case report - medic
TRANSCRIPT

CASE REPORTU TUYẾN NƯỚC BỌT PHỤ
HIẾM GẶP
BS TRƯƠNG NGỌC LỄ

CASE REPORT
Bệnh nhân :Phương T.A,nữ,77 tuổi
Địa chỉ:Quận 6
LDĐK:Nghẹt mũi,ù tai

NỘI SOI VÒM HẦU THANH QUẢN




GPB

Các tuyến tiết nước bọt cho vùng miệng, họng bao gồm: tuyến mang tai, tuyến dưới hàm, tuyến dưới lưỡi và các tuyến nước bọt phụ phân bố rải rác trong khoang miệng, họng và thanh quản. U tuyến nước bọt gặp nhiều nhất ở tuyến mang tai sau đó là tuyến dưới hàm, dưới lưỡi, u tuyến nước bọt phụ rất hiếm gặp nhưng tỷ lệ ác tính lại cao hơn so với u của các tuyến nước bọt chính.

• . Các khối u tuyến nước bọt chiếm vào khoảng 0,2 – 0,6% của tất cả các loạikhối u và khoảng 2 – 4% khối u vùng đầu cổ. Ở Việt Nam, ước tính cókhoảng 0,6 – 0,7 trường hợp u tuyến nước bọt mới mắc/100.000 dân.
• U tuyến nước bọt chủ yếu là u lành tính (80%), chỉ có 20 % các u tuyếnnước bọt là ác tính. Trong đó ung thư tuyến mang tai chiếm 78% trong sốung thư tuyến nước bọt.
• Sự phân bố rải rác của các u tuyến nước bọt phụ làm khó khăn cho việcchẩn đoánUng thư tuyến nước bọt là một bệnh ung thư hiếm gặp, nóđược phát sinh trong bất kỳ các tế bào nào trong tuyến nước bọt như ở: cổ, miệng hay cổ họng.

Nguyên nhân và các yếu tố nguy cơ:
• Nguyên nhân :không rõ ràng. xảy ra khi một số tế bào trong tuyến nước bọtphát triển đột biến DNA.
• Các yếu tố nguy cơ :- Lớn tuổi. Mặc dù nó có thể xảy ra ở mọi lứa tuổi, ung thư tuyến nước bọtthường được chẩn đoán ở người lớn tuổi (thường là trên 40 tuổi).
- Phơi nhiễm bức xạ. chẳng hạn như bức xạ được sử dụng để điều trị ungthư đầu và cổ, làm tăng nguy cơ ung thư tuyến nước bọt.
- Tiếp xúc với các chất hóa học:các hợp kim niken và bụi silica

Triệu chứng :
• thường gặp nhất khiến bệnh nhân phải nhập viện là sưng phồng tại mộtvùng của tuyến nước bọt, nuốt vướng, nuốt đau, liệt mặt(là dấu hiệu gợi ý u ác tính ở tuyến mang tai). Nghẹt mũi và chảy máu mũi thường tập trung ởcác khối u vòm họng, hốc mũi.
• có thể bao gồm:- Sưng phần trên hàm ,cổ hoặc miệng.- Tê một phần mặt.- Yếu cơ ở một bên mặt.- Đau dai dẳng trong một vùng của tuyến nước bọt.- Khó nuốt.- Khó mở miệng rộng.
-Nghẹt mũi,chảy máu mũi.

Biểu hiện lâm sàng và chẩn đoán ung thư tuyến nước bọt được xácđịnh một phần theo vị trí của khối u.-U tuyến mang tai:Phần lớn bệnh nhân có u đơn kín đáo, tiến triển chậm vàkhông triệu chứng.Liệt dây thần kinh mặt đi kèm với khối u tuyến mang tai hầunhư đều liên quan tới u ác tính..
-U tuyến dưới hàm: thường là một khối u không triệu chứng. Các nguyên nhânphổ biến là sỏi và viêm và hiếm khi là do khối u.
-U tuyến nước bọt nhỏ:
+trong khoang miệng có thể là một khối u không đau nằm dưới niêm mạcvòm họng, môi hoặc ở niêm mạc miệng. có thể bị loét .
+ ở khoang mũi hoặc xoang hàm có thể gây ra các triệu chứng như tắc mũi, sung huyết gây nghẹt mũi, thay đổi thị giác hoặc cứng khít hàm.

Chẩn đoán xác định :
-Các triệu chứng lâm sàng:khám hàm, cổ và họng để tìm một nốt hoặc mộtchỗ sưng.
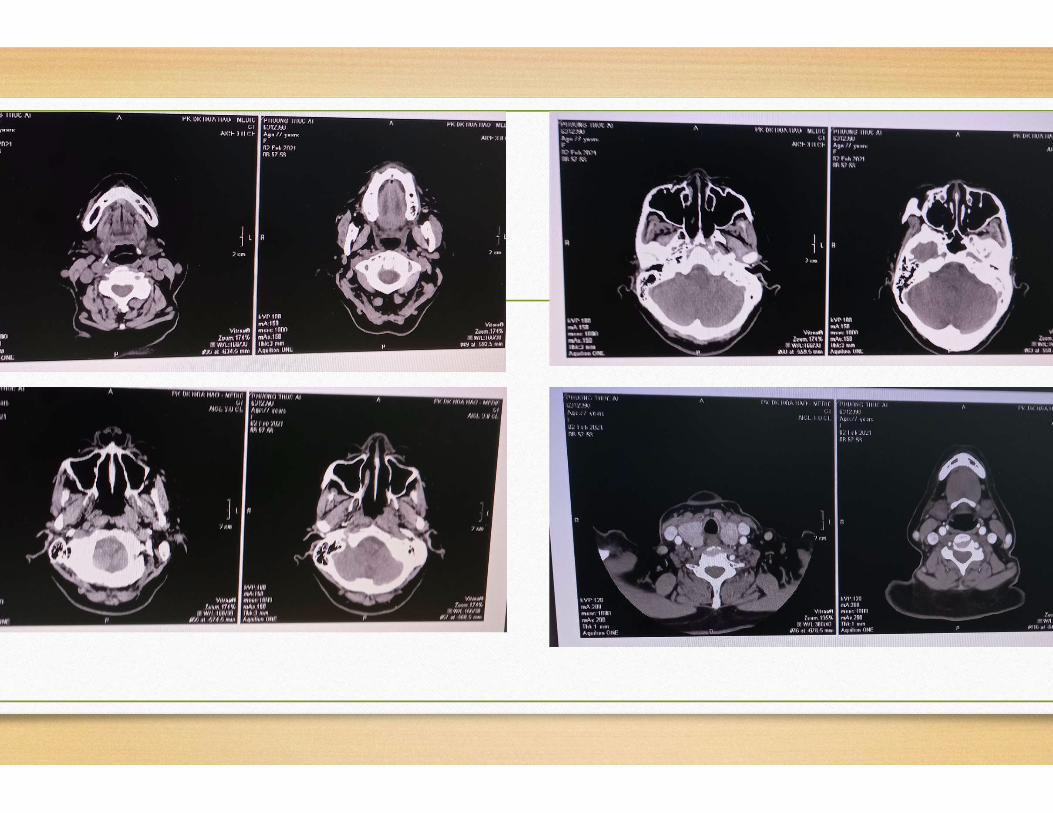
- Chẩn đoán hình ảnh : MRI và CT giúp đánh giá kích thước và vị trí khối u. sự thâm nhiễm vào các mô lân cận và sự xâm lấn vào mạch hoặc xung quanhthần kinh. Chụp cắt lớp là phương pháp tốt nhất để phát hiện ra huỷ xươngthái dương hoặc xương hàm dưới, chụp cộng hưởng từ cho phép đánh giá chi tiết hơn sự thâm nhiễm vào mô mềm, sự xâm lấn vào vùng xung quanh thầnkinh và tổn thương lan vào nội sọ.
-Sinh thiết hay chọc hút tế bào.
Điều trị:
-Phụ thuộc vào kích thước, phân loại và giai đoạn của ung thư tuyếnnước bọt.
-Điều trị ung thư tuyến nước bọt thường liên quan đến phẫu thuật, cóthể kèm xạ trị.

SUMMARY Adenoid cystic carcinoma is a malignant tumour involvingthe salivary glands, rarely developing in the nasopharynx. The biologicalbehaviour of adenoid cystic carcinoma is characterized by slow growthrate, high tendency to local recurrence and metastatic spread.histological features are particularly important for prognostic predictionsolid pattern has the worst �out come. Initial presentationnasopharyngeal adenoid cystic carcinoma with paresis of cranial nervesand Horner’s syndrome is infrequent. The Authors present a case ofrare adenoid cystic carcinoma of the nasopharynx, at admission withHorner’s syndrome, in a 66-year-old male. Magnetic resonance imagingshowed an expansive submucosal lesion of the nasopharynx involvingthe para-pharyngeal space, tensor and levator veli palati muscles andapex of petrous bone. Positron emission tomography excluded distantmetastasis. Definitive histopathological examination revealed an adenoidcystic carcinoma with mixed cribriform and solid pattern. The patientwas treated exclusively with radiotherapy (70 Gy) in 35 fractions withpartial reduction of the neoplastic mass
ACTA otorhinolaryngologica italica 2007;27:216-219
Case report A rare case of adenoid cystic carcinoma of thenasopharynx manifesting as Horner’s syndrome: discussionand review of the literature
Un raro caso di carcinoma adenoido-cistico del rinofaringe manifestatosisindrome di Horner: discussione e revisione della letteratura
Soprani, V. Armaroli, A. Venturini1 , E. Emiliani2 , D. CasolinoDepartment of Otolaryngology, Head and Neck Surgery, Santa Maria delleCroci Hospital, Ravenna; 1 Department of Radiation Oncology, Villa MariaCecilia Hospital, Cotignola (RA); 2 Department of Radiation Oncology, SantaMaria delle Croci Hospital, Ravenna, Ital

Introduction
Adenoid cystic carcinoma (ACC) is a malignant tumour of the exocrine glands. It most commonly arises in the salivary glands (it accounts, in fact, for 12% to 14% of malignant parotid neoplasms, for 31% to 58% of malignant tumours of the submandibular gland and for 33% to 55% of malignant tumours of the minor salivary glands), even if localizations have been described in prostate, lacrymal glands, cervix uteri, breast and bronchial mucosa 1–5.
Nasopharyngeal localization is uncommon, accounting for approximately 0.5% to 4% of all the carcinomas of the nasopharynx and for 2.4% to 3.7% of all head and neck ACC 1 6–8.
Typical features of ACC are: slow growth rate, high propensity for perineural spread, for local recurrence and for distant metastasis, usually involving lung, bones and liver 3 4 9 10.
Histologically, three growth patterns can be recognized for ACC: cribriform, tubular and solid. This is particularly important for prognostic purposes since the predominant tubular pattern has the best prognosis, the predominant solid pattern the worst, being associated with the highest incidence of distant metastasis and perineural infiltration with, consequently, 15 years survival rate of 5% 2 3 11–13.
The reported incidence of invasion of the skull base ranges from 4% to 22% and can realize through various ways of spread: the peritubaric space, the branches of the trigeminal nerve and the internal carotid artery 2 14–16.
These tumours have a long natural history characterized by a typical slow growth rate responsible for the delay in seeking early medical consultation. The interval between onset of the disease and onset of the first symptoms is estimated to be between 2 and 5 years 1 3 17.
The symptoms most commonly found are epistaxis, progressive nasal stenosis, dysfunction of the Eustachian tube and, in relation to the invasion of the skull base, disorders of ocular motility, diplopia, facial pain, dysfunction of IX, X, XI and XII pairs of cranial nerves and, more rarely, Horner’ s syndrome 1 2 17.
Imaging of ACC is based on computed tomography (CT) scan, particularly helpful in detecting bony erosions of the skull base, and on Magnetic Resonance Imaging (MRI) with gadolinium, effective in demonstrating possible involvement of infra-temporal fossa, cavernous sinus, and perineural or perivascular infiltration 3.

Case report
U.R.B., a 66-year-old male, was referred to the ENT Department, complaining of a visual deficit in the lateral look associated with progressive hoarseness, dysphonia and dysphagia both for liquid and solid food which had been present for 2 months.
Clinical history showed chronic lung emphysema. More-over, the patient was in follow-up at the Department of Gastroenterology for a gastric carcinoid tumour successfully removed by endoscopic surgery two years earlier.
Otolaryngologic examination revealed paralysis of the left soft palate and of the left vocal fold. Investigation with flexible endoscopy was negative for macroscopic disease of the nasopharynx.
Neurological evaluation revealed anisocoria due to constriction (miosis) of the left pupil, drooping of the left upper eyelid (ptosis) and light sinking of the eyeball into the bony cavity of the eye (enophthalmos). All these signs led to the diagnosis of Horner’ s syndrome.
High resolution computed tomography (HRCT) scan of the skull base revealed vast erosion of the foramen lacerum extended to the foramen rotundum and ovale, to the apex of petrous bone and to the internal carotid artery.
MRI of the skull base confirmed the presence of an expansive submucosal lesion with involvement of the left para-pharyngeal space reaching the omolateral petrous bone with infiltration of tensor and levator veli palati muscles (Fig. (Fig.11

According to the indications of the HRTC scan and of MRI, multiple biopsies were performed, deeply into the mucosal surface which was healthy in appearance, following the posterior margin of the left Eustachian tube. Intra-operative frozen section examination of nasopharyngeal tissue demonstrated an infiltrating adenocarcinoma. Definitive histological examination confirmed the diagnosis; in particular, the morphological pattern (mixed cribriform and tubular) and immunohistochemical profile (CK7+, CK20-, S100+), indicated an adenoid cystic carcinoma of the minor salivary glands (Fig. (Fig.22).
Definitive histologic examination indicating adenoid cystic carcinoma of minor salivary glands with mixed cribriform and tubular pattern.
Considering the site and the extension of the lesion, treatment with exclusive radiation therapy was prescribed. The patient was immobilized with a thermoplastic mask. Treatment was delivered with conformal high energy photons (6 MV) that included the nasopharynx and skull base. A total dose of 70 Gy, in 35 fractions, was administered.
Treatment was not interrupted with good clinical tolerance; we detected grade 1 mucositis (WHO scale) and weight loss, resolved with adequate therapy.
Post-treatment MRI, performed 6 months after the radiation therapy, showed a reduction of the neoplastic mass (Fig. (Fig.33).
Fig. 3
Post-treatment MRI, performed 6 months after radiation therapy, showing a slight reduction of neoplastic mass.
This radiological finding was the same as that at the MRI control performed 18 months after radiotherapy.
The patient reported improvement in swallowing function.
Otolaryngologic revaluation did not show any significant variations in the clinical aspects found at the time of diagnosis.

Discussion
The best treatment for ACC is unanimously considered radical surgical
resection followed by radiotherapy 1 3 5 13 16–20.
In cases of nasopharyngeal ACC, the frequent perineural and perivascular
infiltrations, associated with the anatomical characteristics of the nasopharynx,
however, make the surgical approach risky on account of technical difficulties,
due substantially to the proximity of surgical margins to critical neural and
vascular structures 8 13.
Surgical treatment, therefore, is often characterized by incomplete oncological
radicality, consequently with increased frequency of local recurrence within 3
years of the initial treatment 3 9 13 21.
This aspect is of great importance considering the study of Sur et al., who,
analysing the prognostic factors influencing the clinical control of the disease,
indicate, in the portion of the residual tumoural mass, the only parameter
indicating therapeutic effectiveness 20.
In cases of ACC, moreover, it should be emphasized that, also when good local
control of the disease has been reached (complete resection of the tumoural
mass), the presence of distant metastases is possible in 39% of the patients 3.
Another aspect to be taken into consideration is that surgical treatment of these neoplasms with extension to the skull base is associated with a significant morbidity rate, due to the frequent appearance of sequels and complications, due to vascular
In the case of ACC with intracranic extension, it, therefore, appears important to
evaluate the real benefits of surgery, also considering that this pathological
condition has a slow clinical progression which allows long-term survival of
many patients, even with advanced or metastatic disease 1 13 14 22–24.
In the literature, moreover, many studies have shown that survival rates, over a
long period of time, in patients with nasopharyngeal ACC do not seem to be
significantly influenced by different (more or less aggressive) types of
treatment 2 3 13 18 21.
Given the proven radiosensitivity of the ACC, this tumour is, in fact, regarded as
a radiosensitive, even if not radiocurable, neoplasm, thus exclusive radiotherapy
can determine a reduction in tumour volume with a meaningful improvement in
the clinical symptoms 1 2 5 8 13 17 20 25 26.
Vikram et al. reported regression of the tumoural mass in 96% of 49 patients
treated only with radiotherapy, although in 93% of the cases they observed
recurrence of the disease within 5 years 24.
Although the surgical approach with attempts of oncological radicality, followed
by radiotherapy, remains the treatment of choice for ACC, also in the case of a
nasopharyngeal localization, exclusive radiotherapy, in those cases in which
surgery is contraindicated, for general reasons or for technical difficulties, offers
a valid therapeutic alternative guaranteeing good control of the disease and
minimal side-effects.

Biomedical Research 2017; 28 (14): 6441-6445
Adenoid cystic carcinoma of nasopharynx: a single-center Retrospective study.Shujun Ding1#, Tongai Jin2#, Min Xu3#, Yong Liang4, Shoufeng Wang2, Lingyun Lv5, De Huai2*
AbstractPurpose: To summarize the characteristics of Adenoid Cystic Carcinoma (ACC) arising fromnasopharynx by analysing 28 cases in a single center, in order to enhance the care of patients with theseunusual neoplasms.Patients and methods: This was a retrospective analysis of 28 patients with nasopharyngeal ACC whowere treated in Huai’an cancer hospital between 1997 and 2011. Kaplan-Meier estimation was used tocalculate Overall Survival (OS).Results: Most patients had locally-advanced lesions at the time of diagnosis. The most commonpresenting complaints were nasal obstruction and blood-stained snot. The peak incidence of the patients
our study is the 5th decade. In this study, 11 of 28 patients received radical surgery, and the restreceived non-surgery treatment (chemoradiotherapy or radiotherapy alone). The 5 y OS rate in surgicaltreatment group was higher than in nonsurgical treatment group (100% vs. 47.1%) and the survivalcurves showed OS in surgical group was better than that in non-surgical group (χ=3.844, P=0.05).
Conclusion: Adenoid Cystic Carcinoma (ACC) in the nasopharynx is an extremely rare entity. Surgeryfollowed by postoperative radiotherapy is the main stay of treatment. Locally advanced patients mayalso benefit from surgical treatment. Our data showed that treatment approach was an important factoraffecting the prognosis.

IntroductionAdenoid Cystic Carcinoma (ACC) is an uncommon malignant tumor, accounting for 3-5% of all neoplasms of the head and neck andapproximately 22% of all salivary gland cancers [1-3]. ACCs are rare variants of adenocarcinoma that most frequently arisen from majorsalivary glands included the parotid, submandibular, sublingual salivary glands, and minor salivary glands, which were located within the upperaerodigestive tract [4]. As demonstrated in the previous studies, ACC is most commonly found in the palate, followed by the paranasal sinusesand other sites of the oral cavity, while it’s rarely found in the nasopharyngeal cavity. Because previous studies have shown that primarynasopharyngeal adenocarcinoma (including ACC) represents less than 0.48% of all types of nasopharyngeal cancers [5,6]. In 1859, Billroth wasfirst described this tumor as the term cylindroma. Subsequently, the current name of ACC introduced by Spies has gained general acceptance[7]. ACC has a distinct propensity for frequent early Perineural Invasion (PNI), and late haematogenous distant metastasis, while rarely spreadto the lymph nodes. Furthermore, this tumor has a strong tendency to local invasion, which undoubtedly increases the difficulty of radicalresection [2,8-12]. In general, planned combined surgery and radiation therapy is the accepted standard of care for minor salivary glandmalignancy. Some studies revealed that the lesions in the nasal cavity or maxillary sinus were generally discovered at a late stage at the time ofISSN 0970-938X www.biomedres.info Biomed Res- India 2017 Volume 28 Issue 14 Biomedical Research 2017; 28 (14): 6441-64456441diagnosis, which increased the difficulty of surgery or even lost the chance of surgery [13,14]. ACC stands for a special diagnostic andtherapeutic challenge due to its extraordinary nature. This study aimed to review our long-term experience based on the study of twenty-eightpatients with nasopharyngeal ACC in the light of the most recent knowledge based on a review of the literature.

DiscussionACC is an uncommon malignant tumor. Several reports in recent years have occasionally shown ACC originates from other than the common sites such as cardia, breast, lung, esophagus [15-18]. While the primary site of the nasopharynx is exceedingly rare. The vast majority of nasopharyngeal carcinomas are keratinizing or non-keratinizing squamous cell carcinoma. Primary nasopharyngeal adenocarcinomas (included ACC) as a group are reported to occupy 0.48% in all types [5,6]. ACC is a tumor of an uncertain age. Not only the old but also the young can be involved. The peak incidence of the patients in our study was the fifth decade (47 y), which was similar to most studies in the literature [19-21]. Controversial also exists about the ratio of male to female. A meta- �analysis by Martin Rodriguez and the colleagues revealed that ACC was found to be more common among women [22]. While, our data revealed that there is no gender predominance between man and woman. Nasopharyngeal ACC was a rare malignancy with special biological features, which has different treatment strategies compared with the common nasopharyngeal cancers. The benefit of concomitant chemoradiotherapy for squamous and poorly differentiated cancers of head and neck has been proven. However, the clinical effort for locally advanced or inoperable salivary gland carcinomas is poorly understood. Taking its indolent clinical behaviour into consideration, surgery does represent a potential treatment option for the lesion. ACC also has distinct propensities for frequent early perineural invasion, local invasion and late haematogenous distant metastases, which is considered to be high-grade malignancy and should be treated with combined-modality therapy. Some efforts have been made on the optimal treatment approaches for patients experienced with nasopharyngeal ACC. Nasopharyngeal malignancies, no matter what kind of pathological types, often faced with a common problem that patients often present without local symptoms. In addition, ACC is characteristic by slow and insidious growth, often discovered at a late and locally advanced stage, as our results have described above [2,8-12]. Radical surgical resection is the main stay of treatment for early nasopharyngeal ACC. However, advanced lesions in the nasopharynx basically lost the chance of surgery. Even so, Schramm and Imola study revealed that patients with locally advanced stage can also benefit from surgical treatment [23]. They enrolled 23 patients presenting with T3-T4 salivary gland malignancies in the nasopharynx who received surgical resection and radiotherapy (6 patients received preoperative radiotherapy and 17 patients received postoperative radiotherapy). The outcomes were as follows: the 5 and 10 y disease free survival rates were 67% and 48%, respectively, and the 5 y local control rate was 77%. A retrospectively study conducted by Iseli et al. reviewed 183 patients with ACC, revealed that the 10 y local recurrence-free survival rate of radiotherapy alone was significantly worse (0%), compared with surgery alone (41.8%, P=0.002) and surgery followed by postoperative radiotherapy (43.5%, P=0.001) [24]. In the present study, our data revealed that the 5 y OS rate in surgical treatment group was higher than in nonsurgical treatment group (100% vs. 47.1%; χ2=3.844, P=0.05), which mainly because the small number of cases failed to highlight the advantages of the operation. In addition, what should to be mentioned was that patients receiving radiotherapy alone were more likely to have the lesions in the primary sites of pharyngeal or hypopharyngeal.
In addition, many studies reported in the literature are recommended surgery followed by postoperative radiotherapy for the management of ACC [25-27]. Posteroperative Radiotherapy (PORT) was mainly applied to patients with poor prognostic factors. Miglianico et al. in a retrospective study revealed that patients in PORT group had a higher 5 y locoregional control rates (78% vs. 44% for surgery alone, patients received surgical treatment,
�and the rest received non surgical treatment. The 5 and 10 y OS in non-surgery group were quite poor compared with the patients in surgery group. Our data showed that the 10 y OS rates in nasopharyngeal ACC were lower than those reported in the literature, which mainly cause by the advanced stage was considered medically unfit for surgery or patients refused surgery. Another reason could explain the poor prognosis of nasopharyngeal ACC, as the outcome described above. Because the lesion in the nasopharynx was proximity to surrounding essential structures such as the parapharyngeal space, skull base, cranial nerves, paranasal sinus, orbit or infratemporal fossa, there is a need to balance functional and cosmetic with oncologic consequences. The complex anatomy undoubtedly increased the difficulty of surgery, interfered with a complete surgical resection and even lost the chance of surgery. Previous reports have also indicated that tumors arising closer to the base of the skull, such as nasopharyngeal ACC, have worse outcomes, which resulted in low local control rate. Cervical lymph node status is an important prognostic predictor for salivary glands tumors. Recent and past studies are consistent in revealing a reduced survival in patients with positive lymph node at time of primary therapy, and the 5 y survival rate was significant different with or without cervical lymph node metastasis (44-48% vs. 73-77%) [28-30]. In spite of the low lymph node metastasis rate of ACC, for patients with clinically positive cervical lymph node, therapeutic neck dissection is still strongly recommended at the time of primary surgery followed by adjuvant RT, regardless of histology or site [20]. In our study, four patients had clinical or radiologic evidence of cervical node metastasis, however, only one patient accepted neck dissection with the evidence of metastatic ACC, the other three patients received radiotherapy. This may be another reason for relatively low survival.
Conclusion ACC in the nasopharynx is an extremely rare entity and continues to pose diagnostic and therapeutic challenges to physicians due to its biological behaviour. Surgery followed by postoperative radiotherapy may be the mainstay treatment, especially for patients presenting with early stage disease. Radiotherapy alone was used if the primary was considered unresectable, or if the patient refused surgery or was considered medically unfit for surgery. Our data showed that treatment approach might be an important factor affecting the prognosis of patients with advanced the nasopharyngeal ACC.
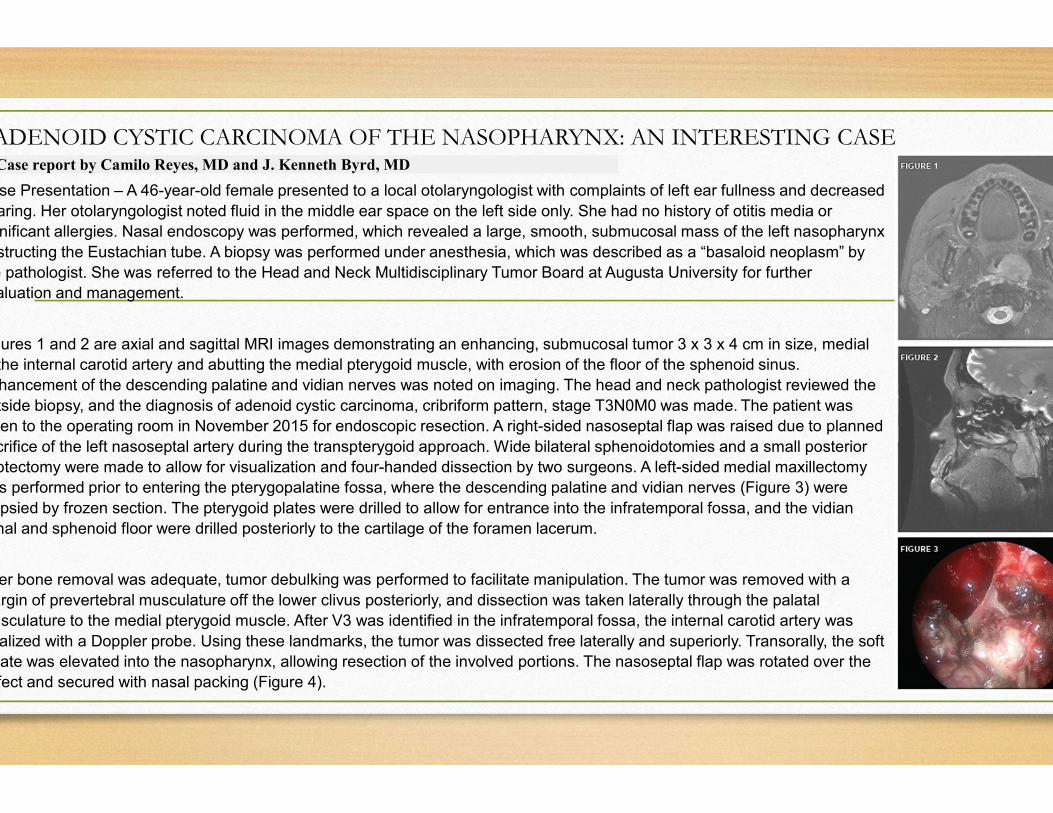
ADENOID CYSTIC CARCINOMA OF THE NASOPHARYNX: AN INTERESTING CASECase report by Camilo Reyes, MD and J. Kenneth Byrd, MD
Case Presentation – A 46-year-old female presented to a local otolaryngologist with complaints of left ear fullness and decreased
hearing. Her otolaryngologist noted fluid in the middle ear space on the left side only. She had no history of otitis media or
significant allergies. Nasal endoscopy was performed, which revealed a large, smooth, submucosal mass of the left nasopharynx
obstructing the Eustachian tube. A biopsy was performed under anesthesia, which was described as a “basaloid neoplasm” by
the pathologist. She was referred to the Head and Neck Multidisciplinary Tumor Board at Augusta University for further
evaluation and management.
Figures 1 and 2 are axial and sagittal MRI images demonstrating an enhancing, submucosal tumor 3 x 3 x 4 cm in size, medial
to the internal carotid artery and abutting the medial pterygoid muscle, with erosion of the floor of the sphenoid sinus.
Enhancement of the descending palatine and vidian nerves was noted on imaging. The head and neck pathologist reviewed the
outside biopsy, and the diagnosis of adenoid cystic carcinoma, cribriform pattern, stage T3N0M0 was made. The patient was
taken to the operating room in November 2015 for endoscopic resection. A right-sided nasoseptal flap was raised due to planned
sacrifice of the left nasoseptal artery during the transpterygoid approach. Wide bilateral sphenoidotomies and a small posterior
septectomy were made to allow for visualization and four-handed dissection by two surgeons. A left-sided medial maxillectomy
was performed prior to entering the pterygopalatine fossa, where the descending palatine and vidian nerves (Figure 3) were
biopsied by frozen section. The pterygoid plates were drilled to allow for entrance into the infratemporal fossa, and the vidian
canal and sphenoid floor were drilled posteriorly to the cartilage of the foramen lacerum.
After bone removal was adequate, tumor debulking was performed to facilitate manipulation. The tumor was removed with a
margin of prevertebral musculature off the lower clivus posteriorly, and dissection was taken laterally through the palatal
musculature to the medial pterygoid muscle. After V3 was identified in the infratemporal fossa, the internal carotid artery was
localized with a Doppler probe. Using these landmarks, the tumor was dissected free laterally and superiorly. Transorally, the soft
palate was elevated into the nasopharynx, allowing resection of the involved portions. The nasoseptal flap was rotated over the
defect and secured with nasal packing (Figure 4).

Discussion – Adenoid cystic carcinoma (ACC) accounts for 3 to 5 percent of all head and neck
malignancies, arising most frequently in minor salivary glands. It is the third most common
sinonasal malignancy overall, following squamous cell carcinoma and adenocarcinoma. Within
sinonasal tract, 47-60 percent arise from the maxillary sinus and 25-30 percent from the
nasal cavity.1,2 ACC of the nasopharynx is very rare, making up less than 0.5 percent of
nasopharyngeal cancers and with fewer than 100 cases reported in the literature.3
Histologically, cribriform (most common) and tubular patterns exhibit low-grade features, and
solid, high-grade pattern confers a worse prognosis. Perineural invasion is common in
adenoid cystic carcinoma and should be assessed preoperatively by thin-section, contrasted
. Approximately 60 percent of skull base ACC have been reported to exhibit perineural
spread.4 Nevertheless, the role of perineural spread on survival is still debated, as some
studies have demonstrated that perineural invasion is not associated with outcome.5,6 When
possible, however, large nerves in the area should be biopsied and cleared by frozen section
extradurally to theoretically prevent spread to the central nervous system.
Surgery followed by postoperative radiation is the treatment of choice for adenoid cystic
carcinoma of the skull base. Complete resection with negative margins, when possible,
associated with better outcome. A recent meta-analysis of skull base ACC concluded
positive or close tumor margins and tumor located in the ethmoid or sphenoid sinuses were
significant predictors of poor outcome.6 Surgical approach, endoscopic vs. open, must
selected according to patient tumor location in relation to neurovascular structures
Although no study has directly compared approaches, the endoscopic approach to
anterior cranial base appears to produce acceptable oncologic outcomes in appropriately
selected patients.7
Intensity-modulated radiotherapy is the most frequently used modality postoperatively,
although there may be a role for stereotactic radiosurgery or proton radiation in some
cases.8 There is no clear benefit to chemotherapy in the treatment of ACC, as in other
salivary malignancies. Regional lymphatic metastases are rare, and therefore, elective
neck dissection is not warranted. However, hematogenous spread can be seen in up to
40 percent of cases to the lungs and long bones and may occur even after 10 years. With
aggressive, multidisciplinary treatment, five- and 10-year overall survival may be as high
78 percent and 50 percent, respectively, although a significant number of these patients
be alive with disease.9 Local recurrences and isolated metastases may be re-resected
endoscopically and/or treated with stereotactic radiosurgery.
In this patient, early diagnosis allowed for complete endoscopic resection with negative
margins. As in other sinonasal and nasopharyngeal tumors, symptoms may be vague
lead to advanced stage at the time of diagnosis. In this case, the referring otolaryngologist
performed nasopharyngoscopy due to the unilateral middle ear effusion, leading
diagnosis of the tumor. The correct diagnosis of ACC by the pathologist, rather
nasopharyngeal carcinoma, was particularly important in selecting appropriate treatment
for this patient. Undifferentiated nasopharyngeal carcinoma, which may look similar to
solid pattern of ACC in a limited biopsy, is primarily treated with radiation or concurrent
chemoradiation, which is not an effective treatment for adenoid cystic carcinoma.

BÀN LUẬN-ACC vòm họng rất hiếm gặp.(<0.5% K vòm họng)
-Ung thư tuyến nước bọt phụ là một bệnh ung thư rấthiếm gặp, nhưng tỷ lệ ác tính lại cao hơn so với u của cáctuyến nước bọt chính
-Sự phân bố rải rác của các u tuyến nước bọt phụ và triệuchứng khá nghèo nàn và biểu hiện bằng triệu chứng củacác cơ quan lân cận:nghẹt mũi ,chảy máu mũi,ù tai… làmkhó khăn cho việc chẩn đoán,nên bệnh nhân thường đếnkhám ở giai đoạn muộn.
-Giải phẩu bệnh có 3 dạng,liên quan tiên lượng,trong đódạng rắn tiên lượng xấu nhất.
-Phẩu thuật kết hợp xạ trị là phương pháp điều trị chính.

REFERENCE• A rare case of adenoid cystic carcinoma of the nasopharynx manifesting as Horner’s syndrome: discussion and review of the
literature Un raro caso di carcinoma adenoido-cistico del rinofaringe manifestatosi con sindrome di Horner: discussione erevisione della letteratura F. Soprani, V. Armaroli, A. Venturini1 , E. Emiliani2 , D. Casolino
• Adenoid cystic carcinoma of nasopharynx: a single-center retrospective study. Shujun Ding1#, Tongai Jin2#, Min Xu3#,Yong Liang4 , Shoufeng Wang2 , Lingyun Lv5 , De Huai2
• Nasopharyngeal Adenoid Cystic Carcinoma: Report of Five Cases and Treatment Outcome Bijan Khademi*, HajarBahranifard**, Sayed Hamed Kabiri***, Samiraz Razzaghi****, Seyed Basir Hashemi**, Mahmood Shishegar**, MohammadMohammadianpanah*
• Research Article Open Access Quality in Primary Care (2015) 23 (5): 309-314 Research Article 2015 Insight MedicalPublishing Group Adenoid Cystic Carcinoma of the Head and Neck– literature review Pinakapani R, MDS
• Salivary Gland Tumors .Mayo Clinic
• Salivary Gland Cancer. Cancer.net
• Salivary Gland Disorders. Harvard Health
• Minor Salivary Glands.Radiology Reference Article
• Salivary Gland Cancer. American Cancer Society
• Oral Cancer.Johns Hopkins Medicine
CÁM ƠN QUÝ THẦY CÔ VÀ ANH CHỊĐÃ THEO DÕI