artículo traumato
TRANSCRIPT

Ia
WD
a
ARAA
KTEI
1
tjtitaatwns
2
fwpwn
2h
CASE REPORT – OPEN ACCESSInternational Journal of Surgery Case Reports 4 (2013) 276– 278
Contents lists available at SciVerse ScienceDirect
International Journal of Surgery Case Reports
j ourna l ho me pa ge: www.elsev ier .com/ locate / i j scr
ntra-articular correction of extra-articular tibial deformities with total kneerthroplasty
. Chua ∗, W. Wangepartment of Orthopaedic Surgery, National University Hospital, Singapore, 5 Lower Kent Ridge Road, Singapore 119074, Singapore
r t i c l e i n f o
rticle history:eceived 14 December 2012ccepted 17 December 2012vailable online 21 December 2012
eywords:otal knee arthroplastyxtra-articular deformitiesntra-articular correction
a b s t r a c t
INTRODUCTION: Extra-articular leg deformities may occur in the femur or tibia from mal-unions fromprevious trauma or metabolic bone disease. Secondary osteoarthritis at the knee occurs due to loss ofmechanical alignment of the limb. At surgery for total knee arthroplasty, mechanical alignment can berestored intra-articularly with appropriate bone cuts and soft tissue balancing.PRESENTATION OF CASE: We describe 2 case studies with extra-articular tibial deformities (9◦ and 24◦
varus deformity) which were corrected with a 1 stage procedure of total knee arthroplasty with intra-articular deformity correction.DISCUSSION: Patient selection, pre-operative considerations and surgical technique are discussed with
reference to the literature.CONCLUSION: One stage intra-articular correction of extra-articular deformity is suitable for mild degreesof varus deformities (<30◦). Staged corrective procedures with larger deformities in the tibia or femurcan be performed with extra-articular osteotomies on top of intra-articular corrections. Considerationshould be given to the use of computer navigation when conventional jigs cannot be applied to deformedbone.© 2
. Introduction
Patients with a history of malunion in tibial or femoral frac-ures invariably develop early secondary osteoarthritis at the kneeoint. Total knee arthroplasty (TKA) in such patients aims not onlyo restore function and relieve pain, but also to restore the mechan-cal axis of the leg. Current literature suggests 3 approaches to thisechnically difficult procedure1: firstly, a 2 stage procedure of extra-rticular osteotomy followed by total knee arthroplasty, secondly,
one stage procedure where the osteotomy and TKA are done athe same operation or thirdly, a one stage intra-articular correctionith TKA. We describe case studies of 2 patients with tibial malu-ions and secondary osteoarthritis in the knee managed with a onetage intra-articular correction.
. Case 1
A 50-year-old male presented with a history of 2 previousractures of his right tibia. These had been managed surgically
ith plating. Metalwork had been removed 10 years prior toresentation except for 1 interfragmentary screw. He presentedith gradually worsening right knee pain over the last 3–5 years,ow being able to ambulate for a maximum of 10 min with∗ Corresponding author. Tel.: +65 91139864; fax: +65 64635191.E-mail address: wei liang [email protected] (W. Chua).
210-2612/$ – see front matter © 2012 Surgical Associates Ltd. Published by Elsevier Ltdttp://dx.doi.org/10.1016/j.ijscr.2012.12.001
012 Surgical Associates Ltd. Published by Elsevier Ltd. All rights reserved.
difficulty going downstairs. On clinical examination, he had a varusdeformity of his knee and a range of motion of 0–140◦. Radio-graphic measurements revealed 9◦ of varus deformity with 11◦ ofrecurvatum.
At operation, the remaining screw was removed, followed bya standard medial parapatellar approach to the knee. Femoraland tibial cuts were achieved with pre-operative planning,intramedullary femur jig and an extramedullary tibial jig. Soft tis-sue releases include deep medial collateral and posterior releasefollowed by osteophyte resection at the posterior medial tibialmargin. A fixed bearing posterior stabilised implant was usedalong with an offset tibial stem (4 mm lateral) that bypassed theremaining screw hole. The patient had an uncomplicated 9-dayinpatient stay before being discharged.
The post-operative long leg films showed a mechanical align-ment of 0◦. The patient was followed up regularly for 3years and achieved a post-operative range of motion of 0–120◦
(Fig. 1).
3. Case 2
A 67-year-old lady presented with left knee pain and a progres-sive varus deformity of her left leg. She previously had a stress
fracture of her left tibia, which was managed surgically with plat-ing 8 years ago. Premorbidly she was independently ambulant buthad progressively worsening left knee pain. On clinical examinationshe had a severe varus deformity with a range of motion of 0–110◦.. All rights reserved.
CASE REPORT – OPEN ACCESSW. Chua, W. Wang / International Journal of Surgery Case Reports 4 (2013) 276– 278 277
Rn
wawtrlatTu
my
4
istc
t3Tpro1
Meticulous pre-operative planning is imperative in such cases.One has to consider the degree of deformity which may appearin 3 planes (coronal, sagittal and axial). Secondly, the cuts whichare performed perpendicular to the mechanical axis should not
Fig. 1. Long leg films of Case 1 before and after.
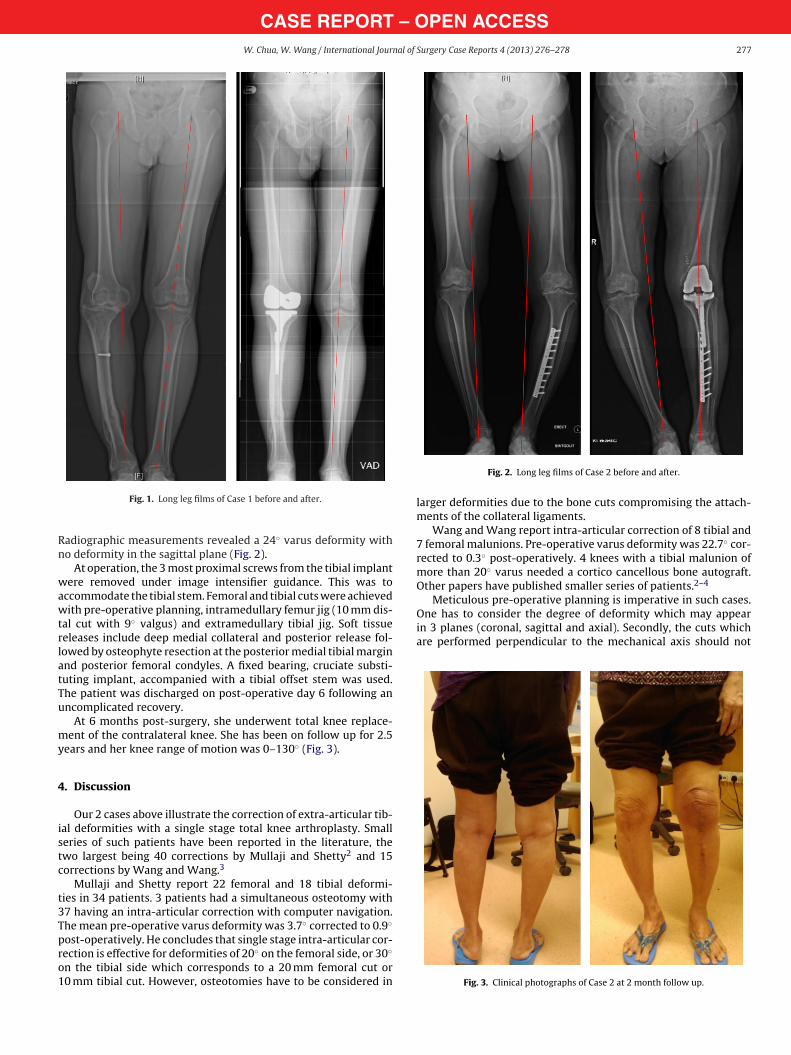
adiographic measurements revealed a 24◦ varus deformity witho deformity in the sagittal plane (Fig. 2).
At operation, the 3 most proximal screws from the tibial implantere removed under image intensifier guidance. This was to
ccommodate the tibial stem. Femoral and tibial cuts were achievedith pre-operative planning, intramedullary femur jig (10 mm dis-
al cut with 9◦ valgus) and extramedullary tibial jig. Soft tissueeleases include deep medial collateral and posterior release fol-owed by osteophyte resection at the posterior medial tibial marginnd posterior femoral condyles. A fixed bearing, cruciate substi-uting implant, accompanied with a tibial offset stem was used.he patient was discharged on post-operative day 6 following anncomplicated recovery.
At 6 months post-surgery, she underwent total knee replace-ent of the contralateral knee. She has been on follow up for 2.5
ears and her knee range of motion was 0–130◦ (Fig. 3).
. Discussion
Our 2 cases above illustrate the correction of extra-articular tib-al deformities with a single stage total knee arthroplasty. Smalleries of such patients have been reported in the literature, thewo largest being 40 corrections by Mullaji and Shetty2 and 15orrections by Wang and Wang.3
Mullaji and Shetty report 22 femoral and 18 tibial deformi-ies in 34 patients. 3 patients had a simultaneous osteotomy with7 having an intra-articular correction with computer navigation.he mean pre-operative varus deformity was 3.7◦ corrected to 0.9◦
ost-operatively. He concludes that single stage intra-articular cor-
ection is effective for deformities of 20◦ on the femoral side, or 30◦n the tibial side which corresponds to a 20 mm femoral cut or0 mm tibial cut. However, osteotomies have to be considered in
Fig. 2. Long leg films of Case 2 before and after.
larger deformities due to the bone cuts compromising the attach-ments of the collateral ligaments.
Wang and Wang report intra-articular correction of 8 tibial and7 femoral malunions. Pre-operative varus deformity was 22.7◦ cor-rected to 0.3◦ post-operatively. 4 knees with a tibial malunion ofmore than 20◦ varus needed a cortico cancellous bone autograft.Other papers have published smaller series of patients.2–4
Fig. 3. Clinical photographs of Case 2 at 2 month follow up.

– O2 nal of
catasti
fibdaf(fo
nndtUugnt
atOts
5
Tco
1
2
3
4
5
OTpc
CASE REPORT78 W. Chua, W. Wang / International Jour
ompromise the attachments of the collateral ligaments. Addition-lly, in severe deformities, augments and stemmed implants haveo be on hand if required to achieve stable fixation. Medial-lateralnd flexion-extension balance has to be achieved with extensiveoft tissue release, and if the deformity is too severe to achieve softissue balance, extra-articular osteotomies should be performednstead.
Lonner et al.5 stated concerns of a single stage TKA where theemoral component may not sit flush on concave cut bone lead-ng to early failure. Additionally, he had concerns that there woulde ligamentous imbalance in extension in large deformities. Heescribed a series of 11 knees with femoral deformities treated with
single stage femoral osteotomy and TKA. Fixation options of theemoral osteotomy include blade plate (7 patients), retrograde nail2 patients) and femoral long stem (2 patients). One patient withemoral long stem fixation underwent non-union of the femoralsteotomy. All other femoral osteotomies healed within 16 months.
Klein et al.4 and Kim et al.6 both emphasise the use of computeravigation in one stage intra-articular correction as using computeravigation. Conventional intramedullary jigs were not usable ineformed femurs and tibias and the surgeon can implant the pros-hesis in a position consistent to the true mechanical axis of the leg.sing computer navigation also allows one to use software to sim-late the femoral component size thus achieving flexion-extensionap balance. In populations where coronal femoral bowing is a sig-ificant factor, computer navigation bypasses that concern by usinghe femoral head and knee centre to compute the mechanical axis.
Additional points to consider are that previously implanted met-lwork should be retained as far as possible to avoid compromiseo the skin condition by having as few skin incisions as possible.nly sufficient metalwork should be removed for implantation of
he knee prosthesis. The tibial stem component should bypass thetress risers created from where the screws have been removed.
. Conclusion
There are roles for both intra- and extra-articular corrections.he majority of deformities are within the range of intra-articularorrections, thus achieving the potential benefits of a less invasiveperation, shorter hospital stay and shorter rehabilitation period.
6
pen Accesshis article is published Open Access at sciencedirect.com. It is distribermits unrestricted non commercial use, distribution, and reproductredited.
PEN ACCESSSurgery Case Reports 4 (2013) 276– 278
However, extra-articular osteotomies have to be considered inmore severe deformities. The use of computer navigation is usefulif the use of traditional jigs is precluded by deformities, and also toobtain alignment of the total knee prosthesis with the mechanicalaxis.
Conflict of interest statement
None.
Funding
None.
Ethical approval
Written informed consent was obtained from the patient forpublication of this case report and accompanying images.
Author contributions
Weiliang Chua collected the data and wrote the manuscript.Wilson Wang supervised the research work.
References
. Koenig JH, Maheshwari AV, Ranawat AS, Ranawat CS. Extra-articular defor-mity is always correctable intra-articularly: in the affirmative. Orthopedics2009;32(September (9)).
. Mullaji A, Shetty GM. Computer-assisted total knee arthroplasty for arthritis withextra-articular deformity. Journal of Arthroplasty 2009;24(December (8)), 1164-9.e1.
. Wang JW, Wang CJ. Total knee arthroplasty for arthritis of the knee withextra-articular deformity. Journal of Bone and Joint Surgery 2002;84-A(October(10)):1769–74.
. Klein GR, Austin MS, Smith EB, Hozack WJ. Total knee arthroplasty usingcomputer-assisted navigation in patients with deformities of the femur and tibia.Journal of Arthroplasty 2006;21(February (2)):284–8.
. Lonner JH, Siliski JM, Lotke PA. Simultaneous femoral osteotomy and total kneearthroplasty for treatment of osteoarthritis associated with severe extra-articulardeformity. Journal of Bone and Joint Surgery 2000;82(March (3)):342–8.
. Kim KI, Ramteke AA, Bae DK. Navigation-assisted minimal invasive total kneearthroplasty in patients with extra-articular femoral deformity. Journal of Arthro-plasty 2010;25(June (4)), 658.e17–658.e22.
uted under the IJSCR Supplemental terms and conditions, whichion in any medium, provided the original authors and source are