hausen H. W i z a t i o n of viral DNA repli- cation in sections of human warts by nucleic acid hybridization with complementary RNA of human papilloma virus type 1, Arch Dermarol Re5 1979: 26455-57.

Detection of Squamous Cell Carcinoma Antigen in Normal Squamous Epithelia and in Squamous Cell Carcinomas of the
Uterine Cervix
GERD CROMBACH, MD.' ANTON SCHARL, MD.' MA'ITHIAS VIERBUCHEN, MD.t HANNELORE WÜRL, PIID.' AND ACHIM BOLTE, MD'
N 1977, Kat0 and Torigoe isolated the tumor antigen I TA-4 from a cervical squamous cell carcinoma.' TA- 4 is a glycoprotein with a molecular Sue of 4 8 . W daltons which is located in the cytoplasm of normal squamous epithelia and squamous cell carcinomas of the uterine cervix.'.' wuamous cell carcinoma (SCC) antigen is one of 14 subfractions of TA-4, purif~ed from liver metastam of a cervical squamous ceü carcinoma.' The clinical value of TA-4 and SCC antigen as serum tumor markers for cervical cancer has been demonstrated in numerous stud- ies,2.S-15 The sensitivity is 44% to 67% in primary and 67% to 100% in recumnt cervical squamous cell carcinomas.
carcinoma and the prognssion or e o n of the tumor during follow-up. However, neither antigen is specific for cervical squamous cell carcinomas. Elmied serum levels arc alu, found in 24% to 53% of patients with squamous cell carcinomas of the head and neck, esophagus and
%Nm lCVCk Of both antigens Efl& the extent Of the
From the aprtmcnis of Wlsctne ' indOynmlosyandtPathoiogy. Univmity of Colagne. F d d RcpuMK of Gnminy. The authors thank Dons p*en for teehnieil uriauia. Addrcss for reprints: GCNI Cmmbach. MD. UnivmitW+Frauenklinik
K(lln,KerpnerStr. )4 ,DSOOOKMn4I ,Fcden lR~Mico f~any . Aax!ptd for publication o*& 24.1988.
1337
and in 8% to 42% of patients with adenocar- cinomas of the uterus, ovary, and
Until now, detailed studies on the distribution of SCC antigen in diffmnt body tissues have not bcen publied, probably due to the lack of a suitable antibody for im- munohistochemical analysis. The current study evaluates the specifici*. of SCC antigen and the factors influencing the release of the antigen into the circulation. Antigen concentrations wm simultaneously mcasurcd in tissue extracts and sera of patients with normal epithelia 01 dif- ferent carcinomas of the female gcnitai tract. Serum con- centrations of SCC antigen in patients with cervical squa- mous cell carcinomas were correlated to the ciinical stage and to the degree of histologic differentiation of the tu- mors.
M i t d iad Methods
One hundrcd tifiy-sevm t i m e &mens were obtained from 108 patinis undewoing s q q for nonmaiignant gyna~ologic disorders (myoma, endometriosis, desceasus, fibroadenoma) (n = 45) or for malignant gynacologic tu- mors (n = 63). In 21 of the 45 women with benign lesions, tissue sections were simultaneously pnpand from two or

1338 CANCER Ap
SCC Wmo cp
1MWz)-
1OW-
I
f.
4- " *r
I + :
I
100- I .. I
r ir .. 10, I
I ... c N m r d s < r r m i N m n * Mera- - c H s- S"Sh0ni. glh.Lm Cuckana. mh.Lm ni45 "-22 n- 24 n- 41
FIG. I . squamous all caminoms antigen concentrations (ns/mr a l l protein) in the cytosol ofnornul epithdu and &nomar ofthe vulva, vagina, uterine &r, endomeuium. ovary, and breast (-: median value).
more sites of the genital tract. The following biopsy specimens were taken: ( I ) normal squamous epithelia of the exocewix (n = 31), vagina (n = 7), and bnast skin (n = 5); (2) normal glandular epithelia of the endocervix (n = 17) and endometrium (n = 17); (3) normal stroma of the arVicpl wall (n = 17); (4) squamous cell carcinomas of the uterine cervix (n = 15), vulva (n = 5). and vapina (n = 2); and (5) adenocarcinomas of the endocervix (n = 4), endometrium (n = 17). ovary (n = lo), and breast (a = IO).
Tissue specimens were divided into two parts for his- tologic examination and for CytoJOl preparation. Fresh biopsy specimens wen cooled on ice immediately after excision, cut and weighed, puivcrized under liquid nitro- gen (wing a microdismembrator, obtained from Braun- Melningen, FRG), extracted with a four-fold amount of phorphite buffer (0.01 mom, pH 7, containing 10% of giycerol) and centrifuged for 45 minutes at IOOOOO X g.
The cytosol was separated from the Wel and the Lipid l aw . The totai pmtcin content waa determined axodq to iowry d d.'' and was wmcted for scmm albumin contamination by radial immunodiñusion (usins M-Par- tisen htes from Behnnswerke, Marb~ug, FRG). C y t d
ril I 1989 Vol. 63
specimens were stored at - 7 O T until used. A volume of 0.1 mlpunordiiutedcytosolwasuscdforeachasay.
Serum samples were obtained from 82 of the above- mentioned 108 patients, from 93 women with primary squamous ceU carcinomas and from 13 patients with re- current squamous cell carcinomas of the uterine cervix. AU sera wm stored at -2O'C until used. Diagnosis was conürmed by histologic examination in all cases. Clinicai siaging of primary ceMcal squamous cell carcinomas was bascd on the criteria of the International Fo'deration of Gynecologists and Obstetricians (FiGO). cmical squa- mous d carcinomas wm c M e d aswcüdüTcrcntiatcd (Grade I), moderately di&nntiated (Grade 2). and poorly diñerentiated (Grade 3) tumors. Criteria of c lad id ion w m the polymorphism of ceUs and nuclei, nucleus/cy- toplasm ratio, mitotic activity, and kmtin formation."
The SCC concentrations in the cytosol (Wmg ceU pro- tein [CP]) and serum (ng/ml) were determined by a dou- ble-antibody radioimmunoassay (Abbott-Diagnostics, Wiesbaden, FRG), based on the d v i t y of a polyclonal goat antibody. The limit of the normal range in serum corresponded to the threshold value of 95% specificity in healthy female controls and was 2.5 ng/ml." The coeffi- cients of intraassay and interassay variation were 13.8% and 15.0%. mpcctively.
The Mann-Whitney test was applied for evaluation of signiñcant differences between individual groups of tissue specimens or serum samples. Differences w m considered significant when the probability of error was below 5% (P < 0.05).
ReSnltl
The disixibution of SCC aniigm concentrations in the cytosol of normal epithelii of the female gcnitai tract and of gynecologic carcinomas is shown in F i i 1. The an- tigen values ranged from 194 to 25.033 ng/mgCP in nor- mai squamous epithelia, from 350 to 6917 Wrng CP in squamous cell carcinomas, from 1 to 975 numg CP in normal columnar epithelia, and from 1 to 850 ng/mg CP in adenocarcinomas. The median values in these groups wen 4529,2477, 15, and 3 ng/w CP, rcsp&vely. The an*n concentrations in normal squamous epithelll and in squamous cell carcinomas were sionifcantiy higher than those in normai columnar epithelia and in adeno- carcinomas (P 0.oooOi). The SCC antigen valua ex-
loo0 Wmg CP wm mep(uítd in 40 of43 normal squamous epitheli and in 18 of 22 squamous cell car- cinomas, but in none of 34 normal columnar epithelia or of41 adenocarcinomas.
The highat SCC antigen levels wm found in the cy- todofnodsquamousepithdi.ofthecxoaniix(Tabk I). In nine of 3 I casu the valua iay above 1O.oo0 Wmg

No. 7 SCC ANTIGEN I N i H E UTERINE CZRViX * CrOfdJUCh d d. I339
L.
- . L. 1
TABLE I. Squamous CCU cuiinoni Anli#m Conmtmions in the cytoool oí Normal bilhclium and Stroma (Wnu Cell W n ) and in Serum (Wml)
Squamous cpithdium E x d x 31 194-25,033 6ou) V a n a 7 2008-8671 MI3 B w &in 5 2696060 2520
Columnar epithelium Endocervix 17 4-975 Endomnnum 17 1-57
Stmma Cmical Wall 17
97 6
22
2/19 0.3-5.6 1.7 I 16 0.3-5.6 I .6 o14 0.3-2.0 0.8
1/12 1.2-3.3 I .9 1/12 1.2-3.3 I .9
1/12 1.2-3.3 I .9
C P all protein.
CP. The median concentration in this group was 2.3-fold
(Table 2). The antigen values of that groups wen Sip- nificantly different (P < 0.0005). Dcspite the extremely high antigen concentrations in normal squamous portio epithelia, only two of 19 patients had inrrcascd SCC an- tigen levels in serum (3.3 and 5.6 ne/mi, rrspCtively). In contrast, women with exvical squamous all carcinomas had lower cytosol concentrations, but bigher aniigen val- ues in serum (Tables 1 and 2). Elevated serum lcvels up to 61.9 ne/mi wen found in eight of 13 patients. Linear rcgrcJsion d* showed no correlation between cytosol concentrations and serum levels in cervical squamous all carcinomas (r = O. 18). Cyiosol concentrations in normal epithelia of the vagina and breast skin wen of the same order of magnitude as those in squamous cell carcinomas of the excccrvix, vulva, and vagina (Tables I and 2). The median concentrations of SCC antigen in normal
squamous epithelia and in squamous cell carcinomas of
hie& than that in squamous cell carcinomas of the arvix the exoccrvix wen five to &fold higher than thosc in normal muma and adenocarcinomas of the endocervix and 100-fold to 6ooo.fold higher then thosc in normal endometrium, cervical stroma, and adenocarcinomas of the endometrium, ovary, and breast (Tables 1 and 2). Antigen concentrations lying above the lowest values measured in normal squamous portio epithelia (194 ne/ m g CP) and in Cmiical squamous cell carcinomas (350 wmg CP) wcre only found in a few specimens of normal mucosa and of adenocarcinomas ofthe endoccrvix. How- ever, the highest concentrations measured in normal and malignant lesions of the endooemX did not c x d loo0 ne/- CF'. Elevated SCC antigen kvels in serum werc only found in one of 12 women with normal glanduiar epithciia and cervical stroma and in two of 34 patients (6%) with adenocarcinomas.
Patients with primary cervical squamous cell carcino- mas had elevated SCC aniigen serum levels in 61% of -. Thc positivity rate and the m m concentrations
TABLE 2. Squamous Cell Carcinoma An- Conantntions in the Cytoml of Squamous Ccll C a r i n o m and Adenoareinomu (Wmg Cell Rotein) and in Smim (Wml)
Cytosol Smim
&nBc Median Elevatcd kvels Rinec Mdmn n (Wnu CP) twnu CP) (>2.5 Wml) (WmU . (WmU
Squamous all carcinoma cervix I5 350-4578 2483 8/13 1.3-6 I .9 3.7 Vulva 5 1905-69 I7 2520 015 0.5-1.8 I .o Vagina 2 2124-2450 2287 012 I .3- I .4 I .4
Adenomrhoma cervix 4 167-850 508 114 1.3-2.7 1.9 Endomnnum 17 1-141 10 0110 0.5-2.0 1 . 1 OWrj IO 1-6 I 1/10 0.5-6.0 0.8 Blurt IO 1-14 2 O110 0.6-2.4 I .o C P cell protein.
-

1340
~~ ~ ~~ ~
CANCER April I 1989 Vd. 63
TABLE 3. Incukna of Elevated Squamous Cell Carnnoma Antigen Lrvclr (>2 5 ne/ml) and Mediui Conanuruona in Serum ocpcndiq on Tumor Styc and M the üegm of Hiaolopic DiRmnlution of R i m w C m a l Squunous Cell Carcinompr
Histologic grading
O1 G2 O3 T d
1 214 2.3 5/17 2.2 2/10 1.6 9/31 (2%) I .9
11.7 lb? 21.2 w25 (88%) 14.5 I1 Ill 111 414 36.5 17/19
3.3 14/21 3.6 316 3.6 18/28 (64%) 3.5
1v - - 616 48.1 213 6.4 8/9 (89% 33.1
Toul 7 P (78%) 7.7 42/63 (67%) 4.8 8/21 (38%) I .8
FIOO: Intcmationai FcQauion of oynsolcgy and Obst*r*r
measured depended on tumor extent and on the dcpe of Ilhtologic di&rentiatim (Table 3). The incidence of pathologic valued increpsed from 29% in Stage I to 89% in Stage tV, and the median d u e s from 1.9 ng/ml to 33.1 ng/ml. Antigen kVcL in Stage III/lV wen signif- icantly di&nnt from those in Stages I and I1 (P < 0.01).
entiatcd carcinomas bad paihologic antigen levels in 78% and 67% of cases, rcspeCtivciy. The positivity rate in women with poorly di&mitisted tumors was only 38%. ThcsenrmconmtrationsinGradc 1 andGrade2tumon wen genificantly higher thanthoac in<jrade 3 carcinomas (P 0.05). The median valua were hiest in Gradc 1 (7.7 &mi) and 10- in Grade 3 (1.8 Wml) tumors. Similar rcsults were found in women with recurrent ccí- vical squamous cell carcinomas. Elevated rrmm concen- trations were measured in all eight patients with Gradc 2 tumon, but only in two of five women with Grade 3 car- cinomas. However, the value$ üom patients with rrcurrmt Grade 2 tumon wen not sigdicautly di&rrnt üom t h e with Grade 3 carcinomas (P > 0.0s).
Mediaa $02 antigen co~~ccntratiom in the cytosoi of squamous ceü carcinomas wen higher in Grade I and Grade 2 tumon (n - 10, t = 2522 ng/mg CP) than in Gnde 3 csrcinomas (n = 5, i - 970 CP). However, the antigen ranps in both groups wen similar (350-4578
Patierits with well-diffmntiatcd or moderateiy
and 42- 10 n g / q CP, nspcctiVely). SUtbtid al- uation of the cytosol conccIItratiom meskd no seniñcpnt difFerenccs (P > 0.05).
r)bcoMh
High conantrations dsCC anwn were deteaed in
mow cell aminomne. The median concentrations were 300.foId to 1500-foM hi#her than those in n o d &I- dulu epithelia and in adeiioam 'nomas (Fi I). The
the @ of U O ~ S~UXUOUS epitheli. and of qua-
highest median value was found in normal squamous portio epithelia e x d u g that of cervical squamous ceU carcinomas by a factor of 2.3. In &adular epithelia the antigen conmtratiom wm in normal muwsu and in carcinomas of the endocervix. Some v d u a even overlapl>sd with the lowa5t concentrations incammi in squamous epithelia This fact could be attributed to the contamination of some endocmid iissuc apecimen with small parts of adjacent squamous epithelia Entirely pun tissue Prepantions of normal giandular epithciia and ad- enocarcinomas of the endometrium, ovary and breast without squamous piuo contained only very low antigen concentrations.
Similar resuits were reporttd by MonokaZi who found 10-fold to SO-fold TA-4 concentrations in normal and malignant lesions of squamous portio epithelia than in normal cndoceMcai mucos& Neither ceMcal stroma and n o d endometrium nor ~ d n o m a s of the endoarvix, endom&um, and ovary had mcawmbie TA- 4 activitia. In contraed to the nsultc of the cumnt study, the mean TA-4 concentrations measured in ceMcal spuamousdca ranomaswere f i ~ fdd~ thanthe in normal zquamous portio epithelia. According to the results of Bow cytometric analpis in cervical squamous cells, the TA-4 content in CPI~CCI cells waa indeed eight tima greater than in n o d ceüs.=
Howem, in the esophaeis aignibmtly higher SCC a n w n concentrations were measured in n o d squa- mous epithelu than in squamous ceü carcinomaa." The reason for the di&nng TA-4 and SCC antigen mtioa in thcq studiu may be the hcterosnieity of the JycoProtnn TA4 which coushía of 14 Subfiactiona witb isoelectric points (IEP) m@ng from 5.44 to 6.624 The SCC aniigen is a ncariy pure protein with a carbohydrate content of less than 0.6% and har the most neutral IEF' (6.62) of all subfdoas."'2 Qto n al." dcmonssnted in an d e r study that aeutrpl TA-4 (IEP, 6.3-6.6) bth~ prrdomiannt
1 in mr
I
L

No. 7 ScC ANTIGEN IN THE UTERINE CERVIX - Crombach n d. 1341
M o a in mnmriioii.nt squamous epithelia, whmps acidic T A 4 (IEP, 5.9-6.2) is mainly present in the tissue Ud mum of patienis with cervical squamous ail carci- noms%. Since it is not clm which subfraction of TA-4 was measured in the studies of Monoka” and Sasaki et al.,= tissue mcasuiements of TA-4 and SCC antigen can- not k directly compared. The d t s of TA-4 and SCC antigen daenninatioas
in the cytorol ur in apemeat with the data of an im- munohiaxhemical study by Ueda et al.,’ who detected T A - ~ in all n o d squamous portio epithelia, in most of cervial squamous all carcinomas and in a few normal columnar epitheiia and adenocarcinomas of the ende Cmu, but not in nonnal glandular Cpithdia and in car- cinomas ofthe endometrium.
Desplrc the high SCC antigen conantrations in the cyton01 of normal squamous epithelia, serum levels were &y always within the normal range. Women with CCI-
vical squamous cell carcinomas had lower tissue concen- trations, but higher serum values of SCC antigcn. Ac- cording to our own results and to the data of Morioka?’ thm was no correlation between cytosol concentrations and serum levels of SCC antigen or TA-4 in cervical squa- mous all carcinomas. The median serum concentrations and the incidence of elevated serum levels increased with tumor extent. niese findings indicate that the release of SCC an@ into the circulation depends on infiltrative tumor pmih and on tumor mass, but not on the local anaen content in the tissue.
Analgous findings have been reported for carcinoem- bryonic antigen (CEA). Them was no correlation bmvcen piamia and tumor concentrations of CEA in carcinomas of the liver, lung, gsstrointeStiaal, and female genital tract.*” Van Nagell et al?’ supposed that plasma CEA reüects the total tumor burden (i.e.. tumor CEA concen- tration X tumor mass) rather than the tumor CEA con- centration alone.
Howver, thew conclusions cannot explain the fact that 10% to 20% of patients with cervical squamous cell a- cinomasS~l~andIVhavenomialSCCantigen~enim levels. Apparently, additional factors influence the release of the marker, one of those being the differentiation of the d n o m a s . The incidence of elevated SCC antigen levels and the median serum values were higher in patients with well-diffmntiated and moderately Wemntiated cervical squamous cell carcinomas than in women with poorly differentiated tumors. Mcdian cytosol conmtra- tiom in Grade 1 and Grade 2 minomas were higher than in Grade 3 tumors. Similar data were found in squa- mous cell carcinomas of the esophagus.’* These findings are also conñrmed by the msults of immunohistochemical studies. In the normal squamous epithelium of the a n i x ,
TA-4 was detenabk only ¡n di&rratiiud squimous cells of the intermediate hyn; and not in the immature ceils
TA-4 was positive in more di&rentiated tumora such as large cell kmtininng and luge cell nonkrntinlling a- cinomas, but never in mall cell nonkerstinizing &- nomas?.’o
The results of our invdgdon show that SCC antisen is not tumor ~ 6 c . Hi@ quantities arc pnicnt not only in squamous cell carcinomp* but also in the cytoplasm of normal squamous epithelia. The releaac of the antigcn into the circuiation depends on infiitrative p w I h and the mass of the tumm rcither than on the local tissue content. Apparently, SCC an&cn is a marker of cell dif- fmntiation for squamous cdls. Further chuactmzati . ‘on of SCC antigen requires simultaneous histologic exami- nations, immunohWciwmd ’ studiegandmeuwemnit of concentrations in the cytosol and serum in a large number of patiente with &cal squamous all carcino- mas. Biochemical studies are needed to elucidate the dif- ferences between TA-4, SCC antigen, and other sub- tions.
of the basal laycr?J2 In caviai squamous cell arcinornag
REFERENCES
I . Kat0 H, Torigoe T. RdiQnimunoupy for tumor antksn of hu- man a w b l squamous cdl Minoma. Cmuer 1977; 40:1621-1628.
2. Kat0 H, Mniolu H, Arrmiti S, Tor ip T. RdioimmunoPrPy for tumorantipniofhumuiem*J~quimousall&nom. CdlMd Biol1979; 2551-56.
3. U& G. lnoue Y , Yiminlii M n a/. Immunohiaochcm*ll &m- onstration of tumor anika TA-4 in gyaaolopic himon. lm J GynrOr Pahol1984.3291-298.
4. lk& 1. Two& D d i o i m m u n o ~ c (nndwieh) m a y of s<x: uitign wing monodonil i n n ¡ In: Ksto H, de üruijn HWA, Etai W. Hnkrmui Rñ, Johnem IT.& Squimwr Cdl cucimmi Anlism in the M-t of5qiuiaaa Cdl cUnwn>.. Rinedon: EaCaW Medics, 1987; 215-226.
5. Km0 H, Miyawhi F, Maioiu H, Fqmo T. To r ip T. Tumor ~t igmofhumuicmi~ . l~ore inom:Carr*t ionofe i r - culiting kvds with diax prcsus C m 1979; 43385-390. 6. Km0 H, Mniolu H, Tairaii H, Anmiki S, T ~ ~ i s o e T. Vdue of
h i m n u i f i s c n ~ A ~ ) o f q ~ c d l c u c u I o r m u I ~ ~ ~ r r t m t ofcmicai cancer. Cancer 1982, XkI.294-12%.
7. Kat0 H, Moriolu H, AnrmLi S, T m u K, To~igoc T. Rogioatic significance of the tumor mlip~ TA-4 in squmow cdl &noma of the utcnne cervix. Am J W n GymccuI1983; 145350-354.
8. Keto H, Tuiui K. MorioLi H. Npú M, Nipya T, Torigac T. Tumornnti~TA-4intbcdc<rctionofrswmnainemierlquunous all arcinom. Cancer 19% sJ:ISU-1546.
9. Kat0 H, Tam¡ K. N.pyp T. NSpi M, Torigac T. Tñe we of tumor antigen TA-4 for tbc m u y m n t nf squamous all &nom. Cam DAen ñpv 1985: 8:155-.159.
IO. Mamo T. ShibsU K. Kirnun A, Hoahina M, Mocbiniü M. Tu- moru30cistcdint¡ga.TA-4, ¡n tbcmoni~o f the~WSof lhC lapy forsquunousall mmiMnudthelrrmnecmicMx. Cancer 1985: 56M2- 308.
I I . Oba~Y.TdokomM,KiuboSnal.BiUcenlvsfionofmcs- s u ~ m m t ofthe m m knl dqumnow all oreinoma-relited antigen (SCC) and its vdue following imdiition of cancer of the utmne a M x . Gan No Rinsho 1987: 33óü-M.
I I
I !
i i 1 1 I
I 1 I
1 i

-___I
1342 CANCER April 1 1989 Vol. 63
12. Kuo ü, Modolu H. Huhimoto K n d Sccuityn and in cliaiaiapphtbnr in: W H . de h i j n HWA, Ebut W. Habaiaia RE, IOhnWn JT, & %lWllOUI CdlcUaMnU An- in the MM- sgemat dSqumour Cell curinom. Rinceto~ hcetpm Media, 1987; 1-14,
in the m m dpmienn with Minomi of the cavix umi. GebunJlibé Fmuenhtilkd 1987; 47439445.
EK, You@ YM. Weiicr P h S p m r CE, M&c SE. H&ALAnsnliutiondanumo<ndatrimnvmtyninphBO mtharv ia l squ imwra l l cun~nnrAmJObnnG~1987; I57 433439.
IS. ouhi T. MMM T, Y d M, M~~l~ ¡zuk¡ M. ?diction dthe rreu~~nce ofsqwmoua d at r i~mi of fhe utainc cmix by mom- torin< mum TA-4. Nippon Sank Fqiinka G&i -hi 1987; 3 9 799-806. 16. Ebai W. I&nu>n IT. Tumormarken in the Mamgmat of
Squunwr Cdi curinom of the Had, Neck and Lun, Rinc~n: ExcapU Mcdla, 1987. 17. Muuolu T. Mitucda Y. Dokawa H, Wiunibc K, Mimoto S.
Tbc mcpunmnt of SCC in- in aqulmwr all atriaom of the lun& Gon No Rimho 198% 31.)14-9l8.
18. Oini M, Miom R Dinidi R üruxagnin O. SCC in* in paticno with crophi<t.l ca~%¡nomr In: Kato H. dc ümün H W h Ebut W, H&crnm Ra. Johnson JT, CQ SquunouiCell cueinorm A&en
13. Cromb& O. WUn H, Bdtc A. DctcmiiMtioa ofSCC M~
14.
in thc Mnsgmmt of Squimau Cdl curinohm Rimton: Excupm M d a 1987; l3J-141. 19. Lowry DH. Roxbmw NI, Fur& Fud.u RJ. Rotan ma-
suremat mtb the Mn mad m<cnt. J Bid Chon 1951: 193265- 275. a. FSrmay A cucinomiindotba~uUainthimaroftbcc+Nu.
In: ühu.ustan A. rd. R t h o l ~ ofthe Fmiilc 0cnit.l Tnct, ed 2. New Yo* S ~ ~ ~ I I E C I , 1982; I8CuT 21. Monolu H. Tumor ar&m CrA-4) daqumnoua d d n o m
in tu8ic dlltriñition and ¡la rrbtpiubip to m m TA-4 mn0cntmtion.s. Asia Oceania J ObsIet G+ 1980; 691-97. 22. Snaki K, Na#i M, W H . to rig^^ T, Nlpminc Y, Tiuuibi
M. Flow cyiom&c Uuiylir ofiumoran~ TA-4 in aMal aquamom cella. Gam 1984,73703-706.
TA-4 daqtumour d Muionu in relation to in ippmwc in the circulation. Can 1984,15433435. 24. Khoo SK, Wuncr NL, Lion. c.ianoanbryonie e d v i t y
o f t i i n u c e x V M ; A q u l i l t i t i t i i n h d y o f ~ a n d ~ ~ plism*Nmoticliva.nomuldultandfetilmpnrImJCanm1973; 11:681-687. 25. Van N.acU IR Donildroii ES, Wood Eo. Slurkey RM. oddcii-
bcr# DM. nie grqnonic &¡kana of Minaembyonic in- in the pLm and tumm of paticnu with cndometrul d n i d n o m a Am JObsrn G y n d 1977; 12áM8-313.
23. Kat0 H, Nlpiya T, T o w T. Hcmqnwty ’ Of8hiWUl-

TECHNICAL NOTES
I ' !
I Sensitivity of the Cytologic Diagnosis of Cervical Condyloma
* . . , . ., -,
L
in Comparison With HPV-DNA Hybridization Studies Achim Schneider, M.D., Oabriele Melnhrirdt, C.T.. Ethel-Michele DeVilliers. M.D.. end Lutr Gi8smann. Ph.0.
The cytolo@c diagnosis of nrvicai condyloma is bawd on witrrio dwrloprd o w thr Inst 10 yrars. Ir has now brcomr possiblr to documrnt the prcsencr of humon popilioma virus (HPV) DNA dirrciiy in cervical y b s by thr highly srnsitive irchnique of DNA filter hybridiraiion in situ. The purpose of this article is to evaluotr critically thr rmpirirollr established c~tologic criteria of condyloma b j amparing them with HPV- DXA hybridiration studies in the ramr matrriol. The rrsults of this study indicotr that Wassic'* kuilorytatis and djskrrorocy- tosis arr not highly slnsitiw criteria for the prrsencr of HPV infrction, identfiing only 15% of the HPV-DXA-positive cars mrrectly. In on attempt IO improw the srnsitivity of the cyiolo@c diagnosis of HPVinfrctionr. a panrl of nine 'honclas- sic" criterio was rvaluated. Thr fiw most valuable s i p s were 'kiild koilocyiosis." mild dyskrratwytosis. " hyperchromotic nuclei. bi- and multinuclration, and & a n d cytoplasm. Using ihese critrria in eombination. storistically discriminant 0 ~ 1 j - sis muld correctly idrntify 84% of the HPV-positive p u p . Diagn Cytopataoi 1987;3250-255.
Kry Words: Human papillonu virus; DNA, Cervical wndy loma
Molecular-bioiogical methods using DNA hybridization are the most sensitive techniques with which to identify human papilloma virus (HPV) infections. DNA frag- ments of ccnain HPV types could k recognized with this technique in up to 60% of cervical cancer biopsies that had been completely negative by light and electron microscopy as well as by immunoperoxidase techniques using a groupspecific antigen against papilloma virus-
Received AIILUSI 22.1986. Acap<ed Fehary 28. 1987. From the Pithologs Liborators d the Dcpnmeni or Obstetrics and
Gynsdop).. University d Ulm. West Germany. 8nd ihc ücpanment or Vim Rcrurch. Gmnin Gnoa RaaKh Cmtcr. Heidelberg, U'UI Ganuny.
SuPWId by the Dcutvhe farhunppnwinvhsft (Gi 128/I-i). Add- rrpint requa í u) Achim Scbnaidcr, M.D.. DcpPnment of
GyneodSs. University of Uim. Priitwiusr. 43, D-79 Uim. U'SI Germany.
250 Diognosiir Cytq>oihologv. I'ofolJ. .Ko3. Sepentber IV87
es?-' Condyloma of the cervix in its exophytic and fiat form is the mort coinmon manifestation of HPV infection of the female genital tract. By using generally accepted criteria, condyloma is diagnosed in I%-Z%of asymptom- atic female patients of a nonrisk population by cytologic techniques.'-'
The sensitivity of the cytologic diagnosis of an HPV infection based on the generally accepted criteria has never been established. The cytologic criteria were dewl- oped by assuming that an HPV infection presents in morphologically similar fashion in histologic sections as in cytologic smears. The purpose of this study was to test the validity of this assumption by relating the "classic" cytomorphologic criteria currently in use to HPV-DNA hybridization studies. A trial was made to improve the sensitivity of cytology for the detection of condyloma by using a panel of "nonclassic" cytologic signs.
Material and Metsods Cmical smears were taken during routine gynecologic examination of 1,052 women visiting the Outpatient Clinic of the Department of Gynecology and Obstetrics, University of Ulm. between July I. 1984, and June 30. 1985. All patients were asymptomatic; none had a previ- ous history of abnormal cytology. Smears were taken from ihe ecto and endocerrix by mtton-tipped applica- tor. Half of the material obtained was smeared on a glass slide, processed for conventional cytologic examination. and classified according to establiñhed cytomorphologic criteria? The other half was submitted for filter hybrid- iuition in situ in order to detect HPV-DNA. The details of this test haw been described pmiously." The filters were hybridized uith HPV-I 1 (which a l r o d e t ~ s HPV-6 under the conditions used) and separately with a mixture of HPV-I6 and HPV-18. Papanicolaou-stained smears from I O0 patients positive for HPV-DNA were selccted
e l U 7 IOAKUSIK114 MW1CALMUIHUS.I~

,'...
L,,.
fa rrrcrrening. Anoibcr I00 smea~s obtained from pticnu mqativc for HPV-DNA and matched for age were rclcetcd for comporison. Thee 200 smun are the buir of this study.
Cells with nuclear atypia. defined as enlargemcni of tbe aucleus o m b i d with an irregular chromatin pat- tern. w m absent in all smears that were part of this siudy. Tbac smtpn were rescreened retrospcctivcly, with knowledge of the HPV-DNA rault, for the presence of the "cluric" cytomorphologic signs of koilocytosis (Fig. IA) and dyskeratocytosis (Fig. ZA). In addition. nine nonelassic cytologic signs were cval~~aled.
, I !
* I. Mild koilocytosis isdistinguished from its classic coun- cerpart by the absence of nuclear atypia and a less well-defined border between the central cavity and the peripheral cytoplasm (Fig. 1 B).
4 2. Mild dyskeratocytosis is diñerentiated from classic dyskeratocytosis by size and shape of the nucleus (Fig. 28). Threcdimcnsional arrangement and orangeo-
-1 c El
CERVICAL CONDYLOMA
A
Fig. Z (A) Chic dyikentoeylais m ria suprhci.1 qwmour alls with hypcrcbranitk. slightly cnlr)ed nuclei. mall allulir size. and m n p p h i k cylophnic niin (x400).- Q) Mild ncnchic dyrkera- urytair in a shea of uipibeil quamow alis with -1-sized. rclulir nuclei, nan~wphilic cytoplasm. and tbrccdimcnrionil irnnpmcnt (XUX)).
philic cytoplasmic stain are additional features of this cytologic sign.
6 3. Cleared cytoplasm (Fig. 3) consists of an evident lack of stainable matter between nucleus and cell border. This diagnosis was only made in the absence of bacte- rial cytolysis as Doederlcin bacteria can cause a simi- lar phenomenon.
4. Keratohyalin and keratobyalin-like granules (Fig. 4) consist of basophilic or e<ninophilic staining condensa- tions varying in size between 1 and 10 pm. Frequently. the nucleus is missing in thee cells. Ocfasionally, the entire cytoplasmic matter has condensed intogranuler, making the remaining cytoplasm appear empty ("measle cells").
5. Condensation of filaments (Fig. 5) was Seen as crack- like fissura in the cytoplasm with faint stainability of the cytoplasm. -
DiogmsrirCyroparhdol). Vd3. N03.SrptmbrrIW7 251

'I SCHNEIDER ET AL. c
c A ,.g I, ?V
6. Spindle cells (Fe. 6) represent a more pronounced form of dyskentocyta and are distinguished by a regular chromatin pattern from similar cells found in keratinirinp squamous carcinoma. - @ 7. Nuclear hy&rchromatism consisted of increased stainability in the absence of irregularities of the
i- chromatin and nuclear membrane, discriminating this criterion from nuclear atypia. * 8. The presence of bi- or multinucleation (Fin. 4) is a c . - . nonclassic sign.
9. The presence of perinuclear halos is a nonclassic sign.
Statistical analysis for each criterion was done in a two-dimensional contingency table according to the Bon- ferroni inequality. A probability of error of Ins than a half percent bad to k found in order to yield statistical
& 5. Condensed iilimcnu in four supr(kiil4iunrw dlr (x4üü).
significance of 5%. A discriminant analysis was p r - formed to establish a combination of the most valuable cytomorphologic signs for @e identification of HPV- infected smears.
Results Of a total sample of 1.052 patients, 100 were positive for HPV-DNA (9.5%). Thirty-eight smears were infected with HPV-6/11.45 with HPV-16/18, and 17 with HPV- 6/i 1 and HPV-16/18. The mean age of the patimu was 32 yr (range, 18-73). Contraceptive methods used and vaginal flora were similarly distributed in the HPV- positive and HPV-negative groups.
The classic cytomorphologic signs of koilocytosis and/ or dyskeratocytosis could be identified in I S of 100 HPV-positive smears and three of 100 HPV-negative samples (Table I).
For the nonclassic criteria, statistical analysis con-
1
I Noir t sips
nuck
firm HP\
prev was nona neg: sign chrr plar Will
acc
exce
nun of
j
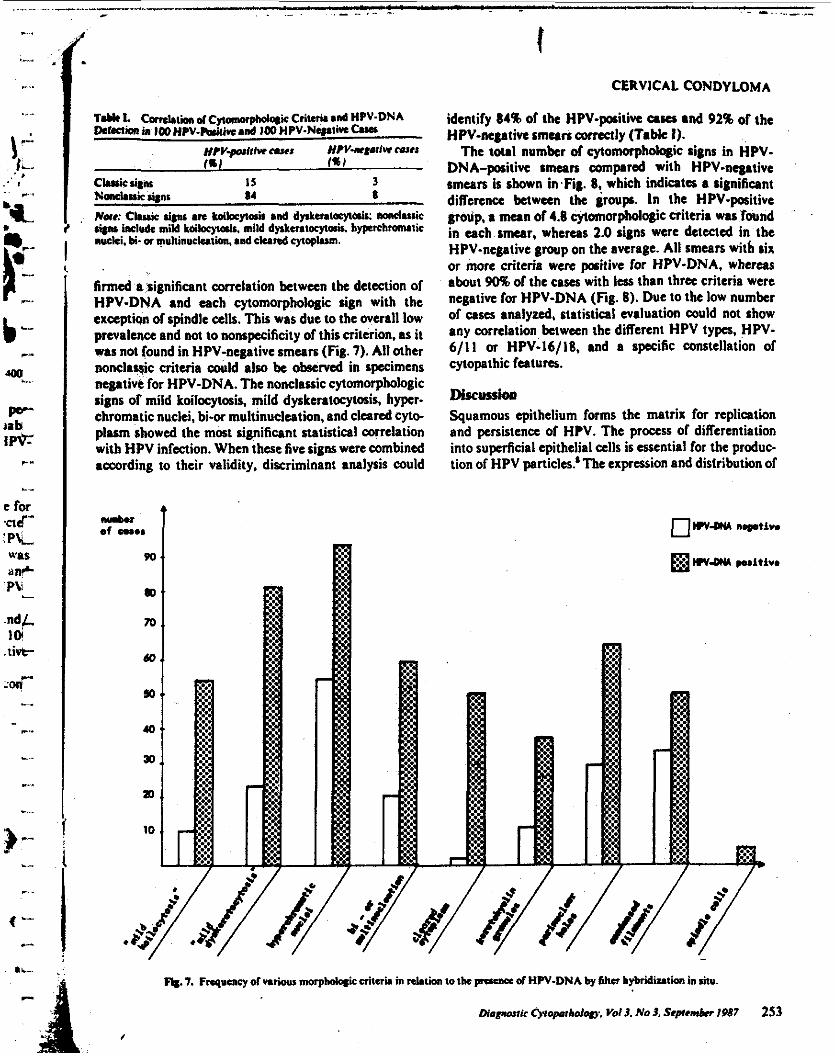
I t
T.uI I. Ik<rñmin IWHPV.bi~kind 1WHPV-Nq.liwCuar
Comtiim dcytomoiphdqic Criteria and HPV-DNA
/%I fa) Hpv-perlriu CuII HIV-nrWiVr w e 8
cludc utnr 15 3
Nom: Clwis sips arc koibqia¡c and dy*enioycair: mnelauic include mild kakc)lo*r. mild dy*mtocyt& byprchronuiic
wki. ü- a multinnckiiim. and ckired cytoplasm.
Nond.ssic u p s 14 8
firmed a significant melation between the detection of HPV-DNA and each fytomorphologic sign with the exception of spindle cells. This was due to the overall low prevalence and not to nonspecificity of this criterion. as it was not found in HPV-negative smears (Fig. 7). All other nonclayic criteria could 81x1 be observed in specimens negative for HPV-DNA. The nonclassic cytomorphologic signs of mild koilccytoris. mild dyrkeratocyWis. hyper- chromatic nucki, bi-or multinudeation. and cleared cyto- plum showed the most significant statistical correlation with HPV infection. When these five signs were combined according to their validity, discriminant analysis could
t CERVICAL CONDYLOMA
identify 84% of the HPV-positive ases rnd 92% of the HPV-negative smmn corre*ly (Table I).
The toul number of cytomoiphdogic signs in HPV- DNA-positive smears compared with HPV-negative smears is shown in Fig. 8, which indicates a significant diñerence between the groups. In the HPV-positive group. r mean of 4.8 cytomorphologic criteria was found in uch smear. whereas 2.0 signs were detected in the HPV-negative group on the average. All smears with six or more criteria were positive for HPV-DNA, whereas about 905ó of the c a w with lers than thra criteria were negative for HPV-DNA (Fig. 8). Due 10 the low number of cases analyzed, statistical evaluation could not show any correlation between the different HPV typcs, HPV- 6/11 or HPV-16/18. and a specific constellation of cytopathic futures.
DiJruUioii !Squamous epithelium forms the matrix for replication and persistence of HW. The process of diñerentiation into superficial epithelial cells is essential for the produc- tion of HPV particles.' The expression and distribution of
*. 7. Fnqucncy of variwr mwpholqic M I M in & t h IO the prcsu= of HW-DNA by sihcr bybr¡diz&sn in UIU.
Diapawir Qmpahdogy . Vd 3. No 3. Septwabu 1987 253
I

d r-
,/ -_ 'XHNEIDER ET AL.
gnor w e
r-
m. 8. Number of cytcinorpholqic criteria in relition IO the presence of HPV-DNA by ñltn hybridintion in situ. v-
i-
cytoplasmic products are influenced by viral interaction resulting in a recalled cytopathic virus effect. which may
L k &pecific for certain viruses as shown for cutaneous HPV kaiohs! For genital HPV infections. koilocytosis - and dyskeratocytosis were considered to represent
Li , pathogmmmic cytologic chang6 as HPV panicles or Ppilioau vim antigen could k identified in thae cell
in addition, other criteria have k c n reported in ibc literature: cytoplasmic granules,'+15 muitinuciea-
..- tion,'' perinuclear halo formation,"" and vacuolization of tbe cytoplasm." On the basis of our HPV studies. we &fined these and additional cytologic criteria as nonclas- ...- a k signs and found a good correlation with the presence of HPV when using the five most,valuable signs; this was in - contrast to a poor detection rate of 15% for the classic
c signs (Table I). When comparing the detection rate of each nonclassic
I dterion in the HPV-positive and HPV-negative group. a d a r a i t diñerenee can k observed (Fig. 8). N o sign .- rcm~ to be pathognomonic for subclinical HPV infection; all of them kside spindle cells are also found in HPV- negative casa (Fig. 8). This may partly k due to a
L. nkty of dirordcn causing rimilar cytopathic phenom- ena. Keratohyalin-like granules may represent a HPV-
p' I y p specific protein product as shown for HPV-I- i, induced m y m i a s ? On the other hand, keratohyalin
c
P-
C^
2% DiatmsiIc C y i o o ~ o w . V d J. No J. Srprmbrr lVd7
granules, which arc morphologically identical to kcrat* hyalin-like granules, are found in any abnormal keratin¡- ration p r ocwcawd by nonvira1 agents, e.&. by mechan- ¡cal irritation. Aggregation of tonofilament bundles either focally or in the peripheral cytoplasm is a common feature of HPV-infected E C I ~ ' . ~ ~ " but an identical dfcft can k evoked by several other infeaions.
It is conceivable that the specificity of these*noncl&hdc signs is higher than may be concluded from the data of this study. Applying a molc sensitive method for HPV- DNA detection, such as Southern blot analysis, about twice as many samples are positive for HPV-DNA com- pared with filter hybridization in situ." Thus, some of the HPV-negative sman positive for classic (Table I) and nonclassic cytologic criteria may be Icen as positive for HPV-DNA using another hybridization method.
Four or more of the cytomorphologic sigm had to k present in the HPV-positive group and more than w e n criteria absent in the HPV-negative casa to yield a good correlation with the mult of HPV-DNA detection (Fig. 8). This was confirmed by discriminant analysis using the results of the five mort valuable signs to identify an acceptable rate of cases correctly (Table I). We conclude from our data that ihc classic cytologic criteria, koilocyto- sir and dyskeratocytorir are not very sensitive signs for the detection of cervical condyloma. Subclinical H P V
I