Mucormycosis: an update
Livio Pagano
Istituto di Ematologia
Roma

Fungal agents
Yeasts Moulds
Candida
Cryptococcus
Trichosporon spp
Rhodotorula
Modified from de Pauw et al, Med J Hematol Infect Dis 2011
SEPTATE
HYPHAE
Aspergillus spp
Scedosporium
Fusarium
ASEPTATE
HYPHAE
Zygomycetes
Dermatophytes
Trichophyton
Microsporon
Dimorphics
Histoplasma
Blastomyces
Coccidioides
Penicillium

Chamilos et al, Haematologica 2006 91: 986-9
Spectrum of Invasive Mold Infections at
autopsy
MD Anderson Hospital
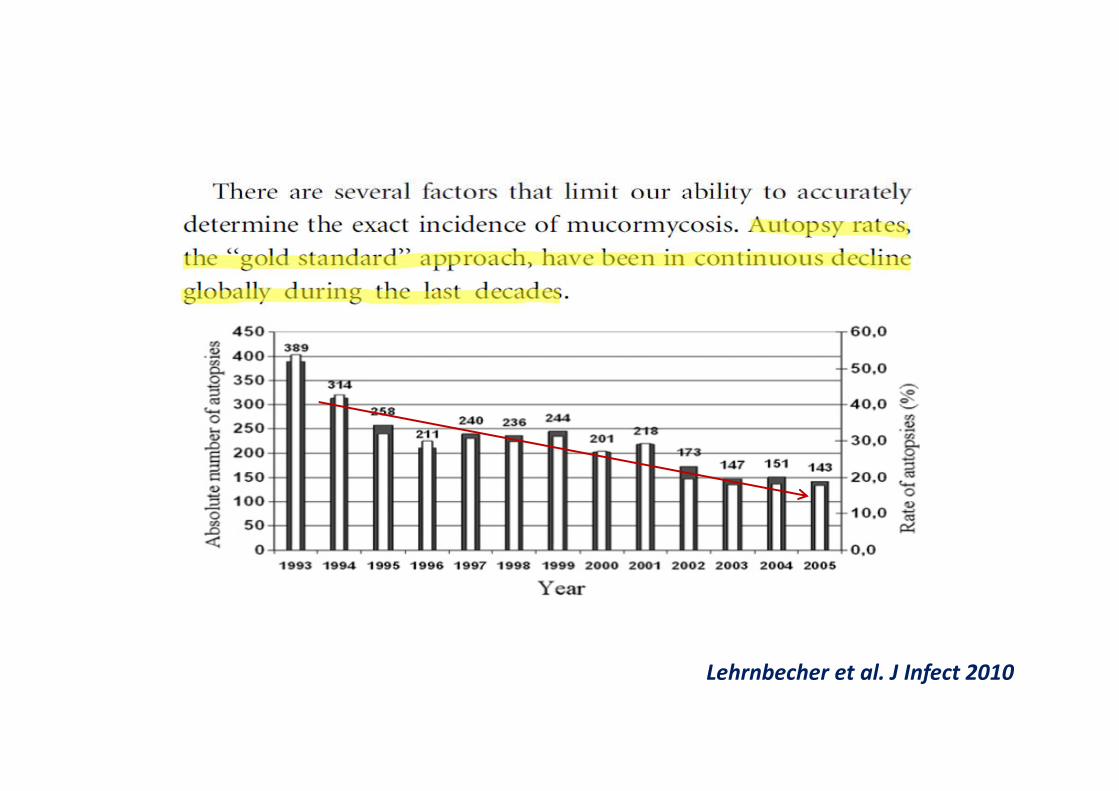
Lehrnbecher et al. J Infect 2010

Mucorales are characterized by wide hyphaes (10-20 mm), irregularly shaped, with acute angle
ramifications.
They are ubiquitarian, saprophytic, aerobic agents, that find an otpimal substratum for their growth in meat and sugar at a temperature of about 25°C-35°C

Virchows Arch [Pathol Anat] 102: 543-564 , 1885

direct inoculationinhalation
Fungus acquisition

Pathogenesis and classes of “high risk” patients for Mucormycosis
Substratum with high acidity (Ketoacidosis)
Macrophage inhibition in controlling spores germination (steroids = Autoimmune diseases)
Altered neutrophils chemotaxis (Diabetes)
Ferrioxamine transformation in ferrirhizoferrin (IRCand Trasfusion overload recipients)
Immunodepressant therapy (graft = HSCT and SOT)
NEUTROPENIA (hematological malignancy= ↑↑AML)

GR SPA FRA FRA BEL CH ITA EU
Mono Multi Multi Multi Mono Mono Multi Multi
24 6 531 101 31 19 60 230
Petrikkos et al. CMI 2014
Case-series collected
between 1993-2007

Proportion of HMs in IM case-series:
developed vs developing countries
Years All cases % HMs
cases
Roden et al, 2005 Global 1940-2003 929 21%
Bitar et al, 2009 France 1997-2006 531 17.3%
Ruping et al, 2010 Global 2006-2009 41 63.4%
Saegeman et al, 2010 Belgium 2000-2009 31 77%
Kara et al, 2009 Turkey 2001-2005 20 60%
Skiada et al, 2011 Europe 2004-2007 212 54%
Chakrabarti et al, 2009 India 2006-07 178 1.1%

Invasive Non-Aspergillus Mold Infections in
HSCT Recipients, United States, 2001-200615,820 HSCT 77 with Mucorales/983 IFDs
(0.08%)
Overall 12-month cumulative
incidence: 0.3%
0.85%
Park et al, Emerg Infect Dis 2011

Over a 10-year period
31 proven/probable cases

Strasfeld et al. Clin Lymph Myeloma & Leuk 2013

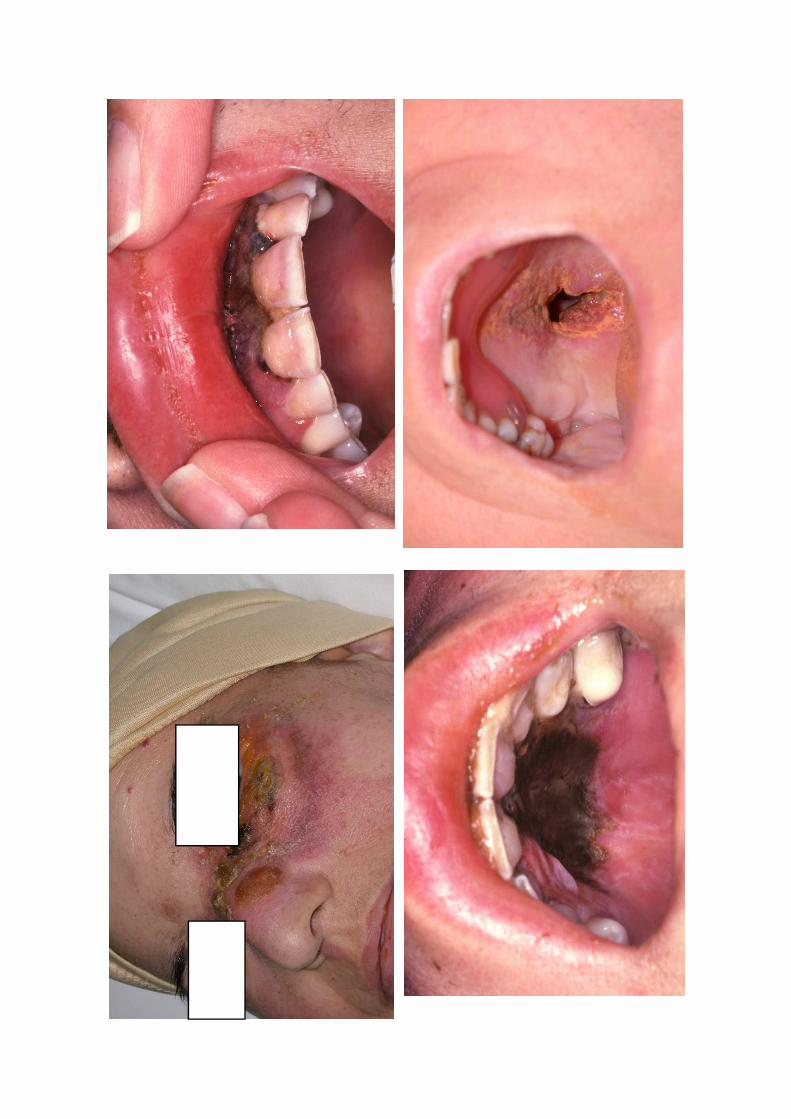
The most frequent
infection form is the
rino-cerebral
one, linked to the capability of fungi to
penetrate in the body through nasal and
nosepharyngeal mucosa
(typical of diabetic patient)
In neutropenic patients
can be instead more
easily observed the
picture of mycotic
pneumonia with a
penetration mechanism
similar to the previous
one

Petrikkos et al. CMI 2014
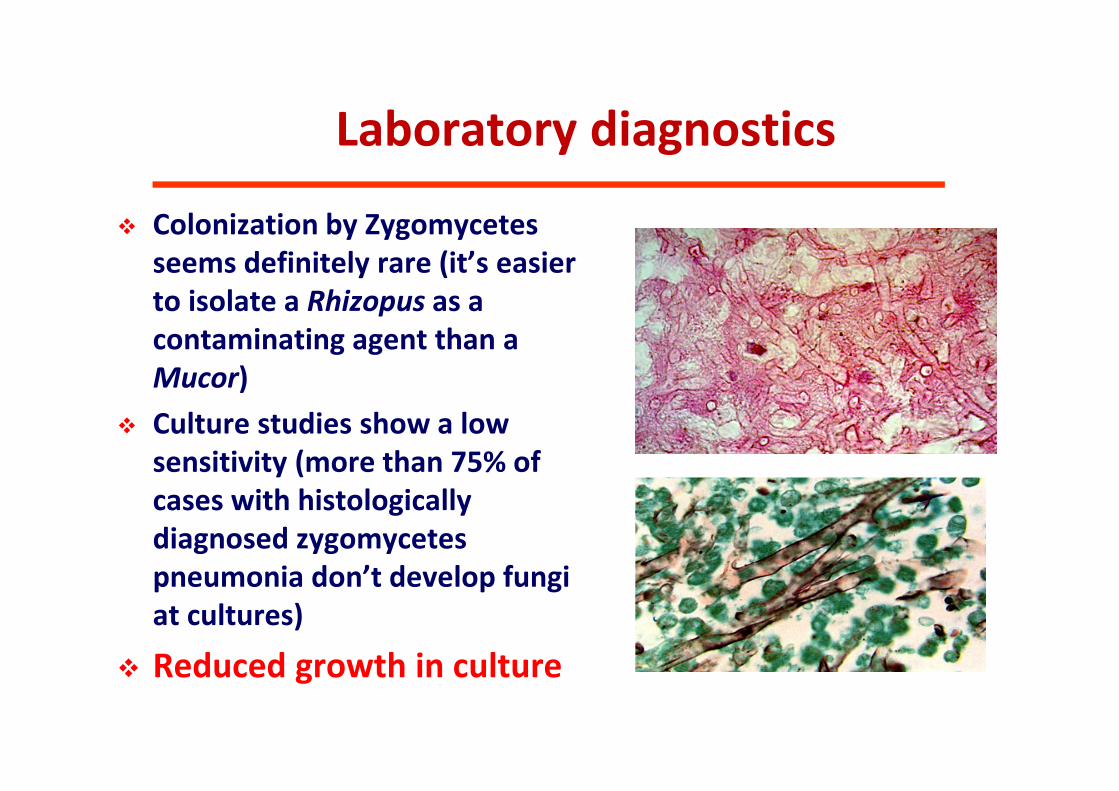
Laboratory diagnostics
Colonization by Zygomycetes
seems definitely rare (it’s easier
to isolate a Rhizopus as a
contaminating agent than a
Mucor)
Culture studies show a low
sensitivity (more than 75% of
cases with histologically
diagnosed zygomycetes
pneumonia don’t develop fungi
at cultures)
Reduced growth in culture

Galactomannan
negative in case of mucormycosis (as well as glucan)
Galactomannan
mold active prophylaxis decrease the predictive value (low
incidence of IA)
serum GM assay
o not reliable as surveillance in asymptomatic pts on
effective prophylaxis (results negative or FP)
o useful to diagnose pts with a clinical suspicion
Duarte CID 2014;

Evidence of Zygomycetes in the
BAL fluid
Fungiflora Y staining clearly showed fungal walls because the
fluorescence specifically attached to polysaccharides, such as
cellulose or chitin, which are present in fungal walls. Under
fluorescent microscopy, typical hyphae displayed brilliant green
fluorescence, which readily differentiated them from exfoliated
cells

Radiological Pictures
Halo-Sign
Air-Crescent-Sign
Mucormycete
s
Aspergillus
No radiological differences
But “reversed halo sign” may be suggestiveLegouge et al, CID 2014
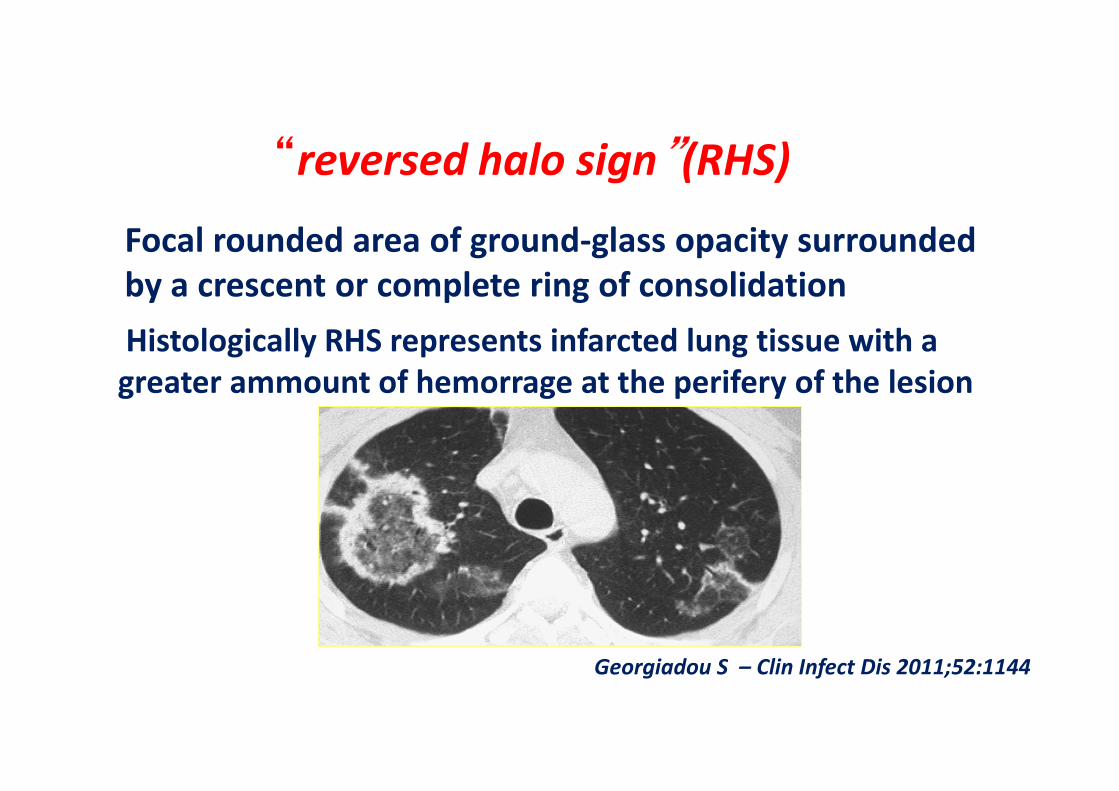
Focal rounded area of ground-glass opacity surrounded
by a crescent or complete ring of consolidation
Histologically RHS represents infarcted lung tissue with a
greater ammount of hemorrage at the perifery of the lesion
“reversed halo sign”(RHS)
Georgiadou S – Clin Infect Dis 2011;52:1144
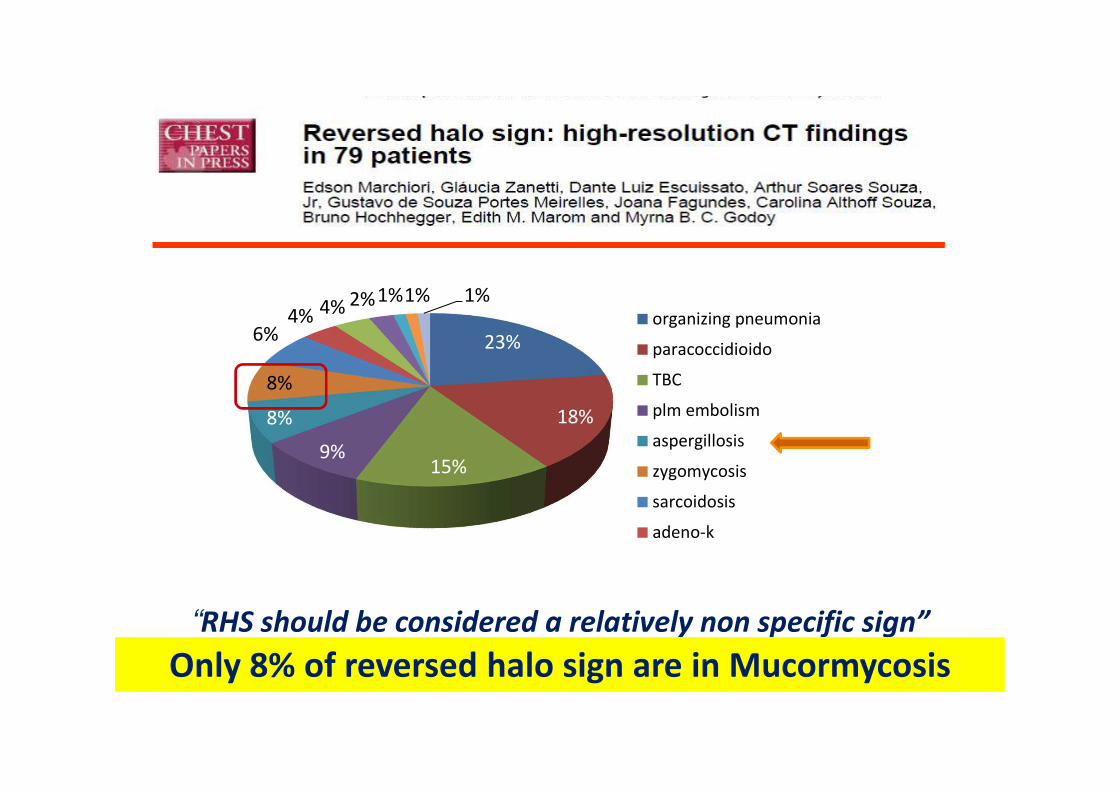
23%
18%
15%9%
8%
8%
6%4% 4% 2%1%1% 1%
organizing pneumonia
paracoccidioido
TBC
plm embolism
aspergillosis
zygomycosis
sarcoidosis
adeno-k
“RHS should be considered a relatively non specific sign”
Only 8% of reversed halo sign are in Mucormycosis

Stanzani et al. Clin Infect Dis 2012

Clin Nucl Med 2012

• Optimal for PCR-based diagnosis• Complications <1%. • NO false positivity
(NO CONTAMINATION)• Sensibility 80%; PPV 100% • Diagnosis in 53% of not diagnostic BAL
Int J Hematol. 2009 Jun; 89(5):624-7. Epub 2009 May 27.
Role of CT-guided percutaneous lung biopsyin diagnosis of pulmonary fungal infection
in patients with hematologic diseases.Shi JM, Cai Z, Huang H, Ye XJ, He JS, Xie WZ, Zhang J, Zhou XY, Luo Y, Lin Y, Li L, Zheng WY, Wei GQ, Lin MF.
Nosari A et al, Haematologica 2003Carrafiello G et al Radiol Med 2006
Laas-Florl et al Clin Infect Dis 2007
Gupta S. Hematologic Oncology 2009

The role of PCR
Hammond et al, JCM 2011
This is a useful tool that can improve tissue diagnosis of mucormycosis and
characterization of culture-negative IMD, thus facilitating targeted antifungal
therapy, but performed on formalin-fixed paraffin-embedded tissue samples
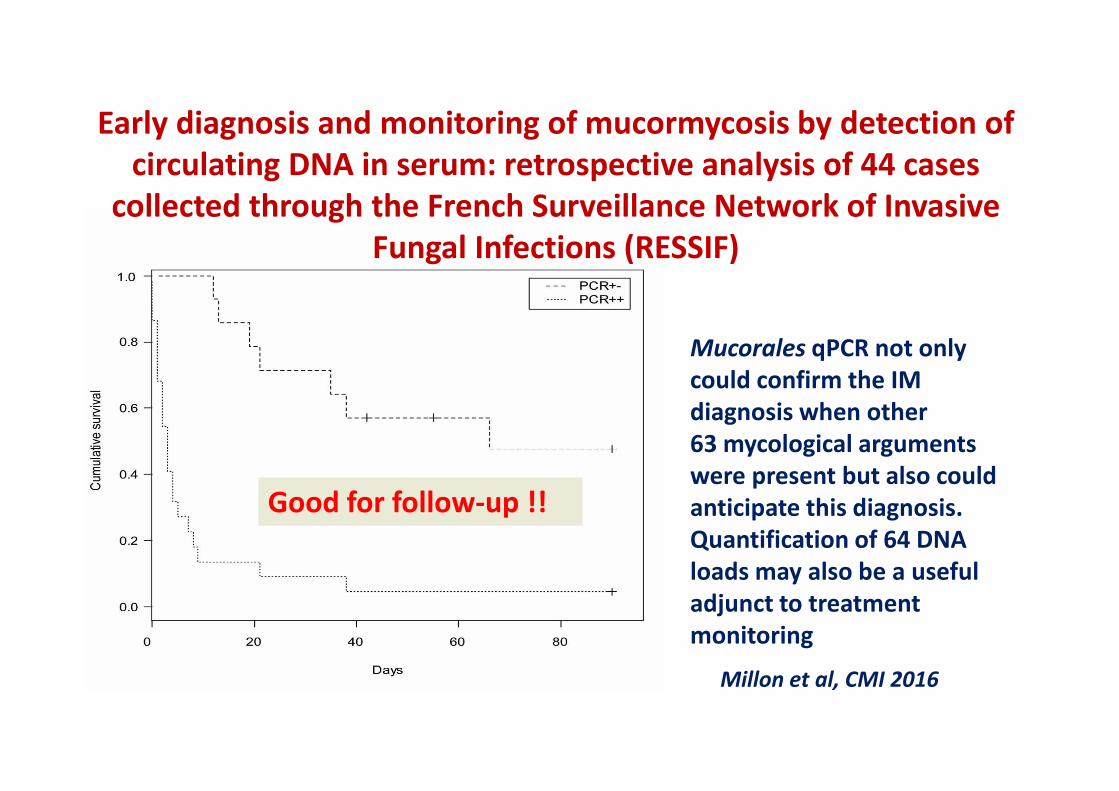
Early diagnosis and monitoring of mucormycosis by detection of
circulating DNA in serum: retrospective analysis of 44 cases
collected through the French Surveillance Network of Invasive
Fungal Infections (RESSIF)
Mucorales qPCR not only
could confirm the IM
diagnosis when other
63 mycological arguments
were present but also could
anticipate this diagnosis.
Quantification of 64 DNA
loads may also be a useful
adjunct to treatment
monitoring
Millon et al, CMI 2016
Good for follow-up !!

Mucorales-specific T cells as surrogate
diagnostic marker in high-risk patients
3 proven Mucormycosis
Mucorales-specific T cells, produced predominantly IL-4, IFN-γ, IL-10, may be
detected only in patients with IM
These cells specific were able to directly induce damage of Mucorales
Specific T cells contribute to human immune responses against Mucorales and
could be evaluated as a surrogate diagnostic marker of IM
Potenza et al, Blood 2011

ALGORITMO NEL PAZIENTE EMATOLOGICO
Pagano et al., Br J Haematol 2009; 146(6):597-606

Jeong et al. Mycoses 2015
2005-2014
30 pts with
proven/probable IM

Amphotericin B, posaconazole, and isavuconazole have activity against Mucorales
References: 1. Sabatelli F, et al. Antimicrob Agents Chemother. 2006;50(6):2009-2015. 2. Yamazaki T, et al. Int J Antimicrob Agents. 2010;36(4):324-31. 3. González GM.
Med Mycol. 2009;47(1):71-76. 4. The European Committee on Antimicrobial Susceptibility Testing. www.eucast.org. Accessed 31 March 2016. 5. Pfaller MA, et al. Diagn
Microbiol Infect Dis. 2015;82(4):303-313. 6. Thompson GR 3rd, et al. J Antimicrob Chemother. 2009;64(1):79-83. 7. Al-Hatmi AM, et al. J Antimicrob Chemother.
2015;70(4):1068-1071. 8. Deng S, et al. Antimicrob Agents Chemother. 2013;57(4):1974-1977. 9. Chowdhary A, et al. Clin Microbiol Infect. 2014;20(suppl 3):47-75. 10.
Najafzadeh MJ, et al. Antimicrob Agents Chemother. 2014;58(9):5629-5631. 11. Guinea J, et al. Antimicrob Agents Chemother. 2008;52(4):1396-1400. 12. Lackner M, et al.
Antimicrob Agents Chemother. 2012;56(5):2635-2642. 13. Arendrup MC, et al. Antimicrob Agents Chemother. 2015;59(12):7735-7742. 14. Cresemba, SPC.
Activity Variable activity Little or no activity
TRIAZOLES
AMB
FIRST GENERATION SECOND GENERATION
Fluconazole Itraconazole Voriconazole Posaconazole Isavuconazole
Aspergillus spp1-4
Fusarium spp.1,7
Chromoblastomycosis1,8
Phaeohyphomycoses1,9,10
Scedosporium apiospermum1,11,12
Scedosporium prolificans1,11,12
Mucorales1,13
Number of
isolates
MIC50 VALUES
Voriconazole Posaconazole Isavuconazole AMB
Lichtheimia corymbiferaa 12 16 0.125 1 ≤0.03
Rhizopus oryzaea 6 8 0.5 1 0.25
Rhizopus microsporusa 26 8 0.5 1 0.125
Rhizomucor pusillusa 9 8 0.06 0.5 ≤0.03
Lichtheimia ramosaa 5 8 ≤0.03 0.25 ≤0.03
Mucor circinelloides G-Ia 5 >16 0.5 8 ≤0.03
Mucor circinelloides G-IIa 9 >16 2 8 0.06
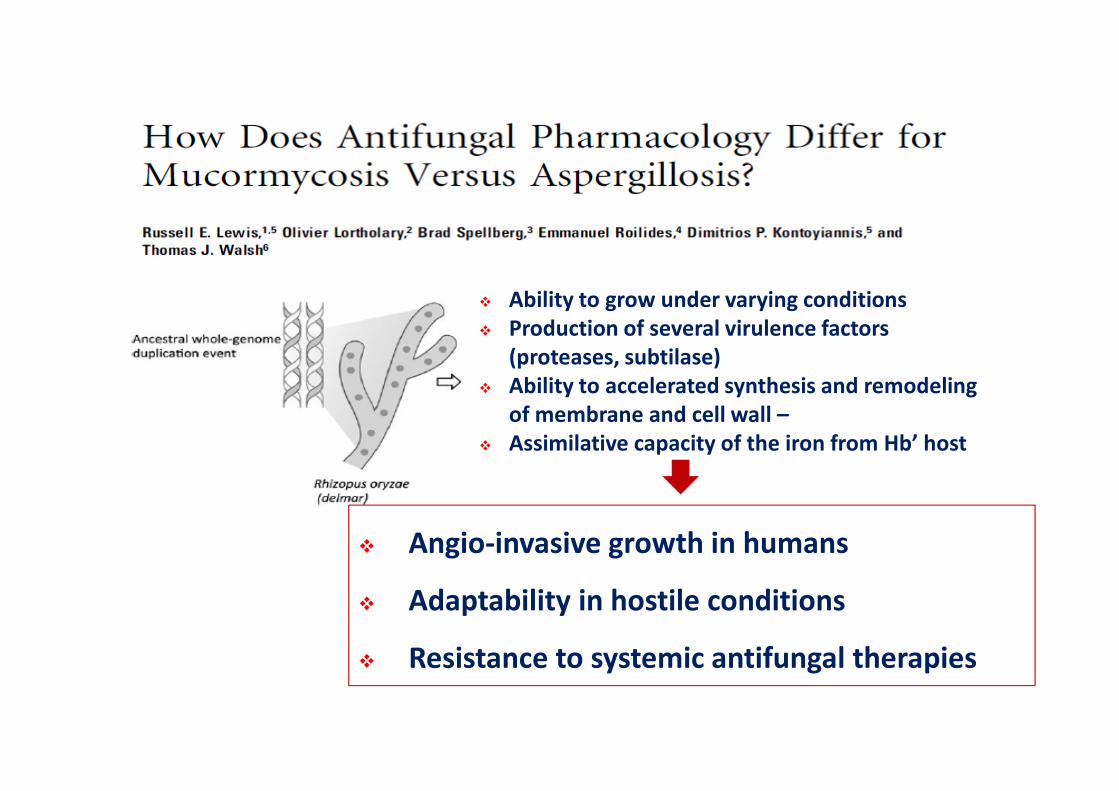
Ability to grow under varying conditions
Production of several virulence factors
(proteases, subtilase)
Ability to accelerated synthesis and remodeling
of membrane and cell wall –
Assimilative capacity of the iron from Hb’ host
Angio-invasive growth in humans
Adaptability in hostile conditions
Resistance to systemic antifungal therapies
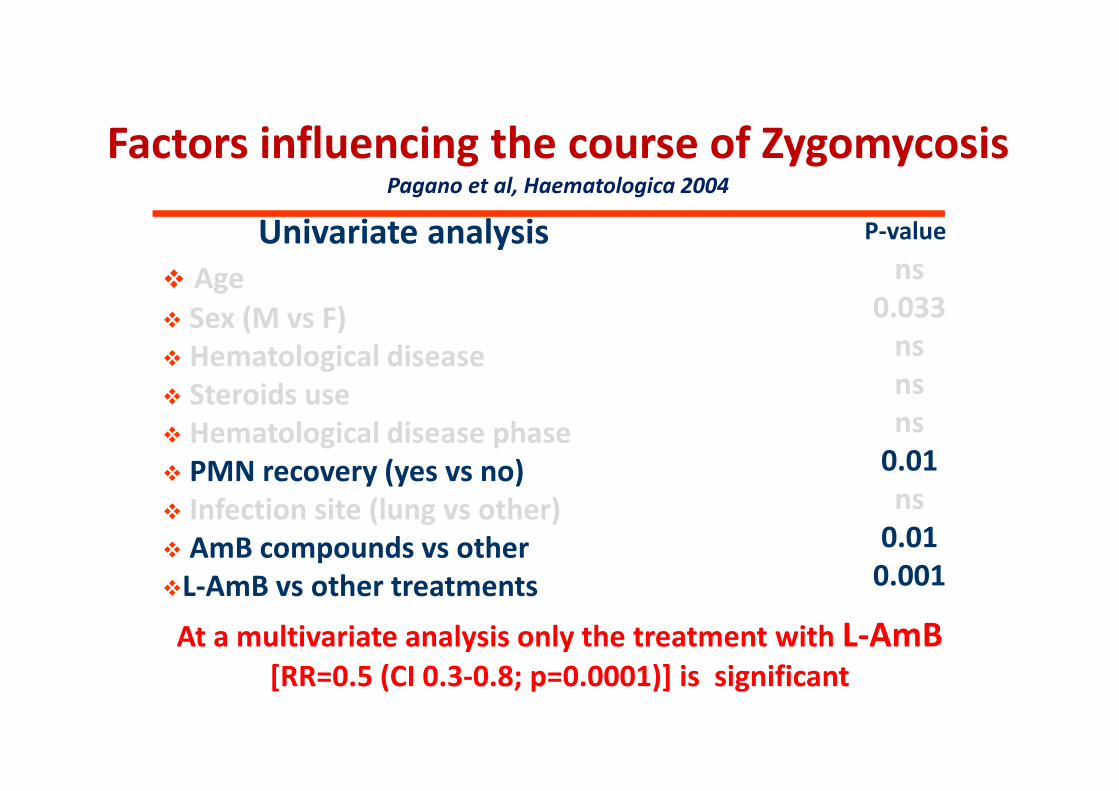
Factors influencing the course of ZygomycosisPagano et al, Haematologica 2004
Univariate analysis
Age
Sex (M vs F)
Hematological disease
Steroids use
Hematological disease phase
PMN recovery (yes vs no)
Infection site (lung vs other)
AmB compounds vs other
L-AmB vs other treatments
P-value
ns
0.033
ns
ns
ns
0.01
ns
0.01
0.001
At a multivariate analysis only the treatment with L-AmB[RR=0.5 (CI 0.3-0.8; p=0.0001)] is significant

How is the better dose of L-AmB ?
3 mg/kg ? (Pagano et al, Haematologica 2004)
3 → 5 mg/kg ? (Petrikkos et al, Eur J Clin Micr Infect Dis 2003)
7.5 →15 mg/kg ? (Walsh et al, AAC 2001)
Probably 6-7 mg/kg must be considered the better
dosage
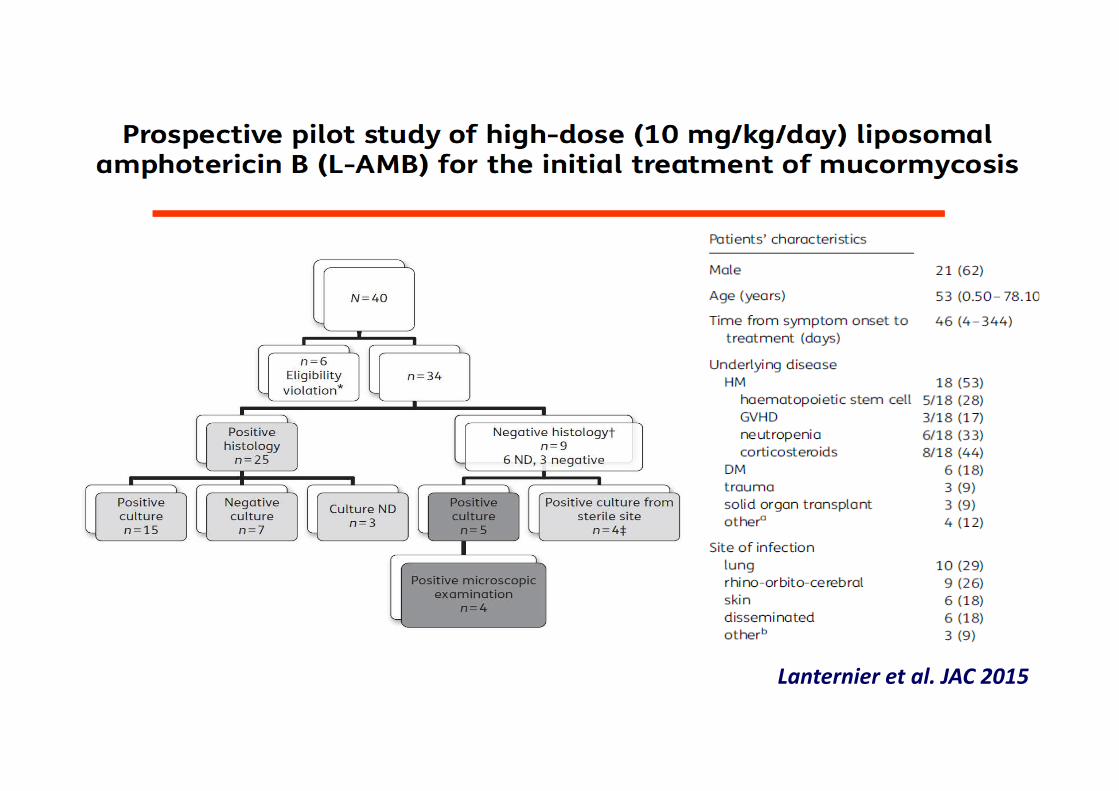
Lanternier et al. JAC 2015
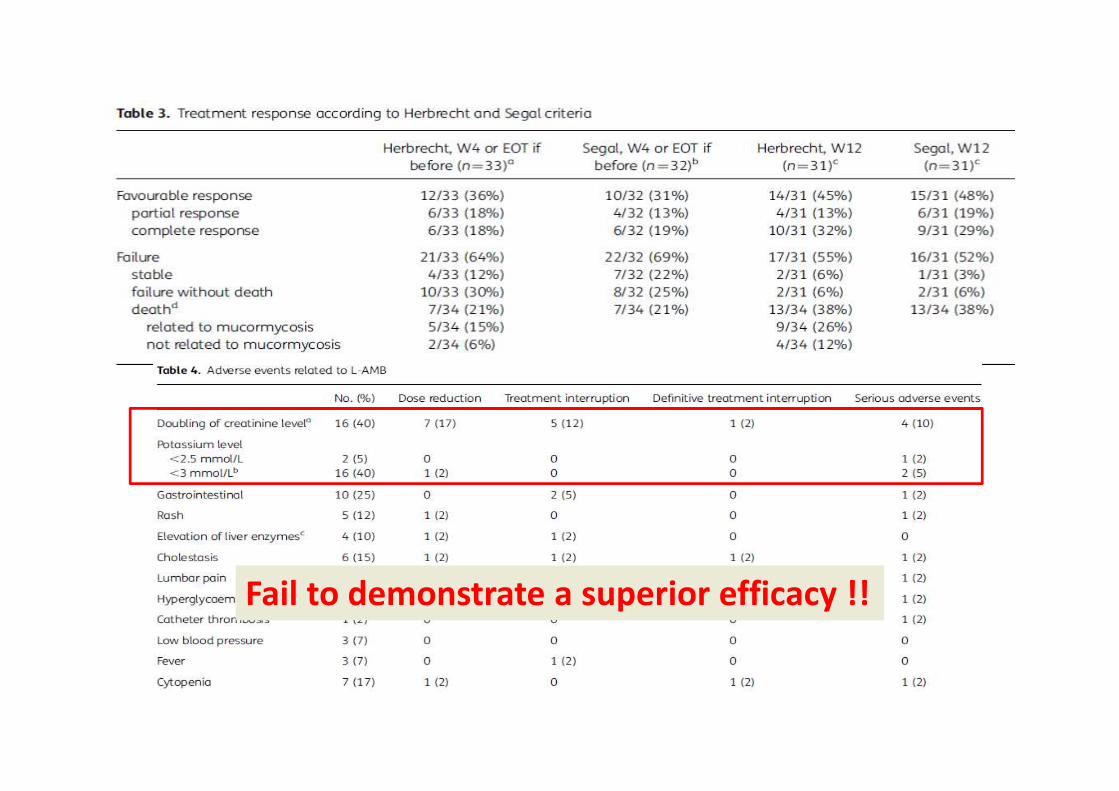
Fail to demonstrate a superior efficacy !!

Delaying > 6 days AMB-based therapy was
associated with a doubling in mortality
≤6, n=35
>6, n=35
48,6%82,9%
0%
20%
40%
60%
80%
100%
% m
ort
ality
at 12
weeks p=0.029, ≤6 days vs. >6 days
Chamilos et al. Clin Infect Dis 2008
0%
20%
40%
60%
80%
100%
0 5 10 15 20 25 30 35 40 45
Days from symptoms to initiation of appropriate therapy
Mort
ality
at 12 w
eeks
CART identified breakpoint

Posaconazole in the treatment of
proven/probable Mucormycosis
Van Burik et al, CID 2006Greenberg et al, AAC 2006
Patients: 24 Recovered: 19
79%
All refractory or resistant
11 rhino-CNS infection, 4 pneumonia
POS 800 mg/d (200 mg x4 o 400 mg x2)
Duration therapy ranged from 8 to 1004 d
Patients: 91 Recovered: 55
60%
All refractory or resistant
22 rhino-CNS infection, 37 pneumonia
POS 800 mg/d (200 mg x4 o 400 mg x2)
Duration therapy ranged from 6 to 1005 d
Two separate, but overlapping series of patients receiving posaconazole within compassionate use
protocols of the manufacturer have been published
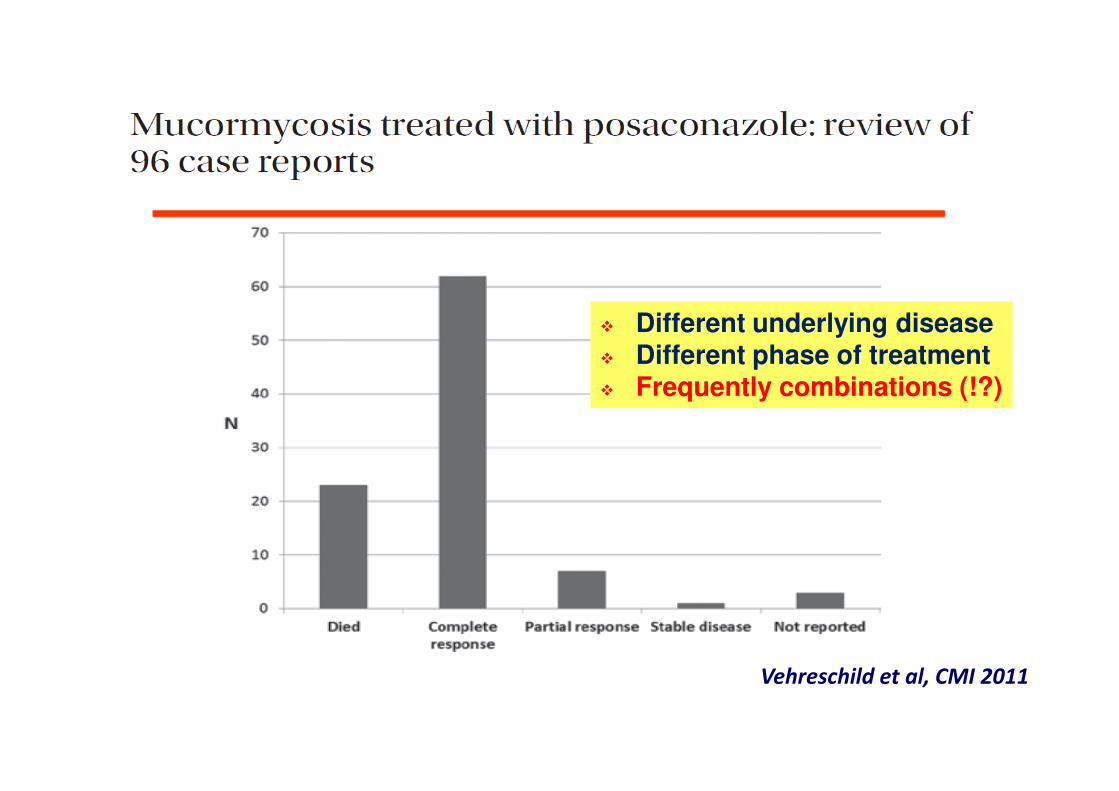
Vehreschild et al, CMI 2011
Different underlying disease Different phase of treatment Frequently combinations (!?)
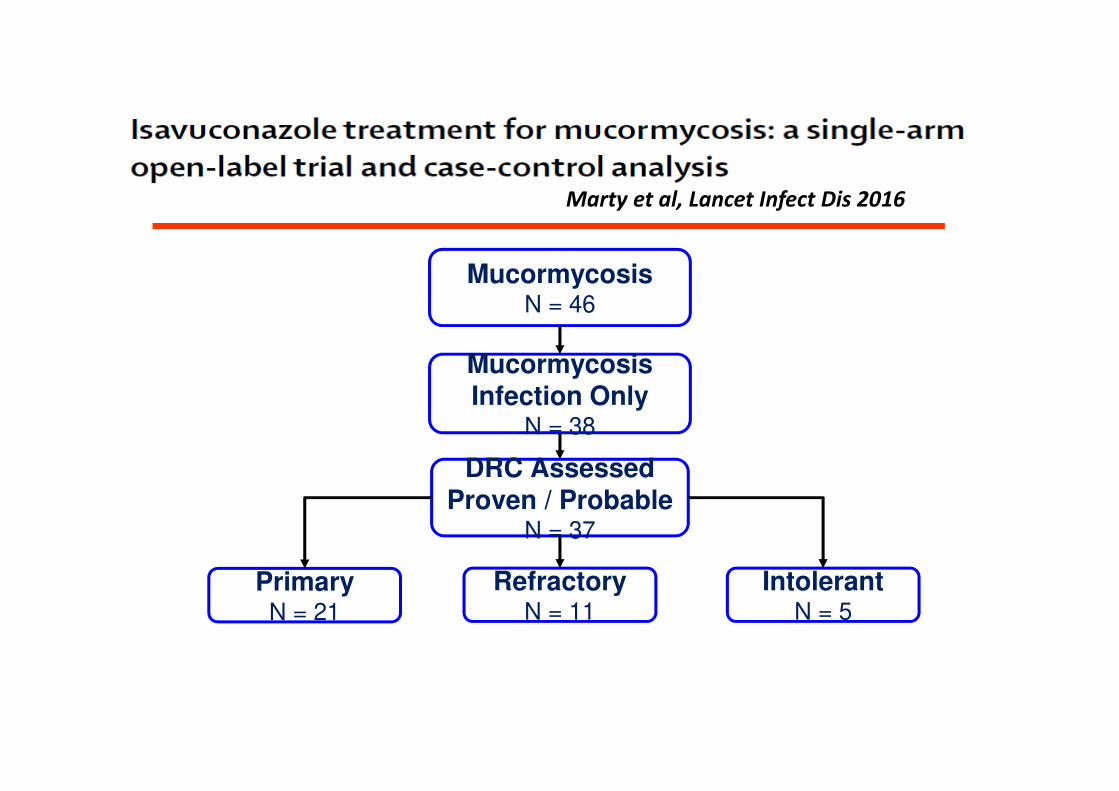
Mucormycosis Infection Only
N = 38
MucormycosisN = 46
DRC Assessed Proven / Probable
N = 37
IntolerantN = 5
RefractoryN = 11
PrimaryN = 21
Marty et al, Lancet Infect Dis 2016

Overall Response for Mucormycosis
Overall Response at EOT
Primary N = 21
%
RefractoryN = 11
%
IntolerantN = 5
%
Total N = 37
%
Success 31.6 36.4 20.0 31.4
Complete 15.8 18.2 0 14.3
Partial 15.8 18.2 20.0 17.1
Failure 68.4 63.6 80.0 68.6
Stable 31.6 18.2 40.0 28.6
Progression 36.8 45.5 40.0 40.0
WHY?
WHAT?
The mortality rate of mucormycosis with
monotherapy remains unacceptable
The proposed strategy should have shown:
1) Markedly improved survival in relevant animal
models of IM.
2) Available retrospective or observational clinical
data, concordant with preclinical models
3) Involvement of agents already approved for the
use in humans

Echinocandins:
Caspofungin
After the primary damage due to the others drug, penetrates into
the cell and block the glucan synthesis
Azoles:
Itraconazole
Posaconazole
Voriconazole
Antagonist of
ergosterol biosynthesis
Polyenes:
Amphotericin B
Lipid AmB
Nystatin
Act on cell membrane
integrity
Combination Therapy in mucormycosis:
Mechanism of interaction
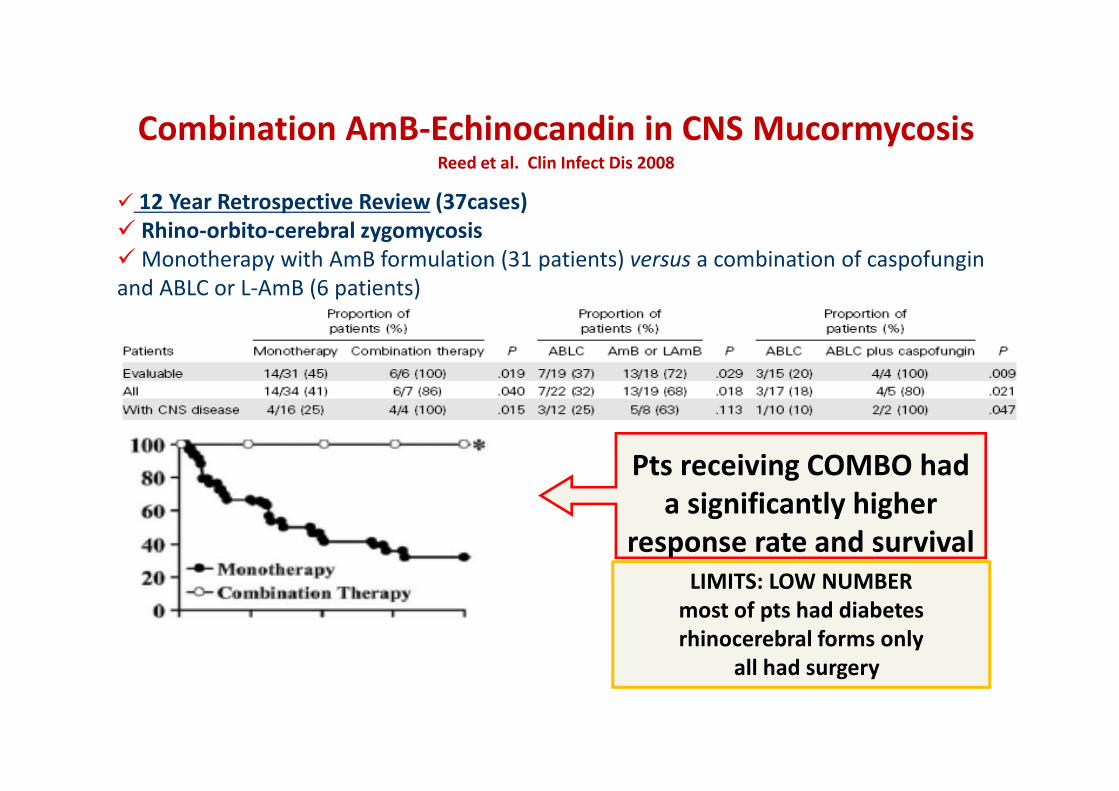
12 Year Retrospective Review (37cases)
Rhino-orbito-cerebral zygomycosis
Monotherapy with AmB formulation (31 patients) versus a combination of caspofungin
and ABLC or L-AmB (6 patients)
Pts receiving COMBO had
a significantly higher
response rate and survival
LIMITS: LOW NUMBER
most of pts had diabetes
rhinocerebral forms only
all had surgery
Combination AmB-Echinocandin in CNS Mucormycosis Reed et al. Clin Infect Dis 2008

Skiada et al, CMI 2011
34%
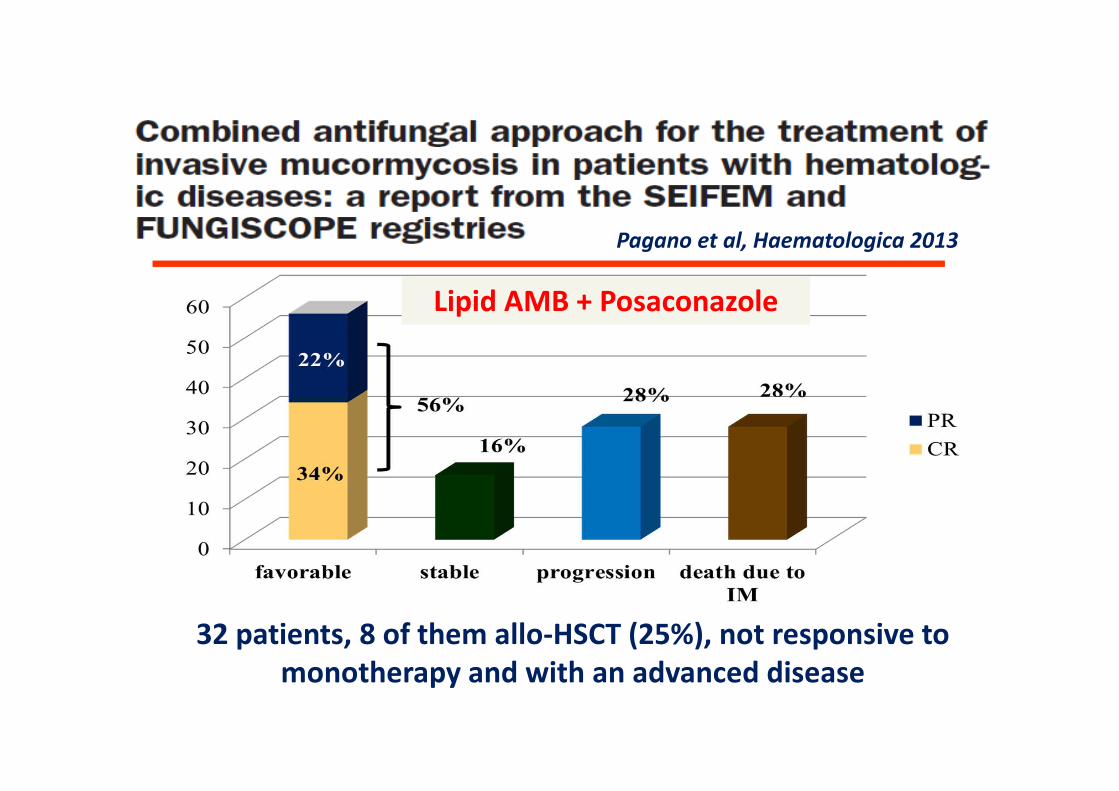
32 patients, 8 of them allo-HSCT (25%), not responsive to
monotherapy and with an advanced disease
Pagano et al, Haematologica 2013
Lipid AMB + Posaconazole
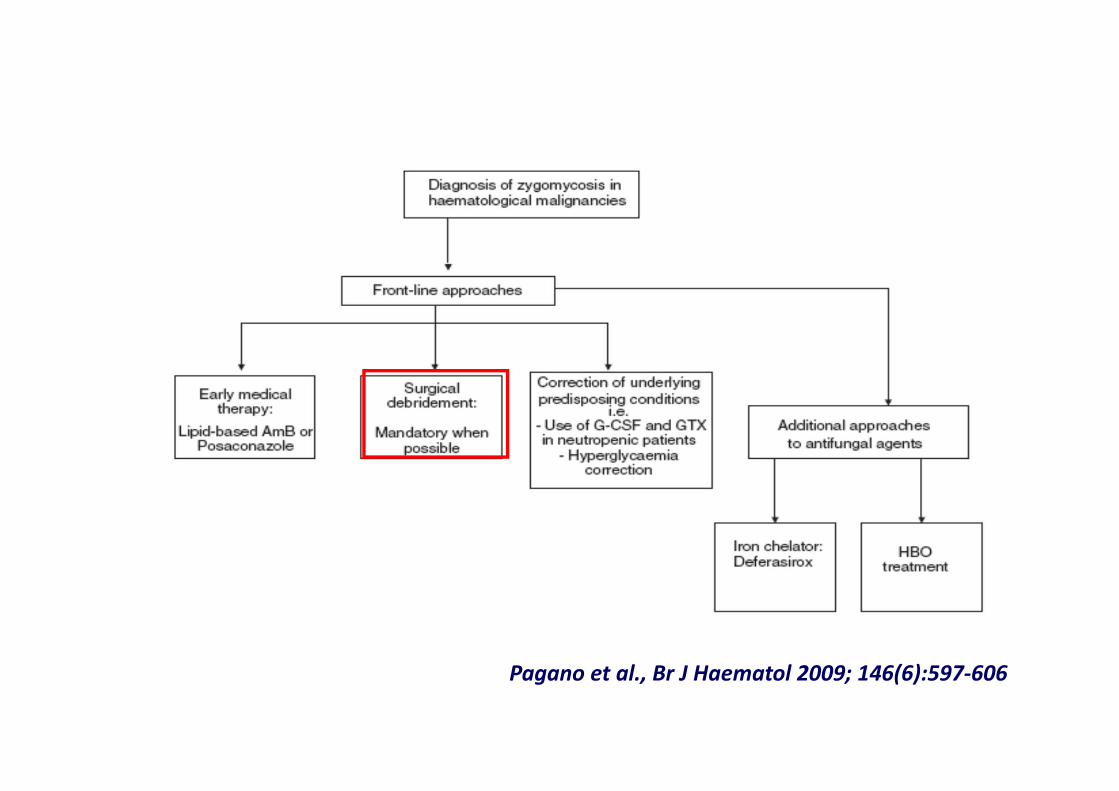
ALGORITMO NEL PAZIENTE EMATOLOGICO
Pagano et al., Br J Haematol 2009; 146(6):597-606
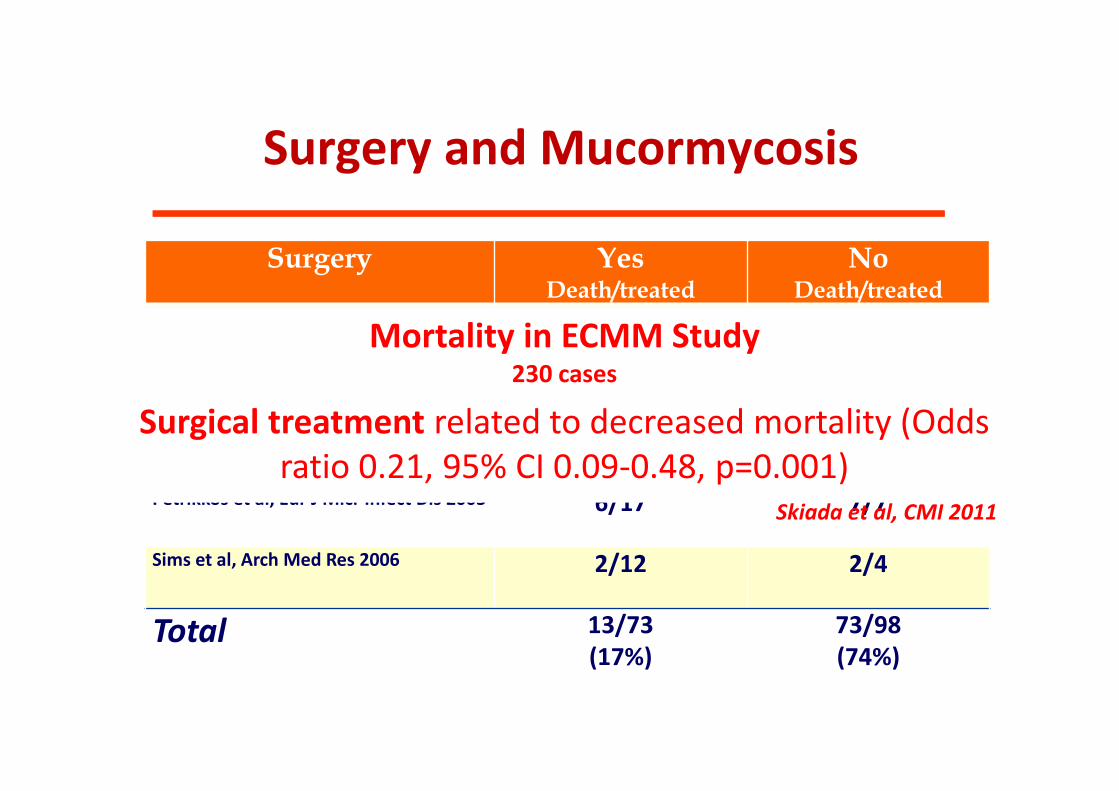
Surgery and Mucormycosis
Surgery YesDeath/treated
NoDeath/treated
Morrison et al,
BMT 19931/3 9/10
Tedder et al,
Leuk & Lymph 19944/36 38/56
Pagano et al,
Br J Haematol 19970/5 17/21
Petrikkos et al, Eur J Micr Infect Dis 2003 6/17 7/7
Sims et al, Arch Med Res 2006 2/12 2/4
Total 13/73
(17%)
73/98
(74%)
Mortality in ECMM Study230 cases
Surgical treatment related to decreased mortality (Odds
ratio 0.21, 95% CI 0.09-0.48, p=0.001)
Skiada et al, CMI 2011

ALGORITMO NEL PAZIENTE EMATOLOGICO
Pagano et al., Br J Haematol 2009; 146(6):597-606

Efficacy of growth factors or granulocyte
transfusion in MucormycosesDeaths Improved p-value
Pagano et al, Br J
Haematol 1997
7 2 n.s.
Kontoyiannis et al,
Clin Infect Dis 2000
5 7 n.s.
Roden et al *
CID 2005
3 15 n.r.
Pagano et al,
Haematologica
2004
9 9 n.s.
Kara et al,
Int J Clin Pract
2007
2 3 n.s.
ECMM-Italy 2008 4 4 n.s.
Deaths Improved
Kontoyiannis et al, *
Clin Infect Dis 2000
4 4
Gleisser et al, §Leuk & Lymph 2004
0 1
Mousset et al,**
Ann Hematol 2005
2 4
Roden et al, §CID 2005
5 2
Total 11 11
GTXG-CSF Failure !!

Saoulidis et al, CMI 2014

Lovastatin is able to induce apoptosis-like death of Mucor
racemosus (Roze et al Fungal Genet Biol 1998;25:119-33.)
Control + statin and D-eritro-sfingosin
Statins showed both in vitro and in vivo activity against
zygomycetes (Lukacs et al, J Clin Microbiol 2004;42:5400-2; Chamilos et al, Antimicrob
Agents Chemother 2006; 50:96-103 )

ALGORITMO NEL PAZIENTE EMATOLOGICO
Pagano et al., Br J Haematol 2009; 146(6):597-606

Hyperbaric Oxygen Therapy
Chamilos & Kontojiannis Clin Microbiol Infect 2005
N°28
Mean age 31 (0.5-74)
Underlying diseases
•Diabetes
•Trauma
•Others
17
5
6
Principal site: CNS 21
Post operative 23/25 (92%)
Median sesssion 22 (2-85)
Overall Survival 86%
Better outcome
24 sessions Vs. 6
p= 0.009
Cut-off 9 sessions p=0.003
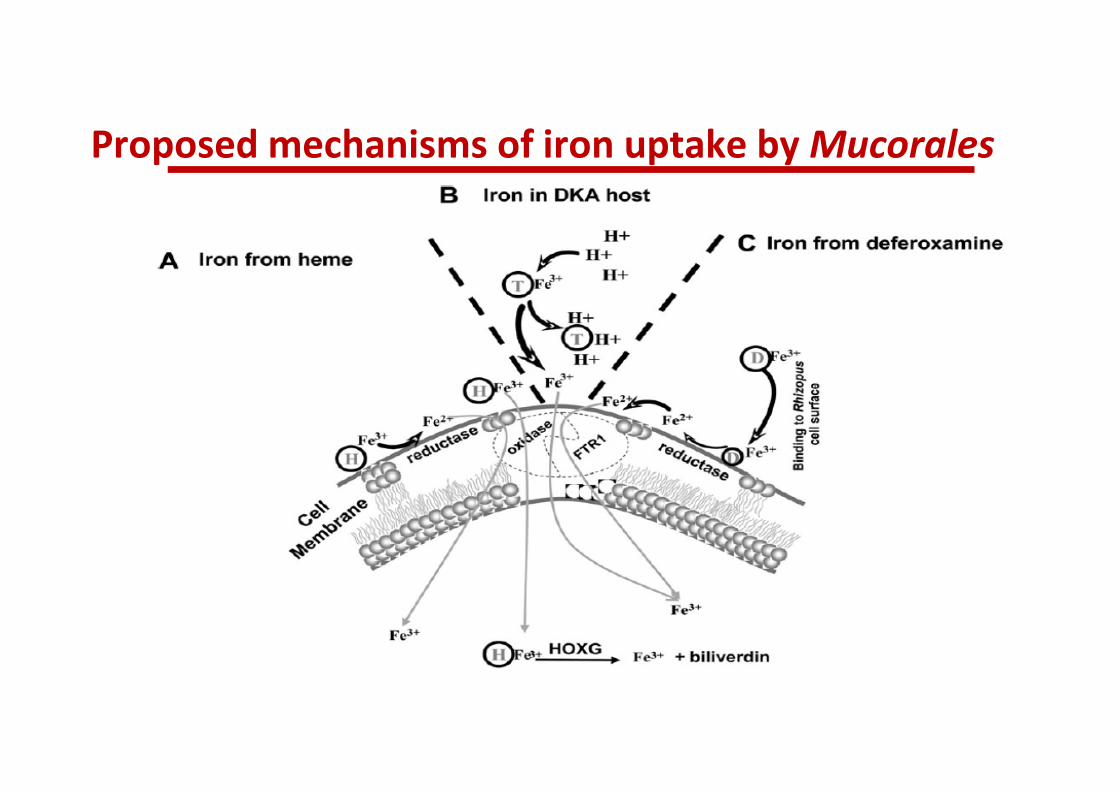
Proposed mechanisms of iron uptake by Mucorales

Risk
factors
Site of infection Antifungal agents outcome
Diabetes
SOT
Rhino-orbital-cerebral, lung, sinus, gastric
Lipid-AmB+ posaconazole
Lipid-AmB+echinocandin
monotherapy
5/8 cured
8 patients treated with combination therapy including
DFX at the dose of 15-20 mg/Kg
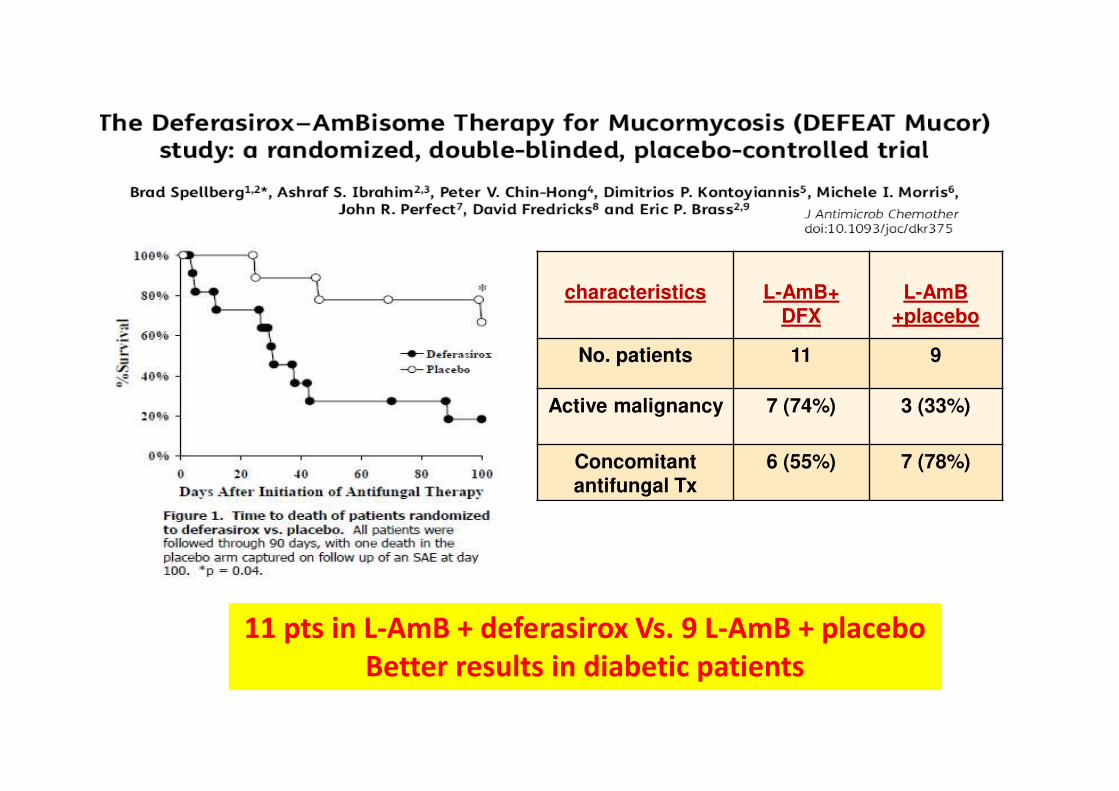
11 pts in L-AmB + deferasirox Vs. 9 L-AmB + placebo
Better results in diabetic patients
characteristics L-AmB+DFX
L-AmB +placebo
No. patients 11 9
Active malignancy 7 (74%) 3 (33%)
Concomitantantifungal Tx
6 (55%) 7 (78%)
2009







