“Qué papel van a jugar los nuevos tratamientos para eltratamiento de la hiperlipemia”
Fernando CiveiraHospital Universitario Miguel Servet, IIS Aragón
Universidad de Zaragoza

La relación entre reducción de cLDL yreducción de eventos está bien establecida

Concentración de LDLc en ensayos clínicos y eventoscardiovasculares
Meta-analysis used individual patient data from 8 randomised controlled statin trials, in which conventional lipids andapolipoproteins were determined in all study participants at baseline and at 1-year follow-up. N=38 153

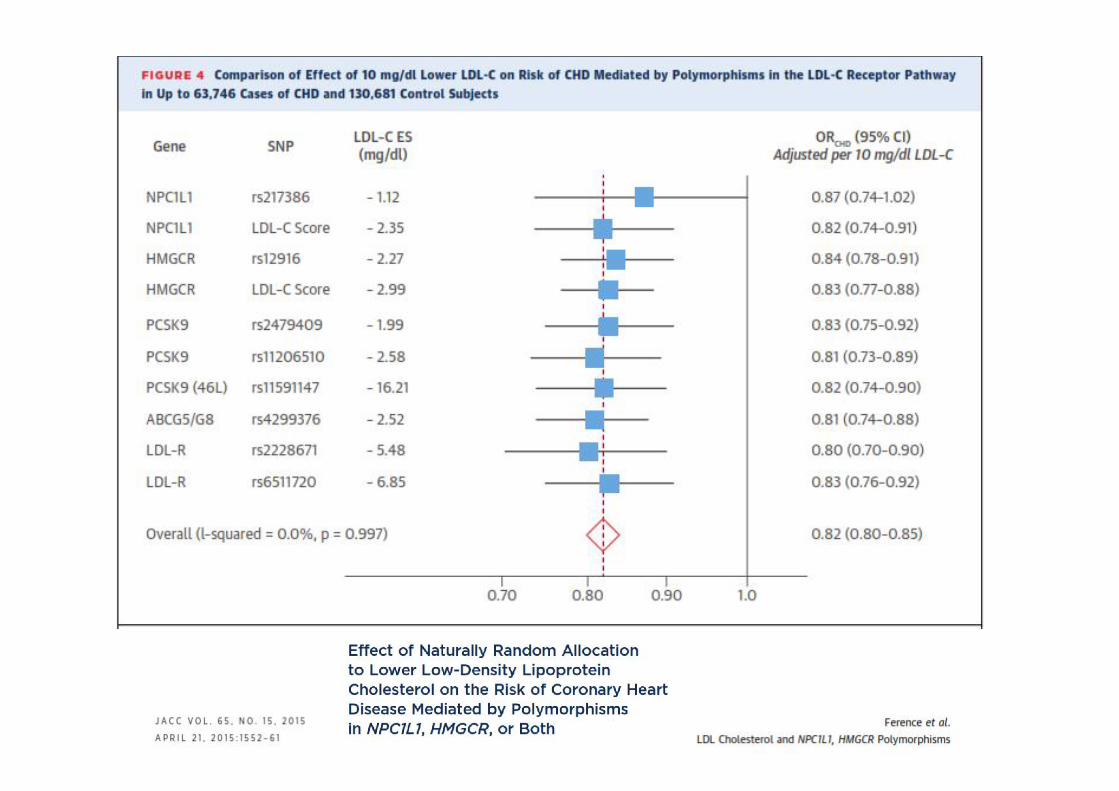


Reducción de eventos cardiovasculares mayores en relacióncon el descenso de LDLc según diferentes intervenciones
7



Objetivos en nuestros pacientes Post SCA / Post IM.Percepción y Realidad
RESULTADOS REPAR2
ESPAÑAEUROASPIRE IV- Global1
26%
74%
< 70mg/dl> 70mg/dl
N= 1395CARD= 140
1.- Kotseva et al EUROASPIRE IV: A European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management ofcoronary patients from 24 European countriesE. European Journal of Preventive Cardiology. DOI: 10.1177/2047487315569401 2.- Galve E, et al.Grado de control liipídico en pacientes coronarios y medidas adoptadas por los médicos. Estudio REPAR. Rev Esp Cardiol. 2016.http://dx.doi.org/10.1016/j.recesp.2016.02.013

¿Qué papel van a jugar los nuevostratamientos?
• Eficaces reduciendo el cLDL• Seguros• Reduzcan la enfermedad cardiovascular• Coste-efectivos
• Eficaces reduciendo el cLDL• Seguros• Reduzcan la enfermedad cardiovascular• Coste-efectivos

13
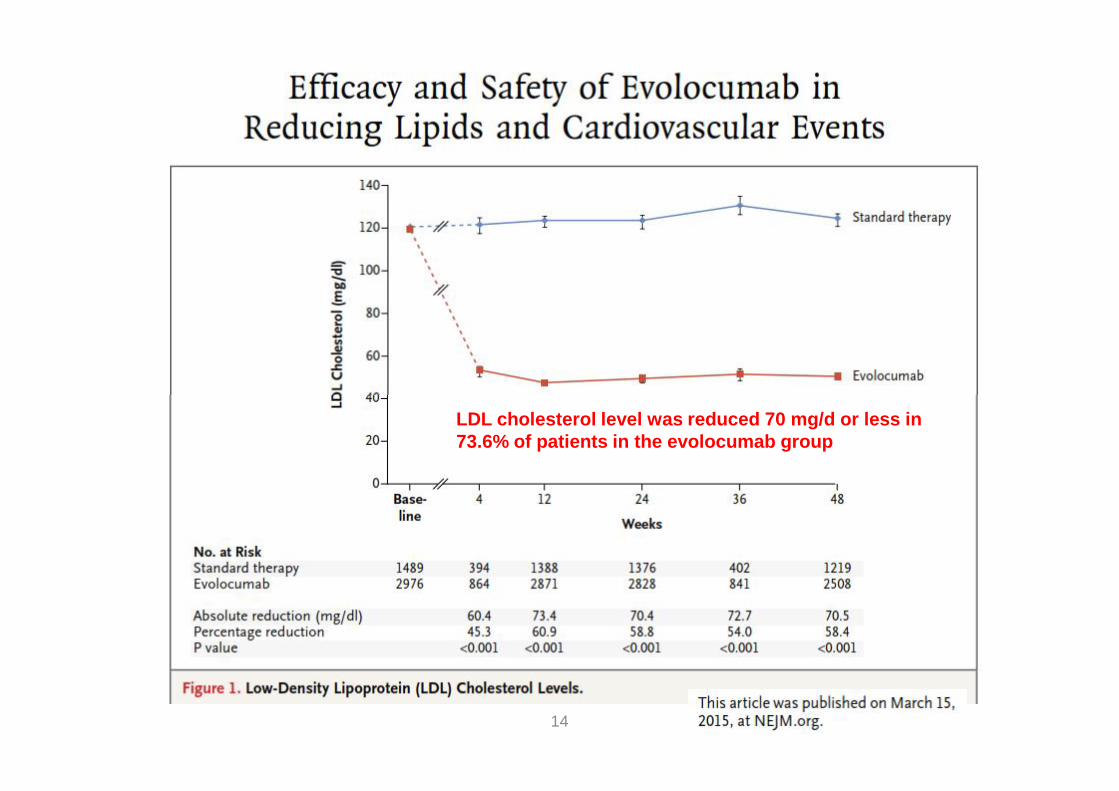
14
LDL cholesterol level was reduced 70 mg/d or less in73.6% of patients in the evolocumab group


Robinson J et al. N Engl J Med 2015;372:1489-99
LDL cholesterol level was reduced 70 mg/d or less in79.3% of patients in the alirocumab group
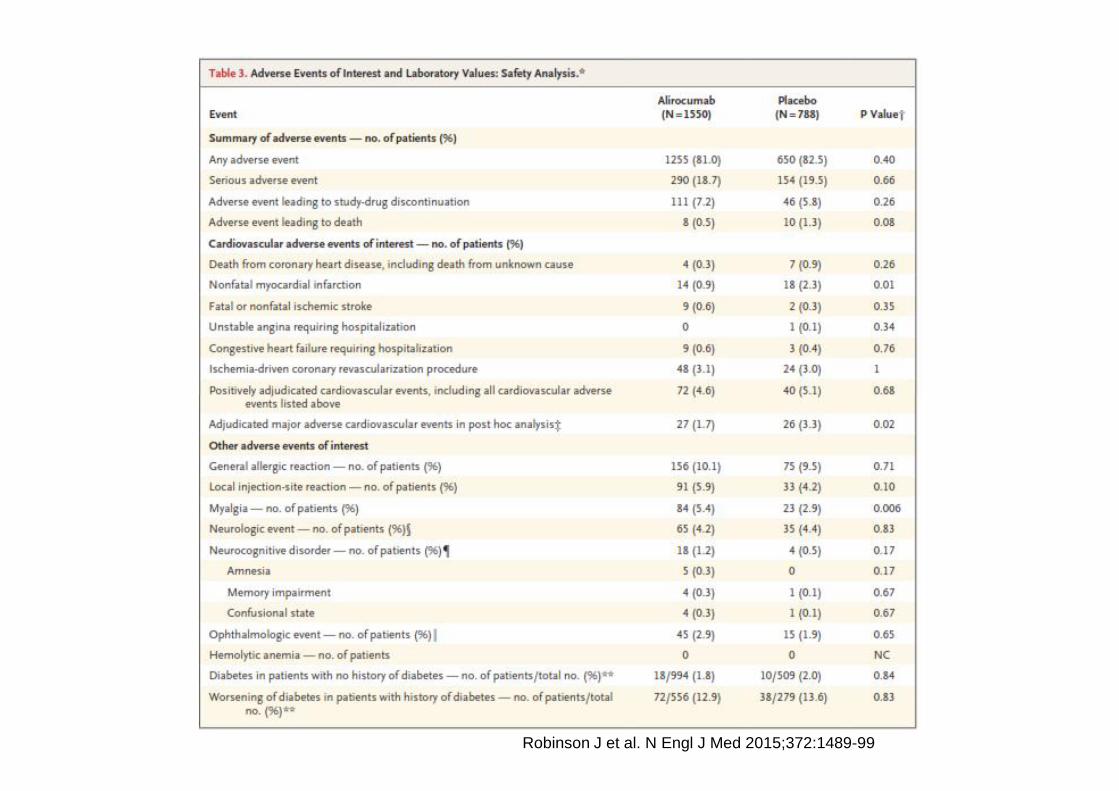
Robinson J et al. N Engl J Med 2015;372:1489-99

FH I and FH II% Reaching LDL-C Goals* at W24FH I and FH II% Reaching LDL-C Goals* at W24
50
60
70
80
90
Patie
nts (
%)
72.2%
81.4%
Alirocumab
Placebo
19
0
10
20
30
40
50
Patie
nts (
%)
2.4%
FH I
11.2%
FH II
P< 0.0001
ITT Analysis. Kastelein JP et al. ESC 2014* Very high risk < 1.8 mmol/L (70mg/L); high risk < 2.6 mmol/L (100mg/dL)

20
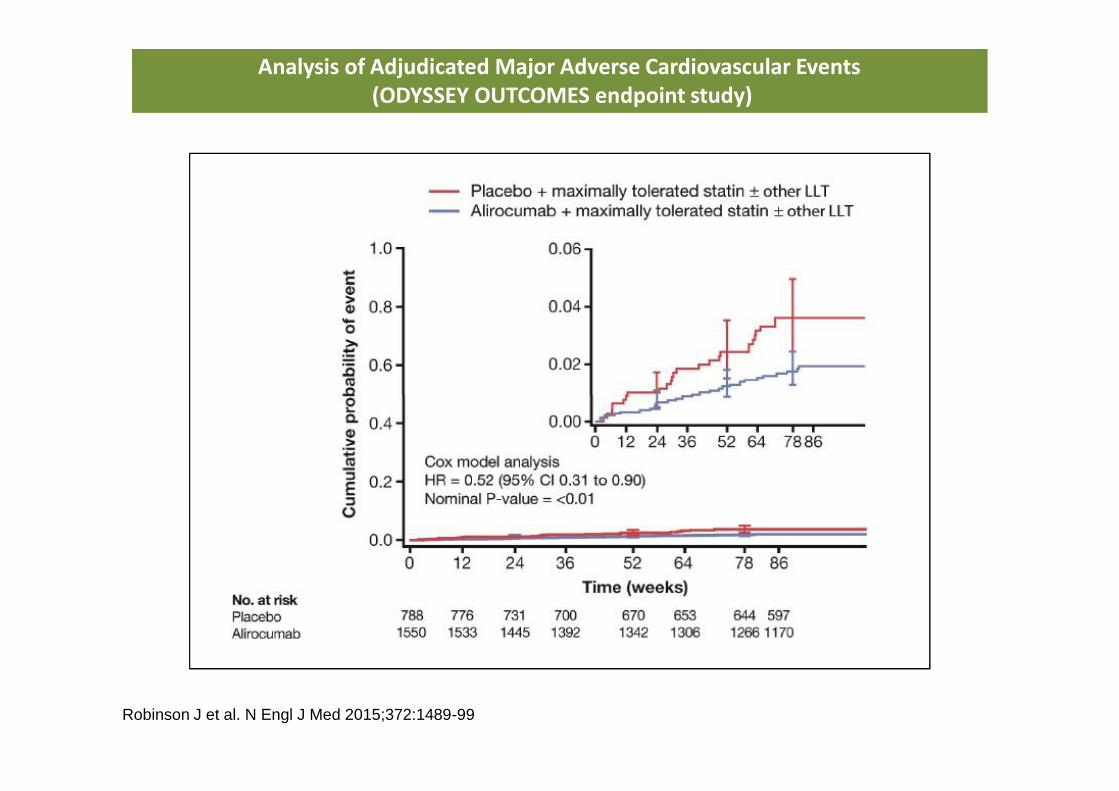
Analysis of Adjudicated Major Adverse Cardiovascular Events(ODYSSEY OUTCOMES endpoint study)
Analysis of Adjudicated Major Adverse Cardiovascular Events(ODYSSEY OUTCOMES endpoint study)
Robinson J et al. N Engl J Med 2015;372:1489-99

PCSK9 MetaPCSK9 Meta--AnalysisAnalysisAll Cause MortalityAll Cause Mortality
Navarese EP, et al. Ann Intern Med. 2015;doi:10.7326/M14-2957.

PCSK9 MetaPCSK9 Meta--AnalysisAnalysisCardiovascular MortalityCardiovascular Mortality
PCSK9 MetaPCSK9 Meta--AnalysisAnalysisCVCV MortalityMortality
Navarese EP, et al. Ann Intern Med. 2015;doi:10.7326/M14-2957.

PCSK9 MetaPCSK9 Meta--AnalysisAnalysisMyocardial InfarctionMyocardial Infarction
PCSK9 MetaPCSK9 Meta--AnalysisAnalysisOn MIOn MI
Navarese EP, et al. Ann Intern Med. 2015;doi:10.7326/M14-2957.

25

26
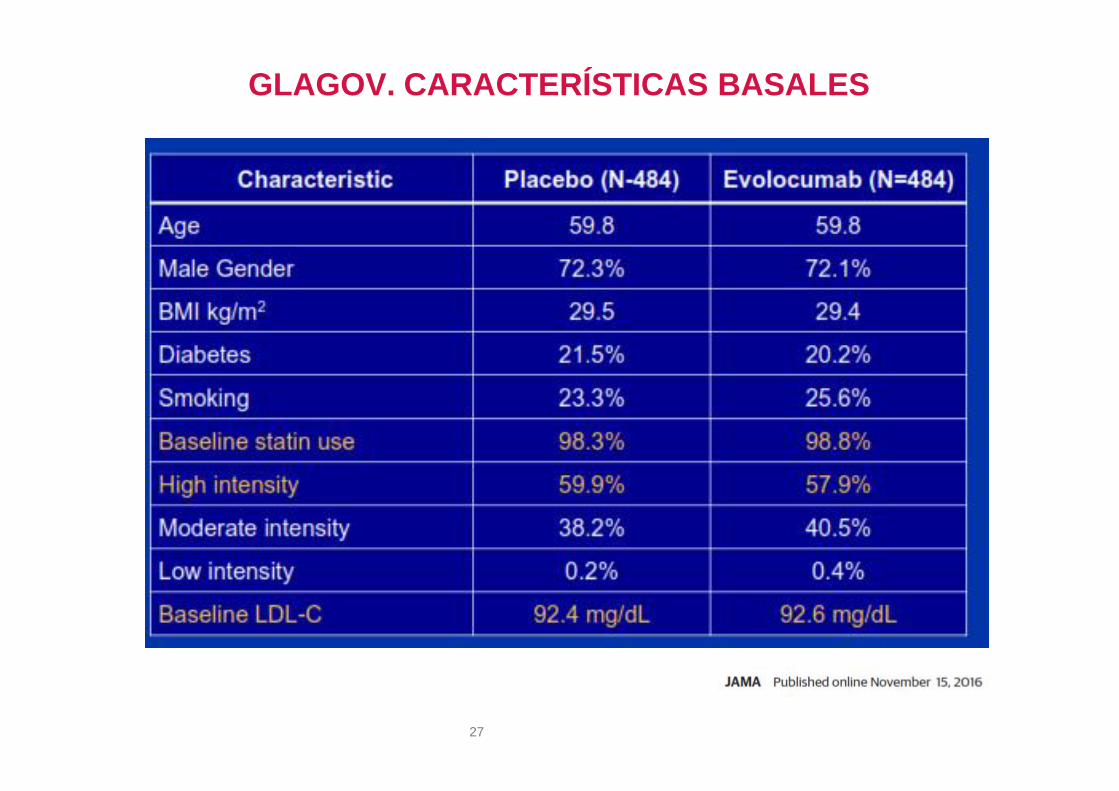
GLAGOV. CARACTERÍSTICAS BASALES
27

GLAGOV. CAMBIOS EN C-LDL
28
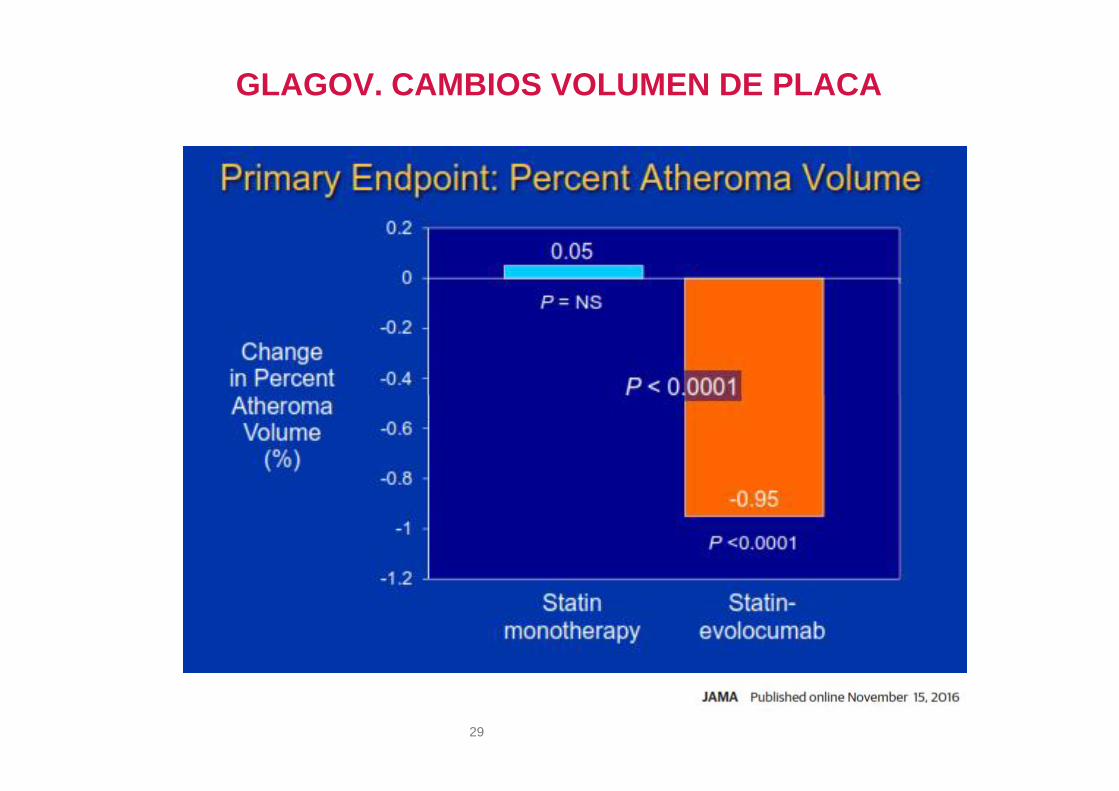
GLAGOV. CAMBIOS VOLUMEN DE PLACA
29

GLAGOV. CAMBIOS VOLUMEN DE PLACA
30

GLAGOV. CAMBIOS VOLUMEN DE PLACA
31

32

33

Phase 3 Trials: Alirocumab, Evolocumab, Bococizumab
PatientPop’n
Evolocumab (PROFICIO program) Alirocumab (ODYSSEY program) Bococizumab (SPIRE program)
Trial NPP TxDur’n(m)
PredictedPt
Exposure(Pt-Y)*
Min B/LLDL-C
(mg/dL)Trial N
PP TxDur’n(m)
PredictedPt
Exposure(Pt-Y)*
Min B/LLDL-C
(mg/dL)Trial N
PP TxDur’n(m)
PredictedPt
Exposure(Pt-Y)*
Min B/LLDL-C
(mg/dL)
ComboTherapy LAPLACE-2 1896 3 286 ≥80
COMBO I 311 12 205 ≥ 70HR 711 12 356 >70COMBO II 707 24 934 ≥70
OPTIONS I 345 6 51 ≥70LDL 2139 12 1070 >70OPTIONS II 298 6 51 ≥70
CHOICE I 803 12 573 NoneAPPRISE 1300 30 3250‡ ≥100
Mono MENDEL-2 614 3 77 ≥100 MONO 103 6 26 ≥70 AI 299 3 56 ≥70
HeFHRUTHERFORD-2 329 3 55 ≥100
FH I 485 18 483 ≥70 FH 370 12 185 >70FH II 247 18 249 ≥70
HIGH FH 107 18 107 ≥160HAUSER (paed) 150 6 50† ≥130
Numbers shown are based on estimated patient enrollment for ongoing studies and ITT populations for completed studies.No head-to-head studies available. No direct study comparison intended. This overview is intended to be used for scientific illustrative purposes only.
HAUSER (paed) 150 6 50† ≥130Apheresis 50 1.5 4† ≥100 ESCAPE 63 4 11 None
HoFHTESLA 49 3 8 ≥130
TAUSSIG (OL) 300 60 1500‡ ≥100Statin
IntoleranceGAUSS-2 307 3 51 None ALTERNATIVE 310 6 63 ≥70 SI 184 6 37 ≥70GAUSS-3 491 6 73 ≥100 CHOICE II 233 6 88 >70
Long termDESCARTES 901 12 599 ≥75 LONG-TERM 2310 18 2295 ≥70 LL 746 12 497 ≥100
OSLER-2 (OL) 3681 24 4908† None OLE (OL) 1000 40 3400 NoneAtheroma GLAGOV 968 18 726 ≥60
Lp(a) NCT02729025 120 4 27† ≥100
DMNCT02739984 400 3 67† None
DM 500 6 167† ≥70NCT02662569 900 3 150† ≥100TOTALS Patients: 7575 Predicted Pt Yrs: 8825 Patients: 7485 Predicted Pt Yrs: 11,627 Patients: 4202 Predicted Pt Yrs: 2561
CVDOutcomes FOURIER 27,564 Event
driven NA ≥70 OUTCOMES 18,000 Eventdriven NA ≥70
SPIRE-1 17,000 Eventdriven
NA ≥70SPIRE-2 11,000 NA ≥100
Neurocogevents EBBINGHAUS 1972 in
FOURIEREnd of
FOURIER N/A ≥70
*Predicted exposure to investigational product; †When randomisation not stated, assumed 2:1 in favour of investigational product; ‡Single-arm study. PP = per protocol; Tx = treatment; Dur’n = Duration; Pt Y = patient years
References to support data: see slide notes

Abstract: Xanthelasmas are superficial fat depositsaround the eyelids commonly present in differenthyperlipidemias and associated with increasedcardiovascular risk. Statins or other lipid-loweringtreatments do not usually modify them. We presentthe case of a middle-age man with severe high levels ofLDL cholesterol from youth due to a genetically definedheterozygous familiar hypercholesterolemia(HeFH). He presented large xanthelasmas of both innereyelids in spite of long term treatment with statins andezetimibe that disappeared after treatment withalirocumab75 mg every 2 weeks for 26 months. His LDLcholesterol went from 164 mg/dL to 47 mg/dL withalirocumab. Xanthelasma regressionwas not previously reported with lipid-lowering drugsin HeFH. This case demonstrates that regression of skinlipid lesions can be achieved with very low LDLcholesterol concentrations.
Abstract: Xanthelasmas are superficial fat depositsaround the eyelids commonly present in differenthyperlipidemias and associated with increasedcardiovascular risk. Statins or other lipid-loweringtreatments do not usually modify them. We presentthe case of a middle-age man with severe high levels ofLDL cholesterol from youth due to a genetically definedheterozygous familiar hypercholesterolemia(HeFH). He presented large xanthelasmas of both innereyelids in spite of long term treatment with statins andezetimibe that disappeared after treatment withalirocumab75 mg every 2 weeks for 26 months. His LDLcholesterol went from 164 mg/dL to 47 mg/dL withalirocumab. Xanthelasma regressionwas not previously reported with lipid-lowering drugsin HeFH. This case demonstrates that regression of skinlipid lesions can be achieved with very low LDLcholesterol concentrations.

¿Qué papel van a jugar los nuevostratamientos?
• Eficaces reduciendo el cLDL• Seguros• Reduzcan la enfermedad cardiovascular• Coste-efectivos
• Eficaces reduciendo el cLDL• Seguros• Reduzcan la enfermedad cardiovascular• Coste-efectivos





Determinantes recurrencias enfermedadcardiovascular
Registro prospectivo REduction of Atherothrombosis for Continued Health (REACH)
• Edad• Sexo• Tabaquismo activo• Diabetes• Nº de vasos afectos• Evento clínico en el último año• Historia de insufiencia cardiaca• Fibrilación auricular• No tomar antiagregación• LDL colesterol• Lp(a)
• Edad• Sexo• Tabaquismo activo• Diabetes• Nº de vasos afectos• Evento clínico en el último año• Historia de insufiencia cardiaca• Fibrilación auricular• No tomar antiagregación• LDL colesterol• Lp(a)


Indicaciones SEA anticuerpos anti PCSK9


Indicaciones financiadas con cargo al SistemaNacional de Salud
• Pacientes con Hipercolesterolemia familiar heterocigota (HFHe) nocontrolados con la dosis máxima tolerada de estatinas (C-LDL superior a100 mg/dl).
• Pacientes con Hipercolesterolemia familiar homocigota (HFHo) a partir delos 12 años no controlados con la dosis máxima tolerada de estatinas (C-LDL superior a 100 mg/dl).
• Pacientes con enfermedad cardiovascular establecida (cardiopatíaisquémica, enfermedad cerebrovascular isquémica y enfermedad arterialperiférica) no controlados con la dosis máxima tolerada de estatinas (C-LDL superior a 100 mg/dl).
• Cualquiera de los pacientes de los grupos anteriores, que seanintolerantes a las estatinas o en los que las estatinas están contraindicadasy cuyo nivel de LDL sea superior a 100 mg/dl.
• Pacientes con Hipercolesterolemia familiar heterocigota (HFHe) nocontrolados con la dosis máxima tolerada de estatinas (C-LDL superior a100 mg/dl).
• Pacientes con Hipercolesterolemia familiar homocigota (HFHo) a partir delos 12 años no controlados con la dosis máxima tolerada de estatinas (C-LDL superior a 100 mg/dl).
• Pacientes con enfermedad cardiovascular establecida (cardiopatíaisquémica, enfermedad cerebrovascular isquémica y enfermedad arterialperiférica) no controlados con la dosis máxima tolerada de estatinas (C-LDL superior a 100 mg/dl).
• Cualquiera de los pacientes de los grupos anteriores, que seanintolerantes a las estatinas o en los que las estatinas están contraindicadasy cuyo nivel de LDL sea superior a 100 mg/dl.

Conclusiones• La reducción del colesterol LDL es una herramienta
extraordinariamente eficaz para reducir la enfermedadcardiovascular ateromatosa y, por tanto, un objetivoterapéutico inexcusable en paciente de alto riesgo
• En sujetos de muy alto riesgo la concentración de colesterolLDL debe estar, al menos, < 70 mg/dL
• El tratamiento para conseguirlo son las medidas higiénico-dietéticas y dosis altas de estatinas potentes
• Cuando no es suficiente con lo anterior, la ezetimiba en elmomento actual es el fármaco de elección en tratamientocombinado
• Los inhibidores de PCSK9 consiguen llevar a objetivos decLDL a la casi totalidad de pacientes y están indicados enpresencia de muy alto riesgo en el corto medio plazo ycifras de cLDL lejos de objetivo con tratº máximo tolerado
• La reducción del colesterol LDL es una herramientaextraordinariamente eficaz para reducir la enfermedadcardiovascular ateromatosa y, por tanto, un objetivoterapéutico inexcusable en paciente de alto riesgo
• En sujetos de muy alto riesgo la concentración de colesterolLDL debe estar, al menos, < 70 mg/dL
• El tratamiento para conseguirlo son las medidas higiénico-dietéticas y dosis altas de estatinas potentes
• Cuando no es suficiente con lo anterior, la ezetimiba en elmomento actual es el fármaco de elección en tratamientocombinado
• Los inhibidores de PCSK9 consiguen llevar a objetivos decLDL a la casi totalidad de pacientes y están indicados enpresencia de muy alto riesgo en el corto medio plazo ycifras de cLDL lejos de objetivo con tratº máximo tolerado







