essilor n68 gb-esp - web version · la luz y las funciones no visuales - claude gronfier luz azul -...
TRANSCRIPT

Vision of SeniorsBlue Light
Visión de las personas mayoresLuz azul
THEMES
TEMAS
SPRING / PRIMAVERA 2013BI-ANNUAL / SEMESTRAL© 2013 ESSILOR INTERNATIONAL
68
vueINTERNATIONAL REVIEW OF OPHTHALMIC OPTICS
REVISTA INTERCIONAL DE ÓPTICA OFTÁLMICA
Points de

PRÓLOGO
__ Efectos del envejecimiento en el sistema visual - Yves Pouliquen
__ El azul malo, el azul bueno, los ojos y la visión - Thierry Villette
VISIÓN DE LAS PERSONAS MAYORES
CIENTÍFICO MÉDICO
__ Fotosensibilidad y luz azul - Brigitte Girard
VISIÓN DE LAS PERSONAS MAYORES
CIENTÍFICO NO MÉDICO
__ Los conductores mayores: Las implicaciones de los cambios visuales que ocurren con la edad - Joanne M. Wood, Alex Black
__ Visualizando la visión, comprendiendo las necesidades de la visión de las personas mayores- Nathalie Bar, Bidisha Rudra, Anne-
Catherine Scherlen
LUZ AZUL - CIENTÍFICO MÉDICO
__ Nuevos descubrimientos y terapias relativas a la fototoxicidad retiniana- Serge Picaud, Émilie Arnault
__ La luz azul y la cronobiología: La luz y las funciones no visuales - Claude Gronfier
LUZ AZUL - CIENTÍFICO NO MÉDICO
__ Los LED (Light Emitting Diodes) y el Riesgo de la Luz Azul - Christophe Martinsons
__ La percepción del color azul y el filtrado espectral - Françoise Viénot
PRODUCTO
__ Varilux S Series™: 4D Technology™ El cálculo binocular personalizado en función del ojo director - Hélène de Rossi,
Laurent Calixte, Damien Paille, Isabelle Poulain
ARTE Y VISIÓN
__ Patología ocular en la obra de Picasso
FOREWORD
__ The effects of ageing on the visual system - Yves Pouliquen
__ Bad blue, good blue, eyes and vision - Thierry Villette
VISION OF SENIORS - MEDICAL SCIENTIFIC
__ Photosensitivity and blue light - Brigitte Girard
VISION OF SENIORS - NON-MEDICAL SCIENTIFIC
__ Older drivers: Implications of Visual changes with age - Joanne M. Wood, Alex Black
__ Envisioning the vision: Understanding the vision needs for seniors - Nathalie Bar, Bidisha Rudra,
Anne-Catherine Scherlen
BLUE LIGHT - MEDICAL SCIENTIFIC
__ New discoveries and therapies in retinal phototoxicity - Serge Picaud, Émilie Arnault
__ The good blue and chronobiology: Light and non-visual functions - Claude Gronfier
BLUE LIGHT - NON-MEDICAL SCIENTIFIC
__ Light Emitting Diodes (LEDs) and the Blue Light Risk - Christophe Martinsons
__ Perception of blue and spectral filtering - Françoise Viénot PRODUCT
__ Varilux S Series™ : 4D Technology™ Personalised binocular calculation based on the dominant eye - Hélène de Rossi, Laurent Calixte,
Damien Paille, Isabelle Poulain
ART AND VISION
__ Ocular pathology in the work of Pablo Picasso - Enrique Santos-Bueso,
Julián García-Sánchez
SUMMARY / SUMARIO
SPRING / PRIMAVERA 2013BI-ANNUAL / SEMESTRAL© 2013 ESSILOR INTERNATIONAL
68
TO READ ON WWW.POINTSDEVUE.NET
19
14
16
11
09
07
04
27
23
29
32
__ Corneal biomechanical and high order aberration changes with aging - Danyang Wang, Quan Liu
__ Ageing and the crystalline lens - Pedro Arriola-Villalobos,
Julián García-Feijoo
__ Future treatments of exudative AMD - Gisèle Soubrane
__ Ageing of the visual system - Avinoam B. Safran
__ Hazards of Solar Blue Light - Tsutomu Okuno
PARA LEER EN WWW.POINTSDEVUE.NET
__ Cambios biomecánicos en la córnea y en las aberraciones de alto orden con el envejecimiento - Danyang Wang, Quan Liu
__ Envejecimiento y cristalino Pedro Arriola-Villalobos, Julián García-Feijoo
__ Los tratamientos futuros de la DMAE Gisèle Soubrane
__ La senescencia del sistema visual Avinoam B. Safran
__ Los riesgos de la luz azul solar Tsutomu Okuno
51
46
48
43
41
39
36
59
55
61
64

Points de Vue - n°68 - Spring / Primavera - 2013 3
FOREWORDEDITORIAL
Dear Readers,
As part of a permanently evolving process at Points de Vue magazine, this first issue for 2013 translates our desire for a change of policy: new director of publication, new format with a bilingual format comprising 2 booklets one after the other, new editorial line.
Points de Vue magazine continues to target all ophthalmic optics professionals and it will continue to be published at the same intervals: Spring and Autumn. We will now address one or two themes per issue, linked to news of our new lens products or to scientific news. The magazine will contain at least three main sections: in-depth articles corresponding to the chosen theme, written by authors known to their peers, “product” articles written by Essilor authors and articles on art and vision. Articles supporting the theme will aim to provide scientific grounding that will inform the reader about the theme’s various different aspects.
In parallel, the www.pointsdevue.net website continues to develop, also with new video-interviews with vision science researchers, introduced periodically and linked to the magazine’s current themes. Every one of the magazine’s issues will now go on line, with the exception of the last one, which will be the paper version only. Complementary articles to the ones published in the magazine will be published on this website, specifically designed for on-screen reading and intended for wider distribution and access. Points de Vue will also now feature on social networks such as Facebook, Twitter and YouTube.
As a follow-up to the ultra-violets theme in the previous issue, we look here at blue light, with its variety of effects on our visual and non-visual systems, as well as at the risks linked to visual health and lighting. Short wavelengths have a lifelong cumulative effect and we thought it would be interesting to place alongside this topic a second theme which is that of
JEAN-PIERRE CHAUVEAU Director of Publication
senior vision. Indeed, with the lengthening of life expectancy, this debate is raised increasingly frequently at ophthalmology and optometric conferences, whence the importance of addressing here this subject which is very much in the news. These two themes are prefaced by prestigious authors, Professor Yves Pouliquen on the seniors topic and Doctor Thierry Villette on blue light.
After revealing the secrets of the new generation of Varilux S Series in the previous issue, we now introduce you to the secrets of the personalised version of the Varilux S Series, with 4D technology. You will find details in particular of the physiological basis that has permitted this innovation which deals with aspects of binocular vision, and apply to the binocular calculation of progressive lenses.
As part of our Art & Vision section, today we offer an article on ocular pathology in the works of Picasso and more particularly on blindness which haunted the artist throughout his life. On behalf of everyone at Points de Vue, I would like to thank our outgoing Director of Publication Marc Alexandre for his work and commitment to this magazine over the past twenty years, giving it, thanks to its international network of leaders of opinion, an international image and scientific legitimacy in the field of visual health and vision correction. We wish him a long and happy retirement.
Happy reading.
Director of Publication

Points de Vue - n°68 - Spring / Primavera - 20134
FOREWORD
T H E E F F E C T S O F A G E I N G
O N T H E V I S U A L S Y S T E M
__ THERE IS A TERRIBLE DEFINITION OF OLD AGE, given to us
at the very end of the 16th century by Shakespeare in his own way
in As You Like It, “Last scene of all… is second childishness
and mere oblivion, sans teeth, sans eyes, sans taste, sans everything.”
and this was at a time when great age could be seen as a blessing!
This is truly an atrocious image that he introduces into the script
of a comedy, an image where eyes play their part. The literary genius
has nonetheless, and paradoxically, extended to the majority
of men and women the unavoidable fate of Man, this fatal stage
in their ageing process. Up until recent times, in fact, most people
living never even reached the age of presbyopia. Life expectancy
at birth, and life expectancy at the age of 65 have, we can happily
say, considerably increased. Infant mortality, horrifying in the past,
and seen as an inevitability, decreased in remarkable proportions
over the past century, and for the past thirty years the improvements
in hygiene conditions and medical progress have led to
an impressive reduction in morbidity amongst elderly people,
many of whom now live without any major incapacity to over 80 years
and beyond. Of course ageing is still inevitable but it has become
partially influenceable, even though the biological evolutions that
govern it still retain numerous unknowns. Why do we age?
The important question that we all ask ourselves still remains,
when our past abilities are substituted by new and increasing
inabilities that mark every stage on our final journey.
What we do know is “Ageing follows a period of growth and reproduction. Death may occur when the immortality of the
germinal line has been ensured. In other cases it results from gradual
cellular deterioration.”1 Experimental studies on the C. elegans worm,
the D. melanogaster fly (fruit fly) and mice have been
used to demonstrate four routes that are involved in senescence:
• Inhibition of the Insulin/IGF-1 pathway,
• The production of reactive oxygen species,
• Telomere shortening,
• Lysosomal autophagia.
Not to mention genetic factors which also play their part in ageing.
So our various organs age in their own specific ways: blood
vessels lose their suppleness, the heart is invaded by fibrosis,
the brain by neurofibrillar degeneration and the appearance of senile
plate, the kidney function declines, immune defences are down
and the frequency of cancer increases with age.
The eye itself evolves in its own way. The first obvious signs
of its ageing are the appearance of a difficultly in reading close up,
which is known as presbyopia. In reality this is merely the revelation
of a long process that affects the accommodative power of the
crystalline lens. If one compares this power, at the age of 20,
with that of a four year-old child, it is already clear that a large part
of the accommodative power has already been considerably reduced.
But at that time it is still of no consequence. It is only around the age
of forty-five that someone with emmetropia 2 begins to experience some
difficulties with reading, which will only increase with age and which
requires optical assistance. The causes of presbyopia are due
to structural changes in the crystalline lens and the ciliary muscles
which are responsible for modifying the curves of the lens.
Up until the thirteenth century this was a major handicap for
intellectuals and was resolved only by the introduction of magnifying
lenses. Today we can consider that presbyopia has found its remedy
in the remarkable solutions provided by designers of corrective
lenses and, in a word, progressive lenses have now almost completely
removed this first and inevitable consequence of ageing.
Indeed, presbyopia is so painfully perceived by some that, today,
it has resulted in the use of surgical techniques to avoid the wearing
of spectacles, which show one’s age.
Everyone knows that primitive form cataract 3 occurs with age.
It is the main cause of changes to vision after the age of sixty-five.
This gradual change in the crystalline lens, which leads to
modifications in its transparency results in a range of visual effects,
such as reduced acuity, glare or an alteration in contrast, which
become increasingly debilitating and lead to surgery which,
FOREWORD
It is in the retina that the signs
of ageing are the most harmful
to vision and the origin of major
visual handicaps.
1 Biologie du vieillissement Jean-Yves Le Gall et Raymond Ardaillou. Rapport à l’Académie Nationale de Médecine du 3 février 2009.2 A person with normal refraction.3 As opposed to cataracts that are secondary to various pathologies.
YVES POULIQUENof the Académie française member of the Academy of medicineFrance

Points de Vue - n°68 - Spring / Primavera - 2013 5
FOREWORD
in our times and thanks to remarkable technical developments,
is now a precise, short, out-patient procedure which restores normal
vision. This condition, which has been recognised since antiquity,
but whose nature was not specified before the start of the 18th century,
was previously treated by lowering the crystalline lens 4. It was Jacques
Daviel 5 who proposed, in around 1760, substitution of this lowering
by extraction of the crystalline lens, thus opening the way to a surgical
technique that has been gradually perfected to reach current practice.
It is in the retina that the signs of ageing are the most harmful to
vision and the origin of major visual handicaps. Age-related macular
degeneration (AMD) is the most common of these handicaps and is,
understandably, feared amongst the ageing population. With age
the retina regularly loses photo-receptor cells (cone and rods) but
without affecting vision, since 30% of them are enough to maintain
what we consider to be normal vision. On the other hand, AMD
affects around 25 to 30% of men and women aged over 80.
It is the consequence of a degenerative alteration of the retina, which
is expressed in an impact to central vision, vision which is used for
reading and seeing colours, whereas peripheral vision is maintained.
It can occur from the age of around sixty, but only in a very low
percentage of cases. This percentage increases regularly with age.
AMD is expressed in two ways: the most common is a slow-progression,
dry form, characterised by the presence of lipid deposits or “drusen”
on the macula and, to a lesser extent, a fast-progressing
exudative or “wet” form, characterised by major vascular proliferation.
It is in this second form that injections of anti-vascular proliferation
factors into the vitreous humour permit clear but fragile stabilisation
of macular alterations. Dry forms of AMD do not require this treatment,
which is the first real treatment available for the wet forms of AMD.
We now know what drusen are made of and we know in part
the reasons for their formation. It has been clearly established that
high-risk factors encourage the appearance of AMD (age, tobacco,
oxidative) but also that major genetic factors are involved and these
are beginning to be identified with precision. The result of all these
causes being the alteration of microglial cells which contribute
to the formation of “drusen” and crucial modifications to the cells
in the pigmentary epithelium which we know to play an essential role
in the biology of photoreceptors.
Although AMD is the major retinal complication during the ageing
process, added to it are slow degenerative modifications to the retinal
periphery or the role of degeneration of the vitreous humour which,
since they cause the separation of its intimate relations with the retina,
may be the cause of retinal tears which are themselves responsible
for retinal detachment. There is a particularly large incidence of these
cases in myopics over the age of fifty. Is it incongruous to attribute
to ageing the aggravation of the lesions of a pigmentary retinopathy
which, whilst compatible with a normal life up until middle age lead,
over the last years, to total blindness?
It is often during an examination by the ophthalmologist
that a patient is found to have ocular hypertension and glaucoma.
Patients are usually unaware that they are suffering from this
terrible disease since at the outset it is entirely without symptoms.
Without treatment we know that it leads to optic atrophy.
Although genetic factors now appear to be responsible
for some of these cases of glaucoma, it is nonetheless true
that it is modifications to the trabecular space which are responsible
for the failure in excretion from the aqueous humour,
which conditions ocular hypertony. These alterations are conditioned,
more or less, by age which, in any case, will intervene in late failure
of the optic nerve, due to associated vascular factors.
Although open angle glaucoma, to which we have just referred,
is influenced by age, there is another condition that is totally linked
to it: closed angle glaucoma 6, which is acute sudden-onset glaucoma,
causing terrible eye pain and vomiting, and requiring emergency
treatment. It is caused by the narrowness of the iris-corneal
angle, which has remained sufficiently open for most
of the patient’s life but which suddenly closes for a variety
4 The eye and the crystalline lens were transfixed with a thorn or needle; it was detached and lowered into the vitreous body where it remained and was more or less well tolerated.5 Jacques Daviel, Un oculiste au siècle des lumières, Yves Pouliquen, Odile Jacob, 1999.6 The angle is the narrow area between the root of the iris and the posterior side of the prelimbic cornea. It is where the aqueous humour is filtered, which being secreted by the ciliary body comes out of the eye through the intermediary of this filter. Its obstruction is responsible for chronic hypertony of open angle glaucoma and acute closed angle glaucoma.
Our various organs
age in their
own specific ways.
FIG. 1 Giovanni Serodine (1594-1630), “Ritratto del padre” (Portrait of the artist’s father), 1624. Oil on Canvas, 152 x 98 cm. Lugano, Museo Civico d’Arte Lugano. Photo: akg-images / André Held

Points de Vue - n°68 - Spring / Primavera - 20136
FOREWORD
surgeon. Distortion, with their eversion position in the ectropion,
bearing witness to very great age, require surgical
treatment in order to avoid corneal-conjunctival complications.
And what to think about the “bags” that hang over or underline
the eyelids and which are linked to the failing of an orbital septum,
itself the victim of tissular degeneration? And why do old people
so often have watery eyes?
A condition that causes eyelid distortion and, above all,
late onset obliteration of the tear ducts. This is an extremely common
and unpleasant handicap but to a lesser extent than the reverse,
the constitution of ocular dryness, which is responsible for chronic
keratitis and the need to humidify the eye several times a day…
All small ailments in the face of other more major disorders.
Those we have taken a look at and also those which no doubt
find their most painful expression in lesions to the optic pathways
which can be caused by ageing. Factors which are for the most
part of vascular origin – linked to atheroma, hypertension, diabetes –
are responsible for serious and often irreversible visual disorders
in the retina: obliteration of the central artery, thrombosis of the
central vein, in the optic nerve, acute ischemic optic nevritis
of the retrochiasmatic visual pathways, with the consequence,
most often, of homonymous lateral hemianopsia or even cortical
blindness. Stable hemianopsia, which should not be confused
with hemianopsic scotoma, which rapidly resolves the ophthalmic
migraine that is so frequently encountered after the age of seventy,
is entirely benign.
Will we be able to write another story one day? The story
of humans who could live up to the limits estimated by science,
at least thirty years longer than our current averages, without any
expression of ageing, where one can imagine how difficult
it would be to have to die, without understanding the reason. •
FIG. 2 Jean Fouquet (1420-1481), “Portrait of the Ferrara Court Jester Gonella”, 1442. Vienna, Austria.© De Agostini Picture Library / The Bridgeman Art Library
of reasons, either due to drugs making the dilated iris
responsible for obstruction of this narrow angle, or due
to swelling of the crystalline lens with cataract, encouraging
occlusion of the angle under the effect of an associated
cause. A simple iridotomy 7 by laser can now avoid it when
observation of the anterior segment shows that it may occur.
Although expressions of ageing on the eye mainly affect
the clinical forms previously mentioned, there are many other signs.
We have all noticed the changes that affect the eyes with age.
Those eyes that were so fascinating lose their sparkle and those
previously highly colourful irises have now become dull.
De-pigmentation of the iris is the cause of this, the pupil
that was previously so black turns greyish in colour and the cornea
that was so transparent often bears at its periphery a white ring,
known as arcus senilis. The conjunctiva itself becomes dull
and its pingueculas look more yellowish. And what about the eyelids
that crease due to alterations to the conjunctive tissue that filled them
out? The folds that occur cause many patients to contact a plastic
7 Perforation of the iris at its root.
It is often during an examination
by the ophthalmologist
that a patient is found
to have ocular hypertension
and glaucoma.

Points de Vue - n°68 - Spring / Primavera - 2013 7
FOREWORD
B A D B L U E , G O O D B L U E ,E Y E S A N D V I S I O N
__ THE COLOUR BLUE INSPIRES THE ARTS, blue vibrates through literature,
but we really should be referring to blues: from Aragon’s Blue sun
of dreams, and Balzac’s Life as blue as a pure sky, there is only a
breath, a ray to tip us towards Gorki’s Blue fires of anger or Bobin’s The
blue of disasters seen through the window. “Bad Blue v. Good Blue”,
there’s the challenge and the focus of this latest issue of Points de Vue,
which seeks to answer the new questions that have arisen from recent
scientific discoveries and clinical observations linking the blue-violet
fraction of the visible spectrum – 380 to 500nm – to the eye and vision:
• Is high energy blue harmful to ocular tissue?
• What more do we know today about the physiological roles of blue
light?
• What would be the benefits for human health of suppressing some
of the blue and what would be the risks of suppressing too much of it?
• Are we exposed more today to harmful blue, and if so, why?
Significant progress has been made since the mid-nineties in terms
of physiopathological knowledge about the consequences of exposing
the eye to various types of blue light.
Previously, and since the advent of lasers in the seventies, the scientific
community and public authorities controlling radio- and photo-protection
performed experiments on animals in order to establish the thermal
and photochemical danger thresholds of light, mainly involving UV rays
and the anterior segment of the eye. This research also involved
“high energy visible light”, the blue-violet light renamed “blue light”
for simplification, which is the light that potentially presents a danger
of photochemical lesions in the retina. We know in fact that, except
during childhood, ocular tissue filters out almost all UV rays and that
it is indeed this “blue light” which is today incriminated in certain
ocular pathologies.
In the nineties, progress made in cellular and molecular photobiology
enabled exploration into which bands of visible light were the most
harmful for the retina, which toxicity mechanisms were activated,
distinguishing acute toxicity from chronic toxicity. This work was
stimulated by the increased use of new intra-ocular implants that filter
out blue, and also by the need to assess the risks to the retina
of exploratory or eye surgery instruments.
Acute toxicity is the consequence of exposure to high intensity light over
a short period, and results in thermal destruction of the retina’s cells
and cell death by necrosis.
Chronic toxicity is more insidious because photochemical mechanisms
of oxidant stress lead to the accumulation of photo-sensitising components
and oxidising reactive species (singulet oxygen, hydrogen peroxide, etc.)
which, year after year, increase the danger to exposed cells from blue light
and contribute to certain chronic ocular pathologies, such as AMD
– Age-Related Macular Degeneration – or pigmentary retinopathies.
FOREWORD
350 400 450 500 550
Wavelength (nm)
1.00
0.75
0.50
0.25
0.0
Abso
rpsi
on
FIG. 2 Spectra of lutein and zeaxanthin, in ethanol, illustrate the characteristic differences in the absorption properties of the two carotenoids - Landrum JT, Bone RA. Lutein, Zeaxanthin and the Macular Pigment. Arch. Biochem. Biophys. 2001 (385) 28-40.
FIG. 1 The topography and age relationship of lipofuscin concentration in the retinal pigment epithelium. - Wing G.L., Blanchard G.C., Weiter J.J.. IOVS (1978) 17(7) 601-7.
120
110
100
90
80
70
60
50
40
30
20
10
0
Lipo
fusc
in c
onte
nt (a
rbitr
ary
Uni
ts)
0 10 20 30 40 50 60 70 80 90
Age (Years)
THIERRY VILLETTE PhD, Essilor International Director R&D Disruptive Neuro-bio-sensoryFrance

Points de Vue - n°68 - Spring / Primavera - 20138
FOREWORD
1. Sunlight and the 10-Year Incidence of Age-Related Maculopathy. The Beaver Dam Eye Study. Arch Ophthalmol. 2004;122:750-757.
2. IOVS 2000 (41) 3984-90.
3. Photochem. Photobiol. 2005 (81) 1305-30.
4. Exp. Eye Res. 2005 (80) 595-606 ; IOVS 2000 (41) 1981-9.
REFERENCES
From a clinical point of view, the correlation between exposure to blue
light and the prevalence of AMD is difficult to establish. Nevertheless
several epidemiological studies, including the “Beaver Dam Eye Study”
have concluded that cumulative exposure to the sun increases the risk
of AMD, and that it is more due to visible light than to UV rays [1].
In terms of cells, the photoreceptors (cones and rods) and the retinal
pigment epithelial cells (RPE), two groups closely linked to cells
in the retina, have been identified as being the main cells involved both
as contributors and victims to this oxidant stress and this chronic blue
light phototoxicity, resulting in cell death by apoptosis (programmed cell
death). The RPE is essential to photoreceptors because it supplies them
with oxygen and nutrients and, in return, ensures phagocytosis of their
external segments for each visual cycle, and the metabolic regeneration
of the visual pigment (rhodopsin).
The dangers of blue light to photoreceptors have been demonstrated
in animals. C. Remé and C. Grimm showed in 2000 [2] in rats
that blue light, unlike green, causes photoreversal of the whitening
of photoreceptors; this rapid regeneration of the rhodopsin caused
by high energy blue light leads to degeneration of the photoreceptors
by apoptosis. Molecular mechanisms were explored further
by M. Rozanowksa [3] who showed a combined role played
by rhodopsin and the 11-cis-retinal and 11-trans-retinal retinoids
(“ATR” all-trans-retinal) the accumulation of which contributes
to the phototoxicity mechanism on photoreceptors.
The action spectrum of light phototoxicity on RPE cells was studied
by J. Sparrow and M. Boulton [4] who demonstrated the central role
of lipofuscin accumulation in the amplification of photo-oxidation
mechanisms, resulting in cell death by apoptosis. Death of the RPE
leads, in turn, to the loss of photoreceptors, because they are
inter-dependant. The granules of lipofuscin form in large numbers
when the phagocytosis of the oxidised segments of photoreceptors
is incomplete, which leads to cascades of inflammation and oxidant
stress. Made of lipids and proteins, these granules contain a particularly
photosensitising molecule, bisretinoid “A2E”, made from two ATR,
which has an absorption peak in blue at around 440 nm, which explains
the particular toxicity of blue light for the RPE, with a spectrum of action
that does not follow the light energy level exactly. The collections of
lipofuscin in the RPE increase with age, during childhood and then again
after the age of 45 (fig.1), as well as in pathological conditions such
as AMD or pigmentary retinopathy. Moreover, with age, ocular diseases
and bad diet, the natural mechanisms of retinal defence against oxidant
stress are reduced: reduced “detoxifying” enzymatic activity (catalase,
SOD, etc.), reduced fixing of the macular pigment in the centre of the
retina, notably of lutein and zeaxanthin, which are absorbed
from food, the maximum levels of absorption and protection of which
are astonishingly close to the maximum toxic absorption of A2E.
Recently, a team of photobiologists from the Vision Institute in Paris
(UPMC, Inserm, CNRS), Dr Serge Picaud and Dr Emilie Arnault, under
the direction of Professor José-Alain Sahel, and in collaboration with
Essilor, sought to narrow the spectrum of action of blue light phototoxicity
on RPE cells, by putting the cells, for the first time, in chronic toxicity
illumination physiological conditions, in stages of 10nm, taking account
of the spectral ratios of the solar spectrum and of filtering by ocular media.
They present their work here, for Points de Vue.
Thus, all the in vitro work done confirms the dangers of cumulative
exposure to a certain blue light, Bad Blue.
But, in 2002, chronobiologists discovered a 3rd photoreceptor
in the retina, which furthered the clinical knowledge of the eighties
in terms of the extent and mechanisms of the eye’s non-visual functions,
modulated by a blue-turquoise band, Good Blue, centred at 480nm
(ca. 465-495nm). This photoreceptor projects onto several non-visual
areas of the brain, enabling resynchronisation of the so-called circadian
physiological functions over the 24 hours of the Earth’s rotation: sleep,
vigilance, mood and body temperature are just a few examples of these
functions, demonstrating the importance of not disturbing this Good Blue,
if ever we were to seek to cut out all or some of the Bad Blue. Doctor
Claude Gronfier (Inserm, Lyon) develops, in this issue of Points de Vue,
the current level of knowledge of blue light and circadian rhythms.
Bad Blue, Good Blue, between “chagrin of Azure” (Louis Aragon,
Elsa’s Eyes) and “the magnificent radiation of a heavenly eye”
(Victor Hugo, The Rhine, Letters to a friend), our eyes, our exposure
to the new artificial lighting (see C. Martinsons in this issue),
our vision of colours (see F. Viénot in this issue), our predisposition
to eye diseases, or quite simply to glare (see B. Girard in this issue),
our body, our rhythms, in short our whole physical and psychic life
is influenced by light acting on our retinal and cortical sensors and,
more specifically, by its proportions of Good Blue and Bad Blue. •
FIG. 3 UV/Vis, excitation, and emission spectra of A2E in methanol. The absorbance spectrum had a major peak at 435 nm and lesser peak at 335 nm.
The excitation spectrum monitored at 600 nm emission, was similar in shape with a maximum at 418 nm. A 400 nm excitation wavelength generated a yellow emission centered around 602 nm. Inset, structure of A2E. Sparrow JR et al. IOVS 2000 (41) 1981-9
Wavelength (nm)
A2E
10
8
6
4
0
Rela
tive
Inte
nsity
350 400 450 500 550 600 650 700
Excitation UV/Vis Emission
NCH2CH2OH

Points de Vue - n°68 - Spring / Primavera - 2013 9
VISION OF SENIORS
Medical scientific
P H O T O S E N S I T I V I T Y A N D B L U E L I G H T
__ PHOTOPHOBIA IS THE PAINFUL SENSATION felt by a patient
on exposure to light. It is responsible for the reflex closing
of the eyelids, which protects the retina from too much
exposure to light rays, and particularly the sun’s rays,
due to the phototoxicity of light on the chorioretinal layers.
Photosensitivity occurs only within the spectrum of visible light.
This sensorial information can be exacerbated and in this case
we then refer to it as photophobia. Some diseases cause photophobia
and it is seen as one of the symptoms. The most common diseases
of this type affect the integrity of the eye or vision paths,
such as corneal lesions, traumatic corneal ulcers, corneal abscesses
or superficial punctate keratitis, which are common in all dry eye
syndromes. Uveitis may also be mentioned here, along with retrobulbar
neuropathy or extra-ocular conditions such as migraine or meningitis.
__ SPECIALISED GANGLION CELLS
Photophobia originates in specialised ganglion cells known
as “ipRGCs” (intrinsically photosensitive retinal ganglion cells).
At the current stage of research we do not yet know whether
these cells sub-divide according to the wavelength presented.
These ipRGCs are located in the retina’s layer of ganglion cells.
At the outset their axons take the same path as all the retinal nerve
fibres and head towards the optic nerve. Their specific path has only
recently been discovered, and is called the non-visual path of the
optic nerve, which arrives at the posterior section of the thalamus or
pulvinar [6]. These non-visual paths, individualised using the techniques
of Diffusion MR tractography provide an anatomo-physiological basis
for the pain engendered by light. There are also nerve connections
between the pulvinar and the nucleus of the trigeminal nerve
which can explain photophobia in all ocular lesions that stimulate
the ophthalmic branch of the trigeminal nerve.
After direct connection by the optic nerve to the pulvinar,
the route of the non-visual path connects the cortex, both visual
(Brodmann occipital areas 18, 19, 20), parietal (association area,
Brodmann area 7), frontal and pre-frontal. The connections of this
non-visual path interact with motor and sensorial paths (olfactive).
This non-visual path, activated by photic stimulation, acts on the
excitation limit of the trigeminal neurones in the lateral posterior
and posterior nucleus of the thalamus (rat) increasing
the feeling of pain to light exposure in migraine. A functional IRM
study [8] has also shown an increase in pulvinar activity during
central cerebral sensitisation (migraine), thus explaining
photophobia. The pulvinar is divided into four areas, three of which
(medial, superior and inferior) concentrate visual information [3].
The pulvinar is therefore a major centre for the integration
and modulation of sensorial inputs, particularly those conveyed by
the ipRGCs and the non-visual path which itself has connections with
the suprachiasmatic nucleus (SCN), the habenula, the pineal gland,
the intergeniculate leaflet (IGL) and the olivary pretectal nucleus (OPN).
The latter is connected to the ciliary ganglion and to the Edinger-Westfal
nucleus which is involved in photo-dependent pupil reflexes.
__ THE TOXICITY OF BLUE LIGHT
To protect itself from the harmful effects of high energy light
radiation, nature has established numerous filters. A, B and some
C ultraviolet rays, which have even higher energy than blue light,
do not reach the retina because they are halted by the ozone layer,
then the cornea and the crystalline lens. On the other hand,
the various radiations of the visible spectrum of light do reach
photoreceptors. The blue light wavelength has the most high-energy.
It is located at between 400 and 510nm. It includes violets,
indigo-blue and cyan (fig.1). Blue light is absorbed by the yellow
pigments of the crystalline lens (fig. 2), which gradually appear as age
progresses (fig. 3) and in the retina by pigments, rhodopsin, lipofuscin
and the macular pigments (lutein, zeaxanthin, meso-zeaxanthin).
The photochemical reaction is responsible not only for
phototransduction but also for the formation of free radicals during
VISION OF SENIORS
Medical scientific
BRIGITTE GIRARD Associate Professor at the Paris Hospitals College of Medicine Tenon Hospital, France
Light energy:E (eV) = h�� (Hertz) = 1/ � (nm)
FIG. 1 Photon energy depending on wavelength, within the visible light spectrum.
3,54 3,10 2,48 eV
350 400 500 nm
857 750 600 THz

Points de Vue - n°68 - Spring / Primavera - 201310
VISION OF SENIORS
Medical scientific
1. Dillon J, Zheng L, Merriam J, Gaillard E.: Transmission of light to the aging human retina: possible implications for ARMD. Exp Eye Res 2004 Dec; 79(6): 753-9.
2. Glazer-Hockstein C, Dunaief J.: Could blue light-blocking lenses decrease the risk of ARMD. Retina 2006; 26(1): 1-4.
3. Grieve KL, Acuna C, Cudeiro J.: The primate pulvinar nuclei/Vision and action. Trends Neurosci. 2000;23: 35-39.
4. Lane N.: To block or not to block-is blue light the enemy? ESCRS-Eurotimes, July 2007;12: 7.
5. Mainster MA , Turner PL: Blue light : to block or not to block. J Cataract Refract Surg today Europe 1, May 2007;1-5.
6. Maleki N, Beccera L, Upadhyay J, Burstein R, Borsook D.: Direct optic nerve pulvinar connections defined by diffusion MR tractography in humans: imlications for photophobia. Human brain mapping. 2012; 33: 75-88.
7. Munch M., Kobialka S., Steiner R., Oelhafen P., Wirz-Justice A., Cajochen C.: Wavelength-dependent effects of evening light exposure on sleep architecture and sleep EEG power density in men. Am J Physiol Regul Integr Comp Physiol, 2006; 290: 1421-1428.
8. Noseda R, Kainz V, Jakubowski M, Gooley JJ, Saper CB, Digre K, Burstein R.: A neural mechanism for exacerbation of headhache by light.Nat Neurosci, 2010;13: 239-245.
REFERENCES
oxidative phenomena. These free radicals, which are ionic
unstable, are toxic directly on cellular membranes and intracellular
metabolites, causing a slow-down in retinal metabolism, non-renewal
of the external articles of photoreceptors and their apoptosis.
Photophobia is the retina’s final protection against their oxidative
phenomena, blocking the input of light by means of a blepharospasm
(blinking) reflex.
Results in literature are still contradictory in stating the trigger
role played by blue light in the genesis of AMD (fig. 4) and cataract,
but a certain number of articles come down in favour of this
hypothesis. The generations of yellow crystalline lens implants, which
block out blue light, are the results of these scientific hypotheses.
The debate is still open, but optical filters which block both UV
and blue light are still more efficient. Blue light is however of major
importance to the body, in addition to better scotopic perception
by means of stimulation of the rods, there is also regulation of the
circadian cycle and mood regulation [5]. Melanopsin, the retinal
pigment that absorbs blue, with an absorption peak of 480nm,
controls the diurnal cycle via the non-visual path that stimulates
the pineal gland directly as well as the secretion of melatonin [7].
Changes in serum melatonin levels are responsible for sleep cycles
and mood (photodependent or seasonal depression).
Photosensitivity is a natural phenomenon that gives humans
their diurnal behaviour, with regulation of the internal biological clock.
The ipRGCs mediated by the non-visual path control hormonal
circadian cycles, sleep and mood. Photophobia triggers retinal
protection against light energy and more particularly blue light, which
has the most high-energy and is responsible for irreversible cellular
lesions with apoptosis of the photoreceptors during photochemical
mechanisms that release toxic oxidative residues. •
FIG. 2 Natural ageing of the crystalline lens; cortical nuclear cataract .
Transparent at birth, the crystalline lens is gradually loaded with yellow pigments through the product of oxidation of the tryptophan and protein glycosylation; cataractogenic role of short wavelengths in the case of nuclear cataract: attenuation, followed by non perception of blues and violets. Protective role of the retina?
FIG. 3 Light absorption in a phakic or pseudophakic patient.
350 400 450 500 550 600 650 700
WAVELENGTH (nm)
TRAN
SMIT
TAN
CE (%
) 100
90
80
70
60
50
40
30
20
10
0
Traditional UV-absorbing IOL, +20. D
25-year-old human crystalline lens
54-year-old human crystalline lens
FIG. 4 AMD.
Change in the pigmentary epithelium; cicatricial fibroglial appearance. Atrophia of the photoreceptors. Accumulation of lipofuscin and cellular deterioration products caused by the oxidative mechanisms of phototransduction.

Points de Vue - n°68 - Spring / Primavera - 2013 11
VISION OF SENIORS
Non-medical scientific
O L D E R D R I V E R S : I M P L I C A T I O N S O F
V I S U A L C H A N G E S W I T H A G E
__ SUMMARY
Visual impairment increases significantly with age as a result
of the normal aging process, as well as through the increase
in prevalence of ocular disease. These visual changes have a number
of implications for driving performance and safety. This article
discusses the impact of these age-related changes in visual function
on driving ability and describes current evidence linking performance
on visual tests and driving performance and crash risk.
Driving is a complex task that involves integration of a range of visual,
cognitive and psychomotor skills, many of which are impaired with
increasing age. As driving is considered to be a highly complex visual
task, as illustrated in figure 1, it has been suggested that the high
prevalence of visual impairment in older populations contributes
to the decrement in driving ability seen in older drivers.
The increased prevalence of visual impairment with age results both
from normal age-related changes as well as the age-related increase
in ocular diseases including cataracts, glaucoma and age-related
macular degeneration. These changes result in reductions in visual
acuity, contrast sensitivity, visual fields, motion sensitivity
and increased glare sensitivity and speed of visual processing.
Visual acuity is the most commonly used vision test for determining
driving eligibility, despite the fact that the link between reduced acuity
and increased crash risk is unclear. The earliest studies of visual acuity
and crash risk, showed only a weak correlation between acuity
and crash rates [1]. More recent studies, using a range of sample sizes
and methodologies, also reported only a weak relationship between acuity
and crash risk [2-6], and others have failed to find any association [7-12].
This weak association between visual acuity and crash risk is not
surprising given that the ability to resolve static high contrast targets
is unlikely to represent the visual demands of the normal driving
environment, which includes both static and moving objects
of different sizes and contrast levels both in central and peripheral
vision; tests of contrast sensitivity, peripheral vision and motion
sensitivity may provide better measures of visual performance for driving.
Decina and Staplin [7] reported that contrast sensitivity, visual acuity
and visual fields were strongly related to crash rates in older drivers
and impaired contrast sensitivity is associated with retrospective [1],
but not prospective crashes [9,11,12]. Importantly, these increased crash
rates occur despite the fact that older drivers with impaired contrast
sensitivity self-regulate and reduce their driving exposure [14-16].
Interestingly, crash-involved drivers with cataracts were eight times
more likely to have reduced contrast sensitivity than controls [17].
Closed road studies have also demonstrated a significant relationship
between contrast sensitivity and driving performance for drivers
with simulated [18] and true cataracts [19], and contrast sensitivity
also predicts drivers’ recognition performance (signs, hazards
and pedestrians) under both day and night-time conditions [20].
Studies linking visual field loss and crash risk have reported mixed
results. Johnson and Keltner [21] demonstrated that binocular field
loss more than doubled crash rates compared to controls, while other
studies have failed to find a significant relationship between field
loss and crash risk [1,7,9,22]. However, a more recent population-based
study [11], and smaller scale studies of drivers with glaucomatous field
defects [23,24], provide support for Johnson and Keltner’s [21] initial
findings, demonstrating that only those with more extensive field loss
have impaired driving performance and increased crash risk.
This is reflected in closed road studies which demonstrated that
performance is not significantly impaired until simulated field loss
is more extensive [25]. Similarly, on-road driving studies reported that
it was only the drivers with more severe binocular defects that had
significantly impaired driving ability [26,27,28]. Indeed, it has been
suggested that merging the two monocular threshold fields, known as
the integrated visual field (IVF), may be useful in assessing fitness
to drive in patients with a range of field losses [29,30], particularly as
monocular fields are routinely assessed in patients with ocular disease;
however, the link between IVF and crash risk has yet to be determined.
The ability to see moving targets has often been considered with
respect to driving, given the dynamic nature of the driving environment.
Recent research has shown that motion sensitivity, using computer-
based tests of motion discrimination and detection, is strongly
correlated with driving ability in older adults [19,31-34]. Increased age
FIG. 1 Illustration of the visual complexity of the vehicle and driving environment.
VISION OF SENIORS
Non-medical scientific
JOANNE M. WOOD BSc (Hons), PhD, MCOptom, FAAOSchool of Optometry and Vision Science Institute of Health and Biomedical Innovation, Queensland University of Technology, Australia
ALEX BLACKBAppSc (Hons), MPH, PhDSchool of Optometry and Vision Science, Institute of Health and Biomedical Innovation, Queensland University of Technology, Australia

Points de Vue - n°68 - Spring / Primavera - 201312
VISION OF SENIORS
Non-medical scientific
is associated with impairments in time-to-contact judgments,
as well as in the perception of speed and heading [35,36],
which are critical skills in enabling smooth and fast responses
o road hazards. Even brief delays in detecting moving targets
may have fatal consequences, and reduced ability to discriminate
speed or time to contact could result in increased crash risk.
A large body of research has also evaluated the ability of visual
processing speed and divided attention to predict driving safety,
using the Useful Field of View (UFOV) [37,38]. The UFOV is a computer-
generated task, involving simultaneous identification of central
and peripheral targets presented in the presence or absence of
distracters and relies on selective and divided attention and rapid
visual processing speed which decrease with age [37]. Reduced UFOV
performance strongly predicts both retrospective [13,39] and prospective
crashes in general populations of older adults [9,11,12] as well as in
those with ocular disease [24]. A 40 per cent UFOV reduction was
associated with a 2.2 times higher likelihood of incurring a crash than
for those with no UFOV impairment [9]. Studies have also reported
strong associations between reduced UFOV scores and unsafe on-road
performance [19,40], and driving simulator performance [41]. The UFOV
is also effective at predicting prospective crash risk when administered
in a driver licensing setting [42], providing further support for its
inclusion for screening older drivers. Figure 2 shows the importance
of UFOV within the context of a real-world driving scene.
Older adults also experience higher levels of disability glare than
younger adults, due to an increase in intraocular light scatter which
reduces visual acuity and contrast sensitivity, particularly in the
presence of cataracts [43]. Driving situations in which disability glare
may cause difficulties include at night from approaching headlights,
and at dawn and dusk from the low-sun. Accordingly, older drivers
with higher levels of disability glare self-regulate and reduce their
driving exposure, particularly at night [14]. While previous research
has failed to find significant links between disability glare and at-fault
crash-rates [17], there is some evidence that increased glare sensitivity
is linked with crash involvement in older drivers [11].
This is consistent with findings from a simulator study of older
adults which demonstrated poorer driving safety when performing
turns against on-coming traffic in the presence of glare, particularly
for low-contrast vehicles [44].
With the rise in eye diseases among older adults, and associated
reductions in visual functions, it is not surprising that many eye
diseases are linked with reduced driving performance and increased
crash risk. The most common eye conditions affecting older adults,
and their ability to drive safety, include cataracts, glaucoma and age-
related macular degeneration [45].
Many people live with cataracts for extended periods before cataract
removal [46], with around a quarter of these continuing to drive,
even if their vision does not meet the legal driving standards [47,48].
Drivers with cataracts report increased driving difficulties,
drive shorter distances and avoid challenging driving situations [46].
Despite limiting their driving exposure, drivers with cataracts have
2.5 times more crashes than controls [46], and as discussed above,
those involved in crashes are eight times more likely to have reduced
contrast sensitivity [17]. These findings are supported by closed
and open road studies, which have shown that drivers with either
simulated [49,50], or true cataracts [19,51,52], have impaired driving
performance compared to controls.
Cataract surgery has a positive impact on crash rates and driving
performance. A recent meta-analysis suggested that cataract surgery
is associated with a 88% reduction in the risk of driving-related
difficulties [53]. Crash rates for cataract patients who undergo surgery
were half those who did not have surgery [54]. Retrospective analysis
of population-linked data (1997-2006) demonstrated that cataract
surgery reduced crash risk by 13% with savings of $4.3 million [55].
Consistent with these findings, closed road driving performance
improved following bilateral cataract surgery, with the improvement
being best predicted by the change in better eye contrast sensitivity [56].
These studies provide compelling evidence that cataract surgery
can provide tangible benefits to road safety [54], and should be targeted
at an earlier rather than later stage to maintain safe driving.
Patients with glaucoma also report driving difficulties, including
problems with glare and night driving [57]. Glaucoma is cited as one
of the main reasons that older drivers give up driving [58]; patients
with bilateral glaucoma are three times more likely to cease driving
that those without glaucoma [59]. Glaucoma has been shown to
be an important risk factor for both self-reported crashes [60] and
state-recorded crashes [23,24,61,62]. Patients with moderate or severe
FIG. 2 Illustration of the importance of the Useful Field of View in a real-world driving situation.

Points de Vue - n°68 - Spring / Primavera - 2013 13
VISION OF SENIORS
Non-medical scientific
glaucomatous field loss were six times more likely to have an at-fault
crash and four times more likely to cause any crash than those with no
field loss [23], while people involved in injurious crashes were 3.6 times
more likely to have glaucoma than those who were crash-free [61].
The increased crash risk for drivers with glaucoma has also been linked
to their deficits in UFOV performance [24].
On-road assessment of glaucoma patients has highlighted problems
with lane-keeping, negotiating curves and anticipatory skills [26], and
they are more likely to have a driver instructor intervention during
on-road driving assessments compared to controls [63]. Early detection
and treatment of glaucoma is clearly critical, not just to minimise
irreversible visual field loss, but also to maintain safe driving ability.
Few studies have addressed the impact of age-related macular
degeneration (AMD) on driving, with most focussing on the self-
reported aspects of driving rather than objective measures of driving
performance and safety. Drivers with AMD report more difficulty
driving [64], self regulate their driving habits and avoid challenging
driving situations [16, 65], and exhibit less risk taking behaviours [66]
than drivers without AMD. While older adults with AMD exhibited
poorer driving performance on an interactive driving simulator
and an in-traffic road test [66], these impairments were not reflected
in higher crash rates [8]. The paucity of data in this area highlights
the need for further research to evaluate the extent to which AMD
impacts on driving performance and crash risk, and to identify
strategies to improve driver safety in this population.
One of the problems for older drivers is that changes in their vision
can occur gradually; they may thus be unaware that their vision
has become impaired until a driving incident occurs or they are
advised of visual changes following an eye examination.
It is unlikely that changes in visual ability relevant to driving will be
detected if high contrast acuity continues to be used to assess visual
performance for driver licensing. While recent evidence strongly
suggests that alternative measures of visual function, including
the UFOV, contrast sensitivity and motion sensitivity may be more
relevant to driving performance and safety, evaluation and validation
of these tests has yet to be completed. In addition, while there is
strong evidence linking the presence of ocular disease and driving
difficulties, further research is needed in order that appropriate
advice can be provided to older drivers with these conditions. •
REFERENCES
1. Burg A. The relationship between vision test scores and driving record: General findings. Los Angeles: Department of Engineering, University of California - Los Angeles; 1967:1-89.
2. Hofstetter HW. Visual acuity and highway accidents. J Am Optom Assoc 1976; 47:887-893.
3. Davison PA. Inter-relationships between British drivers’ visual abilities, age and road accident histories. Ophthalmic Physiol Opt 1985; 5:195-204.
4. Gresset J, Meyer F. Risk of accidents among elderly car drivers with visual acuity equal to 6/12 or 6/15 and lack of binocular vision. Ophthalmic Physiol Opt 1994; 14:33-37.
5. Marottoli RA, Richardson, E.D., Stowe, M.H., Miller, E.G., Brass, L.M., Cooney, L.M. & Tinetti, M.E. Development of a test battery to identify older drivers at risk for self-reported adverse driving events. J Am Geriatr Soc 1998; 46:562-568.
6. Ivers RQ, Mitchell P, Cumming RG. Sensory impairment and driving: The Blue Mountains eye study. Am J Public Health 1999; 89:85-87.
7. Decina LE, Staplin L. Retrospective evaluation of alternative vision screening criteria for older and younger drivers. Accid Anal Prev 1993; 25:267-275.
8. McCloskey LW, Koepsell TD, Wolf ME, Buchner DM. Motor vehicle collision injuries and sensory impairments of older drivers. Age Ageing 1994; 23:267-272.
9. Owsley C, Ball, K., McGwin, G., Sloane, M.E., Roenker, D.L., White, M.F. & Overley, T. Visual processing impairment and risk of motor vehicle crash among older adults. JAMA 1998; 279:1083-1088.
10. Keeffe JE, Jin CF, Weih LM, McCarty CA, Taylor HR. Vision impairment and older drivers: who’s driving? Br J Ophthalmol 2002; 86:1118-1121.
11. Rubin GS, Ng ES, Bandeen-Roche K, Keyl PM, Freeman EE, West SK. A prospective, population-based study of the role of visual impairment in motor vehicle crashes among older drivers: the SEE study. Invest Ophthalmol Vis Sci 2007; 48:1483-1491.
12. Cross JM, McGwin G, Jr., Rubin GS, et al. Visual and medical risk factors for motor vehicle collision involvement among older drivers. Br J Ophthalmol 2009; 93:400-404.
13. Ball K, Owsley C, Sloan ME, Roenker DL, Bruni JR. Visual attention problems as a predictor of vehicle crashes in older drivers. Invest Ophthalmol Vis Sci 1993;34:3110-3123.
14. Brabyn JA, Schneck ME, Lott LA, Haegerstrom-Portnoy G. Night driving self-restriction: vision function and gender differences. Optom Vis Sci 2005; 82:755-764.
15. Keay L, Munoz B, Turano KA, et al. Visual and cognitive deficits predict stopping or restricting driving: the Salisbury Eye Evaluation Driving Study (SEEDS). Invest Ophthalmol Vis Sci 2009; 50:107-113.
16. Ball K, Owsley C, Stavey B, Roenker DL, Sloane ME, Graves M. Driving avoidance and functional impairment in older drivers. Accid Anal Prev 1998; 30:313-322.
17. Owsley C, Stalvey BT, Wells J, Sloane ME, McGwin G, Jr. Visual risk factors for crash involvement in older drivers with cataract. Arch Ophthalmol 2001; 119:881-887.
18. Wood JM, Dique T, Troutbeck R. The effect of artificial visual impairment on functional fields and driving performance. Clin Vis Sci 1993; 8:563-575.
19. Wood JM. Age and visual impairment decrease driving performance as measured on a closed-road circuit. Hum Factors 2002; 44:482-494.
20. Wood JM, Owens DA. Standard measures of visual acuity do not predict drivers’ recognition performance under day or night conditions. Optom Vis Sci 2005; 82:698-705.
21. Johnson CA, Keltner JL. Incidence of visual field loss in 20,000 eyes and its relationship to driving performance. Arch Ophthalmol 1983; 101:371-375.
22. Council FM, Allen JA. A study of the visual fields of North Carolina drivers and theri relationship to accidents. Chapel Hill: University of North Carolina. Highway Research Saferty Centre.; 1974.
23. McGwin G, Jr., Xie A, Mays A, et al. Visual field defects and the risk of motor vehicle collisions among patients with glaucoma. Invest Ophthalmol Vis Sci 2005; 46:4437-4441.
24. Haymes SA, Leblanc RP, Nicolela MT, Chiasson LA, Chauhan BC. Risk of falls and motor vehicle collisions in glaucoma. Invest Ophthalmol Vis Sci 2007;48:1149-1155.
25. Wood JM, Troutbeck R. The effect of restriction of the binocular visual field on driving performance. Ophthalmic Physiol Opt 1992; 12:291-298.
26. Bowers A, Peli E, Elgin J, McGwin G, Owsley C. On-road driving with moderate visual field loss. Optom Vis Sci 2005; 82:657-667.
27. Racette L, Casson EJ. The impact of visual field loss on driving performance: evidence from on-road driving assessments. Optom Vis Sci 2005; 82:668-674.
28. Wood JM, McGwin Jr G, Elgin J, et al. On-road driving performance by persons with hemianopia and quadrantanopia. Invest Ophthalmol Vis Sci 2009;50:577-585.
29. Crabb DP, Fitzke FW, Hitchings RA, Viswanathan AC. A practical approach to measuring the visual field component of fitness to drive. Br J Ophthalmol 2004; 88:1191-1196.
30. Chisholm CM, Rauscher FG, Crabb DC, et al. Assessing visual fields for driving in patients with paracentral scotomata. Br J Ophthalmol 2008; 92:225-230.
31. Henderson S, Donderi DC. Peripheral motion contrast sensitivity and older drivers’ detection failure accident risk., Proceedings of the Third International Driving Symposium on Human Factors in Driver Assessment, Training and Vehicle Design. Rockport, Maine; 2005:41-50.
32. Henderson S, Gagnon S, Bélanger A, Tabone R, Collin C. Near peripheral motion detection threshold correlates with self-reported failures of attention in younger and older drivers. Accid Anal Prev 2010; 42:1189-1194.
33. Raghuram A, Lakshminarayanan V. Motion perception tasks as potential correlates to driving
difficulty in the elderly. Journal of Modern Optics 2006; 53:1343-1362.
34. Wood JM, Anstey KJ, Kerr GK, Lacherez P, Lord S. A multi-domain approach for predicting older driver safety under in-traffic road conditions. J Am Geriatr Soc 2008; 56:986-993.
35. Conlon E, Herkes K. Spatial and temporal processing in healthy aging: Implications for perceptions of driving skills. Aging, Neuropsychol Cog 2008; 15:446-470.
36. DeLucia PR, Mather R. Motion extrapolation of car-following scenes in younger and older drivers. Hum Factors 2006; 48:666-674.
37. Ball KK, Beard BL, Roenker DL, Miller RL, Griggs DS. Age and visual search: expanding the useful field of view. J Am Optom Assoc 1988;5:2210-2219.
38. Ball K, Owsley C. The useful field of view test: a new technique for evaluating age-related declines in visual function. J Am Optom Assoc 1992; 63:71-79.
39. Owsley C, Ball, K., Sloane, M.E., Roenker, D.L. & Bruni, J.R. Visual/cognitive correlates of vehicle accidents in older drivers. Psychol Aging 1991; 6:403-415.
40. Myers RS, Ball KK, Kalina TD, Roth DL, Goode KT. Relation of useful field of view and other screening tests to on-road driving performance. Percept Mot Skills 2000; 91:279-290.
41. Roenker DL, Cissell GM, Ball KK, Wadley VG, Edwards JD. Speed-of-processing and driving simulator training result in improved driving performance. Hum Factors 2003; 45:218-233.
42. Ball K, Roenker DL, Wadley VG, et al. Can high-risk older drivers be identified through performance-based measures in a Department of Motor Vehicles setting? J Am Geriatr Soc 2006; 54:77-84.
43. Elliott DB, Bullimore MA. Assessing the reliability, discriminative ability, and validity of disability glare tests. Invest Ophthalmol Vis Sci 1993; 34:108-119.
44. Gray R, Regan D. Glare susceptibility test results correlate with temporal safety margin when executing turns across approaching vehicles in simulated low-sun conditions. Ophthalmic Physiol Opt 2007; 27:440-450.
45. Wang JJ, Foran S, Mitchell P. Age-specific prevalence and causes of bilateral and unilateral visual impairment in older Australians: the Blue Mountains Eye Study. Clin Experiment Ophthalmol 2000; 28:268-273.
46. Owsley C, Stalvey B, Wells J, Sloane ME. Older drivers and cataract: drivng habits and crash risk. J Gerontol 1999; 54A:M203-M211.
47. Monestam E. Impact of cataract surgery. A population based approach. Acta Ophthalmol Scand 1999; 77:729.
48. Pager CK, McCluskey PJ, Retsas C. Cataract surgery in Australia: a profile of patient-centred outcomes. Clin Experiment Ophthalmol 2004; 32:388-392.
49. Wood JM, Troutbeck R. Effect of visual impairment on driving. Hum Factors 1994; 36:476-487.
50. Wood JM, Troutbeck R. Elderly drivers and simulated visual impairment. Optom Vis Sci 1995; 72:115-124.
51. Wood JM, Mallon K. Comparison of driving performance of young and old drivers (with and without visual impairment) measured during in-traffic conditions. Optom Vis Sci 2001; 78:343-349.
52. Wood JM, Carberry TP. Older drivers and cataracts: measures of driving performance before and after cataract surgery. Transportation Research Record 2004; 1865:7-13.
53. Subzwari S, Desapriya E, Scime G, Babul S, Jivani K, Pike I. Effectiveness of cataract surgery in reducing driving-related difficulties: a systematic review and meta-analysis. Inj Prev 2008; 14:324-328.
54. Owsley C, McGwin G, Jr, Sloane M, Wells J, Stalvey BT, Gauthreaux S. Impact of cataract surgery on motor vehicle crash involvement by older adults. JAMA 2002; 288:841-849.
55. Meuleners LB, Hendrie D, Lee AH, Ng JQ, Morlet N. The effectiveness of cataract surgery in reducing motor vehicle crashes: a whole population study using linked data. Ophthalmic Epidemiol 2012; 19:23-28.
56. Wood JM, Carberry TP. Bilateral cataract surgery and driving performance. Br J Ophthalmol 2006; 90:1277-1280.
57. Janz NK, Musch DC, Gillespie BW, Wren PA, Niziol LM. Evaluating clinical change and visual function concerns in drivers and nondrivers with glaucoma. Invest Ophthalmol Vis Sci 2009; 50:1718-1725.
58. Hakamies-Blomqvist L, Wahlstrom B. Why do older drivers give up driving? Accid Anal Prev 1998; 30:305-312.
59. Ramulu PY, West SK, Munoz B, Jampel HD, Friedman DS. Driving cessation and driving limitation in glaucoma: the Salisbury Eye Evaluation Project. Ophthalmology 2009; 116:1846-1853.
60. Tanabe S, Yuki K, Ozeki N, et al. The association between primary open-angle glaucoma and motor vehicle collisions. Invest Ophthalmol Vis Sci 52:4177-4181.
61. Owsley C, McGwin G, Ball K. Vision impairment, eye disease, and injurious motor vehicle crashes in the elderly. Ophthalmic Epidemiol 1998;5:101-113.
62. Hu PS, Trumble DA, Foley DJ, Eberhard JW, Wallace RB. Crash risks of older drivers: a panel data analysis. Accid Anal Prev 1998;30:569-581.
63. Haymes SA, Leblanc RP, Nicolela MT, Chiasson LA, Chauhan BC. Glaucoma and on-road driving performance. Invest Ophthalmol Vis Sci 2008; 49:3035-3041.
64. Mangione CM, Gutierrez PR, Lowe G, Orav EJ, Seddon JM. Influence of age-related maculopathy on visual functioning and health-related quality of life. Am J Ophthalmol 1999; 128:45-53.
65. Weaver Moore L, Miller M. Driving strategies used by older adults with macular degeneration: assessing the risks. Appl Nurs Res 2005; 18:110-116.
66. Szlyk JP, Pizzimenti CE, Fishman GA, et al. A comparison of driving in older subjects with and without age-related macular degeneration. Arch Ophthalmol 1995; 113:1033-1040.

Points de Vue - n°68 - Spring / Primavera - 201314
VISION OF SENIORS
Non-medical scientific
E N V I S I O N I N G T H E V I S I O N : U N D E R S T A N D I N G T H E V I S I O N
N E E D S F O R S E N I O R S
__ INTRODUCTION
Aging is a global phenomenon. By 2030, 55 countries are expected
to see people aged 60 and over make up at least 20 percent of their
total populations. There are more people aged 60 and older than the
entire populations of Russia, Japan, France, Germany and Australia
combined. Worldwide, there are 800 million people aged 60 and above,
By 2020, the global populations for 60 and older is projected to be
1 billion and by 2050, the number of people age 60 and older will
double to 2 billion with more than 1 in of 4 people aged 60 and older
in Europe, USA, and China. Population aging not only brings forth new
challenges but also some new opportunities. Current research on aging
populations reveals that the majority of the seniors are comfortable with
aging, are leading healthier and happy lives, have a positive attitude
and enjoy a busy life engaged in both indoor and outdoor activities.
Therefore, it is evident that society needs to provide a variety
of services in order for populations to age with a good quality of life.
__ VISION ISSUES AMONG YOUNG AND MATURE SENIORS
A recent survey from IPSOS – 2011[1] has shown that seniors
report vision issues mainly related to light conditions;
approximately 60% of the respondents (in the age group
of 60 and above) interviewed acknowledged experiencing vision
problems such as near vision difficulties in low light conditions,
sensitivity to bright light or problems with night vision.
Even with a good pair of corrective eyeglasses they encounter some
discomfort. Several respondents mentioned difficulty in reading small
print, for instance, reading instructions for use on medicines.
Many seniors also mentioned discomfort in reading due to low contrast,
for example, reading print on coloured backgrounds in magazines.
Additionally, most of the 60+ population admitted to experiencing
sensitivity to sunlight in the outdoor environment, and 17% of this age
group also affirmed to have been bothered from outside glare.
These symptoms are even higher when considering people who have
cataracts: before surgery, over 75% of the seniors suffer from several
of the above mentioned vision issues. Cataract surgery alleviates some
of these problems, but light sensitivity is still an uncorrected problem
and the mature age group, in an attempt to protect their eyes, end up
wearing sunglasses to lessen the adverse effect of light on their eyes.
__ PHYSIOLOGICAL CHANGES DUE TO AGING
Even though presbyopia stabilises at the age of 60, physical changes
can occur in almost every organ and can affect seniors‘ health and
lifestyle. Overall, the changes in later life entail a general slowing
down of all organ systems due to a gradual decline in cellular activity.
Along with a variety of physiological changes that accompany the aging
process, changes in the sensory (vision, hearing, skin sensitivity, taste
and smell) also occur[3]. About 65% of all people who are visually
impaired are aged 50 and older. With an increasing elderly population
in many countries, more people will be at risk of age-related visual
impairment[14]. Although visual impairment can be linked to neural
losses, the major decline is due to changes in the eye‘s optics [9,13].
In general, visual acuity decreases with age (from 10/10 to 6/10 from
65 to 90 years). This decrease is even more significant when the
NATHALIE BARSenior Market Research Manager Essilor InternationalFrance
BIDISHA RUDRAPh.D, Associate Director, Decision Science, Market Research & Analysis, Essilor of AmericaUSA
ANNE-CATHERINE SCHERLENPhD, Head of Research, Optics – Low Vision R&D, Vision Institute, Essilor InternationalFrance
FIG. 1 Night driving: loss of contrast sensitivity, glare.
VISION OF SENIORS
Non-medical scientific

Points de Vue - n°68 - Spring / Primavera - 2013 15
VISION OF SENIORS
Non-medical scientific
__ LOOKING AHEAD
In today’s times of technological advancements, the retired, elderly
population not only still feels young but also enjoys a much more active
life than their predecessor. Having good sight, good vision is really
the key to their continued productivity and overall well-being.
This will enable them to keep on doing their regular activities and also
stay independent.
In conclusion, it is not only crucial to detect pathological
and physiological issues experienced by the senior population, but
it is also very important to dedicate time to listen and understand
their daily visual needs. Following a detailed and thorough discussion
with seniors will help in providing necessary and effective solutions
which will allow them to enjoy the benefits of good vision leading
to a long, independent and comfortable life. •
contrast is low [10]. Indeed, the difficulty of reading in low light expressed
by the elderly is associated with a decline in spatial contrast sensitivity.
Retinal luminance in older eyes is reduced due to pupillary miosis
and the increased density of the crystalline lens [4,9]. There is also an
increased intraocular light scatter and increased optical aberrations
during the aging process [12]. Some studies also report that with aging,
neural cell density declines. By age 60-70 years old, the density
of rod photoreceptors and ganglion cell decreases dramatically
in the peri macula. Older adults require on average three times the
contrast of younger adults in order to determine a target. Although
major discomfort reported by seniors is the loss of visual performance
in low light, the first sign of retinal aging is the time it takes for dark
adaptation of the peripheral retina [6]. This scotopic sensitivity loss
is due to the slowed photopigment regeneration (rhodospin).
Older people feel more difficulty to adapt to changes in brightness
and this explains, the difficulties associated with night driving.
Visual performance declines during the time it takes for the retina
to process visual acuity, contrast sensitivity, attentional field and
motion perception are considerably slower to adapt [7,9]. With no available
remedy to these problems, elderly people simply avoid night driving.
On the other hand, the presence of too much light also strongly
penalizes the visual comfort of the elderly [8]. This time, the decrease
of the time regeneration of the cone visual pigment (called opsine)
of the central retina affects the recovery time in light [11,2].
The retina gets flooded with light which leads to a dazzled effect
on the eye, associated with several types of discomfort such as pain,
loss of contrast sensitivity and visual acuity. Time to visual recovery
depends on the age and on the duration of time exposed to light.
Natural aging affects several visual functions which adversely impact
the day-to-day life activities for an individual. It is also important
to note that the presence of visual pathology, such as cataract,
age related macular degeneration and glaucoma, will amplify the loss
of visual functions mentioned above. For example, the discomfort
related to the glare is amplified by the phenomenon of light
scattering in the eye caused by opacities (cataracts, for example) or
photoreceptor loss such as Age-related Macular Degeneration (AMD) [2].
FIG. 3 Aging effect of contrast sensitivity.
FIG. 2 Intraocular light scatter.
REFERENCES
1. Ipsos Public Affairs, Observatoire de la Maturité, 2011.
2. Aguirre RC, Colombo EM, Barraza JF. (2011) Effect of glare on reaction time for peripheral vision at mesopic adaptation. J Opt Soc Am A Opt Image Sci Vis. Oct 1; 28(10):2187-91.
3. Brabyn J, Schneck M, Haegerstrom-Portnoy G, Lott L. (2001) The Smith-Kettlewell Institute (SKI) longitudinal study of vision function and its impact among the elderly: an overview. Optom Vis Sci, 78:264-269.
4. Franssen L, Tabernero J, Coppens JE, van den Berg TJ. (2007) Pupil size and retinal straylight in the normal eye. Invest Ophthalmol Vis Sci. May; 48(5):2375-82.
5. He, W., Muenchrath M.N., Kowal, P (2012) Shades of Gray: A Cross-Country Study of Health and Well-Being of the Older Populations in SAGE Countries, 2007-2010.
6. Jackson, G. R., Owsley, C., & McGwin, G. Jr. (1999) Aging and dark adaptation. Vision Research, 39, 3975-3982.
7. Kaleem MA, Munoz BE, Munro CA, Gower EW, West SK. (2012) Visual characteristics of elderly night drivers in the Salisbury Eye Evaluation Driving Study. Invest Ophthalmol Vis Sci. Aug 3; 53(9):5161-7.
8. Mainster MA, Turner PL. (2012) Glare’s causes, consequences, and clinical challenges after a century of ophthalmic study. Am J Ophthalmol. Apr; 153(4):587-93.
9. Owsley, C. (2010) Aging and vision: review. Vision Research, Jul 1; 51(13):1610-22.
10. Schneck ME, Haegerström-Portnoy G. (2003) Practical assessment of vision in the elderly. Ophthalmol Clin North Am. Jun; 16(2):269-87.
11.Stringham JM, Garcia PV, Smith PA, McLin LN, Foutch BK. (2011) Macular pigment and visual performance in glare: benefits for photostress recovery, disability glare, and visual discomfort. Invest Ophthalmol Vis Sci. Sep 22; 52(10).
12. Van den Berg TJ, Franssen L, Coppens JE. (2009) Straylight in the human eye: testing objectivity and optical character of the psychophysical measurement. Ophthalmic Physiol Opt. May; 29(3): 345-50.
13. Werner, J. S., Schefrin, B. E., & Bradley, A. (2010) Optics and vision of the aging eye. In Handbook of optics. In M. Bass, J. M. Enoch, & V. Lakshminarayanan (Eds.). Vision and vision optics (Vol. 3, 3rd ed., pp. 14.11-14.38). New York: McGraw-Hill.
14. World Health Organisation, World report on disability 2011. ISBN 978 92 4 156418 www.who.int/disabilities/world_report/2011/en/index.html.
http://linkedage.com/read/facts
Points de Vue - n°68 - Spring / Primavera - 201316
BLUE LIGHT
Medical scientific
N E W D I S C O V E R I E SA N D T H E R A P I E S
I N R E T I N A L P H O T O T O X I C I T Y
__ INTRODUCTION
Age-related Macular Degeneration, AMD, is one of the major causes
of visual impairment in industrialised countries, along with diabetic
retinopathy and glaucoma. In the United States, AMD is considered
to be the cause of 54.4% of visual impairments and 22.9% of cases
of blindness [1]. It is estimated that in 2010, 9.1 million Americans
aged over 50 presented early-stage AMD [2] and that this number is set
to double by 2050, to reach 17.8 million. At least 12% of the American
and European populations aged over 80 is affected by advanced AMD [3-5].
Amongst risk facts for AMD identified in literature, sunlight is indicated
as being a factor that can cause cumulative damage to the retina.
The highest energy portion of the visible spectrum, at between
400nm and 500nm, also known as blue light, is incriminated here.
Ophthalmic appliances already claim to offer protection against blue
light. Spectacle lenses or intraocular implants mostly contain high-pass
filters that absorb a wide band of blue light. However, such unselective
filtering can lead to maladjustment of the eye‘s visual and non-visual
functions. Colour perception is disturbed, scotopic vision is limited
and the body clock of wake/sleep cycles, which is controlled by certain
wavelengths of blue light, is potentially thrown out of kilter.
The limited specificity of the filtering mechanisms in existence is due
to a lack of information concerning the relative toxicity to the retina
of each wave length within the visible spectrum. This is the reason
why Essilor International and the Vision Institute went into partnership
in 2008 in order to define the harmfulness of blue light to the retina
more clearly and develop more selective, protective filtering lenses.
__ LIGHT: A RISK FACTOR FOR AMD
Since the causes of AMD are currently poorly identified, there are
no efficient preventive and curative solutions. Numerous
epidemiological studies demonstrate a large variety of potential
risk factors. Although the first proven factors are age [5], tobacco
consumption [5-8] and lack of carotenoids [9], light is also being blamed
as probably playing a part in the prevalence of AMD [10-14].
One of the characteristics of AMD is the appearance of sub-retinal
deposits known as drusen [15, 16]. These deposits are made up of
lipofuscin, a product of the deterioration of the external segment
of the photoreceptors and of the visual pigment. Lipofuscin,
because of its photosensitising characteristics, is thought to be involved
in the retinal damage caused by exposure to light.
__ BLUE LIGHT: HOW DANGEROUS IS IT FOR THE RETINA?
In the retina, light is mainly absorbed by the visual pigments
contained in the external segments of the photoreceptors.
The visual pigments of vertebrates are made up of a transmembrane
protein, opsin, combined with a vitamin A derivative 11-cis-retinal.
In the rod photoreceptors, this visual pigment is rhodopsin.
Most ultraviolet radiation is naturally filtered by ocular tissues located
in front of the retina, particularly the cornea and the crystalline lens [17, 18].
The most energetic light that reaches the retina is therefore mainly blue
light, at between 400nm and 500nm. Because of its high energy level,
it induces and accelerates photochemical reactions and cellular damage
via the production of radical species that are highly reactive
in the presence of oxygen. In particular, the toxic potential of blue light
on the external retina acts at two cellular levels: photoreceptors and the
cells in the retinal pigment epithelium.
In the rod photoreceptors, absorption of a photon by rhodopsin causes
isomerisation and the release of the 11-cis-retinal as all-trans-retinal.
Free all-trans-retinal is not only toxic as a reactive aldehyde, it also
presents strong sensitivity to blue light [19, 20]. Under moderate light
exposure conditions, the all-trans-retinal is recycled continuously into
11-cis-retinal by the cells of the retinal pigment epithelium and does
not cause any danger to the cell. When exposure to light happens over
a longer or more intense period, the all-trans-retinal accumulates and
its activation by blue light may be the cause of oxidative stress which
damages the cellular components of the photoreceptors. This oxidative
stress is normally compensated for by the presence of the numerous
antioxidants in the retina. However, with age and certain genetic
and environmental factors, such as tobacco consumption or a diet
that is low in antioxidants, anti-oxidative defences are reduced [21, 22]
and can no longer compensate for the stress caused by prolonged
or intensive exposure to blue light.
The function of the cells in the retinal pigment epithelium is to ensure
renewal of the external segment of photoreceptors. They eliminate
the distal part of them by ingestion, or “phagocytosis”, whilst the
growth of these external segments occurs continuously [23]. When the
external segments are too damaged by oxidative stress, their membrane
components are difficult for the retinal pigment epithelium to break
down. Intracellular digestion is then incomplete and generates an
accumulation of residual granular bodies, in the form of lipofuscin.
The granules of lipofuscin contain a large amount of polyunsaturated fat,
a target for oxidation. The lipophilic extract of lipofuscin contains
a potential photosensitiser, which forms a triplet excited state with
a maximum of absorption in blue at 440nm [24, 25]. One of the components
of lipofuscin, A2E, has been identified as being involved in the
photosensitising nature of the lipid residue. The energy of the triplet
state is sufficient to be transferred and react with oxygen in the blood.
SERGE PICAUDPhD, Research director at INSERM Vision InstituteFrance© Inserm/L.Prat
EMILIE ARNAULTPhD, Head of Photobiology project at the Pierre et Marie Curie University, Vision InstituteFrance
BLUE LIGHT
Medical scientific

Points de Vue - n°68 - Spring / Primavera - 2013 17
BLUE LIGHT
Medical scientific
Photoactivation of the lipofuscin granules by blue light then generates
reactive oxygen species (superoxide, hydrogen peroxide, lipid hyperoxides
and malondialdehyde) [26, 27]. When the number of these species exceeds
the cellular defence capacity, the retinal pigment epithelium cells die by
apoptosis. Deprived of these support cells that provide their energy supply,
the photoreceptors deteriorate in turn, contributing to the loss
of vision diagnosed in patients suffering from AMD.
In conclusion, the suggested mechanism by which light is involved
in the appearance and progression of AMD may happen at two levels:
on the one hand in photoreceptors via absorption of blue light
by rhodopsin and then in the near ultraviolet blue by the all-trans-retinal,
and, on the other, in the retinal pigment epithelium via absorption
of blue by lipofuscin.
__ THE LIMITATIONS OF EXISTING STUDIES
The toxic effects of visible light and blue light in particular on the
retina have already been demonstrated experimentally on cellular [28-30]
and animal [31] models of degenerative retinal pathologies.
However, the studies performed to date have not enabled
characterisation of the respective toxicity of each wavelength. Also, they
suffer from certain limitations. In fact comparisons of results are difficult
from one study to another because units fluctuate between energetic
and visual units. Also, the illumination systems used are not calibrated
on the illumination of the light sources existing in our environment,
whether natural (the sun) or artificial (neon, LED, halogen, etc.) and
therefore do not reflect true conditions of exposure to light. Finally, none
of the illumination systems used to date enables step by step definition
of the toxic spectrum of light on the cells of the retina.
The only recurrent information is that the highest toxicity levels are
contained within the spectral interval [400nm; 500nm].
__ THE CONTRIBUTION MADE BY THE VISION INSTITUTE AND ESSILOR INTERNATIONAL
The objective of this contribution was, in partnership with Essilor
International, to establish a photobiology laboratory at the Vision
Institute, to enable us to define precisely the specific toxicity on the
retina of each wavelength in the blue section of the visible spectrum.
The first action taken involved the development of a cellular illumination
system. This enabled the production of visible wavelengths of very
narrow bandwidths and at given illumination in order to model the
desired luminous spectrum. The light source to which we are the most
exposed and which is the most intense is the sun and the work was
therefore carried out using, for each wavelength, radiation values relative
to the sun‘s spectrum.
The second direction for work involved development of a model
of cultured cells, reproducing in vitro the degeneration of retinal cells,
as observed in AMD, with the presence of a lipofuscin component: A2E.
__ EQUIPMENT AND METHOD
The system of illumination that has been developed is a multi-
wavelength generator used to illuminate the cells being cultured inside
an incubator. The light source comprises a set of light-emitting diodes
(LEDs), each connected to the incubator and the cells by means of
optical fibres. The range of wavelengths covered extends from 390nm
to 520nm in bandwidths of 10nm (fig.1). The whole unit can thus,
with each optical fibre, restrict illumination to 10nm of the spectrum
arriving in the retina.
In order to model the accumulation of lipofuscin in the retina,
cells cultured in pig‘s pigmentary epithelium were treated with various
concentration of A2E, one of the components of lipofuscin (fig. 2).
These cells were then exposed to a light bandwidth of 10nm
FIG. 1 View from above of a cell culture plate lit by various wavelengths, from 390 to 520nm.

Points de Vue - n°68 - Spring / Primavera - 201318
BLUE LIGHT
Medical scientific
for 18 hours. Six hours after exposure, the effects of the light on the
cells were characterised according to three parameters: the percentage
of live cells, apoptotic activity of the cells and the percentage of cells
undergoing necrosis.
__ RESULTS
Quantification of live cells shows that exposure to light leads to cell
death only when the cells have been treated with A2E (fig. 3).
This phototoxicity is shown by activation of an enzyme, caspase-3,
which is involved in programmed death processes (apoptosis).
On the other hand, we did not observe any cell necrosis under these
experimental conditions. Our results also show that the greater the
concentration of A2E, the greater the toxic effect of light. These results
demonstrate that an A2E dose-dependent effect exists, and therefore
probably one of lipofuscin too, in induction of phototoxicity.
This can be related to the influence of age in AMD, because it has been
observed that drusen and lipofuscin accumulate with age and are present
in greater quantities in elderly patients suffering from AMD [15, 16, 32, 33].
__ CONCLUSION AND PROSPECTS
The joint work carried out by the Vision Institute and Essilor
International has resulted in the establishment of an experimental
process using a cellular model of AMD to define the precise spectrum
of sunlight toxicity on the retina. These results provide information
of capital importance in terms of the need to be protected from highly
specific blue light wavelengths. It is important to note that these
wavelengths are also present in variable proportions in the various
sources of artificial light (neon, LED, xenon, halogen, etc.) and
that the potential effects of lengthy exposure should not be neglected.
This project supplies elements of understanding of the
physiopathological processes taking place in AMD, with the possibility
of therapeutic or preventative solutions for this major pathology.
This type of therapeutic solution could be extended to other retinal
pathologies involving oxidative stress processes leading to degeneration
of the photoreceptors, such as pigmentary retinitis and Stargardt‘s disease.
The association of the respective skills of the Vision Institute in terms
of the cellular biology of the retina, and of Essilor International in optics
was essential in setting up this innovative ophthalmological project. •
REFERENCES
1. Congdon, N., et al., Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol, 2004. 122(4): p. 477-85.
2. Rein, D.B., et al., Forecasting age-related macular degeneration through the year 2050: the potential impact of new treatments. Arch Ophthalmol, 2009. 127(4): p. 533-40.
3. Augood, C.A., et al., Prevalence of age-related maculopathy in older Europeans: the European Eye Study (EUREYE). Arch Ophthalmol, 2006. 124(4): p. 529-35.
4. Friedman, D.S., et al., Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol, 2004. 122(4): p. 564-72.
5. Smith, W., et al., Risk factors for age-related macular degeneration: Pooled findings from three continents. Ophthalmology, 2001. 108(4): p. 697-704.
6. Seddon, J.M., S. George, and B. Rosner, Cigarette smoking, fish consumption, omega-3 fatty acid intake, and associations with age-related macular degeneration: the US Twin Study of Age-Related Macular Degeneration. Arch Ophthalmol, 2006. 124(7): p. 995-1001.
7. Evans, J.R., A.E. Fletcher, and R.P. Wormald, 28,000 Cases of age related macular degeneration causing visual loss in people aged 75 years and above in the United Kingdom may be attributable to smoking. Br J Ophthalmol, 2005. 89(5): p. 550-3.
8. Khan, J.C., et al., Smoking and age related macular degeneration: the number of pack years of cigarette
smoking is a major determinant of risk for both geographic atrophy and choroidal neovascularisation. Br J Ophthalmol, 2006. 90(1): p. 75-80.
9. Ma, L., et al., Lutein and zeaxanthin intake and the risk of age-related macular degeneration: a systematic review and meta-analysis. Br J Nutr, 2012. 107(3): p. 350-9.
10. Butt, A.L., et al., Prevalence and risks factors of age-related macular degeneration in Oklahoma Indians: the Vision Keepers Study. Ophthalmology, 2011. 118(7): p. 1380-5.
11. Vojnikovic, B., et al., Epidemiological study of sun exposure and visual field damage in children in Primorsko-Goranska County--the risk factors of earlier development of macular degeneration. Coll Antropol, 2011. 34 Suppl 2: p. 57-9.
12. Fletcher, A.E., et al., Sunlight exposure, antioxidants, and age-related macular degeneration. Arch Ophthalmol, 2008. 126(10): p. 1396-403.
13. Mitchell, P., W. Smith, and J.J. Wang, Iris color, skin sun sensitivity, and age-related maculopathy. The Blue Mountains Eye Study. Ophthalmology, 1998. 105(8): p. 1359-63.
14. Darzins, P., P. Mitchell, and R.F. Heller, Sun exposure and age-related macular degeneration. An Australian case-control study. Ophthalmology, 1997. 104(5): p. 770-6.
15. Curcio, C.A. and C.L. Millican, Basal linear deposit and large drusen are specific for early age-related maculopathy. Arch Ophthalmol, 1999. 117(3): p. 329-39.
16. Sarks, S., et al., Relationship of Basal laminar
deposit and membranous debris to the clinical presentation of early age-related macular degeneration. Invest Ophthalmol Vis Sci, 2007. 48(3): p. 968-77.
17. Boettner, E.A. and J.R. Wolter, Transmission of the ocular media. Investigative Ophthalmology, 1962. 1(6).
18. Lund, D.J., et al., A Computerized Approach to Transmission and Absorption Characteristics of the Human Eye, in CIE 203:2012. 2012, International Commission on illumination. p. 68.
19. Rozanowska, M. and T. Sarna, Light-induced damage to the retina: role of rhodopsin chromophore revisited. Photochem Photobiol, 2005. 81(6): p. 1305-30.
20. Ng, K.P., et al., Retinal pigment epithelium lipofuscin proteomics. Mol Cell Proteomics, 2008. 7(7): p. 1397-405.
21. Kaya, S., et al., Comparison of macular pigment in patients with age-related macular degeneration and healthy control subjects - a study using spectral fundus reflectance. Acta Ophthalmol. 90(5): p. 399-403.
22. Raman, R., et al., Macular pigment optical density in a South Indian population. Invest Ophthalmol Vis Sci. 52(11): p. 7910-6.
23. Strauss, O., The retinal pigment epithelium in visual function. Physiol Rev, 2005. 85(3): p. 845-81.
24. Rozanowska, M., et al., Blue light-induced singlet oxygen generation by retinal lipofuscin in non-polar media. Free Radic Biol Med, 1998. 24(7-8): p. 1107-12.
25. Gaillard, E.R., et al., Photophysical studies on human retinal lipofuscin. Photochem Photobiol, 1995. 61(5): p. 448-53.
26. Boulton, M., et al., Lipofuscin is a photoinducible free radical generator. J Photochem Photobiol B, 1993. 19(3): p. 201-4.
27. Rozanowska, M., et al., Blue light-induced reactivity of retinal age pigment. In vitro generation of oxygen-reactive species. J Biol Chem, 1995. 270(32): p. 18825-30.
28. Sparrow, J.R., et al., Involvement of oxidative mechanisms in blue-light-induced damage to A2E-laden RPE. Invest Ophthalmol Vis Sci, 2002. 43(4): p. 1222-7.
29. Wood, J.P., et al., The influence of visible light exposure on cultured RGC-5 cells. Mol Vis, 2008. 14: p. 334-44.
30. Youn, H.Y., et al., Effects of 400 nm, 420 nm, and 435.8 nm radiations on cultured human retinal pigment epithelial cells. J Photochem Photobiol B, 2009. 95(1): p. 64-70.
31. Putting, B.J., et al., Blue-light-induced dysfunction of the blood-retinal barrier at the pigment epithelium in albino versus pigmented rabbits. Exp Eye Res, 1994. 58(1): p. 31-40.
32. Ahlers, C., et al., Imaging of the retinal pigment epithelium in age-related macular degeneration using polarization-sensitive optical coherence tomography. Invest Ophthalmol Vis Sci, 2010. 51(4): p. 2149-57.
33. Gehrs, K.M., et al., Age-related macular degeneration-emerging pathogenetic and therapeutic concepts. Ann Med, 2006. 38(7): p. 450-71.
Non-treated cells Cells + A2E
FIG. 2 Pig’s retinal pigment epithelium cells with or without treatment with A2E, one of the components of lipofuscin.
The cells’ nuclei are visible in blue and inter-cellular junctions are coloured red. On the left the A2E internalised by the cells is visible by autofluorescence in green when it is iluminated with blue light.
Dark Light
FIG. 3 Pig’s retinal pigment epithelium cells treated with A2E kept in the dark or exposed to light. On the left the cells kept in the dark are healthy because they are hexagonal in shape and will join to each other (at confluence).
On the contrary, exposure to light (on the right) causes cell death, visible from their rounded shape and reduced density.

Points de Vue - n°68 - Spring / Primavera - 2013 19
BLUE LIGHT
Medical scientific
T H E G O O D B L U E A N D C H R O N O B I O L O G Y :
L I G H T A N D N O N - V I S U A L
F U N C T I O N S
CLAUDE GRONFIERPh.D, Inserm U846, Stem Cell and Brain Research Institute, Department of Chronobiology, Lyon, France
__ INTRODUCTION
Over the past ten years there has been a wealth of discoveries in the
field of chronobiology. Since the discovery of a new retinal photoreceptor
in 2002 (melanopsin ganglion cells), shown to be involved in the
synchronisation of the circadian clock, it is now clear that the eye is
not for seeing only, it is also involved in a range of non-visual functions,
directly stimulated by light. The mechanisms involved are mainly yet
to be explored but all biological responses to photic stimulus show the way
to clinical applications of light in a range of disorders and pathologies,
from sleep to alertness, from cognition to memory and mood.
__ LIGHT AND THE CIRCADIAN BIOLOGICAL CLOCK
The link between light and the internal biological clock was discovered
in humans in 1980. The circadian clock (from the Latin circa “close
to” and dies “day”) is a physiological component that is essential to life
since it has been observed in almost all the living organisms that have
been studied, from prokaryotes through to humans [4].
Two fundamental properties characterise the circadian clock [4]:
1. Its rhythmic activity is endogenous. Located in the suprachiasmatic
nuclei (SCN) of the hypothalamus in mammals [7], its circadian electric
activity is supported by around ten clock genes whose cyclic activity
is responsible for the near 24-hour rhythm of each of its neurons [9].
2. Its activity must be synchronised to 24 hours. Its endogenous period
is actually close to but slightly different from a 24-hour period.
Therefore, the clock has to be synchronised (reset in time) in order to
enable its activity to be in phase with the solar day. In mammals, light
is the most powerful clock synchroniser, and its effect takes place solely
through the eye.
__ FUNCTIONS CONTROLLED BY THE CIRCADIAN CLOCK
Lots of physiological functions work according to circadian rhythm.
Figure 1 shows circadian control over several functions in humans.
The clock acts like an orchestra conductor, enabling the expression
of physiological activities at the right time. Alertness, cognitive
performance, memory, body temperature and blood pressure
are at their highest during day time (awake). On the contrary, secretion
of the hormone melatonin, muscle relaxation and sleep pressure
are at their highest during the night (sleep).
Many circadian biological activities have been discovered over the past
30 years, both in the periphery and at central level. Depending on the
tissue, between 8 and 20% of the genome is expressed rhythmically via
the endogenous clock.
The circadian system is involved in the control of cell division,
apoptosis in cancer [10] and in the repair of DNA [11]. Because of this,
these results can be used to understand how desynchronisation
of the circadian system could be responsible for the increased
prevalence of certain cancers in shift work [12].
The importance of the circadian system and its synchronisation
therefore appears to be crucial to human health.
FIG. 1 Diagram of the biological functions controlled by the circadian biological clock (non exhaustive list).
The structures indicated in colour are respectively in red: the suprachiasmatic nucleus, in orange: the pineal gland, in blue: the hypothalamus (containing the VLPO [ventrolateral preoptic area], known as the sleep switch), in beige: the brain stem (containing the ascending activator cortical pathway and the slow wave / paradoxical sleep sleep switch), in green: the thalamus (responsible for cortical activation and synchronisation of the EEG. (Modified diagram by Mignot et al. Nature 2002 [3] and Gronfier et al. 2012 [6]).
Mood
Cognitive performances
Autonomic nervous system
Motor activity
Memory
Hormones
Peripheral clocks
Cell cycle
Sleep
LIGHT
BIOLOGICAL CLOCK
Hypothalamus
Brain stem
Pineal gland - Melatonin
PVN
Cortex
Thalamus
BLUE LIGHT
Medical scientific

Points de Vue - n°68 - Spring / Primavera - 201320
BLUE LIGHT
Medical scientific
__ THE CONSEQUENCES OF CIRCADIAN DESYNCHRONISATION
In humans the importance of synchronisation is clear in symptoms
of “jet lag” or in night work (20% of the population in industrialised
countries). A lack of synchronisation of the clock is generally translated
by a change in numerous physiological functions (sleep, alertness,
cognitive performance, cardio-vascular system, immune systems [4,13,14]),
the deterioration of neurocognitive processes (cognitive performance,
memory) and a disturbance of sleep and alertness [15].
These changes are also found, chronically, in night workers, elderly
patients, blind people, in certain psychiatric pathologies and in certain
degenerative diseases of the central nervous system (Alzheimer‘s and
Parkinson‘s disease [16]). Chronobiological disorders associated with
these normal or pathological conditions have major socio-economic
consequences since they can lead to a fall in the general state of health
and to an increase in associated pathological risks.
The French Society of Occupational Medicine has just published
a report under the aegis of the High Health Authority (Haute Autorité
de Santé) on the consequences of shift work, including
recommendations for detecting them and ways in which
to minimise them [17].
__ ENDOGENIC PROPERTY OF THE CIRCADIAN CLOCK
In light conditions that are unsuitable for the synchronisation
of the circadian system, the endogenous clock functions according
to a rhythm that is no longer that of a 24 hour day.
In this case it expresses its own endogenic rhythmicity (period).
Just like a mechanical clock that has not been adjusted to time
regularly, the circadian clock loses time or runs fast, depending
on the individual (according to the length of the period of their own
clock) in the absence of any synchronisation by the environment.
This phenomenon, known as “free run”, is observed in blind people
in whom the absence of any light means that the biological clock
cannot synchronise to the 24-hour period [18]. This explains why about
75% of blind people complain that their sleep is not of good quality
and consult their doctors for recurrent sleep disorders [19].
It should be noted that the length of the clock‘s period is a highly
precise individual characteristic. It does not vary with age in adults [20],
but is relatively flexible during childhood and adolescence (lengthening
of the period in adolescence could explain in part the late-to-bed
factor, or even disorder of the delayed phase type observed
in the 15-25 age range [21]).
Thanks to the use of strictly controlled experimental protocols [20],
it has been possible to demonstrate that the length of the clock period
in humans is very close to 24 hours (24.2 hours on average [20]).
One of the direct impacts of the endogenous period in everyday life
is the chronotype. Individuals with a short period (a fast clock)
are generally those who go to bed early (morning chronotypes)
whereas people who go to bed late (evening chronotypes) have a longer
period (a slower clock) [22].
__ SYNCHRONISATION OF THE CLOCK
Because the endogenic period is close to, but not exactly, 24 hours,
the circadian clock must be constantly synchronised to 24 hours.
In mammals it is light that is the most powerful synchroniser
of the internal clock.
The term synchronisation of the biological clock corresponds,
just as with a wrist watch, to setting the time, whether the watch
is running fast or slow, in order to get it back into phase with the
environment. For an “evening” individual, whose endogenic period
is 24 hrs and 30 mins, the clock has to be put forward by 30 minutes
every day in order to be synchronised to 24 hours, if not it will be
another 30 minutes late every day. On the other hand, in a “morning”
person, whose period is 23 hrs and 30 mins, the circadian clock
has to be delayed by an average of 30 minutes every day.
Animals have different synchronisers, which are less efficient in humans.
They are known as “non photic” synchronisers because they do not
involve light. Eating and physical exercise have a synchronising effect
on the human clock but this is not very strong.
Studies carried out in the fifties had led researchers to believe that
social synchronisers were more powerful than light in Humans [23].
We now know that this is not the case.
The best proof that non-photic synchronisers have, if anything,
an extremely limited effect, has been obtained from the observation
that the vast majority of blind people – with no perception of light –
are in a state of non synchronised “free run”, despite a social life
and activities set out according to the 24-hour period (work, going
to bed / rising, eating meals, physical and intellectual activities, etc.).
The hormone melatonin is the only non-photic synchroniser
for which the effect on the human circadian clock is without a doubt [24].
It should be considered as a priority approach in the treatment
of “free run” in blind people.
__ CIRCADIAN PHOTORECEPTION
Until recently it was accepted that the cones and rods of the external
retina were the only photoreceptors responsible for the transduction of
light information to the endogenic clock. Studies carried out since the
year 2000 in both humans and animals show that two retinal systems
are involved in circadian photoreception (fig. 2):
LIGHT Visual structures
MelanopsinipRGCs Non-visual pathway
Circadian clock(SCN)
Cones - Rods
FIG. 2 Diagram of the eye (section) with an enlarged representation of the retina (in the centre).
Surrounding light is perceived by the retina. The cones and rods project towards visual structures (perceptive vision). Melanopsin ganglion cells are involved in the regulation of biological rhythms via their projection towards the suprachiasmatic nucleus (modified image by webvision and Gronfier et al. [1]).

Points de Vue - n°68 - Spring / Primavera - 2013 21
BLUE LIGHT
Medical scientific
(10000 lux) [32]. A stimulus given at the same time for the same length
of exposure, with a light intensity of 100 lux, i.e. 10% of the maximum
intensity tested, produces a delay of about 1 hour, i.e. 50% of the
maximum observed [32]. Recent studies show that the circadian clock is
actually particularly sensitive to low light intensities, and that exposure
to a LED computer screen (between 40 and 100 lux) for 2 hours
partially inhibits melatonin secretion, activates alertness, and delays
the biological clock and sleep onset [33].
The effect of the light depends on its spectrum. As shown in figure 3,
the circadian system is at maximum sensitivity to a coloured light of
between 460-480nm [34]. A monochromatic blue light (wavelength
480nm) can be as efficient on the circadian system as a fluorescent
white light 100 times more intense (comprising 100 times more
photons). This property is based on the sensitivity of melanopsin
ganglion cells.
Finally, the effect of light depends on the time at which it is perceived.
The phase response graph shows that the light to which we are exposed
in the evening and at the beginning of the night (on average between
5pm and 5am) has the effect of delaying the clock, whereas light
received at the end of the night and in the morning
(on average between 5am and 5pm) has the reverse effect of advancing
the clock [54]. It is this specific temporal sensitivity that explains the
clock‘s daily synchronisation under normal circumstances and its non-
synchronisation in the presence of jet-lag and night work.
__ LIGHT AND NON-VISUAL FUNCTIONS
Since the discovery of melanopsin ganglion cells in the retina 10 years
ago, a range of non-visual, light-sensitive functions have been described.
These functions involve anatomical pathways and cerebral structures
1. The photoreceptors involved in conscious vision (cones and rods).
2. The intrinsically photosensitive retinal ganglion cells: (ipRGC) involved
in a large number of non-visual functions [25]. In the absence of these
2 systems, the circadian system is “blind” in rodents and functions
in “free run”, expressing its endogenic rhythmicity [26]. It is currently
thought that the light information responsible for synchronisation
of the biological clock passes through the melanopsin ganglion cells,
either by stimulating these cells directly or by stimulating them
indirectly through cones and rods. Because of this fact, it is now
considered that the eye is not used for vision only,
but that it possesses both visual and non-visual functions (fig. 2 and 4).
The two types of photoreceptors in the external and internal retina are
phylogenetically and functionally different. Unlike cones and rods,
melanopsin ganglion cells require high illuminances and show
a peak of sensitivity at around 480nm (in all the mammals studied).
These rhabdomeric type cells also show the property of bistability,
which makes them virtually insensitive to bleaching [29].
These photoreceptors are currently the subject of a great deal
of research, aimed at developing methods for treating certain
chronobiological disorders (including disorders of the circadian rhythms
of sleep and seasonal affective disorders), which could be faster
and more efficient than the current methods which use fluorescent
white lights [29].
The circadian system’s response to light depends on photic characteristics. The effect of light on the clock depends on the intensity
of light and how long it lasts. The more intense the light stimulus[30],
and/or the longer it lasts[31], the greater the effect. For example,
nocturnal exposure to light lasting for 6.5 hours leads to a delay of more
than 2 hours in the melatonin rhythm when intense white light is used
480 nm1,0
0,8
0,6
0,4
0,2
0,0
Rela
tive
Sens
ibili
ty
400 450 500 550 600 650 700
Wavelength (nm)
SW
mel
rods
MW
LW
Melatonin suppression
FIG. 3 The spectral sensitivity of standard photoreceptors (cones SW, MW, LW and rods) and of melanopsin (mel) in Humans (Najjar et al. [2]).
The sensitivity of the circadian system in Humans (estimated by the suppression of melatonin – black dots) is optimal at ~480 nm, corresponding to the peak of sensitivity of melanopsin. Cones and rods are involved in circadian photoreception but their relative contribution is unknown.
SerotoninRaphe
Visual structuresLGN, SC
DopamineVTA
Pupilary reflexOPN
RewardLH
Motor activitySPZ
Circadian clockSCN
Sleep/wake switchVLPO
MoodAmygdala
CognitionMemoryHypothalamus
FIG. 4 The retinal melanopsin ganglion cells project towards a range of structures involved in the regulation of the circadian system (SCN), pupil reflex (OPN), motor activity (vSPZ, IGL), sleep (VLPO) and alertness (LC). These projection pathways are the non-visual pathways of light. Modified diagram by [5,8].

Points de Vue - n°68 - Spring / Primavera - 201322
BLUE LIGHT
Medical scientific
that are different to those involved in vision, and do not lead to the
formation of images (fig. 4). Studies in animals [35] show projections
of melanopsin ganglion cells towards structures involved in the
regulation of biological rhythms, the regulation of alertness and sleep
states, the regulation of locomotor activity, the pupil reflex, etc.
In humans, studies show that melanopsin ganglion cells, via non-visual
pathways, are involved in the effect of light on the resetting of melatonin
phase [36], the increase in alertness, body temperature and heart rate [37],
expression of the PER2 gene [38], resetting of the rhythm of the PER3
gene [39], the increase in psychomotor performances and EEG activity [40],
sleep structure [41], and activation of cerebral structures involved
in memory and mood regulation [42-51]. Light, via non-visual retinal
projections, will therefore directly stimulate the cerebral structures
involved in the control of alertness, sleep, mood and cognitive and
psychomotor performances.
Before the identification of two anatomical pathways (visual and non-
visual), it has been known since 1995 that some blind people
who do not have any conscious visual perception can have a light-
sensitive circadian system [52]. The visual system of these patients
is blind, but their non-visual functions (including their circadian clock)
are not blind and receive photic information. These cases are probably
rare (very few individuals have been studied worldwide) and the majority
of patients with ocular pathologies leading to partial or total privation
of photic information have an increased prevalence of sleep and
biological rhythm disorders (their circadian rhythms are most often
expressed through “free run” and this clinical condition is associated
with sleep disorders in over 75% of cases [19]). Nevertheless,
ophthalmologists should be aware of the eye‘s non-visual function
and its importance in the synchronisation of the circadian system.
In view of the risk of adding a blind circadian system (and the free-run
symptoms with their associated treatments) to a defective vision,
the non-visual sensitivity to light should be evaluated prior
to enucleation of a blind patient.
__ CONCLUSIONS
In view of the importance of the circadian system synchronisation
and the nature of the non-visual functions, light appears to be a
biological requirement essential to health. It is predictable that light
will be used in the future in the treatment of numerous normal
or pathological conditions, in which a physiological malfunction
will be corrected through activation of the eye‘s non-visual functions. •
REFERENCES
1. Gronfier, C. Consequences and physiological effects of light: Sleep and biological clock in night and shift work. Arch. Mal. Prof. Environ. 70, 253-261 (2009).
2. Najjar, R., et al. Aging of non-visual spectral sensitivity to light: compensatory mechanisms? Under Review
3. Mignot, E., Taheri, S. & Nishino, S. Sleeping with the hypothalamus: Emerging therapeutic targets for sleep disorders. Nat. Neurosci 5 Suppl, 1071 (2002).
4. Dunlap, J.C., Loros, J.J. & DeCoursey, P.J. Chronobiology: Biological Timekeeping, (Sinauer, 2004).
5. Do, M.T. & Yau, K.W. Intrinsically photosensitive retinal ganglion cells. Physiol Rev 90, 1547-1581 (2010).
6. Taillard, J. & Gronfier, C. Circadian and homeostatic control of sleep (Regulation homeostasique et circadienne du sommeil). in Sleep Disorders (Les troubles du Sommeil), Da (eds), Elsevier, 2012. (ed. Elsevier) 25-43 (2012).
7. Moore, R.Y. & Eichler, V.B. Loss of a circadian adrenal corticosterone rhythm following suprachiasmatic lesions in the rat. Brain Research 42, 201-206 (1972).
8. Hattar, S., et al. Central projections of melanopsin-expressing retinal ganglion cells in the mouse. J Comp Neurol 497, 326-349 (2006).
9. Reppert, S.M. & Weaver, D.R. Coordination of circadian timing in mammals. Nature 418, 935-941 (2002).
10. Granda, T.G., et al. Circadian regulation of cell cycle and apoptosis proteins in mouse bone marrow and tumor. Faseb J 19, 304-306 (2005).
11. Collis, S.J. & Boulton, S.J. Emerging links between the biological clock and the DNA damage response. Chromosoma 116, 331-339 (2007).
12. (2010), I. Painting, firefighting, and shiftwork. IARC Monogr Eval Carcinog Risks Hum 98, 9-764 (2010).
13. Brandenberger, G., Gronfier, C., Chapotot, F., Simon, C. & Piquard, F. Effect of sleep deprivation on overall 24 h growth-hormone secretion. The Lancet 356, 1408-1408 (2000).
14. Spiegel, K., Leproult, R. & Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 354, 1435-1439 (1999).
15. Wright Jr, K.P., Hull, J.T. & Czeisler, C.A. Relationship between alertness, performance, and body temperature in humans. Am J Physiol Regul Integr Comp Physiol 289, R1370 (2002).
16. Vezoli, J., et al. Early presymptomatic and long-term changes of rest activity cycles and cognitive behavior in a MPTP-monkey model of Parkinson’s disease. PLoS ONE 6, e23952 (2011).
17. Travail, S.F.d.M.d. Surveillance médico-professionnelle des travailleurs postés et/ou de nuit. Recommandation de Bonne Pratique (Label HAS). (2012).
18. Miles, L.E., Raynal, D.M. & Wilson, M.A. Blind man living in normal society has circadian rhythms of 24.9 hours. Science 198, 421-423. (1977).
19. Leger, D., Guilleminault, C., Defrance, R., Domont, A. & Paillard, M. Blindness and sleep patterns. Lancet 348, 830 (1996).
20. Czeisler, C.A., et al. Stability, precision, and near-24-hour period of the human circadian pacemaker. Science 284, 2177-2181 (1999).
21. Roenneberg, T., et al. A marker for the end of adolescence. Curr Biol 14, R1038-1039 (2004).
22. Duffy, J.F., Rimmer, D.W. & Czeisler, C.A. Association of intrinsic circadian period with morningness-eveningness, usual wake time, and circadian phase. Behav Neurosci 115, 895 (2001).
23. Aschoff, J. Human circadian rhythms in activity, body temperature and other functions. Life Science Space Research 5, 159 (1967).
24. Arendt, J. & Rajaratnam, S.M. Melatonin and its agonists: an update. Br J Psychiatry 193, 267-269 (2008).
25. Berson, D.M., Dunn, F.A. & Takao, M. Phototransduction by retinal ganglion cells that set the circadian clock. Science 295, 1070-1073 (2002).
26. Hattar, S., et al. Melanopsin and rod-cone photoreceptive systems account for all major accessory visual functions in mice. Nature 424, 75-81 (2003).
27. Dacey, D.M., et al. Melanopsin-expressing ganglion cells in primate retina signal colour and irradiance and project to the LGN. Nature 433, 749-754 (2005).
28. Dkhissi-Benyahya, O., Gronfier, C., De Vanssay, W., Flamant, F. & Cooper, H.M. Modeling the role of mid-wavelength cones in circadian responses to light. Neuron 53, 677-687 (2007).
29. Mure, L.S., et al. Melanopsin bistability: a fly’s eye technology in the human retina. PLoS One 4, e5991 (2009).
30. Zeitzer, J.M., Dijk, D.J., Kronauer, R., Brown, E. & Czeisler, C. Sensitivity of the human circadian pacemaker to nocturnal light: melatonin phase resetting and suppression. J Physiol 526, 695-702. (2000).
31. Chang, A.M., et al. Human responses to bright light of different durations. J Physiol 590, 3103-3112 (2012).
32. Zeitzer, J.M., Dijk, D.J., Kronauer, R.E., Brown, E.N. & Czeisler, C.A. Sensitivity of the human circadian pacemaker to nocturnal light: Melatonin phase resetting and suppression. J Physiol 526, 695-702 (2000).
33. Chellappa, S.L., et al. Non-visual effects of light on melatonin, alertness and cognitive performance: can blue-enriched light keep us alert? PLoS ONE 6, e16429 (2011).
34. Brainard, G.C., et al. Action spectrum for melatonin regulation in humans: Evidence for a novel circadian photoreceptor. J Neurosci 21(16), 6405 (2001).
35. Gooley, J.J., Lu, J., Fischer, D. & Saper, C.B. A broad role for melanopsin in nonvisual photoreception. Journal of the Neurological Sciences 23, 7093-7106 (2003).
36. Lockley, S.W., Brainard, G.C. & Czeisler, C.A. High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength light. J Clin Endocrinol Metab 88, 4502-4505 (2003).
37. Cajochen, C., et al. High sensitivity of human melatonin, alertness, thermoregulation, and heart rate to short wavelength light. J Clin Endocrinol Metab 90, 1311-1316 (2005).
38. Cajochen, C., et al. Evening exposure to blue light stimulates the expression of the clock gene PER2 in humans. Eur J Neurosci 23, 1082-1086 (2006).
39. Ackermann, K., Sletten, T.L., Revell, V.L., Archer, S.N. & Skene, D.J. Blue-light phase shifts PER3 gene expression in human leukocytes. Chronobiol Int 26, 769-779 (2009).
40. Lockley, S.W., et al. Short-wavelength sensitivity for the direct effects of light on alertness, vigilance, and the waking electroencephalogram in humans. Sleep 29, 161-168 (2006).
41. Munch, M., et al. Wavelength-dependent effects of evening light exposure on sleep architecture and sleep
EEG power density in men. Am J Physiol Regul Integr Comp Physiol 290, R1421-1428 (2006).
42. Carrier, J., et al. Sleep slow wave changes during the middle years of life. Eur J Neurosci (2011).
43. Vandewalle, G., et al. Spectral quality of light modulates emotional brain responses in humans. Proc Natl Acad Sci U S A 107, 19549-19554 (2010).
44. Vandewalle, G., Maquet, P. & Dijk, D.J. Light as a modulator of cognitive brain function. Trends Cogn Sci 13, 429-438 (2009).
45. Vandewalle, G., et al. Functional magnetic resonance imaging-assessed brain responses during an executive task depend on interaction of sleep homeostasis, circadian phase, and PER3 genotype. J Neurosci 29, 7948-7956 (2009).
46. Schmidt, C., et al. Homeostatic sleep pressure and responses to sustained attention in the suprachiasmatic area. Science 324, 516-519 (2009).
47. Vandewalle, G., et al. Brain responses to violet, blue, and green monochromatic light exposures in humans: prominent role of blue light and the brainstem. PLoS ONE 2, e1247 (2007).
48. Vandewalle, G., et al. Robust circadian rhythm in heart rate and its variability: influence of exogenous melatonin and photoperiod. J Sleep Res 16, 148-155 (2007).
49. Vandewalle, G., et al. Wavelength-dependent modulation of brain responses to a working memory task by daytime light exposure. Cereb Cortex 17, 2788-2795 (2007).
50. Vandewalle, G., et al. Daytime light exposure dynamically enhances brain responses. Curr Biol 16, 1616-1621 (2006).
51. Perrin, F., et al. Nonvisual responses to light exposure in the human brain during the circadian night. Curr Biol 14, 1842-1846 (2004).
52. Czeisler, C.A., et al. Suppression of melatonin secretion in some blind patients by exposure to bright light. New Eng J Med 332, 6 (1995).
53. Sack, R.L., Lewy, A.J., Blood, M.L., Keith, L.D. & Nakagawa, H. Circadian rhythm abnormalities in totally blind people: Incidence and clinical significance. J. Clin. Endocrinol. Metab. 75, 127 (1992).

Points de Vue - n°68 - Spring / Primavera - 2013 23
BLUE LIGHT
Non-medical scientific
L I G H T E M I T T I N GD I O D E S ( L E D S )
A N D T H E B L U E L I G H T R I S K
BLUE LIGHT
Non-medical scientific
__ THIS ARTICLE PRESENTS AN OVERVIEW OF THE KNOWLEDGE regarding the potential toxicity of light emitted by LEDs on the retina. Due to their
high brightness and their emission spectrum containing a significant
fraction of blue light, the so-called “blue light hazard” has been
considered and studied for several years. Several independent studies
carried out by health agencies have shown that the risk posed by LEDs
used as general lighting sources is low, but cannot be neglected in the
case of some sensitive populations, considering the increasing optical
performances of LEDs and their fast mass market distribution.
Traditional lighting sources such as the well-known incandescent
lamp and the compact fluorescent lamp are rapidly being replaced by
products based on light emitting diodes (LED) (fig. 1). The so-called
“solid-state lighting” (SSL) presents many advantages such as longer
lifetime, reduced energy consumption and lower environmental impact.
Many governments have therefore started to progressively ban older
lighting technologies, paving the way for the massive usage of LEDs
in the general lighting market. As a matter of fact, leaders of the
lighting industry believe that over 90% of all lighting sources in the
world will be based on SSL products and LEDs by 2020.
As any new and emerging technologies, SSL products should
be proven to be at least as safe as the products they intend
to replace. Furthermore, some unique properties of LEDs such
as their compactness have generated many new lighting applications
for which older technologies could not be employed. For instance,
some kinds of toys and clothes now incorporate LEDs. The safety of
products using LEDs should be assessed considering the interactions
with the human body in existing and new ways of using them.
The potential adverse effects of optical radiation on the skin and
on the eyes are known as photobiological hazards. LEDs currently used
in lighting applications have the advantage of emitting a negligible
amount of ultraviolet (UV) and infrared (IR) radiation 1.
The only photobiological hazards to consider when assessing the safety
of LEDs are linked to visible light, and more particularly the blue part
of the spectrum.
Several health agencies such as ANSES 2 and SCENIHR 3 have
investigated and reviewed the scientific literature on photobiological
hazards related to the use of LEDs. Two key features of LEDs have
drawn the attention of experts:
• LEDs are very bright small sources of visible light, which can be
glaring. Due to their high brightness, LEDs also have very high radiance
CHRISTOPHE MARTINSONSHead of Lighting and Electromagnetism Division, Department of Health and Comfort Centre Scientifique et Technique du Bâtiment - CSTB GrenobleFrance
1 As they emit negligible amounts of UV and IR, LEDs should not be expected to contribute to the onset of photokeratitis and cataract.2 Agence nationale de sécurité sanitaire de l’alimentation, de l’environnement et du travail (French National Agency for Food, Environmental and Work Safety).3 Scientific Committee on Emerging and Newly Identified Health Risks.
FIG. 1 Photographs of several types of solid-state lighting products.
a: Directional luminaire (spot light) using an LED.
b: SSL lamp based on three LEDs and used to replace an incandescent lamp.
c: Outdoor high power SSL luminaire using 121 LED modules.
d: Typical single LED component, used in many SSL products. This type of LED consumes about 1 W of electricity and generates a luminous flux of about 100 lm. Its luminance can be as high a 107 cd/m².
c d
ba

Points de Vue - n°68 - Spring / Primavera - 201324
BLUE LIGHT
Non-medical scientific
4 International Commission for Non-Ionising Radiation Protection.
(a photometric quantity expressing the “concentration” of light),
which in turn produces a high illuminance level upon the retina.
• The vast majority of white LEDs producing white light rely on a chip
emitting blue light associated with layers of fluorescent materials
(luminophores) to produce longer wavelengths. As a consequence,
the emission spectrum of a white LED consists in a narrow primary
blue peak and a large secondary peak in the yellow-orange-red part
of the spectrum. The two peaks are separated by a region of very low
emission in the blue-green part of the spectrum (fig. 2).
__ RISKS RELATED TO BLUE LIGHT
Visible light on the retina can cause thermal damage and
photochemical damage. The exposure levels needed to result in
thermal damage on the retina cannot be met with light emitted by
LEDs of current technologies. The photochemical risk is associated
with blue light retinal illuminance. Due to the high brightness of
LEDs, the retinal illuminance levels are potentially high and must be
carefully considered. In general, the photochemical damage of the
retina depends on the accumulated dose to which the person has been
exposed, which can be the result of a high intensity short exposure
but can also appear after low intensity exposures repeated over long
periods. Blue light is recognised as being harmful to the retina, as a
result of cellular oxidative stress.
Blue light is also suspected to be a risk factor in age-related macular
degeneration (ARMD).
Retinal blue light exposure can be estimated using the ICNIRP 4
guidelines. A quantity called the blue-light weighted radiance LB can
be estimated as a function of the viewing distance and the exposure
time. Maximum permissible exposure values (MPEs) were set by
ICNIRP to provide limits for LB as a function of exposure time.
For the past three years, blue light exposure data about LEDs have
been provided by LED manufacturers and professional lighting
associations but also by independent laboratories and governmental
agencies.
It was found that the retinal blue light exposure levels LB produced
at a distance of 200mm from the user by blue and cold-white LEDs
(bare LEDs and LEDs equipped with a focusing lens) exceed the MPE
limits set by ICNIRP after an exposure time comprised between
a few seconds for high power blue LEDs to a few tens of seconds
for high power cold-white LEDs. As a consequence, the potential
toxicity of some LED components viewed at short distances cannot be
neglected. However, when the viewing distance is increased to one
metre, the maximum permissible exposure time rapidly increases
to a few thousands of seconds, up to a few tens of thousands
of seconds. These very long exposure times provide a reasonable safety
margin to assert that there is virtually no possible blue light retinal
damage caused by LEDs at longer viewing distances (statement valid
for state of the art LEDs at the time of writing).
Several classes of products and applications based on bare LEDs
or LEDs covered by a focusing lens (collimator) are directly related
to a potentially high level of retinal blue light exposure when short
viewing distances are possible. Examples are (but are not limited to):
• Tests and adjustments of high power blue and cold white LEDs
by operators in lighting manufacturing facilities or by lighting installers
• Toys using LEDs, given that the higher degree of transparency of the
crystalline lens of children makes them more susceptible to higher
blue light retinal exposures
• Automotive LED daytime running lights when activated near children
and other sensitive subjects
• Some types of directional LED lamps sold for home applications.
These lamps can be viewed from distances as short as 200mm
FIG. 2 The blue curve represents the typical emission spectrum of a white LED. The blue peak reaches its maximum value at about 435nm.
It corresponds to the primary light generated by the LED semiconducting structure itself (the LED die). The secondary peak reaches a maximum value at 550nm (yellow colour) and is the secondary light emitted by luminophores excited by the blue light (fluorescence). The combination of the direct blue light and the yellow/red secondary light produces white color.
The red curve is a plot of the blue light retinal phototoxicity function. It reaches a maximum value at wavelengths corresponding to the blue light peak emitted by LEDs.
380 430 480 530 580 630 680 730 780
Wavelength (nm)
1,0
0,9
0,8
0,6
0,5
0,4
0,3
0,2
0,1
0,0
Arbi
trary
Uni
ts

Points de Vue - n°68 - Spring / Primavera - 2013 25
BLUE LIGHT
Non-medical scientific
The conclusions drawn for single LED components or LED modules
cannot be extended to all SSL applications because the photobiological
safety of a final SSL product must be assessed independently of its
LED components. As a matter of fact, the LB value of an SSL product
is generally very different from the LB value of the LED components
that it uses. For instance, a higher LB can be obtained with a lamp
using an assembly of low LB LEDs. Reversely, a lower LB can be
obtained with a lamp using a diffuser in front of a high LB LED.
For all LEDs and products using LEDs, a photobiological blue light risk
assessment must be carried out to determine whether or not the MPEs
can be exceeded in the conditions of usage. Such risk assessments
can be performed by test laboratories specialised in light sources
photometry such as CSTB 5 and LNE 6 in France.
The main tool used to perform photobiological risk assessment is the
CIE 7 S009 publication whose content was included in an international
standard (IEC 62471) and other national standards (IESNA RP27,
JIS C8159, etc.).
__ THE PHOTOBIOLOGICAL SAFETY STANDARD IEC 62471
This standard deals with the photobiological safety of lamps
and devices using lamps and includes a classification of the light
source in several risk groups. The standard considers all of the
photobiological hazards that may affect the skin and the eye (thermal
and photochemical hazards) from ultraviolet to infrared wavelengths.
Four risk groups are defined: Risk Group 0 (RG0, no risk), Risk Group
1 (RG1, low risk), Risk Group 2 (RG2, moderate risk), Risk Group 3
(RG3, high risk). The risk group depends on the maximum permissible
exposure time (MPE time) assessed at a given viewing distance.
__ RISK ASSESSMENTS METHODOLOGY
IEC 62471 defines two different criteria to determine the viewing
distance. Light sources used in general lighting should be assessed
at a distance corresponding to an illuminance of 500 lx. Other types
of light sources should be assessed at a fixed distance of 200mm.
For LED components, there is no ambiguity in the distance since
LED components are not used per se in general lighting. In this case,
IEC 62471 requires using the distance of 200mm. The application
of the IEC 62471 measurement technique at 200mm leads to RG2
classification (moderate risk) for some high power blue and cold white
LEDs.
However, the choice of the viewing distance in IEC 62471 is sometimes
ambiguous and not realistic in the context of the real usage conditions.
For instance, in the case of stage lighting (theatres, concert halls)
where artists are exposed to an illuminance level higher than 500 lx.
Applying the 500 lx criterion would underestimate the exposure while
the 200mm criterion would largely overestimate it. In a more usual
situation, directional household lamps fall under the 500 lx criterion,
which corresponds to a typical viewing distance of a few metres.
It is however quite common to have shorter viewing distances,
as short as 200 or 500mm at home. Another example is street lighting
where the illuminance level is much lower than 500 lx, typically
a few tens of lx. Assessing the exposure to blue light emitted
by a street lighting luminaire at the distance giving an illuminance
of 500 lx is clearly not appropriate. A future revision of IEC 62471
should bring a more accurate definition of the distance at which
the risk group is determined.
It is interesting to note that the strict application of CIE S009
and IEC 62471 to indoor LED lamps and luminaires lead to RG0
and RG1 classifications, similar to traditional indoor light sources
(fluorescent lamps, incandescent and halogen lamps). Nevertheless,
when the 200mm viewing distance is chosen, several measurement
campaigns reveal that a small number of indoor LED lamps and
luminaires belonged to RG2 while traditional indoor light sources
(fluorescent and incandescent) were still in RG0 or RG1.
This result shows that LED technology potentially raises the blue
light risk in home applications where the viewing distance is not limited
and light sources are accessible to children and other sensitive people.
At the time of publication, the general public remains unaware
of potential risks to the eye since no mandatory labeling system
is currently in place for consumer SSL products.
The notion of a safety distance would actually be more appropriate to
communicate to installers and to users, especially the general public.
The safety distance of an SSL product would be the minimum distance for
which the blue light hazard risk group does not exceed RG1. Measurement
campaigns carried out by several laboratories showed that the vast majority
of indoor LED lamps and luminaires have a safety distance of 200mm
which is compatible with most lighting applications.
It is important to note that other widely used lighting sources,
particularly high intensity discharge lamps used for outdoor lighting are
in RG2 (moderate risk). However, these lamps are intended for clearly
identified uses and can only be installed by professionals who should
be aware of the safety distance required to limit the exposure.
__ OTHER LIMITATIONS OF IEC 62471 AND CIE S009 AND SENSITIVE POPULATIONS
The maximum exposure limits defined by the ICNIRP and used
to define the Risk Groups in both IEC 62471 and CIE S009 are not
appropriate for repeated exposures to blue light as they were calculated
for a maximum exposure in one 8-hour day. They do not take into
account the possibility of exposure over an entire lifetime.
Neither CIE S009 nor IEC 62471 takes into account the sensitivity
of certain specific population groups, which can be characterised
by an accrued sensitivity to visible light:
• People having pre-existing eye or skin conditions for which artificial
lighting can trigger or aggravate pathological symptoms
• Aphakic (people with no crystalline lens) and pseudophakic people
(with artificial crystalline lenses) who consequently either cannot or
can only insufficiently filter short wavelengths (particularly blue light)
• Children
• Elderly people as their eyes are more sensitive to optical radiation
The photobiological standards for lighting systems should be extended
to cover children and aphakic or pseudophakic individuals, taking
into account the corresponding phototoxicity curve published by the
ICNIRP in its guidelines.
In addition to proven photochemical damage of the retina resulting
from acute exposure to blue light, uncertainty still remains surrounding
the effects of chronic exposure at low doses. These effects are
still being investigated by ophthalmologists, biologists and optical
scientists.
In France, the RETINALED project 8 is investigating the effects
of chronic low exposure of rodents to light emitted by LEDs.
5 Centre Scientifique et Technique du Bâtiment (French Technical and Scientific Research Center on Construction and Buidling).6 Laboratoire National de Métrologie et d’Essais (National Testing and Metrology Laboratory).7 Commission Internationale de l’Eclairage (International Commission on Illumination).8 The RETINALED project is carried out by INSERM, CSTB and ENVA. It is supported by ADEME (French Environmental and Energy Management Agency).

Points de Vue - n°68 - Spring / Primavera - 201326
BLUE LIGHT
Non-medical scientific
Certain categories of workers are exposed to high doses of artificial
light (long exposure times and/or high retinal illuminances) during their
daily activities (examples: lighting professionals, stage artists, etc.).
Since the damage mechanisms are not fully understood yet, exposed
workers should use appropriate individual means of protection as a
precautionary measure (glasses filtering out blue light for instance).
__ CONCLUSIONS
Due to their unique light emission properties, LEDs are currently on
the verge of becoming the dominant lighting source of this century.
However, the risks posed by these new sources of light are also rooted
in their intrinsic characteristics: high optical output in a small package
(producing a high radiance level) associated with a significant blue
light emission. The combination of these two factors can potentially
increase the risk of photochemical damage of the retina, in comparison
with the incandescent lamp and the fluorescent lamp.
Lighting industry leaders are well aware of the photobiological safety
of their products. Many lighting products using LEDs now emit warmer
shades of white light (reduction of the blue light content in the
spectrum) or use diffusers to reduce glare (reduction of the radiance).
Most lighting products are found to present low risks or no risk at all
for the general population when the viewing distance is equal to or
greater than 200mm.
However, measurement campaigns carried out by independent
agencies pointed out a few lighting products with significantly higher
risk levels below a distance of one metre or more. At the present time,
no mention is made by lighting manufacturers of a “safety distance”.
It is therefore impossible for the public to identify lamps or luminaires
with a higher risk level.
The blue light risk assessment related to LEDs can be performed
by test laboratories using the IEC 62471 standard which is not
perfectly clear about the viewing distance to consider. In addition,
this standard does not consider sensitive populations such as children,
aphakic, pseudophakic and elderly people, despite the fact that these
populations are exposed to a higher level of blue light on the retina.
The current knowledge of the mechanisms of blue light phototoxicity
is far from being complete. The effects of chronic exposure and
accumulated low exposure over very long periods of time are still an
active subject of research. As far as LEDs are concerned, the better
comprehension of the possible long term effects of the blue light
on the retina is fundamental to guaranteeing that the “LED revolution”
will not compromise our vision of the future. •
REFERENCES
F. Behar-Cohen, C. Martinsons, F. Viénot, G. Zissis, A. Barlier-Salsi, J.P. Cesarini, O. Enouf, M. Garcia, S. Picaud, D. Attia, Light-emitting diodes (LED) for domestic lighting: Any risks for the eye?, Progress in Retinal and Eye Research, Volume 30, Issue 4, July 2011, Pages 239-257.
« Effets sanitaires des systèmes d’éclairage utilisant des diodes électroluminescentes (LED) », Saisine n°2008-SA-0408, Rapport d’expertise collective de l’Agence Nationale de Sécurité Sanitaire de l’Alimentation, de l’Environnement et du Travail (ANSES), www.anses.fr
“Health Effects of Artificial Light”, Opinion of the Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR), European Commission, March 2012, ISSN 1831-4783, http://ec.europa.eu/health/scientific_committees/policy/index_en.htm
EN 62471, European Standard, “Photobiological Safety of Lamps and Lamp Systems”, 2008.
BIOGRAPHY
Christophe Martinsons received a Ph.D in Physics from the University
of Reims Champagne-Ardenne in 1998. Up to 2000, he held a research
scientist position at the National Physical Laboratory (NPL).
From 2000 to 2007, he worked in the field of home automation for
the HAGER Group. In 2007, he joined CSTB to head the Lighting,
Electricity and Electromagnetism division.
He currently conducts research and consultancy work in the field of
combined daylighting and artificial lighting in order to promote energy-
efficiency in buildings while providing the best visual comfort conditions
for users. His approach to lighting is put forward in the new French
building energy code (RT 2012).
For the past four years, Christophe Martinsons has been leading
laboratory measurement campaigns for French governmental agencies
while working on independent studies concerning health and
environmental aspects of solid-state lighting and LEDs.

Points de Vue - n°68 - Spring / Primavera - 2013 27
BLUE LIGHT
Non-medical scientific
400 500 600 700
Cone
Spe
ctra
l Sen
sitiv
ity
Wavelength (nm)
P E R C E P T I O N O F B L U EA N D S P E C T R A L F I L T E R I N G
__ INTRODUCTION
The sky is blue. Physicians give us an explanation for this:
it is due to the preponderance of short wavelengths in the light
diffused by the atmosphere. But why do we see it blue?
Seeing the world in colour and identifying its characteristics
requires processing of the image formed by the distribution of photons
on the retina.
__ 1. HOW IS THE COLOUR SENSE CREATED?
First we need to remember the various stages involved
in how colour vision works.
The photons reaching the retina are absorbed by photoreceptors:
cones for daytime vision and rods for vision when the light is dim,
and very often both cones and rods if light is slightly reduced.
The photoreceptors generate a signal when they capture a photon,
whatever the wavelength involved. Due to very extensive spectral
sensitivity in the field of wavelengths, almost all the photoreceptors
are able to absorb short wavelength photons. It is only the rate
of absorption that differentiates them. So, “S” cones (improperly
named “blue”) are preferentially sensitive to short wavelengths
of around 450nm, “M” cones (“green”), to medium wavelengths
of around 540nm, “L” cones (“red”), to around 570nm,
and rods to around 507nm. However, the probability exists
that, for example, a 450nm photon hitting the retina is absorbed
by a photoreceptor other than an “S” cone.
Immediately on exit, the photoreceptors signals are
recombined, and it is mainly contrast signals, of luminous
or spectral origin, that enter the numerous visual paths
in the retina. As for the retinal signals that head for the cortex,
they are subject again to several recombinations, of variable
importance, before resulting in the colour sense. In general,
in these recombinations, signals from all the cone groups come
into play, with variable importance. Colour is therefore
an appearance attribute, constructed by our visual system.
It is the tone that essentially characterises the colour
of materials, and its definition is exceptionally stable
within our natural environment. This phenomenon of relative
stability is known as colour constancy.
With regard to the effect of spectral filtering, we note that:
In practice, every group of photoreceptors can be stimulated
at short wavelengths.
An imbalance in the signals generated in cones can lead
to a change in the contrasts perceived and a disturbance in colour
perception which is not radical, however, as long as the three cone
groups remain intact.
__ 2. SPECIFIC CHARACTERISTICS OF BLUE VISION
In colour vision, blue, or more exactly the retinal pathway of signals
issuing from the “S” cones, has a particular status. These signals
contribute only slightly to luminous contrast at high spatial or temporal
FRANÇOISE VIÉNOTNational Natural History Museum (MNHN), Collection Conservation Research Centre (CRCC) Paris France
BLUE LIGHT
Non-medical scientific
FIG. 1 Spectral sensitivity of the three groups of retinal cones.

Points de Vue - n°68 - Spring / Primavera - 201328
BLUE LIGHT
Non-medical scientific
frequencies. Because of this fact, neither acuity nor sensitivity to
flicker is based on these signals. We even speak of foveal tritanopia
or small field tritanopia to indicate the reduction of colour vision due
to the inability of “S” cones to process certain colour contrasts.
On the other hand, “S” cone signals contribute massively
to the distinction of colours and play an essential role in identifying
shades of colours. For example the difference between yellow or white,
or the distinction between warm white or cold white lights, is based
on the response of “S” cones.
In summary, in terms of spectral filtering: A strong reduction in signals from “S” cones should not affect acuity,
but could lead to deterioration in the distinction of shades of colour
and change colour sense.
But as long as a few “S” cone signals, even weak signals,
pass through into the networks of retinal neurons, modifications
to colour often go unnoticed.
__ 3. WHAT WOULD BE THE IMPACT OF A BREAK IN VISIBLE SHORT WAVELENGTHS?
As long as the three groups of cones can maintain activity,
colour vision, which is based on contrasts, is possible. So, everything
depends on the position of the break in the visible spectrum.
A break at around 450nm, which leaves a gap at the entrance in “S”
cones of almost 50% of the available photons, will have only a low
impact on colour vision. Moreover, this is what happens naturally with
ageing and cataract. The sky remains blue through until advanced old
age. The effect of perceptive constancy, and in this case of “colour
constancy”, stabilises the colours of materials in the environment,
each in relation to the others, whatever the light variations.
If the break happens at around 500nm, a marked deterioration
in the distinction of shades of colour is foreseeable in blue-green
and purples, as well as for certain colour pairs such as yellow
and white or dark blue and black. Acuity should be preserved.
On the other hand, in night vision, the subject may suffer from
a notable lack of light.
__ CONCLUSION
Any kind of spectral filtering leads to perception deficiency.
Although colour distinction is always weakened, higher functions,
that is to say the appearance and recognition of colours,
are actually well preserved. In terms of colour, the visual response
adjusts to the environment. As long as the light is polychromatic,
the physiological adaptation capacities of humans compensate
for a deficiency of light at source. •
REFERENCES
Peter Gouras (2009) Color Visionhttp://webvision.med.utah.edu/book/part-vii-color-vision/color-vision/
J. D. Mollon (1989) “Tho’ she kneel’d in that Place where they Grew”. J. exp. Biol. 146, 21-38
F. Viénot, J. Le Rohellec (2012) Colorimetry and physiology: the LMS specification. In : C. Fernandez-Maloigne, F. Robert-Inacio, L. Macaire, Digital color. Acquisition, Perception, Coding and Rendering Digital Signal and Image Processing Series, ISTE, Wiley, pp. 1-27.
FIG. 2 Illustration of the difficulty in perceiving certain colour details that are based on a variation in the signal from “S” or “blue” cones. Whereas the surface occupied by the letters in the words “Points de Vue” is less than the surface area of the rectangle, the latter stands out more.

Points de Vue - n°68 - Spring / Primavera - 2013 29
PRODUCT
The two images must be of good quality and have a high degree
of resemblance (fig. 2) so that the brain can analyse their similarities
and differences in order to merge them into a unique, three dimensional
perception. This process is known as binocular vision.
Binocular vision not only enables one to see but also improves visual
performance compared to monocular performance; this is thanks
to the phenomenon of binocular summation [1, 2].
Requirements for good binocular vision
According to Castro et al. [3], binocular summation is optimal when
both eyes have the same level of optical quality. The authors have used
the Strehl ratio as an indicator of the eye’s optical quality, and show
that there is a statistically significant correlation between binocular
summation and difference from the Strehl ratio between the two eyes
(fig. 2).
Thus, when the two eyes have the same level of optical quality,
binocular summation is higher, whatever the age of the patient.
Cyclopean eye and binocular visual direction
Like the Cyclops in Greek mythology, although our two eyes each
receive and analyse an image of the surrounding world, in binocular
vision we see a single image from a virtual point of view known as the
Cyclopean eye.
V A R I L U X S S E R I E S ™ :4 D T E C H N O L O G Y ™
P E R S O N A L I S E D B I N O C U L A R C A L C U L A T I O N
B A S E D O N T H E D O M I N A N T E Y E
PRODUCT
Until now binocular vision has not been taken completely into
consideration in any progressive lens. And yet respecting the various
aspects of binocular vision, whatever the prescriptions for both eyes,
is necessary for optimal visual perception. Further, the dominant eye
plays a highly specific role in the ocular pair. Taking this parameter into
account enables us to improve the wearer’s binocular visual performance
still further. For the very first time 4D TechnologyTM enables these
various parameters to be taken into account in the calculation
of progressive lenses.
__ BINOCULAR VISION: THE PHYSIOLOGICAL BASIS
Human beings have two eyes separated by a short distance in space,
such that a large part of the visual field is perceived simultaneously from
different points of view. The two retinas transmit disparate monocular
images to the cortex via visual pathways (fig. 1).
HÉLÈNE DE ROSSILAURENT CALIXTEDAMIEN PAILLEISABELLE POULAINR&D Optique, Essilor Saint Maur, France
FIG. 1 Cortical mechanism of binocular vision.
FIG. 2 Binocular summation a function of the differences of optical quality between the two eyes (Castro et al. 2009).
Interocular differences in Strehl ratio
Bino
cula
r Sum
mat
ion
1.55
1.50
1.45
1.40
1.35
1.30
1.25
1.20
1.15
0.00 0.01 0.02 0.03 0.04 0.05 0.06
r 2 = 0,80p < 0.01
Observed scene
Right eye retinal image
Left eye retinal image
Visual Cortex
Perceived scene
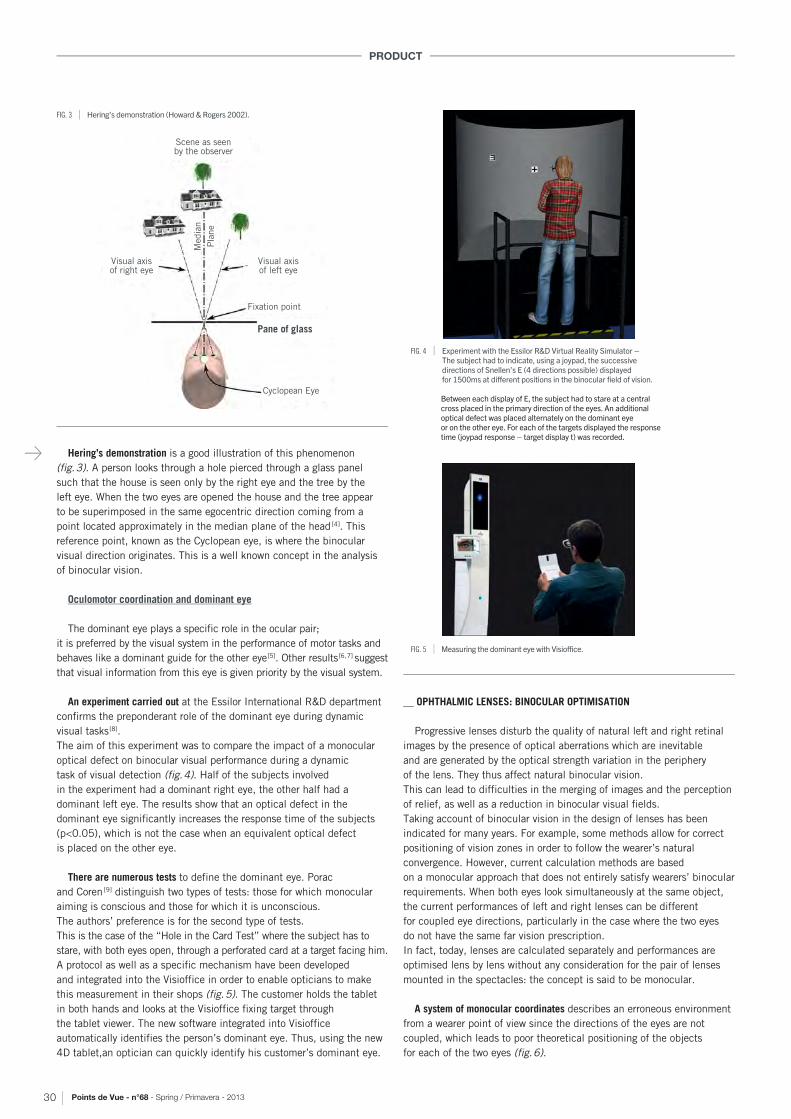
Points de Vue - n°68 - Spring / Primavera - 201330
PRODUCT
Hering’s demonstration is a good illustration of this phenomenon
(fig. 3). A person looks through a hole pierced through a glass panel
such that the house is seen only by the right eye and the tree by the
left eye. When the two eyes are opened the house and the tree appear
to be superimposed in the same egocentric direction coming from a
point located approximately in the median plane of the head [4]. This
reference point, known as the Cyclopean eye, is where the binocular
visual direction originates. This is a well known concept in the analysis
of binocular vision.
Oculomotor coordination and dominant eye
The dominant eye plays a specific role in the ocular pair;
it is preferred by the visual system in the performance of motor tasks and
behaves like a dominant guide for the other eye [5]. Other results [6, 7] suggest
that visual information from this eye is given priority by the visual system.
An experiment carried out at the Essilor International R&D department
confirms the preponderant role of the dominant eye during dynamic
visual tasks [8].
The aim of this experiment was to compare the impact of a monocular
optical defect on binocular visual performance during a dynamic
task of visual detection (fig. 4). Half of the subjects involved
in the experiment had a dominant right eye, the other half had a
dominant left eye. The results show that an optical defect in the
dominant eye significantly increases the response time of the subjects
(p<0.05), which is not the case when an equivalent optical defect
is placed on the other eye.
There are numerous tests to define the dominant eye. Porac
and Coren [9] distinguish two types of tests: those for which monocular
aiming is conscious and those for which it is unconscious.
The authors’ preference is for the second type of tests.
This is the case of the “Hole in the Card Test” where the subject has to
stare, with both eyes open, through a perforated card at a target facing him.
A protocol as well as a specific mechanism have been developed
and integrated into the Visioffice in order to enable opticians to make
this measurement in their shops (fig. 5). The customer holds the tablet
in both hands and looks at the Visioffice fixing target through
the tablet viewer. The new software integrated into Visioffice
automatically identifies the person’s dominant eye. Thus, using the new
4D tablet,an optician can quickly identify his customer’s dominant eye.
__ OPHTHALMIC LENSES: BINOCULAR OPTIMISATION
Progressive lenses disturb the quality of natural left and right retinal
images by the presence of optical aberrations which are inevitable
and are generated by the optical strength variation in the periphery
of the lens. They thus affect natural binocular vision.
This can lead to difficulties in the merging of images and the perception
of relief, as well as a reduction in binocular visual fields.
Taking account of binocular vision in the design of lenses has been
indicated for many years. For example, some methods allow for correct
positioning of vision zones in order to follow the wearer’s natural
convergence. However, current calculation methods are based
on a monocular approach that does not entirely satisfy wearers’ binocular
requirements. When both eyes look simultaneously at the same object,
the current performances of left and right lenses can be different
for coupled eye directions, particularly in the case where the two eyes
do not have the same far vision prescription.
In fact, today, lenses are calculated separately and performances are
optimised lens by lens without any consideration for the pair of lenses
mounted in the spectacles: the concept is said to be monocular.
A system of monocular coordinates describes an erroneous environment
from a wearer point of view since the directions of the eyes are not
coupled, which leads to poor theoretical positioning of the objects
for each of the two eyes (fig. 6).
FIG. 4 Experiment with the Essilor R&D Virtual Reality Simulator – The subject had to indicate, using a joypad, the successive directions of Snellen’s E (4 directions possible) displayed for 1500ms at different positions in the binocular field of vision.
Between each display of E, the subject had to stare at a central cross placed in the primary direction of the eyes. An additional optical defect was placed alternately on the dominant eye or on the other eye. For each of the targets displayed the response time (joypad response – target display t) was recorded.
FIG. 5 Measuring the dominant eye with Visioffice.
FIG. 3 Hering’s demonstration (Howard & Rogers 2002).
Visual axis of right eye
Scene as seen by the observer
Visual axis of left eye
Media
n
Pla
ne
Fixation point
Cyclopean Eye
Pane of glass

Points de Vue - n°68 - Spring / Primavera - 2013 31
PRODUCT
Binocular Optical Target
Left Lens
Right Lens
Optimal for sighting
dominant eye
Step 2 Step 3
Sighting Dominant Eye
ERC Cyclopean Eye
Step 1
(αBino,
3D Environment Binocular reference system
Performance of lenses in binocular
reference system
Right Eye
Right Lens
Left Lens
Left Eye
Cyclopean Eye
(αBino, OBino
ERC
Nasal
Nasal
Temporal
Temporal
ERC
ERC
3D Environment Monocular reference system
ERC
ERC
ORight OLeft
Right Eye
Left Eye
α
α
β
β
Since each eye is considered separately from the other, a monocular
eye direction (�,�) does not correspond to the same object point for each
eye (ORight and OLeft). The gap between these two points in the object
space ORight and OLeft is greater the bigger the difference between the
prescriptions for the two eyes.
The result is an inexact calculation of the optical characteristics
of each of the lenses (strength, astigmatism, gradients, etc.).
Binocular marker and Cyclopean eye
To have a true representation of the environment, it is necessary
to establish a system of binocular coordinates, originating in the
Cyclopean eye (fig. 7). We can then define the relationship between each
object in the environment observed by both eyes simultaneously and the
corresponding pair of left and right eye directions. The eye directions for
each pair are said to be “equivalent” or “coupled”
- (�R �R and (�L �L – because they are used simultaneously
by the wearer to look at the same object. They correspond to a virtual
binocular eye direction (�Bino, �Bino) linked to the Cyclopean eye.
The optical performances of each lens can then be analysed according
to these new binocular references. On the right of figure 7 are shown
the astigmatism performances of two lenses calculated by monocular
concept. The binocular performances of the two lenses are different.
Thus, the right and left images, which form on the corresponding
retinas, have a different optical quality. Merging of the images
is not optimal. The result is also narrower binocular fields of vision.
4D TechnologyTM: binocular calculation that takesaccount of the dominant eye
Binocular calculation used in 4D TechnologyTM consists of adjusting
performances between the two lenses such that the optical qualities
of the left and right retinal images corresponding to the coupled
eye directions are similar whilst ensuring optimal vision for the dominant
eye (fig. 8).
To achieve this, a unique new binocular optical design is defined
for the two lenses in the pair. It is built up, amongst other things,
from the prescriptions for the two eyes and information about the
dominant eye. For each binocular visual direction, a range of binocular
criteria is thus defined and expresses the binocular physiological
requirements of wearers. Definition of this new binocular design
is based on the know-how we have acquired from the evaluation tests
we continually carry out on wearers.
Each lens is them optimised to ensure that optical performances
achieve the binocular optical design thus defined.
The method, which takes the dominant eye into account in the
definition of performance and ensures right left performance symmetry
in the binocular coordinates systems, means that optimal binocular
performance can be achieved whilst improving speed of detection
in wider binocular fields of vision.
__ CONCLUSION
Binocular calculation implemented in 4D TechnologyTM favours
the dominant eye with the aim of preserving its role whilst minimising
the optical quality differences between the two eyes. The wearer retains
good image qualities for both eyes and binocular vision is improved
as well as dynamic vision performance. •
FIG. 8 4D Technology binocular calculation.
REFERENCES
1. Cagenelleo R, Arditi A, Halpern D.L. Binocular enhancement of visual acuity. J. Opt. Soc. Am. A. 1993 ; 10(8): 1841-1848.
2. Legge G.E. Binocular contrast summation. I. Detection and discrimination. Vis. Res. 1984 ; 24: 373-383.
3. Castro J.J, Jiménez J.R, Hita E, Ortiz C. Influence of interocular differences in the Strehl ratio on binocular summation. Ophthalmic Physiol Opt. 2009 ; 29(3):370-374.
4. From Ono, H. Binocular wVisual Directions of an Object when Seen a s Single or Double, in Regan D (ed). Binocular Vision Vol 9 pp.9-12 in Vision and Visual Dysfunction, 1991.
5. Kawata H, Ohtsuka K. Dynamic asymmetries in convergence eye movements under natural viewing conditions. Jpn J Ophthalmol. 2001 ; 45(5):437-44.
6. Minucci P.K, Conners M. M. Reaction time under three viewing conditions: Binocular, dominant eye and nondominant eye. J Exp Psychol. 1964 ; 67:268-275.
7. Shneor E, Hochstein S. Eye dominance effects in conjunction search. Vision research. 2008 ; 48: 1592-1602.
8. Poulain I, Marin G, Baranton K, Paillé D. The Roleof Sighting Dominant Eye during Target saccades, Arvo annual meeting 2012.
9. Porac C, Coren S. The dominant eye. Psychol Bull. 1976 ; 83(5): 880-897.
FIG. 6 Monocular references – A monocular reference is defined for each eye based on its centre of rotation (CRO) with angular expression of the directions of the eye (�,�). For each eye the radius from the CRO, passing through the centre of the pupil, is deviated by the lens and associates a point O of the object space, modelled by a 3D environment, with its images formed on the retina.
FIG. 7 Binocular references and binocular performances of monocular concept lenses.
Points de Vue - n°68 - Spring / Primavera - 2013 33
PRÓLOGO
Estimados lectores,
En el permanente proceso de evolución de la revista Points de Vue, en este primer número del año 2013 se plasma la voluntad de evolución de su política con un nuevo director de publicación, un nuevo formato bilingüe con dos cuadernos consecutivos así como una nueva línea editorial.
La revista Points de Vue sigue dirigiéndose a todos los profesionales de la óptica oftálmica y su frecuencia de publicación permanece idéntica, es decir, en primavera y en otoño. A partir de ahora, hemos optado por abordar uno o dos temas por número relacionados con la actualidad de los nuevos productos de lentes o con la actualidad científica. Contendrá por lo menos tres secciones principales: los artículos de fondo que corresponden al tema seleccionado, escritos por autores reconocidos por sus pares, los artículos sobre los «productos», escritos por autores de Essilor y los artículos sobre el arte y la visión. Los artículos que sustentan el tema tendrán como objeto constituir la base científica apta para ilustrar al lector sobre las diferentes facetas del tema.En paralelo, la página web www.pointsdevue.net sigue también su evolución incorporando nuevas entrevistas y vídeos de investigadores en ciencias de la visión que se van introduciendo periódicamente y en conexión con los temas corrientes de la revista. De ahora en adelante, todos los números de la revista estarán en línea, salvo el último, que tendrá la primicia de la versión en papel. En esta página se publicarán artículos complementarios a los de la revista, específicos para una lectura en pantalla y destinados a una difusión y reputación más amplia. Además, a partir de ahora, Points de Vue estará presente en las redes sociales como Facebook, Twitter y Youtube.
Continuando con el tema de los ultravioleta del número precedente, en este número abordamos el de la luz azul y sus efectos sobre nuestro sistema visual y no visual, así como los riesgos asociados a la salud visual y a la iluminación. Las longitudes de onda cortas tienen un efecto acumulativo a lo largo de toda la vida y nos pareció interesante poder incorporar así un segundo tema, que es el de la visión de los mayores. En efecto, con la prolongación de la esperanza
JEAN-PIERRE CHAUVEAU El Director de la publicación
de vida, se plantea este debate con mayor frecuencia en los congresos de oftalmología y optometría, de ahí la importancia de tratar aquí este tema de actualidad.
Estos dos temas cuentan con prefacios de autores prestigiosos: el profesor Yves Pouliquen para el tema de las personas mayores y el Doctor Thierry Villette para el tema de la luz azul.Tras haber revelado los secretos de la nueva generación del Varilux S Series en el número anterior, hacemos descubrir ahora los de la versión personalizada de Varilux S Series, con la tecnología 4D. En particular, usted podrá encontrar las bases fisiológicas que han permitido esta innovación sobre los atributos de la visión binocular y aplicados al cálculo binocular de las lentes progresivas.
Fieles a nuestra sección Arte y Visión, les ofrecemos hoy un artículo sobre la patología ocular en la obra de Picasso y más particularmente la ceguera, tema que siempre ha estado presente a lo largo de toda la vida del pintor.
En nombre del equipo de Points de Vue, me gustaría agradecer encarecidamente a Marc Alexandre, Director de la Publicación saliente por su dedicación a esta revista en el transcurso de estos últimos veinte años y que ha sabido conferirle, gracias a su red internacional de líderes de opinión, una imagen internacional y una legitimidad científica en el ámbito de la salud visual y de la corrección de la visión. Le deseamos una larga y feliz jubilación.
Deseándoles una buena lectura,Atentamente,
El Director de la publicación
EDITORIAL

Points de Vue - n°68 - Spring / Primavera - 201334
PRÓLOGO
__ HACIA FINALES DEL SIGLO XVI, SHAKESPEARE, en su obra «Como
gustéis» (As you like it) hizo una definición terrible de la vejez, muy
a su manera: «Es el olvido total, sin dientes, sin ojos, sin gusto, sin
nada»; no obstante, en su época, el ser de una edad avanzada, como
él, podía considerarse una gracia. En realidad esta imagen atroz que,
muy sui generis, él ha introducido en la trama de una comedia, es una
imagen en la que el ojo desempeña un papel. Ineluctable destino del
hombre cuyo genio ha logrado, a pesar de todo y, paradójicamente,
que la mayoría de los hombres y las mujeres alcancen esta etapa fatal
del envejecimiento. Efectivamente, hasta no hace mucho tiempo,
una mayoría de seres vivos no alcanzaban ni siquiera la edad de la
presbicia. La esperanza de vida al nacimiento y la esperanza de vida a
los 65 años han aumentado considerablemente, y nosotros somos los
felices testigos de este hecho. La mortalidad infantil, anteriormente
algo terrible que se vivía como una fatalidad, ha disminuido en
proporciones notables en el transcurso del último siglo y, desde hace
unos treinta años, la mejora de la higiene y los avances de la medicina
han conducido a una reducción impresionante de la morbidez en las
personas mayores, que pueden vivir sin discapacidades significativas
más allá de los 80 años. Es verdad que este envejecimiento sigue
siendo ineluctable pero ahora se puede influenciar parcialmente,
incluso si la evolución biológica que lo rige todavía conserva un gran
número de elementos desconocidos. ¿Por qué envejecemos? Queda,
efectivamente, esta pregunta esencial que todos
nos planteamos mientras que a nuestras capacidades anteriores se van
sustituyendo nuevas incapacidades que van marcando cada una de las
etapas de la última fase de nuestra vida.
Lo que sabemos es que «el envejecimiento sucede a un periodo de
crecimiento y de reproducción. Para algunos, la muerte ocurre cuando la
inmortalidad de la línea germinal ha sido garantizada. Para otros, ésta es el
resultado inevitable del desgaste celular».1 Estudios experimentales en el
gusano C. elegans, la mosca D. melanogaster y en ratones han conducido a
la puesta en evidencia de cuatro vías implicadas en la senescencia:
• la inhibición del eje Insulina/IGF-1;
• la producción de las especies reactivas del oxígeno;
• la reducción de los telómeros;
• la autofagia en los lisosomas.
Sin contar con los factores genéticos que también contribuyen al
envejecimiento.
De esta manera, nuestros diferentes órganos envejecen con sus propias
particularidades: los vasos pierden su flexibilidad, el corazón queda
invadido por la fibrosis, el cerebro por una degeneración neurofibrilar y,
mediante la aparición de placas seniles, la función renal disminuye,
las defensas inmunitarias bajan y la frecuencia de los cánceres aumenta
con la edad.
El ojo tiene sus propias modalidades evolutivas. Los primeros signos
sensibles de su envejecimiento se caracterizan por el inicio
de la dificultad para leer de cerca: lo que se llama presbicia.
En realidad, se trata simplemente de la revelación de un largo proceso
que afecta el poder de acomodación del cristalino. Si se hiciera una
comparación de este poder de acomodación a la edad de 20 años con
un niño de cuatro años, se puede observar que, sorprendentemente,
una gran parte del poder de acomodación ha disminuido. Sin embargo,
a esa edad esto no tiene consecuencias; más bien hacia los cuarenta
y cinco años el emétrope 2 comienza a tener algunas dificultades para
leer que irán acrecentándose con la edad y por lo tanto, necesitará
ayudas ópticas. Se atribuyen las causas de la presbicia a modificaciones
estructurales del cristalino y de los músculos ciliares que se encargan
de modificar su curvatura. Hasta el siglo XIII, para los intelectuales,
este estado fue una discapacidad significativa que solo encontró una
solución al llevar gafas de aumento. Actualmente, se puede considerar
que la presbicia tiene remedio gracias a las notables soluciones que los
diseñadores de lentes correctoras han encontrado y que, resumiendo
en pocas palabras, las lentes correctoras eliminan esta primera y fatal
consecuencia del envejecimiento de manera casi perfecta. El hecho de
que algunos perciben la presbicia como una etapa dolorosa ha dado
lugar a la puesta a punto de técnicas quirúrgicas que permiten evitar el
porte de gafas, marca de la edad.
PRÓLOGO
1 Biologie du vieillissement (Biología del envejecimiento) de Jean-Yves Le Gall y Raymond Ardaillou. Informe ante la Academia Nacional de Medicina 3 de febrero de 2009.2 Sujeto cuya refracción es normal.3 Por oposición a las cataratas secundarias con patologías diversas.
E F E C T O S D E L E N V E J E C I M I E N T O E N E L S I S T E M A V I S U A L
Las marcas del envejecimiento más nocivas para la visión se encuentran en la retina y éstas pueden originar discapacidades visuales significativas.
YVES POULIQUEN de l’Académie française miembro de la Academia de medicinaFrancia

Points de Vue - n°68 - Spring / Primavera - 2013 35
PRÓLOGO
Nadie ignora que la catarata en su forma primitiva 3 sobreviene
con la edad. Se trata de la causa principal de alteración de la visión
después de los sesenta y cinco años. Esta alteración progresiva
del cristalino, que conduce a modificaciones de su transparencia,
se traduce en un conjunto de manifestaciones visuales, como
son la disminución de la agudeza visual, el deslumbramiento
o la alteración del contraste; estas manifestaciones, al volverse
molestas, tienen una indicación operatoria, y, gracias a los avances
técnicos notables, se trata actualmente de un procedimiento preciso,
breve, ambulatorio y que permite restaurar una visión normal.
El tratamiento de esta afección, conocida desde la alta antigüedad
y cuya índole solo se detalló hacia inicios del siglo XVIII
era el abatimiento del cristalino 4. Hacia 1760, Jacques Daviel 5
propuso sustituir este procedimiento mediante la extracción
del cristalino, abriendo así una vía de operaciones quirúrgicas
que se ha venido perfeccionando hasta nuestros tiempos.
Las marcas del envejecimiento más nocivas para la visión
se encuentran en la retina, y estas pueden originar discapacidades
visuales significativas. La degeneración macular asociada a la edad
(DMAE) es la forma más común y más temida, de manera justificada,
entre las personas mayores. Con la edad, la retina va perdiendo
regularmente las células fotorreceptoras (conos y bastones),
pero sin provocar ninguna alteración visual, puesto que el 30 %
de estas son suficientes para mantener una visión percibida como
normal. En cambio, la DMAE afecta aproximadamente al 25 o 30 %
de los hombres y mujeres mayores de 80 años. Esta es la consecuencia
de una alteración degenerativa de la retina, que se manifiesta
con una afección de la visión central (la que permite la lectura
y la visión de los colores), a la vez que deja intacta la visión periférica.
Puede ir apareciendo hacia los sesenta años, aunque en proporciones
limitadas, pero que van aumentando paulatinamente con la edad.
La DMAE se manifiesta en dos formas. La más común es una forma
seca y de desarrollo lento, caracterizada por la presencia de depósitos
lipídicos en la mácula, o «drusas»; con menor frecuencia
aparece una forma húmeda o exudativa con desarrollo rápido,
y que se caracteriza por una proliferación vascular importante. En esta
segunda forma, las inyecciones de factores de antiproliferación vascular
en el humor vítreo permiten una neta estabilización, aunque frágil,
de las alteraciones maculares. A las formas secas no se les puede aplicar
esta terapia, que constituye el primer tratamiento verdadero de estas
DMAE. Ahora ya se conocen cuáles son los elementos
constitutivos de las drusas y se conoce en parte las razones de su
formación. Se ha establecido claramente que los factores de riesgo
favorecen la aparición de la DMAE (edad, tabaco, elementos oxidantes),
pero que también depende de factores genéticos significativos
que se empiezan a identificar con precisión.
El resultado de todas estas causas es la alteración de las microglías
que participan en la formación de las drusas y las modificaciones
determinantes de las células del epitelio pigmentario
de las que se sabe desempeñan un papel esencial en la biología
de los fotorreceptores.
Aunque la DMAE sigue siendo la complicación principal de la
retina durante el envejecimiento, hay que añadir las modificaciones
degenerativas lentas de la periferia retiniana o el papel de la
degeneración del cuerpo vítreo, que, al provocar la separación de sus
relaciones íntimas con la retina, puede originar desgarros retinianos,
responsables, a su vez, del desprendimiento de la retina. Existe una
incidencia particularmente elevada en las personas miopes a partir
de los cincuenta años. ¿Es incongruente atribuir al envejecimiento
la agravación de las lesiones de una retinopatía pigmentaria,
que, puesto que es compatible con una vida correcta hasta la mitad
de la vida, conduce a la ceguera total en los últimos años?
Con gran frecuencia, con motivo de un examen oftalmológico,
se descubren en el paciente hipertensión ocular y glaucoma.
Esta enfermedad temible es desconocida porque el que la padece
no tiene ningún síntoma. En sus inicios, esta enfermedad
es totalmente asintomática.
Sabemos que, sin tratamiento, esta conduce a la atrofia óptica.
Aunque los factores genéticos parecen ahora asumir la responsabilidad
4 Se perforaba el ojo el ojo con una espina o una aguja, se desprendía el cristalino y se le abatía en el cuerpo vítreo en donde permanecía y quedaba más o menos tolerado.5 Yves Pouliquen, «Jacques Daviel un oculista en el siglo de las luces», Odile Jacob, 1999.
Nuestros diferentes órganos envejecen con sus propias particularidades.
FIG. 1 Giovanni Serodine (1594-1630), «Ritrato del padre» (Retrato del padre del pintor), 1624. Óleo sobre lienzo, 152 x 98. Lugano, Museo Civico d’Arte Lugano.Fotografia: akg-images / André Held

Points de Vue - n°68 - Spring / Primavera - 201336
PRÓLOGO
FIG. 2 Jean Fouquet (1420-1481), «Retrato de Gonella, bufón de la corte de Ferrara», 1442. Viena, Austria. © De Agostini Picture Library / The Bridgeman Art Library
opacos. La despigmentación del iris es la responsable, la pupila antes
tan negra, se ha vuelto grisácea, y la córnea, tan transparente,
lleva ahora en su periferia un anillo blanco denominado
arco senil. La conjuntiva pierde su brillo y sus pinguéculas se vuelven
más amarillas. ¿Qué decir también de estos párpados que se arrugan
por la alteración del tejido conjuntivo que los mantenía?
Sus pliegues incitan a una gran cantidad de pacientes a recurrir
a la cirugía estética. Las deformaciones en su posición eversión
en el ectropión, inversión en el entropión, testigos de la edad muy
avanzada, requieren tratamientos quirúrgicos con el fin de evitar
complicaciones corneo-conjuntivales.
Pero, ¿qué pensar de estas «bolsas» que hacen caer o que subrayan
los párpados, y que se deben a un fallo del septum orbital, víctima,
a su vez, de una degeneración tisular? Y también,
¿por qué este lagrimeo tan frecuente en las personas mayores?
Lagrimeo que condiciona las deformaciones de los párpados pero, sobre
todo, las obliteraciones tardías de las vías de excreción
lagrimal. Discapacidad muy difundida y desagradable pero menos
grave que su contrario, es decir, la sequedad ocular,
responsable de una queratitis crónica y de la obligación
de humidificar el ojo varias veces al día...
Males pequeños en comparación con los grandes. Hemos repasado
algunos pero hay otros, que, sin duda, tienen su expresión más
dolorosa en las lesiones de las vías ópticas que el envejecimiento
puede alcanzar. Se trata de factores de origen mayoritariamente
vascular, ocasionados por el ateroma, la hipertensión o la diabetes,
todos ellos responsables de trastornos visuales graves, y a menudo
irreversibles, en la retina: obliteración de la arteria central,
trombosis de la vena central; o en el nervio óptico, neuritis óptica
isquémica aguda, vías ópticas retroquiasmáticas con, como
consecuencia más frecuente, una hemianopsia lateral homónima,
incluso una ceguera cortical. Una hemianopsia estable
que no hay que confundirla con el escotoma hemianópsico,
rápidamente resolutivo de la migraña oftálmica tan frecuente después
de los setenta años y totalmente benigna.
¿Podremos un día escribir otra historia? La de un ser humano
que viviría hasta los límites estimados por la ciencia y superiores al
menos 30 años a nuestra media actual, sin ninguna manifestación de
envejecimiento y que uno puede imaginar cuán difícil será entonces
de una parte de estos glaucomas, lo que sigue estando claro es que las
modificaciones del espacio trabecular, responsables del defecto
de excreción del humor acuoso, condicionan la hipertonía ocular.
Se trata de alteraciones condicionadas más o menos por la edad,
que, de todas formas, contribuirán al fallo tardío del nervio óptico,
mediante factores vasculares asociados. Aunque el glaucoma de ángulo
abierto que acabamos de abordar se ve influenciado por la edad, existe
otro totalmente asociado a ella: el glaucoma de ángulo cerrado 6,
un glaucoma agudo de inicio repentino y responsable de dolores oculares
atroces, vómitos, y que requiere un tratamiento de urgencia. Se origina
en la estrechez del ángulo irido-corneal, suficientemente abierto durante
la mayor parte de la vida pero que se cierra repentinamente por diversas
razones. Estas pueden ser por administración de medicamentos, que
provocan la dilatación del iris responsable de la obstrucción de este
ángulo estrecho, o bien por la hinchazón de un cristalino con catarata
que favorece la oclusión del ángulo bajo el efecto de una causa anexa.
Una simple iridotomía 7 con láser permite ahora evitarla cuando
la observación del segmento anterior del ojo lo deja prever.
Aunque las manifestaciones del envejecimiento en el ojo abarcan
principalmente las formas clínicas precedentes, existen muchas
otras marcas. Todos hemos observado los cambios que sufre la mirada
con la edad. Esos ojos que solían ser tan fascinantes van perdiendo
su resplandor y esos iris anteriormente tan brillantes se han vuelto
Con gran frecuencia, con motivo de un examen oftalmológico, se descubre en un paciente una hipertensión ocular y un glaucoma.
6 Se llama ángulo a la zona estrecha comprendida entre la raíz del iris y la cara posterior de la córnea prelímbica. Es una zona de filtración del humor acuoso que, al ser secretado por el cuerpo ciliar, sale del ojo mediante este filtro. Su obstrucción es responsable de la hipertonía crónica del glaucoma de ángulo abierto y del glaucoma agudo de ángulo estrecho.7 Perforación de la raíz del iris.

Points de Vue - n°68 - Spring / Primavera - 2013 37
PRÓLOGO
E L A Z U L M A L O, E L A Z U L B U E N O,
L O S O J O S Y L A V I S I Ó N
__ EL COLOR AZUL ES FUENTE DE INSPIRACIÓN EN LAS ARTES, el azul
vibra a través de la literatura y deberíamos hablar bien de los azules,
en plural: desde el «Sol azul de los sueños» de Aragón, o «La vida
es azul como lo es un cielo puro» de Balzac, pero basta con un soplo,
una radiación, para pasar al otro extremo hacia las «Lenguas azules
de la cólera» de Gorki o «El azul de las catástrofes que se miran
por la ventana» de Bobin. «El azul malo contra el azul bueno»,
este es el desafío y el contenido de este nuevo número de Points de
Vue, que contribuye a dar respuestas a las nuevas preguntas que han
surgido de los recientes descubrimientos científicos y observaciones
clínicas
que ligan la fracción azul-violeta del espectro visible, de 380 a 500
nm, al ojo y a la visión:
• ¿Es el azul de alta energía nefasto para los tejidos oculares?
• ¿Qué más se sabe hoy en día sobre los roles fisiológicos de la luz
azul?
• ¿Por qué sería conveniente para la salud humana suprimir una parte
del azul, y cuál sería el riesgo si se suprimiera de este?
• ¿Estamos más expuestos hoy al azul nocivo? ¿Por qué?
Desde mediados de los años 90 se han venido realizado progresos
significativos en los conocimientos fisiopatológicos sobre las
consecuencias de la exposición del ojo a diferentes tipos de luz azul.
Antes de este período, y desde la llegada de los láseres en los años 70,
la comunidad científica y las agencias públicas de foto y radiovigilancia
y protección habían llevado a cabo experimentos en animales para
establecer los umbrales de peligros térmicos y fotoquímicos de la luz,
centrándose principalmente en los UV y el segmento anterior del ojo,
aunque también en la «luz visible de alta energía», la luz azul-violeta
rebautizada como luz azul-violeta en aras de la simplificación,
«luz azul», que presenta riesgos potenciales de lesiones fotoquímicas
en la retina. De hecho, sabemos que, salvo durante la infancia,
los tejidos oculares filtran prácticamente todas las radiaciones de los
UV, y que actualmente se acusa a esta «luz azul» de estar involucrada
en algunas patologías oculares.
En los años 90, los progresos de la fotobiología celular y molecular
han permitieron determinar cuáles eran las bandas de luz visible más
nocivas para la retina, qué mecanismos de toxicidad se activaban,
haciendo la distinción entre la toxicidad aguda y la toxicidad crónica.
Estos trabajos se beneficiaron de un fuerte impulso por la difusión
y multiplicación de nuevos implantes intraoculares que filtraban el azul,
y también por la necesidad de evaluar el riesgo para la retina de los
instrumentos de exploración o de cirugía oculares.
La toxicidad aguda es debida a exposiciones luminosas de alta
intensidad y de corta duración, y sus efectos se dejan sentir a nivel
de las células de la retina en una destrucción térmica y una muerte
celular por necrosis.
La toxicidad crónica es más insidiosa porque intervienen en ella
mecanismos fotoquímicos de estrés oxidativo que conducen a la
acumulación de componentes fotosensibilizadores y especies reactivas
PRÓLOGO
350 400 450 500 550
Longitud de onda (nm)
1.00
0.75
0.50
0.25
0.0
Abso
rció
n
FIG. 2 Las imágenes espectrales de la luteína y la zeaxantina en etanol ilustran las diferencias características de las propiedades de absorción de ambos carotenoides - Landrum JT, Bone RA. Lutein, Zeaxanthin and the Macular Pigment. Arch. Biochem. Biophys. 2001 (385) 28-40
FIG. 1 La topografía y la relación con la edad de la concentración de lipofuscina en el epitelio pigmentario de la retina. - Wing G.L., Blanchard G.C., Weiter J.J.. IOVS (1978) 17(7) 601-7.
120
110
100
90
80
70
60
50
40
30
20
10
0
Lipo
fusc
in c
onte
nt (A
rbitr
ary
Uni
ts)
0 10 20 30 40 50 60 70 80 90
Age (Years)
THIERRY VILLETTE PhD, Essilor International, Director I&D Disruptivas y Neuro-bio-sensorialesFrancia

Points de Vue - n°68 - Spring / Primavera - 201338
PRÓLOGO
1. Sunlight and the 10-Year Incidence of Age-Related Maculopathy. The Beaver Dam Eye Study. Arch Ophthalmol. 2004;122:750-757.
2. IOVS 2000 (41) 3984-90.
3. Photochem. Photobiol. 2005 (81) 1305-30.
4. Exp. Eye Res. 2005 (80) 595-606 ; IOVS 2000 (41) 1981-9.
REFERENCIAS
oxidantes (oxígeno singlete, peróxido de hidrógeno, etc.), que año tras
año van amplificando el peligro de la luz azul en las células expuestas,
y contribuyen así a ciertas patologías oculares crónicas como la
DMAE (degeneración macular asociada a la edad) o las retinopatías
pigmentarias.
En el plano clínico, la correlación entre la exposición a la luz azul
y la prevalencia de la DMAE es difícil de establecer.
No obstante, varios estudios epidemiológicos, entre los que figura
el «Beaver Dam Eye Study», han llegado a la conclusión de que la
exposición acumulativa al sol aumenta el riesgo de DMAE,
y que se debe más a la luz visible que a los UV [1] .
A nivel celular, los fotorreceptores (conos y bastones) y las células
del epitelio pigmentario (RPE), dos familias de células de la retina
íntimamente relacionadas, han sido identificados como las principales
células a la vez actrices y víctimas de este estrés oxidativo y de esta
fototoxicidad crónica de la luz azul, cuyo desenlace es una muerte
celular por apoptosis (muerte celular programada). El RPE es esencial
para los fotorreceptores, porque les aporta oxígeno y nutrientes y,
a cambio, asegura a cada ciclo visual la fagocitosis de sus segmentos
externos y la regeneración metabólica del pigmento visual (la rodopsina).
Se han puesto en evidencia en animales los peligros de la luz azul en
los fotorreceptores. De esta manera, C. Remé y C. Grimm en 20038 [2]
demostraron en ratas que la luz azul, a diferencia de la verde, acarrea
una fotorreversión del blanqueado de los fotorreceptores. Esta rápida
regeneración de la rodopsina inducida por la luz azul de alta energía
acarrearía una degeneración de los fotorreceptores por apoptosis.
Con anterioridad, M. Rozanowksa [3] había explorado los mecanismos
moleculares y demostró el papel combinado de la rodopsina y de los
retinoides 11-cis-retinal y 11-trans-retinal («ATR», all-transretinal),
cuya acumulación contribuye al mecanismo de fototoxicidad en los
fotorreceptores.
El espectro de acción de la fototoxicidad de la luz en las células RPE
fue estudiado por J. Sparrow et M. Boulton[4] quienes pusieron
en evidencia el papel central de la acumulación de lipofuscina
en la amplificación de los mecanismos de fotooxidación conducentes
a una muerte celular por apoptosis. La muerte del RPE acarrea, a su
vez, la pérdida de los fotorreceptores, porque son interdependientes.
Los gránulos de lipofuscina se forman en grandes cantidades cuando
la fagocitosis de los segmentos oxidados de los fotorreceptores es
incompleta, lo cual acarrea cascadas de inflamación y de estrés
oxidativo. Estos gránulos, constituidos por lípidos y proteínas, encierran
una molécula particularmente fotosensibilizadora, el bisretinoide «A2E»,
formada a partir de dos ATR, con un pico de absorción en el azul en
torno a los 440 nm, lo cual explica la nocividad particular para el RPE
de la luz azul, con un espectro de acción que no sigue exactamente
el nivel energético de la luz. La acumulación de lipofuscina en el RPE
aumenta con la edad, durante la infancia y luego una vez más después de
los 45 años (fig.1), así como en situaciones patológicas como la DMAE
o la retinitis pigmentaria. Por lo demás, con la edad, las enfermedades
oculares, los malos comportamientos alimentarios, los mecanismos
naturales de defensa retiniana contra el estrés oxidativo disminuyen:
baja la actividad enzimática «detoxificante» (catalasa, SOD…),
disminución de la fijación en el centro de la retina del pigmento
macular, particularmente la luteína y la zeaxantina, absorbidas por la
alimentación, cuyos valores máximos del espectro de absorción y de
protección son sorprendentemente cercanos al máximo de absorción
tóxica del A2E.
Recientemente, un equipo de fotobiólogos del Instituto de la Visión
de París (UPMC, Inserm, CNRS), el Dr. Serge Picaud y la Dra. Emilie
Arnault, bajo la dirección del Profesor José-Alain Sahel y en colaboración
con Essilor, se fijó como objetivo afinar el espectro de acción de la
fototoxicidad de la luz azul en las células RPE al poner a las células, por
primera vez, en las condiciones fisiológicas de iluminación en toxicidad
crónica, por tramos de 10 nm, tomando en consideración los ratios
espectrales del espectro solar y el filtrado de los medios oculares.
Ellos exponen aquí sus trabajos para Points de Vue.
De esta manera, todos los trabajos in vitro confirman los peligros
de una exposición acumulada a un cierto tipo de luz azul, el azul malo.
Pero en 2002 algunos científicos cronobiólogos descubrían un tercer
fotorreceptor en la retina, que permitió profundizar los conocimientos
clínicos de los años 80 en el ámbito de la extensión y mecanismos de
las funciones no visuales del ojo moduladas por una banda de azul
turquesa, el azul bueno, centrado en los 480 nm (aprox. 465-495 nm).
Este fotorreceptor proyecta en varias áreas no visuales del cerebro y
permite sincronizar de nuevo las funciones fisiológicas denominadas
circadianas con arreglo a las 24 horas de rotación de la Tierra: el sueño,
la vigilia, el humor y la temperatura corporal son solo algunos ejemplos
de estas funciones que muestran la importancia de no perturbar este
azul bueno en el caso de que deseáramos filtrar total o parcialmente
al azul malo. El doctor Claude Gonfrier (Inserm, Lyon) desarrolla
en este Points de Vue el estado actual de los conocimientos sobre la luz
azul y los ritmos circadianos.
El azul malo y el azul bueno, entre el «azul en quejumbre»
(Louis Aragon, Los Ojos de Elsa) o el «magnífico resplandor de un ojo azul
celeste» (Victor Hugo, El Rín. Cartas a un amigo), nuestros ojos,
la exposición a nuevas iluminaciones artificiales (cf. C. Martinsons en este
número), nuestra visión de los colores (cf. F. Vienot, en este número),
nuestra predisposición a enfermedades oculares o simplemente al
deslumbramiento (cf. B. Girard, en este número), nuestro cuerpo, nuestros
ritmos; en resumen, toda nuestra vida física y psíquica está influenciada
A2E
10
8
6
4
0
Inte
nsid
ad re
lativ
a
350 400 450 500 550 600 650 700
Excitación UV/Vis Emisión
NCH2CH2OH
FIG. 3 Imágenes espectrales de la emisión, excitación y UV/Vis de la A2E en metanol. El espectro de absorbancia registró el pico mayor a 435 nm y el pico menor a 335 nm. El espectro de ecitación monitoreado a emisiones de 600 nm era similar en su forma con un máximo a los 418 nm. Una longitud de onda de excitación a 400 nm generó una emisión amarilla centrada alrededor de los 602nm. Sparrow JR et al. IOVS 2000 (41) 1981-9
Longitud de onda (nm)

Points de Vue - n°68 - Spring / Primavera - 2013 39
VISIÓN DE LAS PERSONAS MAYORES
Científico médico
F O T O S E N S I B I L I D A DY L U Z A Z U L
__ LA FOTOFOBIA ES LA SENSACIÓN DOLOROSA que siente el sujeto ante
la exposición a la luz. Esta última es responsable del cierre reflejo de
los párpados protegiendo de esta manera a la retina de una exposición
demasiado fuerte a los rayos luminosos y especialmente a los rayos
solares debido a la fototoxicidad de la luz en las capas coriorretinianas.
La fotosensibilidad solo ocurre en presencia del espectro de la luz
visible. Cuando esta información sensorial es exacerbada se habla
entonces de fotofobia. Algunas enfermedades ocasionan, una fotofobia
que forma parte integrante de los síntomas. Las más frecuentes afectan
la integridad del ojo o de las vías visuales, se pueden citar las lesiones
corneales, las úlceras corneales traumáticas, los abscesos corneales
o las queratitis punteadas superficiales, frecuentes en todos los
síndromes de sequedad ocular. También puede tratarse de una uveítis,
de una neuropatía retrobulbar, o enfermedades extraoculares como
la migraña o la meningitis.
__ CÉLULAS GANGLIONARES ESPECIALIZADAS
El origen de la fotofobia se sitúa en las células ganglionares
especializadas de la retina «ipRGCs» (intrinsically photosensitive retinal
ganglion cells). En el estado actual de la investigación
todavía no sabemos si estas células se subdividen según la longitud
de onda presentada.
Estas ipRGC se sitúan en la capa de las células ganglionares
de la retina. Al principio, su axón recorre el mismo trayecto que todas
las fibras nerviosas retinianas para dirigirse hacia el nervio óptico.
Se acaba de descubrir recientemente un trayecto propio y ha sido
denominado vía no visual del nervio óptico, y que llega
a la parte posterior del tálamo o pulvinar[6]. Estas vías no visuales
así individualizadas por técnicas de tractografía en difusión MR
proporcionan una base anatomofisiológica al dolor generado por la luz.
Existen, además, conexiones nerviosas entre el pulvinar y el núcleo
del trigémino que pueden explicar la fotofobia en todas las lesiones
oculares que estimulan la rama oftálmica del nervio trigémino.
Después de la conexión directa del nervio óptico al pulvinar, el
trayecto de esta vía no visual conecta con el córtex, tanto el visual
(área occipital de Brodmann 18, 19, 20) como el parietal (área
de asociación, área de Brodman 7), el frontal y el prefrontal. Las
conexiones de estas vías
no visuales interactúan con las vías motrices o sensoriales (olfativas).
Estas vías no visuales activadas por un estímulo fótico, actúan en el
umbral de excitación de las neuronas del trigémino del núcleo postero-
lateral y posterior del tálamo (en ratas) aumentando la sensación
de dolor a una exposición luminosa durante la migraña. Un estudio
de IRM funcional [8] también ha demostrado un aumento de la actividad
del pulvinar durante una sensibilización cerebral central (migraña)
explicando la fotofobia. El pulvinar está dividido en cuatro zonas,
de las cuales tres (medial, superior e inferior) concentran la
información visual 3. El pulvinar es, por lo tanto, un centro principal
de integración y de modulación de los influjos sensoriales, en
particular los transmitidos por las ipRGC y la vía no visual que tiene,
por sí misma, conexiones con el núcleo supraquiasmático (SCN), la
habénula, la epífisis, el fascículo haz intergeniculado (IGL) y el núcleo
pretectal olivar (OPN). Este último está conectado al ganglio ciliar y al
núcleo
de Edinger-Westfal implicado en los reflejos pupilares
fotodependientes.
__ TOXICIDAD DE LA LUZ AZUL
Para protegerse de la nocividad de las radiaciones luminosas de alta
energía, la naturaleza suministra numerosos filtros. Efectivamente,
los ultravioletas A, B y una parte de los C, aún más energéticos
que la luz azul, no llegan a la retina porque, en primer lugar,
la capa de ozono los detiene, luego la córnea y luego el cristalino.
En contraste, las diversas radiaciones del espectro visible de la luz sí
llegan a los fotorreceptores. La longitud de onda de la luz azul es la más
energética. Se sitúa entre los 400 y los 510 mm y cubre los violetas,
VISIÓN DE LAS PERSONAS MAYORES
Científico médico
BRIGITTE GIRARDDRA., Profesora asociada del Colegio de Medicina de los Hospitales de ParísHospital Tenon, Francia
Energía de la luz:E (eV) = h�� (Hz) = 1/ � (nm)
FIG. 1 Energía de los fotones según su longitud de onda, en el espectro de la luz visible.
3,54 3,10 2,48 eV
350 400 500 nm
857 750 600 THz
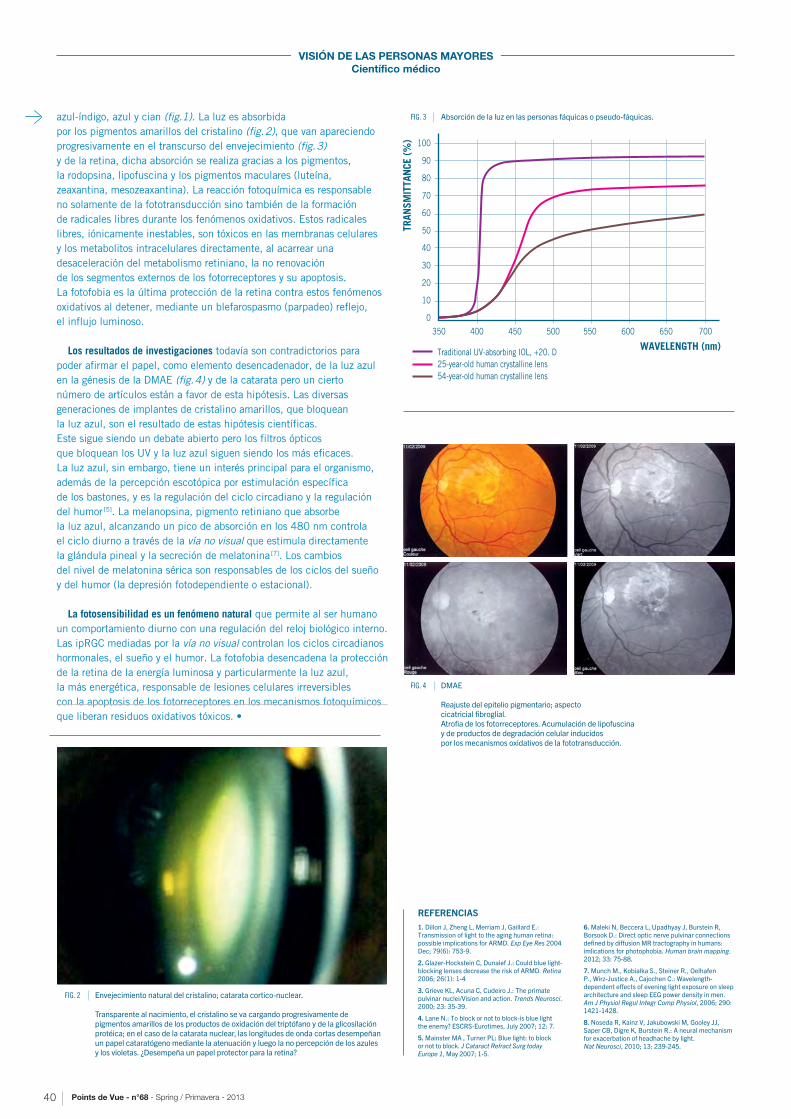
Points de Vue - n°68 - Spring / Primavera - 201340
VISIÓN DE LAS PERSONAS MAYORES
Científico médico
1. Dillon J, Zheng L, Merriam J, Gaillard E.: Transmission of light to the aging human retina: possible implications for ARMD. Exp Eye Res 2004 Dec; 79(6): 753-9.
2. Glazer-Hockstein C, Dunaief J.: Could blue light-blocking lenses decrease the risk of ARMD. Retina 2006; 26(1): 1-4
3. Grieve KL, Acuna C, Cudeiro J.: The primate pulvinar nuclei/Vision and action. Trends Neurosci. 2000; 23: 35-39.
4. Lane N.: To block or not to block-is blue light the enemy? ESCRS-Eurotimes, July 2007; 12: 7.
5. Mainster MA , Turner PL: Blue light: to block or not to block. J Cataract Refract Surg today Europe 1, May 2007; 1-5.
6. Maleki N, Beccera L, Upadhyay J, Burstein R, Borsook D.: Direct optic nerve pulvinar connections defined by diffusion MR tractography in humans: imlications for photophobia. Human brain mapping. 2012; 33: 75-88.
7. Munch M., Kobialka S., Steiner R., Oelhafen P., Wirz-Justice A., Cajochen C.: Wavelength-dependent effects of evening light exposure on sleep architecture and sleep EEG power density in men. Am J Physiol Regul Integr Comp Physiol, 2006; 290: 1421-1428.
8. Noseda R, Kainz V, Jakubowski M, Gooley JJ, Saper CB, Digre K, Burstein R.: A neural mechanism for exacerbation of headhache by light. Nat Neurosci, 2010; 13: 239-245.
REFERENCIAS
azul-índigo, azul y cian (fig.1). La luz es absorbida
por los pigmentos amarillos del cristalino (fig. 2), que van apareciendo
progresivamente en el transcurso del envejecimiento (fig. 3)
y de la retina, dicha absorción se realiza gracias a los pigmentos,
la rodopsina, lipofuscina y los pigmentos maculares (luteína,
zeaxantina, mesozeaxantina). La reacción fotoquímica es responsable
no solamente de la fototransducción sino también de la formación
de radicales libres durante los fenómenos oxidativos. Estos radicales
libres, iónicamente inestables, son tóxicos en las membranas celulares
y los metabolitos intracelulares directamente, al acarrear una
desaceleración del metabolismo retiniano, la no renovación
de los segmentos externos de los fotorreceptores y su apoptosis.
La fotofobia es la última protección de la retina contra estos fenómenos
oxidativos al detener, mediante un blefarospasmo (parpadeo) reflejo,
el influjo luminoso.
Los resultados de investigaciones todavía son contradictorios para
poder afirmar el papel, como elemento desencadenador, de la luz azul
en la génesis de la DMAE (fig. 4) y de la catarata pero un cierto
número de artículos están a favor de esta hipótesis. Las diversas
generaciones de implantes de cristalino amarillos, que bloquean
la luz azul, son el resultado de estas hipótesis científicas.
Este sigue siendo un debate abierto pero los filtros ópticos
que bloquean los UV y la luz azul siguen siendo los más eficaces.
La luz azul, sin embargo, tiene un interés principal para el organismo,
además de la percepción escotópica por estimulación específica
de los bastones, y es la regulación del ciclo circadiano y la regulación
del humor [5]. La melanopsina, pigmento retiniano que absorbe
la luz azul, alcanzando un pico de absorción en los 480 nm controla
el ciclo diurno a través de la vía no visual que estimula directamente
la glándula pineal y la secreción de melatonina [7]. Los cambios
del nivel de melatonina sérica son responsables de los ciclos del sueño
y del humor (la depresión fotodependiente o estacional).
La fotosensibilidad es un fenómeno natural que permite al ser humano
un comportamiento diurno con una regulación del reloj biológico interno.
Las ipRGC mediadas por la vía no visual controlan los ciclos circadianos
hormonales, el sueño y el humor. La fotofobia desencadena la protección
de la retina de la energía luminosa y particularmente la luz azul,
la más energética, responsable de lesiones celulares irreversibles
con la apoptosis de los fotorreceptores en los mecanismos fotoquímicos
que liberan residuos oxidativos tóxicos. •
FIG. 4 DMAE
Reajuste del epitelio pigmentario; aspecto cicatricial fibroglial. Atrofia de los fotorreceptores. Acumulación de lipofuscina y de productos de degradación celular inducidos por los mecanismos oxidativos de la fototransducción.
FIG. 2 Envejecimiento natural del cristalino; catarata cortico-nuclear. Transparente al nacimiento, el cristalino se va cargando progresivamente de pigmentos amarillos de los productos de oxidación del triptófano y de la glicosilación protéica; en el caso de la catarata nuclear, las longitudes de onda cortas desempeñan un papel cataratógeno mediante la atenuación y luego la no percepción de los azules y los violetas. ¿Desempeña un papel protector para la retina?
FIG. 3 Absorción de la luz en las personas fáquicas o pseudo-fáquicas.
350 400 450 500 550 600 650 700
WAVELENGTH (nm)
TRAN
SMIT
TAN
CE (%
) 100
90
80
70
60
50
40
30
20
10
0
Traditional UV-absorbing IOL, +20. D
25-year-old human crystalline lens
54-year-old human crystalline lens

Points de Vue - n°68 - Spring / Primavera - 2013 41
VISIÓN DE LAS PERSONAS MAYORES
Científico no médico
L O S C O N D U C T O R E S M A Y O R E S : L A S I M P L I C A C I O N E S
D E L O S C A M B I O S V I S U A L E S
Q U E O C U R R E N C O N L A E D A D
__ RESUMEN
Las discapacidades visuales aumentan significativamente con
la edad como resultado del proceso normal de envejecimiento, así como
a través del aumento de la prevalencia de enfermedades oculares.
Dichos cambios en la visión tienen toda una serie de implicaciones
en la conducción y la seguridad al volante. En este artículo, se plantea
el impacto de estos cambios en las funciones visuales, debidos
a la edad, en la capacidad de conducción y se describen las pruebas
actuales que establecen una relación entre los resultados en las pruebas
visuales con la capacidad de conducción y los riesgos de accidente vial.
La conducción es una tarea compleja que implica la integración
de un abanico de capacidades visuales, cognitivas y psicomotoras, muchas
de las cuales se van deteriorando con la edad. Puesto que la conducción
es considerada una tarea visual altamente compleja, como se ilustra
en la figura 1, se ha sugerido que la alta prevalencia de discapacidades
visuales en las personas mayores contribuye a la disminución en la
capacidad de conducción observada en los conductores mayores.
Con la edad, se observa una mayor prevalencia de discapacidades
visuales, y esto se debe tanto a los cambios normales asociados a la
edad, como al aumento de enfermedades oculares asociadas a la edad,
como catarata, glaucoma y la degeneración macular (DMAE). Estos
cambios acarrean la disminución de la agudeza visual, de la sensibilidad
al contraste, del campo visual, de la sensibilidad al movimiento, de la
velocidad de procesamiento visual, así como una mayor sensibilidad al
deslumbramiento.
La agudeza visual es la prueba de visión más comúnmente utilizada
para determinar la capacidad para conduci, a pesar del hecho
de que no se ha establecido claramente la relación entre una agudeza
reducida y un mayor riesgo de accidente. Los primeros estudios sobre
la agudeza visual y el riesgo de accidente solo mostraron una baja
correlación entre la agudeza visual y las estadísticas de accidentes [1].
Estudios más recientes, utilizando una gama de tamaños de muestreo
y metodologías, solo encontraron una baja relación entre agudeza y
riesgo de accidente [2-6] y otros no encontraron ninguna relación [7-12].
Esta baja relación entre la agudeza visual y el riesgo de accidente
no es sorprendente, puesto que es poco probable que la capacidad
de resolución de objetivos estáticos de alto contraste represente
adecuadamente las demandas visuales de un entorno normal
de conducción, en el que se presentan tanto objetos estáticos, como
en movimiento, de diferentes tamaños y contrastes tanto en la visión
central como en la periférica. Las pruebas de sensibilidad al contraste,
visión periférica y la sensibilidad al movimiento pueden suministrar
mejores mediciones de la eficacia visual para la conducción.
Decina y Staplin [7] determinaron que la sensibilidad al contraste,
la agudeza visual y los campos visuales estaban fuertemente
relacionados con las tasas de accidente entre conductores mayores
una discapacidad en la sensibilidad al contraste está relacionada
con accidentes retrospectivos [13] y no con los prospectivos [9,11,12].
Es importante señalar que estas mayores tasas de accidente ocurren
a pesar del hecho de que los conductores mayores con una discapacidad
de sensibilidad al contraste se autorregulan y disminuyen su exposición
a la conducción [14-16]. Es interesante observar que los conductores con
catarata involucrados en accidentes tenían 8 veces más probabilidades
de tener una sensibilidad reducida al contraste en comparación con
el grupo control [17]. Estudios en ruta a circuito cerrado también han
demostrado una relación significativa entre la sensibilidad al contraste
y la buena conducción en conductores con catarata simulada [18] y
verdadera [19] y la sensibilidad al contraste también pronostica la eficacia
de reconocimiento de los conductores (señales, peligros y peatones),
tanto en condiciones diurnas como nocturnas [20].
Los estudios que rrelacionan la pérdida de campo visual y el riesgo
de accidente han registrado resultados dispares. Johnson y Keltner [21]
demostraron que la disminución del campo visual más que duplicaba las
tasas de accidente en comparación con el grupo control, mientras que
otros estudios no consiguieron encontrar una relación significativa entre
la disminución de campo y el riesgo de accidente [1, 7, 9, 22]. No obstante,
un estudio poblacional más reciente [11], así como estudios a menor
escala sobre conductores con defectos glaucomatosos de campo [23, 24]
han venido a apoyar los resultados iniciales de Johnson y Keltner [21],
al demostrar que solo aquellos con una pérdida de campo visual más
extensa tienen una conducción deficiente y un aumento del riesgo
de accidente. Esto se refleja en estudios de ruta a circuito cerrado en
los que se ha demostrado que la conducción no es significativamente
deficiente hasta que la pérdida de campo simulada sea más extensa [25].
De la misma manera, algunos estudios realizados en ruta han
determinado que solo aquellos conductores con defectos binoculares
más severos tenían una capacidad de conducción significativamente
deficiente [26,27,28]. Efectivamente, se ha sugerido que el fusionar
los dos campos del umbral monocular, fenómeno conocido como
FIG. 1 Ilustración de la complejidad visual del entorno del vehículo y su conducción.
VISIÓN DE LAS PERSONAS MAYORES
Científico no médico
ALEX BLACKLicenciado en Ciencias (con honores) Máster en Salud Pública, PhD Escuela de Optometría y Ciencias de la Visión Instituto de Sanidad e Innovación Biomédica Universidad de Tecnología de Queensland, Australia
JOANNE M. WOOD Licenciada en Ciencias (con honores), PhDMiembro del colegio de optometría, miembro de la Fundación de la Academia Americana de Oftalmología Escuela de Optometría y Ciencias de la Visión, Instituto de Sanidad e Innovación Biomédica Universidad de Tecnología de Queensland, Australia

Points de Vue - n°68 - Spring / Primavera - 201342
VISIÓN DE LAS PERSONAS MAYORES
Científico no médico
el campo visual integrado (IVF, según sus siglas en inglés), puede ser útil
a la hora de evaluar la capacidad de conducción en pacientes con toda
una serie de pérdidas de campo visual [29,30], especialmente en la medida
en que los campos monoculares son evaluados de manera rutinaria
en los pacientes con enfermedades oculares; no obstante, la relación
entre el IVF y el riesgo de accidente todavía está por determinar.
En la conducción, siempre se ha tomado en consideración la capacidad
para ver blancos en movimiento debido a la naturaleza dinámica
el entorno de conducción. Estudios recientes, al utilizar pruebas
con ordenadores sobre discriminación y detección de movimientos,
han demostrado que la sensibilidad al movimiento está altamente
correlacionada con la capacidad de conducción en adultos mayores [19,31-
34]. Una mayor edad está relacionada con la discapacidad de poder estimar
el tiempo antes del contacto, así como con la percepción de la velocidad y
dirección [35,36], capacidades críticas a la hora de dar respuestas rápidas y
fluidas ante los riesgos de la ruta. Incluso demoras breves en la detección
de blancos en movimiento pueden tener consecuencias fatales, y una
capacidad disminuida para discriminar la velocidad o el tiempo antes del
contacto pueden resultar en mayor riesgo de accidente.
Toda una serie de estudios también han evaluado la capacidad de
rapidez de procesamiento visual y la atención dividida para predecir
la seguridad de conducción, utilizando el UFOV Useful Field of
View (campo de visión útil) [37,38]. El UFOV es una tarea generada por
ordenador, que incluye la identificación simultánea de blancos centrales
y periféricos presentada en presencia o en ausencia de distractores,
y se basa en la atención dividida y selectiva, así como en la velocidad
de procesamiento visual rápido, que disminuye con la edad [37].
Una disminución en la eficacia del UFOV permite realizar un pronóstico
bastante fiable de los accidentes retrospectivos [13,39] como prospectivos
en grupos generales de adultos mayores [9,11,12] así como en los que
padecen de enfermedades oculares [24]. Se ha asociado una reducción
del 40 % del UFOV con 2,2 más probabilidad de estar involucrado
en un accidente en comparación con aquellos que no tienen ninguna
deficiencia del UFOV [9]. Algunos estudios también han encontrado
fuertes relaciones entre notas reducidas del UFOV y un comportamiento
poco seguro en la ruta [40,19] y los resultados en el simulador de
conducción [41]. El UFOV también es efectivo en la predicción del riesgo
de accidente prospectivo cuando se aplica en un contexto de obtención
del carné de conducir [42], lo cual suministra motivos adicionales para
que se incluya en la selección de conductores mayores. La figura 2
muestra la importancia del UFOV dentro del contexto de una escena
de conducción en el mundo real.
Los adultos mayores también experimentan niveles más elevados de
discapacidad ante el deslumbramiento en comparación con los jóvenes
adultos, debido a un aumento en la difusión de luz intraocular que reduce
la agudeza visual y el contraste a la sensibilidad, especialmente en
presencia de catarata [43]. Las situaciones de conducción en las que
el deslumbramiento discapacitante puede causar dificultades son
por la noche cuando los faros de otro coche aparecen delante del conductor
y también cuando el sol está bajo, al alba y en el crepúsculo. De esta
manera, los conductores mayores con niveles superiores de discapacidad
ante el deslumbramiento se autorregulan y reducen su exposición
a la conducción, especialmente durante la noche [14]. Mientras que
investigaciones anteriores no han podido encontrar relaciones significativas
entre la discapacidad por deslumbramiento y tasas de accidente con
culpa [17], sí hay pruebas que afirman que una mayor sensibilidad al
deslumbramiento está asociada al involucramiento en accidentes entre
los conductores mayores [11]. Estos hallazgos están en coherencia con los
hallazgos de un estudio con un simulador entre adultos mayores en donde
se demostró que ellos conducían de una manera menos segura cuando se
realizaban giros contra el tráfico y ante el deslumbramiento, especialmente
cuando los vehículos eran de bajo contraste [44].
Con el aumento de enfermedades oculares entre adultos mayores y las
reducciones asociadas en las funciones visuales, no es sorprendente que
muchas enfermedades oculares estén relacionadas con la disminución de
la eficacia de conducción y el aumento del riesgo de accidente.
Las patologías oculares más comunes que afectan a los adultos mayores y
su capacidad de conducir de manera segura incluyen la catarata,
el glaucoma y la degeneración macular asociada a la edad [45].
Muchas personas viven con cataratas durante periodos largos antes
de que estas sean extirpadas [46], y aproximadamente un cuarto de
estas personas siguen conduciendo incluso si su visión no cumple con
las normas legales de conducción [47,48]. Los conductores con catarata
registran mayores dificultades de conducción, conducen distancias más
cortas y evitan conducir en situaciones difíciles para ellos [46].
A pesar de limitar su exposición a la conducción, los conductores con
catarata tienen 2,5 veces más accidentes que el grupo control [46],
y, como se ha mencionado anteriormente, aquellos involucrados en
accidentes tienen 8 veces más probabilidades de tener una sensibilidad
al contraste reducida [17]. Estos hallazgos son sustentados por estudios
abiertos y cerrados, que han permitido demostrar que los conductores
con catarata simulada [49,50], o verdadera [19,51,52], tienen una conducción
deficiente en comparación con el grupo control. La cirugía de catarata
tiene un impacto positivo en las tasas de accidente y la eficacia en la
conducción. Un metaanálisis reciente sugiere que la cirugía de catarata
está asociada con una reducción del 88 % del riesgo de tener dificultades
en la conducción [53]. La tasa de accidentes en pacientes de catarata que
se operan son la mitad de los que no se operan [54]. Un análisis poblacional
retrospectivo (1997-2006) demostró que la cirugía de catarata redujo el
riesgo de accidente en un 13 %, lo cual supuso ahorros de 4,3 millones de
dólares [55]. En coherencia con estos hallazgos, la eficacia de la conducción
en la ruta a circuito cerrado mejoró después de la cirugía de catarata
bilateral, y el cambio mejor pronosticado fue la mayor sensibilidad al
contraste [56]. Estos estudios proporcionan pruebas convincentes de que
la cirugía de catarata puede proporcionar beneficios tangibles en la
seguridad en ruta [54], y debería realizarse en etapas más tempranas y no
tan tardías para mantener a los conductores seguros.
Los pacientes con glaucoma también encuentran dificultades
de conducción, incluyendo problemas con el deslumbramiento
y la conducción nocturna [57]. Se ha citado al glaucoma como una
de las razones principales por las que los conductores mayores dejan
de conducir [58]; pacientes con glaucoma bilateral tienen tres veces más
probabilidades de dejar de conducir que aquellos sin glaucoma [59].
Se ha demostrado que el glaucoma es un factor de riesgo significativo,
tanto en los accidentes que los pacientes mismos informan [60] como
los encontrados en los registros estatales de accidentes [23,24,61,62].
Los pacientes con pérdida de campo visual de origen glaucomatoso
Disminución del 50% del campo visual útil
Campo visual útil normalFIG. 2 Ilustración de la importancia del Campo Visual Útil
(UFOV) en una situación real de conducción.

Points de Vue - n°68 - Spring / Primavera - 2013 43
VISIÓN DE LAS PERSONAS MAYORES
Científico no médico
moderado o severo tenían 6 veces más probabilidades de tener un
accidente con culpa y 4 veces más probabilidades de ocasionar
cualquier tipo de accidente en comparación con aquellos que no tenían
ninguna pérdida de campo visual [23]. Aquellas personas involucradas
en accidentes con daños corporales tenían 3,6 veces más probabilidades
de padecer de glaucoma que aquéllos que no han sufrido accidentes [61].
El mayor riesgo de accidentes para los conductores con glaucoma
también se ha relacionado con sus deficiencias del UFOV [24].
Las evaluaciones en ruta de pacientes con glaucoma han puesto
de relieve las dificultades para no salirse de su carril, negociar curvas
y las capacidades de anticipación [26], y tienen mayores probabilidades
de que su instructor tenga que intervenir durante las evaluaciones en
ruta en comparación con los grupos control [63]. Una detección
y tratamiento precoces del glaucoma son críticos no solo para
minimizar la pérdida irreversible del campo visual, sino para mantener
la capacidad de conducir de manera segura.
Pocos estudios han abordado el impacto de la DMAE (degeneración
macular asociada a la edad) en la conducción, la mayoría de los
estudios se han focalizado en los aspectos que los mismos pacientes
informan de la conducción en vez de realizar mediciones objetivas
de la eficacia y seguridad de conducción. Los conductores con DMAE
afirman tener mayores dificultades para conducir [64], autorregulan sus
costumbres de conducción, evitan encontrarse en situaciones difíciles
de conducción [16,65] y adoptan comportamientos menos arriesgados [66]
en comparación con los conductores sin DMAE. Mientras que los
adultos mayores con DMAE han presentado niveles de conducción
inferiores en el simulador de conducción interactivo y en un test
de conducción en la ruta con tráfico [66], estas discapacidades no se
reflejaron en mayores tasas de accidentes [8]. La escasez de datos en
esta área pone de relieve la necesidad de realizar mas investigaciones
para evaluar el grado hasta el cual la DMAE tiene un impacto en la
conducción y el riesgo de accidente para poder identificar estrategias
para mejorar la seguridad de los conductores de este colectivo.
Uno de los problemas de los conductores mayores es que los cambios
en su visión pueden ir ocurriendo paulatinamente, de manera que
pueden no ser conscientes de que su visión ha alcanzado el grado
de ser una discapacidad, hasta que se produce un accidente en ruta o,
se diagnostica esta discapacidad a raíz de un examen de la visión.
Es poco probable que se detecten los cambios en las capacidades
visuales necesarias a la conducción si se sigue utilizando
la agudeza al alto contraste para evaluar las capacidades de
conducción en la obtención del carné. Mientras que pruebas
recientes sugieren claramente que las mediciones alternativas de la
función visual, incluyendo el UFOV, la sensibilidad al contraste y al
movimiento pueden ser más pertinentes para la eficacia y seguridad de
conducción, todavía queda por completar la evaluación y la validación
de estas pruebas. Además, mientras que existen pruebas contundentes
asociando la presencia de enfermedades oculares a las dificultades
de conducción, se necesitan estudios adicionales para
que se puedan proporcionar recomendaciones adecuadas a los
conductores mayores con estas discapacidades. •
REFERENCIAS
1. Burg A. The relationship between vision test scores and driving record: General findings. Los Angeles: Department of Engineering, University of California - Los Angeles; 1967:1-89.
2. Hofstetter HW. Visual acuity and highway accidents. J Am Optom Assoc 1976; 47:887-893.
3. Davison PA. Inter-relationships between British drivers’ visual abilities, age and road accident histories. Ophthalmic Physiol Opt 1985; 5:195-204.
4. Gresset J, Meyer F. Risk of accidents among elderly car drivers with visual acuity equal to 6/12 or 6/15 and lack of binocular vision. Ophthalmic Physiol Opt 1994; 14:33-37.
5. Marottoli RA, Richardson, E.D., Stowe, M.H., Miller, E.G., Brass, L.M., Cooney, L.M. & Tinetti, M.E. Development of a test battery to identify older drivers at risk for self-reported adverse driving events. J Am Geriatr Soc 1998; 46:562-568.
6. Ivers RQ, Mitchell P, Cumming RG. Sensory impairment and driving: The Blue Mountains eye study. Am J Public Health 1999; 89:85-87.
7. Decina LE, Staplin L. Retrospective evaluation of alternative vision screening criteria for older and younger drivers. Accid Anal Prev 1993; 25:267-275.
8. McCloskey LW, Koepsell TD, Wolf ME, Buchner DM. Motor vehicle collision injuries and sensory impairments of older drivers. Age Ageing 1994; 23:267-272.
9. Owsley C, Ball, K., McGwin, G., Sloane, M.E., Roenker, D.L., White, M.F. & Overley, T. Visual processing impairment and risk of motor vehicle crash among older adults. JAMA 1998; 279:1083-1088.
10. Keeffe JE, Jin CF, Weih LM, McCarty CA, Taylor HR. Vision impairment and older drivers: who’s driving? Br J Ophthalmol 2002; 86:1118-1121.
11. Rubin GS, Ng ES, Bandeen-Roche K, Keyl PM, Freeman EE, West SK. A prospective, population-based study of the role of visual impairment in motor vehicle crashes among older drivers: the SEE study. Invest Ophthalmol Vis Sci 2007; 48:1483-1491.
12. Cross JM, McGwin G, Jr., Rubin GS, et al. Visual and medical risk factors for motor vehicle collision involvement among older drivers. Br J Ophthalmol 2009; 93:400-404.
13. Ball K, Owsley C, Sloan ME, Roenker DL, Bruni JR. Visual attention problems as a predictor of vehicle crashes in older drivers. Invest Ophthalmol Vis Sci 1993;34:3110-3123.
14. Brabyn JA, Schneck ME, Lott LA, Haegerstrom-Portnoy G. Night driving self-restriction: vision function and gender differences. Optom Vis Sci 2005; 82:755-764.
15. Keay L, Munoz B, Turano KA, et al. Visual and cognitive deficits predict stopping or restricting driving: the Salisbury Eye Evaluation Driving Study (SEEDS). Invest Ophthalmol Vis Sci 2009; 50:107-113.
16. Ball K, Owsley C, Stavey B, Roenker DL, Sloane ME, Graves M. Driving avoidance and functional impairment in older drivers. Accid Anal Prev 1998; 30:313-322.
17. Owsley C, Stalvey BT, Wells J, Sloane ME, McGwin G, Jr. Visual risk factors for crash involvement in older drivers with cataract. Arch Ophthalmol 2001; 119:881-887.
18. Wood JM, Dique T, Troutbeck R. The effect of artificial visual impairment on functional fields and driving performance. Clin Vis Sci 1993; 8:563-575.
19. Wood JM. Age and visual impairment decrease driving performance as measured on a closed-road circuit. Hum Factors 2002; 44:482-494.
20. Wood JM, Owens DA. Standard measures of visual acuity do not predict drivers’ recognition performance under day or night conditions. Optom Vis Sci 2005; 82:698-705.
21. Johnson CA, Keltner JL. Incidence of visual field loss in 20,000 eyes and its relationship to driving performance. Arch Ophthalmol 1983; 101:371-375.
22. Council FM, Allen JA. A study of the visual fields of North Carolina drivers and theri relationship to accidents. Chapel Hill: University of North Carolina. Highway Research Saferty Centre.; 1974.
23. McGwin G, Jr., Xie A, Mays A, et al. Visual field defects and the risk of motor vehicle collisions among patients with glaucoma. Invest Ophthalmol Vis Sci 2005; 46:4437-4441.
24. Haymes SA, Leblanc RP, Nicolela MT, Chiasson LA, Chauhan BC. Risk of falls and motor vehicle collisions in glaucoma. Invest Ophthalmol Vis Sci 2007;48:1149-1155.
25. Wood JM, Troutbeck R. The effect of restriction of the binocular visual field on driving performance. Ophthalmic Physiol Opt 1992; 12:291-298.
26. Bowers A, Peli E, Elgin J, McGwin G, Owsley C. On-road driving with moderate visual field loss. Optom Vis Sci 2005; 82:657-667.
27. Racette L, Casson EJ. The impact of visual field loss on driving performance: evidence from on-road driving assessments. Optom Vis Sci 2005; 82:668-674.
28. Wood JM, McGwin Jr G, Elgin J, et al. On-road driving performance by persons with hemianopia and quadrantanopia. Invest Ophthalmol Vis Sci 2009;50:577-585.
29. Crabb DP, Fitzke FW, Hitchings RA, Viswanathan AC. A practical approach to measuring the visual field component of fitness to drive. Br J Ophthalmol 2004; 88:1191-1196.
30. Chisholm CM, Rauscher FG, Crabb DC, et al. Assessing visual fields for driving in patients with paracentral scotomata. Br J Ophthalmol 2008; 92:225-230.
31. Henderson S, Donderi DC. Peripheral motion contrast sensitivity and older drivers’ detection failure accident risk., Proceedings of the Third International Driving Symposium on Human Factors in Driver Assessment, Training and Vehicle Design. Rockport, Maine; 2005:41-50.
32. Henderson S, Gagnon S, Bélanger A, Tabone R, Collin C. Near peripheral motion detection threshold correlates with self-reported failures of attention in younger and older drivers. Accid Anal Prev 2010; 42:1189-1194.
33. Raghuram A, Lakshminarayanan V. Motion perception tasks as potential correlates to driving
difficulty in the elderly. Journal of Modern Optics 2006; 53:1343-1362.
34. Wood JM, Anstey KJ, Kerr GK, Lacherez P, Lord S. A multi-domain approach for predicting older driver safety under in-traffic road conditions. J Am Geriatr Soc 2008; 56:986-993.
35. Conlon E, Herkes K. Spatial and temporal processing in healthy aging: Implications for perceptions of driving skills. Aging, Neuropsychol Cog 2008; 15:446-470.
36. DeLucia PR, Mather R. Motion extrapolation of car-following scenes in younger and older drivers. Hum Factors 2006; 48:666-674.
37. Ball KK, Beard BL, Roenker DL, Miller RL, Griggs DS. Age and visual search: expanding the useful field of view. J Am Optom Assoc 1988;5:2210-2219.
38. Ball K, Owsley C. The useful field of view test: a new technique for evaluating age-related declines in visual function. J Am Optom Assoc 1992; 63:71-79.
39. Owsley C, Ball, K., Sloane, M.E., Roenker, D.L. & Bruni, J.R. Visual/cognitive correlates of vehicle accidents in older drivers. Psychol Aging 1991; 6:403-415.
40. Myers RS, Ball KK, Kalina TD, Roth DL, Goode KT. Relation of useful field of view and other screening tests to on-road driving performance. Percept Mot Skills 2000; 91:279-290.
41. Roenker DL, Cissell GM, Ball KK, Wadley VG, Edwards JD. Speed-of-processing and driving simulator training result in improved driving performance. Hum Factors 2003; 45:218-233.
42. Ball K, Roenker DL, Wadley VG, et al. Can high-risk older drivers be identified through performance-based measures in a Department of Motor Vehicles setting? J Am Geriatr Soc 2006; 54:77-84.
43. Elliott DB, Bullimore MA. Assessing the reliability, discriminative ability, and validity of disability glare tests. Invest Ophthalmol Vis Sci 1993; 34:108-119.
44. Gray R, Regan D. Glare susceptibility test results correlate with temporal safety margin when executing turns across approaching vehicles in simulated low-sun conditions. Ophthalmic Physiol Opt 2007; 27:440-450.
45. Wang JJ, Foran S, Mitchell P. Age-specific prevalence and causes of bilateral and unilateral visual impairment in older Australians: the Blue Mountains Eye Study. Clin Experiment Ophthalmol 2000; 28:268-273.
46. Owsley C, Stalvey B, Wells J, Sloane ME. Older drivers and cataract: drivng habits and crash risk. J Gerontol 1999; 54A:M203-M211.
47. Monestam E. Impact of cataract surgery. A population based approach. Acta Ophthalmol Scand 1999; 77:729.
48. Pager CK, McCluskey PJ, Retsas C. Cataract surgery in Australia: a profile of patient-centred outcomes. Clin Experiment Ophthalmol 2004; 32:388-392.
49. Wood JM, Troutbeck R. Effect of visual impairment on driving. Hum Factors 1994; 36:476-487.
50. Wood JM, Troutbeck R. Elderly drivers and simulated visual impairment. Optom Vis Sci 1995; 72:115-124.
51. Wood JM, Mallon K. Comparison of driving performance of young and old drivers (with and without visual impairment) measured during in-traffic conditions. Optom Vis Sci 2001; 78:343-349.
52. Wood JM, Carberry TP. Older drivers and cataracts: measures of driving performance before and after cataract surgery. Transportation Research Record 2004; 1865:7-13.
53. Subzwari S, Desapriya E, Scime G, Babul S, Jivani K, Pike I. Effectiveness of cataract surgery in reducing driving-related difficulties: a systematic review and meta-analysis. Inj Prev 2008; 14:324-328.
54. Owsley C, McGwin G, Jr, Sloane M, Wells J, Stalvey BT, Gauthreaux S. Impact of cataract surgery on motor vehicle crash involvement by older adults. JAMA 2002; 288:841-849.
55. Meuleners LB, Hendrie D, Lee AH, Ng JQ, Morlet N. The effectiveness of cataract surgery in reducing motor vehicle crashes: a whole population study using linked data. Ophthalmic Epidemiol 2012; 19:23-28.
56. Wood JM, Carberry TP. Bilateral cataract surgery and driving performance. Br J Ophthalmol 2006; 90:1277-1280.
57. Janz NK, Musch DC, Gillespie BW, Wren PA, Niziol LM. Evaluating clinical change and visual function concerns in drivers and nondrivers with glaucoma. Invest Ophthalmol Vis Sci 2009; 50:1718-1725.
58. Hakamies-Blomqvist L, Wahlstrom B. Why do older drivers give up driving? Accid Anal Prev 1998; 30:305-312.
59. Ramulu PY, West SK, Munoz B, Jampel HD, Friedman DS. Driving cessation and driving limitation in glaucoma: the Salisbury Eye Evaluation Project. Ophthalmology 2009; 116:1846-1853.
60. Tanabe S, Yuki K, Ozeki N, et al. The association between primary open-angle glaucoma and motor vehicle collisions. Invest Ophthalmol Vis Sci 52:4177-4181.
61. Owsley C, McGwin G, Ball K. Vision impairment, eye disease, and injurious motor vehicle crashes in the elderly. Ophthalmic Epidemiol 1998;5:101-113.
62. Hu PS, Trumble DA, Foley DJ, Eberhard JW, Wallace RB. Crash risks of older drivers: a panel data analysis. Accid Anal Prev 1998;30:569-581.
63. Haymes SA, Leblanc RP, Nicolela MT, Chiasson LA, Chauhan BC. Glaucoma and on-road driving performance. Invest Ophthalmol Vis Sci 2008; 49:3035-3041.
64. Mangione CM, Gutierrez PR, Lowe G, Orav EJ, Seddon JM. Influence of age-related maculopathy on visual functioning and health-related quality of life. Am J Ophthalmol 1999; 128:45-53.
65. Weaver Moore L, Miller M. Driving strategies used by older adults with macular degeneration: assessing the risks. Appl Nurs Res 2005; 18:110-116.
66. Szlyk JP, Pizzimenti CE, Fishman GA, et al. A comparison of driving in older subjects with and without age-related macular degeneration. Arch Ophthalmol 1995; 113:1033-1040.

Points de Vue - n°68 - Spring / Primavera - 201344
VISIÓN DE LAS PERSONAS MAYORES
Científico no médico
V I S U A L I Z A N D O L A V I S I Ó N , C O M P R E N D I E N D O L A S N E C E S I D A D E S
D E L A V I S I Ó N
D E L A S P E R S O N A S M A Y O R E S
__ INTRODUCCIÓN
El envejecimiento de la población es un fenómeno global.
Se ha proyectado que, de aquí al 2030, en 55 países, la población
de 60 años y mayores representará por lo menos el 20 % de la población
total. Actualmente, hay una mayor cantidad de personas de 60 años
y mayores que el total de las poblaciones de Rusia, Japón, Francia,
Alemania y Australia sumadas. A nivel mundial, hay 800 millones
de personas de 60 años o mayores. Se proyecta que en el 2020,
la población mundial de personas de 60 años y mayores alcanzará los
1.000 millones y hacia 2050, la cantidad de este colectivo se duplicará
para llegar a 2.000 millones con más de una de cada cuatro personas
de 60 años y mayores que vivirán en Europa, EE. UU. y China.
El envejecimiento de la población no solo plantea nuevos desafíos sino
también nuevas oportunidades. Estudios actuales sobre la población que
envejece revelan que la mayoría de las personas mayores aceptan bien
el envejecimiento, tienen vidas más sanas y felices, tienen una actitud
positiva y disfrutan de su vida con actividades tanto en espacios interiores
como exteriores. Por lo tanto, es evidente que la sociedad necesita ofrecer
una variedad de servicios para envejecer con una buena calidad de vida.
__ PROBLEMAS DE VISIÓN ENTRE LAS PERSONAS MAYORES JÓVENES Y LAS MÁS MADURAS
Según un estudio reciente del IPSOS - 2011[1] las personas mayores
tienen problemas de visión relacionados principalmente con las condiciones
luminosas. Aproximadamente el 60 % de los encuestados (en el grupo
de edad de 60 y mayores) han reconocido experimentar problemas
de la visión como por ejemplo dificultades en la visión cercana con poca
luz, sensibilidad a la luz brillante o problemas en la visión nocturna.
Incluso con un buen par de gafas correctoras experimentan una cierta falta
de comodidad. Algunos encuestados mencionaron dificultad para leer letras
pequeñas, por ejemplo las instrucciones de uso de los medicamentos.
Muchas personas mayores también han mencionado
una cierta falta de comodidad en la lectura debido al poco contraste,
por ejemplo, al leer las letras sobre fondos de color en las revistas.
Además, la mayoría de la población de 60 años o más ha admitido
experimentar la sensibilidad a la luz solar en exteriores, y el 17 %
de este grupo de edad también ha afirmado haber tenido algunas
molestias con el deslumbramiento proveniente del exterior.
Estos síntomas son aún mayores en las personas que sufren de cataratas.
Antes de la cirugía, más del 75 % de las personas mayores sufrían de
varios de los problemas de visión anteriormente mencionados. La cirugía
de catarata permite aliviar varios de estos problemas,
pero la sensibilidad a la luz sigue siendo un problema no corregido y el
grupo de edad de personas más maduras, al tratar de proteger sus ojos,
termina llevando gafas de sol para disminuir el efecto adverso de la luz.
__ CAMBIOS FISIOLÓGICOS DEBIDOS AL ENVEJECIMIENTO
Aunque la presbicia se estabiliza a la edad de 60 años, pueden
ocurrir cambios físicos en casi todos los órganos que pueden afectar
la salud y estilo de vida de las personas mayores. En general,
los cambios en las últimas etapas de la vida acarrean una disminución
general de todos los sistemas de los órganos debido a un declive
gradual en la actividad celular. Junto con una gran variedad
de cambios fisiológicos que acompañan el proceso de envejecimiento,
también ocurren cambios sensoriales (visión, oído, sensibilidad
de la piel, gusto y olor) [3]. Aproximadamente, el 65 % de las personas con
discapacidades visuales tienen 50 años o más. Con una población
cada vez más envejecida en muchos países, será mayor el número
de personas que se encontrarán ante el riesgo de discapacidades visuales
asociadas a la edad [14]. Aunque la discapacidad visual puede asociarse
a pérdidas neuronales, el declive principal se debe a cambios en los
elementos ópticos de los ojos [9,13].
En general, la agudeza visual disminuye con la edad (de 10/10 a 6/10
NATHALIE BAR Responsable de los estudios de mercado Essilor InternationalFrancia
BIDISHA RUDRA Ph.D, Director Asociado, Decision Science, Market Research & Analysis, Essilor of AmericaEEUU
ANNE-CATHERINE SCHERLEN PhD, Encargada de la investigación I&D Óptica - Baja Visión, Instituto de la Visión - Essilor InternationalFrancia
FIG. 1 Conducción de noche. Pérdida de la sensibilidad al contraste, deslumbramiento.
VISIÓN DE LAS PERSONAS MAYORES
Científico no médico

Points de Vue - n°68 - Spring / Primavera - 2013 45
VISIÓN DE LAS PERSONAS MAYORES
Científico no médico
incrementará la pérdida de las funciones visuales mencionadas
anteriormente. Por ejemplo, la falta de comodidad relacionada
con el deslumbramiento es aumentada por el fenómeno de dispersión de
la luz en el ojo ocasionada por opacidades (las cataratas,
por ejemplo) o pérdidas de fotorreceptores como la degeneración macular
asociada a la edad (DMAE) [2].
__ PROYECTÁNDONOS EN EL FUTURO
En la época actual, con tantos avances tecnológicos, los jubilados,
las personas mayores no solamente todavía se sienten jóvenes sino que
también disfrutan de una vida mucho más activa que las generaciones
precedentes. Una buena visión es realmente la clave para su productividad
continua y bienestar general. Esto les permitirá mantener realizando sus
actividades regulares a la vez que siguen siendo independientes.
En conclusión, no solamente es crucial detectar los problemas
patológicos y fisiológicos que experimentan las personas mayores sino que
también es muy importante dedicar tiempo para escuchar y comprender
sus necesidades visuales diarias. Una charla detallada y exhaustiva con
las personas mayores, contribuirá a suministrar las soluciones necesarias y
efectivas que permitirán disfrutar los beneficios de una buena visión para
vivir una vida larga, independiente y cómoda. •
entre 65 y 90 años). Esta disminución es aún mayor cuando el contraste
es bajo [10]. Efectivamente, la dificultad para leer con luminosidad baja
como lo expresan las personas mayores se asocia a un declive en la
sensibilidad al contraste espacial. La luminancia retiniana en los ojos de
las personas mayores se reduce debido a la miosis y al aumento de la
densidad del cristalino [4,9]. También hay una mayor dispersión de la luz
intraocular y mayores aberraciones ópticas durante el envejecimiento [12].
Algunos estudios también han determinado que la densidad de las células
neurales disminuye con el envejecimiento. Hacia los 60-70 años, la
densidad de los fotorreceptores de los bastones y las células ganglionares
disminuyen drásticamente en la perimácula. Los adultos mayores
necesitan, de media, tres veces más contraste que los adultos más
jóvenes para poder determinar una diana. Aunque la falta de comodidad
principal de las personas mayores es la pérdida de la eficacia visual con
poca luminosidad, el primer signo del envejecimiento retiniano es el
tiempo que necesita la retina periférica para adaptarse a la oscuridad [6].
Esta pérdida de sensibilidad escotópica se debe a la menor velocidad de
la regeneración de los fotopigmentos (rodopsina). Las personas mayores
sienten mayores dificultades para adaptarse a los cambios de la brillantez,
lo cual explica las dificultades asociadas con la conducción nocturna. El
rendimiento visual disminuye durante el tiempo que necesita la retina
para llevar a cabo sus procesos. La agudeza visual, la sensibilidad al
contraste, el campo de atención y la percepción del movimiento necesitan
aún un mayor tiempo de adaptación [7,9].
Sin ningún remedio disponible a estos problemas, el colectivo
de personas mayores simplemente evitan conducir de noche.
Por otro lado, la presencia de demasiada luz también penaliza
considerablemente la comodidad visual de las personas mayores [8]. En
este caso, la disminución del tiempo de regeneración del pigmento visual
de los conos (llamado opsina) de la retina central afecta al tiempo de
recuperación en presencia de luz [11,2]. La retina queda inundada de luz
lo cual conduce a un efecto de deslumbramiento del ojo, asociado con
diferentes faltas de comodidad como dolores, pérdida de la sensibilidad al
contraste y agudeza visual. El tiempo de la recuperación visual depende
de la edad y del tiempo de exposición a la luz.
El envejecimiento natural afecta a varias funciones visuales lo cual
impacta negativamente las actividades de la vida diaria de un individuo.
Es importante recalcar que la presencia de una patología visual, como
las cataratas, la degeneración macular asociada a la edad o el glaucoma,
FIG. 2 Dispersión de la luz intraocular.
FIG. 3 Efecto del envejecimiento en la sensibilidad al contraste.
REFERENCIAS
1. Ipsos Public Affairs, Observatoire de la Maturité, 2011.
2. Aguirre RC, Colombo EM, Barraza JF. (2011) Effect of glare on reaction time for peripheral vision at mesopic adaptation. J Opt Soc Am A Opt Image Sci Vis. Oct 1; 28(10):2187-91.
3. Brabyn J, Schneck M, Haegerstrom-Portnoy G, Lott L. (2001) The Smith-Kettlewell Institute (SKI) longitudinal study of vision function and its impact among the elderly: an overview. Optom Vis Sci, 78:264-269.
4. Franssen L, Tabernero J, Coppens JE, van den Berg TJ. (2007) Pupil size and retinal straylight in the normal eye.Invest Ophthalmol Vis Sci. May; 48(5):2375-82.
5. He, W., Muenchrath M.N., Kowal, P (2012) Shades of Gray: A Cross-Country Study of Health and Well-Being of the Older Populations in SAGE Countries, 2007-2010.
6. Jackson, G. R., Owsley, C., & McGwin, G. Jr. (1999) Aging and dark adaptation. Vision Research, 39, 3975-3982.
7. Kaleem MA, Munoz BE, Munro CA, Gower EW, West SK. (2012) Visual characteristics of elderly night drivers in the Salisbury Eye Evaluation Driving Study. Invest Ophthalmol Vis Sci. Aug 3; 53(9):5161-7.
8. Mainster MA, Turner PL. (2012) Glare’s causes, consequences, and clinical challenges after a century of ophthalmic study.Am J Ophthalmol. Apr; 153(4):587-93.
9. Owsley, C. (2010) Aging and vision: review. Vision Research, Jul 1; 51(13):1610-22.
10. Schneck ME, Haegerström-Portnoy G. (2003) Practical assessment of vision in the elderly. Ophthalmol Clin North Am. Jun; 16(2):269-87.
11.Stringham JM, Garcia PV, Smith PA, McLin LN, Foutch BK. (2011) Macular pigment and visual performance in glare: benefits for photostress recovery, disability glare, and visual discomfort. Invest Ophthalmol Vis Sci. Sep 22; 52(10).
12. van den Berg TJ, Franssen L, Coppens JE. (2009) Straylight in the human eye: testing objectivity and optical character of the psychophysical measurement. Ophthalmic Physiol Opt. May; 29(3): 345-50.
13. Werner, J. S., Schefrin, B. E., & Bradley, A. (2010) Optics and vision of the aging eye. In Handbook of optics. In M. Bass, J. M. Enoch, & V. Lakshminarayanan (Eds.). Vision and vision optics (Vol. 3, 3rd ed., pp. 14.11–14.38). New York: McGraw-Hill.
14. World Health Organisation, World report on disability 2011. ISBN 978 92 4 156418 http://www.who.int/disabilities/world_report/2011/en/index.html
http://linkedage.com/read/facts

Points de Vue - n°68 - Spring / Primavera - 201346
LUZ AZUL
Científico médico
N U E V O S D E S C U B R I M I E N T O SY T E R A P I A S R E L A T I V A S
A L A F O T O T O X I C I D A D
R E T I N I A N A
LUZ AZUL
Científico médico
__ INTRODUCCIÓN
La degeneración macular asociada a la edad o DMAE es una de las
causas principales de la mala visión en los países industrializados junto
con la retinopatía diabética y el glaucoma. En EE. UU., la DMAE es
considerada la causa del 54,4 % de las deficiencias visuales y del 22,9 %
de los casos de ceguera [1]. Se ha estimado que en el 2010, 9,1 millones
de americanos de más de 50 años presentaban un inicio de DMAE [2],
y que el número podría duplicarse de aquí al 2050 hasta alcanzar
los 17,8 millones. Por lo menos el 12 % de la población de EE. UU.
y de Europa mayor de 80 años está afectada por una DMAE avanzada [3-5].
Entre los factores de riesgo identificados de la DMAE, los estudios han
determinado que la luz solar es un factor que puede inducir daños
acumulativos en la retina. También ha sido identificada como tal
la porción del espectro visible de mayor energía, comprendida entre
los 400 nm y los 500 nm, denominada luz azul.
Algunos dispositivos oftálmicos ya reivindican una protección contra
la luz azul. Se trata de lentes de gafas o de implantes intraoculares
que tienen, la mayoría de ellos, filtros de paso alto que absorben una
franja amplia de la luz azul. Un filtrado tan poco selectivo puede
inducir un desajuste de las funciones visuales y no visuales del ojo. La
percepción de los colores queda perturbada, la visión escotópica es limitada
y el reloj interno de regulación del ritmo circadiano que algunas radiaciones
de la luz azul controla puede quedar potencialmente desajustado.
La poca especificidad de los dispositivos filtrantes existentes está ligada a la
falta de información sobre la toxicidad relativa a cada longitud
de onda del espectro visible en la retina. Por este motivo, en 2008, Essilor
International y el Instituto de la Visión se asociaron para determinar de
manera más fina la nocividad de la luz azul en la retina
y desarrollar lentes filtrantes protectoras más selectivas.
__ LA LUZ: UN FACTOR DE RIESGO EN LA DMAE
Actualmente, las causas de la DMAE están mal identificadas,
no existen soluciones preventivas ni curativas eficaces.
Toda una serie de estudios epidemiológicos ponen en evidencia
una gran variedad de factores de riesgo potenciales. Aunque los primeros
factores bien identificados son la edad [5], el consumo del tabaco [5-8]
y las carencias en carotenoides [9], también se sospecha que la luz está
probablemente implicada en la prevalencia de la DMAE [10-14].
Una de las características de la DMAE es la aparición de depósitos
subretinianos denominados drusas [15, 16]. Dichos depósitos están
constituidos por lipofuscina, un producto de degradación del segmento
externo de los fotorreceptores y del pigmento visual. La lipofuscina,
debido a sus características fotosensibilizadoras, estaría implicada
en los daños retinianos ocasionados por la exposición a la luz.
__ LA LUZ AZUL: ¿CUÁL ES EL PELIGRO PARA LA RETINA?
En la retina, la luz es principalmente absorbida por los pigmentos
visuales contenidos en los segmentos externos de los fotorreceptores.
Los pigmentos visuales de los vertebrados están constituidos
por una proteína transmembranal, la opsina, en asociación con un
derivado de la vitamina A, el 11-cis-retinal. En los fotorreceptores de
tipo bastones, este pigmento visual es la rodopsina.
La mayoría de las radiaciones ultravioletas son filtradas naturalmente
por los tejidos oculares anteriores a la retina, particularmente la córnea
y el cristalino [17, 18]. La luz más energética que alcanza la retina es,
en su mayoría, la luz azul, comprendida entre 400 nm y 500 nm.
Debido a su alto nivel de energía, esta induce y acelera reacciones
fotoquímicas y daños celulares a través de la producción de especies de
radicales muy reactivas en presencia de oxígeno. En particular, el potencial
tóxico de la luz azul en la retina externa actúa en dos niveles celulares:
en los fotorreceptores y en las células del epitelio pigmentario retiniano.
En los fotorreceptores tipo bastones, la absorción de un fotón
por parte de la rodopsina induce a la isomerización y a la liberación
del 11-cis-retinal en all-trans-retinal. El all-trans-retinal libre no
solamente es tóxico en tanto que aldehído reactivo sino que también
presenta una fuerte sensibilidad a la luz azul [19,20]. En condiciones
de exposición luminosa moderada, las células del epitelio pigmentario
retiniano reciclan continuamente el all-trans-retinal en 11-cis-retinal
y no supone ningún peligro para la célula. Cuando la exposición a la
luz se prolonga o es más intensa, el all-trans-retinal se va acumulando
y en su activación, por la luz azul, puede estar al origen de un
estrés oxidativo que daña a los constituyentes celulares de los
fotorreceptores.
Este estrés oxidativo queda normalmente compensado por la presencia
de numerosos antioxidantes presentes en la retina. Pero, con la edad,
y algunos factores genéticos y del entorno, como el consumo de tabaco
o una alimentación pobre en antioxidantes, las defensas antioxidantes
quedan disminuidas [21, 22] y ya no consiguen compensar el estrés
inducido por una exposición prolongada o intensa a la luz azul.
Las células del epitelio pigmentario retiniano tienen como función
asegurar la renovación del segmento externo de los fotorreceptores.
Dichas células eliminan la parte distal por ingestión o «fagocitosis»,
mientras que el crecimiento de estos segmentos externos se realiza
continuamente [23]. Cuando estos elementos externos están
demasiado dañados por el estrés oxidativo, las células del epitelio
pigmentario retiniano pueden difícilmente degradar sus constituyentes
membranales. La digestión intracelular es entonces incompleta
y genera una acumulación de cuerpos granulares residuales bajo forma
de lipofuscina. Los gránulos de lipofuscina contienen muchos lípidos
poliinsaturados, dianas de la oxidación. El extracto lipófilo
de la lipofuscina contiene un fotosensibilizador potencial que forma
SERGE PICAUD PhD, Director de investigación en el Inserm Instituto de la VisiónFrancia© Inserm/L.Prat
EMILIE ARNAULTPhD, Jefe de proyecto en Fotobiología en la Universidad Pierre y Marie Curie Instituto de la visiónFrancia

Points de Vue - n°68 - Spring / Primavera - 2013 47
LUZ AZUL
Científico médico
un estado excitado triplete con un máximo de absorción en el azul
de unos 440 nm [24, 25]. Se ha identificado a uno de los constituyentes
de la lipofuscina, el A2E, como participante en el carácter
fotosensibilizador del residuo lipídico. La energía del estado triplete es
suficiente para ser transferida y reaccionar con el oxígeno sanguíneo.
La fotoactivación de los gránulos de lipofuscina por la luz azul genera
especies de oxígeno reactivas (superóxido, peróxido de hidrógeno,
hiperóxidos lipídicos y malondialdehído) [26, 27]. A partir del momento
en el que el número de estas especies supera la capacidad de las
defensas celulares, las células del epitelio pigmentario retiniano
mueren por apoptsosis. Los fotorreceptores, al quedar privados
de estas células de apoyo que suministraban sus aportaciones
energéticas, a su vez, degeneran y participan en la pérdida de visión
diagnosticada en los pacientes afectados de DMAE.
En conclusión, el mecanismo que se propone en el cual la luz está
involucrada en la aparición y el avance de la DMAE puede apreciarse
en dos niveles. Por un lado, en los fotorreceptores mediante la absorción
de la luz azul por la rodopsina y en el azul cercano a los UV por parte
del all-trans-retinal; y por otro, en el epitelio pigmentario retiniano,
mediante la absorción del azul por la lipofuscina.
__ LIMITACIONES DE LOS ESTUDIOS EXISTENTES
Ya se han puesto en evidencia experimentalmente los efectos tóxicos
de la luz visible y de la luz azul en particular en la retina, en modelos
celulares [28-30] y animales [31] en patologías degenerativas retinianas.
No obstante, los estudios realizados hasta ahora no han permitido
caracterizar la toxicidad respectiva de cada longitud de onda. Además,
estos presentan ciertas limitaciones. Efectivamente, las comparaciones
de los resultados son difíciles de un estudio a otro porque las unidades
fluctúan entre las unidades energéticas y las visuales. Por otra parte,
los sistemas de iluminación utilizados no están calibrados sobre la base
de la iluminación de fuentes de luz existentes en nuestro entorno, ya sean
estas naturales (Sol) o artificiales (neón, LED, halógenos) no pudiendo
así reflejar las condiciones reales de exposición a la luz. Finalmente,
ninguno de los sistemas de iluminación utilizados permite hasta el día
de hoy determinar paso a paso el espectro tóxico de la luz en las células
de la retina. La única información recurrente es que los niveles máximos
toxicidad están contenidos en el intervalo espectral [400 nm; 500 nm].
__ LA CONTRIBUCIÓN DEL INSTITUTO DE LA VISIÓN Y DE ESSILOR INTERNATIONAL
El objetivo de esta contribución consistía en establecer,
en cooperación con Essilor International, un laboratorio de fotobiología
en el Instituto de la Visión que permitiera determinar con precisión
la toxicidad específica en la retina de cada longitud de onda de la parte
azul del espectro visible.
La primera acción se realizó en torno al desarrollo de un sistema
de iluminación celular que permitiera producir longitudes de onda
de la luz visible con anchos de banda muy estrechos y con una
iluminación definida para modelizar el espectro luminoso deseado.
La fuente de luz a la que solemos exponernos más y también la
más intensa, es el Sol. Se realizó todo un trabajo utilizando en cada
longitud de onda valores de irradiancias relativas al espectro solar.
La segunda vertiente se basó en el desarrollo de un modelo de células
en cultivo que reprodujeran in vitro la degeneración de las células
retinianas observada en la DMAE, mediante la presencia de un
constituyente de la lipofuscina, el A2E.
__ MATERIAL Y MÉTODO
El sistema de iluminación desarrollado es un generador multi-
longitud de ondas que permite iluminar a las células en cultivo dentro
de una incubadora. La fuente luminosa está compuesta de un conjunto
de diodos electroluminiscentes (LED), cada uno de los cuales está
unido a la incubadora y hasta las células mediante fibras ópticas.
La gama de longitudes de onda cubierta se extiende de 390 nm
a 520 nm por bandas de 10 nm (fig. 1). De esta manera, el conjunto
permite limitar, en cada fibra óptica, la iluminación hasta los 10 nm
del espectro que llega a la retina.
Para modelizar la acumulación de lipofuscina que actúa en la retina,
se aplicó un tratamiento a las células de cultivo del epitelio pigmentario
de cerdo con diferentes concentraciones de A2E, uno de los constituyentes
de la lipofuscina (fig. 2). Estas células fueron expuestas a un ancho
de banda de luz de 10 nm durante 18 horas. Seis horas después
de la exposición, se caracterizaron los efectos de la luz en las células
con arreglo a tres parámetros: el porcentaje de células vivas, la actividad
apoptótica de las células y el porcentaje de células en necrosis.
FIG. 1 Vista desde arriba de una lámina de cultivo celular iluminada por diferentes longitudes de onda de 390 a 520 nm.

Points de Vue - n°68 - Spring / Primavera - 201348
LUZ AZUL
Científico médico
__ RESULTADOS
La cuantificación de las células vivas revela que la exposición a la luz
induce una mortalidad celular solo cuando las células han sido tratadas
con el A2E (fig. 3). Esta fototoxicidad está indicada por la activación
de una enzima, la caspase-3, involucrada en los procesos de muerte
programada (apoptosis). En contraste, no se observó la necrosis
de las células en estas condiciones experimentales. Nuestros resultados
también muestran que cuanto mayor es la concentración del A2E mayor
es el efecto tóxico de la luz. Estos resultados muestran que existe
un efecto dosis-dependiente de la A2E y, por lo tanto, probablemente
de la lipofuscina en la inducción de la fototoxicidad.
Esto puede relacionarse con la influencia de la edad en la DMAE puesto
que se ha observado que las drusas y la lipofuscina se acumulan con
la edad y están presentes en cantidades superiores en los pacientes
mayores que padecen de DMAE [15, 16, 32, 33].
__ CONCLUSIÓN Y PERSPECTIVAS
El trabajo común del Instituto de la Visión y de Essilor International
ha permitido establecer un proceso experimental que saca partido
de un modelo celular de DMAE para determinar el espectro preciso
de la toxicidad de la luz solar en la retina. Estos resultados suministran
información capital sobre la necesidad de protegerse de longitudes
de onda muy específicas de la luz azul. Es importante observar
que estas longitudes de onda también están presentes en proporciones
variables en diferentes fuentes de luz artificial (neón, LED, xenón,
halógeno, etc.) y que no hay que descuidar los efectos potenciales
de una exposición de larga duración. Este proyecto aporta elementos
de comprensión de los procesos fisiopatológicos que participan
en la DMAE incluso en la propuesta de soluciones terapéuticas
o de prevención, para esta patología tan importante. Este tipo
de soluciones terapéuticas podría extenderse hacia otras patologías
retinianas en las que participan procesos de estrés oxidante
y que inducen a la degeneración de los fotorreceptores,
como la retinitis pigmentaria y la enfermedad de Starfardt.
La asociación de las competencias respectivas del Instituto de la Visión
en biología celular de la retina y de Essilor International en óptica han sido
esenciales para establecer este proyecto innovador en la oftalmología. •
REFERENCIAS
1. Congdon, N., et al., Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol, 2004. 122(4): p. 477-85.
2. Rein, D.B., et al., Forecasting age-related macular degeneration through the year 2050: the potential impact of new treatments. Arch Ophthalmol, 2009. 127(4): p. 533-40.
3. Augood, C.A., et al., Prevalence of age-related maculopathy in older Europeans: the European Eye Study (EUREYE). Arch Ophthalmol, 2006. 124(4): p. 529-35.
4. Friedman, D.S., et al., Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol, 2004. 122(4): p. 564-72.
5. Smith, W., et al., Risk factors for age-related macular degeneration: Pooled findings from three continents. Ophthalmology, 2001. 108(4): p. 697-704.
6. Seddon, J.M., S. George, and B. Rosner, Cigarette smoking, fish consumption, omega-3 fatty acid intake, and associations with age-related macular degeneration: the US Twin Study of Age-Related Macular Degeneration. Arch Ophthalmol, 2006. 124(7): p. 995-1001.
7. Evans, J.R., A.E. Fletcher, and R.P. Wormald, 28,000 Cases of age related macular degeneration causing visual loss in people aged 75 years and above in the United Kingdom may be attributable to smoking. Br J Ophthalmol, 2005. 89(5): p. 550-3.
8. Khan, J.C., et al., Smoking and age related macular degeneration: the number of pack years of cigarette smoking is a major determinant of risk for both
geographic atrophy and choroidal neovascularisation. Br J Ophthalmol, 2006. 90(1): p. 75-80.
9. Ma, L., et al., Lutein and zeaxanthin intake and the risk of age-related macular degeneration: a systematic review and meta-analysis. Br J Nutr, 2012. 107(3): p. 350-9.
10. Butt, A.L., et al., Prevalence and risks factors of age-related macular degeneration in Oklahoma Indians: the Vision Keepers Study. Ophthalmology, 2011. 118(7): p. 1380-5.
11. Vojnikovic, B., et al., Epidemiological study of sun exposure and visual field damage in children in Primorsko-Goranska County--the risk factors of earlier development of macular degeneration. Coll Antropol, 2011. 34 Suppl 2: p. 57-9.
12. Fletcher, A.E., et al., Sunlight exposure, antioxidants, and age-related macular degeneration. Arch Ophthalmol, 2008. 126(10): p. 1396-403.
13. Mitchell, P., W. Smith, and J.J. Wang, Iris color, skin sun sensitivity, and age-related maculopathy. The Blue Mountains Eye Study. Ophthalmology, 1998. 105(8): p. 1359-63.
14. Darzins, P., P. Mitchell, and R.F. Heller, Sun exposure and age-related macular degeneration. An Australian case-control study. Ophthalmology, 1997. 104(5): p. 770-6.
15. Curcio, C.A. and C.L. Millican, Basal linear deposit and large drusen are specific for early age-related maculopathy. Arch Ophthalmol, 1999. 117(3): p. 329-39.
16. Sarks, S., et al., Relationship of Basal laminar deposit and membranous debris to the clinical
presentation of early age-related macular degeneration. Invest Ophthalmol Vis Sci, 2007. 48(3): p. 968-77.
17. Boettner, E.A. and J.R. Wolter, Transmission of the ocular media. Investigative Ophthalmology, 1962. 1(6).
18. Lund, D.J., et al., A Computerized Approach to Transmission and Absorption Characteristics of the Human Eye, in CIE 203:2012. 2012, International Commission on illumination. p. 68.
19. Rozanowska, M. and T. Sarna, Light-induced damage to the retina: role of rhodopsin chromophore revisited. Photochem Photobiol, 2005. 81(6): p. 1305-30.
20. Ng, K.P., et al., Retinal pigment epithelium lipofuscin proteomics. Mol Cell Proteomics, 2008. 7(7): p. 1397-405.
21. Kaya, S., et al., Comparison of macular pigment in patients with age-related macular degeneration and healthy control subjects - a study using spectral fundus reflectance. Acta Ophthalmol. 90(5): p. e399-403.
22. Raman, R., et al., Macular pigment optical density in a South Indian population. Invest Ophthalmol Vis Sci. 52(11): p. 7910-6.
23. Strauss, O., The retinal pigment epithelium in visual function. Physiol Rev, 2005. 85(3): p. 845-81.
24. Rozanowska, M., et al., Blue light-induced singlet oxygen generation by retinal lipofuscin in non-polar media. Free Radic Biol Med, 1998. 24(7-8): p. 1107-12.
25. Gaillard, E.R., et al., Photophysical studies on human retinal lipofuscin. Photochem Photobiol, 1995. 61(5): p. 448-53.
26. Boulton, M., et al., Lipofuscin is a photoinducible free radical generator. J Photochem Photobiol B, 1993. 19(3): p. 201-4.
27. Rozanowska, M., et al., Blue light-induced reactivity of retinal age pigment. In vitro generation of oxygen-reactive species. J Biol Chem, 1995. 270(32): p. 18825-30.
28. Sparrow, J.R., et al., Involvement of oxidative mechanisms in blue-light-induced damage to A2E-laden RPE. Invest Ophthalmol Vis Sci, 2002. 43(4): p. 1222-7.
29. Wood, J.P., et al., The influence of visible light exposure on cultured RGC-5 cells. Mol Vis, 2008. 14: p. 334-44.
30. Youn, H.Y., et al., Effects of 400 nm, 420 nm, and 435.8 nm radiations on cultured human retinal pigment epithelial cells. J Photochem Photobiol B, 2009. 95(1): p. 64-70.
31. Putting, B.J., et al., Blue-light-induced dysfunction of the blood-retinal barrier at the pigment epithelium in albino versus pigmented rabbits. Exp Eye Res, 1994. 58(1): p. 31-40.
32. Ahlers, C., et al., Imaging of the retinal pigment epithelium in age-related macular degeneration using polarization-sensitive optical coherence tomography. Invest Ophthalmol Vis Sci, 2010. 51(4): p. 2149-57.
33. Gehrs, K.M., et al., Age-related macular degeneration--emerging pathogenetic and therapeutic concepts. Ann Med, 2006. 38(7): p. 450-71.
Obscuridad Luz
FIG. 3 Células de epitelio pigmentario retiniano de cerdo tratadas con A2E y mantenidas en la obscuridad o expuestas a la luz. A la izquierda, las células mantenidas en la obscuridad están sanas porque presentan una forma hexagonal y están contiguas las unas a las otras (en confluencia). Por el contrario, la exposición a la luz (a la derecha) provoca la muerte de las células, visible por su forma redondeada y una densidad reducida.
Células no tratadas Células + A2E
FIG. 2 Células del epitelio pigmentario retiniano de cerdo con o sin tratamiento A2E, un constituyente de la lipofuscina. Los núcleos de las células son visibles en azul y las uniones intercelulares están coloreadas en rojo. A la izquierda, la A2E internalizada por las células es visible por autofluorescencia en el verde cuando se ilumina con la luz azul.

Points de Vue - n°68 - Spring / Primavera - 2013 49
LUZ AZUL
Científico médico
L A L U Z A Z U L Y L A C R O N O B I O L O G Í A :
L A L U Z Y L A S F U N C I O N E S
N O V I S U A L E S
CLAUDE GRONFIERPh.D, Inserm U846, Instituto de Investigación del Cerebro y Células Madre Departamento de Cronobiología, Lyon Francia
__ INTRODUCCIÓN
En los últimos diez años se han realizado muchos descubrimientos
en el área de la cronobiología. Desde la puesta en evidencia,
en 2002, de un nuevo fotorreceptor retiniano (las células ganglionares
que contienen melanopsina) implicado en la sincronización del reloj
circadiano, ahora es una evidencia que el ojo no solo sirve para ver, sino
que también participa en todo un conjunto de funciones no visuales
directamente estimuladas por la luz. Los mecanismos involucrados todavía
quedan por explorar en gran medida, pero el conjunto de las respuestas
biológicas ante un estímulo fótico dejan apercibir aplicaciones clínicas
de la luz en toda una serie de trastornos y patologías del sueño,
de la vigilia, cognitivos, de la memoria y del humor.
__ LA LUZ Y EL RELOJ BIOLÓGICO CIRCADIANO
Desde 1980 se conoce la relación entre la luz y el reloj biológico
interno en el ser humano. El reloj circadiano (del latín circa «cerca de»,
y dies «día») es un componente fisiológico esencial para la vida y ha
sido observado en prácticamente todos los organismos vivos estudiados,
desde los procariotes hasta el ser humano [4]. Dos propiedades
fundamentales caracterizan al reloj circadiano [4]:
1. En los mamíferos [7], su actividad rítmica es endógena y está ubicada
en el núcleo supraquiasmático (NSQ) del hipotálamo, su actividad
eléctrica circadiana la sustentan una decena de genes reloj cuya
actividad cíclica es responsable de un ritmo aproximado
a las 24 horas de cada una de sus neuronas [9].
2. Su actividad debe sincronizarse en 24 horas. Efectivamente, su período
endógeno es cercano pero ligeramente distinto de las 24 horas.
Por este motivo, es necesario efectuar la sincronización del reloj
(su puesta en hora) para que su actividad esté en sintonía con el día
solar. En los mamíferos, la luz es el sincronizador más potente de este
reloj y para que surta efecto esta debe pasar únicamente por el ojo.
__ FUNCIONES CONTROLADAS POR EL RELOJ CIRCADIANO
Un gran número de funciones fisiológicas tienen un ritmo circadiano.
La figura 1 ilustra el control circadiano de algunas funciones del ser
humano. El reloj actúa como un director de orquesta que permite
la expresión de las actividades fisiológicas en el momento adecuado.
La vigilia, el desempeño cognitivo, la memoria, la temperatura corporal
y la presión arterial se encuentran al máximo durante el día (vigilia).
Por el contrario, durante la noche (sueño), observamos que la secreción
de la hormona melatonina, la relajación muscular y la presión
del sueño se encuentran en sus niveles máximos.
Se han descubierto un gran número de otras actividades biológicas
circadianas, tanto periféricas como centrales. Dependiendo de los
tejidos, entre el 8 y el 20 % del genoma se expresa de manera rítmica
a través del reloj endógeno. El sistema circadiano está involucrado
en el control de la división celular, de la apoptosis en el cáncer [10]
FIG. 1 Representación esquemática de las funciones biológicas controladas por el reloj biológico circadiano (lista no exhaustiva).
Las estructuras indicadas en colores son, respectivamente, en rojo: el núcleo supraquiasmático, en naranja: la glándula pineal, en azul: el hipotálamo (que contiene el VLPO o área ventro-lateral preóptica, denominada el sleep switch), en beige: el tronco cerebral (que contiene la vía cortical activadora ascendente y el switch del sueño de onda lenta/sueño paradójico), en verde: el tálamo (responsable de la activación cortical y la sincronización del EEG) (figura modificada de Mignot et al. Nature 2002 [3] y Gronfier et al. 2012 [6]).
Humor
Desempeño cognitivo
Sist. nervioso autónomo
Actividad motora
Memoria
Hormonas
Relojes periféricos
Ciclo celular
Sueño
LUZ
RELOJ BIOLÓGICO
Hipotálamo
Tronco cerebral
Glándula
PVN
Cortex
Tálamo
LUZ AZUL
Científico médico

Points de Vue - n°68 - Spring / Primavera - 201350
LUZ AZUL
Científico médico
y en la reparación del ADN [11]. Por este motivo, estos resultados
permiten contemplar cómo la desincronización del sistema circadiano
podría ser responsable de la mayor prevalencia de algunos cánceres en
personas que trabajan en turnos rotatorios [12].
La importancia del sistema circadiano y de su sincronización es por lo
tanto crucial para la salud humana.
__ CONSECUENCIAS DE LA DESINCRONIZACIÓN CIRCADIANA
En el ser humano, la importancia de la sincronización es evidente
cuando se observan los síntomas del «jet lag» o en el trabajo nocturno
(el 20 % de la población en los países industrializados). Un fallo
en la sincronización del reloj se traduce generalmente por la alteración
de numerosas funciones fisiológicas (sueño, vigilia, desempeño cognitivo,
sistema cardiovascular, sistema inmunitario [4, 13, 14]) el deterioro de los
procesos neurocognitivos (desempeño cognitivo, memoria) y la perturbación
del sueño y la vigilia [15]. También se encuentran dichas alteraciones, de
manera crónica, en los trabajadores nocturnos, en las personas mayores, en
los ciegos, en personas con algunas patologías psiquiátricas y en personas
con algunas enfermedades neurodegenerativas centrales (enfermedades
de Alzheimer y de Parkinson [16]). Los desórdenes cronobiológicos
asociados a estos estados normales o patológicos tienen consecuencias
socioeconómicas importantes, porque pueden conducir a una disminución
del estado de salud general y a un aumento de los riesgos patológicos
asociados. La Sociedad Francesa de Medicina Laboral acaba de publicar
un informe bajo la égida de la Alta Autoridad de Salud sobre las
consecuencias del trabajo en turnos, las recomendaciones para detectarlas
y los abordajes para minimizarlas [17].
__ CARACTERÍSTICAS ENDÓGENAS DEL RELOJ CIRCADIANO
En condiciones luminosas inadaptadas a la sincronización del sistema
circadiano, el reloj endógeno funciona a un ritmo que ya no es el de la
jornada de 24 horas. Este expresa entonces su propio ritmo (período)
endógeno. Como en el caso de un reloj mecánico que no marca la
hora regularmente, el reloj circadiano se adelanta o se atrasa según los
individuos (según el período de su reloj) en ausencia de sincronización
por el entorno. Se observa este fenómeno, denominado libre curso en
los ciegos, a quienes la ausencia de luz no permite que sus relojes,
biológicos se sincronicen en las 24 horas [18], lo cual permite explicar que
aproximadamente el 75 % de los ciegos se quejan de no tener un sueño
de buena calidad y consultan por trastornos recurrentes del sueño [19].
Cabe destacar que el período del reloj es una característica individual muy
precisa. Esta no varía en el adulto en el transcurso del envejecimiento [20],
pero sí presenta una cierta plasticidad durante la infancia y la adolescencia
(una prolongación del período en la adolescencia podría explicar en parte la
tendencia a irse a dormir tarde por la noche e incluso el trastorno
de retraso de fase observado en el tramo de edad de 15 a 25 años [21]).
Gracias a la utilización de protocolos experimentales muy
controlados [20], se ha podido poner en evidencia que el período
del reloj en el ser humano es muy cercano a las 24 horas (una media
de 24,4 [20]). Uno de los impactos directos del período endógeno
en la vida diaria es el cronotipo. Los individuos que tienen un período
corto (un reloj rápido) son generalmente personas que se duermen
temprano por la noche (cronotipos matutinos) mientras que las personas
que se van a dormir tarde (cronotipos vespertinos) tienen un período
largo (un reloj más lento) [22].
__ SINCRONIZACIÓN DEL RELOJ
Puesto que el período endógeno es cercano a las 24 horas pero
no exactamente de 24 horas, el reloj circadiano debe sincronizarse
constantemente en 24 horas. En los mamíferos, la luz es el
sincronizador más potente del reloj interno.
El término sincronización del reloj biológico corresponde, al igual
que en un reloj, a una puesta en hora, adelantándolo o retrasándolo,
para ponerlo en sincronía con el entorno. En un individuo que suele
dormirse tarde y cuyo periodo endógeno es de 24 h y 30 min, es
necesario adelantar su reloj de 30 minutos diariamente para que
esté sincronizado en 24 horas, de otra manera, podría ir acumulando
diariamente 30 minutos de retraso. Por el contrario, en un individuo que
suele dormirse temprano y cuyo período sería de 23 h y 30 min, el reloj
circadiano debe retrasarse como media 30 minutos diarios.
Existen otros sincronizadores en los animales, pero son menos
eficaces en el ser humano. Se denominan sincronizadores «no fóticos»
pues no involucran a la luz. La ingesta alimentaria y el ejercicio
físico tienen un efecto sincronizador en el reloj humano pero es poco
significativo. Estudios realizados en los años 1950, han dejado pensar
que los sincronizadores sociales eran más potentes que la luz en el ser
humano23. Se sabe actualmente que esto es falso. La mejor prueba
de que los sincronizadores no fóticos tienen un efecto muy limitado,
en caso de que exista, proviene de la observación de que la gran mayoría
de los ciegos, al no tener ninguna percepción luminosa, están en estado
de libre curso, no sincronizados, a pesar de una vida social y una
actividad estructuradas en torno a las 24 horas (trabajo, irse a dormir/
despertar, hora de los alimentos, actividades físicas e intelectuales, etc.)
El sincronizador no fótico cuyo efecto en el reloj circadiano humano
es indiscutible es la melatonina [24]. Esta debe constituir el abordaje
de primera intención en el tratamiento del libre curso en los ciegos.
LUZ Estructura visual
Melanopsina ipRGCs Melanopsina
Reloj circadianoFIG. 2 Esquema del ojo (corte transversal) con una representación ampliada de la retina
(en el centro).
La retina percibe la luz del entorno. Los conos y bastones proyectan hacia las estructuras visuales (visión perceptiva). Las células ganglionares de melanopsina están implicadas en la regulación de los ritmos biológicos a través de su proyección hacia el núcleo supraquiasmático. (imagen modificada de webvision y Gronfier et al. [1]).
Conos, Bastones

Points de Vue - n°68 - Spring / Primavera - 2013 51
LUZ AZUL
Científico médico
investigaciones cuyo objetivo consiste en poder desarrollar métodos
de tratamiento de algunos trastornos cronobiológicos (entre los
que figuran los trastornos de los ritmos circadianos del sueño y los
trastornos afectivos estacionales), más eficaces y más rápidos que los
métodos actuales que utilizan las luces blancas fluorescentes [29].
La respuesta del sistema circadiano a la luz depende de las características fóticas. El efecto de la luz en el reloj depende de la intensidad luminosa y
de su duración. Cuanto más intenso sea el estímulo luminoso [30],
y/o cuanto más larga es su duración [31], mayor será el efecto.
Por ejemplo, una exposición luminosa nocturna de una duración
de 6,5 horas conduce a un retraso del ritmo de la melatonina de más
de 2 h con una luz blanca intensa (10.000 lux) [32]. Si se da un estímulo
a la misma hora con la misma duración de exposición a unos 100 lux,
es decir un 10 % de la intensidad máxima probada, se produce un
retraso de aproximadamente 1 hora, es decir, el 50 % del efecto máximo
observado [32]. Los estudios recientes muestran que el reloj circadiano
es en realidad particularmente sensible a las bajas intensidades luminosas,
y que la exposición a una pantalla de ordenador con LED
(entre 40 y 100 lux) durante 2 horas inhibe parcialmente la secreción
de melatonina, activa la vigilancia, retrasa el reloj biológico y retrasa
el momento de conciliar el sueño [33].
El efecto de la luz depende de su espectro. Como lo ilustra la figura 3,
el sistema circadiano tiene su máxima sensibilidad a una luz de color
comprendida entre los 460-480 nm [34]. Una luz monocromática azul
(longitud de onda de 480 nm) puede ser tan eficaz en el sistema
circadiano como una luz fluorescente blanca 100 veces más intensa (con
100 veces más fotones). Esta propiedad reside en la sensibilidad de las
células ganglionares de melanopsina.
__ FOTORRECEPCIÓN CIRCADIANA
Hasta hace poco tiempo, se admitía que los conos y bastones de
la retina externa eran los únicos fotorreceptores responsables de la
transducción de la información luminosa hacia el reloj endógeno. Los
estudios realizados desde el 2000 en el ser humano y en animales
muestran que hay dos sistemas retinianos implicados en la fotorrecepción
circadiana (fig. 2):
1. Los fotorreceptores implicados en la visión consciente (conos y bastones);
2. Las células glanglionares de melanopsina, intrínsecamente fotosensibles
(intrinsically photosensitive retinal ganglion cells: ipRGC) implicadas en un
gran número de funciones no visuales [25].
En ausencia de estos 2 sistemas, el sistema circadiano de los roedores es
«ciego» y funciona en libre curso expresando su ritmicidad endógena [26].
Se considera actualmente que la información luminosa responsable de
la sincronización del reloj biológico pasa por las células ganglionares
de melanopsina, ya sea estimulando directamente estas células, ya sea
estimulándolas directamente mediante los conos y los bastones. Por esta
razón, se considera actualmente que el ojo no solo sirve para ver sino que
además de tener una función visual también posee funciones, no visuales
(fig. 2 et 4).
Ambos tipos de fotorreceptores de la retina externa e interna son
filogenética y funcionalmente diferentes. A diferencia de los conos
y de los bastones, las células ganglionares de melanopsina necesitan
altos niveles de irradiancias y presentan un pico de sensibilidad
hacia los 480 nm (en todos los mamíferos estudiados). Además,
estas células de tipo rabdomérico presentan la propiedad
de bioestabilidad, que las hace virtualmente insensibles al bleaching [29].
Actualmente, estos fotorreceptores están sujetos a numerosas
FIG. 4 Las células ganglionares de melanopsina de la retina proyectan hacia un conjunto de estructuras implicadas en la regulación del sistema circadiano (NSQ), del reflejo pupilar (OPN), de la actividad motora (vSPW, IGL), del sueño (VPLO) y de la vigilia (LC). Estas vías de proyección constituyen las vías no visuales de la luz (no visual o «non-image forming» en inglés). Figura modificada [5,8].
480 nm1,0
0,8
0,6
0,4
0,2
0,0
Sens
ibili
dad
rela
tiva
400 450 500 550 600 650 700
Longitud de onda (nm)
FIG. 3 Sensibilidad espectral de los fotorreceptores clásicos (conos SW, MW, LW y bastones: rods) y de la melanopsina (mel) en los hombres (Najjar et al. [2]).
La sensibilidad del sistema circadiano en el hombre (estimada por la supresión de la melatonina - puntos negros) es óptima a ~ 480 nm, correspondiente al pico de sensibilidad de la melanopsina. Los conos y los bastones están implicados en la fotorrecepción circadiana pero no se conoce su contribución relativa.
SerotoninaRafe
DopaminaATV
Sistema de recompensaLH
Reloj circadianoNSQ
Humoramígdalacerebral
Estructuras visualesNGL, CS
Reflejo pupilarOPN
Actividad motrizZona subparaventricular
Interruptor del sueñoVLPO
CogniciónMemoriahipotálamo
SW
melatonina
bastones
MW
LW
supresión de melatonina

Points de Vue - n°68 - Spring / Primavera - 201352
LUZ AZUL
Científico médico
Finalmente, el efecto de la luz depende de la hora a la cual esta
se percibe. La curva de respuesta de fase muestra que la luz a la que
estamos expuestos por la tarde y al inicio de la noche (en media entre las
17 h y las 5 h de la mañana) tiene como efecto retrasar el reloj mientras
que la luz recibida hacia finales de la noche y en la mañana (en media
entre las 5 h de la mañana y las 17 h) tiene el efecto inverso de adelantar
el reloj [54]. Esta sensibilidad temporal específica explica la sincronización
diaria del reloj en condiciones normales y su no sincronización en el jet lag
y el trabajo nocturno.
__ LA LUZ Y LAS FUNCIONES NO VISUALES
Desde el descubrimiento, hace diez años, de las células ganglionares
de melanopsina en la retina, se han descrito una serie de funciones
no visuales, sensibles a la luz. Estas funciones implican vías anatómicas
y estructuras cerebrales diferentes de las implicadas en la visión
y no conducen a la formación de imágenes (fig. 4). Estudios en animales [35]
muestran proyecciones de las células ganglionares de melanopsina
hacia estructuras implicadas en la regulación de los ritmos biológicos, la
regulación de los estados de vigilia y sueño, la regulación de la actividad
locomotora, el reflejo pupilar, etc. En el ser humano, los estudios muestran
que las células ganglionares de melanopsina, a través de las vías no
visuales, están implicadas en el efecto que tiene la luz en el desfase de
la melatonina [36], el aumento de la vigilancia, de la temperatura y de la
frecuencia cardíaca [37], la expresión del gen PER2 [38], el desfase del ritmo
del gen PER3 [39], el aumento de la eficacia psicomotora y de la actividad
EEG [40], la estructura del sueño [41], y la activación de estructuras cerebrales
implicadas en la memoria y la regulación del humor [42-51]. La luz, a través
de las proyecciones retinianas no visuales va a estimular directamente las
estructuras cerebrales implicadas en el control de la vigilancia, el sueño,
el humor y el desempeño cognitivo y psicomotor.
Mientras que la separación de estas dos vías anatómicas (visual y no visual)
no se había identificado claramente, desde 1995 se sabe que algunos
ciegos sin ninguna percepción visual consciente pueden tener un sistema
circadiano sensible a la luz [52]. El sistema visual de estos pacientes es ciego,
pero sus funciones no visuales (entre las que están su reloj circadiano) no
son ciegas, y reciben una información fótica. Estos casos son probablemente
raros (se han estudiado muy pocos individuos en el mundo) y la mayoría de
los pacientes con patologías oculares que conducen a una privación parcial
o total de la información fótica presentan una prevalencia acentuada de
trastornos del sueño y de los ritmos biológicos (con mayor frecuencia sus
ritmos circadianos se expresan en «libre-curso» y esta condición clínica está
asociada a trastornos del sueño en más del 75 % de los casos [53,19].
No obstante, los oftalmólogos deben ser conscientes de la función no visual
del ojo y de su importancia en la sincronización del sistema circadiano.
Habida cuenta del riesgo de añadir un sistema circadiano ciego (y los
síntomas del libre curso con sus tratamientos asociados) a una visión
deficiente, la función no visual debería ser evaluada antes de la enucleación
de un paciente.
__ CONCLUSIONES
Habida cuenta de la importancia de la sincronización del sistema
circadiano y de la naturaleza de las funciones no visuales, la luz
parece ser una necesidad biológica indispensable al buen funcionamiento
del organismo. Además, es probable que la luz se utilice en el futuro
en el tratamiento de un gran número de condiciones
normales o patológicas en las que una disfunción fisiológica podrá
corregirse mediante la activación de funciones no visuales del ojo. •
REFERENCIAS
1. Gronfier, C. Consequences and physiological effects of light: Sleep and biological clock in night and shift work. Arch. Mal. Prof. Environ. 70, 253-261 (2009).
2. Najjar, R., et al. Aging of non-visual spectral sensitivity to light: compensatory mechanisms? Under Review
3. Mignot, E., Taheri, S. & Nishino, S. Sleeping with the hypothalamus: Emerging therapeutic targets for sleep disorders. Nat. Neurosci 5 Suppl, 1071 (2002).
4. Dunlap, J.C., Loros, J.J. & DeCoursey, P.J. Chronobiology: Biological Timekeeping, (Sinauer, 2004).
5. Do, M.T. & Yau, K.W. Intrinsically photosensitive retinal ganglion cells. Physiol Rev 90, 1547-1581 (2010).
6. Taillard, J. & Gronfier, C. Circadian and homeostatic control of sleep (Regulation homeostasique et circadienne du sommeil). in Sleep Disorders (Les troubles du Sommeil), Da (eds), Elsevier, 2012. (ed. Elsevier) 25-43 (2012).
7. Moore, R.Y. & Eichler, V.B. Loss of a circadian adrenal corticosterone rhythm following suprachiasmatic lesions in the rat. Brain Research 42, 201-206 (1972).
8. Hattar, S., et al. Central projections of melanopsin-expressing retinal ganglion cells in the mouse. J Comp Neurol 497, 326-349 (2006).
9. Reppert, S.M. & Weaver, D.R. Coordination of circadian timing in mammals. Nature 418, 935-941 (2002).
10. Granda, T.G., et al. Circadian regulation of cell cycle and apoptosis proteins in mouse bone marrow and tumor. Faseb J 19, 304-306 (2005).
11. Collis, S.J. & Boulton, S.J. Emerging links between the biological clock and the DNA damage response. Chromosoma 116, 331-339 (2007).
12. (2010), I. Painting, firefighting, and shiftwork. IARC Monogr Eval Carcinog Risks Hum 98, 9-764 (2010).
13. Brandenberger, G., Gronfier, C., Chapotot, F., Simon, C. & Piquard, F. Effect of sleep deprivation on overall 24 h growth-hormone secretion. The Lancet 356, 1408-1408 (2000).
14. Spiegel, K., Leproult, R. & Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 354, 1435-1439 (1999).
15. Wright Jr, K.P., Hull, J.T. & Czeisler, C.A. Relationship between alertness, performance, and body temperature in humans. Am J Physiol Regul Integr Comp Physiol 289, R1370 (2002).
16. Vezoli, J., et al. Early presymptomatic and long-term changes of rest activity cycles and cognitive behavior in a MPTP-monkey model of Parkinson’s disease. PLoS ONE 6, e23952 (2011).
17. Travail, S.F.d.M.d. Surveillance médico-professionnelle des travailleurs postés et/ou de nuit. Recommandation de Bonne Pratique (Label HAS). (2012).
18. Miles, L.E., Raynal, D.M. & Wilson, M.A. Blind man living in normal society has circadian rhythms of 24.9 hours. Science 198, 421-423. (1977).
19. Leger, D., Guilleminault, C., Defrance, R., Domont, A. & Paillard, M. Blindness and sleep patterns. Lancet 348, 830 (1996).
20. Czeisler, C.A., et al. Stability, precision, and near-24-hour period of the human circadian pacemaker. Science 284, 2177-2181 (1999).
21. Roenneberg, T., et al. A marker for the end of adolescence. Curr Biol 14, R1038-1039 (2004).
22. Duffy, J.F., Rimmer, D.W. & Czeisler, C.A. Association of intrinsic circadian period with morningness-eveningness, usual wake time, and circadian phase. Behav Neurosci 115, 895 (2001).
23. Aschoff, J. Human circadian rhythms in activity, body temperature and other functions. Life Science Space Research 5, 159 (1967).
24. Arendt, J. & Rajaratnam, S.M. Melatonin and its agonists: an update. Br J Psychiatry 193, 267-269 (2008).
25. Berson, D.M., Dunn, F.A. & Takao, M. Phototransduction by retinal ganglion cells that set the circadian clock. Science 295, 1070-1073 (2002).
26. Hattar, S., et al. Melanopsin and rod-cone photoreceptive systems account for all major accessory visual functions in mice. Nature 424, 75-81 (2003).
27. Dacey, D.M., et al. Melanopsin-expressing ganglion cells in primate retina signal colour and irradiance and project to the LGN. Nature 433, 749-754 (2005).
28. Dkhissi-Benyahya, O., Gronfier, C., De Vanssay, W., Flamant, F. & Cooper, H.M. Modeling the role of
mid-wavelength cones in circadian responses to light. Neuron 53, 677-687 (2007).
29. Mure, L.S., et al. Melanopsin bistability: a fly’s eye technology in the human retina. PLoS One 4, e5991 (2009).
30. Zeitzer, J.M., Dijk, D.J., Kronauer, R., Brown, E. & Czeisler, C. Sensitivity of the human circadian pacemaker to nocturnal light: melatonin phase resetting and suppression. J Physiol 526, 695-702. (2000).
31. Chang, A.M., et al. Human responses to bright light of different durations. J Physiol 590, 3103-3112 (2012).
32. Zeitzer, J.M., Dijk, D.J., Kronauer, R.E., Brown, E.N. & Czeisler, C.A. Sensitivity of the human circadian pacemaker to nocturnal light: Melatonin phase resetting and suppression. J Physiol 526, 695-702 (2000).
33. Chellappa, S.L., et al. Non-visual effects of light on melatonin, alertness and cognitive performance: can blue-enriched light keep us alert? PLoS ONE 6, e16429 (2011).
34. Brainard, G.C., et al. Action spectrum for melatonin regulation in humans: Evidence for a novel circadian photoreceptor. J Neurosci 21(16), 6405 (2001).
35. Gooley, J.J., Lu, J., Fischer, D. & Saper, C.B. A broad role for melanopsin in nonvisual photoreception. Journal of the Neurological Sciences 23, 7093-7106 (2003).
36. Lockley, S.W., Brainard, G.C. & Czeisler, C.A. High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength light. J Clin Endocrinol Metab 88, 4502-4505 (2003).
37. Cajochen, C., et al. High sensitivity of human melatonin, alertness, thermoregulation, and heart rate to short wavelength light. J Clin Endocrinol Metab 90, 1311-1316 (2005).
38. Cajochen, C., et al. Evening exposure to blue light stimulates the expression of the clock gene PER2 in humans. Eur J Neurosci 23, 1082-1086 (2006).
39. Ackermann, K., Sletten, T.L., Revell, V.L., Archer, S.N. & Skene, D.J. Blue-light phase shifts PER3 gene expression in human leukocytes. Chronobiol Int 26, 769-779 (2009).
40. Lockley, S.W., et al. Short-wavelength sensitivity for the direct effects of light on alertness, vigilance, and the waking electroencephalogram in humans. Sleep 29, 161-168 (2006).
41. Munch, M., et al. Wavelength-dependent effects of evening light exposure on sleep architecture and sleep EEG power density in men. Am J Physiol Regul Integr Comp Physiol 290, R1421-1428 (2006).
42. Carrier, J., et al. Sleep slow wave changes during the middle years of life. Eur J Neurosci (2011).
43. Vandewalle, G., et al. Spectral quality of light modulates emotional brain responses in humans. Proc Natl Acad Sci U S A 107, 19549-19554 (2010).
44. Vandewalle, G., Maquet, P. & Dijk, D.J. Light as a modulator of cognitive brain function. Trends Cogn Sci 13, 429-438 (2009).
45. Vandewalle, G., et al. Functional magnetic resonance imaging-assessed brain responses during an executive task depend on interaction of sleep homeostasis, circadian phase, and PER3 genotype. J Neurosci 29, 7948-7956 (2009).
46. Schmidt, C., et al. Homeostatic sleep pressure and responses to sustained attention in the suprachiasmatic area. Science 324, 516-519 (2009).
47. Vandewalle, G., et al. Brain responses to violet, blue, and green monochromatic light exposures in humans: prominent role of blue light and the brainstem. PLoS ONE 2, e1247 (2007).
48. Vandewalle, G., et al. Robust circadian rhythm in heart rate and its variability: influence of exogenous melatonin and photoperiod. J Sleep Res 16, 148-155 (2007).
49. Vandewalle, G., et al. Wavelength-dependent modulation of brain responses to a working memory task by daytime light exposure. Cereb Cortex 17, 2788-2795 (2007).
50. Vandewalle, G., et al. Daytime light exposure dynamically enhances brain responses. Curr Biol 16, 1616-1621 (2006).
51. Perrin, F., et al. Nonvisual responses to light exposure in the human brain during the circadian night. Curr Biol 14, 1842-1846 (2004).
52. Czeisler, C.A., et al. Suppression of melatonin secretion in some blind patients by exposure to bright light. New Eng J Med 332, 6 (1995).
53. Sack, R.L., Lewy, A.J., Blood, M.L., Keith, L.D. & Nakagawa, H. Circadian rhythm abnormalities in totally blind people: Incidence and clinical significance. J. Clin. Endocrinol. Metab. 75, 127 (1992).

Points de Vue - n°68 - Spring / Primavera - 2013 53
LUZ AZUL
Científico no médico
L O S L E D ( L I G H T E M I T T I N G D I O D E S )
Y E L R I E S G O
D E L A L U Z A Z U L
LUZ AZUL
Científico no médico
__ ESTE ARTÍCULO PRESENTA UN PANORAMA GENERAL de los
conocimientos sobre la toxicidad potencial para la retina de la luz que
emiten los LED. Durante varios años, se ha considerado y estudiado
el denominado «riesgo por luz azul» debido a su alto nivel de brillantez
y su espectro de emisión que contiene una fracción significativa de luz
azul. Varios estudios independientes realizados por agencias sanitarias
han demostrado que el riesgo que plantean los LED utilizados como
fuentes de iluminación general es bajo. No obstante, no puede
dejarse de lado el caso de algunos grupos de personas sensibles, si se
considera el desempeño óptico cada vez mayor de los LED, así como
su rápida difusión en el mercado de consumo en general.
Las fuentes tradicionales de iluminación, como la muy conocida
lámpara incandescente y la lámpara fluorescente compacta, están
siendo rápidamente sustituidas por productos a base de diodos emisores
de luz (LED) (fig. 1). La SSL (solid-state lighting) presenta muchas
ventajas, como son un tiempo de vida más largo, un menor consumo
de energía y un menor impacto medioambiental. Por lo tanto, muchos
gobiernos han comenzado a prohibir paulatinamente las tecnologías
de iluminación más antiguas, preparando el terreno para una utilización
masiva de los LED en el mercado general de iluminación. De hecho,
los líderes de la industria de la iluminación consideran que, en el
2020, más del 90 % de todas las fuentes de luz en el mundo utilizarán
productos basados en las tecnologías SSL y LED.
Como cualquier tecnología nueva o emergente, los productos SSL
deberían proporcionar la prueba de que, por lo menos, son tan
seguros como los productos que intentan sustituir. Además, algunas
propiedades únicas de los LED, como su compacidad, han generado
muchas nuevas aplicaciones de iluminación para las cuales las
tecnologías más antiguas ya no se pueden utilizar. Por ejemplo,
algunos tipos de juguetes y ropa actualmente incorporan LED. La
seguridad de los productos que utilizan LED debería ser evaluada
considerando las interacciones con el cuerpo humano, tanto en las
nuevas maneras de utilización como en las ya existentes.
Los efectos adversos potenciales de la radiación óptica en la piel
y en los ojos se conocen como riesgos fotobiológicos. Los LED
actualmente utilizados en aplicaciones de iluminación tienen la ventaja
de emitir una cantidad insignificante de radiaciones ultravioleta (UV)
e infrarrojas (IR) 1. Los únicos riesgos fotobiológicos que hay que
considerar al evaluar la seguridad de los LED están asociados
con la luz visible y, más especialmente, la parte azul del espectro.
Un cierto número de agencias sanitarias como ANSES 2 y SCENIHR 3
han analizado y hecho un repaso de las publicaciones científicas sobre
los riesgos fotobiológicos asociados al uso de los LED.
Dos características principales de los LED han atraído la atención
de los expertos:
• Los LED son fuentes pequeñas pero muy brillantes de luz visible
CHRISTOPHE MARTINSONSResponsable de la división Iluminación y Electromagnetismo, Dirección Salud y ConfortCentro Científico y Técnico de la Construcción - CSTB Grenoble, Francia
1 Con sus emisiones insignificantes de UV e IR, los LED no deberían contribuir a la aparición de queratitis y cataratas.2 Agencia Nacional de Seguridad Sanitaria de la Alimentación, del Medio Ambiente y del Trabajo (Agence nationale de sécurité sanitaire de l’alimentation, de l’environnement et du travail).3 Comité Científico sobre Riesgos Sanitarios Emergentes y Recién Identificados (Scientific Committee on Emerging and Newly Identified Health Risks).
FIG. 1 Fotografías de varios tipos de productos de iluminación sólida.
a: Luminaria direccional (spot light) con LED.
b: Una lámpara SSL con tres LED y utilizada para sustituir a la lámpara incandescente.
c: Una luminaria de exteriores de alta potencia SSL con módulos LED 121.
d: Un componente LED típico, utilizado en muchos productos SSL. Este tipo de LED consume aproximadamente 1 W de electricidad y genera un flujo luminoso de aproximdamente 100 lm. Su luminancia puede ser tan elevada como 107 cd/m².
c d
ba
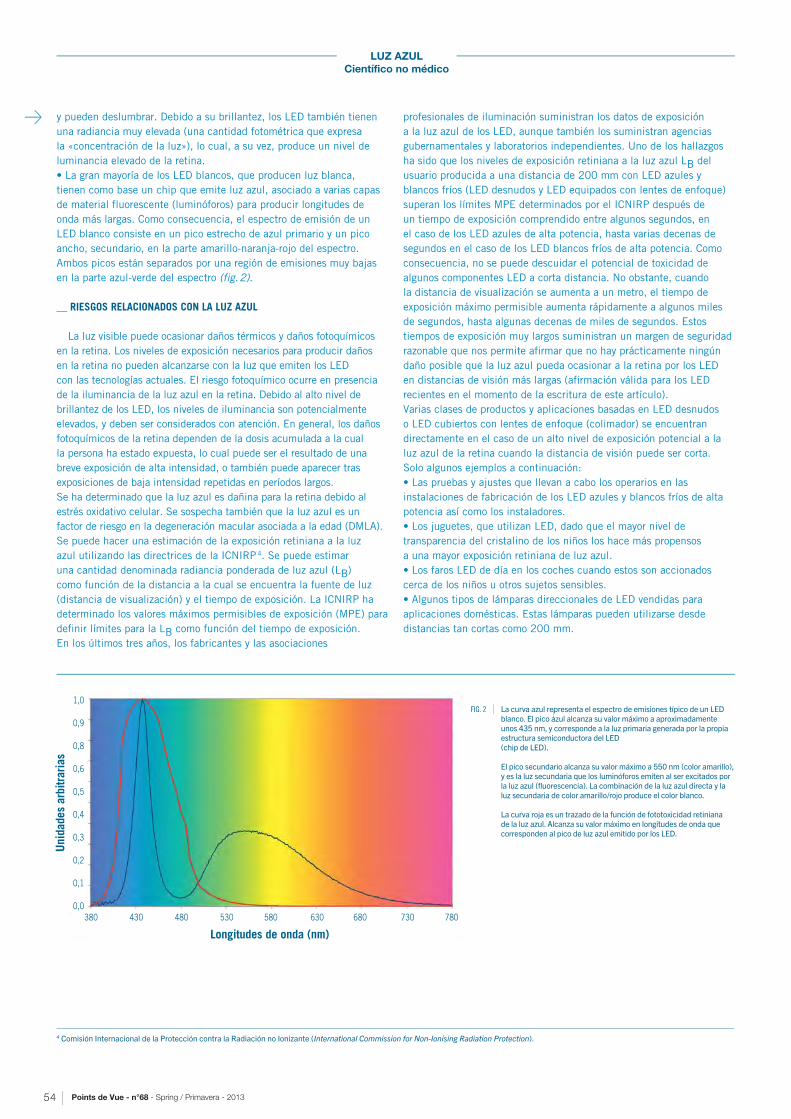
Points de Vue - n°68 - Spring / Primavera - 201354
LUZ AZUL
Científico no médico
4 Comisión Internacional de la Protección contra la Radiación no Ionizante (International Commission for Non-Ionising Radiation Protection).
y pueden deslumbrar. Debido a su brillantez, los LED también tienen
una radiancia muy elevada (una cantidad fotométrica que expresa
la «concentración de la luz»), lo cual, a su vez, produce un nivel de
luminancia elevado de la retina.
• La gran mayoría de los LED blancos, que producen luz blanca,
tienen como base un chip que emite luz azul, asociado a varias capas
de material fluorescente (luminóforos) para producir longitudes de
onda más largas. Como consecuencia, el espectro de emisión de un
LED blanco consiste en un pico estrecho de azul primario y un pico
ancho, secundario, en la parte amarillo-naranja-rojo del espectro.
Ambos picos están separados por una región de emisiones muy bajas
en la parte azul-verde del espectro (fig. 2).
__ RIESGOS RELACIONADOS CON LA LUZ AZUL
La luz visible puede ocasionar daños térmicos y daños fotoquímicos
en la retina. Los niveles de exposición necesarios para producir daños
en la retina no pueden alcanzarse con la luz que emiten los LED
con las tecnologías actuales. El riesgo fotoquímico ocurre en presencia
de la iluminancia de la luz azul en la retina. Debido al alto nivel de
brillantez de los LED, los niveles de iluminancia son potencialmente
elevados, y deben ser considerados con atención. En general, los daños
fotoquímicos de la retina dependen de la dosis acumulada a la cual
la persona ha estado expuesta, lo cual puede ser el resultado de una
breve exposición de alta intensidad, o también puede aparecer tras
exposiciones de baja intensidad repetidas en períodos largos.
Se ha determinado que la luz azul es dañina para la retina debido al
estrés oxidativo celular. Se sospecha también que la luz azul es un
factor de riesgo en la degeneración macular asociada a la edad (DMLA).
Se puede hacer una estimación de la exposición retiniana a la luz
azul utilizando las directrices de la ICNIRP 4. Se puede estimar
una cantidad denominada radiancia ponderada de luz azul (LB)
como función de la distancia a la cual se encuentra la fuente de luz
(distancia de visualización) y el tiempo de exposición. La ICNIRP ha
determinado los valores máximos permisibles de exposición (MPE) para
definir límites para la LB como función del tiempo de exposición.
En los últimos tres años, los fabricantes y las asociaciones
profesionales de iluminación suministran los datos de exposición
a la luz azul de los LED, aunque también los suministran agencias
gubernamentales y laboratorios independientes. Uno de los hallazgos
ha sido que los niveles de exposición retiniana a la luz azul LB del
usuario producida a una distancia de 200 mm con LED azules y
blancos fríos (LED desnudos y LED equipados con lentes de enfoque)
superan los límites MPE determinados por el ICNIRP después de
un tiempo de exposición comprendido entre algunos segundos, en
el caso de los LED azules de alta potencia, hasta varias decenas de
segundos en el caso de los LED blancos fríos de alta potencia. Como
consecuencia, no se puede descuidar el potencial de toxicidad de
algunos componentes LED a corta distancia. No obstante, cuando
la distancia de visualización se aumenta a un metro, el tiempo de
exposición máximo permisible aumenta rápidamente a algunos miles
de segundos, hasta algunas decenas de miles de segundos. Estos
tiempos de exposición muy largos suministran un margen de seguridad
razonable que nos permite afirmar que no hay prácticamente ningún
daño posible que la luz azul pueda ocasionar a la retina por los LED
en distancias de visión más largas (afirmación válida para los LED
recientes en el momento de la escritura de este artículo).
Varias clases de productos y aplicaciones basadas en LED desnudos
o LED cubiertos con lentes de enfoque (colimador) se encuentran
directamente en el caso de un alto nivel de exposición potencial a la
luz azul de la retina cuando la distancia de visión puede ser corta.
Solo algunos ejemplos a continuación:
• Las pruebas y ajustes que llevan a cabo los operarios en las
instalaciones de fabricación de los LED azules y blancos fríos de alta
potencia así como los instaladores.
• Los juguetes, que utilizan LED, dado que el mayor nivel de
transparencia del cristalino de los niños los hace más propensos
a una mayor exposición retiniana de luz azul.
• Los faros LED de día en los coches cuando estos son accionados
cerca de los niños u otros sujetos sensibles.
• Algunos tipos de lámparas direccionales de LED vendidas para
aplicaciones domésticas. Estas lámparas pueden utilizarse desde
distancias tan cortas como 200 mm.
380 430 480 530 580 630 680 730 780
Longitudes de onda (nm)
1,0
0,9
0,8
0,6
0,5
0,4
0,3
0,2
0,1
0,0
Uni
dade
s ar
bitra
rias
FIG. 2 La curva azul representa el espectro de emisiones típico de un LED blanco. El pico azul alcanza su valor máximo a aproximadamente unos 435 nm, y corresponde a la luz primaria generada por la propia estructura semiconductora del LED (chip de LED).
El pico secundario alcanza su valor máximo a 550 nm (color amarillo), y es la luz secundaria que los luminóforos emiten al ser excitados por la luz azul (fluorescencia). La combinación de la luz azul directa y la luz secundaria de color amarillo/rojo produce el color blanco.
La curva roja es un trazado de la función de fototoxicidad retiniana de la luz azul. Alcanza su valor máximo en longitudes de onda que corresponden al pico de luz azul emitido por los LED.

Points de Vue - n°68 - Spring / Primavera - 2013 55
LUZ AZUL
Científico no médico
Las conclusiones que se aplican a los componentes aislados de los LED
o los módulos de LED no se pueden aplicar a todas las aplicaciones
SSL, porque la seguridad fotobiológica de un producto final SSL debe
ser evaluada independientemente de sus componentes LED. De hecho,
el valor LB de un producto SSL es generalmente muy distinto del valor
LB de los componentes LED que utiliza. Por ejemplo, se puede obtener
un LB superior con una lámpara que utiliza todo un conjunto de LED
con un LB bajo. Por el contrario, se puede obtener un LB inferior
con una lámpara a la que se le coloca un difusor delante de un LED
con un LB elevado.
En el caso de todos los LED y los productos que utilizan LED, se debe
llevar a cabo una evaluación de riesgos para determinar si se están
superando o no los límites (MPE) en las condiciones de utilización.
Esta evaluación de riesgos se puede llevar a cabo en laboratorios
de pruebas especializados en la fotometría de fuentes de luz como
el CSTB 5 y el LNE 6 en Francia.
La herramienta principal utilizada para llevar a cabo evaluaciones
de riesgos fotobiológicos es la publicación CIE 7 S009 cuyo contenido
fue plasmado en una norma internacional (IEC 62471) así como otras
normas nacionales (IESNA RP27, JIS C8159, etc.).
__ LA NORMA SOBRE SEGURIDAD FOTOBIOLÓGICA IEC 62471
Esta norma, que trata de la seguridad fotobiológica de lámparas
y aparatos que utilizan lámparas, suministra un sistema de clasificación
de las fuentes de luz en diferentes grupos de riesgo. La norma incluye
todos los riesgos fotobiológicos que puedan afectar la piel y los ojos
(riesgos térmicos y fotoquímicos) de las longitudes de onda ultravioletas
hasta las infrarrojas. Se definen cuatro grupos de riesgos: Grupo de Riesgo 0
(RG 0, sin riesgo), Grupo de Riesgo 1 (RG 1, bajo riesgo), Grupo de Riesgo
2 (RG2, riesgo moderado), Grupo de Riesgo 3 (RG3, riesgo elevado).
El nivel de riesgo del grupo depende del tiempo máximo permisible
de exposición (MPE) evaluado a una distancia de visualización dada.
__ METODOLOGÍA DE EVALUACIÓN DE LOS RIESGOS
La IEC 62471 define dos criterios diferentes para determinar
la distancia de visualización. Las fuentes de luz utilizadas en
la iluminación en general deberían ser evaluadas a la distancia
correspondiente a una iluminancia de 500 lx. Otros tipos de fuentes
de luz deberían evaluarse a una distancia fija de 200 mm.
Para los componentes LED no existe ninguna ambigüedad
en la distancia, ya que los componentes LED no se utilizan per se
en la iluminación general. En este caso, la IEC 62471 requiere que
se utilice una distancia de 200 mm. La aplicación de la técnica de
medición de la IEC 62471 a 200 mm conduce a la clasificación RG2
(riesgo moderado) para algunos LED azules de alta potencia y los LED
blancos fríos.
Sin embargo, la elección de la distancia de visualización según
la IEC 62471 es a veces ambigua y no es realista en el contexto
de las condiciones reales de utilización. Por ejemplo, mencionemos
la iluminación de escenarios (teatros y salas de concierto) donde los
artistas están expuestos a más de 500 lx de nivel de iluminancia.
El aplicar el criterio de los 500 lx podría subestimar la exposición,
mientras que el criterio de 200 mm lo sobreestimaría ampliamente.
En una situación más habitual, las lámparas domésticas direccionales
caen en el criterio de los 500 lx, lo cual corresponde a una distancia
de visualización típica de algunos metros. No obstante, es más común
tener distancias más cortas en una utilización doméstica, de 200
a 500 mm. Otro ejemplo es el alumbrado de la calle en el que el nivel
de iluminancia es muy inferior a los 500 lx, típicamente algunas decenas
de lx. El evaluar la exposición a la luz azul que emite una luminaria
de la calle a la distancia que da una iluminancia de 500 lx, es claramente
inadecuado. En una revisión futura de la IEC 62471 se debería incorporar
una definición más precisa de la distancia con arreglo a la cual se
determina el grupo de riesgo.
Es interesante observar que la estricta aplicación de la CIE S009
y la IEC 62471 en las lámparas LED de interior y las luminarias conducen
a clasificaciones RG0 y RG1, al igual que las fuentes de luz interior
tradicionales (lámparas fluorescentes, incandescentes y halógenas).
No obstante, cuando se elige la distancia de visualización de 200 mm,
varias campañas de medición revelan que un número pequeño de lámparas
LED de interior y luminarias pertenecían a RG2, mientras que las fuentes
de luz interiores tradicionales (fluorescente e incandescente) estaban
todavía en RG0 o RG1. Este resultado muestra que la tecnología LED
potencialmente aumenta el riesgo de luz azul en aplicaciones domésticas
mientras que la distancia de visualización no es limitada y las fuentes
de luz son accesibles a los niños y a otras personas sensibles.
En el momento de la publicación, el público en general sigue estando
inconsciente de los riesgos potenciales a los ojos puesto que no se aplica
ningún sistema de etiquetado obligatorio en los productos SSL para los
consumidores.
La noción de distancia de seguridad sería más adecuada para comunicar
a los instaladores y a los usuarios, especialmente al público en general.
La distancia de seguridad de un producto SSL sería la distancia mínima
en la que el grupo de riesgo por luz azul no supera el RG1. Las campañas
de medición llevadas a cabo por algunos laboratorios han mostrado
que la gran mayoría de las lámparas LED interiores y las luminarias
tienen una distancia de seguridad de 200 mm, lo cual es compatible con
la mayoría de las aplicaciones de iluminación.
Es importante observar que otras fuentes de iluminación ampliamente
utilizadas, especialmente las lámparas de descarga de alta intensidad
utilizadas en exteriores se encuentran en el RG2 (riesgo moderado).
No obstante, estas lámparas tienen utilizaciones claramente
identificadas y solo pueden ser instaladas por profesionales que
tendrían que estar conscientes de los requisitos de distancia de
seguridad para limitar la exposición.
__ OTRAS LIMITACIONES DE LA IEC 62471 Y LA CIE S009; LA TOMA EN CONSIDERACIÓN DE PERSONAS SENSIBLES
Los límites máximos de exposición definidos por la ICNIRP y que son
utilizados para definir los grupos de riesgo tanto en la IEC 62471 como
en la CIE S009 no son adecuados en el caso de exposiciones repetidas
a la luz azul como si fueran calculados para una exposición máxima
en un día de 8 horas. Estos no toman en consideración la posibilidad
de una exposición a lo largo de toda la vida.
Ni la CIE S009 ni la IEC 62471 toman, en consideración la
sensibilidad de algunos grupos de personas específicos que se
caracterizan por una mayor sensibilidad a la luz visible como por
ejemplo:
• Las personas que tienen condiciones oculares o dérmicas
preexistentes y cuyos síntomas patológicos pueden ser desencadenados
o agravados por la luz artificial.
• Los afáquicos (personas sin cristalino) y pseudoafáquicos (personas
con cristalinos artificiales) que, como consecuencia de su estado,
no pueden, o lo hacen de modo insuficiente, filtrar longitudes
de onda cortas (especialmente la luz azul).
• Los niños.
5 Centro Científico y Técnico de la Construcción (Centre Scientifique et Technique du Bâtiment).6 Laboratorio Nacional de Metrología y de Ensayo (Laboratoire National de Métrologie et d’Essais).7 Comisión Internacional de la Iluminación (Commission Internationale de l’Éclairage).

Points de Vue - n°68 - Spring / Primavera - 201356
LUZ AZUL
Científico no médico
• Las personas mayores porque sus ojos son más sensibles a las
radiaciones ópticas.
Las normas fotobiológicas relativas a los sistemas de iluminación
deberían extenderse para cubrir a los niños y a las personas fáquicas
o pseudoafáquicas, tomando en consideración la curva de fototoxicidad
correspondiente publicada por la ICNIRP en sus directrices.
Además del comprobado daño fotoquímico en la retina resultante de
una exposición aguda a la luz azul, todavía hay incertidumbre sobre
los efectos de la exposición crónica en dosis bajas. Dichos efectos
todavía son objeto de investigación por parte de oftalmólogos, biólogos
y científicos ópticos. En Francia, el proyecto RETINALED 8 investiga
los efectos de la baja exposición crónica de los rumiantes a la luz
emitida por los LED.
Algunas categorías de trabajadores están expuestos a altas dosis
de luz artificial (tiempos largos de exposición y/o iluminancias
retinianas elevadas) en sus actividades del día a día (ejemplos:
profesionales
de la iluminación, artistas de escenario, etc.). Puesto que todavía
no se han comprendido completamente los mecanismos que ocasionan
los daños, los trabajadores expuestos deberían utilizar los medios
de protección individual adecuados como una medida de precaución
(lentes que filtran la luz azul, por ejemplo).
__ CONCLUSIONES
Debido a sus propiedades únicas de emisión de luz, los LED se están
convirtiendo en la fuente de luz dominante en este siglo.
No obstante, los riesgos que plantean estas nuevas fuentes de luz
también son inherentes a sus características: alta eficacia óptica
en un dispositivo pequeño (produciendo así un alto nivel de radiancia)
asociado a un nivel significativo de emisiones de luz azul.
La combinación de ambos factores puede potencialmente aumentar
el riesgo de daños fotoquímicos en la retina, en comparación con la
lámpara incandescente y la lámpara fluorescente.
Los líderes de la industria de la iluminación están muy conscientes
de la seguridad fotobiológica de sus productos. Un gran número de
productos de iluminación que utilizan LED emiten ahora tonos más
cálidos de luz blanca (reducción del contenido de luz azul en el espectro)
o bien utilizan difusores para disminuir el deslumbramiento (reducción
de la radiancia). Se ha encontrado que la mayoría de los productos
de iluminación presentan bajos riesgos, o ninguno, para la población
en general cuando la distancia de visualización es igual o mayor a los
200 mm.
Sin embargo, las campañas de medición realizadas por agencias
independientes han señalado algunos productos de iluminación con
riesgos significativamente superiores en una distancia de menos de un
metro o más. Actualmente, los fabricantes de productos de iluminación
no hacen ninguna mención de una «distancia de seguridad».
Por lo tanto, es imposible que el público identifique lámparas
o luminarias con un nivel superior de riesgos.
La evaluación de riesgos por luz azul relacionada con los LED puede
llevarse a cabo por laboratorios de pruebas que utilizan la norma IEC
62471 y que no determina de una manera perfectamente clara la
distancia de visualización que hay que considerar. Además, esta norma
no toma en consideración a los grupos de personas sensibles como
los niños, los afáquicos, los pseudoafáquicos y las personas mayores,
a pesar del hecho de que estas personas están expuestas a niveles
superiores de luz azul en la retina.
Los conocimientos actuales de los mecanismos de la fototoxicidad
de la luz azul distan mucho de estar completos. Los efectos
de la exposición crónica y de la baja exposición acumulada en períodos
muy largos todavía siguen siendo objeto de investigación activa.
REFERENCIAS
F. Behar-Cohen, C. Martinsons, F. Viénot, G. Zissis, A. Barlier-Salsi, J.P. Cesarini, O. Enouf, M. Garcia, S. Picaud, D. Attia, Light-emitting diodes (LED) for domestic lighting: Any risks for the eye?, Progress in Retinal and Eye Research, Volume 30, Issue 4, July 2011, Pages 239-257.
« Effets sanitaires des systèmes d’éclairage utilisant des diodes électroluminescentes (LED) », Saisine n°2008-SA-0408, Rapport d’expertise collective de l’Agence Nationale de Sécurité Sanitaire de l’Alimentation, de l’Environnement et du Travail (ANSES), www.anses.fr
“Health Effects of Artificial Light”, Opinion of the Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR), European Commission, March 2012, ISSN 1831-4783, http://ec.europa.eu/health/scientific_committees/policy/index_en.htm
EN 62471, European Standard, “Photobiological Safety of Lamps and Lamp Systems”, 2008.
8 El INSERM, CSTB y ENVA llevan a cabo el proyecto RETINALED, con el apoyo de la ADEME (Agencia Francesa del Medio Ambiente y Gestión de la Energía).
BIOGRAFIA
Christophe Martinsons obtuvo su Doctorado (Ph.D) de Física
de la Universidad de Reims Champagne-Ardenne en 1998.
Hasta el año 2000, ocupó el puesto de investigador
científico en el Laboratorio Nacional de Física. De 2000 a 2007,
trabajó en el área de la automatización doméstica para el Grupo HAGER.
En 2007, se incorporó a CSTB para dirigir la división de Iluminación,
Electricidad y Electromagnetismo.
Actualmente dirige investigaciones y consultorías en el área
de la iluminación artificial combinada con la luz natural
para la promoción de la eficiencia energética en edificios a la vez
de que se suministran las mejores condiciones de comodidad visual
para los usuarios. El enfoque que él ha desarrollado en torno
a la iluminación se ha incorporado en el nuevo código energético
de la construcción francesa (RT 2012).
En los últimos cuatro años, Christophe Martinsons ha venido
dirigiendo campañas de medición en laboratorio para agencias
gubernamentales francesas, trabajando también en estudios
independientes sobre los aspectos medioambientales y sanitarios
de la iluminación sólida y los LED.

Points de Vue - n°68 - Spring / Primavera - 2013 57
LUZ AZUL
Científico no médico
L A P E R C E P C I Ó N D E L C O L O R A Z U L Y E L
F I L T R A D O E S P E C T R A L
__ INTRODUCCIÓN
Sabemos que el cielo es azul y los físicos nos dan la explicación
de la preponderancia de las radiaciones de longitudes de onda cortas
en la luz difundida por la atmósfera. No obstante, cabe preguntarse
¿por qué vemos el cielo de color azul?
Ver el mundo en colores e identificar sus características requiere un
tratamiento de la imagen formada mediante la distribución de los
fotones en la retina.
__ 1. ¿CÓMO SE ELABORA LA SENSACIÓN DE COLOR?
Primeramente, recordemos las diferentes etapas del funcionamiento
de la visión de los colores. Los fotorreceptores absorben los fotones
que llegan a la retina; se trata de los conos en el caso de la visión de
día, y los bastones para la visión con poca luz y, a menudo, ambos
fotorreceptores, tanto los conos como los bastones, intervienen si la
iluminación es ligeramente reducida. Los fotorreceptores generan
una señal cuando captan un fotón, cualquiera que sea su longitud de
onda asociada. Debido a una sensibilidad espectral muy extendida
en el ámbito de las longitudes de onda, prácticamente todos los
fotorreceptores son aptos a absorber a los fotones de longitud de onda
corta. Lo único que los diferencia es la tasa de absorción.
De esta manera, los conos «S» (nombrados inadecuadamente
«azules») son preferentemente sensibles a las longitudes
FRANÇOISE VIÉNOT Museo Nacional de Historia Natural (MNHN), Centro de Investigación sobre la Conservación de las Colecciones (CRCC) París, Francia
LUZ AZUL
Científico no médico
400 500 600 700
Sen
sibi
lidad
esp
ectra
l de
los
cono
s
Longitud de onda (nm)
FIG. 1 Sensibilidad espectral de las tres familias de conos retinianos.
de onda cortas, hacia los 450 nm; los conos «M» («verdes»)
a las longitudes de onda medias, hacia los 540 nm; los conos «L»
(«rojos») hacia los 570 nm, y los bastones hacia los 507 nm.
No obstante, existe la probabilidad de que un fotón de 450 nm,
por ejemplo, que llegue la retina sea absorbido por otro fotorreceptor
distinto de un cono «S».
Inmediatamente desde su salida, las señales de los fotorreceptores
se recombinan; se trata, esencialmente de señales de contraste,
de origen luminoso o espectral, que entran en las numerosas
vías visuales de la retina. En cuanto a las señales retinianas que se
dirigen hacia el córtex, estas llevan a cabo aún más recombinaciones,
con ponderaciones variables, antes de dar nacimiento a la sensación
de color. Generalmente, en estas recombinaciones, las señales de todas
las familias de conos participan, con ponderaciones variables.
De esta manera, el color es un atributo de apariencia construido por
nuestro sistema visual. Lo que caracteriza esencialmente al color de
los materiales es la tonalidad y su determinación es excepcionalmente
estable en nuestro entorno natural. Este fenómeno de estabilidad
relativa se denomina la constancia del color.
En cuanto al efecto de un filtrado espectral, cabe recordar
que prácticamente todas las familias de fotorreceptores
pueden ser estimuladas por las longitudes de ondas cortas.
Un desequilibrio de las señales generadas en los conos puede acarrear
una modificación de los contrastes percibidos y una perturbación
de la percepción de colores que, sin embargo, no es radical en la
medida en la que las tres familias de conos están intactas.
__ 2. PARTICULARIDADES DE LA VISIÓN DEL AZUL
En la visión de los colores, el azul, o más exactamente el camino
retiniano de las señales emanantes de los conos «S» presenta
un estatuto particular. Estas señales sólo participan ligeramente al
contraste luminoso en frecuencias espaciales o temporales elevadas.
Points de Vue - n°68 - Spring / Primavera - 201358
LUZ AZUL
Científico no médico
Por esta razón, la agudeza o la sensibilidad al parpadeo no se basan
en estas señales. Incluso se habla de tritanopía foveal o tritanopía
de campo estrecho para indicar la reducción de la visión
de los colores debido a la incapacidad de los conos «S» para procesar
algunos contrastes de color.
En cambio, las señales de los conos «S» contribuyen
significativamente a la discriminación de los colores, y desempeñan
un papel esencial en el establecimiento de los tonos. Por ejemplo, la
diferencia entre el amarillo o el blanco, o la diferencia entre las luces
blancas cálidas o blancas frías, depende de la respuesta de los conos
«S».
Resumiendo a propósito del filtrado espectral: Una gran reducción
de las señales de los conos «S» no debería tener un impacto
en la agudeza, pero podría deteriorar la capacidad de discriminación
de los tonos y modificar la sensación coloreada. Sin embargo,
en la medida en la que algunas señales de conos «S», incluso débiles,
pasan por las redes de las neuronas retinianas, los cambios
de colores pasan a menudo desapercibidos.
__ 3. ¿CUÁL SERÍA EL IMPACTO DE UN FILTRO DE LAS LONGITUDES DE ONDA CORTAS VISIBLES?
Mientras las tres familias de conos puedan mantener una
actividad, la visión de los colores, basada en los contrastes, es posible.
Entonces, todo depende de la posición del corte del espectro visible.
Un corte hacia los 450 nm, que dejaría lugar a la entrada en los conos
«S» de casi el 50 % de los fotones disponibles, solo tendrá un bajo
impacto en la visión de los colores. De hecho, es lo que se produce
naturalmente con el envejecimiento y la catarata. El cielo sigue siendo
azul hasta una edad avanzada. El efecto de constancia perceptiva y,
en ese caso, de «constancia del color», estabiliza los colores de los
materiales del entorno los unos con respecto a los otros, cualesquiera
que sean las variaciones de luz.
Si el corte se sitúa hacia los 500 nm, un deterioro marcado
de la discriminación de los tonos es previsible en el azul-verde y en los
violetas, así como en algunos pares de colores como el amarillo y el
blanco, o el azul oscuro y el negro. La agudeza debería mantenerse.
En cambio, en la visión nocturna el sujeto podría sentir cierta molestia
por la falta aparente de luz.
__ CONCLUSIÓN
Cualquier filtrado espectral acarrea un déficit perceptivo. Aunque
la discriminación coloreada sigue estando deteriorada, las funciones
superiores, es decir, la apariencia y el reconocimiento de los colores,
quedan más bien preservadas. En materia de color, la respuesta visual
se adapta al entorno. Mientras la luz sea policromática, las capacidades
de adaptación fisiológica del ser humano compensan un déficit de luz
en la fuente. •
REFERENCIAS
Peter Gouras (2009) Color Vision, http://webvision.med.utah.edu/book/part-vii-color-vision/color-vision/
J. D. Mollon (1989) “Tho’ she kneel’d in that Place where they Grew”. J. exp. Biol. 146, 21-38.
F. Viénot, J. Le Rohellec (2012) Colorimetry and physiology: the LMS specification. In : C. Fernandez-Maloigne, F. Robert-Inacio, L. Macaire, Digital color. Acquisition, Perception, Coding and Rendering Digital Signal and Image Processing Series, ISTE, Wiley, pp. 1-27.
FIG. 2 Ilustración de la dificultad de percibir algunos detalles de colores que dependen de una variación de la señal de los conos «S» o «azules». Mientras que la superficie ocupada por las letras de la expresión «Points de Vue» es más reducida que la superficie del rectángulo, este último sobresale más.

Points de Vue - n°68 - Spring / Primavera - 2013 59
PRODUCTO
FIG. 2 La sumación (o fusión) binocular función de las diferencias de calidad óptica entre ambos ojos (Castro et al. 2009).
FIG. 1 Proceso cortical de la visión binocular.
Ambas imágenes deben ser de buena calidad y muy parecidas (fig. 2)
para que el cerebro pueda analizar sus semejanzas y diferencias
para luego poder fusionarlas en una percepción única
en tres dimensiones. A este proceso se le denomina visión binocular.
La visión binocular no solo permite la visión simple, sino que también
mejora la eficacia visual con respecto a una eficacia monocular,
gracias al fenómeno de sumación (o fusión) binocular [1, 2].
Exigencias para una buena visión binocular
Según Castro et al. [3], la sumación binocular es óptima cuando ambos
ojos tienen el mismo nivel de calidad óptica. Los autores utilizan el
cociente de Strehl como indicador de calidad óptica del ojo, y demuestran
que existe una correlación estadísticamente significativa entre la sumación
binocular y la diferencia del coeficiente de Strehl entre ambos ojos (fig. 2).
De esta manera, cuando ambos ojos tienen el mismo nivel de calidad
óptica, la sumación binocular es más elevada, cualquiera que sea la
edad del sujeto.
Ojo cíclope y dirección visual binocular
Como en el caso del cíclope de la mitología griega, aunque cada
uno de nuestros ojos reciban y analicen una imagen del mundo que nos
rodea, en la visión binocular nosotros percibimos una imagen
única desde un punto de vista virtual denominado el ojo cíclope.
La demostración de Hering ilustra bien este fenómeno (fig. 3).
Un sujeto mira a través de un agujero perforado en una lámina de
vidrio de manera tal que el ojo derecho sólo perciba la casa y el ojo
VARILUX S SER IES™:4D TECHNOLOGY™
E L C Á L C U L O B I N O C U L A R P E R S O N A L I Z A D O
E N F U N C I Ó N D E L O J O D I R E C T O R
PRODUCTO
Hasta el día de hoy, la visión binocular no se ha tomado totalmente
en consideración en ningún tipo de gafas con lentes progresivas.
No obstante, para una obtener una percepción visual óptima,
es necesario respetar los diferentes aspectos de la visión binocular,
cualesquiera que sean las prescripciones de ambos ojos. Para ir aún
más lejos, el ojo director desempeña un papel particular en el conjunto
ocular. Si se toma en consideración este parámetro, se puede mejorar
aún más la eficacia visual binocular del portador. Por primera vez,
la 4D TechnologyTM permite tomar en consideración estos diferentes
factores en el cálculo de las gafas con lentes progresivas.
__ VISIÓN BINOCULAR: LAS BASES FISIOLÓGICAS
Los seres humanos tienen dos ojos separados por una corta distancia
en el espacio, de manera que una amplia porción del campo visual es
percibida simultáneamente desde puntos de vista diferentes.
A través de las vías visuales, las dos retinas transmiten imágenes
monoculares dispares al córtex (fig. 1).
HÉLÈNE DE ROSSILAURENT CALIXTEDAMIEN PAILLEISABELLE POULAINI+D Óptica, Essilor Saint Maur, Francia
Escena observada
Imagen retiniana del ojo derecho
Imagen retiniana del ojo izquierdo
Córtex visual
Escena percibida
Diferencias interoculares en el ratio Strehl
Sum
ació
n bi
nocu
lar
1.55
1.50
1.45
1.40
1.35
1.30
1.25
1.20
1.15
0.00 0.01 0.02 0.03 0.04 0.05 0.06
r 2 = 0.80p < 0.01

Points de Vue - n°68 - Spring / Primavera - 201360
PRODUCTO
FIG. 3 Demostración de Hering (Howard & Rogers 2002).
FIG. 4 Experiencia en el simulador de realidad Virtual Essilor I+D. El sujeto debía indicar, con un dispositivo de videojuego (joypad) las orientaciones sucesivas de la E de Snellen (4 orientaciones posibles) que aparecían durante 1.500 ms en diferentes posiciones en el campo de visión binocular.
Entre cada aparición de la E, el sujeto debía colocar una cruz central ubicada en la dirección primaria de la mirada. Un defecto óptico adicional se colocaba alternativamente en el ojo director o en el otro. Se registró el tiempo de respuesta cada vez que aparecían las dianas (t respuesta joypad - t aparición diana).
izquierdo el árbol. Cuando ambos ojos están abiertos, la casa y el árbol
aparecen superpuestos en la misma dirección egocéntrica proveniente de
un punto situado aproximadamente en el plano mediano de la cabeza [4].
Este punto de referencia, denominado ojo cíclope, sirve de origen
para la dirección visual binocular. Este concepto es muy conocido en
el análisis de la visión binocular.
Coordinación oculomotora y ojo director
El ojo director desempeña un papel muy especial en la pareja ocular;
el sistema visual le da la preferencia en la realización de tareas
motoras y se comporta como un guía direccional para el otro ojo [5].
Otros resultados [6, 7] sugieren que el sistema visual trata la información
visual proveniente de este ojo prioritariamente.
Una experiencia realizada en el departamento de I&D de Essilor
International confirma el papel preponderante del ojo director
en la realización de tareas visuales dinámicas [8].
El objetivo de esta experiencia consistía en comparar el impacto
de un defecto óptico monocular en la eficacia visual binocular
en la realización de una tarea dinámica de detección visual (fig. 4).
La mitad de los sujetos implicados en la experiencia presentaban
un ojo director derecho, la otra mitad un ojo director izquierdo.
Los resultados muestran que un defecto óptico en el ojo director
aumenta de manera significativa el tiempo de respuesta de los sujetos
(p < 0.05), lo cual no es el caso cuando un defecto óptico equivalente
se coloca en el otro ojo.
Existen numerosas pruebas para determinar el ojo director. Porac y
Coren [9] distinguen dos tipos de pruebas: aquellas en las que la acción
de apuntar monocularmente es consciente y aquellas en las que esta es
inconsciente. La preferencia de los autores se orienta hacia el segundo
tipo de pruebas. Este es el caso de la prueba «Hole in the Card Test»
(prueba del agujero en la cartulina), en el que el sujeto debe fijar, con
ambos ojos abiertos, un objetivo que está delante de él, pero a través de
una tarjeta perforada. Se han desarrollado e incorporado un protocolo
y un dispositivo específico en el Visioffice para permitir al óptico
efectuar esta medición en el establecimiento (fig. 5). El cliente sujeta
la tableta con ambas manos y mira el objetivo de fijación del Visioffice
a través de la mira de la tableta. El nuevo software integrado en el
Visioffice determina automáticamente el ojo director de la persona. De
esta manera, al utilizar la nueva tableta 4D, el óptico puede identificar
rápidamente el ojo director de su cliente.
__ LENTES OFTÁLMICAS: LA OPTIMIZACIÓN BINOCULAR
Las lentes progresivas perturban la calidad de las imágenes retinianas
naturales derecha e izquierda con la presencia de aberraciones ópticas,
inevitables, y generadas por la variación óptica de potencia en la
periferia de la lente. De esta manera, estas afectan a la visión natural
binocular. Esto puede acarrear dificultades para la fusión
de las imágenes y la percepción del relieve, así como una reducción
de los campos de visión binocular.
Se viene abogando desde hace ya muchos años por que se tome en
cuenta la visión binocular en el diseño de las lentes. Por ejemplo,
algunos métodos permiten posicionar correctamente las zonas de visión
para seguir la convergencia natural del portador. No obstante, los
métodos de cálculo actuales se basan en un enfoque monocular que no
permite satisfacer totalmente la necesidad binocular de los portadores.
Cuando los ojos ven simultáneamente un mismo objeto, las eficacias
actuales de las lentes derecha e izquierda pueden ser diferentes
en las direcciones de mirada acopladas, especialmente en de que
ambos ojos no tengan la misma prescripción en la visión lejana.
En efecto, actualmente, las lentes son calculadas de manera separada
y las eficacias son optimizadas lente por lente sin considerar el
conjunto (la pareja) de lentes que forman las gafas; se habla en este
caso de diseño monocular.
FIG. 5 Medición del ojo director con el Visioffice.
Eje visual del ojo derecho
Escena tal y como la ve el observador
Eje visual del ojo izquierdo
Pla
no
Medio
Punto de fijación
Ojo cíclope
Vidrio
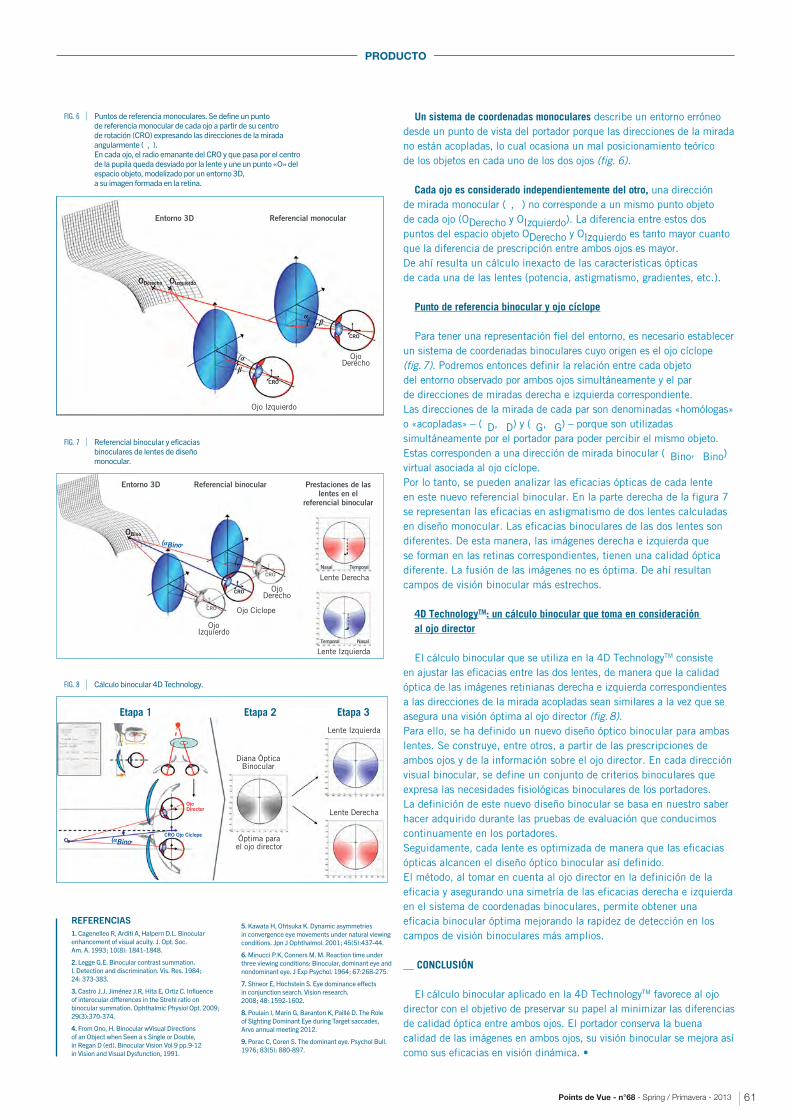
Points de Vue - n°68 - Spring / Primavera - 2013 61
PRODUCTO
FIG. 8 Cálculo binocular 4D Technology.
FIG. 6 Puntos de referencia monoculares. Se define un punto de referencia monocular de cada ojo a partir de su centro de rotación (CRO) expresando las direcciones de la mirada angularmente (�,�). En cada ojo, el radio emanante del CRO y que pasa por el centro de la pupila queda desviado por la lente y une un punto «O» del espacio objeto, modelizado por un entorno 3D, a su imagen formada en la retina.
Un sistema de coordenadas monoculares describe un entorno erróneo
desde un punto de vista del portador porque las direcciones de la mirada
no están acopladas, lo cual ocasiona un mal posicionamiento teórico
de los objetos en cada uno de los dos ojos (fig. 6).
Cada ojo es considerado independientemente del otro, una dirección
de mirada monocular (�, �) no corresponde a un mismo punto objeto
de cada ojo (ODerecho y OIzquierdo). La diferencia entre estos dos
puntos del espacio objeto ODerecho y OIzquierdo es tanto mayor cuanto
que la diferencia de prescripción entre ambos ojos es mayor.
De ahí resulta un cálculo inexacto de las características ópticas
de cada una de las lentes (potencia, astigmatismo, gradientes, etc.).
Punto de referencia binocular y ojo cíclope
Para tener una representación fiel del entorno, es necesario establecer
un sistema de coordenadas binoculares cuyo origen es el ojo cíclope
(fig. 7). Podremos entonces definir la relación entre cada objeto
del entorno observado por ambos ojos simultáneamente y el par
de direcciones de miradas derecha e izquierda correspondiente.
Las direcciones de la mirada de cada par son denominadas «homólogas»
o «acopladas» – (�D, �D) y (�G, �G) – porque son utilizadas
simultáneamente por el portador para poder percibir el mismo objeto.
Estas corresponden a una dirección de mirada binocular (�Bino, �Bino)
virtual asociada al ojo cíclope.
Por lo tanto, se pueden analizar las eficacias ópticas de cada lente
en este nuevo referencial binocular. En la parte derecha de la figura 7
se representan las eficacias en astigmatismo de dos lentes calculadas
en diseño monocular. Las eficacias binoculares de las dos lentes son
diferentes. De esta manera, las imágenes derecha e izquierda que
se forman en las retinas correspondientes, tienen una calidad óptica
diferente. La fusión de las imágenes no es óptima. De ahí resultan
campos de visión binocular más estrechos.
4D TechnologyTM: un cálculo binocular que toma en consideración al ojo director
El cálculo binocular que se utiliza en la 4D TechnologyTM consiste
en ajustar las eficacias entre las dos lentes, de manera que la calidad
óptica de las imágenes retinianas derecha e izquierda correspondientes
a las direcciones de la mirada acopladas sean similares a la vez que se
asegura una visión óptima al ojo director (fig. 8).
Para ello, se ha definido un nuevo diseño óptico binocular para ambas
lentes. Se construye, entre otros, a partir de las prescripciones de
ambos ojos y de la información sobre el ojo director. En cada dirección
visual binocular, se define un conjunto de criterios binoculares que
expresa las necesidades fisiológicas binoculares de los portadores.
La definición de este nuevo diseño binocular se basa en nuestro saber
hacer adquirido durante las pruebas de evaluación que conducimos
continuamente en los portadores.
Seguidamente, cada lente es optimizada de manera que las eficacias
ópticas alcancen el diseño óptico binocular así definido.
El método, al tomar en cuenta al ojo director en la definición de la
eficacia y asegurando una simetría de las eficacias derecha e izquierda
en el sistema de coordenadas binoculares, permite obtener una
eficacia binocular óptima mejorando la rapidez de detección en los
campos de visión binoculares más amplios.
__ CONCLUSIÓN
El cálculo binocular aplicado en la 4D TechnologyTM favorece al ojo
director con el objetivo de preservar su papel al minimizar las diferencias
de calidad óptica entre ambos ojos. El portador conserva la buena
calidad de las imágenes en ambos ojos, su visión binocular se mejora así
como sus eficacias en visión dinámica. •
REFERENCIAS
1. Cagenelleo R, Arditi A, Halpern D.L. Binocular enhancement of visual acuity. J. Opt. Soc. Am. A. 1993 ; 10(8): 1841-1848.
2. Legge G.E. Binocular contrast summation. I. Detection and discrimination. Vis. Res. 1984 ; 24: 373-383.
3. Castro J.J, Jiménez J.R, Hita E, Ortiz C. Influence of interocular differences in the Strehl ratio on binocular summation. Ophthalmic Physiol Opt. 2009 ; 29(3):370-374.
4. From Ono, H. Binocular wVisual Directions of an Object when Seen a s Single or Double, in Regan D (ed). Binocular Vision Vol 9 pp.9-12 in Vision and Visual Dysfunction, 1991.
5. Kawata H, Ohtsuka K. Dynamic asymmetries in convergence eye movements under natural viewing conditions. Jpn J Ophthalmol. 2001 ; 45(5):437-44.
6. Minucci P.K, Conners M. M. Reaction time under three viewing conditions: Binocular, dominant eye and nondominant eye. J Exp Psychol. 1964 ; 67:268-275.
7. Shneor E, Hochstein S. Eye dominance effects in conjunction search. Vision research. 2008 ; 48: 1592-1602.
8. Poulain I, Marin G, Baranton K, Paillé D. The Roleof Sighting Dominant Eye during Target saccades, Arvo annual meeting 2012.
9. Porac C, Coren S. The dominant eye. Psychol Bull. 1976 ; 83(5): 880-897.
FIG. 7 Referencial binocular y eficacias binoculares de lentes de diseño monocular.
Entorno 3D Referencial monocular
CRO
CRO
ODerecho OIzquierdo
Ojo Derecho
Ojo Izquierdo
α
α
β
β
Entorno 3D Referencial binocular Prestaciones de laslentes en el
referencial binocular
Ojo Derecho
Lente Derecha
Lente Izquierda
Ojo Izquierdo
Ojo Cíclope
(αBino, OBino
CRO
Nasal
Nasal
Temporal
Temporal
CRO
CRO
Diana ÓpticaBinocular
Lente Izquierda
Lente Derecha
Óptima parael ojo director
Etapa 2 Etapa 3
OjoDirector
CRO Ojo Cíclope
Etapa 1
(αBino,

COMMITEES / COMITÉS
Bi-annual, International review of ophthalmic opticsRevista intercional semestral de Óptica Oftálmica
Circulation : 10, 000 French/German, English/Spanish,English/Chinese copies in 46 CountriesEdición : 10 000 ejemplares francés/alemán, inglés/español,inglés/chino difundidos en 46 países
ISSN 1290-9661ESSILOR INTERNATIONAL - R.C CRETEIL B 712 049 618147, rue de Paris 94 227 - Charenton Cedex France.Tel: 33 (0)1 49 77 42 24 - Fax: 33 (0)1 49 77 44 85
Marc AlexandreEx-Director of publication.
Ex-Director de la publicación.
Jean-Pierre ChauveauDirector of publication,
Director of World scientific
communication,
Essilor International.
Director de la publicación,
Director de la Comunicación
Científica Mundo,
Essilor Internacional.
Andréa ChopartEditor in Chief,
Redactora in jefe,
__ EDITORIAL COMMITEE / COMITÉ EDITORIAL
__ SCIENTIFIC READING COMMITTEE / COMITÉ CIENTÍFICO DE LECTURA
vueINTERNATIONAL REVIEW OF OPHTHALMIC OPTICS
REVISTA INTERCIONAL DE ÓPTICA OFTÁLMICA
Points de
Prof. Clifford BrooksIndiana University School of
Optometry, United States
Facultad de Optometría de la
Universidad de Indiana, EEUU.
Prof. Christian CorbéInvalides Institute, France
Founder President of the
Representative Association
for low vision Initiatives
(ARIBa), France
Court Expert.
Institut des Invalides, Francia
Presidente fundador
de la Asociación Representativa
de las Iniciativas en Baja Visión
(ARIBa), Francia
Perito Judicial.
Azucena LorenteCoordinator of Varilux
Institute, Essilor Spain.
Coordinador del instituto
Varilux, Essilor España.
Charles-Eric PoussinMarketing Director
Essilor Brazil.
Marketing director,
Essilor Brasil.
Alain RivelineVice President
Global Marketing,
Essilor International,
France
Vicepresidente
Marketing Mundial
Essilor International,
Francia.
Marc StreitTechnical Marketing Manager
Medical & professional
relations, Quality Manager,
Essilor Switzerland.
Responsable de Marketing
Técnico
Relaciones médicas
y profesionales
Responsable Calidad.
Essilor Suiza.
Rod TahranO.D., F.A.A.O.,
American Optometrist,
Vice-President
of Clinical Affairs,
O.D., F.A.A.O., Optometrista
estadounidense, vice Presidente
de las Relaciones Profesionales.
Essilor of America, Inc.
Louise TanguaySpecial projects, schools in optics
and Events Professional relations,
Essilor Canada.
Proyectos especiales,
Escuelas de óptica y
Acontecimientos.
Relaciones profesionales,
Essilor Canada.
Tim ThurnAustralian Optometrist
Director of Profesionnal
Services, Essilor Asia Pacific.
Optometrista australiano,
Director de Servicios
Profesionales, Essilor Asia
Pacifica.
Lily Peng ZhangTechnical Standard Manager,
Shanghai Essilor Optical.
Jefe de Normas Técnicas,
Shanghai Essilor Optical.
Dr. Colin FowlerDirector of Undergraduate
Clinical Studies Optometry
& Vision Sciences,
Aston University, UK.
Director de L’Undergraduate
Clinical Studies Optometry
& Vision Sciences,
Aston University, Reino Unido.
Prof. Julián García SánchezMedical Faculty UCM, Spain
Facultad de Medecina UCM,
España.
Prof. Mo JalieUniversity of Ulster, UK.
University of Ulster,
Reino Unido.
Prof. Farhad HafeziProfessor and Chief Medical
Officer, Ophthalmology
Clinic, Department of Clinical
Neurosciences, Geneva University
Hospitals, Switzerland
Profesor ordinario y médico,
jefe de la sección de oftalmología,
departamento de neurociencias
clínicas, hospitales universitarios
de Ginebra, Suiza
Bernard MaitenazInvetor of Varilux®,
Essilor, France.
Inventor del Varilux®,
Essilor, Francia.
Dr. Daniel Malacara HernándezOptic Research Centre, Mexico
Centro de Investigaciones
en Optica, México.
Prof. Yves PouliquenMember of the Académie
de Médecine, France
and of the Académie française.
Miembro de la Academia
de Medecina, Francia
y de l’Académie française.
Dr. Jack RunningerFormer editor of “Optometric
Management”, United States.
Ex editor de “Optometric
Management”, Estados Unidos.
Conception, Layout / Concepción, Maqueta:Essilor International - William HarrisTel : +33 (0)1 49 77 42 12Textuel La Mine 146, rue du Faubourg-Poissonnière75010 ParisTel : +33 (0)1 53 21 21 00
Printing / Imprenta:Groupe Renard – IMPRIM’VERT ® Tel: +33 (0)1 41 05 48 10
Front cover illustration / Visual de la portada: Colored Light on Black Background © John Rensten/Corbis
Any reproduction, in full or in part, of the articles included in this magazine, performed without the agreement of the autors concerned, is illegal. (art. 40 all. de la loi du 11 mars 1957) / Es totalmente ilícita de la reproducción, total o parcial de los artìculos de esta revista, efectuada sin haber previamente obtenido el consentimiento de sus autores. (Art. 40 all. des Gesetzes vom 11. März 1957).

V I S I T O U R
W E B S I T E
V I S I T E
N U E S T R O
S I T I O W E B
www.pointsdevue.net