Innovación terapéutica en cáncer de pulmón
Dr A. Artal
Hospital Universitario Miguel Servet
Zaragoza
INMUNOTERAPIA
NINTEDANIB

INMUNOTERAPIA
NINTEDANIB

Study Intervention Target PFS, months OS, months Primary
endpoint
ESCAPE1
(n=926)
CB/PTX/placebo CB/PTX/sorafenib
VEGFR-2, -3, PDGFR-ß, Flt-3,
b-RAF, c-kit
5.4 4.6
HR: 0.99 (0.84–1.16)
10.6 10.7
HR: 1.15 (0.94–1.41) OS
NExUS2
(n=772)
CIS/GEM/placebo CIS/GEM/sorafenib
5.5 6.0
HR: 0.83 (0.71–0.97)
12.5 12.4
HR: 0.98 (0.83–1.16) OS
ZEAL3
(n=534)
Pemetrexed/placebo Pemetrexed/vandetanib
VEGFR, EGFR, RET
2.8 4.1
HR: 0.86 (0.69–1.06)
9.2 10.5
HR: 0.86 (0.65–1.13) PFS
ZODIAC4
(n=1391)
Docetaxel/placebo Docetaxel/vandetanib
3.2 4.0
HR: 0.79 (0.70–0.90)
10.0 10.6
HR: 0.91 (0.78–1.07) PFS
SUN10875
(n=960)*
Erlotinib/placebo Erlotinib/sunitinib
VEGFR-1, -2, -3, PDGFR-ɑ, -ß,
Flt-3, c-kit
2.0 3.6
HR: 0.81 (0.70–0.94)
8.5 9.0
HR: 0.92 (0.80–1.07) OS
VITAL6 (n=913)
Docetaxel/placebo Docetaxel/aflibercept
VEGF-A, -B, PIGF
4.1 5.2
HR: 0.82 (0.72–0.94)
10.4 10.1
HR: 1.01 (0.87–1.17) OS
BETA7 (n=636)
Erlotinib/placebo Erlotinib/bevacizumab
VEGF-A 1.7 3.4
HR: 0.62 (0.52–0.75)
9.2 9.3
HR: 0.97 (0.80–1.18) OS
Fir
st
lin
e
Seco
nd
lin
e
*280 patients received >1 prior treatment lines. CB = carboplatin; PTX = paclitaxel; CIS = cisplatin; GEM = gemcitabine; OS = overall survival; PFS = progression-free survival; HR = hazard ratio;
VEGF = vascular endothelial growth factor receptor; PDGFR = platelet-derived growth factor receptor; RAF = rapidly accelerated fibrosarcoma; PIGF = placental growth factor receptor.
1. Scagliotti G, et al. J Clin Oncol 2010;28:1835–42; 2. Paz-Ares LG, et al. J Clin Oncol 2012;30:3084–92; 3. de Boer R, et al. J Clin Oncol 2011;29:1067–74; 4. Herbst R, et al. Lancet Oncol
2010;11:619–26; 5. Scagliotti GV, et al. J Clin Oncol 2012;30:2070–8; 6. Ramlau R, et al. J Clin Oncol 2012;30:3640–7; 7. Herbst R, et al. Lancet Oncol 2011;377:1846–54.
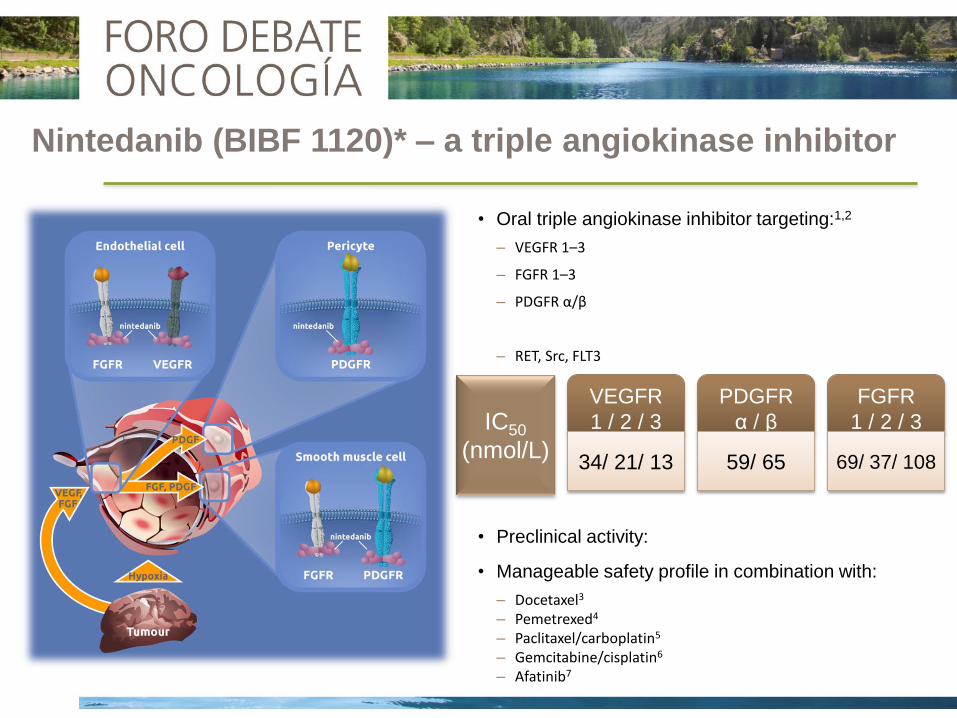
Nintedanib (BIBF 1120)* – a triple angiokinase inhibitor
• Oral triple angiokinase inhibitor targeting:1,2
– VEGFR 1–3
– FGFR 1–3
– PDGFR α/β
– RET, Src, FLT3
• Preclinical activity:
• Manageable safety profile in combination with:
– Docetaxel3
– Pemetrexed4
– Paclitaxel/carboplatin5
– Gemcitabine/cisplatin6
– Afatinib7
IC50
(nmol/L)
VEGFR
1 / 2 / 3
34/ 21/ 13
PDGFR
α / β
59/ 65
FGFR
1 / 2 / 3
69/ 37/ 108
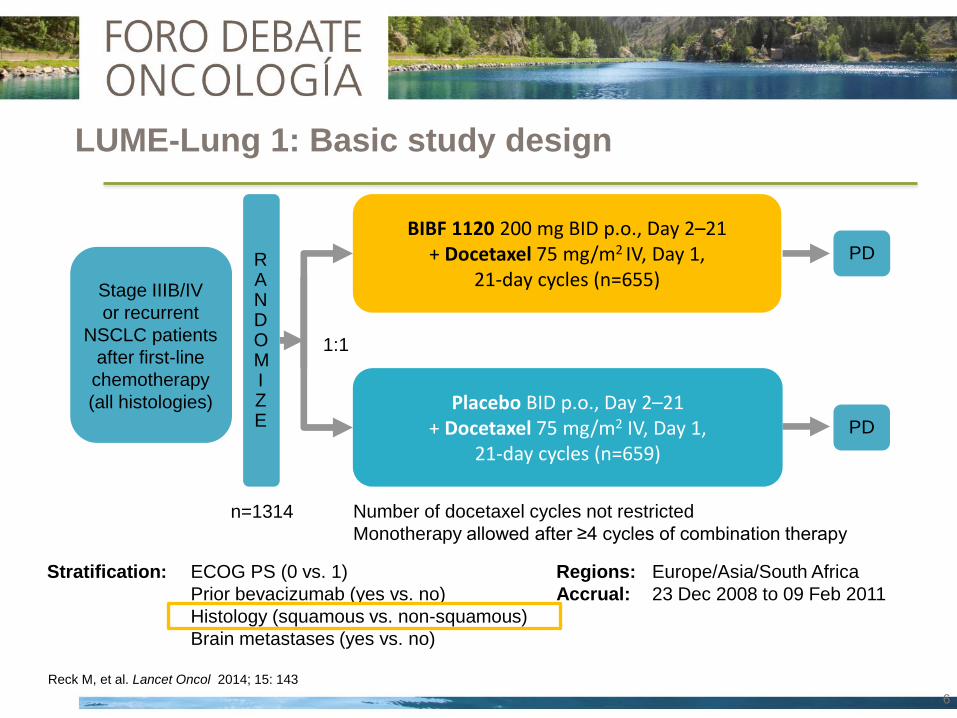
LUME-Lung 1: Basic study design
BIBF 1120 200 mg BID p.o., Day 2–21 + Docetaxel 75 mg/m2 IV, Day 1,
21-day cycles (n=655)
Placebo BID p.o., Day 2–21 + Docetaxel 75 mg/m2 IV, Day 1,
21-day cycles (n=659)
n=1314
RANDOMIZE
Stratification: ECOG PS (0 vs. 1)
Prior bevacizumab (yes vs. no)
Histology (squamous vs. non-squamous)
Brain metastases (yes vs. no)
Stage IIIB/IV
or recurrent
NSCLC patients
after first-line
chemotherapy
(all histologies)
1:1
PD
PD
Number of docetaxel cycles not restricted
Monotherapy allowed after ≥4 cycles of combination therapy
Regions: Europe/Asia/South Africa
Accrual: 23 Dec 2008 to 09 Feb 2011
Reck M, et al. Lancet Oncol 2014; 15: 143
6
Key Inclusion
• Histologically or cytologically confirmed, locally advanced and/or metastatic, stage
IIIB–IV or recurrent NSCLC
• All NSCLC histologies
• Failure after first-line chemotherapy (adjuvant /neoadjuvant allowed)
• ECOG PS 0 or 1
Key Exclusion
• Prior docetaxel or VEGF/VEGFR inhibitors (other than bevacizumab)
• Active brain metastases or leptomeningeal disease
• Centrally located tumours with radiographic evidence (CT or MRI) of local invasion
of major blood vessels or radiographic evidence of cavitary or necrotic tumours
• History of clinically significant hemoptysis within the past 3 months (greater than
one teaspoon of fresh blood per day)
Major Eligibility Criteria

LUME-Lung 1: Statistical design
Primary objective: PFS (centrally reviewed)
Secondary objectives: OS
PFS (investigator assessment)
Response rate
Safety analysis
PFS: 713 events HR 0.78, power 90%): 1300 patients (10% attrition)
Futility analysis with 50% of events
OS: 1151 deaths (HR 0.85, power 80%)
*Stratified for baseline ECOG PS , tumour histology, brain metastases and prior treatment with Bevacizumab.
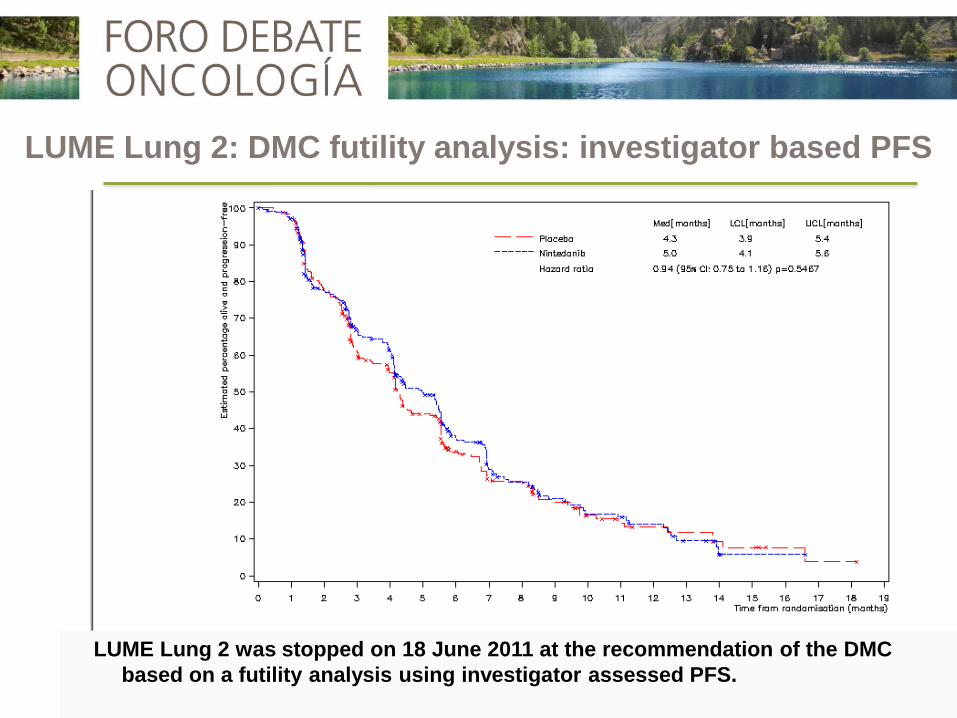
LUME Lung 2 was stopped on 18 June 2011 at the recommendation of the DMC
based on a futility analysis using investigator assessed PFS.
LUME Lung 2: DMC futility analysis: investigator based PFS

Baseline variables investigated for LUME Lung 1 + 2
Baseline variables
Race (Asian yes / no)*
Gender* (male / female)
Stage at diagnosis* (<IIIB/IV vs. IIIB vs. IV)
Age (<65 / ≥65 years)*
Smoking history* (ever smoked vs. never smoked)
Adrenal metastasis** (yes / no)
Liver metastasis* (yes / no)
Number of metastatic organs**
Therapy with bisphosphonates* (yes / no)
LDH level** (≤1 vs >1)
Best response to 1st line* (CR,PR,SD vs. PD vs. UNK )
Time since start of 1st line treatment * (continuous variable)
Stratification factors
ECOG performance score
Bevacizumab pre-treatment
Brain metastases at baseline
Tumour histology
* Pre-specified in the protocol or identified from
literature** as potential prognostic or predictive variable.
Kaiser R, et al. Eur J Cancer 2013; 49: 3479

OS Adenocarcinoma
T<9mo
Key secondary endpoint: OS • Stepwise testing
time since start of 1st line therapy (T) <9 months all adenocarcinoma all histologies
• 80% power*, HR 0.80
• Two sided stratified log-rank test, α=0.0494**
• Two-sided stratified log-rank test, α=0.05
Primary endpoint: Independently assessed PFS • All histologies
• 90% power after 713 PFS events, HR 0.78
Statistical Design
p<0.0494 p<0.0494 p<0.0494
1
2
Next analysis step only allowed if PFS confirmed
with all PFS events at time point of OS analysis
OS
OS
*Fixed-sequence order testing implemented prior to database lock to validate biomarker findings from independent study
LUME-Lung 2 (Hanna N, et al. ASCO 2013. Abstract #8034; Hanna N, et al. ESMO 2013. Abstract #3418;
Kaiser R, et al. ESMO 2013 Abstract #3479); Reck M, et al. Lancet Oncol 2014; 15: 143**Overall α=0.05
All adenocarcinoma All histologies

Patient characteristics
Nintedanib Placebo
Age 60 (53-67) 60 (54-66)
Gender (Male) % 72.7 72.7
PS 0/ 1 % 28.5/ 71.3 28.7/ 71.3
Never smoker % 25.2 24.4
Brain met. % 5.8 5.8
Squamous/ Adenoca % 42.1/ 49.2 42.3/ 51.0
Months 1st diagnosis 8.8 (5.4-13.6) 8.6 (5.4-13.6)
Prior platinum % 97.2 97.7
Prior bevacizumab % 4.1 3.5
Best response (CR/ PR/ SD) % 2.0/ 33.1/ 38.5 2.9/ 27.2/ 38.2
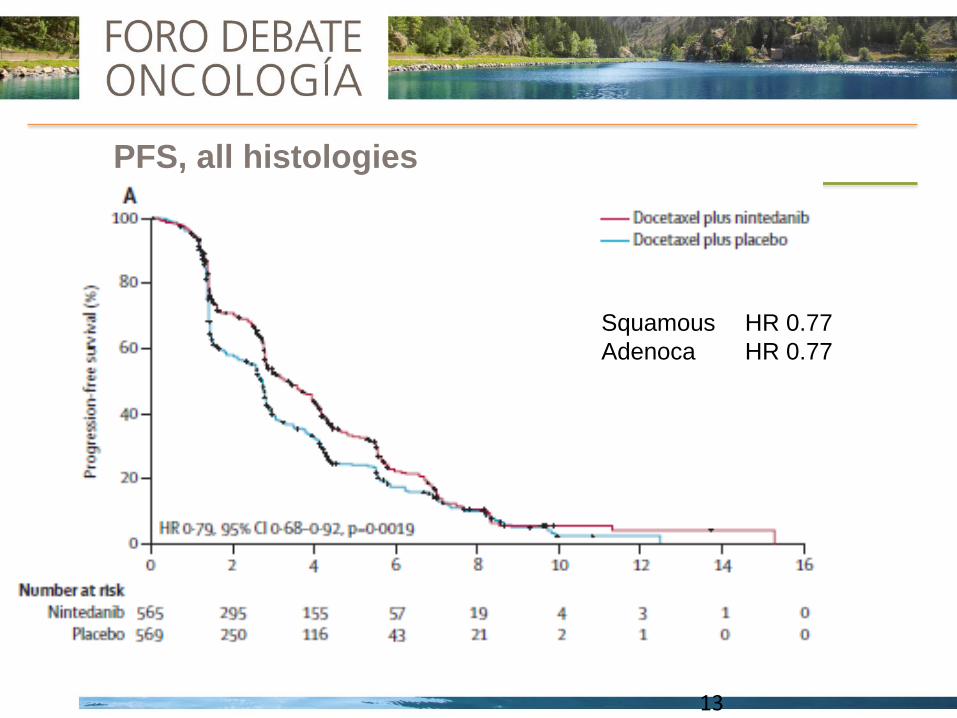
PFS, all histologies
13
Squamous HR 0.77
Adenoca HR 0.77
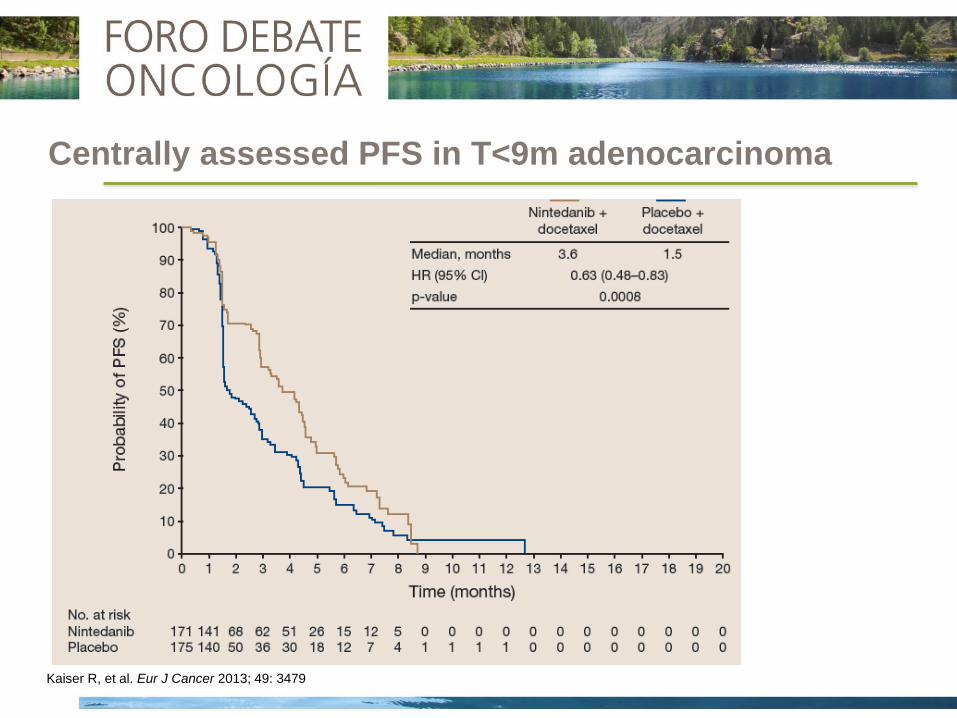
Centrally assessed PFS in T<9m adenocarcinoma
OS
Kaiser R, et al. Eur J Cancer 2013; 49: 3479
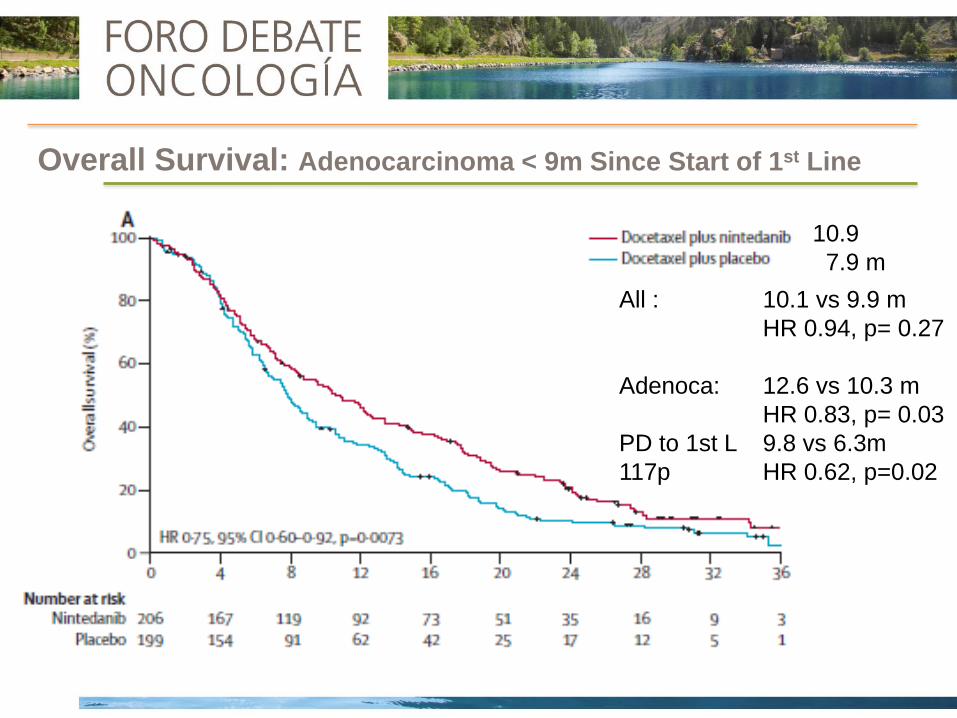
Overall Survival: Adenocarcinoma < 9m Since Start of 1st Line
All : 10.1 vs 9.9 m
HR 0.94, p= 0.27
Adenoca: 12.6 vs 10.3 m
HR 0.83, p= 0.03
PD to 1st L 9.8 vs 6.3m
117p HR 0.62, p=0.02
10.9
7.9 m
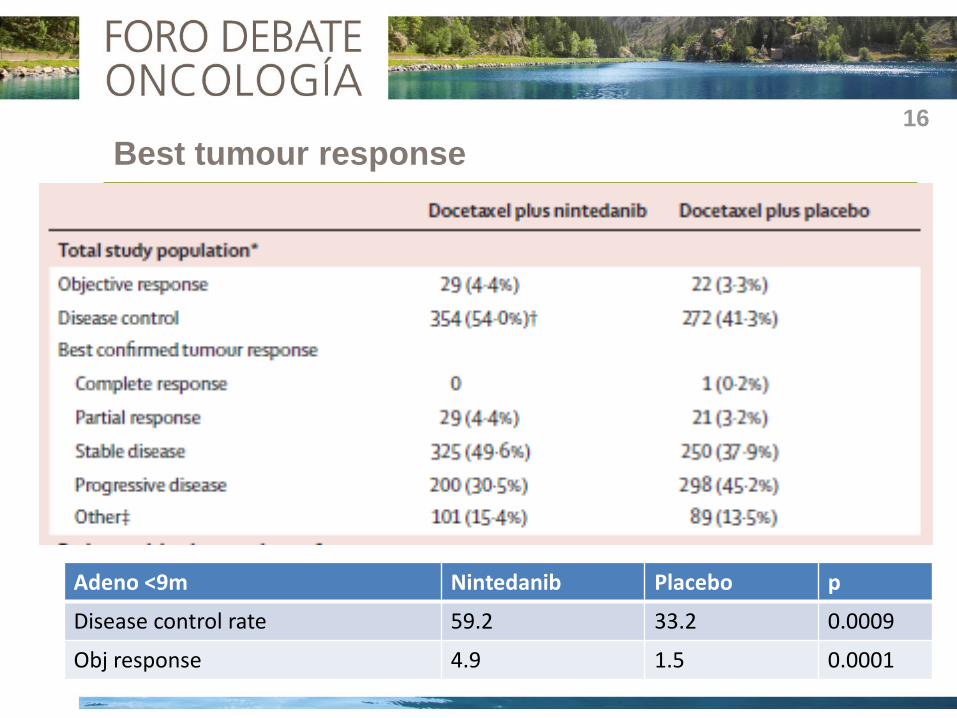
Best tumour response
Adenocarcinoma, T<9 months (n=405) 16
Adeno <9m Nintedanib Placebo p
Disease control rate 59.2 33.2 0.0009
Obj response 4.9 1.5 0.0001

Overall Survival: Adenocarcinoma Histology

Safety in All Treated Patients
45
40
35
30
25
20
15
10 5
0
Pati
en
ts (
%)
All CTCAE grades ≥15% incidence
CTCAE grades ≥3 ≥1% incidence
Nintedanib + docetaxel
Placebo + docetaxel
50
45
40
35
30
25
20
15
10 5
0
50
HBP, bleeding, intestinal perforation: No differences
First positive trial of a targeted agent in second line therapy of NSCLC
along with standard chemotherapy
LUME-Lung1 met its primary endpoint: PFS (HR 0.79, p=0.0019) in all
histologies
Nintedanib + Docetaxel significantly improved OS in adenocarcinoma
histology (HR 0.83, p=0.0359, median OS 10.3 to 12.6 m)
Patients with a poor prognosis (time since start of 1st line therapy <9
months) also experienced significant OS improvement
AEs with Nintedanib + Docetaxel were generally manageable with dose
reductions and symptomatic treatment
Summary
Absolute benefit was small, increased toxicity in a palliative setting,
absence of biomarkers

INMUNOTERAPIA
NINTEDANIB

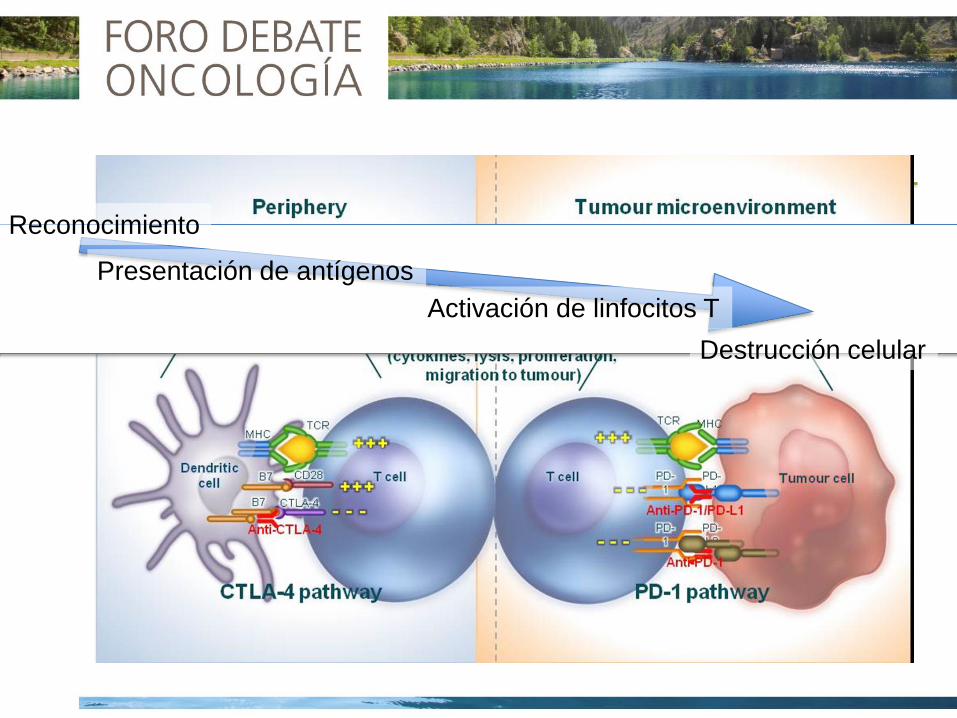
Reconocimiento
Presentación de antígenos
Activación de linfocitos T
Destrucción celular




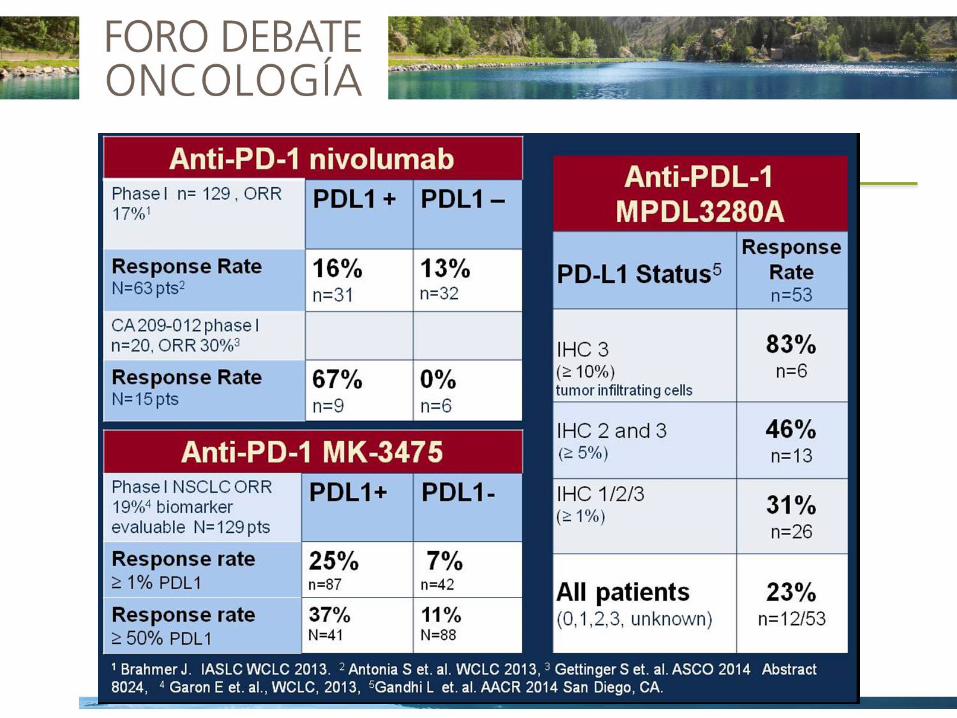
Anti- N RO (%) IrRO(%)
Nivolumab PD1 129 17.1 21.7
MK3475 PD1 221 15 21
MPDL3280A PD-L1 85 23 -
BMS936559 PD-L1 207 10 -
MEDI4736 PD-L1 26 15 -
Eficacia

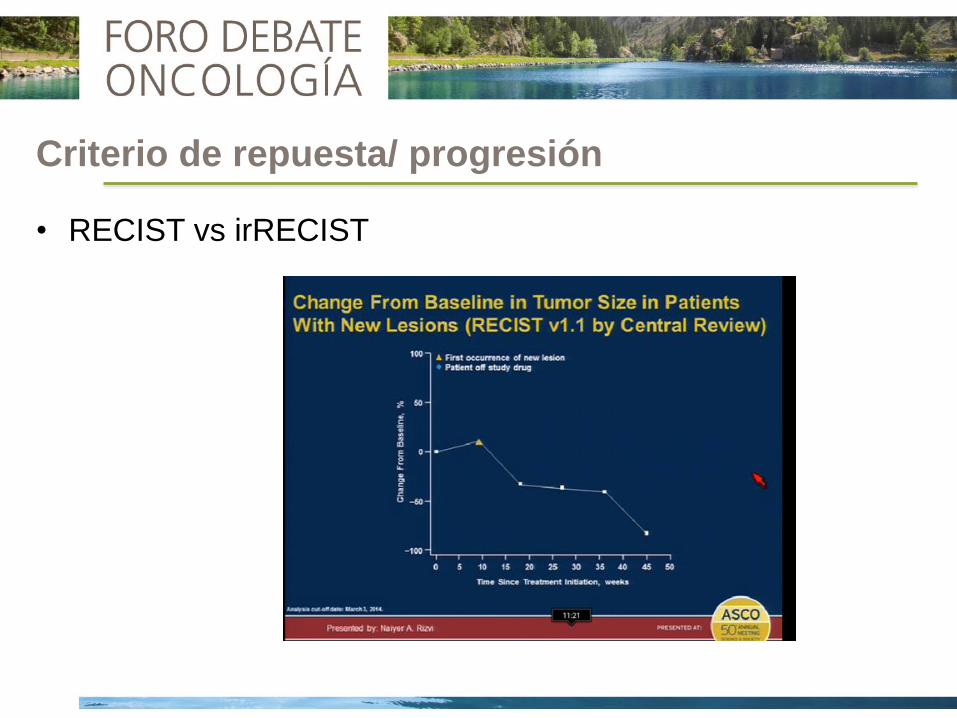
Criterio de repuesta/ progresión
• RECIST vs irRECIST

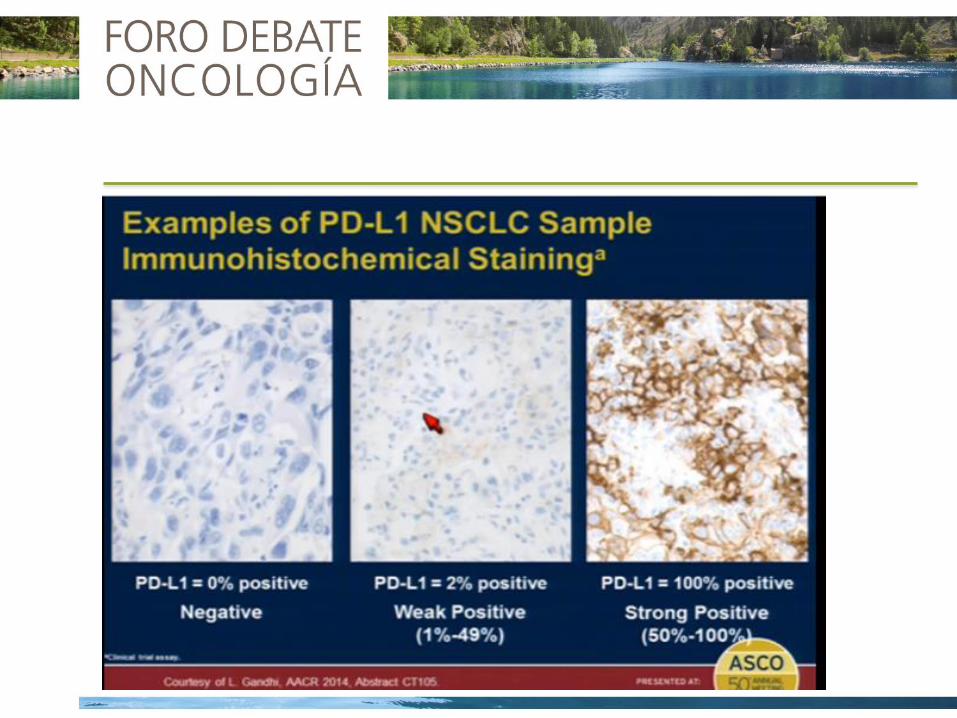

• Dificultad recuperación en FFPE
• Heterogeneidad tumoral
• Prevalencia
• Influencia de tratamientos previos
• Criterio de positividad (1/ 5/ 10/ 50%?)
• Positividad en céls. tumorales o linfocitos
• Diferentes pruebas (problemas metodológicos + intereses
comerciales)
Concordancia?
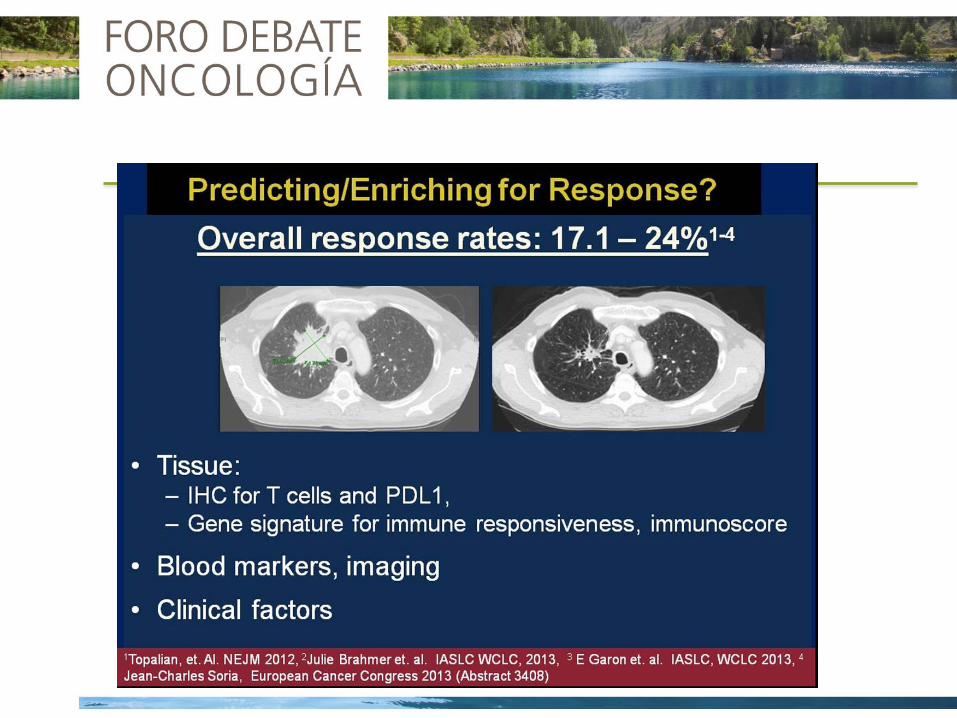
Respuestas en tumores PD-L1 negativo (8-15%)
PD-L1como biomarcador

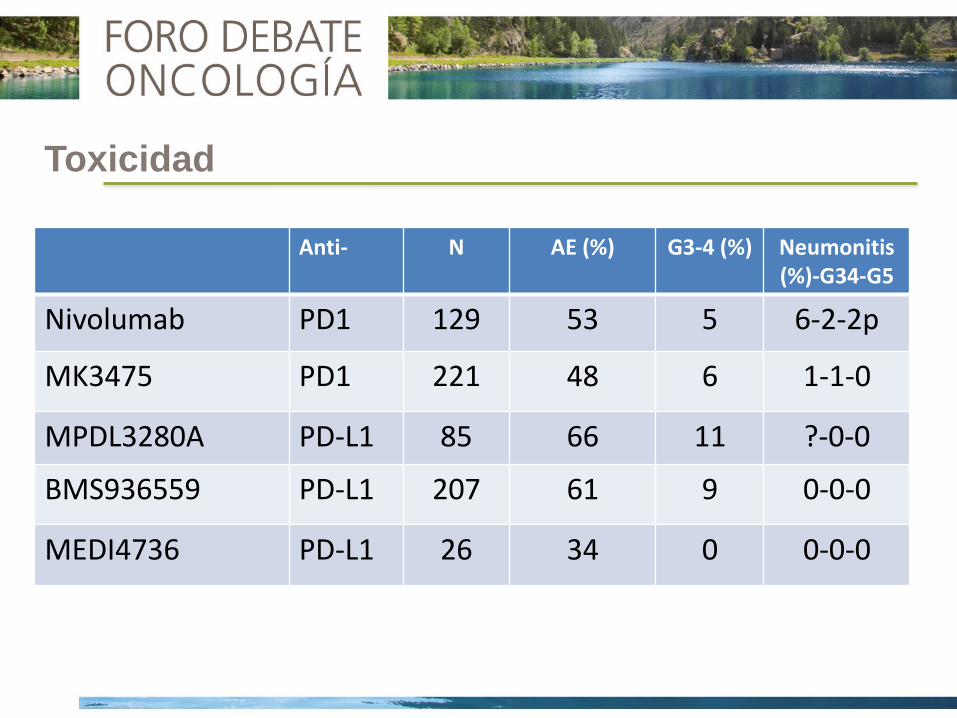
Toxicidad
Anti- N AE (%) G3-4 (%) Neumonitis (%)-G34-G5
Nivolumab PD1 129 53 5 6-2-2p
MK3475 PD1 221 48 6 1-1-0
MPDL3280A PD-L1 85 66 11 ?-0-0
BMS936559 PD-L1 207 61 9 0-0-0
MEDI4736 PD-L1 26 34 0 0-0-0
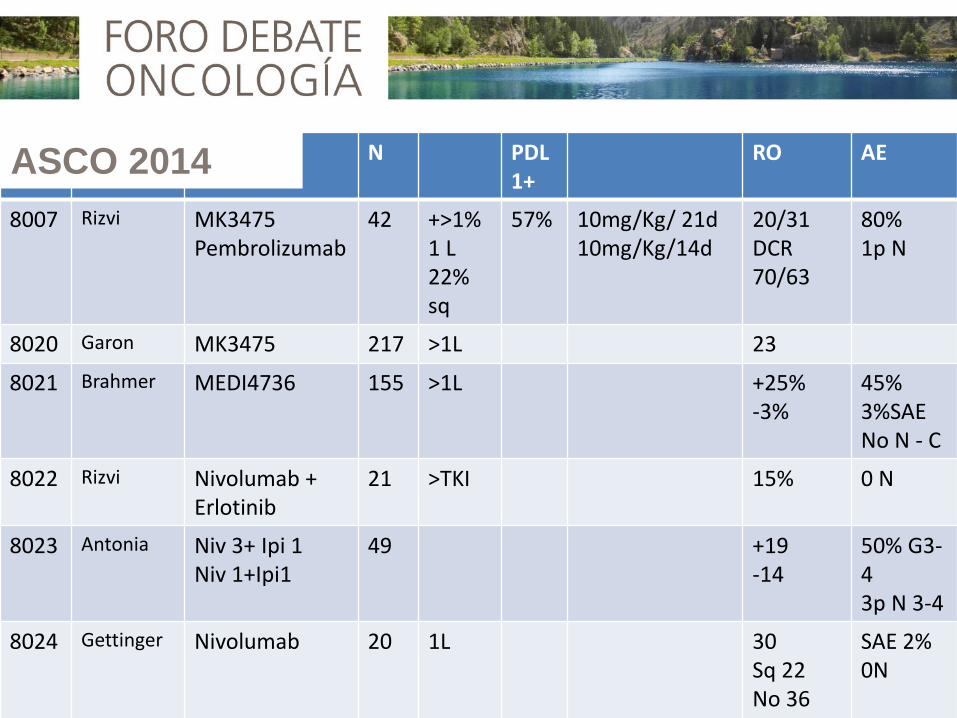
N PDL1+
RO AE
8007 Rizvi MK3475 Pembrolizumab
42 +>1% 1 L 22% sq
57% 10mg/Kg/ 21d 10mg/Kg/14d
20/31 DCR 70/63
80% 1p N
8020 Garon MK3475 217 >1L 23
8021 Brahmer MEDI4736 155 >1L +25% -3%
45% 3%SAE No N - C
8022 Rizvi Nivolumab + Erlotinib
21 >TKI 15% 0 N
8023 Antonia Niv 3+ Ipi 1 Niv 1+Ipi1
49 +19 -14
50% G3-4 3p N 3-4
8024 Gettinger Nivolumab 20 1L 30 Sq 22 No 36 +50, -0%
SAE 2% 0N
ASCO 2014
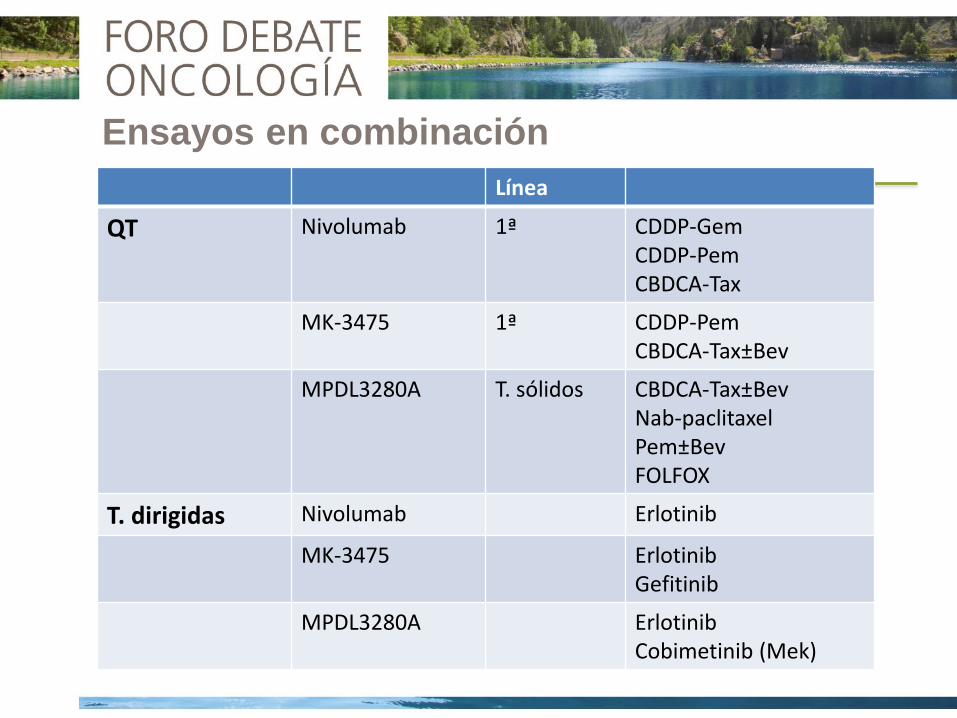
Ensayos en combinación
Línea
QT Nivolumab 1ª CDDP-Gem CDDP-Pem CBDCA-Tax
MK-3475 1ª CDDP-Pem CBDCA-Tax±Bev
MPDL3280A T. sólidos CBDCA-Tax±Bev Nab-paclitaxel Pem±Bev FOLFOX
T. dirigidas Nivolumab Erlotinib
MK-3475 Erlotinib Gefitinib
MPDL3280A Erlotinib Cobimetinib (Mek)
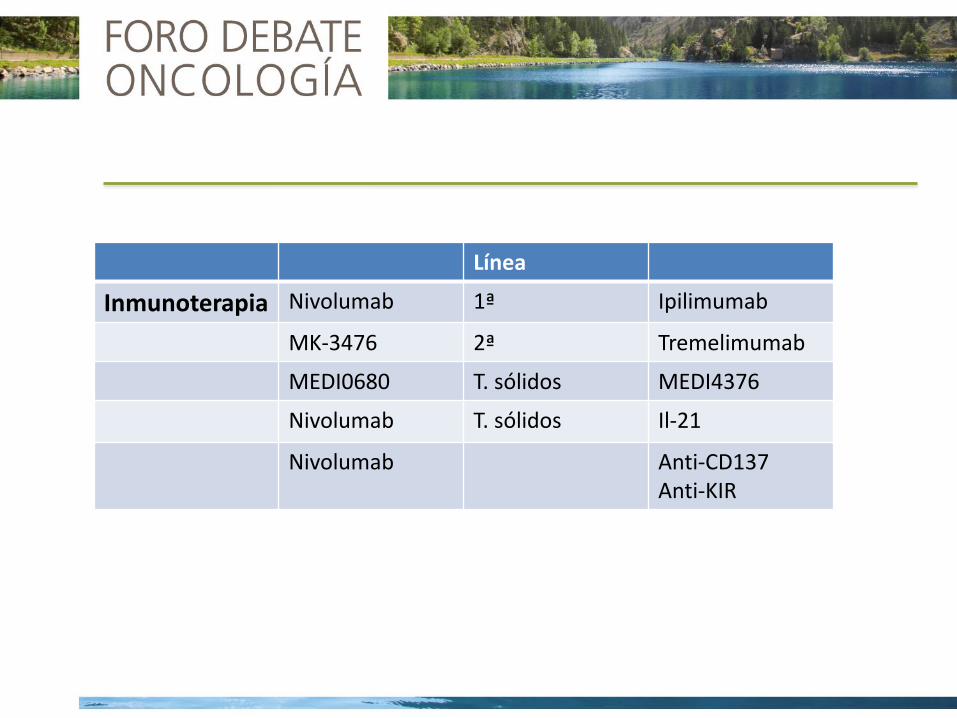
Línea
Inmunoterapia Nivolumab 1ª Ipilimumab
MK-3476 2ª Tremelimumab
MEDI0680 T. sólidos MEDI4376
Nivolumab T. sólidos Il-21
Nivolumab Anti-CD137 Anti-KIR
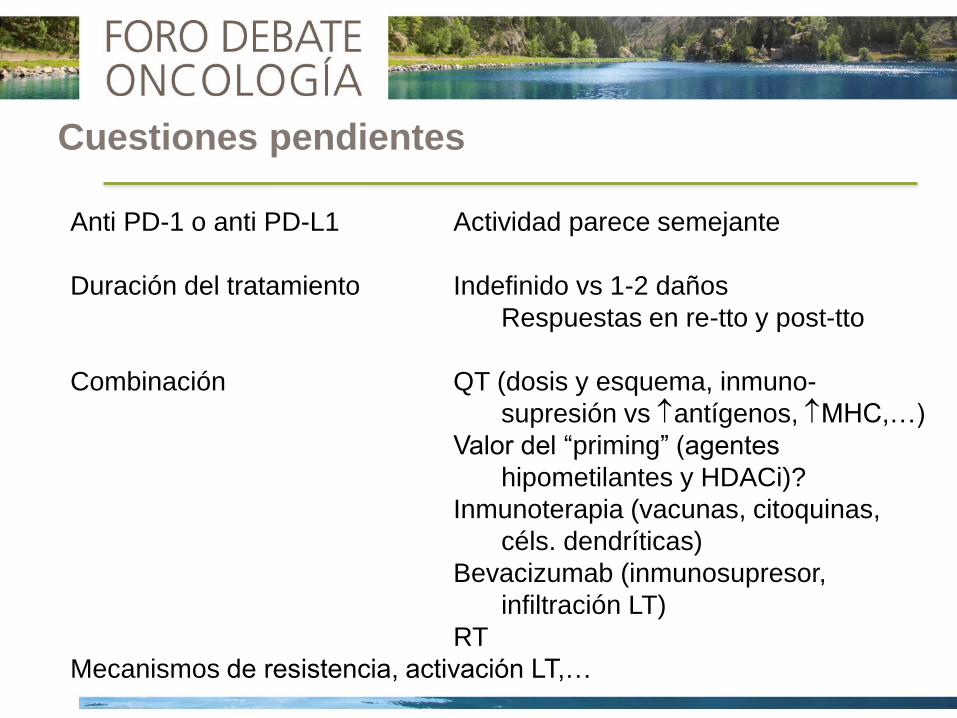
Cuestiones pendientes
Anti PD-1 o anti PD-L1 Actividad parece semejante
Duración del tratamiento Indefinido vs 1-2 daños
Respuestas en re-tto y post-tto
Combinación QT (dosis y esquema, inmuno-
supresión vs antígenos, MHC,…)
Valor del “priming” (agentes
hipometilantes y HDACi)?
Inmunoterapia (vacunas, citoquinas,
céls. dendríticas)
Bevacizumab (inmunosupresor,
infiltración LT)
RT
Mecanismos de resistencia, activación LT,…