dislipidemia, el otro secuaz - ace · dm enfermedad cardiovascular erc paciente > 40 años de...
TRANSCRIPT

Dislipidemia, el otro secuaz
DR LUIS FERNANDO DURAN
MEDICO INTERNISTA
JEFE DEL DEPARTAMENTO MEDICINA INTERNA, HOSPITAL UNIVERSITARIO DE NEIVA
DOCENTE MEDICINA INTERNA, UNIVERSIDAD SURCOLOMBIANA
Aspectos generales
Enfermedad cardiovascular produce mas de 4 millones de muertes al año
en Europa
Muertes en mujeres > hombres. Aunque < 65 años mueren mas los
hombres por enfermedad cardiovascular.
Hay mas pacientes que sobreviven a un evento cardiovascular con alto
riesgo de recurrencia por el incremento en los factores de riesgo CV.
La prevención es efectiva en reducir el impacto de la enfermedad
cardiovascular
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
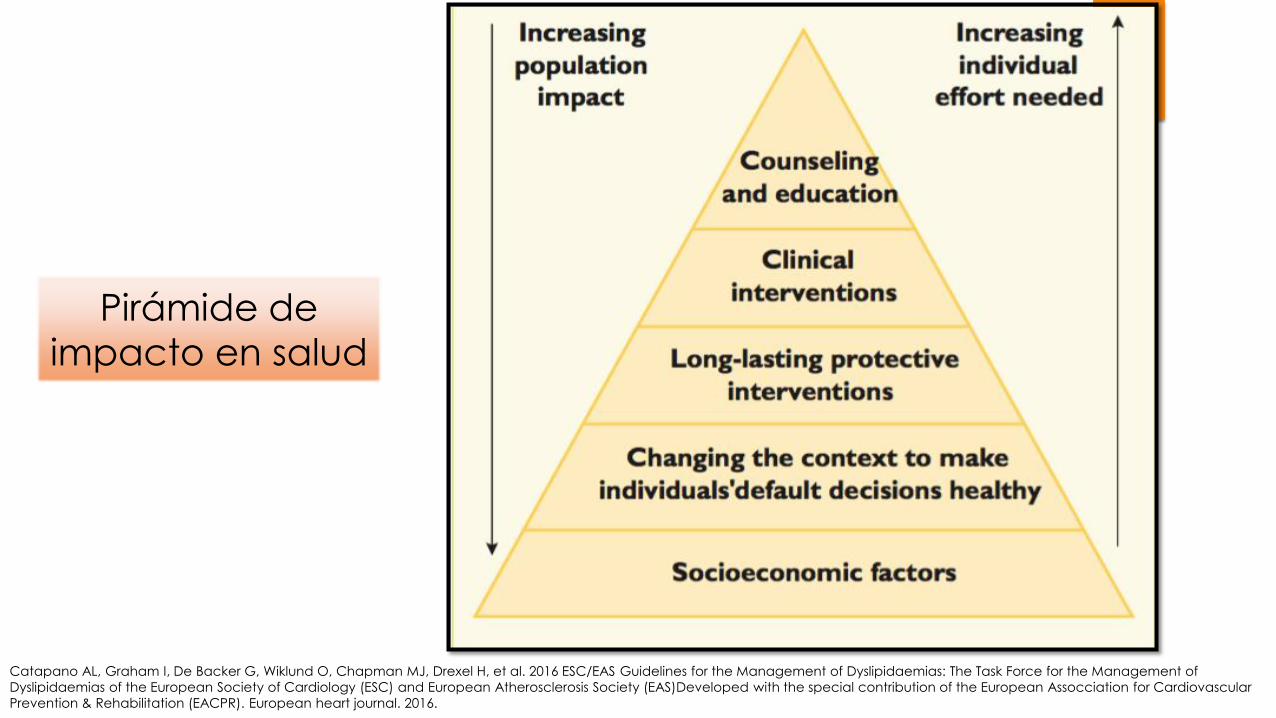
Pirámide de
impacto en salud
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
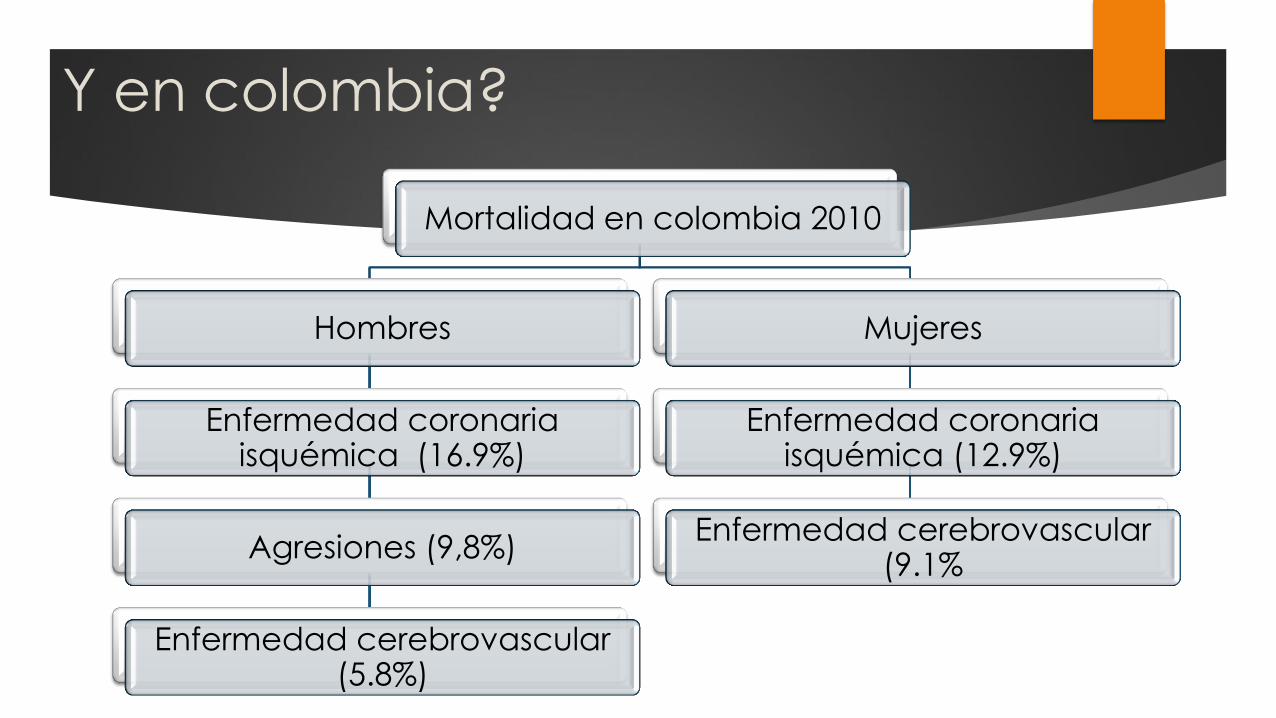
Y en colombia?
Mortalidad en colombia 2010
Hombres
Enfermedad coronaria isquémica (16.9%)
Agresiones (9,8%)
Enfermedad cerebrovascular (5.8%)
Mujeres
Enfermedad coronaria isquémica (12.9%)
Enfermedad cerebrovascular (9.1%
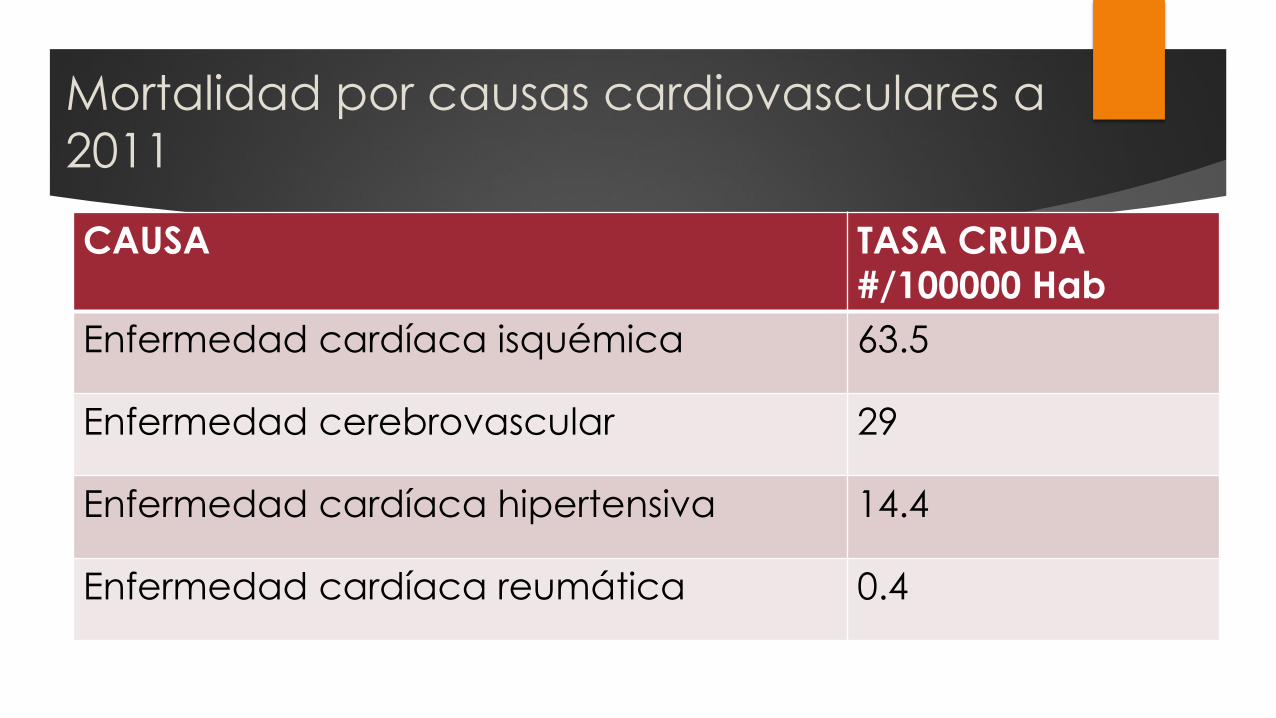
Mortalidad por causas cardiovasculares a
2011
CAUSA TASA CRUDA
#/100000 Hab
Enfermedad cardíaca isquémica 63.5
Enfermedad cerebrovascular 29
Enfermedad cardíaca hipertensiva 14.4
Enfermedad cardíaca reumática 0.4

Etiología de las dislipidemias
Trastornos genéticos
Hipercolesterolemia familar homocigota-heterocigota
Hiperlipidemia familiar combinada,
Hipertrigliceridemia familiar
Hipoalfalipoproteinemia genética
Trastornos secundarios adquiridos (40-50%)
Obesidad
Resistencia a la insulina
Hipotiroidismo
DM
Sedentarismo
Tabaquismo
Medicamentos (P ej Tto VIH)
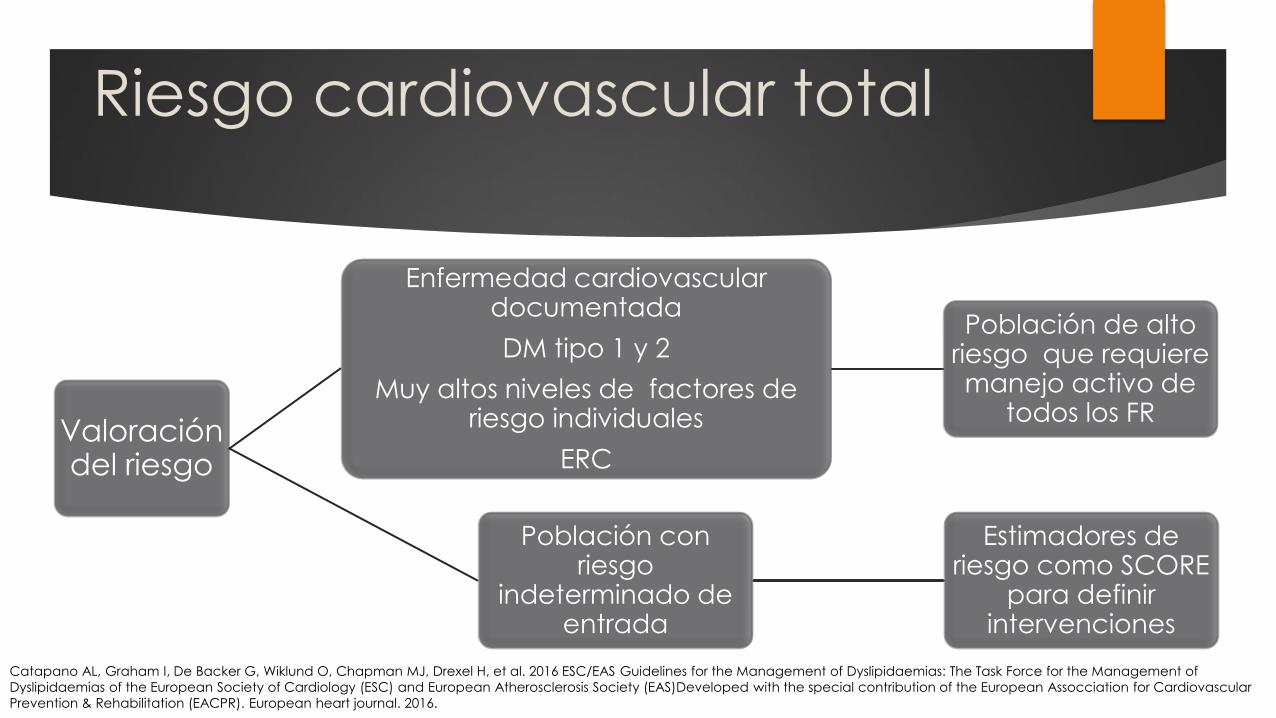
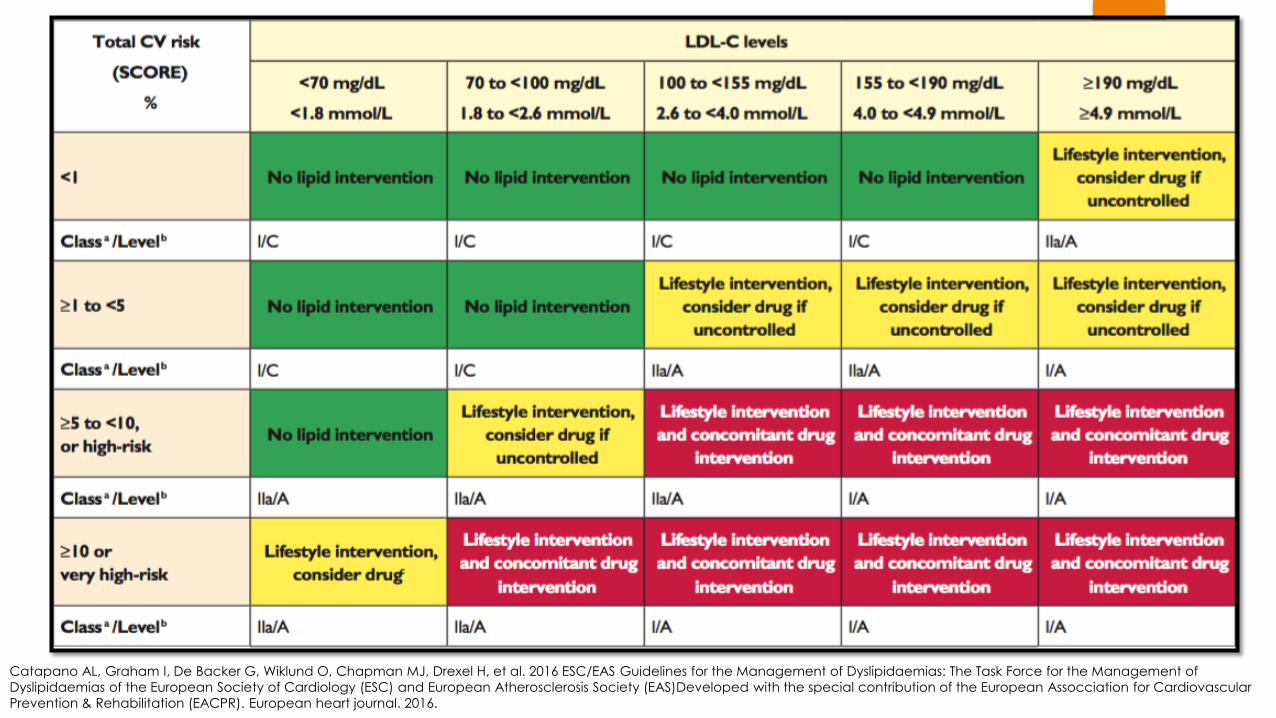
Riesgo cardiovascular total
Valoración del riesgo
Enfermedad cardiovascular documentada
DM tipo 1 y 2
Muy altos niveles de factores de riesgo individuales
ERC
Población de alto riesgo que requiere manejo activo de
todos los FR
Población con riesgo
indeterminado de entrada
Estimadores de riesgo como SCORE
para definir intervenciones
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
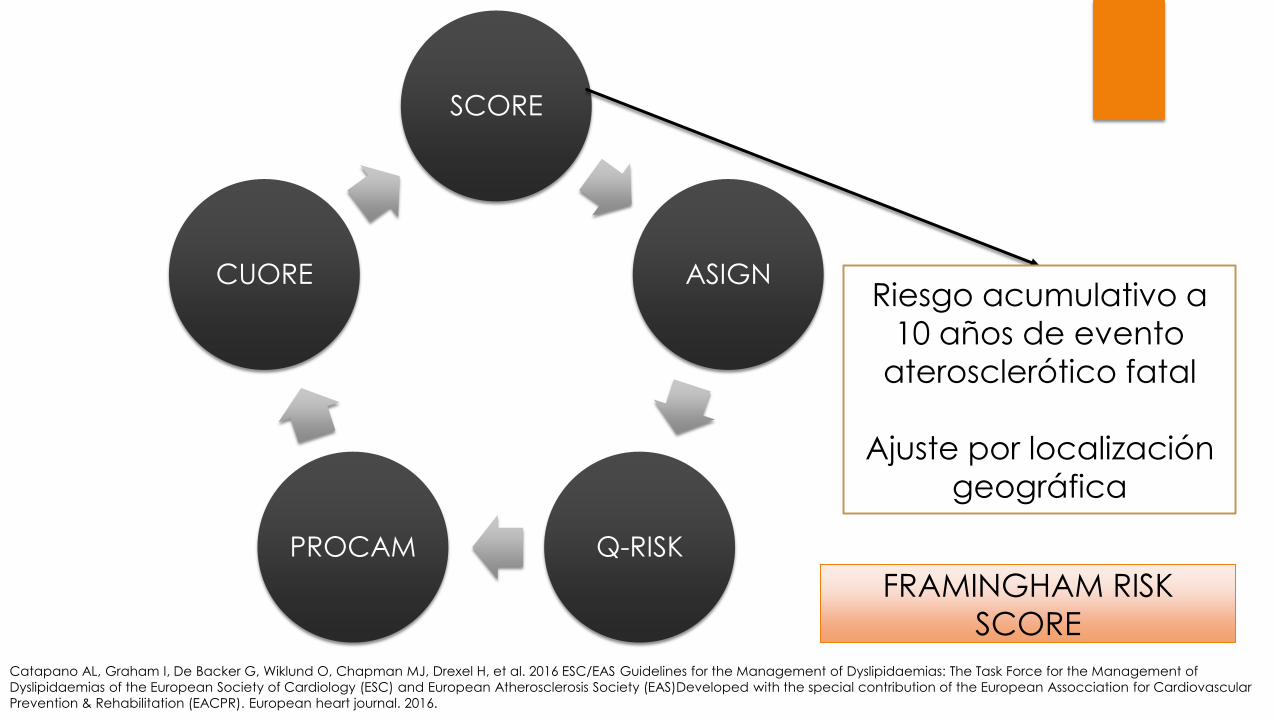
SCORE
ASIGN
Q-RISK PROCAM
CUORE Riesgo acumulativo a
10 años de evento
aterosclerótico fatal
Ajuste por localización
geográfica
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
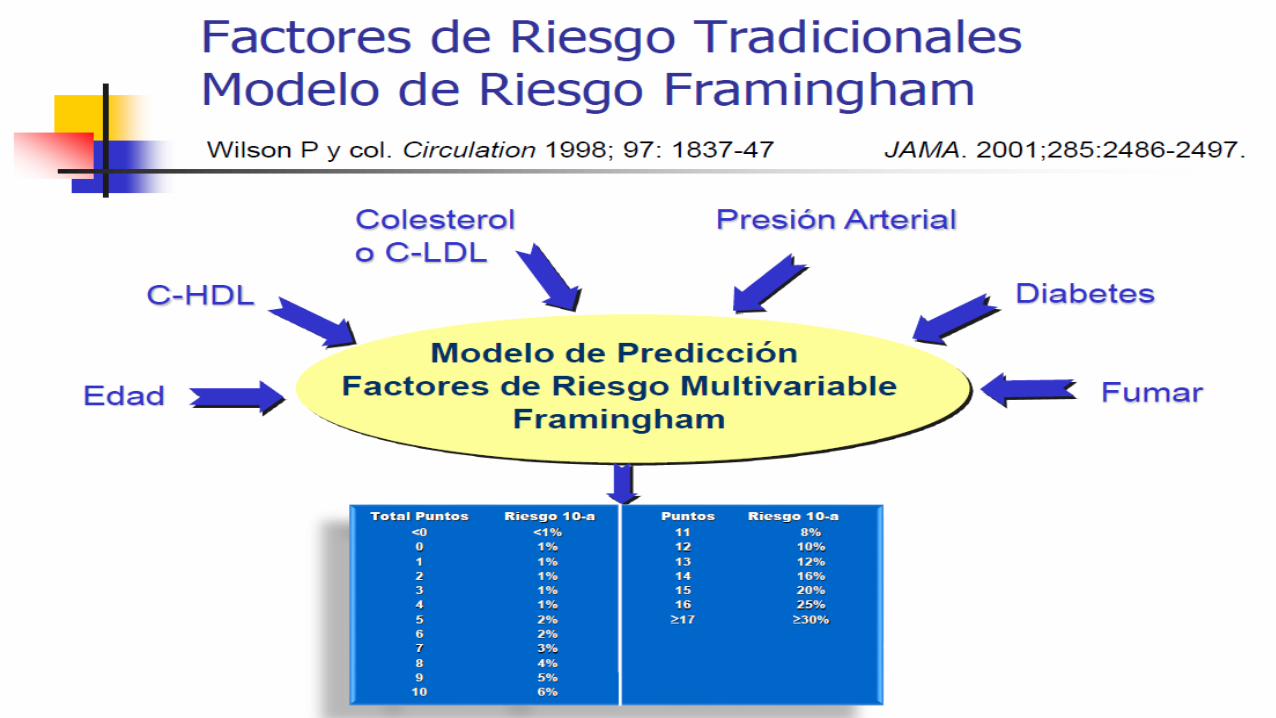
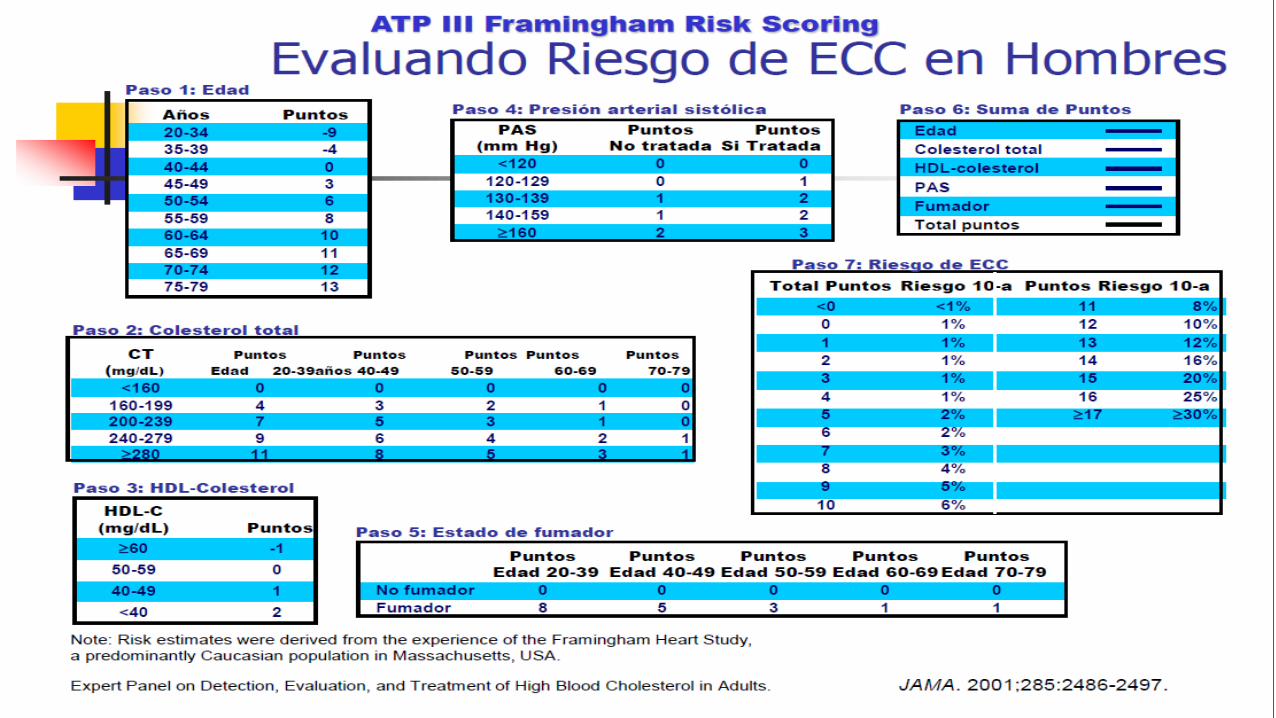
FRAMINGHAM RISK
SCORE
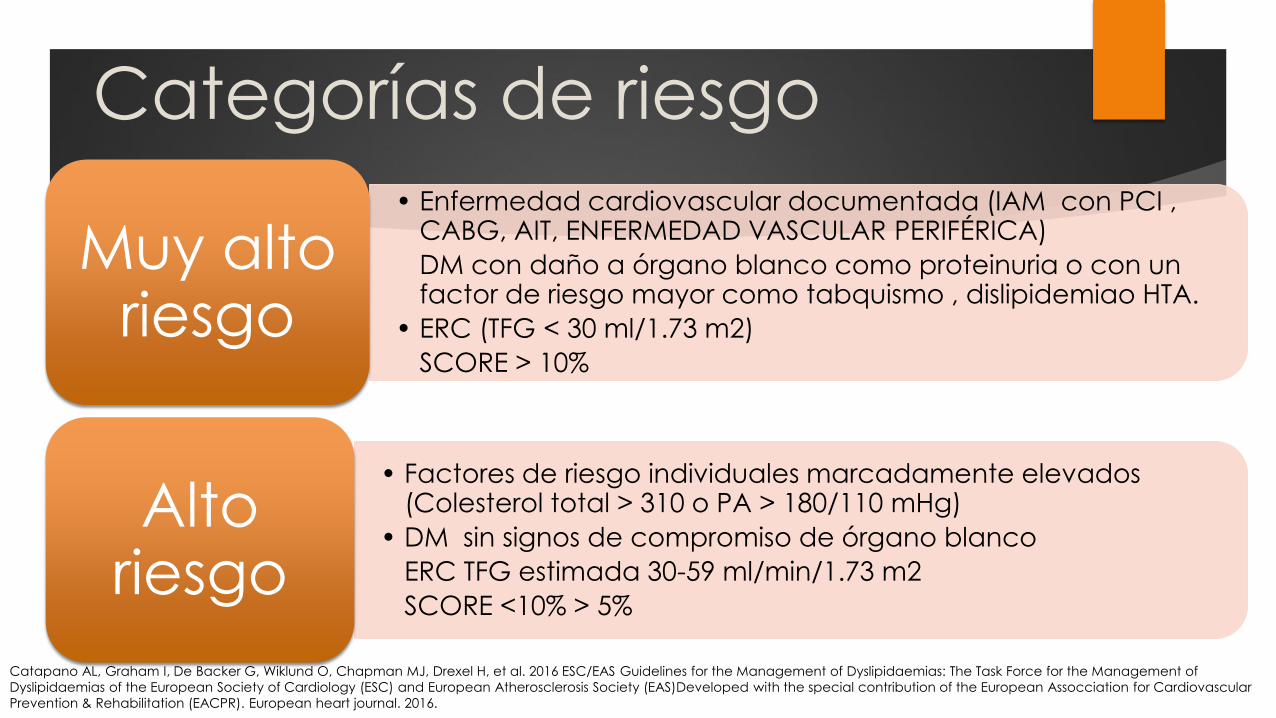
Categorías de riesgo
• Enfermedad cardiovascular documentada (IAM con PCI , CABG, AIT, ENFERMEDAD VASCULAR PERIFÉRICA)
DM con daño a órgano blanco como proteinuria o con un factor de riesgo mayor como tabquismo , dislipidemiao HTA.
• ERC (TFG < 30 ml/1.73 m2)
SCORE > 10%
Muy alto riesgo
• Factores de riesgo individuales marcadamente elevados (Colesterol total > 310 o PA > 180/110 mHg)
• DM sin signos de compromiso de órgano blanco
ERC TFG estimada 30-59 ml/min/1.73 m2
SCORE <10% > 5%
Alto riesgo
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
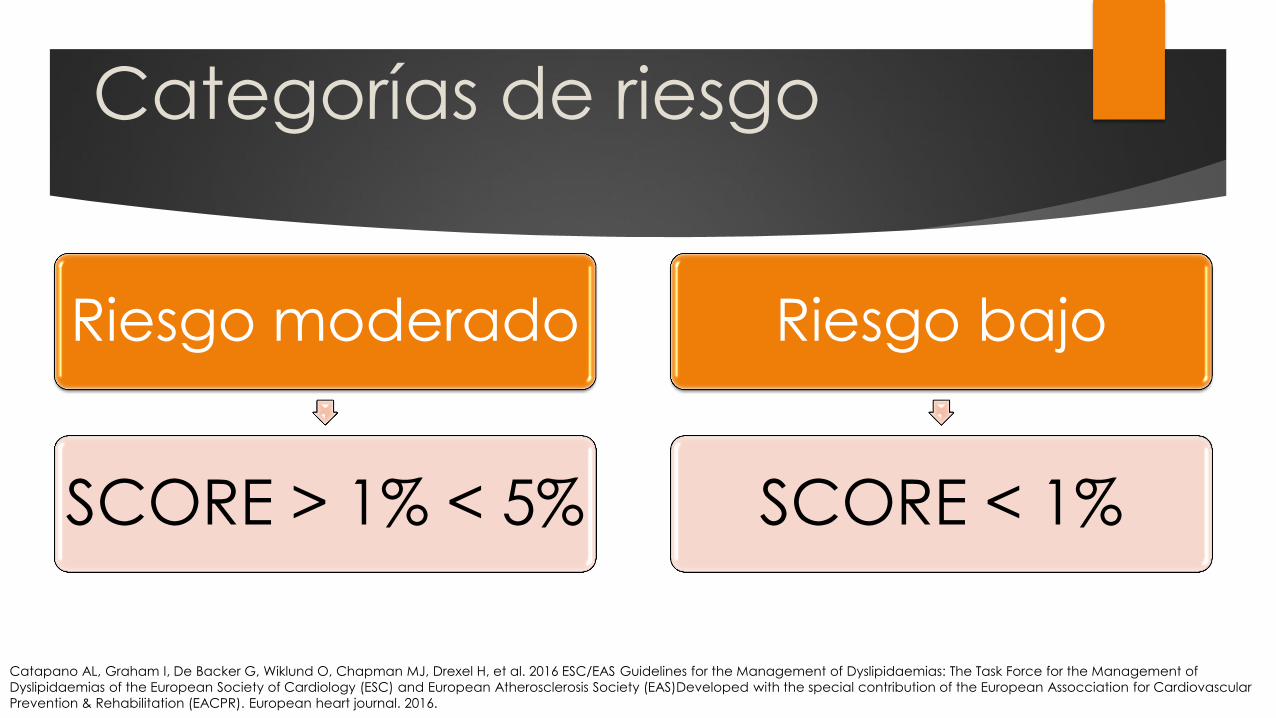
Categorías de riesgo
Riesgo moderado
SCORE > 1% < 5%
Riesgo bajo
SCORE < 1%
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
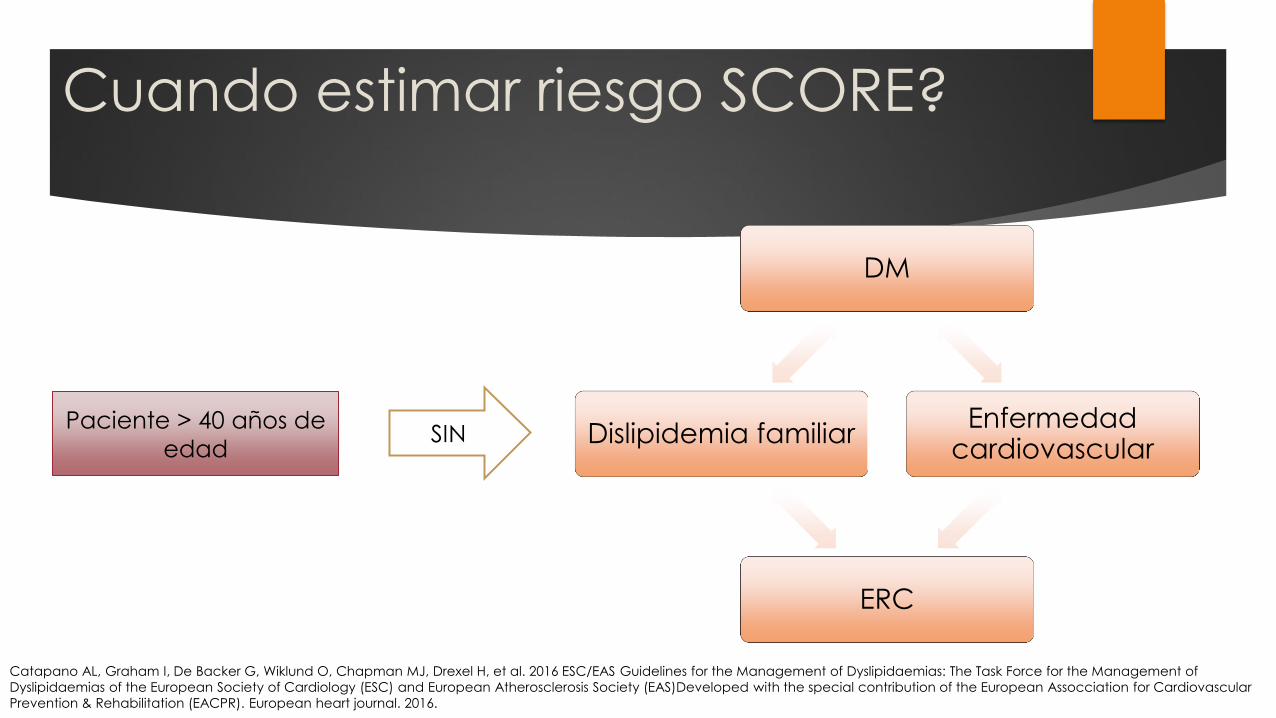
Cuando estimar riesgo SCORE?
DM
Enfermedad cardiovascular
ERC
Dislipidemia familiar Paciente > 40 años de
edad SIN
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
HERRAMIENTA DE ESTRATIFICACIÓN COLOMBIA Evaluación de riesgo cardiovascular
En la población colombiana, ¿el modelo de Framingham, comparado con
los modelos PROCAM (Prospective Cardiovascular Munster) y SCORE
(Systematic Coronary Risk Evaluation), tiene mejor desempeño en la
predicción de desenlaces cardiovasculares y cerebrovasculares en
pacientes con diagnóstico de dislipidemia?
Recomendación
1. En la población de prevención primaria o sin enfermedad cardiovascular
clínicamente manifiesta, se recomienda utilizar la escala de Framingham
recalibrada para Colombia con el fin de clasificar el riesgo cardiovascular.
Recomendación fuerte a favor de la intervención.
Calidad de la evidencia: ⊕⊕⊕⊝ Moderada.
Puntos de buena práctica clínica
Las personas en los siguientes grupos tienen condiciones que por sí
mismas implican un riesgo mayor y manejo farmacológico. Por tanto, no
es necesario utilizar tablas para cálculo de riesgo:
• Historia de enfermedad cardiovascular aterosclerótica.
• Hipercolesterolemia con niveles de LDL mayores que 190 mg/dL.
• Diabetes mellitus.
• Es aconsejable que en la consulta de primera vez el médico tenga un
tiempo disponible de 30 minutos; esto, con el fin de:
Facilitar una adecuada aplicación de las tablas de riesgo, como la
propuesta por Framingham.
Asegurar una suficiente explicación al paciente sobre el significado del
riesgo coronario y el tratamiento y el pronóstico correspondientes.
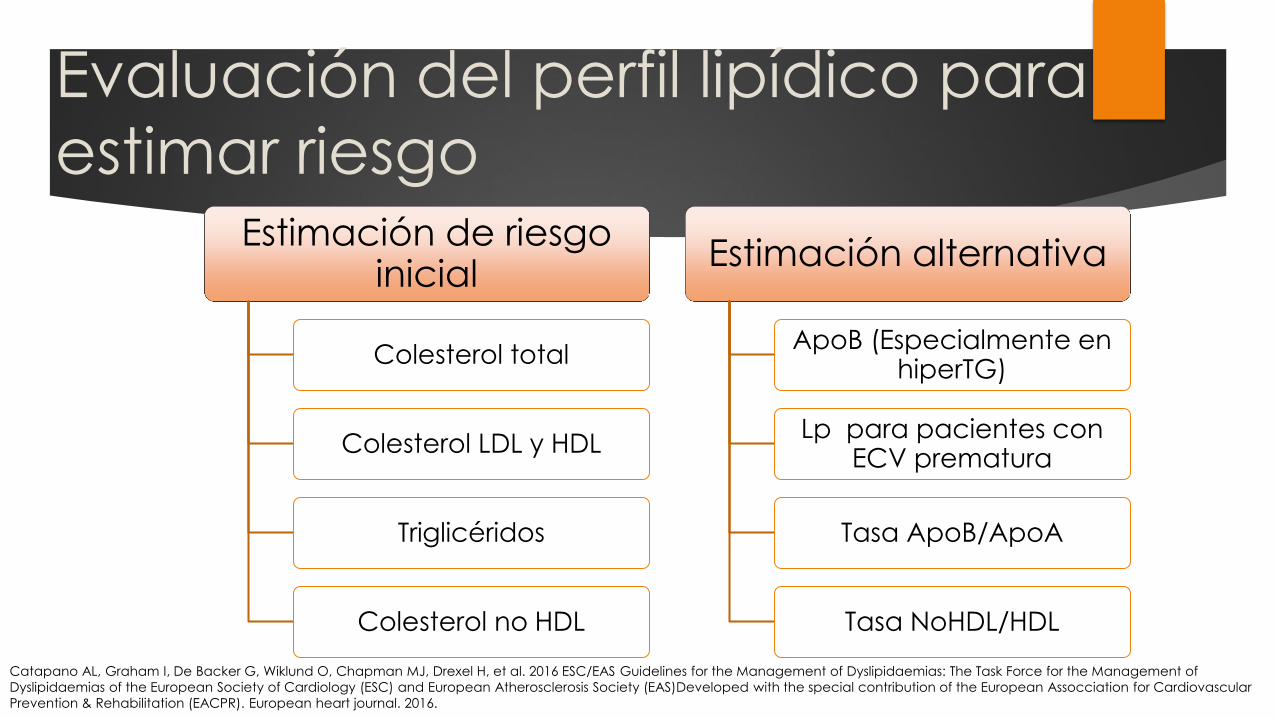
Evaluación del perfil lipídico para
estimar riesgo Estimación de riesgo
inicial
Colesterol total
Colesterol LDL y HDL
Triglicéridos
Colesterol no HDL
Estimación alternativa
ApoB (Especialmente en hiperTG)
Lp para pacientes con ECV prematura
Tasa ApoB/ApoA
Tasa NoHDL/HDL
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.

Evaluación del perfil lipídico
previo a TTO.
HDL
LDL
TG
No-HDL-C Alternativas Lp
Colesterol
total
ApoB
Usualmente no permite
clasificar el trastorno
Diagnóstico: estrategia de tamizaje
En la población adulta en Colombia, ¿cuál es la estrategia más
adecuada de tamización de dislipidemia (medición del perfil lipídico
completo, comparado con medición de colesterol total)?
Recomendaciones
1. Para la tamización de dislipidemias en la población adulta colombiana,
se sugiere la medición en sangre venosa periférica de CT, HDL, TG y
cálculo de LDL, mediante la fórmula de Friedewald, cuando el valor de
los TG es menor que 400 mg/dL, o medición directa si el valor de los TG es
mayor que 400 mg/dL.
Cuándo realizar screening
para lipoproteina?
Enfermedad cardiovascular prematura
Hipercolesterolemia familiar
Historia familiar de enfermedad cardiovascular prematura y/o Lp
elevada
Enfermedad cardiovascular recurrente a pesar de terapia
hipolipemiante óptima
Riesgo fatal > 5% a 10 años de acuerdo a SCORE
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
Objetivos de TTO
Primarios
LDL
CT (Sólo si LDL no disponible)
Secundarios
No- HDL-C ,
ApoB
No son
objetivos Tasa ApoB/ApoA ,
Tasa No HDL-C/HDL
HDL
Metas de tratamiento
No exposición al tabaco
2,5-5 h de actividad física por semana o 30-60 min mayoria de los dias
IMC 20-25 Kg/m2, PA <94 hombres , < 80 mujeres
Presión arterial < 140/90 mmHg
DM: HbA1C < 7%
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
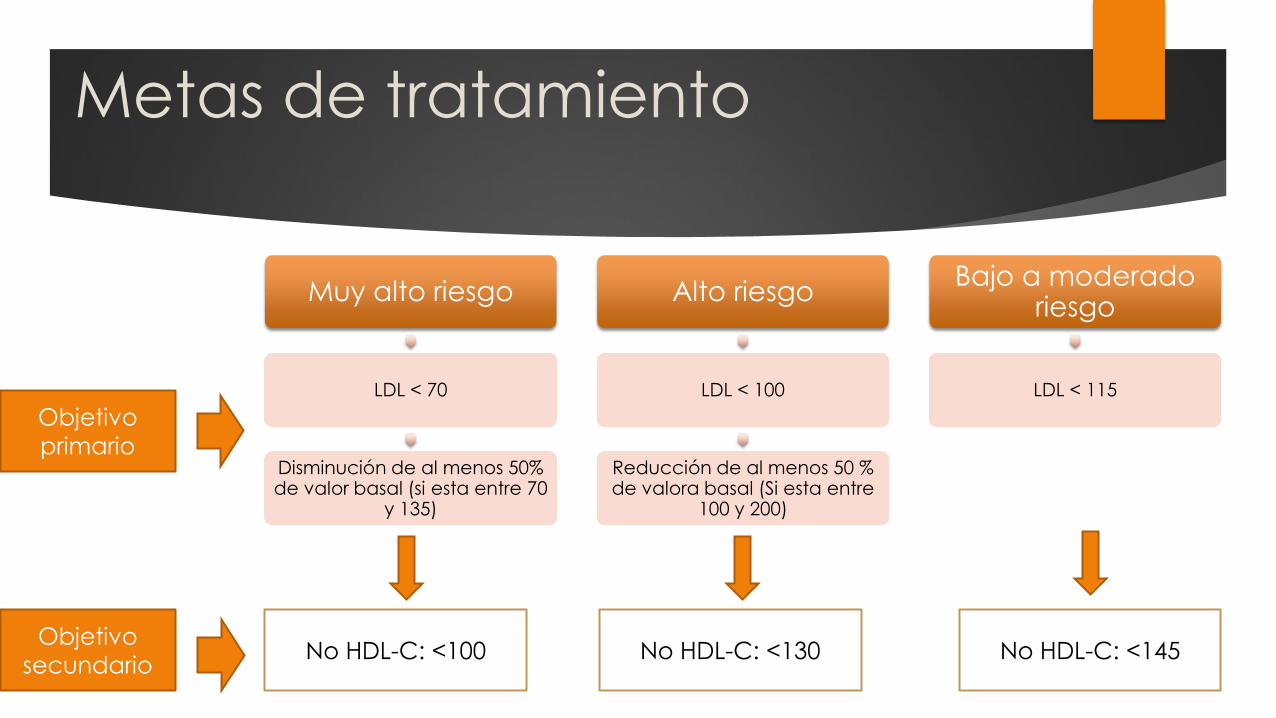
Metas de tratamiento
Muy alto riesgo
LDL < 70
Disminución de al menos 50% de valor basal (si esta entre 70
y 135)
Alto riesgo
LDL < 100
Reducción de al menos 50 % de valora basal (Si esta entre
100 y 200)
Bajo a moderado riesgo
LDL < 115
Objetivo
primario
Objetivo
secundario No HDL-C: <100 No HDL-C: <130 No HDL-C: <145
Otros valores pronósticos
HDL > 40 en hombres y > 48 en mujeres
TG < 150
Indicadores de bajo riesgo
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
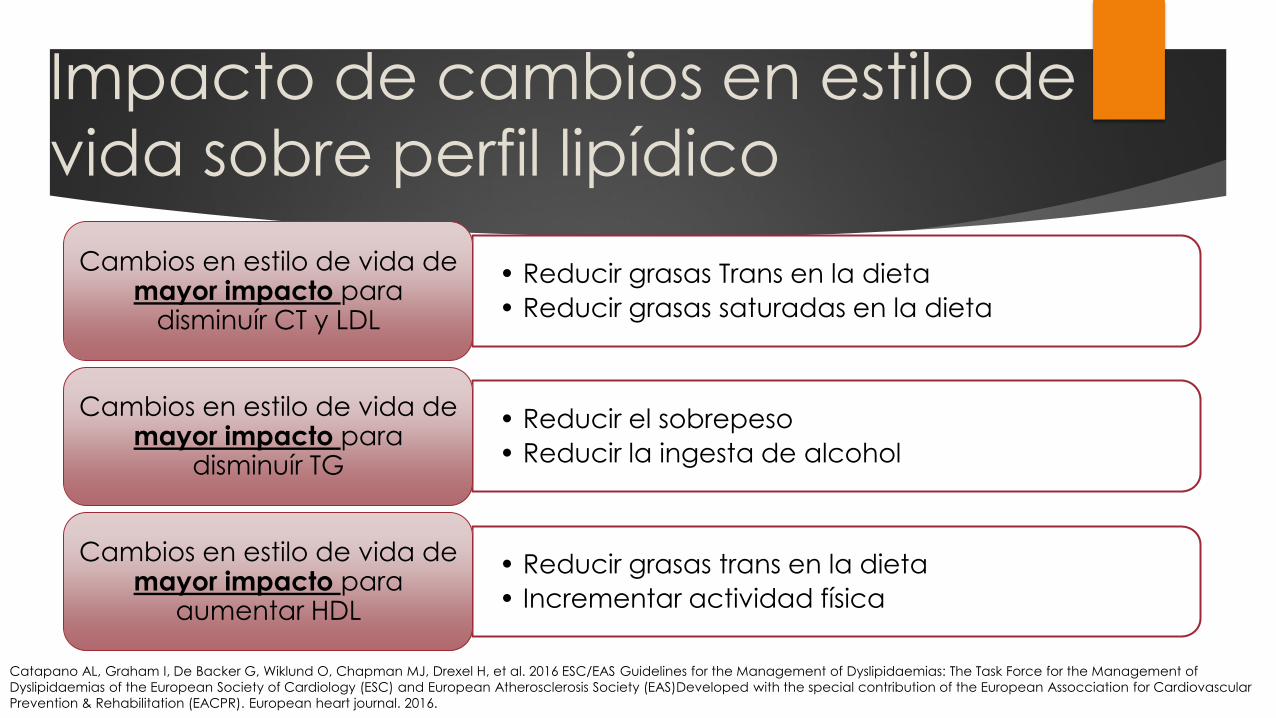
Impacto de cambios en estilo de
vida sobre perfil lipídico
• Reducir grasas Trans en la dieta
• Reducir grasas saturadas en la dieta
Cambios en estilo de vida de mayor impacto para
disminuír CT y LDL
• Reducir el sobrepeso
• Reducir la ingesta de alcohol
Cambios en estilo de vida de mayor impacto para
disminuír TG
• Reducir grasas trans en la dieta
• Incrementar actividad física
Cambios en estilo de vida de mayor impacto para
aumentar HDL
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.

Principios del
tratamiento
farmacológico
Tratamiento hipolipemiante
Medicamentos para hipercolesterolemia
1. Estatinas
2.Secuestrantes de ácido biliar
3.Inhibidores de absorción de
colesterol
4.Inhibidores PCSK9
5. Ácido nicotínico
6.Medicamentos combinados
Medicamentos para
hipertrigliceridemia
1. Estatinas
2. Fibratos
3. Ácido nicotínico
4.Ácidos grasos n3
Medicamentos que afectan
HDL-C
1. Estatinas
2. Fibratos
3. Ácido nicotínico
4.Inhibidores de proteína colesteril-ester transferasa
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of
Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular
Prevention & Rehabilitation (EACPR). European heart journal. 2016.
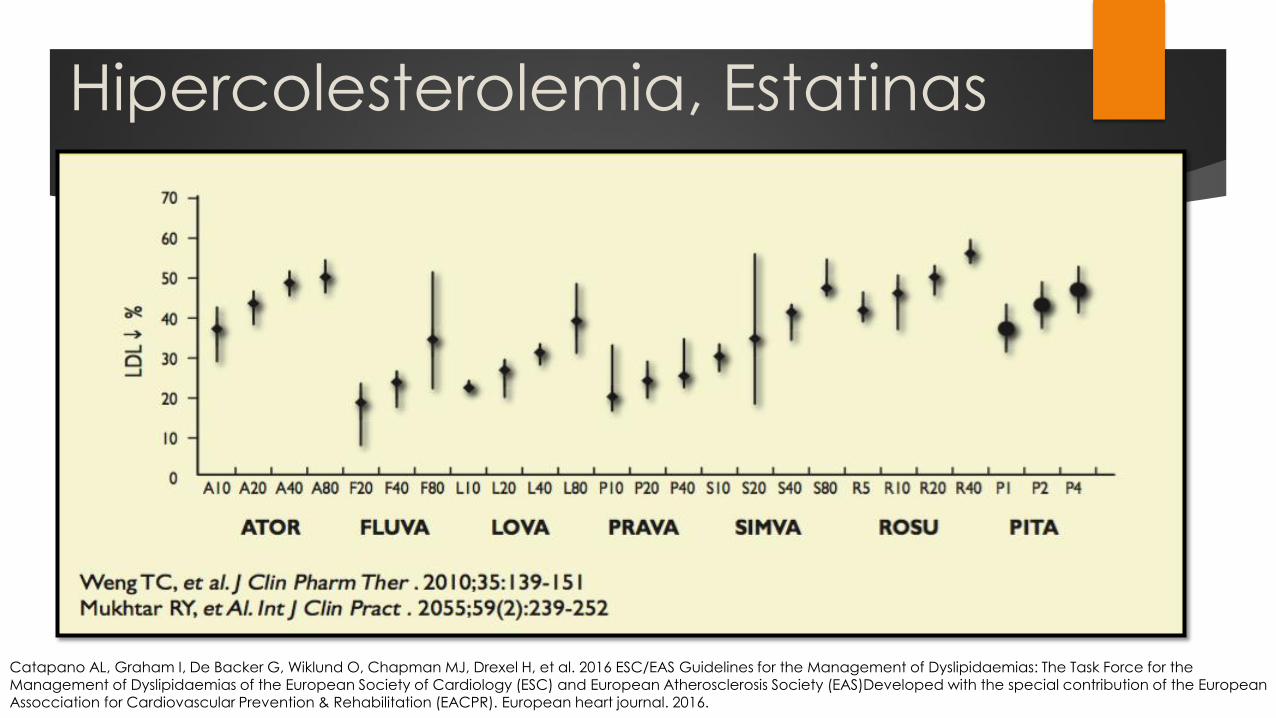
Hipercolesterolemia, Estatinas
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
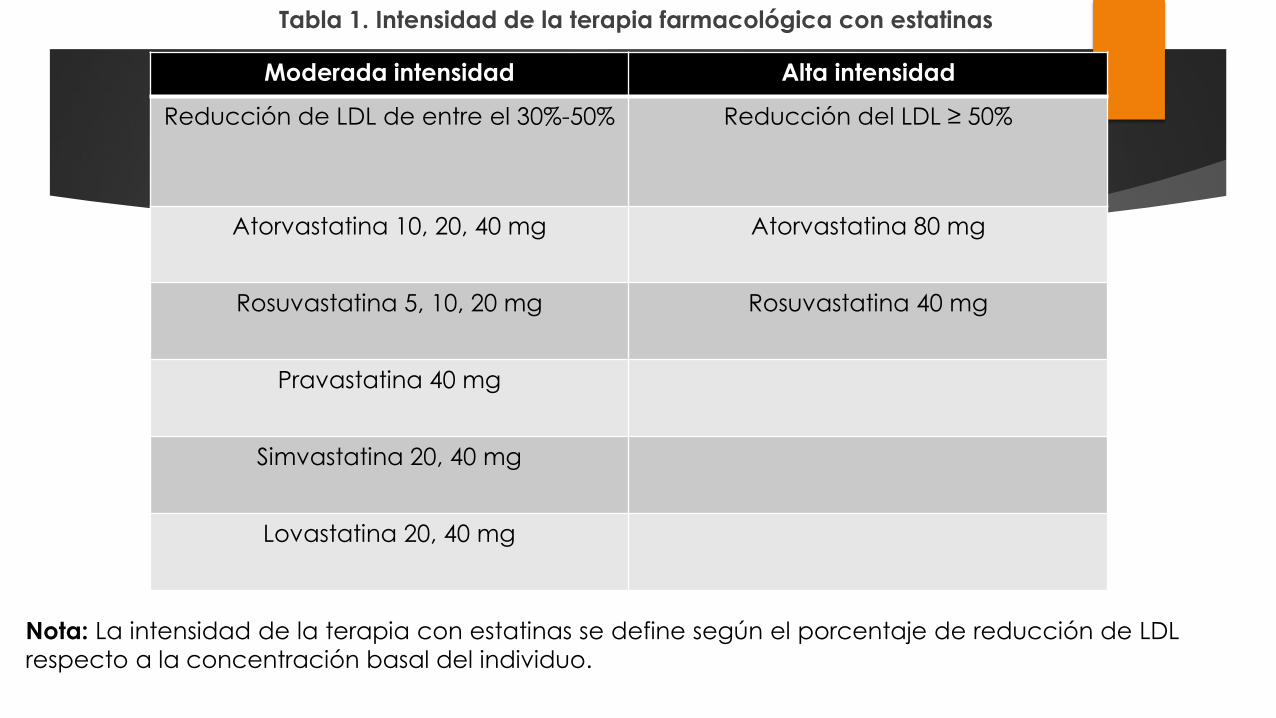
Tabla 1. Intensidad de la terapia farmacológica con estatinas
Moderada intensidad Alta intensidad
Reducción de LDL de entre el 30%-50%
Reducción del LDL ≥ 50%
Atorvastatina 10, 20, 40 mg
Atorvastatina 80 mg
Rosuvastatina 5, 10, 20 mg
Rosuvastatina 40 mg
Pravastatina 40 mg
Simvastatina 20, 40 mg
Lovastatina 20, 40 mg
Nota: La intensidad de la terapia con estatinas se define según el porcentaje de reducción de LDL
respecto a la concentración basal del individuo.
Hipercolesterolemia,
Estatinas
Se deben prescribir estatinas a la dosis mas alta indicada o
la mas alta tolerada con el fin de alcanzar metas de LDL
Si hay intolerancia a las estatinas se debe considerar
manejo con Ezetimibe o secuestrante de ácido biliar o
terapia combinada con estos
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
Utilidad de estatinas
Disminución de 10% en mortalidad por todas las causas y 20%
en muertes por enfermedad cardiovascular con reduccion de 40
mg dL en LDL-C
Riesgo de evento coronario disminuyó 23%, Riesgo de ECV
disminuyó 17% con la reducción de 40 mg dL de LDL-C
Efectos pleiotrópicos múltiples (Antioxidante, Antiinflamatorio)
Reducen TG 30-50%
Aumentan HDL-C 5-10% Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
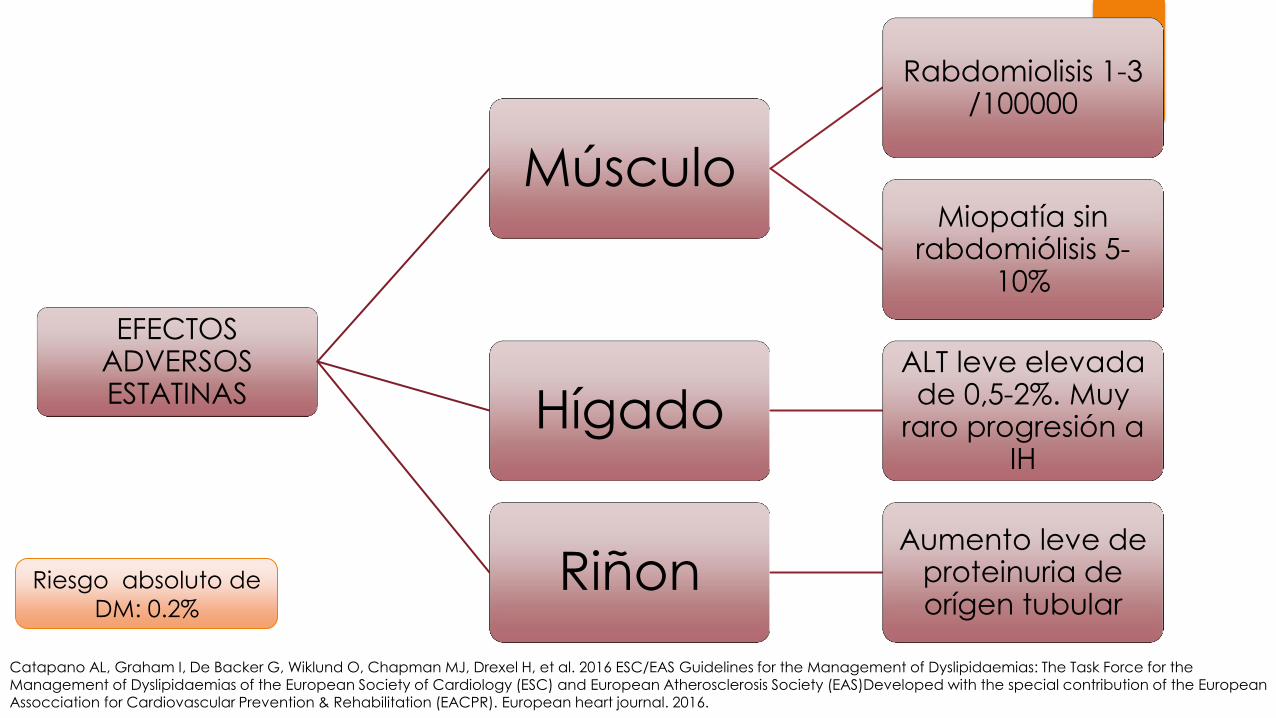
EFECTOS ADVERSOS ESTATINAS
Músculo
Rabdomiolisis 1-3 /100000
Miopatía sin rabdomiólisis 5-
10%
Hígado ALT leve elevada de 0,5-2%. Muy
raro progresión a IH
Riñon Aumento leve de
proteinuria de orígen tubular
Riesgo absoluto de
DM: 0.2%
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
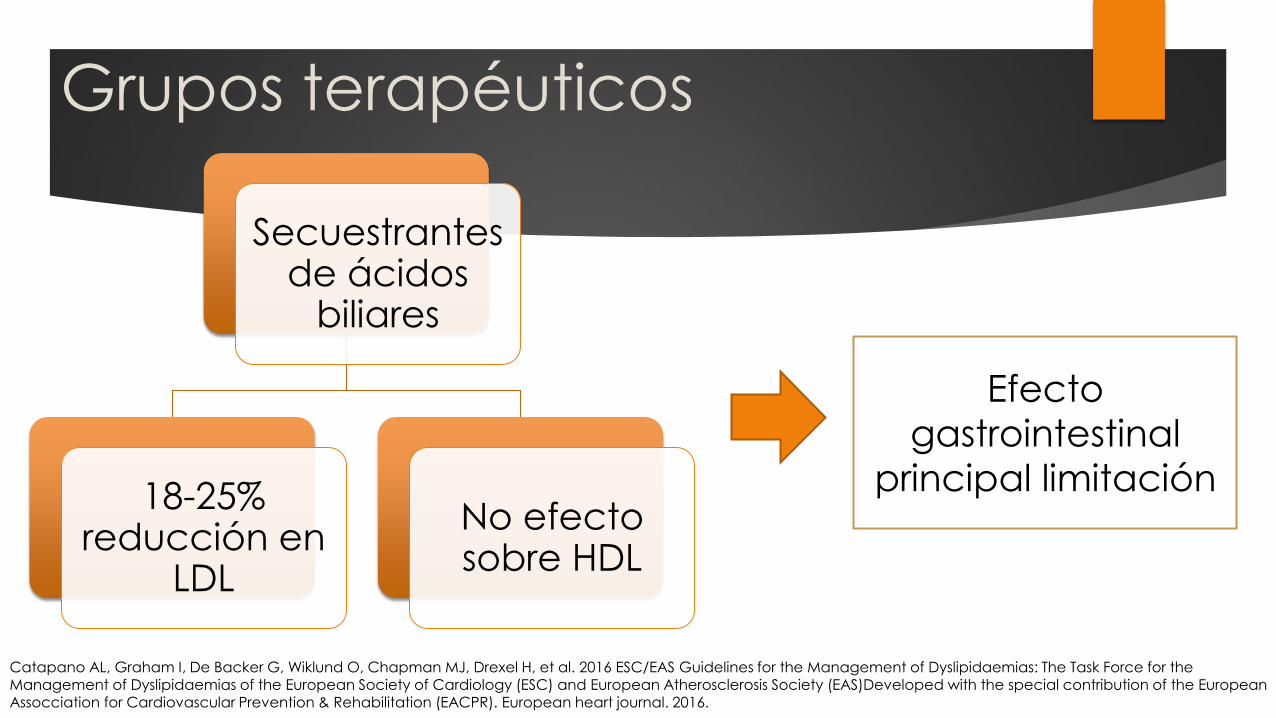
Grupos terapéuticos
Secuestrantes de ácidos
biliares
18-25% reducción en
LDL
No efecto sobre HDL
Efecto
gastrointestinal
principal limitación
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
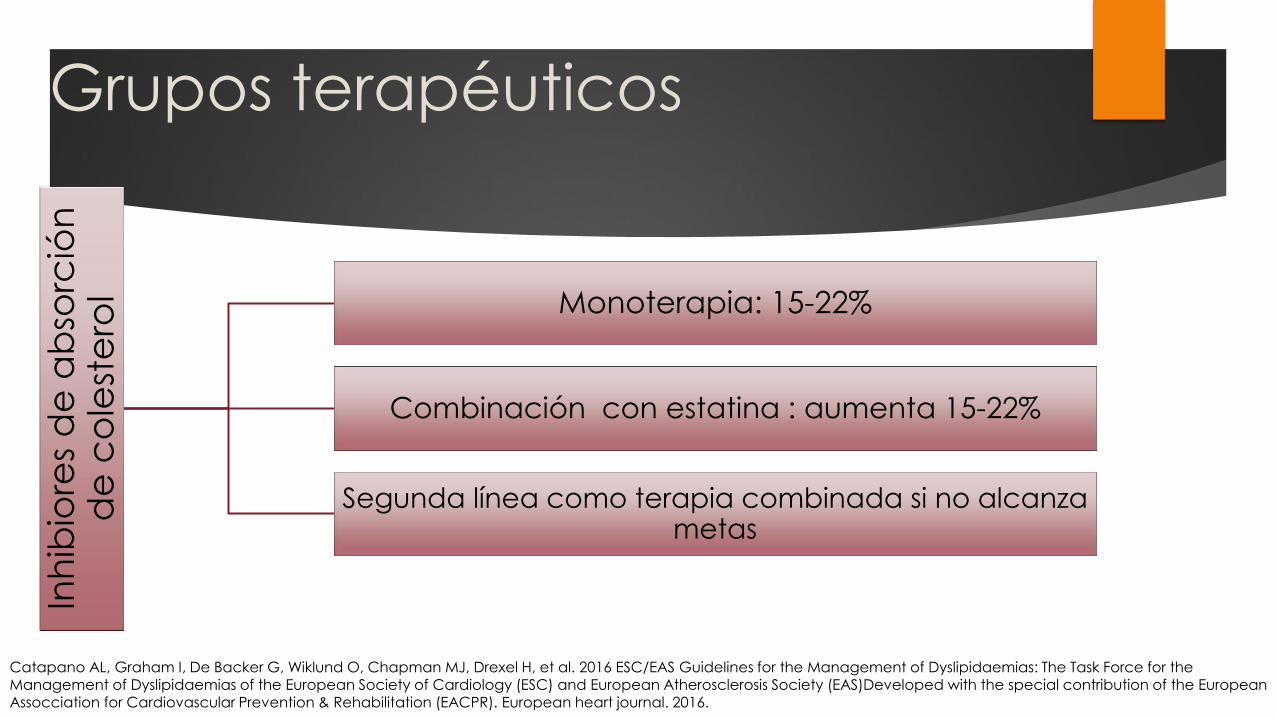
Inh
ibio
res
de
ab
sorc
ión
d
e c
ole
ste
rol Monoterapia: 15-22%
Combinación con estatina : aumenta 15-22%
Segunda línea como terapia combinada si no alcanza metas
Grupos terapéuticos
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
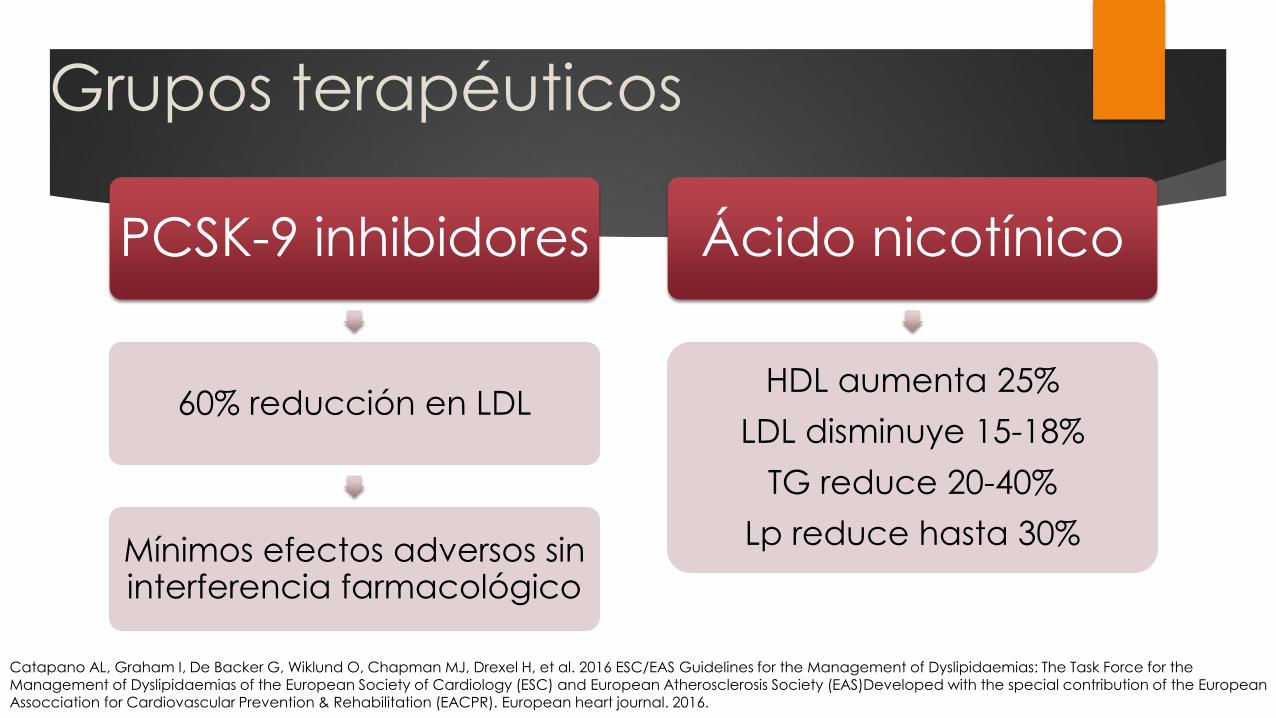
Grupos terapéuticos
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
PCSK-9 inhibidores
60% reducción en LDL
Mínimos efectos adversos sin interferencia farmacológico
Ácido nicotínico
HDL aumenta 25%
LDL disminuye 15-18%
TG reduce 20-40%
Lp reduce hasta 30%
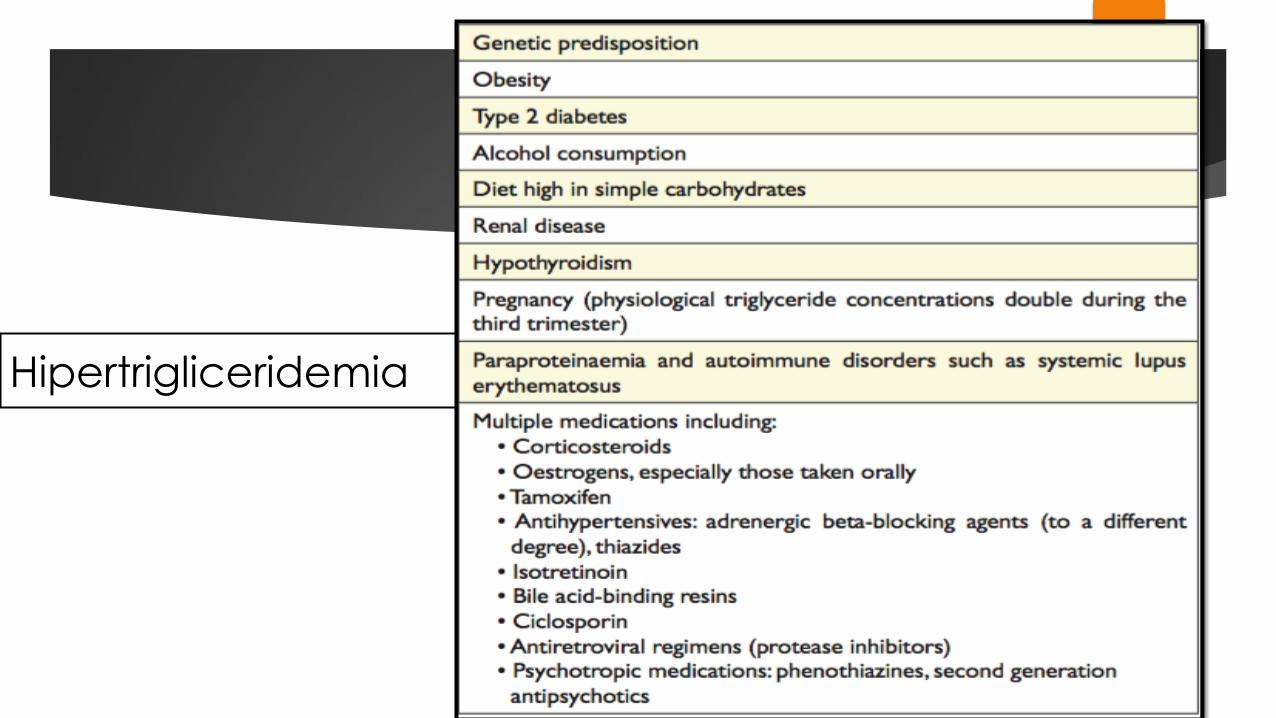
Hipertrigliceridemia
Recomendaciones de tratamiento
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
Pacientes de alto riesgo TG>200
Primera elección : Estatinas en pacientes de alto riesgo
Pacientes de alto riesgo sin mejoría con tratamiento (TG> 200) , administrar fenofibrato.
Mensajes para llevar a casa
Prevención como estrategia mas importante
Inicio temprano de terapia hipolipemiante en pacientes de muy
alto riesgo
Individualizar terapia
Cambios en el estilo de vida que mas impactan en perfil lipídico
y mortalidad cardiovascular.
Monitoreo y seguimiento de los pacientes para verificar
adherencia , respuesta clínica y/o eventos adversos
Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS)Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal. 2016.
GRACIAS