anestesia en el trasplante pulmonar - aymon.es · • reduce la necesidad de sng • evita...
TRANSCRIPT
ANESTESIA EN EL TRASPLANTE
PULMONAR
Ana González Román
Sº Anestesia y Reanimación
Hospital Universitario Puerta de Hierro Majadahonda
RECUERDO HISTORICO
"El milagro de San Cosme y San Damián“ S. XII-XIII

RECUERDO HISTORICO
• 1963 → Hardy realiza 1er Tx pulmonar en humanos.
• 1968 → Denton Cooley
Fritz Derom
• 1983 → Cooper (Toronto, Canadá)
• 1990 → Ramón Arcas (Hospital Gregorio Marañón, España)
• INMUNOSUPRESION??
• 1990-2006 España → 1641 Tx pulmonares (36% EPOC).

ACTIVIDAD tx pulmon españa

El equipo de Coordinación…
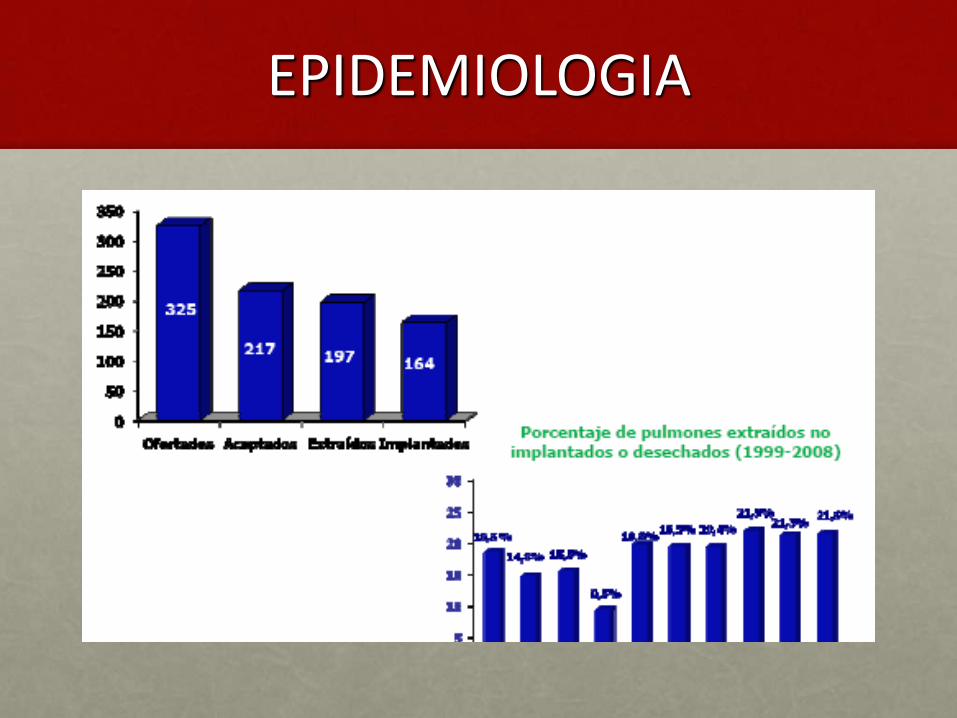
EPIDEMIOLOGIA
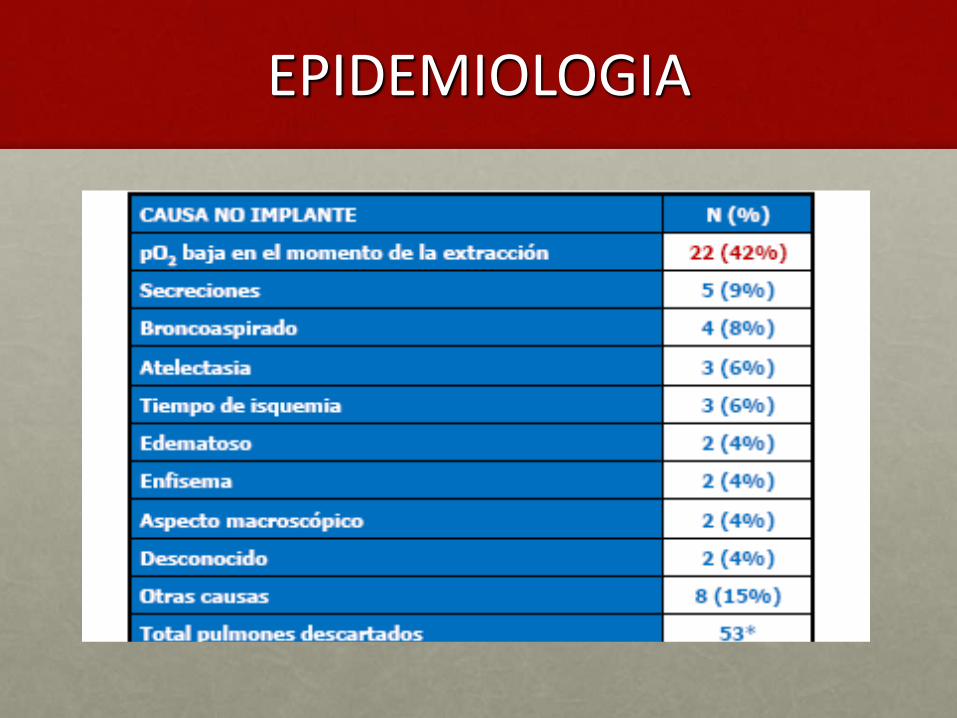
EPIDEMIOLOGIA

JAMA 2010; 304:2620-2627
Donante
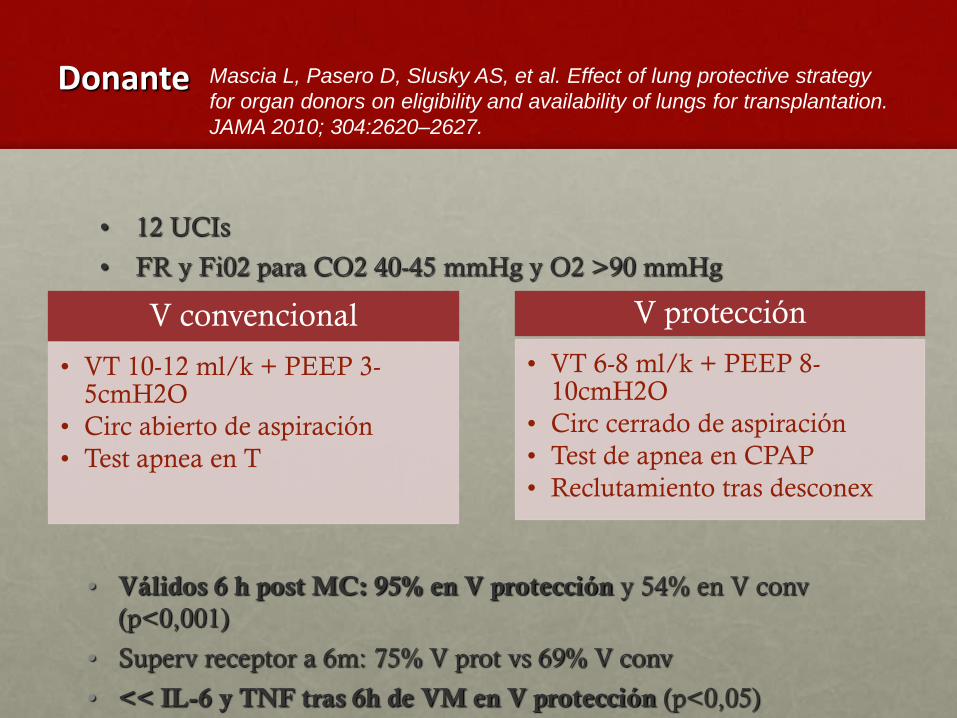
• 12 UCIs
• FR y Fi02 para CO2 40-45 mmHg y O2 >90 mmHg
• Válidos 6 h post MC: 95% en V protección y 54% en V conv
(p<0,001)
• Superv receptor a 6m: 75% V prot vs 69% V conv
• << IL-6 y TNF tras 6h de VM en V protección (p<0,05)
Mascia L, Pasero D, Slusky AS, et al. Effect of lung protective strategy
for organ donors on eligibility and availability of lungs for transplantation.
JAMA 2010; 304:2620–2627.
V convencional
• VT 10-12 ml/k + PEEP 3-5cmH2O
• Circ abierto de aspiración
• Test apnea en T
V protección
• VT 6-8 ml/k + PEEP 8-10cmH2O
• Circ cerrado de aspiración
• Test de apnea en CPAP
• Reclutamiento tras desconex
¿Cuándo está indicado el trasplante?
• ¿La gravedad de la enfermedad justifica la consideración del trasplante?
• Clase funcional NYHA III-IV.
• Expectativa de vida limitada 1-2 a.
• Deterioro progresivo a pesar de tto médico optimizado.
• Limite edad:
• Tx unipulmonar → 65 a.
• Tx bipulmonar → 60 a.
• ¿Existe enfermedad de otro órgano que contraindique el procedimiento?
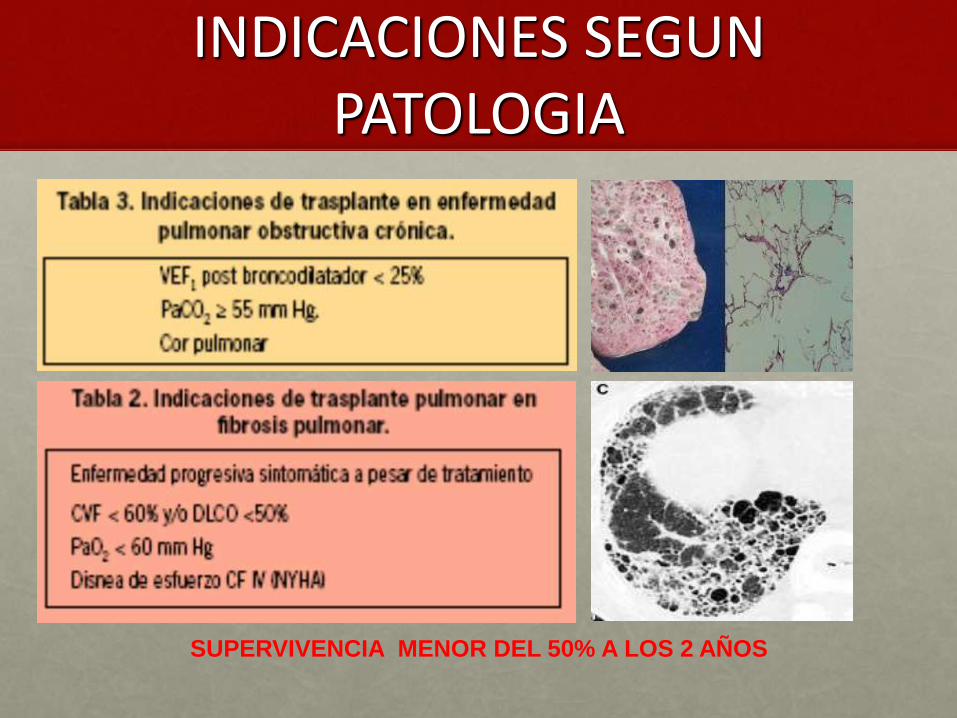
INDICACIONES SEGUN PATOLOGIA
SUPERVIVENCIA MENOR DEL 50% A LOS 2 AÑOS
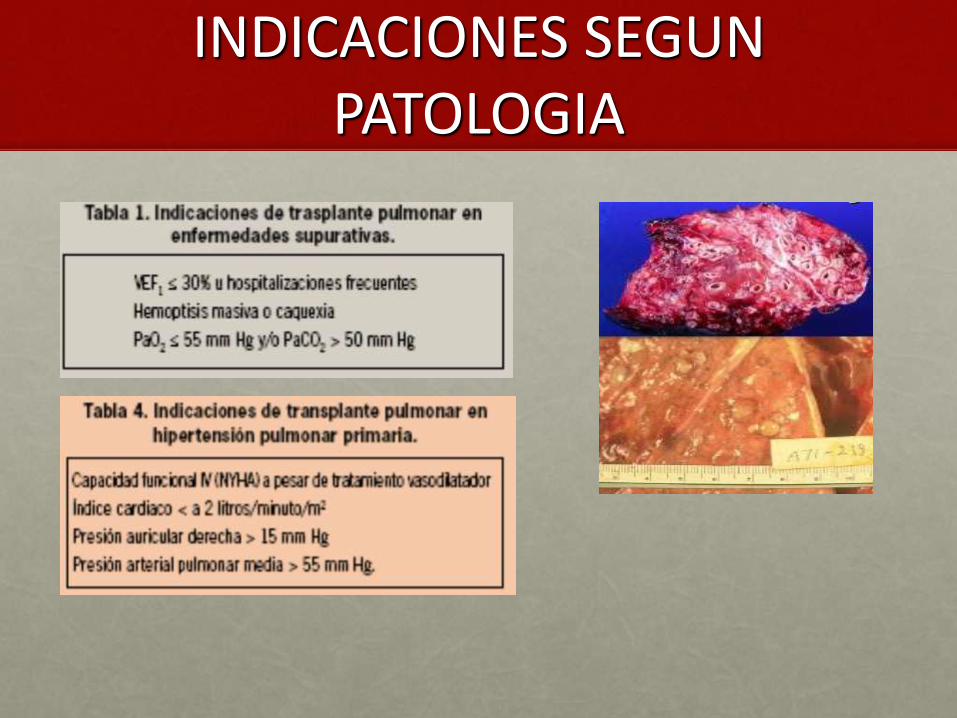
INDICACIONES SEGUN PATOLOGIA
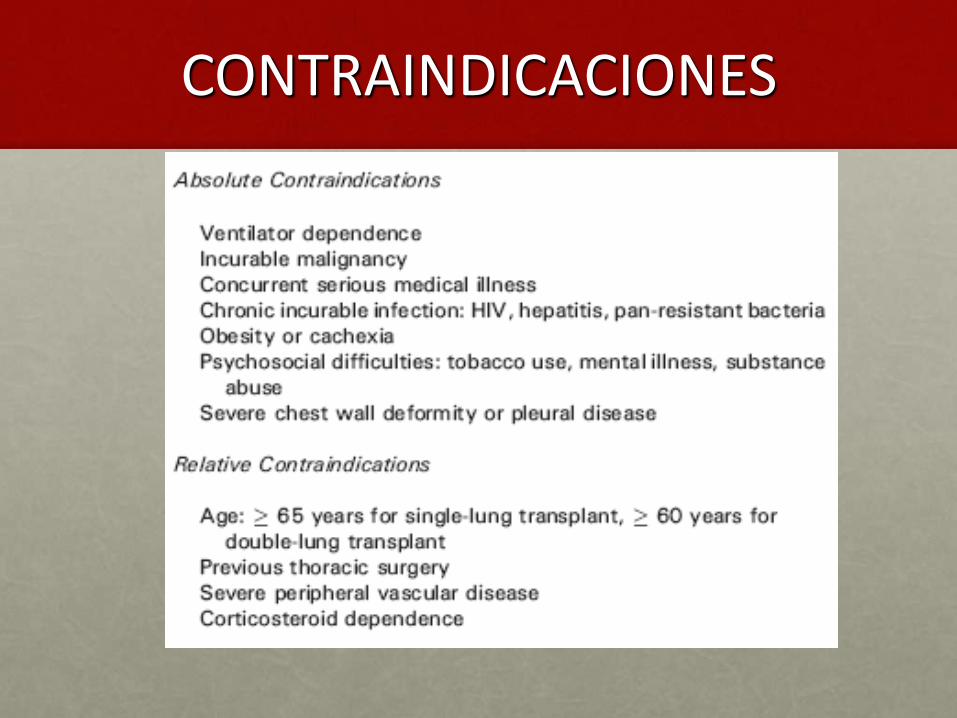
CONTRAINDICACIONES
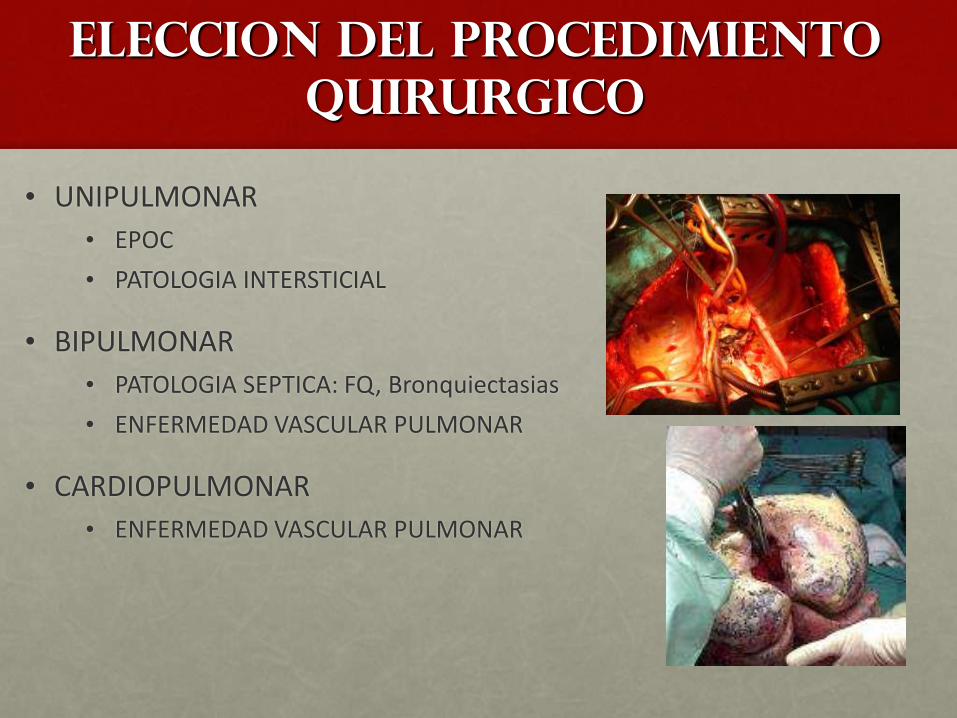
ELECCION DEL PROCEDIMIENTO
QUIRURGICO
• UNIPULMONAR
• EPOC
• PATOLOGIA INTERSTICIAL
• BIPULMONAR
• PATOLOGIA SEPTICA: FQ, Bronquiectasias
• ENFERMEDAD VASCULAR PULMONAR
• CARDIOPULMONAR
• ENFERMEDAD VASCULAR PULMONAR
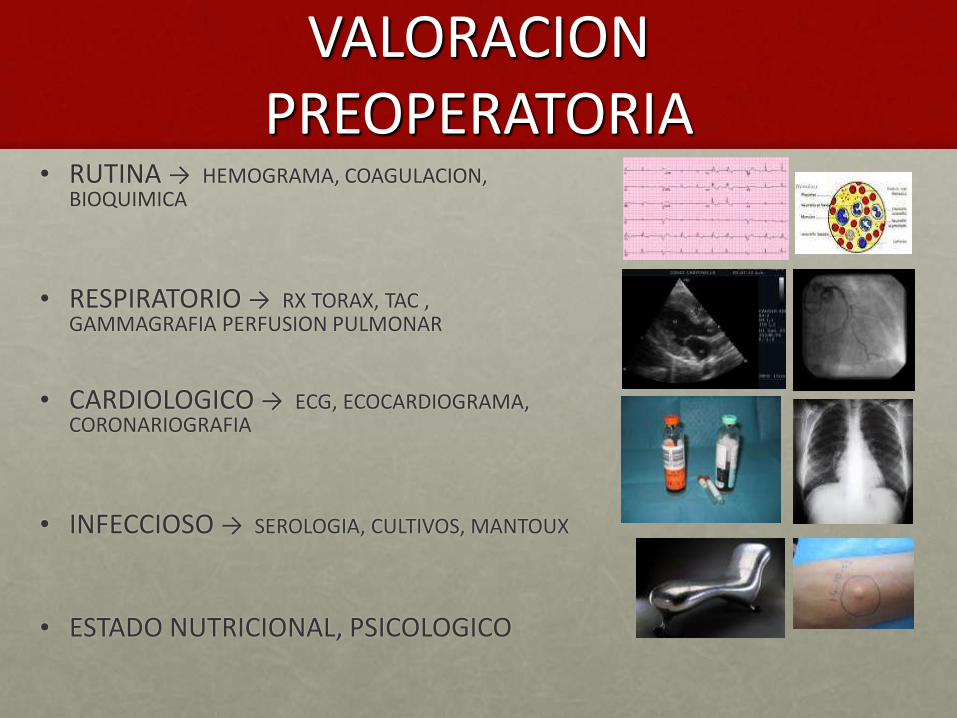
VALORACION PREOPERATORIA
• RUTINA → HEMOGRAMA, COAGULACION, BIOQUIMICA
• RESPIRATORIO → RX TORAX, TAC , GAMMAGRAFIA PERFUSION PULMONAR
• CARDIOLOGICO → ECG, ECOCARDIOGRAMA, CORONARIOGRAFIA
• INFECCIOSO → SEROLOGIA, CULTIVOS, MANTOUX
• ESTADO NUTRICIONAL, PSICOLOGICO
Valoración preoperatoria
• Fisiopatología de la enfermedad de base
• Patología asociada
• Valoración cardiológica completa
( ECG, Eco , Coronariografía ( HTP, FE biventricular)
• Estado nutricional
• Rehabilitación con fisioterapia
• Valoración psiquiátrica
Fisiopatología
• EPOC: Disminución de flujos espiratorios, atrapamiento aéreo,
↑ volumen residual y espacio muerto.
• Enf. bronquiectasica ( patrón mixto).
• Enf. intersticiales : Restricción de todos los volúmenes
pulmonares, disminución de la elasticidad y complianza.
• Enf. vascular pulmonar: Primaria o secundaria a enf. cardiaca o
extracardiaca.
Ventilacion MecaNica no invasiva
Indicaciones
Fallo respiratorio hipercápnico
• IRCA
• Fallo respiratorio postextubación
• En lista de espera de TX PULMONAR
• Pacientes no candidatos a IOT
Fallo respiratorio hipoxémico
. Edema cardiogénico sin inestabilidad HD
. Fallo respiratorio postoperatorio
. Pacientes no candidatos a intubación

VMNI
Ventajas
• Aplicación de forma intermitente
• Fácil de retirar y reinstaurar
• Mayor confort ?
• Reduce necesidad de sedación
• Reduce la necesidad de SNG
• Evita complicaciones asociadas a la IOT ( menor nº de infecciones nosocomiales)
• Menor incidencia de atrofia muscular
• Instauración precoz
• Reducción de tiempo de estancia en UCPQ
MANEJO INTRAOPERATORIO

Monitorización
• Paciente despierto
• Premedicación ligera
• ECG 5 derivaciones
• SatO2
• ETCO2
• PAI
• Catéter Swan-Ganz
(PAP,PVC,GC,SVO2,RVP,RVS)
• ECO Transesofágico
• Tª,TOF,BIS,INVOS
• Monitorización respiratoria y
gasometrías seriadas
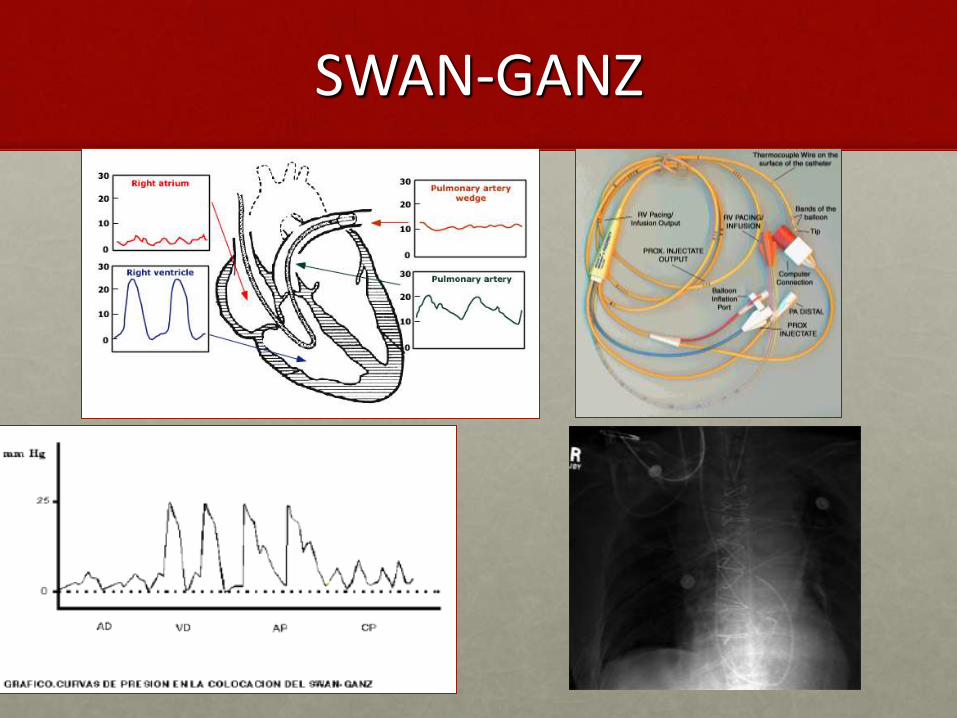
SWAN-GANZ
Inducción
• Lenta y progresiva ( ↓↓brusca de catecolaminas endógenas: hipotensión)
• Farmacos poco depresores
• Inotrópicos cargados
• Parámetros ventilatorios prefijados.
EVITAR VENTILACION MANUAL
• Tubo doble luz (fibrobroncoscopio)
En BQ y FQ tubo de una luz previo para limpieza de secreciones
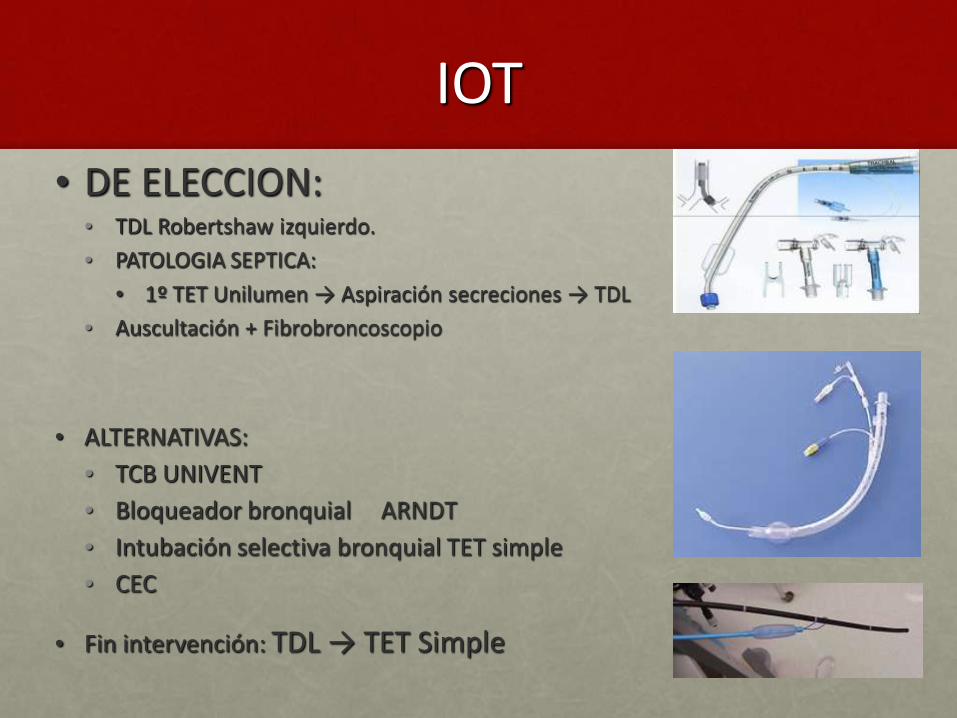
IOT
• DE ELECCION: • TDL Robertshaw izquierdo.
• PATOLOGIA SEPTICA:
• 1º TET Unilumen → Aspiración secreciones → TDL
• Auscultación + Fibrobroncoscopio
• ALTERNATIVAS:
• TCB UNIVENT
• Bloqueador bronquial ARNDT
• Intubación selectiva bronquial TET simple
• CEC
• Fin intervención: TDL → TET Simple
Ventilación en paciente
con EPOC
Objetivos:
- Evitar atrapamiento aéreo
- Preservar tiempo espiratorio
Métodos:
- Evitar VT elevados
- Evitar Frecuencias Respiratorias elevadas
- Acortar la relación I:E ( 1:3-1:4- 1:5). Desconexiones intermitentes
- Flujos inspiratorios elevados
Mantener Pplateau < 25-30 cmH2O
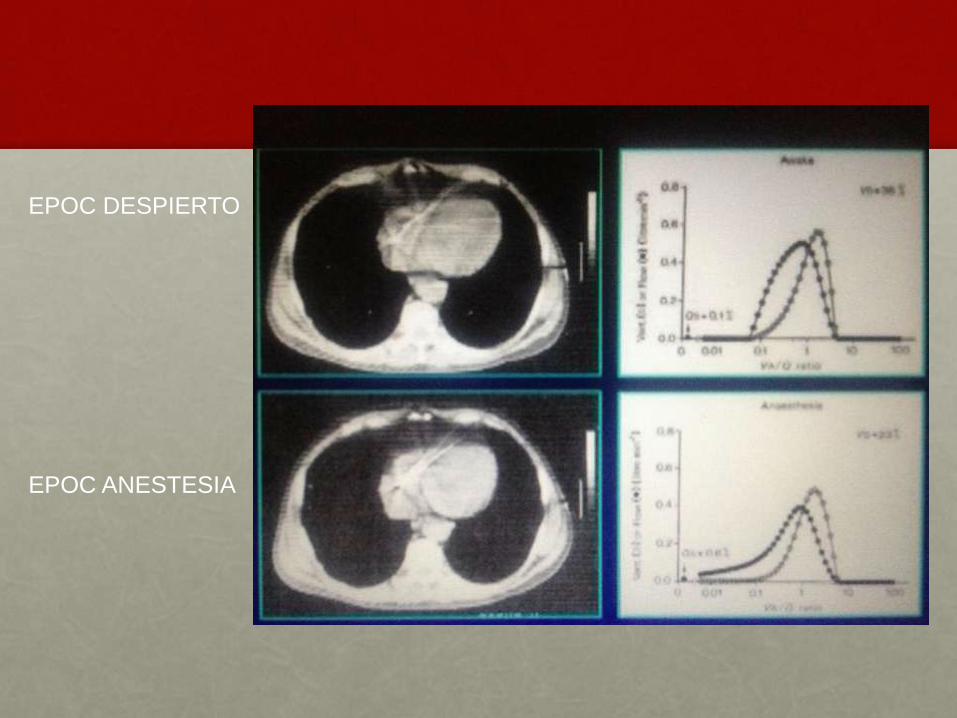
EPOC DESPIERTO
EPOC ANESTESIA
Enfisema severo
MONITORIZACION
. Vía central yugular ipsilateral abordaje alto
. Paciente despierto : dtco clínico de neumotorax
PATRON VENTILATORIO
Evitar P intratorácicas altas
• VT bajos
• FR normales→ HIPERCAPNIA PERMISIVA
• Relación I/E : 1/4, 1/5, desconexiones intermitentes
OJO!! NEUMOTORAX PULMON DEPENDIENTE

Enfermedad de base
Hipercapnia permisiva
• Vasodilatación cerebral.
• Aumento de la PIC
• Narcosis
• Convulsiones
• Depresor miocárdico. Disminuye la contractilidad
• Incremento de la actividad simpática
Paso de respiración espontánea
a ventilación mecánica
• -↑ P.intratorácica media-↓ Retorno venoso ( En obstructivos- autopeep; restrictivos-disminución distensibilidad)
• -Hiperinsuflación en pacientes enfisematosos( Atrapamiento- neumotaponamiento- test de apnea)
• Fenómeno de interdependencia ventricular( la disfunción del VD reduce la complianza diastólica del VI por desviación del tabique IV)

Interacción con el V.I.
• Interdependencia ventricular
– Crecimiento en espacio pericárdico limitado
– Comparten septo interventricular
– Llenado izquierdo comprometido: GC reducido
Fases del Tx
PRIMER PULMON
-Peor relación V/Q
-Disfunción precoz del
injerto con > frecuencia
• Clampaje bronquial
• Clampaje arterial
• Reperfusión
SEGUNDO PULMON
. Clampaje bronquial
• Clampaje arterial
• Reperfusión
CLAMPAJE BRONQUIAL
Ventilación unipulmonar→SHUNT→HIPOXIA
- Reclutamiento
- FiO2 100%
- CPAP
- PEEP
- Ventilación intermitente
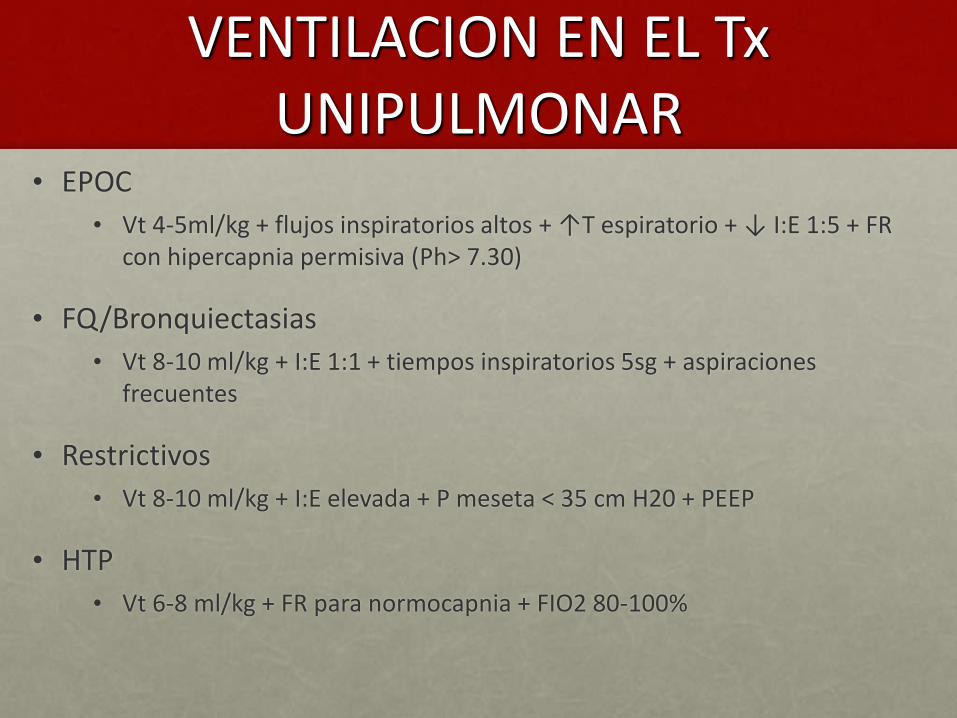
VENTILACION EN EL Tx UNIPULMONAR
• EPOC
• Vt 4-5ml/kg + flujos inspiratorios altos + ↑T espiratorio + ↓ I:E 1:5 + FR con hipercapnia permisiva (Ph> 7.30)
• FQ/Bronquiectasias
• Vt 8-10 ml/kg + I:E 1:1 + tiempos inspiratorios 5sg + aspiraciones frecuentes
• Restrictivos
• Vt 8-10 ml/kg + I:E elevada + P meseta < 35 cm H20 + PEEP
• HTP
• Vt 6-8 ml/kg + FR para normocapnia + FIO2 80-100%
VENTILACION EN EL Tx BIPULMONAR SECUENCIAL
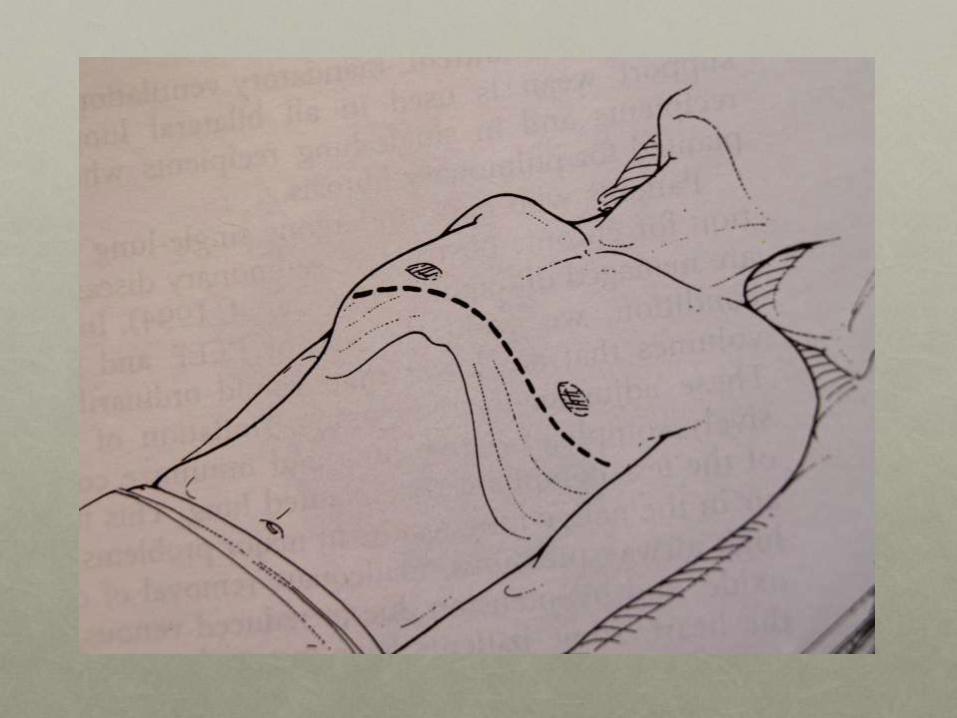
• Toracotomía bilateral
• Inicio pulmón con peor V/Q
• Clampaje arteria 2º pulmón:
¡↑RIESGO EDEMA REPERFUSION + ENTRADA EN CEC!
• MANEJO
• Vt 6-8ml/kg + I:E 1:2 - 1:3 + PEEP 5-10 cm H2O + FIO2 ↑
CLAMPAJE ARTERIA PULMONAR
-Aumento RVP ↑ PAP
EVITAR FVD
- Vasodilatadores pulmonares ( NO, PGs)
- Inodilatadores ( dobutamina, milrinona)
- Noradrenalina para mantener PAM ¡PRESION DE PERFUSION!
ECO TRANSESOFAGICO
Valoración disfunción VD, anastomosis vasculares, detección
precoz de trombosis
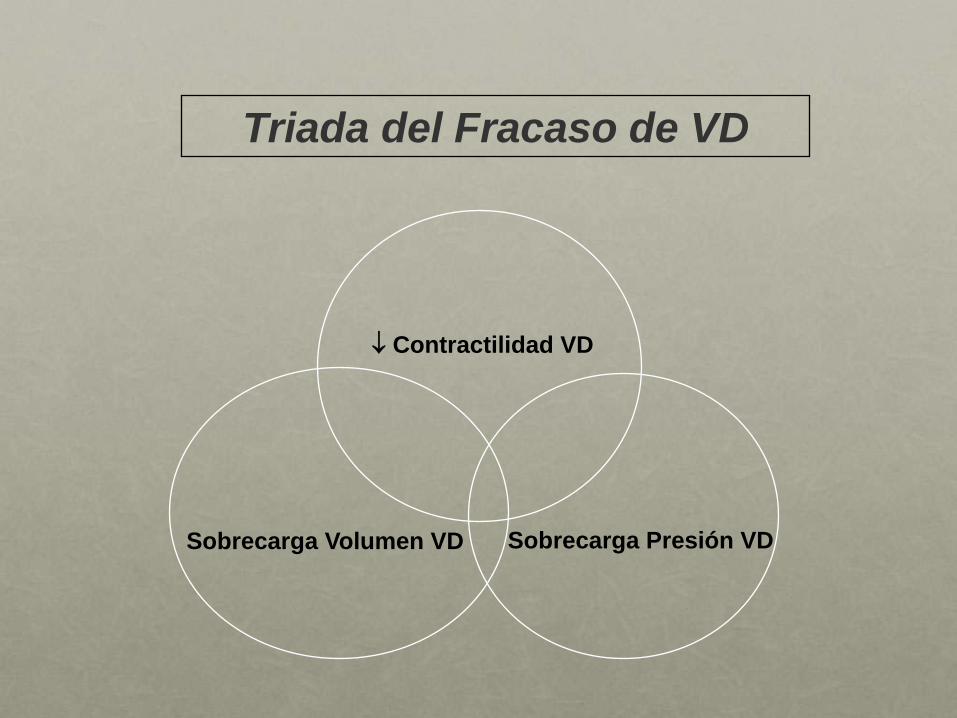
Sobrecarga Presión VD Sobrecarga Volumen VD
Contractilidad VD
Triada del Fracaso de VD
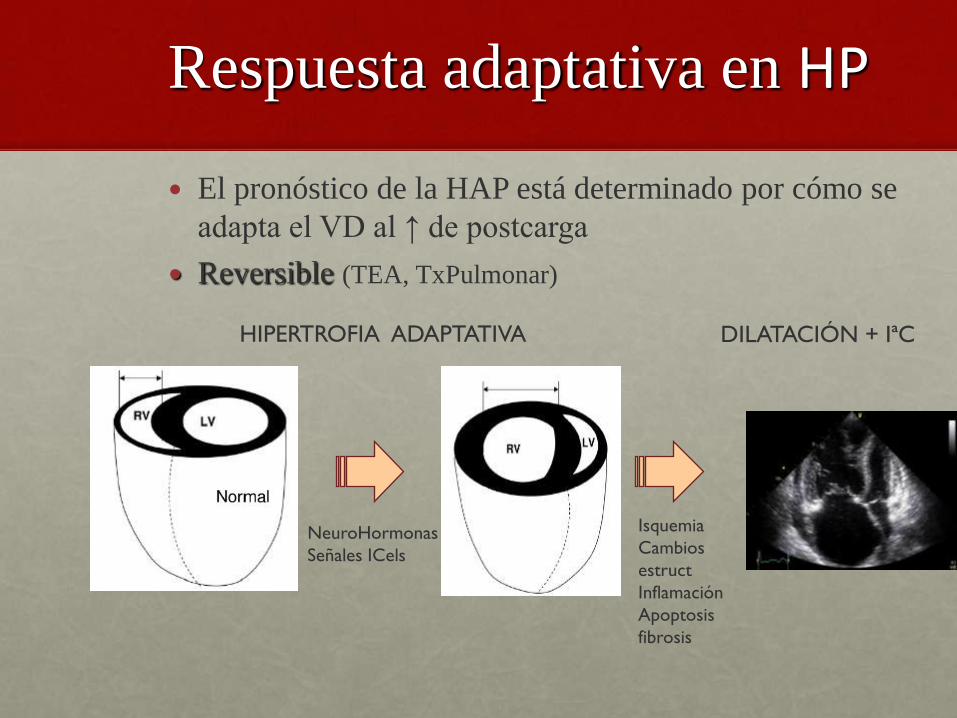
Respuesta adaptativa en HP
El pronóstico de la HAP está determinado por cómo se
adapta el VD al ↑ de postcarga
Reversible (TEA, TxPulmonar)
HIPERTROFIA ADAPTATIVA DILATACIÓN + IªC
Isquemia
Cambios
estruct
Inflamación
Apoptosis
fibrosis
NeuroHormonas
Señales ICels
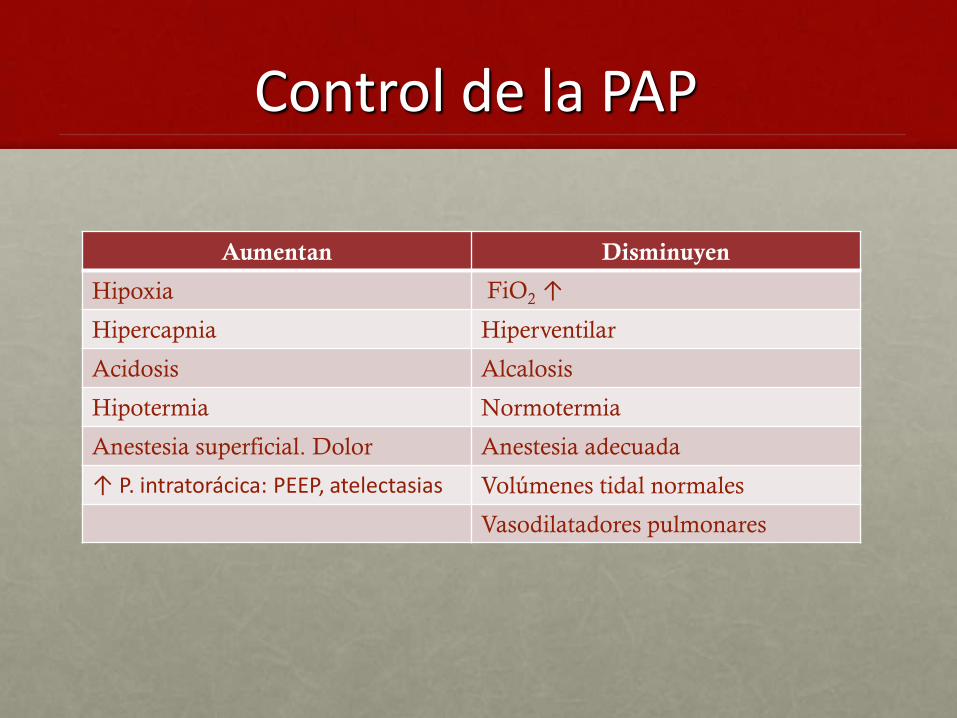
Control de la PAP
Aumentan Disminuyen
Hipoxia FiO2 ↑
Hipercapnia Hiperventilar
Acidosis Alcalosis
Hipotermia Normotermia
Anestesia superficial. Dolor Anestesia adecuada
↑ P. intratorácica: PEEP, atelectasias Volúmenes tidal normales
Vasodilatadores pulmonares

Vasodilatadores pulmonares
inhalados
↓ RVP
Poca repercusión TAS
Mejoran
ventilación/perfusión
Mejoran oxigenación arterial
iNO
( 10 – 40 ppm)
t½ = 2 – 6 sg
Admón. contínua
HP de rebote
Toxicidad clínica ( metaHb, N02
)
Técnicamente complejo
Iloprost
(10-20 µg)
t½ = 20 -30
min
Admón. 15 – 30 min.
Fácil aplicación.
Nebulizador ultrasónica r.inspir
Milrinona
NTG
De elección



HEMODINAMICA EN EL Tx PULMONAR
NPS, NTG y la PGI2, producen una vasodilatación indiscriminada en todo el parénquima pulmonar. El resultado es un efecto favorable sobre la resistencia venosa pulmonar (RVP) y la resistencia venosa sistémica (RVS), pero por otro lado aumenta el cortocircuito arteriovenoso (Qs/Qt), con lo que disminuye la tensión parcial de oxígeno arterial (PaO2). En contrapartida, el •NO reduce la RVP, no modifica la RVS y, muy importante, aumenta la PaO2 y reduce el Qs/Qt
CAUSAS DE CEC
•Hipoxia
•HTP
•FVD
•Dificultades técnicas
•Cirugía cardíaca asociada

¿CUANDO ENTRAR EN CEC?
• INDICACIONES:
• IC< 2 l/min/m
• SVO2 < 60%
• PAM < 50-60 mm Hg
• Sat < 85%
• Ph < 7
• EFECTOS SECUNDARIOS
• Disfunción de injerto
• ↑ tiempo quirúrgico
• Sobrecarga líquidos
• ↑ Necesidades transfusión
Manejo de CEC
• Heparinización: 3mg/K inicial; 1mg/k/h. ACT>450
• Normotermia→ PAM 50-60
• Ultrafiltración para evitar hemodilución y politransfusión
• Antifibrinolíticos ( tranexámico)
• Reversión heparina con protamina 1/1,5
• En perfusiones largas coagulopatía (hemoderivados: plasma,plaquetas, fibrinogeno)
• TROMBOELASTOGRAMA
Objetivos en la desconexión CEC
INICIAR LA VENTILACIÓN ANTES DE PERFUNDIR
- Prevención del FRACASO VENTRICULO DCHO
- Corrección de la COAGULACION
- Mantenimiento de la NORMOTERMIA
Sobrecarga Presión VD Sobrecarga Volumen VD
Contractilidad VD
Triada del Fracaso de VD

REPERFUSIÓN
- Reexpansión del pulmón implantado
(VT 6- 8 ml/kg , PEEP 6-10, Gasometrías seriadas)
- Desclampaje progresivo REPERFUSIÓN CONTROLADA
( compresión digital→ Hiperaflujo : aumento brusco de ETCO2)
- Arritmias
- Desviación del GC por ↓↓ brusca de RVP (
normovolemia)
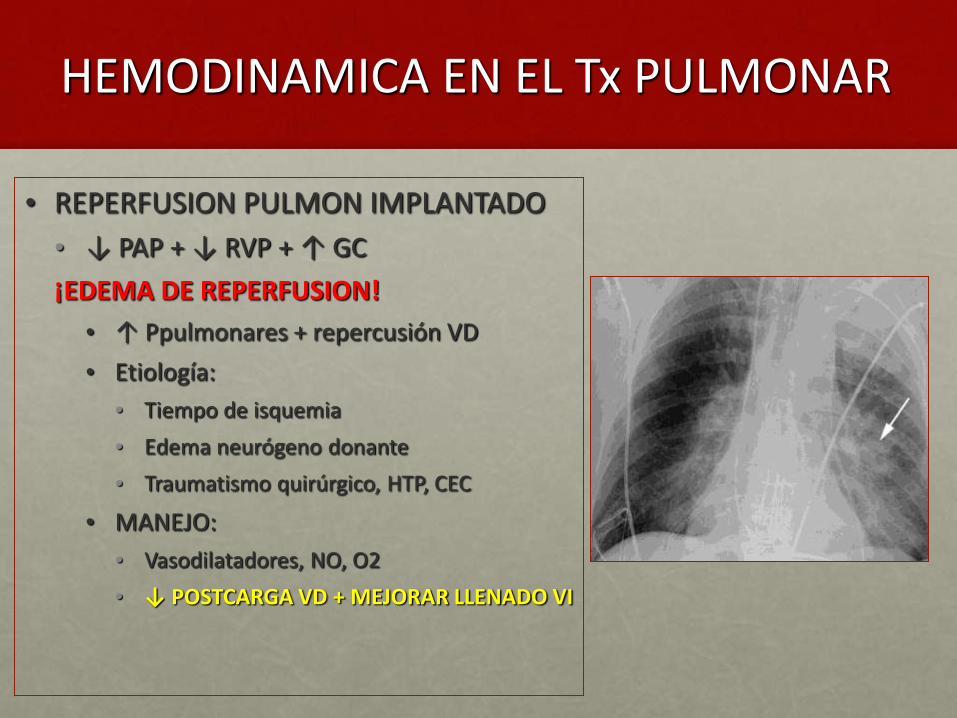
HEMODINAMICA EN EL Tx PULMONAR
• REPERFUSION PULMON IMPLANTADO
• ↓ PAP + ↓ RVP + ↑ GC
¡EDEMA DE REPERFUSION!
• ↑ Ppulmonares + repercusión VD
• Etiología:
• Tiempo de isquemia
• Edema neurógeno donante
• Traumatismo quirúrgico, HTP, CEC
• MANEJO:
• Vasodilatadores, NO, O2
• ↓ POSTCARGA VD + MEJORAR LLENADO VI
Mantenimiento
• O2/AIRE
• FiO2 para mantener SAT O2>90
• Farmacos anestésicos según arte
• Inotrópicos para optimizar estado hemodinámico
• Manta térmica e infusores de sueros calientes
• Protección postural
• Cambio tubo una luz (fibrobroncoscopio: limpieza de secreciones, toma de muestras, comprobación suturas) y Traslado a la U. de Recuperación
Momentos críticos
• RESPIRACION ESPONTANEA → VM
• VENTILACION UNIPULMONAR
• CLAMPAJE ARTERIA PULMONAR
• REPERFUSION PULMON TX
• TRASLADO
POSTOPERATORIO

CONTROL HD Y RESPIRATORIO
• HEMODINAMICO
• PRIORIZAR ESTABILIDAD HD A BALANCE NEGATIVO
• RESTRICCION LIQUIDOS + PAM 50-60 mm Hg
• FLUIDOTERAPIA si:
• IC < 2.5 l/min/m, PCP < 6 mm Hg, PVC < 5 mm Hg
• RESPIRATORIO
• PO2 > 90 con < FIO2
• Ventilación protección pulmonar
• Intentar desconexión lo antes posible
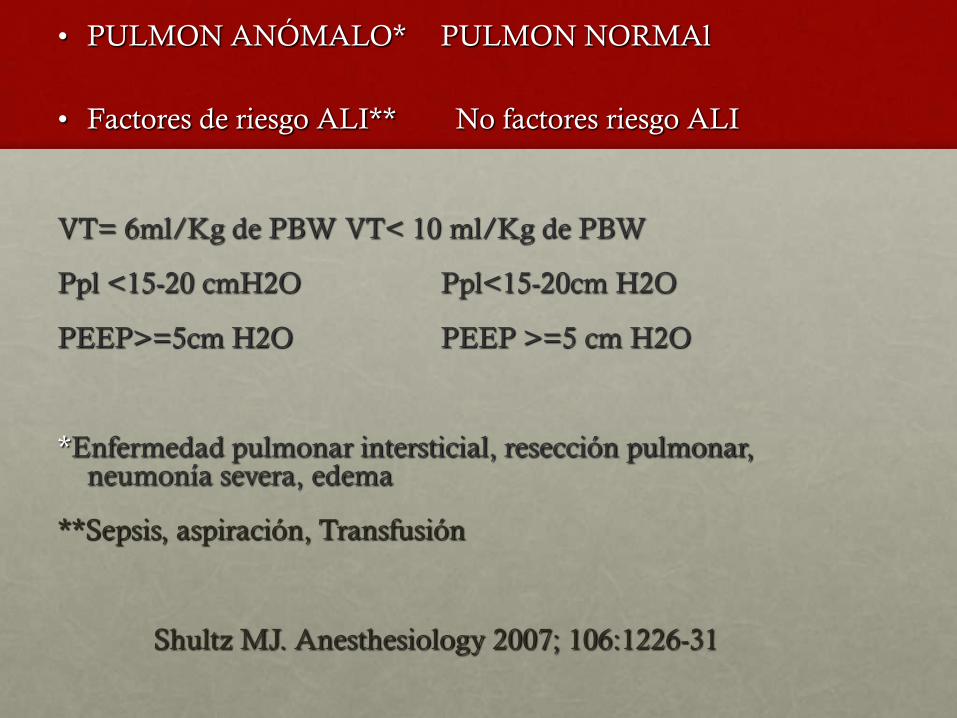
• PULMON ANÓMALO* PULMON NORMAl
• Factores de riesgo ALI** No factores riesgo ALI
VT= 6ml/Kg de PBW VT< 10 ml/Kg de PBW
Ppl <15-20 cmH2O Ppl<15-20cm H2O
PEEP>=5cm H2O PEEP >=5 cm H2O
*Enfermedad pulmonar intersticial, resección pulmonar, neumonía severa, edema
**Sepsis, aspiración, Transfusión
Shultz MJ. Anesthesiology 2007; 106:1226-31

Parámetros para la ventilación
pulmonar selectiva
• “Intentar” FiO2 < 0,8-1
• Disminuir VT
• Pplat < 25 cmH2O VT<= 10 ml/Kg PBW
• Pplat 25-30 cmH2O VT 6-8 ml/Kg PBW
• Pplat > 30 cmH2O VT < 6ML/kg
PEEP>=5 cmH2O
• Ajustar FR para mantener VE
• Reclutamiento
Steinberg K, Kacmarek R
Respiratory Care 2007; 52: 556-567
Anesthesiology 2011; 114: 1102-10

“PEEP should be utilized in the same fashion as any
potent drug, ie dose should be tailored to each patient
according to his needs and response. Since the degree of
parenchymal injury varies from patient to patient the
requeriment for a specific level of PEEP may be
expected to vary. Arbitary selection of an upper (or
lower) limit prevents optimal utilitation of this
potentially live-saving technique”
Kirby 1975
Current opinion in anesthesiology 2012; 25 ,121-122

Receptor
• Grado variable de DPI: 90%
Causa más frecuente de muerte en el postoperatorio inmediato
•Edema, hipoxemia, infiltrados, < complianza, HTP, fracaso VD
•Rechazo agudo
•ECMO / Novalung
• Hiperinsuflación dinámica del nativo
•Hipoxemia, hipercapnia, hipoTA
•Vent para enfisematoso desconexión V independiente
PCV
VT< 6 ml/kg
PEEP moderada
Pinsp <20 cmH2O
Hipercapnia
permisiva
Receptor
• Fracaso de la extubación:
• CEC, DPI, IMC < 17 kg/m2…
• VMNI
• Traqueo percutánea precoz
• Disfunción frénica
• Broncoscopias
VMNI
CoNTRAINDICACIONES
• Inestabilidad hemodinámica
• Fallo multiorgánico
• Inestabilidad ECG con evidencia de isquemia o
arritmias ventriculares
• Necesidad de proteger la vía aérea ó manejo de
secreciones
• Hipoxemia severa

Criterios de suspension VMNI
• Intolerancia a la mascarilla por disconfort o dolor
• Disnea persistente
• No mejoría en la gasometría ( acidosis o hipoxemia
severas)
• Inestabilidad HD ó ECG
• Encefalopatía hipercápnica que no mejora en los
primeros minutos

Conclusiones
V protección
• VT 6-8 ml/k + PEEP 8-10cmH2O
• Circ cerrado de aspiración
• Test de apnea en CPAP, no en T
• Reclutamiento tras desconex
PCV
VT< 6 ml/kg
PEEP moderada
Pinsp <20 cmH2O
Hipercapnia
permisiva
DONANTE.
PREOPERATORIO
RECEPTOR.
POSTOPERATORIO
INMUNOSUPRESION
• SIMULECT (Baxilisimab)
• SOLUMODERIN (Metilprednisolona)
• CICLOSPORINA
• IMUREL (Azatioprina)
• En casos de retrasplante
• Se mantienen mismos fármacos: • FK (Prograf)
• Mofetilmicofenolato (Cellcept)
• Esteroides a las mismas dosis
PROFILAXIS ANTIINFECCIOSA
• PROFILAXIS ANTIBACTERIANA • Amoxicilina-clavulánico o según cultivos previos.
• PROFILAXIS ANTIVÍRICA • En todos (excepto Receptor - / Donante +):
• Ganciclovir
• Si Receptor -/ Donante +: • + Citotec
• PROFILAXIS ANTINEUMOCISTIS CARINI • A partir día 14 del po:
• Septrim forte
• PROFILAXIS ANTIFÚNGICA • Ambisome nebulizado

COMPLICACIONES HD
• SANGRADO
• FR:
• Qx Torácica previa
• Pleurodesis química
• CEC
• Hipotermia
• Manipulación quirúrgica
• TTO
• Medidas conservadoras
• Reintervención:
• Sangrado > 200 ml/h
• Inestabilidad HD
• ARRITMIAS
• Frecuente (80%)
• Supraventriculares:
• FA
• Flutter
• FR:
• Hipoxia, acidosis
• Tx bipulmonar
• > 60 a

COMPLICACIONES HD
• SINDROME BAJO GC
• Se define por:
• IC < 2.5 ml/min/m
• PAM <65 mmHg
• PCP > 18 mmHg
• Oliguria
• Signos de mala perfusión periférica o cerebral
• TTO:
• Optimizar FC, precarga
• DVA
• BCIAo
• DISFUNCION VD
• Se define:
• ↓ GC, PA
• ↑ PTDVD
• TTO:
• ↓ Postcarga: VD
• Precarga: Fluidoterapia
• ↑ Contractilidad:
• Dobutamina
• Adrena, NA → ↑ RVP (mant. PA)
• - PDE: RVS ↑
• Levosimendan, BCIAo
COMPLICACIONES HD
• ESTENOSIS VV. PULMONARES
• Poco frecuente
• Pronóstico fatal
• DESCARTAR SI EDEMA PERSISTENTE
• Dx: ETE, Arteriografía, TC
• Dx Diferencial:
• DPI
• Rechazo
• Infección
• TTO: Reqx
• ESTENOSIS ARTERIA PULMONAR
• Poco frecuente
• Clínica:
• Asintomático
• Persistencia HTP, fracaso VD
• Dx : ETE, Arteriografía
• TTO:
• Conservador
• Angioplastia con balón
• Stent
• Corrección quirúrgica
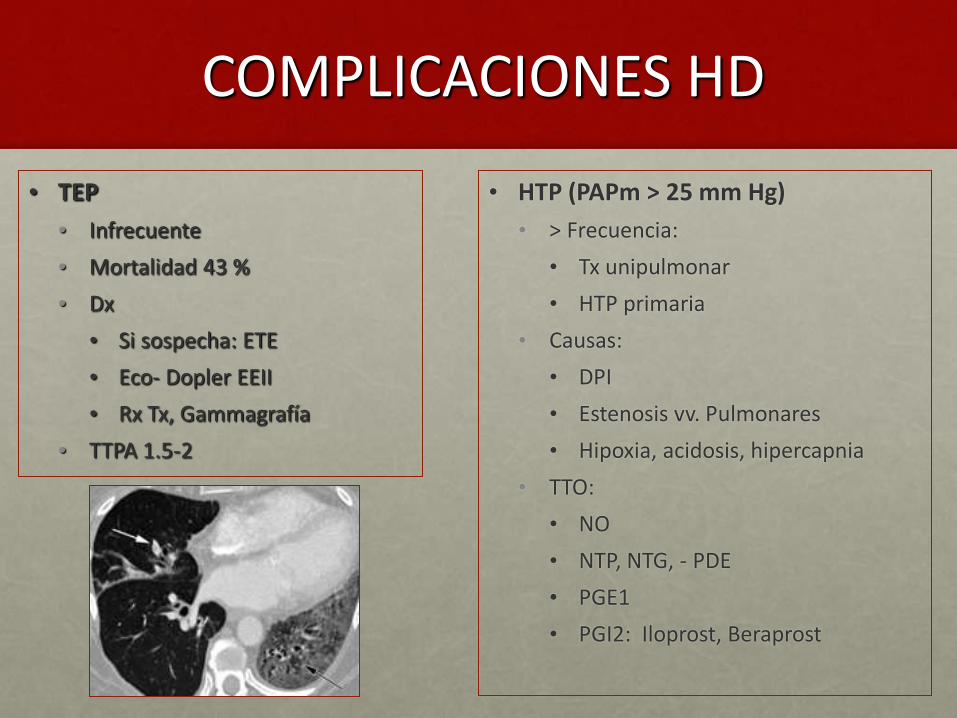
COMPLICACIONES HD
• HTP (PAPm > 25 mm Hg)
• > Frecuencia:
• Tx unipulmonar
• HTP primaria
• Causas:
• DPI
• Estenosis vv. Pulmonares
• Hipoxia, acidosis, hipercapnia
• TTO:
• NO
• NTP, NTG, - PDE
• PGE1
• PGI2: Iloprost, Beraprost
• TEP
• Infrecuente
• Mortalidad 43 %
• Dx
• Si sospecha: ETE
• Eco- Dopler EEII
• Rx Tx, Gammagrafía
• TTPA 1.5-2

COMPLICACIONES RESPIRATORIAS
• DISFUNCION PRECOZ DE INJERTO (DPI)
• RECHAZO AGUDO
• COMPLICACIONES ANASTOMOTICAS
• INFECCIONES
• NEUMOTORAX
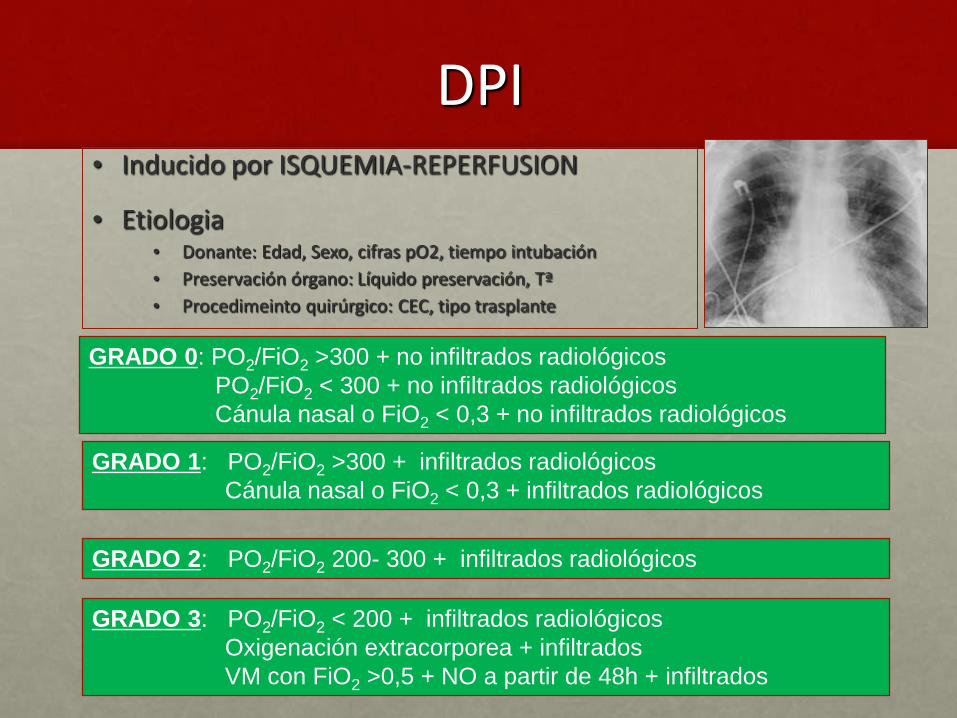
DPI • Inducido por ISQUEMIA-REPERFUSION
• Etiologia • Donante: Edad, Sexo, cifras pO2, tiempo intubación
• Preservación órgano: Líquido preservación, Tª
• Procedimeinto quirúrgico: CEC, tipo trasplante
GRADO 0: PO2/FiO2 >300 + no infiltrados radiológicos
PO2/FiO2 < 300 + no infiltrados radiológicos
Cánula nasal o FiO2 < 0,3 + no infiltrados radiológicos
GRADO 1: PO2/FiO2 >300 + infiltrados radiológicos
Cánula nasal o FiO2 < 0,3 + infiltrados radiológicos
GRADO 2: PO2/FiO2 200- 300 + infiltrados radiológicos
GRADO 3: PO2/FiO2 < 200 + infiltrados radiológicos
Oxigenación extracorporea + infiltrados
VM con FiO2 >0,5 + NO a partir de 48h + infiltrados

DPI
Dx DIFERENCIAL
TRATAMIENTO
- Rechazo hiperagudo humoral
- Obstrucción venas pulmonares
- Edema Cardiogénico
- Neumonía
- TRALI
MANEJO HD
•Restricción fluidos Hto 25-30 %
•Vasopresores sistémicos +/- VD
pulmonares
•Uso preventivo de UF o diálisis”
MANEJO RESPIRATORIO
•Bajos Vt (6-8 ml/kg)
•P. meseta < o = 25-30cm H2O
•PEEP
• FR para mantener adecuada PCO2
. PCV
PREVENCION DE DISFUNCIÓN DEL INJERTO
- VT 6-8ml/k
- PEEP 5-10
- I/E : 1/2-1/3
- NO, PGs, Acetilcisteina??
- Inodilatadores
Objetivo HD→ Disminuir postcarga del VD
→ Mejorar contractilidad VD
→Mejorar llenado de VI
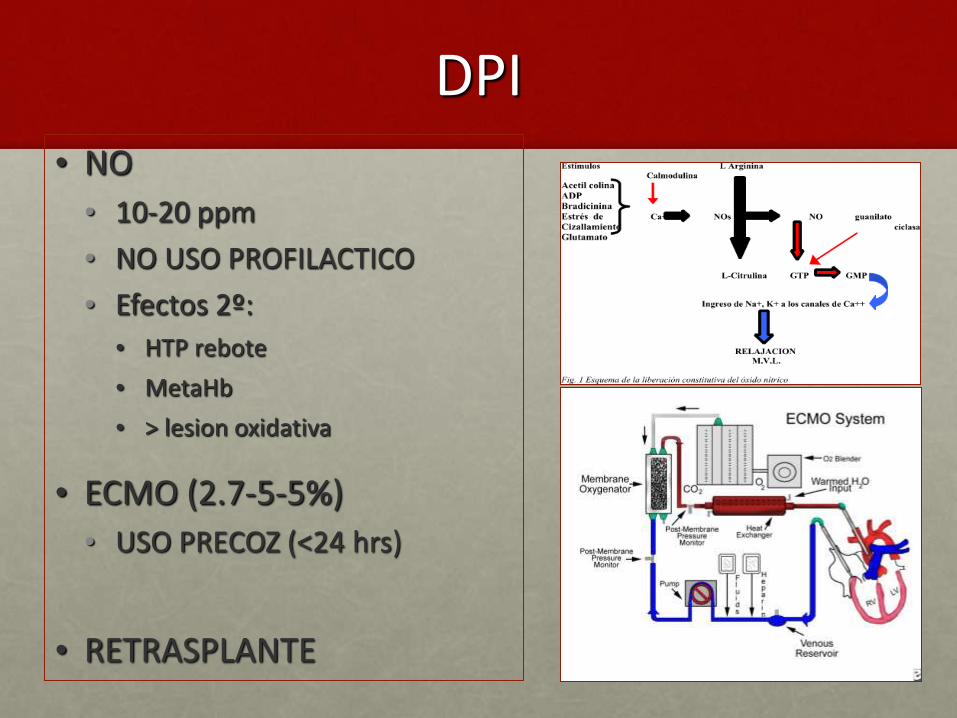
DPI • NO
• 10-20 ppm
• NO USO PROFILACTICO
• Efectos 2º:
• HTP rebote
• MetaHb
• > lesion oxidativa
• ECMO (2.7-5-5%)
• USO PRECOZ (<24 hrs)
• RETRASPLANTE

Novalung como puente al Tx
en HAP
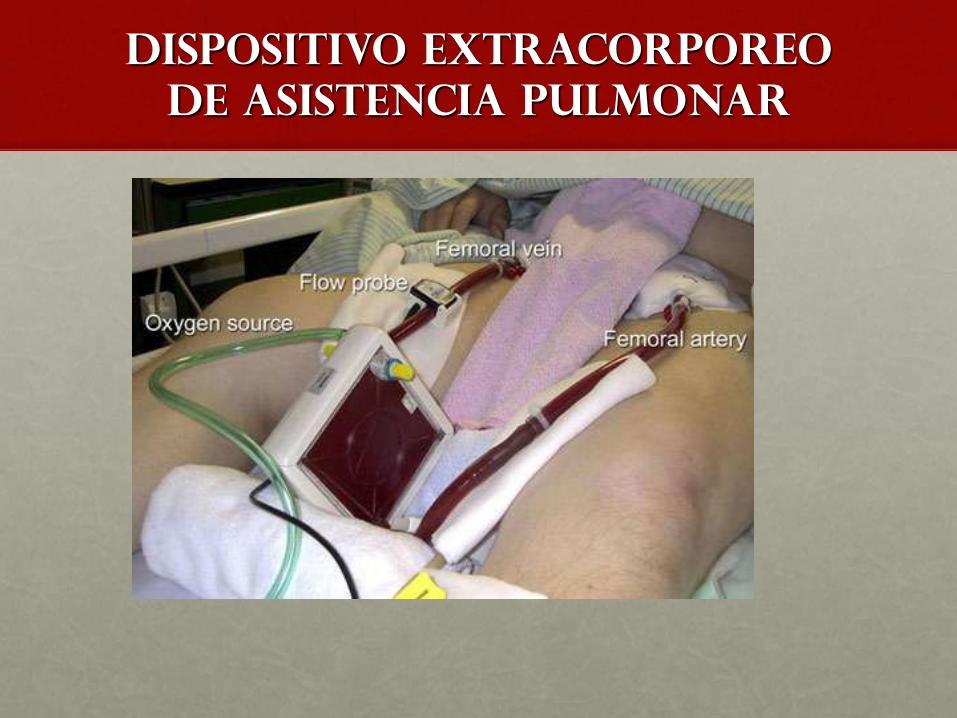
Dispositivo extracorporeo
de asistencia pulmonar
87 87
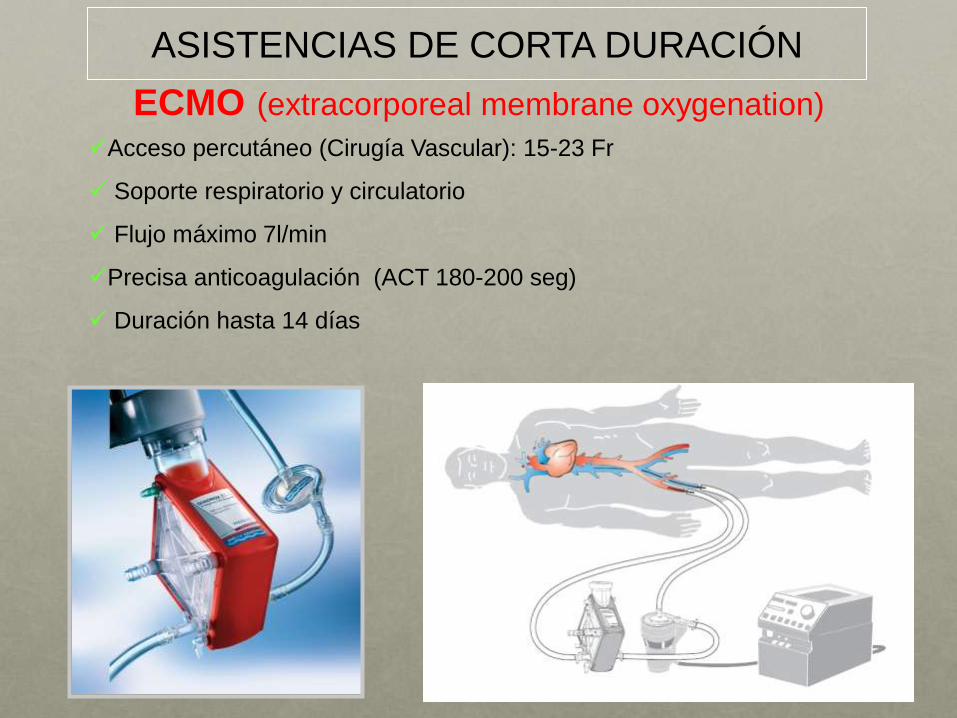
ECMO (extracorporeal membrane oxygenation)
Acceso percutáneo (Cirugía Vascular): 15-23 Fr
Soporte respiratorio y circulatorio
Flujo máximo 7l/min
Precisa anticoagulación (ACT 180-200 seg)
Duración hasta 14 días
ASISTENCIAS DE CORTA DURACIÓN
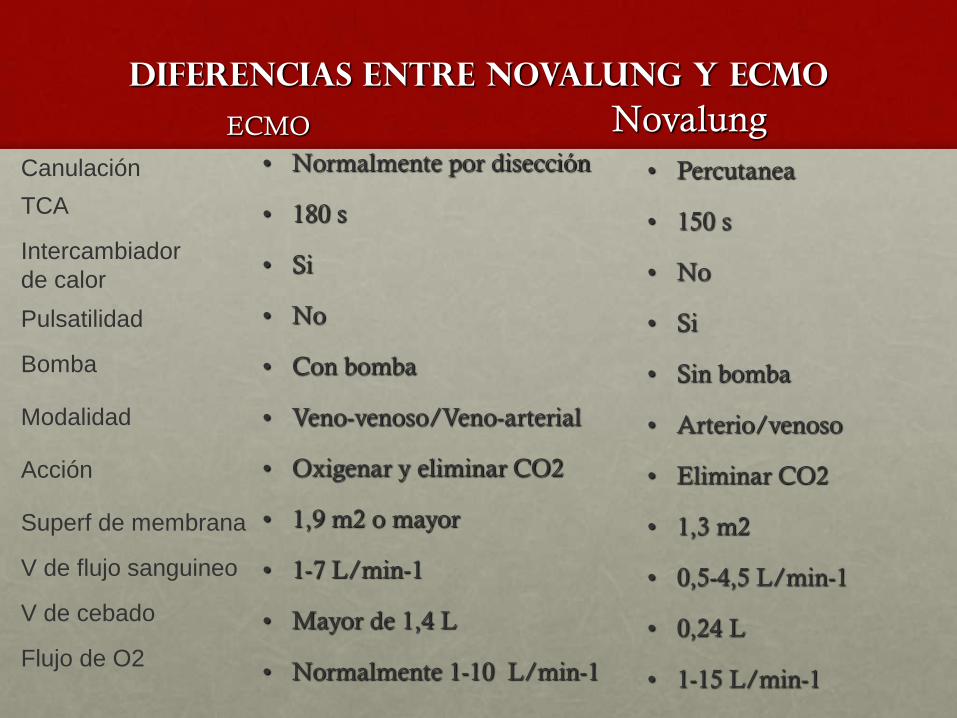
DIFERENCIAS ENTRE novalung Y ecmo
ECMO
• Normalmente por disección
• 180 s
• Si
• No
• Con bomba
• Veno-venoso/Veno-arterial
• Oxigenar y eliminar CO2
• 1,9 m2 o mayor
• 1-7 L/min-1
• Mayor de 1,4 L
• Normalmente 1-10 L/min-1
Novalung
• Percutanea
• 150 s
• No
• Si
• Sin bomba
• Arterio/venoso
• Eliminar CO2
• 1,3 m2
• 0,5-4,5 L/min-1
• 0,24 L
• 1-15 L/min-1
Canulación
TCA
Intercambiador
de calor
Pulsatilidad
Bomba
Modalidad
Acción
Superf de membrana
V de flujo sanguineo
V de cebado
Flujo de O2
Volver a número Nueva búsqueda
Anterior Documento 6 de 23 Siguiente
Otros formatos Cita Texto completo Mostrar entradas duplicadas de otras bases de datos
Mostrar más detalles
11. Doyle TW, Washko GR, Fernandez IE, Nishino M, Okajima Y,
Yamashiro T, Divo MJ, Celli BR, Sciurba FC, Silverman EK, et al.
Interstitial lung abnormalities and reduced exercise capacity. Am
J Respir Crit Care Med 2012;185:756–762.
12. du Bois RM, Weycker D, A lbera C, Bradford WZ, Costabel U, Kartashov
A, Lancaster L, Noble PW, Sahn SA, Szwarcberg J, et al. Six-minute-walk
test in idiopathic pulmonary fibrosis: test validation and minimal clinically
important difference. Am J Respir Crit Care Med 2011;183:1231–1237.
13. Washko GR, Lynch DA, Matsuoka S, Ross JC, Umeoka S, Diaz A ,
Sciurba FC, Hunninghake GM, San Jose Estepar R, Silverman EK,
et al. Identification of early interstitial lung disease in smokers from
the COPDGene study. Acad Radiol 2010;17:48–53.
Copyright ª 2012 by the American Thoracic Society
DOI: 10.1164/ rccm.201202-0222ED
Ext racorporeal Membrane Oxygenat ion as “ Br idge”t o Lung Transplant at ion: What Remains in Ordert o Make It St andard of Care?
Since its introduction into clinical practice, lung transplantation
(LTx) isgradually becoming a worldwide standard treatment forpatients with a broad spectrum of end-stage respiratory diseases(1–3). From 1995 to 2010, more than 30,000 LTx have beenperformed, and it is worth noting that in recent years the num-ber of LTx has been progressively increasing to more than3,000/year in 2010, with a post-transplant graft half-life that
went from 4.7 in the 1990s to 5.9 in the new millennium (4).However, the crude mortality rate of patients awaiting LTx ishigher than mortality for other solid organs. Mortality rate in2009 for patients on the waiting list for LTx was about 14.1% inNorth A merica (www.srtr.org) and 14.7% in Italy (www.airt.it).What are the reasons for these unacceptable mortality rates?
First, patients have to wait for the graft longer than patientswaiting for other organs because of the small number of lungssuitable for transplantation (5). Second is the lack of supportivetherapies that are able to replace respiratory function when
the primary pulmonary diseases evolve from “ respiratory in-sufficiency” to “ respiratory failure,” characterized by refrac-tory hypoxemia and hypercapnia.
HOW TO MANAGE SHORTAGE OF GRAFTS FOR LUNGTRANSPLANTATION
Different linesof investigation have been developed with the goalof increasing lung suitability from the multiorgan donor. In par-ticular, a recent study demonstrated that a lung-protective me-chanical ventilation strategy applied in potential donors mightsignificantly increase the eligibility of the lungs for transplant(6). Moreover, a very innovative technique of ex vivo lung per-
fusion has been shown effective in a clinical trial examining re-conditioning human lungs from high-risk donors, which wouldhave been declined according to conventional criteria (7).
HOW TO “ BRIDGE” PATIENTS TO LUNGTRANSPLANTATION
Invasive mechanical ventilation (IMV), which is usually appliedin these cases, may not fulfill the goals of an optimal bridge toLTx. In fact, IMV is a potential cause of ventilator-associatedpneumonia and ventilator-induced lung injury, which can furtherenhance the initial lung damage and lead to multiorgan dysfunc-
tion, resulting in clinical unsuitability for LTx (“ too sick to betransplanted” ).
Extracorporeal life support (ECLS), such as extracorporealmembrane oxygenation (ECMO), after initially discouraging
experiences, is being progressively recognized as an optimal
strategy to bridge patientswith lung failure to LTx. In fact, ECLS
can potentially provide an adequate level of respiratory supportfor the patient’s requirements, thereby minimizing the clinicalimpact of mechanical ventilation and increasing the chance to
receive a successful LTx (8, 9). A lthough suggested by a number
of case reports (10–12), this hypothesis has never been system-
atically investigated.In this issue of the Journal (pp. 763–768), the article pub-
lished by Dr. Fuehner and colleagues is a welcome next step in
this line of study (13). The authors reported on the outcome of
26 patients awaiting LTx, who developed end-stage respiratory
failure and were supported with ECMO while awake, as bridge
to definitive treatment. These data were compared with those of
34 historical control patients, who were supported traditionally
with IMV as a bridging treatment to LTx. The results of this
study confirmed that ECMO isa very efficient strategy to bridge
patients to LTx and, furthermore, suggested that for this pur-
pose ECMO may be even more efficacious than IMV. In fact,
although both groups were comparable in terms of duration of
support (9 d vs. 15 d) and percentage of patients that received
LTx (23% vs. 29%), survival at six months after LTx was sig-
nificantly higher in the ECMO group (80% vs. 50%, P ¼ 0.02).
Therefore, ECMO wasaseffective as IMV in extending the pre-
transplant life expectancy to increase the chances to receive an
organ, but probably more effective than IMV in preserving
physiological homeostasis, thus preserving the post-transplant
life expectancy, more closely approaching the ideal “ bridge”
to LTx.
Remarkably, in this experience ECMO was applied as an
alternative to IMV with the declared purpose of avoiding its in-
jurious effects, and not asrescue treatment in patients refractory
to conventional therapy. Therefore, it was applied in extubated,
awake patients at an earlier stage of their progression to respi-
ratory failure. Thisstrategy may also allow patients to ambulate,
receive active physiotherapy, and thus potentially be in better
physical condition to ultimately benefit the most from LTx
(14). However, in 27% of cases in the ECMO group, IMV could
not be avoided. Interestingly, these patients had a post-LTx
survival rate of only 43%. From this data stems the ultimate
need to define the optimal timing and clinical criteria to apply
ECLS as bridge to LTx. Starting ECLS too early might increase
the chance of developing ECLS-related complications, whereas
starting too late may not be optimal to prevent multiorgan
dysfunction.The study by Dr. Fuehner and colleagues is particularly pro-
vocative as it is the first attempt, as far asbridging to LTx iscon-
cerned, to systematically compare ECMO and IMV. Previously,
only case series have generally been published (10–12), demon-
strating bridging feasibility but without the chance to measureSupported by the Italian Ministry of University and Research PRIN 2007 and
Fondazione per la Ricerca sulla Fibrosi Cistica–onlus 2008.
Editorials 699
the impact of the results against a control group. This concern
has been, at least in part, addressed in this report by identifying
historical control patients treated with IMV as bridge to LTx.
It isrecognized that the comparison islimited in that the historical
control patients were nonmatched, and the investigation was only
a retrospective observational analysis of few patients, treated in a
single center. A lthough these are relevant methodological issues,
the study by Dr. Fuehner and colleagues has the merit of provid-
ing a solid background and enticing data for the basis of a multi-
center randomized controlled trial (RCT), which is, at this point,
strongly warranted. A n RCT would ultimately clarify an under-
standing of whether the potential increased incidence of ECLS-
related complications outweighs the injuriouseffectsof IMV, asa
bridge to LTx. This step will be key in defining ECLS as the
standard of care in patientswith lung failure waiting for transplant.A re these data sufficient to propose ECLS as standard bridge
procedure for patients waiting for lung transplant? In the lastdecade, there has been a progressive increase in the literatureof publicationson ECLS(seeFigure 1), including ECLSasbridge
to LTx. Interestingly, a relevant increase in publications is gen-erally observed in coincidence with two episodes: (1) the H1N1epidemics (15), and (2) coincident technological advances inECLS (12, 16). This may explain why only very few RCTs have
been published on ECLSfor patientswith respiratory failure, andno RCTs have been performed on strategies to bridge to LTx.
In our view, thecurrent extensiveclinical effortsto improvetheefficacy of the supportive treatments bridging patients to LTxshould adopt the methodological challenges taken by the studies
that have tested strategiesaimingat increasing thenumber of suit-able lungs for transplant from multiorgan donors (6). We ac-knowledge the difficulties of randomizing patients in end-stagerespiratory failure waiting for a transplant, but ultimately clini-cians need to have more solid evidence than that provided byFuehner and colleagues. A lternative methods, including prag-
matic study design and cluster randomization procedure, mayprovide information about ECLS. The technology of mechanicalventilation has evolved and continued to improve over time, andstrategies of protective lung ventilation have improved the per-
formance of mechanical ventilation to support critically il lpatients. A lso, ECLS, which washistorically a costly and imperfecttechnology with significant morbidity, has advanced technologi-cally and come of age—with better performance and an improved
morbidity profile. It is now theoretically truly conceivable to con-sider that ECLS may be more effective and have less overallmorbidity in patients with advanced lung failure. It is time tocompare these two technologies head to head in an RCT.
Author disclosures are available with the text of this article at www.atsjournals.org.
Lor enzo Del Sor bo, M.D.
V. Mar co Ranier i, M.D.
Dipartimento di Anestesiologia e Medicina degli Stati CriticiUniversita di TorinoTorino, I taly
Shaf Keshavjee, M.D.
Toronto L ung Transplant ProgramUniversity of TorontoToronto, Canada
References
1. Cooper JD, Pearson FG, Patterson GA, Todd TR, Ginsberg RJ,
Goldberg M, DeMajo WA. Technique of successful lung transplan-
tation in humans. J Thorac Cardiovasc Surg 1987;93:173–181.
2. Kotloff RM, Thabut G. Lung transplantation. Am J Respir Crit CareMed
2011;184:159–171.
3. Pierre AF, Keshavjee S. Lung transplantation: donor and recipient
critical care aspects. Curr Opin Crit Care 2005;11:339–344.
4. Christie JD, Edwards LB, Kucheryavaya AY, Benden C, Dobbels F,
Kirk R, Rahmel AO, Stehlik J, Hertz MI. The Registry of the Inter-
national Society for Heart and Lung Transplantation: twenty-eighth
adult lung and heart-lung transplant report–2011. J Heart L ung
Transplant 2011;30:1104–1122.
5. Punch JD, Hayes DH, LaPorte FB, McBride V, Seely MS. Organ do-
nation and utilization in the United States, 1996–2005. Am J Trans-
plant 2007;7:1327–1338.
6. Mascia L, Pasero D, Slutsky AS, ArguisMJ, Berardino M, Grasso S, Munari
M, Boifava S, Cornara G, Della Corte F, et al. Effect of a lung protective
strategy for organ donors on eligibility and availability of lungs for
transplantation: a randomized controlled trial. JAMA 2010;304:2620–2627.
7. Cypel M, Yeung JC, Liu M, A nraku M, Chen F, Karolak W, Sato M,
Laratta J, Azad S, Madonik M, et al. Normothermic ex vivo lung per-
fusion in clinical lung transplantation. N Engl J Med 2011;364:1431–1440.
8. Cypel M, Keshavjee S. Extracorporeal life support as a bridge to lung
transplantation. Clin Chest Med 2011;32:245–251.
9. Del Sorbo L, Boffini M, Rinaldi M, Ranieri VM. Bridging to lung trans-
plantation by extracorporeal support. Minerva Anestesiol 2012;78:243–250.
Figure 1. Number of articles on extracorporeal
life support (ECLS) (gray line, left vertical axis)
and ECLS as bridge to LTx (black line, right vertical
axis), published on PubMed for each year from
2000 until 2011.
700 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 185 2012
Extracorporeal Mem brane Oxygenat ion as "Bridge" to Lung Transplantat ion: W hat R… Abrir con el lector de PDF
Volver a número Nueva búsqueda
Anterior Documento 6 de 23 Siguiente
Otros formatos Cita Texto completo Mostrar entradas duplicadas de otras bases de datos
Mostrar más detalles
11. Doyle TW, Washko GR, Fernandez IE, Nishino M, Okajima Y,
Yamashiro T, Divo MJ, Celli BR, Sciurba FC, Silverman EK, et al.
Interstitial lung abnormalities and reduced exercise capacity. Am
J Respir Crit Care Med 2012;185:756–762.
12. du Bois RM, Weycker D, Albera C, Bradford WZ, Costabel U, Kartashov
A, Lancaster L, NoblePW, Sahn SA, SzwarcbergJ, et al. Six-minute-walk
test in idiopathic pulmonary fibrosis: test validation and minimal clinically
important difference. Am J Respir Crit CareMed 2011;183:1231–1237.
13. Washko GR, Lynch DA, Matsuoka S, Ross JC, Umeoka S, Diaz A,
Sciurba FC, Hunninghake GM, San Jose Estepar R, Silverman EK,
et al. Identification of early interstitial lung disease in smokers from
the COPDGene study. Acad Radiol 2010;17:48–53.
Copyright ª 2012 by the American Thoracic Society
DOI: 10.1164/ rccm.201202-0222ED
Ext racorporeal Membrane Oxygenat ion as “ Bridge”t o Lung Transplant at ion: What Remains in Ordert o Make It St andard of Care?
Since its introduction into clinical practice, lung transplantation(LTx) isgradually becoming aworldwide standard treatment forpatientswith a broad spectrum of end-stage respiratory diseases(1–3). From 1995 to 2010, more than 30,000 LTx have beenperformed, and it is worth noting that in recent years the num-
ber of LTx has been progressively increasing to more than3,000/year in 2010, with a post-transplant graft half-life thatwent from 4.7 in the 1990s to 5.9 in the new millennium (4).
However, the crude mortality rate of patients awaiting LTx ishigher than mortality for other solid organs. Mortality rate in2009 for patientson the waiting list for LTx wasabout 14.1% in
North America (www.srtr.org) and 14.7% in Italy (www.airt.it).What are the reasons for these unacceptable mortality rates?
First, patients have to wait for the graft longer than patientswaiting for other organs because of the small number of lungs
suitable for transplantation (5). Second isthe lack of supportivetherapies that are able to replace respiratory function whenthe primary pulmonary diseases evolve from “ respiratory in-
sufficiency” to “ respiratory failure,” characterized by refrac-tory hypoxemia and hypercapnia.
HOW TO MANAGE SHORTAGE OF GRAFTS FOR LUNG
TRANSPLANTATION
Different linesof investigation havebeen developed with thegoalof increasing lung suitability from the multiorgan donor. In par-ticular, a recent study demonstrated that a lung-protective me-chanical ventilation strategy applied in potential donors might
significantly increase the eligibility of the lungs for transplant(6). Moreover, a very innovative technique of ex vivo lung per-fusion has been shown effective in a clinical trial examining re-conditioning human lungs from high-risk donors, which wouldhave been declined according to conventional criteria (7).
HOW TO “BRIDGE” PATIENTS TO LUNG
TRANSPLANTATION
Invasive mechanical ventilation (IMV), which isusually appliedin these cases, may not fulfill the goals of an optimal bridge toLTx. In fact, IMV is a potential cause of ventilator-associatedpneumonia and ventilator-induced lung injury, which can further
enhance the initial lung damage and lead to multiorgan dysfunc-tion, resulting in clinical unsuitability for LTx (“ too sick to betransplanted” ).
Extracorporeal life support (ECLS), such as extracorporealmembrane oxygenation (ECMO), after initially discouragingexperiences, is being progressively recognized as an optimal
strategy tobridgepatientswith lungfailure toLTx. In fact, ECLScan potentially provide an adequate level of respiratory supportfor the patient’s requirements, thereby minimizing the clinicalimpact of mechanical ventilation and increasing the chance to
receive asuccessful LTx (8, 9). A lthough suggested by anumber
of case reports (10–12), this hypothesis has never been system-
atically investigated.
In this issue of the Journal (pp. 763–768), the article pub-
lished by Dr. Fuehner and colleagues is a welcome next step in
this line of study (13). The authors reported on the outcome of
26 patients awaiting LTx, who developed end-stage respiratory
failure and were supported with ECMO while awake, asbridge
to definitive treatment. These data were compared with those of
34 historical control patients, who were supported traditionally
with IMV as a bridging treatment to LTx. The results of this
study confirmed that ECMO isavery efficient strategy to bridge
patients to LTx and, furthermore, suggested that for this pur-
pose ECMO may be even more efficacious than IMV. In fact,
although both groups were comparable in terms of duration of
support (9 d vs. 15 d) and percentage of patients that received
LTx (23% vs. 29%), survival at six months after LTx was sig-
nificantly higher in the ECMO group (80% vs. 50%, P ¼ 0.02).
Therefore, ECMO wasaseffective asIMV in extending thepre-
transplant life expectancy to increase the chances to receive an
organ, but probably more effective than IMV in preserving
physiological homeostasis, thus preserving the post-transplant
life expectancy, more closely approaching the ideal “bridge”
to LTx.Remarkably, in this experience ECMO was applied as an
alternative to IMV with the declared purpose of avoiding its in-
juriouseffects, and not asrescue treatment in patientsrefractory
to conventional therapy. Therefore, it wasapplied in extubated,
awake patients at an earlier stage of their progression to respi-
ratory failure. Thisstrategy may also allow patientsto ambulate,
receive active physiotherapy, and thus potentially be in better
physical condition to ultimately benefit the most from LTx
(14). However, in 27% of cases in the ECMO group, IMV could
not be avoided. Interestingly, these patients had a post-LTx
survival rate of only 43%. From this data stems the ultimate
need to define the optimal timing and clinical criteria to apply
ECLSasbridge to LTx. Starting ECLStoo early might increase
the chance of developing ECLS-related complications, whereas
starting too late may not be optimal to prevent multiorgan
dysfunction.The study by Dr. Fuehner and colleagues isparticularly pro-
vocative asit isthe first attempt, asfar asbridging to LTx iscon-
cerned, to systematically compare ECMO and IMV. Previously,
only case series have generally been published (10–12), demon-
strating bridging feasibility but without the chance to measureSupported by the Italian Ministry of University and Research PRIN 2007 and
Fondazione per la Ricerca sulla Fibrosi Cistica–onlus 2008.
Editorials 699
the impact of the results against a control group. This concern
hasbeen, at least in part, addressed in this report by identifying
historical control patients treated with IMV as bridge to LTx.
It isrecognized that thecomparison islimited in that thehistorical
control patientswere nonmatched, and the investigation wasonly
a retrospective observational analysisof few patients, treated in a
single center. A lthough these are relevant methodological issues,
the study by Dr. Fuehner and colleagues hasthe merit of provid-
ing a solid background and enticing data for the basis of a multi-
center randomized controlled trial (RCT), which is, at this point,
strongly warranted. An RCT would ultimately clarify an under-
standing of whether the potential increased incidence of ECLS-
related complicationsoutweighsthe injuriouseffectsof IMV, asa
bridge to LTx. This step will be key in defining ECLS as the
standard of care in patientswith lung failurewaitingfor transplant.Are these data sufficient to propose ECLSasstandard bridge
procedure for patients waiting for lung transplant? In the last
decade, there has been a progressive increase in the literatureof publicationson ECLS(seeFigure1), includingECLSasbridge
to LTx. Interestingly, a relevant increase in publications is gen-erally observed in coincidence with two episodes: (1) the H1N1
epidemics (15), and (2) coincident technological advances inECLS(12, 16). This may explain why only very few RCTs havebeen published on ECLSfor patientswith respiratory failure, andno RCTs have been performed on strategies to bridge to LTx.
Inour view, thecurrent extensiveclinical effortsto improvetheefficacy of the supportive treatments bridging patients to LTx
should adopt the methodological challengestaken by the studiesthat havetestedstrategiesaimingat increasingthenumber of suit-able lungs for transplant from multiorgan donors (6). We ac-knowledge the difficulties of randomizing patients in end-stagerespiratory failure waiting for a transplant, but ultimately clini-
cians need to have more solid evidence than that provided byFuehner and colleagues. Alternative methods, including prag-matic study design and cluster randomization procedure, mayprovide information about ECLS. The technology of mechanical
ventilation hasevolved and continued to improve over time, andstrategies of protective lung ventilation have improved the per-formance of mechanical ventilation to support critically ill
patients. Also, ECLS, which washistorically acostly and imperfecttechnology with significant morbidity, has advanced technologi-cally and come of age—with better performance and an improved
morbidity profile. It is now theoretically truly conceivable to con-sider that ECLS may be more effective and have less overallmorbidity in patients with advanced lung failure. It is time to
compare these two technologies head to head in an RCT.
Author disclosures are available with the text of thisarticle at www.atsjournals.org.
Lorenzo Del Sorbo, M.D.
V. Marco Ranier i, M.D.
Dipartimento di Anestesiologia e Medicina degli Stati CriticiUniversita di TorinoTorino, Italy
Shaf Keshavjee, M.D.
Toronto Lung Transplant ProgramUniversity of TorontoToronto, Canada
References
1. Cooper JD, Pearson FG, Patterson GA, Todd TR, Ginsberg RJ,
Goldberg M, DeMajo WA. Technique of successful lung transplan-
tation in humans. J Thorac Cardiovasc Surg 1987;93:173–181.
2. Kotloff RM, Thabut G. Lung transplantation. Am JRespir Crit CareMed
2011;184:159–171.
3. Pierre AF, Keshavjee S. Lung transplantation: donor and recipient
critical care aspects. Curr Opin Crit Care 2005;11:339–344.
4. Christie JD, Edwards LB, Kucheryavaya AY, Benden C, Dobbels F,
Kirk R, Rahmel AO, Stehlik J, Hertz MI. The Registry of the Inter-
national Society for Heart and Lung Transplantation: twenty-eighth
adult lung and heart-lung transplant report–2011. J Heart Lung
Transplant 2011;30:1104–1122.
5. Punch JD, Hayes DH, LaPorte FB, McBride V, Seely MS. Organ do-
nation and utilization in the United States, 1996–2005. Am J Trans-
plant 2007;7:1327–1338.
6. MasciaL, Pasero D, Slutsky AS, ArguisMJ, Berardino M, Grasso S, Munari
M, Boifava S, Cornara G, Della Corte F, et al. Effect of a lung protective
strategy for organ donors on eligibility and availability of lungs for
transplantation: arandomizedcontrolled trial. JAMA 2010;304:2620–2627.
7. Cypel M, Yeung JC, Liu M, Anraku M, Chen F, Karolak W, Sato M,
Laratta J, Azad S, Madonik M, et al. Normothermic ex vivo lung per-
fusion in clinical lung transplantation. N Engl JMed 2011;364:1431–1440.
8. Cypel M, Keshavjee S. Extracorporeal life support as a bridge to lung
transplantation. Clin Chest Med 2011;32:245–251.
9. Del Sorbo L, Boffini M, Rinaldi M, Ranieri VM. Bridging to lung trans-
plantation by extracorporeal support. MinervaAnestesiol 2012;78:243–250.
Figure 1. Number of articles on extracorporeal
life support (ECLS) (gray line, left vertical axis)
and ECLSas bridge to LTx (black line, right vertical
axis), published on PubMed for each year from
2000 until 2011.
700 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CAREMEDICINE VOL 185 2012
Extracorporeal Membrane Oxygenation as "Bridge" to Lung Transplantation: What R… Abrir con el lector de PDF
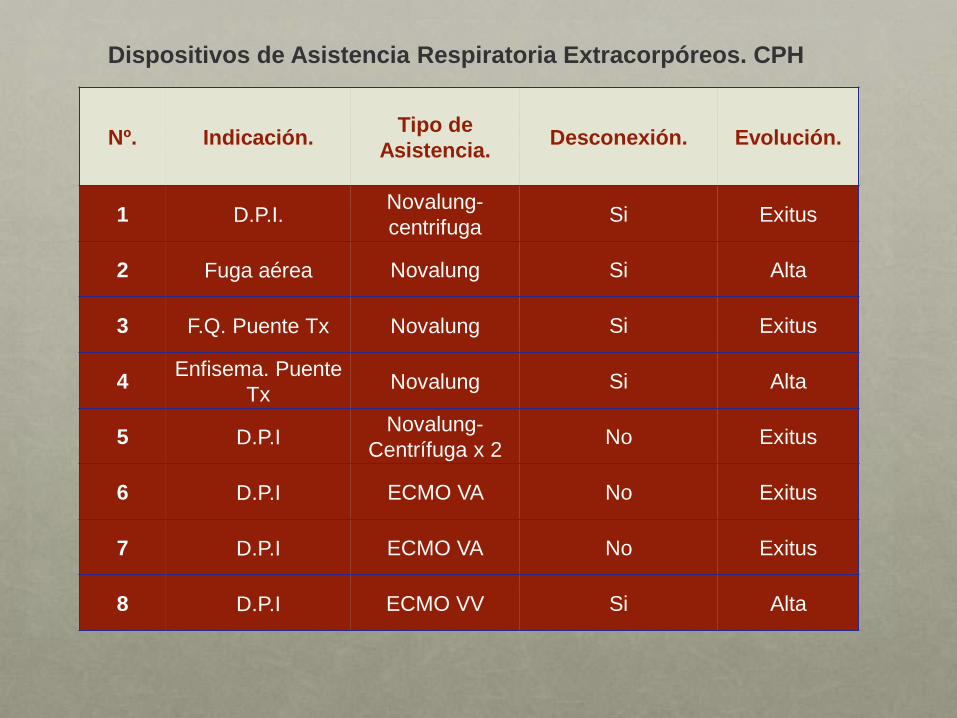
Dispositivos de Asistencia Respiratoria Extracorpóreos. CPH
Nº. Indicación. Tipo de
Asistencia. Desconexión. Evolución.
1 D.P.I. Novalung-
centrifuga Si Exitus
2 Fuga aérea Novalung Si Alta
3 F.Q. Puente Tx Novalung Si Exitus
4 Enfisema. Puente
Tx Novalung Si Alta
5 D.P.I Novalung-
Centrífuga x 2 No Exitus
6 D.P.I ECMO VA No Exitus
7 D.P.I ECMO VA No Exitus
8 D.P.I ECMO VV Si Alta
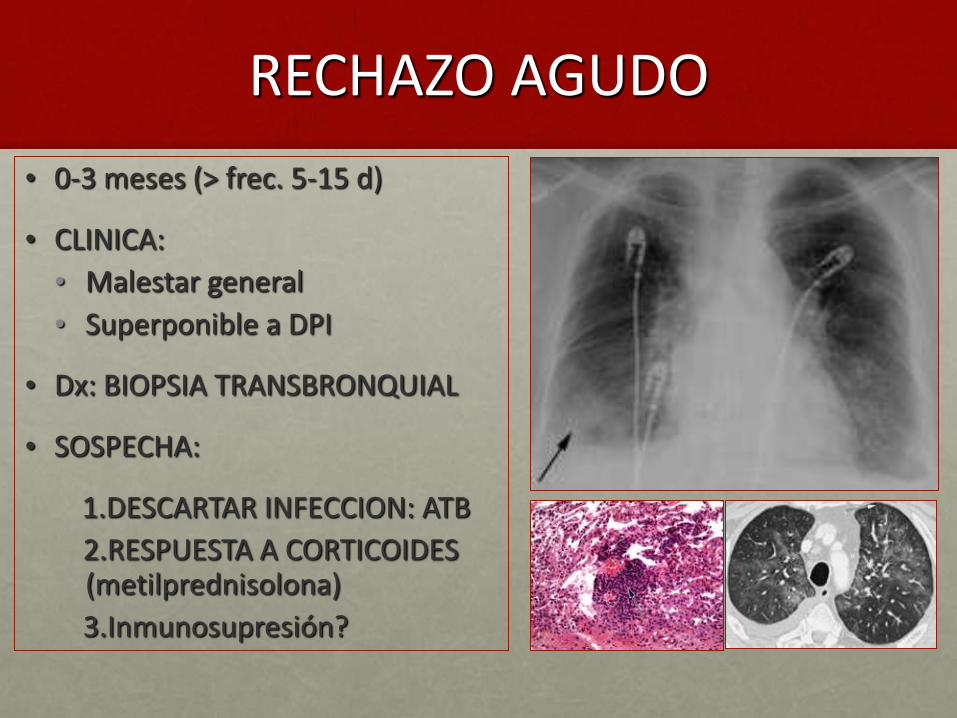
RECHAZO AGUDO
• 0-3 meses (> frec. 5-15 d)
• CLINICA:
• Malestar general
• Superponible a DPI
• Dx: BIOPSIA TRANSBRONQUIAL
• SOSPECHA:
1.DESCARTAR INFECCION: ATB
2.RESPUESTA A CORTICOIDES (metilprednisolona)
3.Inmunosupresión?

OTRAS COMPLICACIONES
• ANASTOMOSIS BRONQUIAL
• INFECCIONES

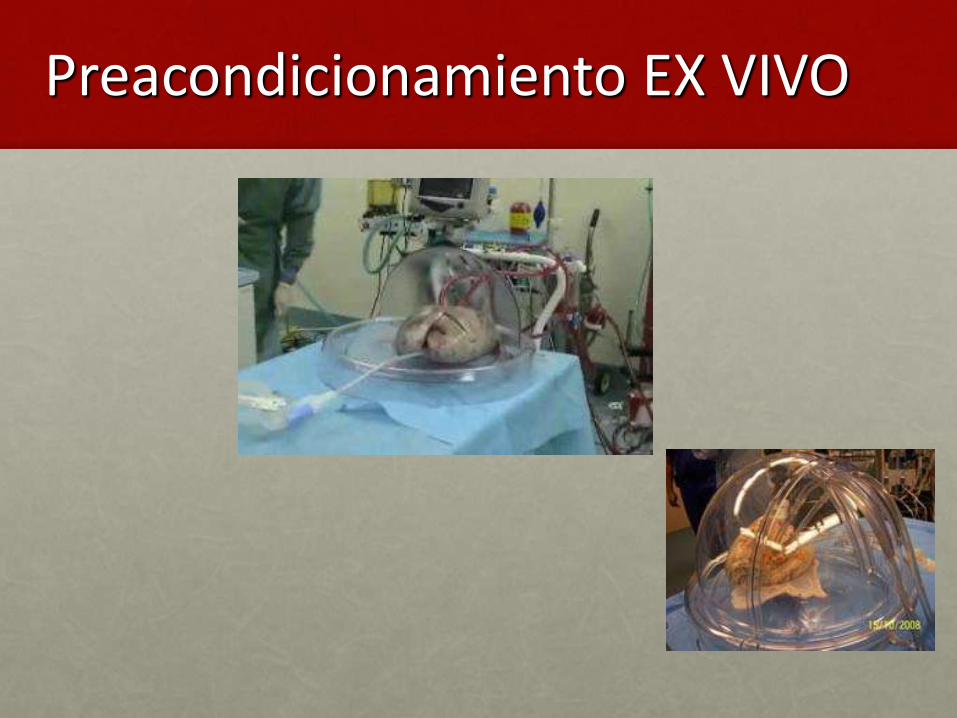
Preacondicionamiento EX VIVO